
Abstract
Porous polyethylene (pPE) is a frequently implanted biomaterial in craniofacial reconstructive surgery. Its rapid vascularization and tissue incorporation are major prerequisites to prevent complications, such as material infection, migration, and extrusion. To achieve this, several sophisticated strategies have been introduced and evaluated during the last 20 years. These include (i) the angiogenic stimulation of the host tissue with epidermal growth factor, basic fibroblast growth factor or macrophage-activating lipopeptide-2, (ii) material modifications, such as increase of surface roughness and incorporation of bioactive glass particles, (iii) surface coatings with growth factors, glycoproteins, acrylic acid, arginine/glycine/aspartic acid peptide as well as components of the plasminogen activation system and autologous clotted blood or serum, and (iv) the seeding with fibroblasts, chondrocytes, stem cells, or adipose-tissue-derived microvascular fragments. The majority of these approaches showed promising results in experimental studies and, thus, may be capable of improving the success rates after pPE implantation in future clinical practice.
Impact statement
This review provides an overview of strategies for the acceleration and improvement of the early vascularization and tissue incorporation of the commonly used implant material porous polyethylene (pPE). These strategies may not only improve the success rates of future clinical pPE implantation, but may also be transferable to other biomaterial applications in the field of tissue engineering and regenerative medicine.
Introduction
The face is considered as one of the most important body parts when undergoing surgery due to its permanent exposure and recognizability. 1 In craniofacial reconstructive surgery, facial-related tissue defects are commonly treated by the implantation of alloplastic biomaterials, particularly porous polyethylene (pPE), which has been developed and introduced into clinical practice in the early 1970s. 2
pPE is widely used for orbital floor restoration,3–5 auricular reconstruction,6–8 augmentation of the nasal architecture,9,10 and contour restorations.11,12 This biomaterial bears many advantages, such as its off-the-shelf availability in various shapes and sizes 13 as well as its long-term durability and stability.14–16 Moreover, pPE exhibits an interconnected porous structure enabling fibrovascular ingrowth and, by this, supporting the incorporation of the material into the surrounding tissue. 1 In addition, the good thermoplasticity of pPE implants allows their convenient adaption to patient-specific anatomic conditions. 17
However, despite all these advantages, most plastic surgeons still prefer autologous tissue for defect reconstruction because of the risk of pPE-associated complications, 18 including infection,19–21 migration,22–24 and extrusion25–28 of the implant material. The occurrence of such unwanted complications is caused by an insufficient early vascularization and incorporation of pPE.29,30 For instance, Stelter et al. 32 reported a high complication rate of >20% due to inadequate pPE vascularization after implantation into severely damaged scar tissue caused by multiple revision rhinoplasties. Hence, they concluded that pPE implants should only be used in (i) vital and healthy tissue, (ii) small pieces that can be totally embedded without any tension, and (iii) primary rhinoplasty under the absence of major scar tissue. 32 Jordan et al. 33 further demonstrated that pPE orbital implants require a longer time of at least 12 weeks for an adequate fibrovascularization in New Zealand albino rabbits when compared with Bio-Eye coralline hydroxyapatite (HA), FCI3 synthetic HA and aluminum oxide (Bioceramic). Accordingly, Tabatabaee et al. 34 reported a ∼5.5-times higher exposure rate of pPE (34%) when compared with HA implants (6.1%) in enucleated patients undergoing orbital floor reconstruction. Moreover, Thakker et al. 35 already detected the ingrowth of a dense fibrovascular tissue into implanted HA matrices after 6 weeks in Yucatan minipigs, whereas this process required at least 12 weeks when implanting pPE.
Taken together, these findings demonstrate that, despite its good reputation as a biomaterial for reconstructive surgery, pPE lacks a rapid and sufficient vascularization, particularly in the early stages after implantation and within poorly vascularized host tissue. To overcome this problem, several strategies have been developed and evaluated during the last years (Fig. 1), as outlined in the following sections.

Strategies for the acceleration of pPE vascularization as outlined in the present review. These strategies include (i) the angiogenic stimulation of the host tissue with EGF, bFGF, or MALP-2, (ii) material modifications, such as alterations of surface roughness and incorporation of bioactive glass particles, (iii) surface coatings with growth factors, glycoproteins, AA, RGD peptide, as well as components of the plasminogen activation system and autologous clotted blood or serum, and (iv) the seeding with fibroblasts, chondrocytes, stem cells (green circles), or MVF (blue lines). AA, acrylic acid; MVF, microvascular fragments; EGF, epidermal growth factor; bFGF, basic fibroblast growth factor; MALP-2, macrophage-activating lipopeptide-2; pPE, porous polyethylene; RGD, arginine/glycine/aspartic acid.
Literature Search
Literature searches were performed in PubMed and Google Scholar for original and review articles written in the English language focusing on vascularization strategies for pPE. The searches included the key words “porous polyethylene” and “Medpor”, which were paired with the key words “angiogenesis”, “vascularization”, “coating”, “growth factors”, “cellular seeding”, “stem cells,” and “microvascular fragments”. The searches included both animal and human studies. No restriction was set for the publication date.
Angiogenic Stimulation of the Host Tissue
A rather simple but effective approach to improve the vascularization of pPE is the local angiogenic stimulation of the host tissue at the implantation site. In a proof-of-principle study, Soparkar et al. 36 implanted pPE cubes into the dorsal paraspinal muscles of rabbits following a daily transcutaneous injection of either epidermal growth factor (EGF) or basic fibroblast growth factor (bFGF) for a total of 10 days. This treatment enhanced the fibrovascular integration of the implants when compared with saline-treated controls. However, in clinical practice such repetitive growth factor injections would not be very convenient for patients. For this purpose, a local single-shot application during the pPE implantation procedure would be much more practicable. This can be achieved by means of the toll-like receptor (TLR)-2/6 agonist macrophage-activating lipopeptide-2 (MALP-2) without inducing any local or systemic side effects. 37 Besides its immunomodulatory action, MALP-2 is a potent autocrine and paracrine stimulator of angiogenesis.38,39 Accordingly, it was demonstrated that a locally applied single shot of MALP-2 dose-dependently accelerates and improves the early vascularization of pPE during the first 14 days after implantation into mouse dorsal skinfold chambers. 37 Noteworthy, this type of topical tissue treatment may be also beneficial during the clinical implantation of other alloplastic biomaterials, because it is not time consuming, easily feasible, and independent from any elaborate material modifications.
Material Modification
Modification of surface roughness
The increase of the surface roughness and, consequently, the hydrophilicity by means of plasma etching is a widely used method to improve the biological response to implanted biomaterials.40,41 Therefore, it was analyzed whether this approach also enhances the vascularization and incorporation of pPE implanted into mouse dorsal skinfold chambers. 30 However, the angiogenic host tissue response to plasma-etched pPE was delayed and less pronounced than that to untreated controls. Scanning electron microscopic analyses further revealed a markedly reduced attachment of seeded human dermal microvascular endothelial cells on the surface of plasma-etched pPE (Fig. 2). 30 This can be explained by the fact that plasma etching changes the original surface of untreated pPE from a micro- to a nanorough topography, which is known to impair cell growth, migration, and adhesion.42,43 Hence, plasma etching may not be recommended to improve the clinical performance of pPE. However, this technique may be beneficial for other polyethylene-based implants, in which tissue ingrowth should be prevented, such as temporarily implanted drainages or catheters.

The effect of plasma etching on cellular attachment to pPE according to Laschke et al.
30
Incorporation of bioactive glass particles
Since the invention of the first 45S5 glass composition (Bioglass®) 50 years ago, 45S5-based and other types of bioactive glasses have been implanted in millions of patients worldwide, particularly for the reconstruction of bony and dental defects. 44 This class of biomaterials is characterized by a high biological activity due to the release of ionic dissolution products into the surrounding tissue. 45 Accordingly, bioactive glasses are osteoconductive, osteoinductive, anti-inflammatory, antibacterial, and proangiogenic.44,46 Based on these beneficial properties, melt-derived 45S5 Bioglass particles were incorporated into pPE in a volume ratio of 30:70. The resulting spherical-shaped composite has been approved by the Food and Drug Administration (FDA) in 2002 and is marketed as Medpor®-Plus™ (Porex Surgical, Newnan, GA). 44 Hence, the incorporation of bioactive glass particles into pPE is so far the only vascularization approach that has entered the stage of clinical application. However, only a few experimental and clinical studies have evaluated the in vivo vascularization properties of this modified pPE. Choi et al. 47 did not detect any significant differences in the extent of fibrovascularization between Medpor-Plus and control pPE orbital implants in rabbits. On the other hand, Naik et al. 48 reported in a small prospective, randomized study involving 10 patients with orbital implants that the vascularization of Medpor-Plus is faster when compared with that of Medpor, as assessed by repetitive planimetric 3-Tesla MRI analyses throughout an observation period of 4.5 months. This sparse and contradictory study situation indicates the need for additional systematic studies to confirm the superiority of Medpor-Plus over conventional pPE in improving fibrovascularization.
Surface Coating
Coating with growth factors
A common method to accelerate the vascularization of biomaterials is their coating with angiogenic growth factors, such as vascular endothelial growth factor (VEGF) or bFGF.49–52 For this purpose, the biomaterials are simply soaked in solutions for covalent growth factor immobilization or coated with growth factor-enriched carrier substrates.52,53 Park et al. 53 reported that bFGF-soaked pPE orbital implants promote the ingrowth of fibrovascular tissue and contain a higher number of proliferating vessels when compared with phosphate-buffered saline-treated controls. Soparkar et al. 54 coated pPE cubes with agarose containing different growth factors, such as EGF, bFGF, and transforming growth factor-α/β. After implantation into adipose and muscle tissue in rabbits, these factors improved both the vascularity and stromal density within the implants. Strieth et al. 55 coated thin pPE sheets with VEGF-supplemented Matrigel®, which represents a mixture of different extracellular matrix (ECM) components, and analyzed the vascularization of the implants by means of intravital fluorescence microscopy in the mouse dorsal skinfold chamber model. Although the vascularization did not markedly differ between VEGF-coated and uncoated pPE, they observed a reduced inflammatory host tissue response to VEGF-coated pPE, which additionally showed a tendency to improved mechanical integration. 55
These findings suggest that the coating of pPE with growth factors is beneficial. However, it should be noted that several studies also reported negative results when applying this vascularization strategy. For instance, Rubin et al. 49 and Sabini et al. 56 found that the coating of pPE implants with bFGF does not improve the ingrowth of vascularized tissue. These discrepancies may be explained by differing growth factor concentrations and delivery systems used in individual studies.
In general, it should be further noted that angiogenesis is a complex dynamic process, which is tightly regulated by the time-dependent interaction of various growth factors. 57 Hence, it may be much more effective to coat pPE with sophisticated delivery systems containing a combination of several growth factors with individually controlled release rates.
Coating with glycoproteins
Laminin, fibronectin and vitronectin are glycoproteins, which are most abundantly present in the ECM and are involved in the formation of new capillaries.58–60 Recently, Hessenauer et al. 31 found a severely compromised vascularization of pPE in knockout mice lacking vitronectin when compared with wild-type animals. Additional proteome profiling showed that the deficiency of vitronectin does not alter the composition and concentration of angiogenic proteins within the implants, indicating that this matricellular protein rather promotes pPE vascularization through mechanisms modulating the activity of angiogenic factors. 31 Hessenauer et al. 31 further found that surface coating with Matrigel enriched with recombinant vitronectin accelerates the vascularization of implanted pPE in wild-type mice and improves the maturation of newly developing microvascular networks. Based on these promising results, it would be interesting to conduct additional studies, investigating whether the coating of pPE with laminin or fibronectin, individually or in combination with vitronectin, also results in an enhanced implant vascularization.
Coating with acrylic acid and arginine/glycine/aspartic acid peptide
The coating of biomaterials with acrylic acid (AA) by plasma treatment involves the attachment of surface carboxylic acid groups, leading to improved cellular adhesion.61,62 Of interest, these groups can also serve as binding partners for the immobilization of additional cell-attracting factors, such as arginine/glycine/aspartic acid (RGD) peptide, which represents an essential cell adhesion peptide sequence in many ECM proteins.63–65 Park et al. 66 combined these two approaches to modify the surface of pPE anophthalmic orbital implants in rabbits. They found an enhanced fibrovascularization of AA-coated implants, which was further improved by additional immobilization of RGD peptides onto the AA-coated surface. Moreover, the inflammatory host tissue response to the surface-modified implants was milder than that to unmodified pPE throughout the first 4 weeks after implantation. This led to the conclusion that this novel approach may be capable of reducing the rate of exposure after anophthalmic socket implant surgery.
Coating with components of the plasminogen activation system
Plasmin is the key enzyme in the fibrinolytic cascade, which prevents thrombus formation by dissolution of fibrin polymers. 67 The activation of its zymogen plasminogen is tightly regulated by the interaction of the two serine proteases tissue plasminogen activator (tPA) and urokinase-type plasminogen activator (uPA) with plasminogen activator inhibitor-1 (PAI-1). 68 Of interest, there is an increasing body of evidence that these components of the plasminogen activation system are also involved in all phases of the angiogenic process. 69 In line with this finding, Reichel et al. 70 demonstrated that tPA, uPA, and PAI-1 exert a strong chemotactic effect on endothelial cells. Accordingly, they found that surface coating with recombinant uPA and to a lesser degree with tPA or PAI-1 significantly accelerates the vascularization of pPE implants in mouse dorsal skinfold chambers. 70
Coating with blood or serum
Soparkar et al. 54 and Sabini et al. 56 coated pPE with autologous clotted blood or serum to improve its in vivo tissue integration. After implantation into rats and rabbits, the coated pPE exhibited an improved vascularization and stromal density when compared with uncoated controls. This approach may be particularly suitable for translation into clinical practice for several reasons. The generation of an autologous blood or serum coating can be easily and rapidly performed during surgery in a cost-effective manner. Moreover, this type of coating bears the major advantage that it contains multiple angiogenic growth factors in a physiological combination that may ideally promote the development of mature microvascular networks within pPE implants.
Cellular Seeding
Seeding with fibroblasts
The involvement of fibroblasts in physiological and pathological angiogenesis is well recognized. 71 These cells produce various angiogenic and immunomodulatory factors. 72 Accordingly, Hussain et al. 73 investigated whether the seeding of pPE with dermal fibroblasts in vitro is also stable in vivo while promoting the vascularization and biocompatibility of the implants. For this purpose, pPE was cultured with green fluorescent protein (GFP)-transfected fibroblasts and subsequently implanted into dorsal skinfold chambers of GFP− mice. This GFP+/GFP− cross-over design revealed that 69% of the fluorescently labeled cells were still detectable at the end of the 10-days observation period. However, fibroblast-seeded pPE did not exhibit an improved vascularization and biocompatibility when compared with nonseeded controls. 73
Seeding with chondrocytes
Monroy et al. 74 used a pig model to show that in comparison to nonseeded controls chondrocyte-seeded pPE implants heal 30% faster when subjected to experimental exposure after a chronic implantation period of 10 weeks. Based on these findings, it was further analyzed whether the early vascularization of pPE is improved by vitalization with human chondrocytes. 75 For this purpose, platelet-rich plasma (PRP) was used as a carrier substrate for the cells. Of interest, after 14 days chondrocyte-seeded pPE exhibited a significantly higher density of blood-perfused microvessels when compared with nonseeded and PRP-seeded implants. Furthermore, the seeded chondrocytes formed a bioprotective layer around pPE, which prevented the accumulation of macrophages and, hence, their fusion into multinucleated giant cells. 75 These results indicate that chondrocytes do not only promote the vascularization of pPE, but also reduce the chronic foreign body reaction to the implant material.
The seeding of chondrocytes on pPE may bear several advantages when compared with other cell types. The isolation, in vitro expansion and seeding of chondrocytes onto various scaffolds is already well established in tissue engineering of cartilage. 76 In addition, chondrocytes have a low metabolic demand and, thus, are able to survive to a certain extent by diffusion alone. Accordingly, these cells may be more resistant to hypoxic cell death during the early phase after pPE implantation.
Seeding with stem cells
Stem cells are the most frequently used cell source in the field of tissue engineering and regenerative medicine. For clinical applications, they may be autologously harvested in large amounts from blood, bone marrow, or adipose tissue, avoiding the need for immunosuppressive therapy to prevent rejection after transplantation. Due to their high plasticity, stem cells are not only suitable for the differentiation into organ-specific cells but also into vascular cell lines. Hence, they offer the unique possibility to generate prevascularized tissue constructs originating from one cell source. 77 Moreover, they release various cytokines and growth factors, which can additionally stimulate the formation of new blood vessels by angiogenesis or vasculogenesis. 78 Accordingly, studies reported that stem cell seeding markedly improves the vascularization of different biomaterials.79–82
In line with these findings, Han et al. 83 found that pPE discs seeded with human bone marrow stromal cells release higher levels of bFGF when compared with fibroblast-seeded and nonseeded controls. The stem cell-seeded pPE also exhibited a significantly increased microvessel density 3 weeks after implantation into the back of rats. Similar results were reported by Moon et al. 84 In a mouse model of diabetic wound healing they showed an improved vascularization of pPE discs seeded with human umbilical cord blood-derived mesenchymal stromal cells when compared with fibroblast-seeded and nonseeded controls. Lee et al. 85 seeded pPE with adipose-derived adult stem cells (ADASCs) to determine their effect on implant vascularization after implantation into the back of athymic nude mice. To facilitate the adherence of the cells to the hydrophobic material, they added fibrin in different concentrations to the cell suspension. After 10 days, ADASC-seeded pPE revealed a significantly higher fibrovascularization when compared with controls. Of interest, a fibrin concentration of 0.5% supported this fibrovascularization, whereas the use of 1.25% fibrin resulted in a decreased vascularization. These results indicate that a too high fibrin concentration reverses its positive effect on cellular activity and microvascular network formation, most probably due to the inhibition of cell mobility. 85
Seeding with adipose tissue-derived microvascular fragments
In recent years, microvascular fragments (MVF)-seeding of various biomaterials, including porous polyurethane, 86 Integra® matrix wound dressing and flowable wound matrix87,88 as well as thermoresponsive hydrogel, 89 has emerged as a novel strategy to accelerate implant vascularization. MVF are a mixture of functional native arteriolar, capillary, and venular segments that can be enzymatically isolated from adipose tissue in a short time of only ∼20 min. 90 Once seeded onto a biomaterial, MVF are able to rapidly reassemble into new microvascular networks and to develop interconnections to the surrounding host microvasculature, resulting in a fast onset of blood perfusion throughout the implant. 91 In line with these findings, we could demonstrate that the biological coating with PRP and MVF improves the vascularization, biocompatibility, and tissue incorporation of pPE. 92 In fact, during the first 14 days after implantation into mouse dorsal skinfold chambers, PRP/MVF-coated pPE exhibited a significantly higher density of blood-perfused microvessels when compared with PRP and uncoated controls (Fig. 3). Moreover, MVF promoted proangiogenic M2 macrophage polarization at the implantation site. 92 These promising experimental findings demand for the translation of this novel vascularization strategy into clinical practice. For this purpose, MVF bear the advantage that they can be harvested from autologous fat during liposuction. In addition, similar to PRP, it may be possible to isolate them by means of automated systems in an intraoperative one-step procedure under good manufacturing practice conditions.
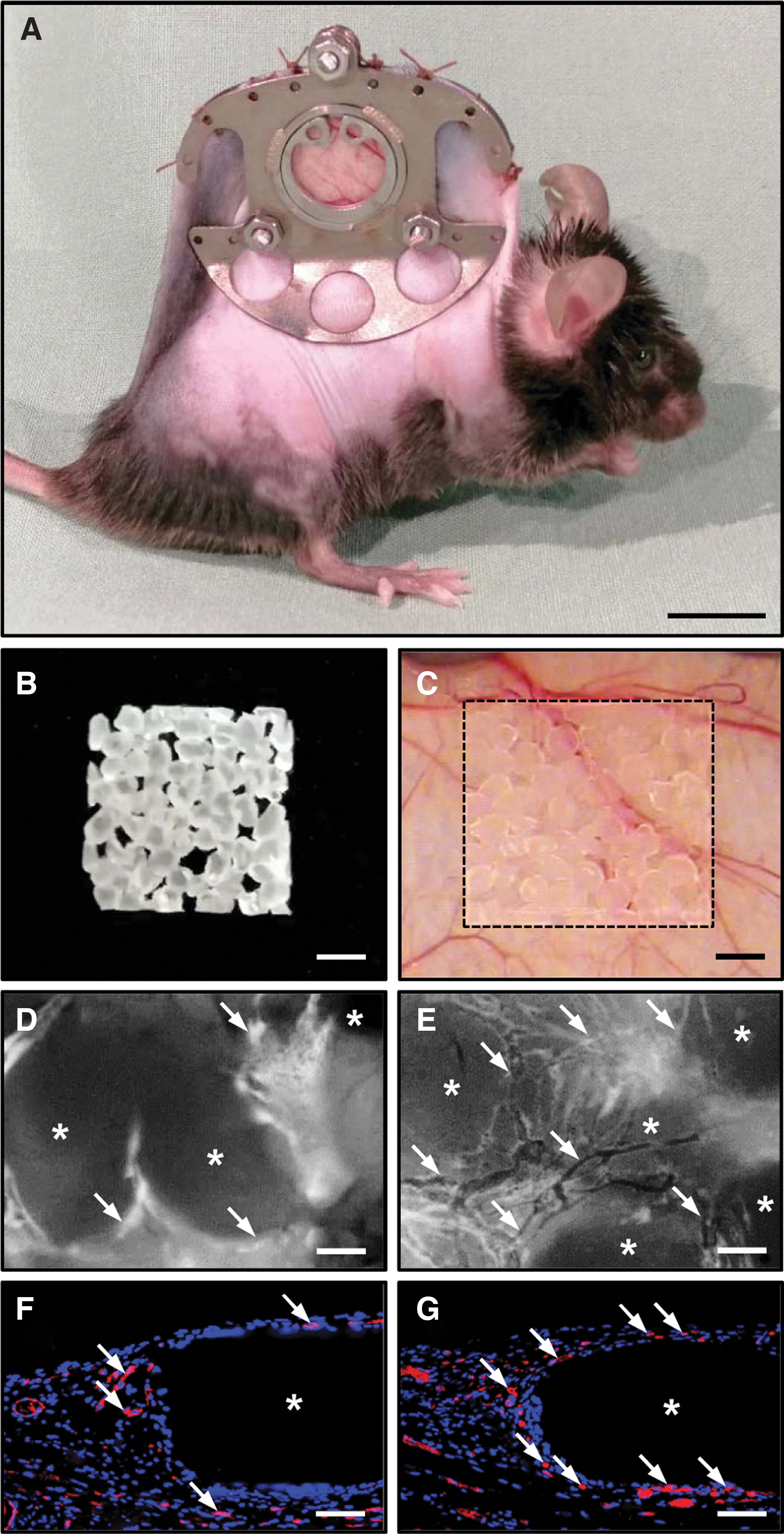
Improvement of pPE vascularization by biological coating with PRP and MVF according to Später et al.
92
Conclusion
During the last 20 years, several strategies have been introduced and evaluated to accelerate and improve the early vascularization and tissue incorporation of implanted pPE, including (i) angiogenic stimulation of the host tissue, (ii) material modifications, (iii) surface coatings, as well as (iv) seeding with cells and MVF (Table 1). The herein presented studies indicate that these strategies may contribute to reduce pPE-associated complications, such as infection, migration, and extrusion, and, thus, may improve the success rates of future clinical pPE implantation.
Major Characteristics of Different Vascularization Strategies for Porous Polyethylene
+, low; ++, medium; +++, high.
AA, acrylic acid; MVF, microvascular fragments; EGF, epidermal growth factor; bFGF, basic fibroblast growth factor; MALP-2, macrophage-activating lipopeptide-2; RGD, arginine/glycine/aspartic acid; tPA, tissue plasminogen activator; uPA, urokinase-type plasminogen activator; PAI-1, plasminogen activator inhibitor-1.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.