
Abstract
The bone repair and substitute have been developed for decades with the bone defect repair applied successfully in clinical. However, implant complications may occur in more challenging situations, bone cell senescence and osteoporosis (OP). Due to certain microenvironment conditions, including hormonal, nutritional, and aging factors, the bone cell responses are regulated to alteration and end into cell senescence and OP. Thus, the bone tissue regeneration is limited with site morbidity increased, leading to bone graft failure. In such pathological state, bone grafts and substitutes are companied with OP therapies to improve bone tissue engineering and to enhance bone graft healing. Those substitutes with OP therapeutic-based applications have been becoming a growing field of interest in bone repair. Bone grafts, such as scaffolds with antiosteoporotic drugs releasing and implants with surface therapeutic modified, are studied to significantly increase low bone density as well as improve impaired bone regeneration. In this review, we discuss a thorough understanding in bone remodeling process, bone cell senescence, and mechanisms of OA and OP. Based on the understanding, the review concentrates on the treatments to the OP and the bone grafts applied in the bone senescence model and provides a future direction in clinical trial.
Impact Statement
This review discusses the tissue engineering and regenerative medicine therapies for aging-related bone diseases, which have been highly concerned in aging society. These therapies can improve the efficacy of bone tissue regeneration, enhance the quality of bone repair, and provide new insights in the field of bone clinical treatments and aging regeneration.
Introduction
As one of the most import organs to support body structure, the study on the human bones has been developed for decades. Bone also serves as the main part for the movement, organs protectors, and the calcium and growth factor storage place. 1 Most of the bone structure and mechanisms have been revealed. However, there are still problems unclear, especially on the aged bone model, which obstructed the development of the bone repair and substitute in this model. In the general human bone, a balance between the cell anabolisms is established. The maintaining cells in the bone tissue contain osteoblasts for depositing new bone tissue, osteoclasts for resorbing the old bone, and osteocytes entombed in the bone matrix for mechanical loading.2–4 There are also important cell types to the bone matrix, including bone marrow cells, 5 endothelial cells,6,7 and mesenchymal stem cells (MSCs).8,9 Those stem cells are important to the bone cell differentiation and new bone tissue formation.10–12 In the macroscopic view, there are two types of the bone, the cancellous bone and the cortical bone. In the cancellous bone, which is called the spongy bone, a series of interconnecting plates of bone increases the mechanical loading at the vertebrae, pelvis, and ends (metaphyses) of long bone. 13 It is reported as the site of osteoblastic, osteoclastic, and osteocytic activity. 14 The open honeycomb structure of trabecular bone tissue houses the bone marrow and the blood vessels that perfuse the bone marrow with blood. 15 In the cortical, or the compact bone, the structure of Haversian systems or osteons format parallel cylinders to the long axis of the diaphysis with the osteocytes. 16
Bone Remodeling
Bone remodeling, which lasts for the life time, is a dynamic process in maintaining bone strength and mineral homeostasis. 17 The remodeling process allows the bone to sustain tremendous loads and to repair the constant microcracks by resorbing old damaged sites and formatting the new tissue. 18 Due to the different bone matrix microenvironment, the microcracks and its repair can involve different cell types in the cancellous bone and in the cortical bone. The bone repair in the cancellous, such as vertebrae and pelvis positions, is close to red marrow containing osteoprogenitor cells. 19 And in the cortical bone remodeling, the osteoprogenitor cells are assumed to travel from red bone marrow through vasculature. 20
In general, the bone remodeling can be separated into four consecutive phases, activation, resorption, reversal, and formation, 1 as shown in Figure 1.

Schematic representation of bone remodeling. Color images are available online.
In the activation stage, the mononuclear preosteoclasts from the circulation are recruited by hormonal or physical stimuli and attached to the bone surface. During this process, the surface marker receptors, such as receptor activator of nuclear factor kappa-B (RANK), on osteoclast precursors are banded to macrophage colony-stimulating factor (M-CSF) 21 and the receptor activator of nuclear factor kappa-B ligand (RANKL), which is released by osteoblasts. 22 Another soluble decoy receptor, osteoprotegerin (OPG), 22 which binds to RANKL, is primarily expressed by bone marrow stromal cells and osteoblasts into the system. RANKL, RANK, and OPG compose a pivotal regulation in the bone remodeling, as the process inhibitor, OPG, has been found to bind RANKL with ∼500-fold higher affinity than RANK, inhibiting osteoclastogenesis and protecting the bone from osteoclast-mediated resorption. In this phase, the cells develop to multinucleated osteoclasts. 23
The resorption phase is the period for the osteoclasts to initiate resorption of organic and mineral bone components. The occurring sites are termed as basic multicellular unit (BMU), which comprises the osteoclasts, osteoblasts, and osteocytes within the bone-remodeling cavity. 24 The BMU is covered by canopy (bone-lining cells) predominantly of mesenchymal cell origin (v infra) after the osteoclast location and imitation. 25 In addition, these mesenchymal origin cells on the bone surface are osteocyte communicated and reestablish the integrity of osteocyte-lining cell system embedded within the bone matrix in the bone remodeling compartment (BRC). 26 Thus, osteocytes are responsive to control the bone remodeling through communication with lining cells. After the osteoclast-resorbed cavities reach a certain size, apoptosis of osteoclasts terminates bone resorption and releases growth factors, such as transforming growth factor (TGF)-β, bone morphogenetic proteins (BMPs), and insulin growth factors (IGFs), to MSCs. 27 The resorption activity in a BMU can take 2–4 weeks and can replace 5–10% skeleton each year (for review, see Sims and Martin 28 ).
In the reversal phase, the resorbed surface is smoothed by lining cells and mononuclear macrophage-like cells with the differentiation of osteoblast precursors initiated. 29 In the formation phase, the osteoblasts, which are derived from MSCs, lay down on the resorbed bone surface and format the new bone tissue. The osteoblast differentiation can be governed by mechanical 30 and biochemical pathways, such as related transcription factor 2 (Runx2),31,32 Wnt signaling pathway, 33 and IGF-1. 34 With the collagen secretion and the bone matrix mineralization, 35 the osteoblasts construct the new bone layer and support hematopoiesis and angiogenesis. The mature osteoblasts produce bone remodeling regulation molecules, such as osteocalcin (bone formation regulator), 36 RANKL (the osteoclast precursor activator), and parathormone (PTH, bone formation stimuli). 37
After the molecular secretion process, osteoblasts can eventually turn into mechanosensory osteocytes or bone-lining cells, which are buried in the matrix in lacunar-canalicular system. 3 The transformed osteocytes can express molecules that control the bone formation and phosphate metabolism. 38
In the BRC process, the canopy sites near a capillary 39 and has intercellular communications with bone cells, endothelial and vascular cells, 40 and immune cells through the blood supply.41–43 To initiate the bone remodeling, more cells, such as hematopoietic stem cells, osteoclast precursors, and MSCs are also evolved with their mechanism. At the bone microcrack or damaged position, the osteocytes recognize the specific area and signaling through their canaliculae to surface cells. 44 The apoptosis of osteocytes signals to attract osteoblasts, osteoclast precursors, and vascular elements by releasing paracrine factors and chemokines. 44 The osteoclasts are formatted from hematopoietic precursors, which are provided by capillary blood supply and penetrate the BRC, 39 and the marrow precursors from nearby. The signals of M-CSF, RANKL, vascular endothelial growth factor, and nitric oxide necessary for programming of osteoclast formation penetrate within the BRC (for review, see Khosla et al. 3 ). However, those vascular-derived osteoblast precursors can be active in mouse model only. 45 An important stimulus for the osteoclast precursor egression from vasculature is sphingosine-1-phosphate (S1P). 46 The 1,25-dihydroxyvitamin-D3 actives the S1P 47 and thus promotes the formation of osteoclasts. However, there are paradoxical actions for the active vitamin D on bone. 48 The inhibition of active vitamin D to the S1PR2, the receptor of osteoclast precursor directing the cell from blood to bone, can inhibit the osteoclast generation and bone resorption. 47
At the last phase of osteoclast activation, the differentiation is stimulated by factors secreted by osteoblasts, which are described above. Some of the researchers reported RANKL expression by osteocytes,49,50 which is against the traditional opinion supporting osteoblast lining cells as the only activator. Thus, more questions remain to be studied in future research.
Cell Senescence and Osteoporosis in Bone
Cell senescence
In the aging area, cell senescence is an inevitable process that affects most cells in biological organisms. It generally refers to the essentially irreversible permanent arrest of cell cycle in response to stress and damage from exogenous and endogenous sources. 51 In detail, the replicative senescence was associated with telomere shortening, erosion, or dysfunction. 52 With the development to the senescence-associated secretory phenotype (SASP), the concept of cell senescence was re-determined. No longer as a singular statement, senescence is a collective phenotype of multiple effector programs, which forms functional networks of senescence and provides additional complexity to the phenotype. 53
Cell senescence phenomena, such as cell damage, cell dysfunction and stem cell exhaustion, and altered intercellular communication, are the characterized aging phenotypes. 54 The mechanisms of cell senescence shown in Figure 2 are described below in detail. In the skeleton system, the aging and senescence result mainly from decreased bone formation, which links to the reduction of stem cell differentiation into osteoblasts, decrease of osteoblast function, 55 and increase of apoptosis of osteoblasts. 56
The mechanism of bone cell senescence. Color images are available online.
Cell senescence in aging condition
The mechanisms of the bone cell senescence are generally associated with telomere shortening, 57 genomic damage, 58 epigenomic damage, 59 and oxidative stress. 60 In the telomere shortening, the telomeres that cap the ends of linear chromosomes are shortened associating with each cell division. 57 To maintain self-renew, the telomere length is maintained by telomerase or protein complexes, 61 and allows cells to extend telomere length. 54 However, the ends of the linear DNA molecules cannot be completely replicated when the polymerases for DNA copying are unidirectional and require a labile primer. 62 Thus, the shortening on the telomeres contributes to the cell replication reduction and life span decrease. In osteoblast progenitor cells, the telomere shortening leads to stem cell population decrease and impaired differentiation in bone-forming cells. 54 Pignolo et al. reported that the telomere defects contributed to osteoblast differentiation and function reduction, with osteoporosis (OP) enhanced. 63 More studies supported that the telomerase overexpression had positive effects on the MSC differentiation and bone formation enhancement.64,65
In the genomic damage, oncogenic stimuli elicit the senescence. 66 Those stimuli contain telomere dysfunction 67 and uncapping. 68 Wang et al. 69 and Coppé et al. 70 demonstrated different types of genomic damage responded to cellular senescence. The increased expression of p53 through the p53-p21-pRb pathway, p16INK4a through the p16-pRB pathway,71,72 and the caveolin 1, 73 which is the principal structural component of caveolae, indicated the cell senescence in chondrocytes 74 and MSCs. 75 The damages in the epigenomic level are linked to the cell senescence and aging by chromatin structure and telomere length. 76 In bone modeling and remodeling, epigenetic mechanisms can affect the osteoclastogenesis by RANKL, 22 OPG, 77 and osteocalcin, 78 and the osteoblastogenesis, by BMP-2, 79 sclerostin, 80 and C/EBPα 81 through DNA methylation. It is also reported that the RANK-induced NFATc1, which regulates the osteoclast differentiation, can be controlled by the histone demethylases. 54 In addition, another epigenetic mechanism to regulate the gene expression and aging is microRNA regulation.82,83 In the bone aging researches, SIRT-1 is reported as a target for cell senescence alleviation.84,85
The oxidative stress can induce the cellular component damage and contributes to aging. 86 With age increasing, the reactive oxygen species causes the cell damage and death in bone cell, which are shown as the bone fragility and aging. 87 In the mouse model, this bone loss hypothesis was proved by the antioxidant treatments to abrogate the increased apoptosis, decrease bone fragility, and attenuate bone loss during loading.88–90 However, Lauing et al. 91 and Iyer et al. 92 reported the Wnt signaling concomitant inhibition limit to the antioxidants. Thus, more work needs to be done on fully understanding the oxidative stress signal pathway to cell senescence.
Cell senescence in pathological condition
Compared to the bone cell damage, dysfunction, and exhaustion in the aging stage, the cell senescence can be caused more commonly in pathological status, such as cancer bone metastasis, osteosarcoma, HIV, diabetes, and inflammation. In those conditions, bone cell senescence is companied with altered microenvironments and pathways.
In the cancer bone metastasis, the main process is dominated by osteolytic, osteoblastic or their mixed activity. 93 In the bone environment, cancer cells, such as breast and prostate cancer cells, secrete a large number of cytokines, create a cytokine network, enhance osteoclastic activity, and imbalance the bone formation and resorption. 94 The increased osteoclast activity produces lymphokines and growth factors, which in turn stimulate the proliferation of tumor cells.95,96 Meanwhile, senescent-induced changes, such as osteoblast senescence, in the bone microenvironment can increase the productive seeding regions within the bone and create a hospitable niche to facilitate metastatic tumor growth.96,97
The osteosarcoma, which arises from the bone microenvironment in the majority cases, 98 also guides the cell senescence in bone microenvironment to an altered condition. From histopathology view, osteosarcoma can be defined as a malignant mesenchymal tumor, in which the tumor cells produce osteoid and bone matrix. 99 In osteosarcoma tissues, neddylation, a post-translational protein modification, is upregulated with two critical components highly expressed and might contribute to tumorigenesis and unrestrained cell proliferation.100,101 Thus, studies targeting the neddylation pathway, such as MLN4924, might be a therapy for cancer led to DNA damage, reduced cell viability, senescence, and apoptosis. 102
Furthermore, it is noticed that the autophagy is observed to be deregulated in osteosarcoma, but could act both as a prosurvival pathway for proliferation and a antitumoral factor. 103 Some autophagy pathways104–106 such as mTOR, IGF2, and RUNX2 are evidenced to be activated and suggest induced autophagy in the osteosarcoma. However, other studies also support that the autophagy can result in an autophagy-mediated cell death, controls osteosarcoma cell fate, and promoted apoptosis.107–109 In osteosarcoma tissue, the apoptosis and senescence are highly concerned with many researches studied. However, the essential understandings of the mechanisms and regulations have not been addressed.
In the HIV condition, the bone cell senescence, caused by the pathological microenvironment and cellular communications, becomes focused due to the lower bone mineral density presence in patients.110,111 Studies have shown that HIV can enhance inflammation and reduce autophagy to induce stem cell senescence in bone.112,113 Beaupere et al. 114 reported that Tat and Nef could reduce the number of available precursors by inducing MSC senescence. Decreases in telomerase activity and shortening of telomere length, which lead to the MSC senescence, are also demonstrated by researches.115,116 Another regulator, HIV protease inhibitors, is shown to enhance the expression of farnesylated prelamin A, induce premature aging of osteoblast precursors, and reduce MSC differentiation potential.117,118 The studies on bone senescence caused by the HIV are limited, which indicate more pathways and mechanisms need to be understand clearly.
In the diabetes, it is generally considered that the bone cell senescence is caused by the high glucose environment and increased oxidative stress.119–121 Caldwell and colleagues reported that the high glucose treatment to the bone cells could overexpress ureahydrolase enzyme arginase 1, increase senescence-associated beta galactosidase activity, and induce cell senescence in diabetic condition. 122 This regulation is also reported by Hemmings et al., 123 Sone and Kagawa, 124 and other researchers.125,126 Recently, more mechanisms and side effects of diabetes are demonstrated to have a relationship with bone cell senescence. Obesity is reported to be associated with the accelerated senescence of bone marrow MSCs,127,128 which can possibly suggest the presence of low bone turnover in obese and Type 2 diabetes patients. 127
In addition, a more common pathological condition, inflammation can also lead to bone cell senescence. As described above, the tumor and diabetes can also lead to inflammation. During the inflammation, the monocytes have increased secretion of tumor necrosis factor-α (TNF-α) and interleukin (IL)-1β. 129 Bone cells, which are undergoing senescence and expressing SASP, involve secretion of proinflammatory cytokines, chemokines, growth factors, and proteases. 130 Thus, the cell senescence can increase cell proliferation, migration, or differentiation to promote tissue repair, theoretically. 131 However, immune cells can also be mobilized into this area by the secretion and may cause neighbor cell dysfunction. The phenotype of senescent cells can be forced on the neighbor cells in nonsenescent condition by autocrine and paracrine effects, 132 which suggests the secretion behavior will not be stopped immediately. 131 In this case, the cell senescence and its caused inflammation can create a closed circle.
Osteoporosis
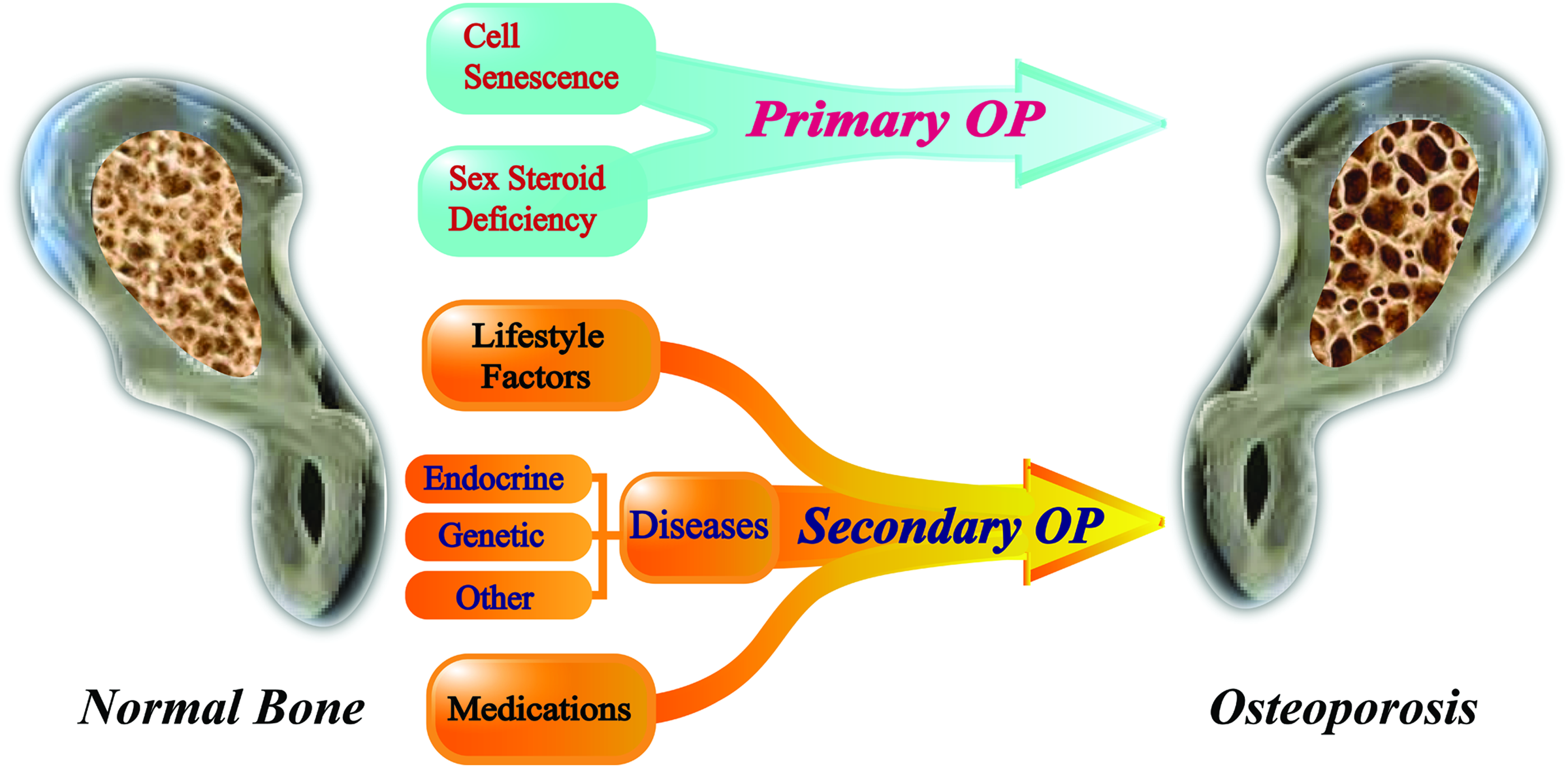
OP is a system skeleton disease, which is generally presented in aged bone system and acts as an obstacle to bone repair and implantation in old people. Used to be a typical disease impacting aged females, OP is getting increasing attention in old male and has been accounted for one of the greatest contributions to morbidity and mortality in men. 133 As the result of aging and cell senescence, OP has decreased bone density and microarchitectural disruption of bone tissue, with a consequent increased skeletal fragility and fracture. 134 Thus, OP is not only the major cause for facture in old population but is also associated with serious complications, especially bedridden. The medical cost for fall injuries totaled $32 billion in 2015 and is expected to exceed $25 for fracture only in 2025 in the United States. 135 In the OP, the impaired bone resorption and remodeling are being observed in the pathophysiological state. The imbalanced bone remodeling activity may be regulated by age and sex hormone deficiency, 136 which cause primary OP, and by several comorbid diseases and/or medications, which cause secondary OP 137 (shown in Fig. 3).

Osteoporosis is resulted from many factors affecting bone metabolism. Color images are available online.
In the primary OP, the bone cell senescence and sex steroid deficiency are the main causes. As described in cell senescence, the oxidative stress, macroautophagy, and telomere shortening or genomic damage that caused apoptosis can contribute to the bone remodeling balance impaired. Osteocyte apoptosis product RANKL increases local bone resorption, hyperminerlizes the osteocyte lacunae, and results in bone brittleness and fragility.138,139 In human, sex steroids not only determine the gender differences in bone structure but also slow down the bone turnover rate in lifetime. Osteoclast activity is downregulated with osteoblast activity upregulated by estrogens to attenuate bone resorption and protect bone. 17 The other sex steroid, androgen, protects bone through another pathway. In this regulation, osteoblasts and osteocytes show the high androgen receptor (AR) expression, of which signaling contributes to the development and maintenance of trabecular and cortical bone. Androgen targets the bone cells by binding ARs, regulates the osteoblast and osteocyte activity, and inhibits significant loss of cancellous bone 140 (for review, see Ji and Yu 141 ).
For the secondary OP, there is another story. Several comorbid diseases or medications, including alcohol abuse, endocrine disorders, hypogonadism, autoimmune disorders, renal disorders, and hematological disorders, attribute to secondary OP, as Table 1 shows. For example, according to the vitamin D cooperation effect with PTH to regulate calcium and phosphate levels, vitamin D deficiency impairs bone mineralization, decreases bone mass, and increases fracture risk.
In addition, the causes of OP have bias between genders, which have differences on lifestyle factors, hormone regulation mechanisms, and endocrine systems. The alcohol abuse, excessive glucocorticoid use, and lowering of androgen mainly cause OP in male. In female, OP is largely attributed to secondary OP, which is usually caused by calcium metabolism imbalance, endocrine system disorders, and hypoestrogenemia, including hypercalciuria, hyperparathyroidism, hyperthyroidism, Cushing's disease, and hypocalciuric hypercalcemia.135,142
Osteoarthritis
As two common aging bone disorder diseases, osteoarthritis (OA) and OP get a high morbidity in old population, act as the principal source of physical disability, and result in impaired quality of life. A negative association is suggested by epidemiological studies between them,143–145 but some recent studies reveal a more complex and controversial relationship existing between OA and OP.146,147
OA is a metabolically active process that involves all joint tissues, affecting mainly knees, hips, and small hand joints leading to pain, impairment of mobility, and activity limitation. 148 In OA condition, multiple etiologies, such as biomechanical stresses, biochemical factors, and genetic factors, may contribute to cartilage lesion by disrupting chondrocyte-matrix associations, provoking a phenotypic shift in chondrocytes, and altering homeostasis in the chondrocytes 149 (as shown in Fig. 4). Several important mechanisms and modulators have been revealed in the past years (see in review 150 ); however, due to the complex conditions and subtypes in OA, more studies are needed to fully understand the etiology.
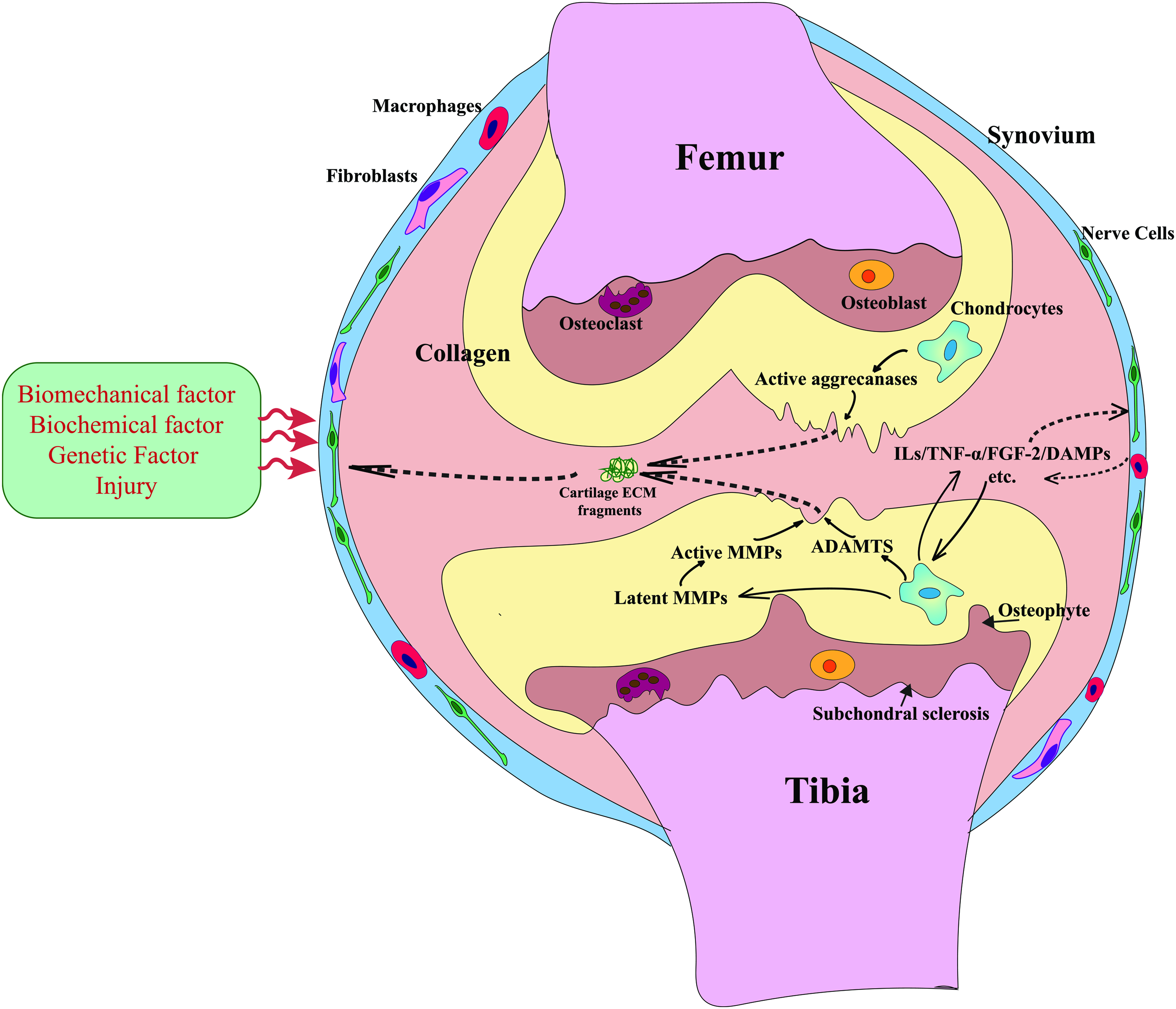
The osteoarthritis may be modulated by factors such as obesity, diet, age, and joint injury, which initiate and maintain dramatic changes in chondrocyte phenotype, cartilage homeostasis, and synovium. Color images are available online.
Aging, which is related to multiple cell cascades, is one of the most common factors for OA. Aging, including autophagy and oxidative stress, affects the whole joint tissue, including cartilage, synovium, subchondral bone, and muscle. In this condition, cell repair response is reduced with TGF-β pathway downregulated and catabolic matrix metalloproteinase (MMP) expression altered from matrix synthesis. 151 In addition, the expressions of Dnmts (methylation) and Tets (demethylation) enzymes are changed in the OA chondrocytes and indicate a different signature pattern displayed by methylation of genomic DNA in aging.152,153 Obesity is recognized to have a close association with OA, 154 including biomechanical loading, low-grade systemic inflammation cytokines by adipose cells, such as IL-1, IL-8, and TNF-α. 155 Those inflammatory pathways trigger the nuclear factor-κB (NF-κB), lead to the MMP upregulation, and stimulate an articular chondrocyte catabolic process. 156 Another major cause for OA is injuries, especially in young adults. In clinical, the destabilization of the medical meniscus, cartilage tear, and ligament strains can lead to biomechanical stresses and inflammation pathway activation. Among all the OA causes, inflammation is commonly observed and affects the entire synovial joint. Besides the conventional inflammatory factors and chemokines mentioned above, innate inflammatory signals also alter cartilage homeostasis and attribute to OA pathogenesis (see in review 157 ). Recent studies clarified an inflammation-chondrocyte re-programming response by ZIP8/Zn+/MTF1 axis, 158 mRNA decay, 159 and toll-like receptor (TLR)2-mediated aggrecan fragment effects 160 (see in review 150 ). In mRNA decay, the short-lived transcripts, such as a disintegrin and metalloprotease with thrombospondin motif (ADAMTS), hyaluronic acid synthase, and heparan sulfate sulfotransferase, are highly associated with catabolic process in OA chondrocytes.161,162 In the aggrecan fragment inflammatory effects, damage-associated molecular patterns, alarmins (S100A8 and S100A9), and complement can modulate the MMPs and ADAMTS through TLRs or the canonical NF-κB pathway.163,164 It is proposed that in OA cartilage, damage can drive changes in the underlying subchondral bone, and they reasoned that bone stiffness was increased by the healing of microfractures, resulting in overloaded cartilage.165–167 Another major cause to the OA is the genetic predisposition, which is highly significant from long-time family-based studies. 168 Meta-analyses and studies on genome-wide association have confirmed that over 80 gene mutations or single-nucleotide polymorphisms, including important structural and extracellular matrix (ECM)-related factors (COMP, Col9a1, and MGP), and critical signaling molecules in the Wnt (Sfrp3, FN1), BMP (Gdf5), and TGF-β (Smad3) signaling pathways, are involved in OA pathogenesis and are mostly implicated in OA by using genetic alteration mouse models,169–173 see in review 157 .
As the definition of OA in clinical is based on the presence of symptoms that drive the sufferer to seek medical help, subtypes of OA with new targets and mechanisms need to be further studied.
Therapies and Treatments to the OP and Bone Cell Senescence
The bone aging or bone cell senescence, as a major health problem worldwide, attracts research attention with drugs and therapies developed. 174 Due to the cell senescence, bone cells lose the ability to divide, which is noted as the major factor to age-related orthopedic diseases, such as OP, OA, bone fractures, and fragility. 175
During the study of bone cell senescence and bone aging, a variety of therapeutic modalities have been used in the treatments of the OP and OA.
In the OP therapies, the PTH and PTH-related protein (PTHrp) treatment are the most accepted and effective methods to regulate the bone anabolic. The human recombinant N-terminal 1–34 PTH (teriparatide) has been applied to the OP treatment, but is limited by treatment time. 176 In the osteoblast life cycle, the PTH and PTHrp, the only other known ligand of the PTH receptor, increase the life span of mature osteoblasts by preventing their apoptosis. 177 Thus, changes in the prevalence of osteoblast apoptosis should increase the total osteoblast population and alter the rate of bone formation. Daddona et al. developed a new teriparatide-coated microneedle patch system (ZP-PTH) to achieve an early increase in hip bone mineral density. 178 However, the microgravity caused by the PTH prevents a longer time use in OP treatment. 179
Oral CaR-antagonists or calcilytics were reported to stimulate endogenous transient PTH secretion and bone formation, and to prevent bone loss in ovariectomized rat model.180,181 MK-5442, a calcium receptor antagonist, was reported to result in transient pulses of PTH with bone formation markers increased quickly and bone resorption markers decreased temporarily. However, another Phase 2 study suggested a negative conclusion due to the bone mass density declined in the comparison with alendronate. 182 Thus, further work is recommended on this area.
Another medication therapy to the OP is antiresorptive drug, including five principal classes of agents: bisphosphonates, estrogens, selective estrogen receptor modulators, calcitonin, and monoclonal antibodies such as denosumab. 183 The antiresorptive therapies are expected to increase bone strength in individuals with OP. In the antiresorptive agents, bisphosphonates, which are given as the first-line prescriptive medications, have been proven for its safety and antifracture efficacy. 184 Currently, denosumab, class RANKL inhibitor, is under development. Preventing the RANKL/RANK interaction on the osteoblast, denosumab leads to the inhibition of osteoclast formation, function, and survival, thereby decreasing bone resorption and increasing bone mass in both cortical and trabecular bone. 176
Antagonists of Wnt-inhibitors, such as Sclerostin (SOST) and dickkopf-1 (dkk1), are used as an OP treatment by inhibiting canonical Wnt/β-catenin pathway specific to bone.185–187 The canonical Wnt/β-catenin pathway regulates the osteoblast precursor cell differentiation by Wnt exposure-caused accumulation of β-catenin in the nucleus. 188 With the β-catenin amount increased, the subsequent gene transcription initiates the to signal-dependent cell differentiation into the progenitor cells. 189 The osteoblast precursors are not exposed to a Wnt signal, so that β-catenin is degraded and osteoblast differentiation and recruitment are stopped. 176
A telomerase-focused therapy, reported by Simonsen et al., is used for MSC life span in immunodeficient mice model. 190 In their report, the human bone marrow stromal cells were stably transduced by a retroviral vector containing the gene for the catalytic subunit of human telomerase (hTERT). With the hydroxyapatite (HA)/tri-calcium phosphate (TCP) substitute, the cells were implanted into mice, formed normal bone tissue, and prevented senescence-associated impaired osteoblast functions.
In the OA therapies, in clinical opinion, all treatment modalities, including patient education, rehabilitation, exercise, modification of activities of daily living, pharmacotherapy, alternative medicine, and surgery should be considered. 191 The patient education, exercise, and pain release pharmacotherapy are parts of the symptom control in treatment modalities, which can help to improve the effect of the medication treatment or surgery therapy.
In medication treatments, alternative medicines have been studied for decades, with some of them applied in clinical. Chondroitin sulfate treatment is available to reduce the cartilage volume loss in knee OA with subchondral bone marrow lesion reduction. 192 Glucosamine sulfate is another popular treatment for OA, which is often taken alone or in combination with chondroitin sulfate. 191 As an amino-monosaccharide and a substrate of glycosaminoglycans and proteoglycans, the glucosamine sulfate has been shown to be as effective as ibuprofen in relieving the pain of OA and increase the joint movement, with no probable side effect shown yet. 193 The injection of hyaluronic acid is regarded as another effective therapy to rescue the meniscus tear and cartilage breakdown, and then decrease OA-related immune cells. 194
Due to the consideration from a plenty of area, the surgical treatment of OA is considered only after failure of nonsurgical treatments. There are four categories of nonbiological procedures considered surgical managements: osteotomy, arthroscopy, arthrodesis, and arthroplasty. 195 Osteotomies are performed in persons with early OA and may relieve symptoms and slow the rate of progression. 196 Arthroscopy can direct the debridement and lavage in cases of degenerative meniscal tears in the presence of mechanical symptoms and is limited by the substantial joint-space narrowing. 195 Arthrodesis is also named as joint fusion, which is commonly performed in the spine and in small joints of the carpus, hand, and foot. The significant defects of arthrodesis include patients' motion loss and major functional deficits at the surgery position. 197 Arthroplasty represents the most significant advancement in the treatment of OA. 198 Recently, the survival year of total knee arthroplasty (TKA) has been increased to 25–30 years, which indicates the reliability of the treatment. 199
Bone Substitute in the Aged Bone Model
Bone substitute or bone implant is a common and important therapy to bone defects in patients. The bone substitutes have been developed for more than 50 years and can meet most of the needs in general orthopedic patient cases. As one of the new developed topics, aging is quite a different area with a lot of studies needed to be done. Thus, the bone substitutes in aged bones draw attention for their specific characters and needs worldwide. Some of the in vitro and in vivo experiments were done on two main types of aged bones, OP and OA.
Bone repair in the OP patients
In age-related OP patients, the osteogenesis impair and angiogenesis impair are resulted by age-related changes in the hemostatic cascade, growth factor expression, osteoblast activity, osteoclast anabolism, and endothelial cell alterations. 200 Thus, numerous mediators have been identified to play a role in the process of fracture healing and direct the bone repair substitutes. Among the most predominant factors are acidic fibroblast growth factor (FGF), basic FGF, IGFs (IGF-1 and IGF-2), platelet-derived growth factor, TGF-β, and BMPs. 201 However, due to the reduction of the growth factor effects in the OP model, most of the current OP researches are focusing on the pharmacological agents, which have been introduced above.
Some of the researchers try to develop a new treatment method on the OP-related defects by implanting scaffold, and to induce the bone healing and repair at the fracture positions.
Zhang et al. fabricated a specific bone replacement material from poly-
Blouin et al. reported an injectable bone substitute (betaTCP/HA/hydroxy-propyl-methyl-cellulose) in the severely osteopenic and aged rat model. 203 The bone substitutes induced new bone formation shortly after implantation, but were resorbed without inducing lamellar bone. In addition, further experiments for the biomaterial trials with long-term implantation periods need to be conducted.
The bone resorption suppression is another method to treat the OP bone defects. A three-dimensional (3D) porous calcium-deficient HA scaffold with phytoestrogens was fabricated for osteoporotic bone tissue regeneration through 3D printing techniques. 204 With the dramatic decrease in osteoclast differentiation and proliferation, the bone formation was enhanced. An estrogen-studied group demonstrated that strontium-containing mesoporous bioactive glass scaffolds enhanced bone defect healing in the femurs of rats induced by ovariectomy. 205 Strontium(II)-doted calcium phosphate cement (CPCs) scaffolds exhibited good biocompatibility with bone formation enhancement in long-term in vivo study. 206 With comparison to the CPCs, the strontium (II)-doted CPCs had a higher bone mass density.
The MSC-associated scaffolds were reported in the OP treatment. 207 A long bone repair case with long-term implantation follow-up was reported successfully in a 41-year-old woman, who was treated with stem cells associated with marcoporous bioceramics. 208 With bone marrow-derived pluripotent MSCs derived into osteoprogenitors and seeded in a 4-cm height cylinder HA scaffold with 60% porosity, the patient was able to walk on the surgery leg after 10 months and had a good integration of the implant maintained after 6–7 years postsurgery.
Bone repair in the OA patients
Currently, the most effective treatments for OA are autologous chondrocyte transplantation and arthroplasty. Compared to the arthroplasty, the autologous chondrocyte transplantation has several limitations, including the need to use neighboring healthy donor cartilage, difficulties in treating large-scale defects, limited expansion capacity of primary chondrocytes, and the need for a periosteal patch to maintain engineered cartilage. 209 Thus, the arthroplasty, especially TKA, is recommended in most of the surgery cases.
In the arthroplasty, autologous bone graft is one of the methods to avoid immune system rejection. Total shoulder arthroplasty with autologous bone graft obtained from the humeral head was reported in treatment to glenohumeral OA with long-term follow-up. 210 Nicholson et al. also demonstrated a 34-patient case study with posterior glenoid bone grafting of humeral head autograft in total shoulder arthroplasty. 211
The decellularized ECM scaffolds and bioceramic grafts with growth factors are the major treatments to OA and can meet most requirements. 212 An implantation of a multiphasic osteochondral scaffold was reported by Di Martino et al. and represented a good option after failure of conservative management for early OA patients. 213 The ECM scaffolds were reported in OA treatment with multiple growth factors and drugs, especially in cartilage regeneration. A subcutaneous tendon/ligament with knitted silk-collagen sponge scaffold achieved satisfactory regeneration in anterior cruciate ligament and OA prevention due to its specific “internal-space-preservation” property in rat model. 214 Meng et al. constructed a composite scaffold combining MSC affinity peptide-modified demineralized bone matrix particles and chitosan hydrogel for cartilage engineering. 215 A microfiber scaffold with anti-inflammatory also aimed at the cartilage regeneration promotion. 216
In the OA treatments, the bioceramic grafts are widely used in the arthroplasties and joint replacements, such as TKA. Multiple bioceramic scaffolds and biocements were reported in the clinical arthroplasty.217,218 Antibiotic-laden bone cement is used in primary arthroplasties throughout Europe. 219 A geometry-specific calcium phosphate sheathed articular spacer was designed and 3D printed for infected hip arthroplasty. 220 During the joint arthroplasty development, new bioceramics are investigated and applied in the clinical, such as silicon nitride (Si3N4) 221 and calcium silicate. 222
Stem cell therapy also attracts attention on the OA treatment area. Arthroscopically obtained cancellous bone scaffold specimens were seeded with autologous human granulocyte colony-stimulating factor-activated peripheral blood stem cells and growth factors to induce the cartilage formation. 223 Monomeric, porous type II collagen scaffolds with chondroitin sulfate promoted chondrogenic differentiation of human bone marrow MSCs, potentially providing an eventual therapy to prevent OA. 224
Conclusion
In the way of understanding the bone aging and bone cell senescence, many hypotheses and models were proposed and proved. However, further investigations on the mechanisms are required. In addition, due to the large number of contributions to the bone remodeling, the normalization of the bone mass density and the balance of the remodeling are being revealed and can be led to changes by even single genetic deletion or factor secretion. There are still remaining questions about crosstalk between the coupling factors, effects of each factor, and their regulation during bone growth and senescence. Thus, the unresolved problems influence the OP and OA understanding and treatment development.
As highly prevalent severe diseases imposing a heavy burden of suffering on patients and costs to society, age-related OP and OA have been highly concentrated areas for decades. Therapies and treatments have been applied in clinic to help patients release their pain and improve life quality. Oral or injection pharmacratic agents are produced and tested in the past years. However, according to the safety consideration of side effects, such as PTH limit, more clinical needs on agents are required. Recently, the bone repair and bone graft were demonstrated as a valuable therapy in the OP following defects and OA surgery. Interestingly, the combination of the pharmacratic drugs and bone scaffolds dramatically enhanced the bone formation, bone cell balance, and bone strength. To continue, the bioscaffolds and bone grafts in the aged bone model will give us a new insight to successfully improve skeletal health.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was sponsored by National Natural Science Foundation of China for Innovative Research Groups (No. 51621002) and Shanghai Pujiang Program 18PJ1402400.