
Abstract
Deferoxamine (DFO) has been in use for half a century as a Food and Drug Administration-approved iron chelator, but recent studies indicate a variety of properties that could expand this drug's application into the fields of tissue and regenerative engineering. DFO has been implicated as an angiogenic agent in studies on ischemia, wound healing, and bone regeneration because of its ability to upregulate hypoxia-inducible factor-1 alpha (HIF-1α) and other key downstream angiogenic factors. DFO has also demonstrated antioxidant capabilities unrelated to its iron-chelating properties, making it a potential modulator of the oxidative stress involved in the inflammation response. Together, these properties make DFO a potential bioactive molecule to promote wound healing and enhance tissue integration of biomaterials in vivo.
Impact Statement
Deferoxamine (DFO) is approved by the Food and Drug Administration as an iron chelator and is been used to treat iron overload. Recent studies indicate that DFO may have important applications in the growing field of tissue regeneration because of its unique properties of downregulating inflammation while promoting vascularization, thereby enhancing wound healing in vivo.
Introduction
Deferoxamine (DFO), also referred to as desferoxamine, desferrioxamine, or its brand name Desferal, was approved by the Food and Drug Administration (FDA) in 1968 for use as an iron chelator. Although iron is present only in trace amounts in the human body, it has a role in several vital functions including oxygen transport, oxygen sensing, electron sensing, electron transfer, energy metabolism, and DNA synthesis.1–6 However, too much iron can lead to unliganded or incompletely liganded iron ions that can react with peroxides to form reactive oxygen species (ROS). These radicals can cause considerable damage should they contact important biological compounds such as lipid membranes, proteins, or nucleic acids. 7
Iron chelators bind to unliganded or incompletely liganded iron, rendering the ion inert. Iron can coordinate six ligands in an octahedral geometry. Molecules with the highest affinity for iron are hexadentate, binding to iron in a 1:1 (chelator:iron) ratio. Other chelators can be bidentate (3:1) or tridentate (2:1), but these types of ligation are less effective as they can potentially promote free radical generation by redox cycling. 8 DFO is hexadentate, giving it a high affinity for iron (Fig. 1). Upon contacting an iron ion, DFO's straight-chained structure twists, then binds itself to the ion by means of the three hydroxamic acid groups. 9

Chemical structure of DFO. DFO, deferoxamine.
Most commonly, iron chelators are used to treat patients with diseases that require treatment with chronic transfusion therapy. Thalassemia is a genetic blood disorder that causes abnormal hemoglobin production and is often treated with regular red blood cell (RBC) transfusions to combat anemia and bone marrow expansion, two common adverse effects of the disease. 10 Sickle cell disease is a genetic blood disorder that causes production of a mutated form of hemoglobin that distorts RBCs into a crescent shape, instead of the natural disk shape. Sickle cell patients require repeated blood transfusions to supplement the body with healthy RBCs. 11
Myelodysplasia syndromes are a group of disorders in which blood cells in the bone marrow do not mature to healthy blood cells, and these patients generally develop long-term dependence on blood transfusions. 12 Chronic transfusion therapy increases the level of nontransferrin bound iron in the circulatory system that can lead to a toxic accumulation of iron in the liver, spleen, endocrine organs, and the myocardium. 13 DFO has been shown to be effective at trapping and eliminating unbound iron resulting from these hematologic diseases. 14
Increased levels of iron have also been implicated in increasing the risk of cancer. 15 Cancer cells grow and divide rapidly and therefore have a greater metabolic demand for iron than most healthy cells. 16 Consequently, researchers have taken an interest in what effect iron chelators may have on cancerous cells. It has been reported that the general mechanisms by which iron chelators target tumor cells include inhibition of cellular iron uptake and promotion of iron mobilization, inhibition of the rate-limiting, iron-containing enzyme ribonucleotide reductase, induction of cell cycle arrest, inhibition of the epithelial–mesenchymal transition that is critical for metastasis, and by modulating endoplasmic reticulum stress. 16
Iron chelators also have the ability to remove metals essential for tumor growth and to promote redox cycling of bound iron, two additional reasons they have been suggested for potential use as anticancer drugs.17,18 DFO was the focus in early studies of the effect of iron chelators on cancer because of its FDA approval and proven clinical safety and efficacy as a chelator. Although studies showed that the ability of DFO to moderately slow tumor growth, the significant impact it has on the course of the disease as a whole has not been confirmed. 17
DFO has been used clinically to treat a variety of iron overload diseases, often requiring multiple long-term infusions. 19 Even with continuous dosing, DFO use has minimal detrimental side effects and has not been linked to conclusive evidence of acute liver toxicity. 19 In addition, a review of the literature concluded that there was no sufficient evidence to suggest that DFO administration during pregnancy causes DFO toxicity in infants. 20
Iron chelators have also been proposed for use in diseases mediated by oxidative stress including hepatic iron-overload disorders, infectious and neurologic diseases, diabetes, inflammation, and atherosclerosis.21–26 DFO has been at the center of much of this research and, so far, has shown therapeutic value in the treatment of diabetes and atherosclerosis.25,27, In addition to its iron-chelating abilities, DFO has also been examined for its angiogenic and antioxidant properties, and this review will highlight the expanding literature in this field.
Angiogenic Properties of DFO
The circulatory system typically provides peripheral cells with nutrients and a method of waste elimination that, together, help cells execute normal functions. The distance between a cell and the closest blood vessel is limited by the laws governing the rate of diffusion. Cells residing too far from a vessel will not receive the necessary nutrients, and a buildup of metabolites will eventually damage isolated cells. The same laws have limited the thickness of viable tissue grafts and pose an obstacle to tissue-organ regeneration. Therefore, the ability to induce the formation of blood vessels is of great interest to the field of regenerative engineering.
Angiogenesis refers to the normal formation of blood vessels during growth or reparation of damaged tissues. In adults, normal angiogenesis is tightly regulated and reserved for the ovarian cycle and wound healing, though these mechanisms have also been known to be hijacked by rapidly dividing tumors. 28 Key signaling molecules in the induction of angiogenesis include hypoxia-inducible factor-1 alpha (HIF-1α) and vascular endothelial growth factor (VEGF). HIF-1α is an oxygen-sensitive molecule whose expression is upregulated in hypoxic conditions which, in turn, regulates several target genes including VEGF. 29 VEGF acts as a chemotactic agent, an endothelial cell mitogen, and an inducer of vascular permeability. 30
These and other factors provide a local environment that favors the formation of new blood vessels. Efforts to induce or control these events for regenerative engineering applications could minimize the deleterious effects of inflammation, enhance graft or scaffold integration with the host tissue, promote long-term material assimilation, and permit the future clinical success of complex, multilayered tissue grafts.
DFO and ischemia
Ischemia is defined as an inadequate blood supply to a tissue. Without a steady supply of oxygen from the blood, cells cannot generate enough ATP. If these suboptimal conditions last for extended periods of time, ischemic injury can damage the affected tissue, rendering it dysfunctional. Conditions such as high blood pressure and high cholesterol can block blood flow and oxygen to various tissues and put patients at risk for ischemic injury. If blood flow to the brain and heart are blocked, it can result in lethal strokes and heart attacks. With an ever-rising incidence of these conditions, researchers have investigated methods of alleviating ischemia. Prompt return of blood flow to ischemic tissues after stroke or heart attack may be able to salvage the affected tissue and return some functions to the damaged area.
Over the years, the response of DFO to ischemia has been studied in a number of animal models. Two early studies investigated the effects of DFO on angiogenesis and neovascularization using rabbit and sheep models. Rabbit hindlimb ischemia was induced by removal of the left external iliac and femoral arteries. Experimental subjects received an intramuscular injection of DFO encapsulated in fibrin mesh. Analysis of angiography taken immediately post-op and 1-month post-op revealed that the number of arteries and arterioles increased in both control and DFO groups. However, the capillary density measured 1-month post-op was significantly higher in the DFO group compared with the presurgical value and was significantly lower in the post-op control group compared with the presurgical value, indicating that DFO had a role in inducing and sustaining small blood vessel formation. 31
In the sheep model, ischemia was induced in the latissimus dorsi muscle by severing all vessels from the intercostal arteries. Ischemic muscles were then either left untreated or treated with fibrin with and without DFO. After 2 months, the tissue samples were harvested. The samples revealed a marked increase in capillary density in the DFO-treated group compared with the control and fibrin-only groups and compared with the presurgical measurement. 32 The mechanism by which DFO stimulated this neovascularization was not investigated in these studies; however, these earlier studies showed that DFO could have important clinical benefits in addition to its iron-chelating abilities.
In an attempt to elucidate the aforementioned mechanism, Ikeda et al. investigated whether DFO had an Akt and endothelial nitric oxide synthesis (eNOS)-dependent effect since it had been established that the activation of eNOS played a role in angiogenesis in endothelial cells. 33 In vitro, human aortic endothelial cells (HAECs) treated with 1–100 μM DFO showed increased expression of eNOS and increased Akt phosphorylation. DFO also promoted tube formation, proliferation, and migration of HAECs, confirming the compound's ability to stimulate endothelial cell functions.
In a mouse unilateral hindlimb ischemia model, DFO increased capillary density and number of arterioles 14 days post-op compared with vehicle, concurrent with the results of the previously mentioned studies. In addition, endothelial cell proliferation increased, and oxidative stress and apoptosis decreased in DFO-treated ischemic muscles. However, in an eNOS-deficient mouse unilateral hindlimb ischemia model, the ischemia-to-nonischemia blood flow ratio was not found to be different between vehicle and DFO-treated mice, indicating that DFO activation of angiogenesis does indeed have an eNOS-dependent aspect. 34
The role of eNOS activation in DFO-mediated angiogenesis was further demonstrated in a study that investigated the effect of DFO nanoparticles on microvascular regeneration in a mouse orthotopic tracheal transplant model. During the transplant procedures, lecithin nanoparticles with and without encapsulated DFO was topically applied to the trachea. Microvascular perfusion images showed that DFO treatment resulted in >90% perfused area compared with <20% in the nontreated control group at 3 and 10 days post-transplant (Fig. 2). Reverse transcriptase polymerase chain reaction of day 3 post-transplant samples showed increased levels of the angiogenic factors, placental growth factor, and stromal cell-derived factor-1α (SDF-1α) in the DFO group. A twofold increase in eNOS expression in the tracheal endothelial cells was also observed for the DFO group compared with the vehicle group. 35 The ability of this simple topical solution to enhance neovascularization in transplanted tissue could have an enormous impact on the success of transplant and graft procedures. With transplanted tissue already having to survive the shock of an invasive procedure and potential attacks by the host immune response, the establishment of adequate reperfusion of the tissue could help tip the scale away from rejection.
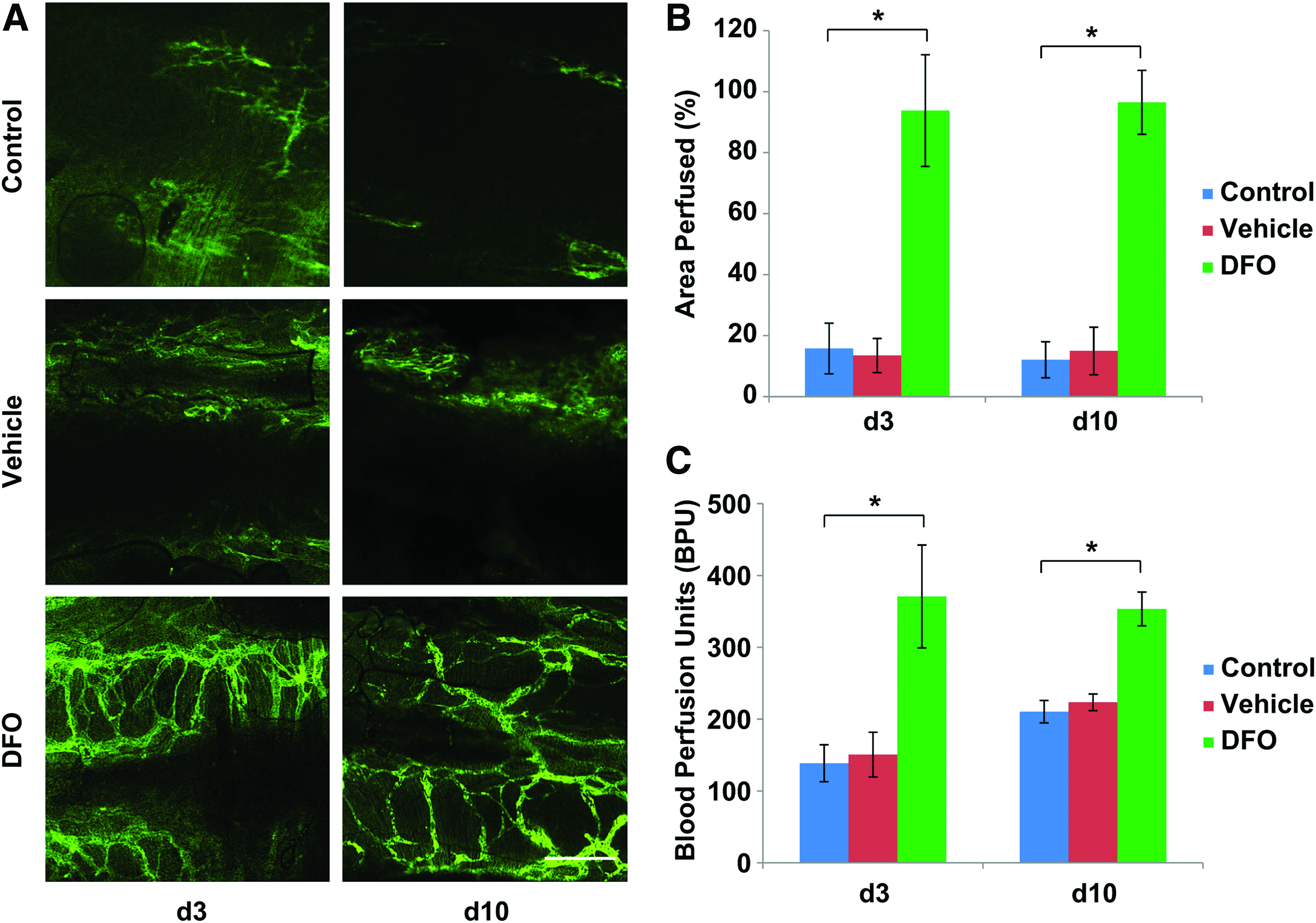
Effect of DFO nanoparticles in promoting airway anastomotic microvascular regeneration and alleviation of airway ischemia. Vascularization of tracheal transplants measured at days 3 and 10 after DFO nanoparticle treatment.
The lack of blood flow in ischemic injury leads to reduced oxygen availability in tissues that can lead to hypoxic conditions. Although HIF-1α upregulation is naturally triggered by hypoxic conditions, DFO promotes HIF-1α accumulation even under normoxic conditions. Protein immunoblotting assays revealed a time- and dose-dependent increase in HIF-1α in neuroblasts treated with DFO and cultured under normoxic conditions. 36 Of interest, this DFO-induced HIF-1α accumulation additionally protected cells from rotenone-induced apoptosis, indicating that DFO may have an additional neuroprotective effect on cells. 36 The ability to upregulate angiogenic factors under normoxic conditions suggests that DFO could serve as a treatment for traditional wound healing in addition to ischemic injury treatment. The suggested molecular mechanism of DFO-mediated VEGF upregulation is given in Figure 3.
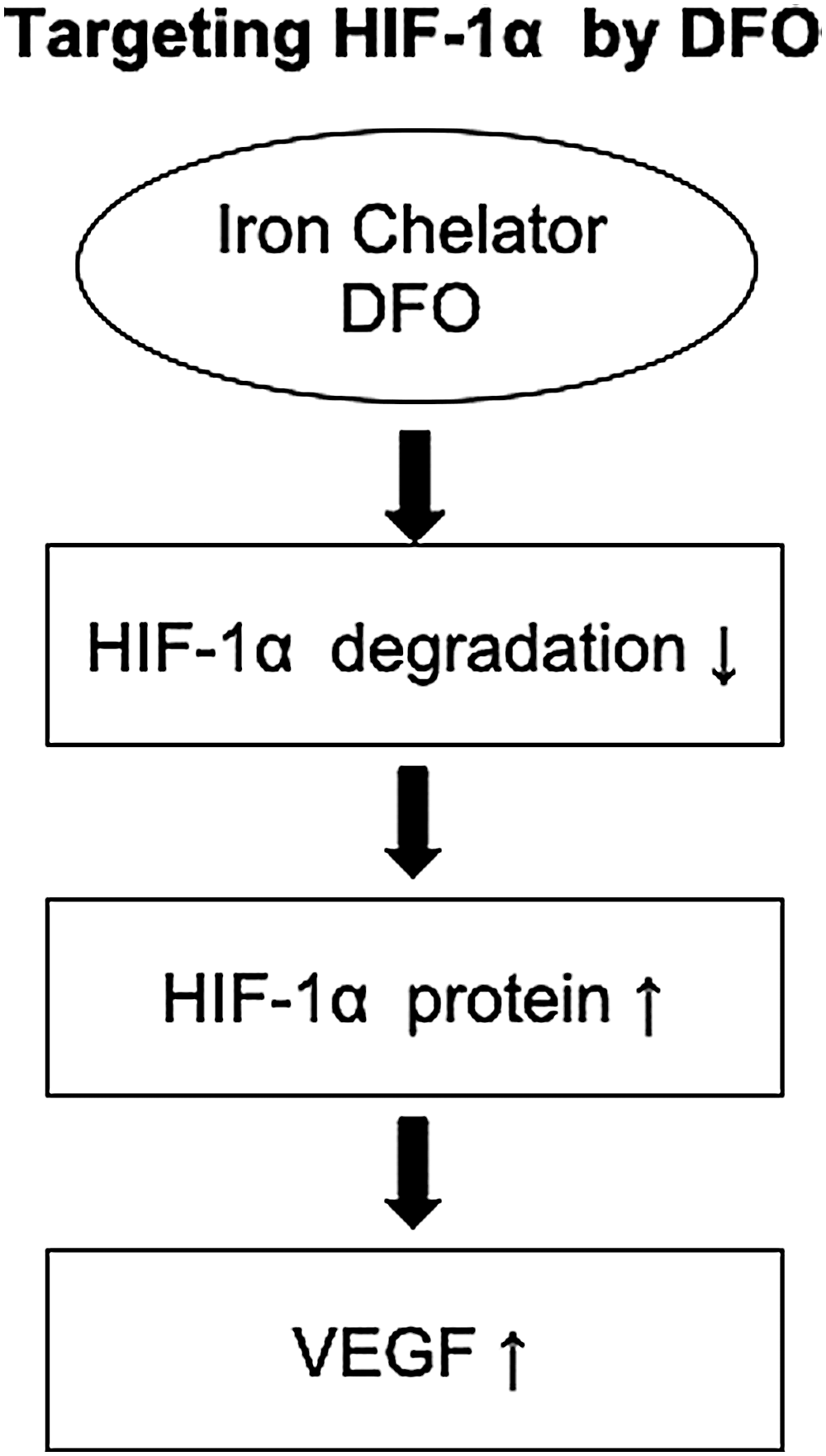
Suggested mechanism of DFO-mediated HIF-1α and VEGF upregulation. Modified from Wu et al. 36 HIF-1α, hypoxia-inducible factor-1 alpha; VEGF, vascular endothelial growth factor.
DFO and wound healing
As of 2015, 30.3 million U.S. citizens suffer from diabetes. 37 In these patients, high blood sugar levels, neuropathy, poor circulation, immune deficiency, and infection make wound healing especially slow or even nonexistent and can all lead to necrotic wounds that typically affect the feet. With DFO inducing angiogenesis in ischemic injury models, researchers began to ask whether similar results could be reproduced in other wound models. The clinical prevalence of diabetes and its ability to be easily induced in animal models made diabetic wounds a natural choice for investigation.
Hou et al. studied the effects of intraperitoneal injection of DFO in diabetic mice with two full-thickness cutaneous wounds compared with a vehicle control group and a VEGF treatment group. Western blot analysis showed DFO significantly upregulated HIF-1α and the target genes including VEGF and SDF-1α, which is an important factor for vasculogenesis (Fig. 4). In addition, the DFO group had a higher number of blood vessels containing RBCs and greater capillary density than other groups. 38 This enhanced vessel formation explains the accelerated wound healing observed by the DFO group, as an increase in circulation near the wound site brings the appropriate nutrients, cells, and factors that help restore damaged tissue.
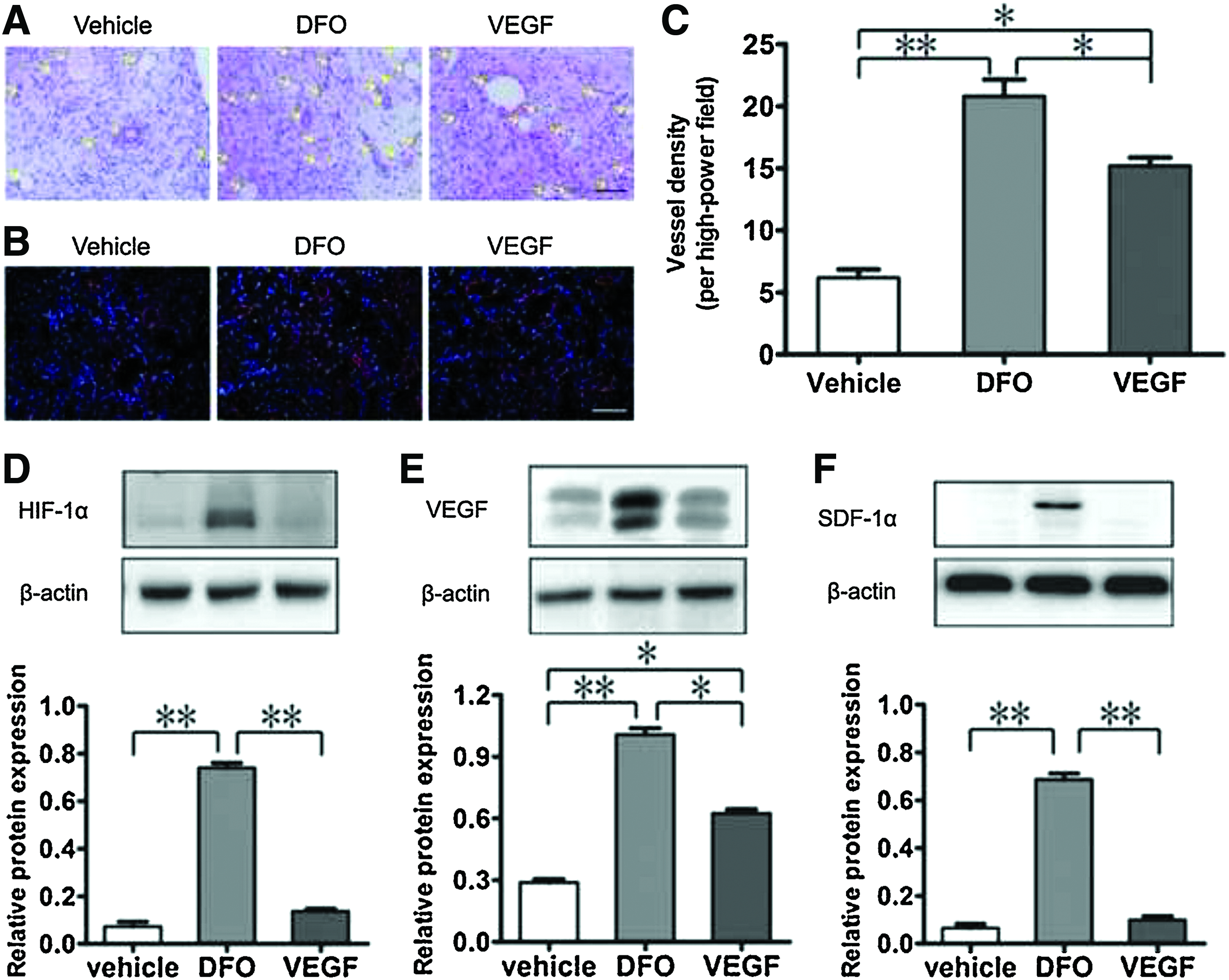
Effect of DFO in enhancing neovascularization and wound healing in diabetic rats. Vascularization of cutaneous diabetic wounds measured at day 7 after DFO treatment.
The group further investigated the effect of DFO on human umbilical vein endothelial cells (HUVECs) to better understand the mechanisms by which DFO enhanced wound healing in their in vivo model. HUVECs treated with various concentrations of DFO showed a dose-dependent increase in HIF-1α expression and dose-dependent increase in tube-like structures. DFO-treated cells also showed increased cell proliferation and migration, although these effects were blocked in HUVECs transfected with HIF-1α siRNA, indicating an HIF-1α-dependent mechanism.
Similar to the findings of Ikeda et al., the study found that DFO treatment can increase phosphorylation of Akt and eNOS and that the positive effects of DFO on cell proliferation and migration can be mitigated by the addition of Wortmannin, a PI3K inhibitor. 38 Taken together, these data suggest an HIF-1α, Akt, and eNOS-dependent mechanism of DFO-mediated angiogenesis.
A study on the effect of DFO on adipose-derived stem cells (ADSCs) from clinically induced diabetic rats found that ADSCs treated with DFO also showed increased expression of HIF-1α, VEGF, and SDF-1 in a dose-dependent manner and increased fibroblast growth factor-2 (FGF-2) expression independent of the dosage. 39 To determine if the DFO-treated ADSCs could activate endothelial cells, HUVECs were treated with media from the DFO-treated ADSCs and found increased cell migration and tube formation in the DFO-treated group compared with the controls. 39 ADSCs are of great use to regenerative engineering because of their ease of isolation and their ability to differentiate into several tissue types. The results of this study indicate that pretreating ADSCs with DFO before implantation could help in activating the endothelial tissue, thereby improving wound healing around ADSC-loaded implants.
DFO released from hydrogel nanofibrous scaffolds have also been shown to successfully promote angiogenesis in diabetic wounds. 40 Sustained release of DFO from polyvinyl alcohol–chitosan electrospun fibers upregulated HIF-1α and VEGF in human dermal fibroblast cells. In a mouse full-thickness wound model, DFO loaded fibers showed a greater decrease in wound area over 18 days and enhanced expression of HIF-1α, VEGF, and SDF-1α compared with fibers without DFO. 40 The enhanced angiogenesis paired with a quick degradation rate of the hydrogel fibers is ideal for wound healing as it helps leave room for the incoming tissue and vessel growth.
An injectable hydrogel containing DFO and bioglass was also studied for use in diabetic wound healing. Given that both DFO and the silicon ions in bioglass have been shown to upregulate VEGF, Kong et al. decided to study the combined effects of the two materials and found that the mixture improved migration, tube formation, and expression of VEGF in HUVECs compared with either material on its own. 41 A sodium alginate hydrogel containing DFO and bioglass demonstrated synergistic effects on the upregulation of HIF-1α and VEGF when injected into the skin wounds of diabetic rats that led to enhanced neovascularization compared with sodium alginate gels containing either material alone. 41 This study has important implications on DFO's ability to work synergistically with other bioactive materials to promote angiogenesis in vivo.
A DFO-loaded transdermal patch has also been studied in the treatment of diabetic symptoms. In full-thickness diabetic ulcer wounds in mice, the DFO patch showed increased wound healing, increased VEGF expression, enhanced neovascularization, and increased dermal thickness compared with a vehicle control patch. 42 In addition, pretreating the skin with the DFO patch followed by attempted induction of diabetic ulcers demonstrated that the DFO patch actually had the ability to prevent the formation of ulcers compared with non-pretreated controls. 42 According to these results, DFO could be a proactive treatment rather than a reactive one, helping to reduce pain and suffering for thousands of diabetic patients.
A trend in regenerative engineering has been to develop controlled, sustained release mechanisms that maintain therapeutic levels of effector molecules for extended periods of time. These mechanisms have the potential to decrease costs and physician visits for patients, eliminate the unpredictability of patient compliance, and ensure optimal efficacy of the effector molecule.
A recent study looked at the effects of controlled, sustained release of DFO and its potential for therapeutic angiogenesis. 43 Free DFO and DFO nanoparticles were encapsulated in chitosan–hyaluronic acid hydrogel. The hydrogels were then implanted subcutaneously into mice. At both 14 and 28 days postinjection, the DFO nanoparticle gels showed a significant increase in the blood vessel density surrounding the injection site. 43 Immunohistochemical staining indicated that these gels also increased HIF-1α expression in the area, which is consistent with many previous studies. This encapsulation and release mechanism could augment the angiogenic potential of biomaterials by ensuring a consistent proangiogenic local environment.
Controlled release of various molecules can also help regulate various steps involved in complex processes such as angiogenesis. For example, O'Neill et al. were able to precisely control the timing and dosage of DFO release through encapsulation of thermosensitive, DFO-loaded liposomes within an injectable hydrogel. 44 They demonstrated this ability by first recruiting cells with the passive release of hepatocyte growth factor, then purposefully delivering an external hyperthermic stimulus to release DFO from the liposomes. 44 The study demonstrated the feasibility to control the amount of DFO released by changing the time period of the thermal signal, with increased time correlating to increased release. 44 This study has important implications on the ability to precisely regulate growth factor release for not only angiogenesis but also nearly any multistep biomolecular process.
The effect of DFO preconditioning of adipose-derived mesenchymal stem cells (MSCs) has also demonstrated to promote paracrine signaling of angiogenic and anti-inflammatory molecules. MSCs treated with 150 or 400 μM DFO for 48 h showed a dose-dependent increase in HIF-1α that lead to downstream increases of the angiogenic factors VEGF and angiopoietin 1 (ANG-1) and the anti-inflammatory cytokines interleukin (IL)-4 and IL-5. 45 In addition, the treatment did not affect the MSC morphology or survival. MSCs are multipotent stem cells with the ability to differentiate down myogenic, chondrogenic, and osteogenic lineages. Given that DFO did not affect the growth of MSCs, the results of this study suggest that DFO could play a key role in the induction and formation of vascularized bone tissue.
DFO and bone regeneration
Bone is an incredibly dynamic tissue regulated in a variety of ways. For example, bone remodeling can be induced by changes in loading as described by Wolff's Law. Bone is also responsive to changes in blood calcium, with osteoclasts being activated by parathyroid hormone when blood calcium is low, and osteoblasts being activated by calcitonin when blood calcium is high. This constant remodeling of bone can only be achieved with a healthy source of growth factors, nutrients, and hormones from the blood that explains why bone is such an abundantly vascularized tissue. Many skeletal diseases including osteonecrosis and osteoporosis involve damaged or improperly functioning vasculature. 46 Fracture of the bone may also interfere with proper blood flow through bone tissue. In all these cases, proper restoration of blood flow is paramount to regeneration of the bone tissue.
One study investigated whether localized DFO injection could help improve fracture healing after radiotherapy through previously suggested angiogenic mechanisms. A tubule formation assay using HUVECs was used comparing control cells, cells that are radiated, cells that are radiated then treated with low dose (25 μM) DFO, and cells that are radiated then treated with high dose (50 μM) DFO. As predicted, less tubule formation was found in response to radiotherapy. Although the low dose of DFO had no significant restorative effect compared with the control, time-lapse video indicated that it was able to improve cellular organization, activity, and locomotion. High-dose DFO showed results consistent with the nonradiated control, suggesting that it was able to remediate the effects of radiotherapy. In addition, the high dose significantly decreased the time to peak tube formation and consolidation compared with the other groups. 47
An in vivo study was then performed in a rat mandible osteotomy model with control, radiated, and radiated with DFO groups. DFO was administered by injection directly to the fracture site every other day starting 4 days post-op and ending 12 days post-op, which coincides with the time period for initiation of angiogenesis in murine fracture models. 47 Three-dimensional angiographic modeling showed that the DFO group significantly increased vascular volume, number, and separation compared with the radiated fracture group (Fig. 5). The DFO group also showed no significant differences in these metrics compared with the nonradiated control, indicating that the DFO was able to reinstate normal vasculature in fracture healing despite radiotherapy. 47 When the gross structure of the mandibles was examined, it was found that the DFO treatment took the radiated mandibles from a 25% union rate to a 67% union rate, compared with a 100% union rate in the nonradiated controls. 47 The study concluded that the improved vascular network induced by the DFO treatment allowed for improved bone fracture healing.
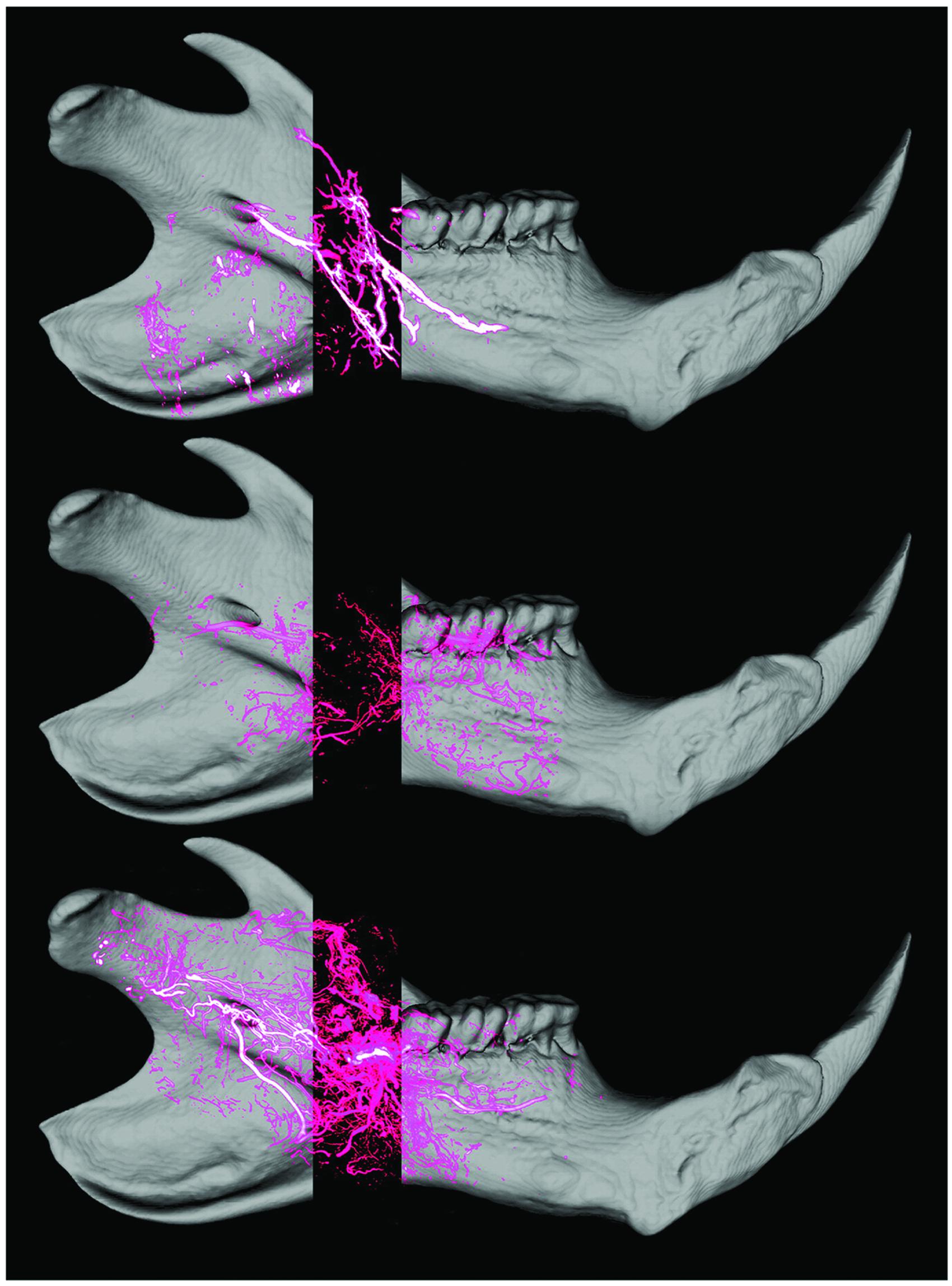
Effect of localized DFO injection in improving vascularity and bony union in pathologic fracture healing after radiotherapy. Control (top), radiated (middle), and radiated with DFO (bottom) rat mandible three-dimensional reconstructed micro-CT angiograms. Vessels are shown in pink. The surrounding bone structure is superimposed to better visualize the location of the vasculature. Reproduced with permission from Donneys et al. 47 Color images are available online.
The effect of local DFO injection was also studied in steroid-induced osteonecrosis of rabbit femoral heads. Given that core decompression was the most commonly used surgical therapy to treat this type of injury, this group chose to compare rabbits with no treatment to rabbits who received bilateral core decompression and rabbits received bilateral core decompression plus DFO. Ink artery infusion angiography and immunohistochemical staining for von Willebrand factor confirmed increased blood vessel and microvessel incidence in the DFO treatment group. 48 Immunohistochemical staining also indicated significantly increased levels of HIF-1α and VEGF in the DFO group compared with the other groups. 48
Histology indicated improved bone formation in the DFO group through a decrease in the number of empty lacunae and increased newly formed trabecular tissue in the tunnel formed by the core decompression. 48 Micro-CT scanning confirmed a statistically significant increase in bone mineral density, bone volume fraction, trabecular number, and trabecular thickness as well as a decrease in trabecular separation when comparing the DFO-treated group with the group that received core decompression therapy alone. 48 Taken together, these results further suggest the role DFO-mediated angiogenesis plays to promote osteogenesis and offer an exciting possibility for the treatment of osteonecrosis.
Another study indicated that DFO may also be useful in the treatment of osteoporosis, a disease that is responsible for >1.5 million fractures annually. 49 In one study, poly(lactic-co-glycolic acid) (PLGA) scaffolds loaded with DFO were compared with PLGA scaffolds. The DFO-loaded scaffolds upregulated HIF-1α and downstream factors including VEGF, FGF-2, and ANG-1. 50 A tubule formation assay confirmed greater organization of HUVECs after 24 h with the DFO scaffold, indicating enhanced angiogenesis. 50 In addition, the DFO scaffolds induced osteogenic differentiation in MSCs that was demonstrated by alkaline phosphatase and alizarin red staining and increased expression of osteocalcin and Runx-2. 50
A rat femur defect study confirmed that the DFO scaffolds increased bone volume fraction, trabecular number, and trabecular thickness while decreasing trabecular separation compared with defects filled with PLGA scaffolds alone and unfilled defects. 50 Microangiography and micro-CT performed 14 days after implantation show that the defects filled with DFO-loaded PLGA scaffolds had a significantly larger total vessel volume than the other groups. 50 In addition, immunohistochemistry demonstrated that there were more endothelial cells building tube-like structures in the DFO treatment group than the PLGA-only group. 50 The outcomes of this study strengthen the link between DFO-induced, HIF-1α-mediated angiogenesis and subsequent bone regeneration while simultaneously suggesting that DFO may have an additional capacity to drive osteogenic differentiation in MSCs.
As mentioned previously, preconditioning adipose-derived MSCs with DFO showed increased expression of HIF-1α, VEGF, ANG-1, IL-4, and IL-5. 45 A study was carried out using periodontal ligament stem cells (PDLSCs) derived from the periodontal ligament of human teeth found similar results, further indicating the use of DFO preconditioning on stem cell-induced angiogenesis. In this study, PDLSCs were pretreated with DFO for 24 h, FGF-2 for 72 h, or a combination of both. Enzyme-linked immunosorbent assay showed that VEGF production increased 1.8-fold for the DFO-treated group, 1.5-fold for the FGF-2 group, and 2.7-fold for the combination treatment. 51 Like MSCs, PDSLCs are multipotent and are able to achieve adipogenic, chondrogenic, and osteogenic differentiation. The combined results of these two studies indicate that DFO preconditioning could be an effective strategy to help induce angiogenesis around stem cell-loaded biomaterials for bone regeneration.
Antioxidant Properties of DFO
Unliganded iron has the potential to react with peroxides to form ROS that can damage numerous biological tissues. 7 The same three hydroxamic acid groups that bind iron have also shown a role in electron transfer, indicating that DFO may also have an antioxidant role unrelated to its iron chelation properties. Davies et al. discovered that DFO could react with ROS to form the deferoxamine nitroxide radical (DfNO•) even without the presence of iron. 52 Since then, it has been determined that DFO is effective at quenching alkoxyl, peroxyl, hydroxyl, and superoxide radicals and, that these effects are enhanced when iron played a role in the reaction systems.53,54
ROS are present in relatively high concentrations in inflamed tissue and are produced by cells such as macrophages and polymorphonuclear neutrophils as signaling molecules in the immune response. However, in high concentrations, ROS can cause damage to the surrounding healthy tissue, including the endothelial cells lining the local vasculature. 55 Local blood vessels are critical for the delivery of nutrients and elimination of waste to the tissue, two basic functions that enhance the efficacy of implanted biomaterials. Therefore, keeping the vessels and surrounding tissue intact by subduing the local immune response would be highly beneficial to support tissue regeneration. Exploiting the antioxidant properties of DFO for these means may then prove to be an effective strategy.
The antioxidant effects of DFO have been demonstrated for several decades. Hartley et al. observed decreased alkoxyl and peroxyl radical concentrations in erythrocyte membranes incubated with DFO at concentrations of 10 mM or greater. 53 This corresponded with an increase in the concentration of DfNO•, indicating the role of the hydroxamic groups in these quenching capabilities. 53 Although the chemical nature of DFO's antioxidant properties had been revealed in this study, further work is needed to understand the biological applications.
Collins et al. investigated the immunosuppressive properties of DFO by treating mice infected with Salmonella typhimurium with DFO. The study showed increased numbers of bacteria in treated mice, suggesting that DFO may have an immunosuppressive effect. 56 It has been suggested that DFO interfered with the ROS killing mechanism of macrophages leading to the increased bacterial growth. The hypothesis was confirmed by treating peritoneal macrophages with DFO and found that it effectively inhibited the production of peroxide radicals compared with control macrophages. 56 These results support the concept of DFO-mediated immunosuppression through antioxidant mechanisms and further support clinical applications DFO in regenerative engineering.
A recent study discussed a potential therapeutic application wherein the potent antioxidant properties of DFO can be used, in relation to the yearly transportation of mineral dust from West Africa to the Caribbean. This transport results in very high levels of airborne metal particulate matter in and around Puerto Rico, which has exacerbated the already high asthma rates in the country. 57 In one study, human bronchial epithelial cells treated with DFO and the prooxidant African Dust Extract (ADE) decreased ROS compared with cells treated with just ADE. 57 These findings also confirm the potent antioxidant activities of DFO.
A mouse orthotopic tracheal transplant model was recently used to study DFO-induced reduction of ROS in the airway. In this study, DFO nanoparticles were topically applied to the airways at the time of transplantation. The DFO was able to reduce perivascular ROS production and thereby prevent endothelial cell death. 35 Together with its angiogenic nature, the DFO treatment was able to increase perfusion area in the transplanted tissue. 35 The dual nature by which DFO is able to promote blood vessel growth makes it an even more attractive choice for tissue and regenerative engineering applications.
As previously mentioned, DFO has been investigated for potential use in treating ischemic injury in relation to its angiogenic capabilities, but its antioxidant properties may also play a role in ameliorating these kinds of wounds. In a 2010 study, six pigs who suffered a combined 70% liver resection and ischemia (150 min)/reperfusion (24 h) injury received 100 mg/kg DFO in continuous intravenous infusion. The DFO-treated pigs showed lower levels of serum markers indicative of hepatocyte damage, lower levels of oxidative markers, and lower concentrations of ammonia and bilirubin compared with nontreated pigs with identical injury. 58 Together, these findings suggest that DFO was able to minimize the damage because of ischemic injury and improve the detoxifying capabilities of the liver compared with the untreated control.
In addition, liver fibrosis may also be a target for DFO treatment. In one study, liver fibrosis was induced in rats by injection of carbon tetrachloride (CCl4). DFO treatment significantly decreased several indices of hepatotoxicity and showed minimal degradation of hepatocytes compared with CCl4 treatment alone. 59 Given that ROS have been known to help initiate hepatic fibrogenesis, the oxidative stress of the livers was also monitored. As expected, DFO counteracted oxidative stress and lipid peroxidation and restored antioxidant enzyme activities. 59 These effects are likely related to the reduced hepatotoxicity in the DFO-treated livers.
A recent clinical study demonstrated a potential application for DFO in the treatment of myocardial infarcts. In this study, patients undergoing primary percutaneous coronary intervention were given an intravenous dose of DFO or saline placebo before their procedure, followed by a 12-h infusion of either DFO or saline placebo. Oxidative stress was measured by F(2)-isoprostane levels in the plasma. 60 F(2)-isoprostanes are products of lipid peroxidation and have been shown to give a reliable measure of oxidative stress in vivo. 61 It was found that DFO decreased plasma levels of F(2)-isoprostane, lowering the oxidative stress in these patients. 60 Given that ROS play a large role in ischemia–reperfusion injury, DFO's ability to reduce ROS insinuates a potential application to treat or prevent these types of wounds.
Conclusions
Although DFO has been in use as an FDA-approved iron chelator for half a century, its multitude of therapeutic properties went unnoticed until the last two decades. Since then, studies regarding this small molecule have revealed that it is an incredibly dynamic drug with chelating, antioxidant, and angiogenic properties. Although each property is useful in its own right, the seemingly related nature of these characteristics makes DFO an ideal candidate for further investigation regarding its biomedical applications. By reducing the effects of damaging ROS and promoting neovascularization through the HIF-1α-dependent pathway, DFO has an impressive range of potential clinical applications. Wound healing, bone regeneration, and the treatment of ischemic injuries are just a few among many promising uses for this versatile molecule.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
P.H. acknowledges support from Uconn Health Research Program student Internship.