
Abstract
Delayed healing and nonunion formation are major challenges in orthopedic surgery, which require the development of novel treatment strategies. Vascularization is considered one of the major prerequisites for successful bone healing, providing an adequate nutrient supply and allowing the infiltration of progenitor cells to the fracture site. Hence, during the last decade, a considerable number of studies have focused on the evaluation of vascularization strategies to prevent or to treat nonunion formation. These involve (1) biophysical applications, (2) systemic pharmacological interventions, and (3) tissue engineering, including sophisticated scaffold materials, local growth factor delivery systems, cell-based techniques, and surgical vascularization approaches. Accumulating evidence indicates that in nonunions, these strategies are indeed capable of improving the process of bone healing. The major challenge for the future will now be the translation of these strategies into clinical practice to make them accessible for the majority of patients. If this succeeds, these vascularization strategies may markedly reduce the incidence of nonunion formation.
Impact statement
Delayed healing and nonunion formation are a major clinical problem in orthopedic surgery. This review provides an overview of vascularization strategies for the prevention and treatment of nonunions. The successful translation of these strategies in clinical practice is of major importance to achieve adequate bone healing.
Introduction
During the last decade, a considerable number of research studies have provided a fast-growing knowledge on the mechanisms of bone healing. However, despite increasing insights in the morphological and molecular basis of fracture repair, the causes of bone healing failure remain mostly unclear. In clinical practice up to 10% of all fractures still show delayed healing or nonunion formation. 1 Especially, segmental bone defects, infections and mechanical instabilities bear a high risk of nonunion formation and, thus, remain a major clinical problem.2,3 For the patient, nonunions are associated with significant pain and loss of function, which requires additional surgical interventions. For the health care system, nonunions cause a substantial economic burden. 4
There are variabilities in the definition of delayed healing and nonunion. 5 The U.S. Federal Drug Administration council defines a nonunion as ‘failure to achieve union by 9 months since the injury, and for which there has been no signs of healing for 3 months'. 6 In contrast, others define nonunion in long bones after a period of 6 months with no radiological signs of fracture healing. 6 It should be noted that the diagnosis of nonunion should consider both the radiological and the clinical examination of the patient. 7
Several treatment strategies have been studied to overcome nonunion formation, but, until today, no ideal management has been established. Autologous bone grafts can be considered the gold standard 8 ; however, they are associated with a high donor site morbidity 9 and they are restricted by a shortage of available bone graft material, in particular if previous harvests have been performed. The use of allografts is not restricted by shortage; however, this technique is limited due to large differences in the interindividual quality of the graft material and by a failure rate of up to 60%. 10 Accordingly, substantial efforts have to be made during the next years to fully understand the pathophysiology of nonunion formation and to develop effective and safe treatment strategies for preventing the failure of bone healing.
Bone is a highly vascularized connective tissue that relies on an adequate spatial and temporal interaction between blood vessels and bone cells. 11 Therefore, angiogenesis and vascularization play a crucial role for successful bone healing, being among the first steps that occur during the physiological sequences of both endochondral and intramembranous fracture repair. 11 After the formation of an organized granulation tissue, newly formed blood vessels provide an adequate nutrient supply to the fracture area and allow the infiltration of cells vital for callus remodeling from avascular cartilage toward mineralized woven bone12–14 (Fig. 1). The importance of this early vascularization for successful bone healing is clearly indicated by animal studies, which revealed that a blockade of angiogenesis by TNP-470, nonsteroidal anti-inflammatory drug, or fumagillin inhibits fracture repair and eventually leads to nonunion formation.15–17 In a closed murine femoral fracture model, radiographical, histological, and biomechanical analyses have shown that the angiogenesis inhibitor TNP-470 completely prevents fracture healing, leading to a bone tissue that resembles an atrophic nonunion. 18 Hence, a disturbed vascular supply must be considered a determinant for the failure of fracture healing, most probably due to hypoxia and a reduced nutrient supply to the site of injury.
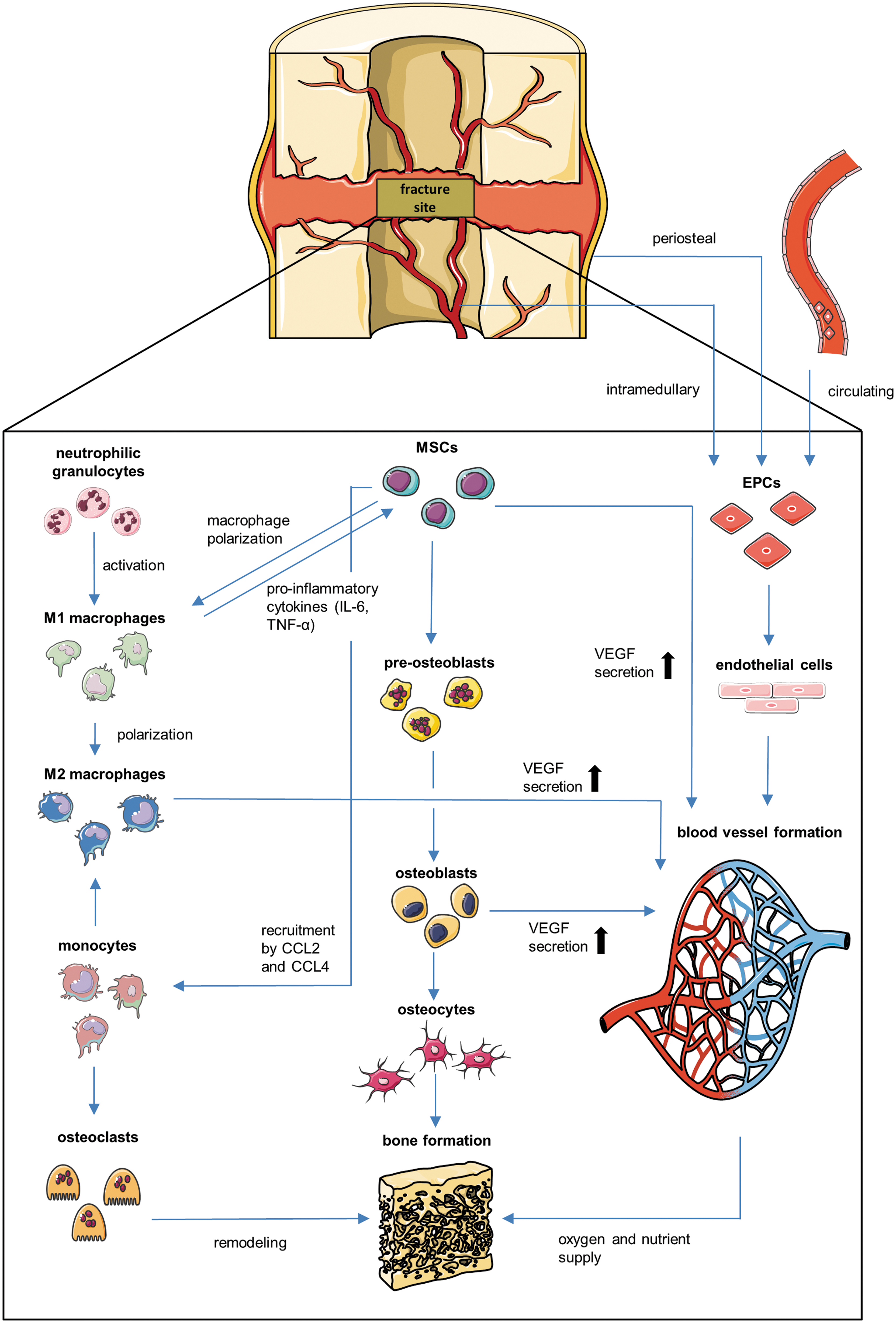
Cellular interactions and mechanisms during fracture healing. During the initial phase of fracture healing, the hematoma triggers an immune response. Neutrophilic granulocytes within the fracture site activate macrophages. Activated M1 macrophages promote the migration of MSCs to the fracture site by proinflammatory cytokines (IL-6 and TNF-α). In turn, MSCs initiate the polarization of macrophages into the M2 phenotype and mediate the recruitment of macrophages by the release of CCL2 and CCL4. Furthermore, MSCs differentiate into preosteoblasts, osteoblasts, and finally osteocytes, which form the bone tissue. In addition, monocytes differentiate into osteoclasts and enable bone remodeling. Blood vessel formation within the fracture callus is mediated by circulating EPCs as well as EPCs originating from the intramedullary and periosteal vasculature. These EPCs develop into endothelial cells and form the vascular network of the callus tissue. MSCs, M2 macrophages, and osteoblasts contribute to the formation of the vascular network by VEGF secretion. CCL2, chemokine ligand-2; CCL4, chemokine ligand-4; EPCs, endothelial progenitor cells; MSCs, mesenchymal stem cells; VEGF, vascular endothelial growth factor.
Based on these findings, the stimulation of vascularization is thought to be of major importance in both the prevention and treatment of nonunions. In this review, we provide an up-to-date overview of currently existing and emerging vascularization strategies to overcome nonunion formation, such as (1) biophysical applications, (2) systemic pharmacological treatment, and (3) tissue engineering, including new scaffold materials, growth factor delivery systems, and cell-based and surgical approaches.
Preclinical Nonunion Models
A large number of preclinical nonunion models are available to study the mechanisms and the treatment of nonunion formation. In the past, large animal models19–21 have been popular to study delayed fracture healing. Today, rodent animal models are preferred. Distinct models in rats, including atrophic and hypertrophic nonunions, have been developed to study healing promoting treatment strategies.22,23 The atrophic models can be categorized as either (1) defects with a size of 3–8 mm or (2) defects <3 mm with induction of additional periosteal or endosteal injury. 22 Large segmental defects have the advantage of mimicking the resection of established nonunions in clinical practice and are especially suited for tissue engineering applications. However, they do not resemble the pathophysiology of trauma-induced fractures, because they are induced by osteotomy. This problem may be overcome by the use of a simple fracture model with additional periosteal injury. 24 The periosteal injury is thought to imitate the avascular and biologically inert environment of atrophic nonunions.
In mice, the development of an appropriate nonunion model is challenging because technically demanding. Accordingly, only few models are described. 22 The first nonunion model in the mouse was developed by Choi et al. 25 It consisted of a tibia osteotomy, which was distracted by an external fixator. Because bone healing failure was observed in only 60%, it may not be acceptable for standardized analyses of nonunion formation.
A nonunion in the mouse can also be induced by osteotomy and periosteal cauterization. 26 This, however, results in a hypertrophic nonunion, which is not the primary interest of most of the researchers. In clinical practice, hypertrophic nonunions are regularly treated with a high success rate just by stable re-osteosynthesis, indicating that they do not represent a major challenge. 22
Because atrophic nonunions represent a critical challenge in orthopedic surgery, there is indeed a need for adequate mouse models to improve the understanding of the mechanisms of healing dysfunction and to develop novel treatment concepts. Today, two standardized atrophic nonunion models in the mouse femur are reported.27,28 In the first, a 1.8-mm osteotomy is stabilized by a pin and a clip, 27 in the second, a 2-mm segmental defect is stabilized with an interlocking nail, comparable to a human intramedullary locking nail. 28 Both models demonstrate reliable atrophic nonunion formation and allow the implantation of new bone substitutes and tissue engineering constructs.
Biophysical Applications
Biophysical stimulation in orthopedic medicine represents a minimal-invasive therapeutic approach to enhance and improve reparative and anabolic tissue activities. Extracorporeal shock wave therapy (ESWT), low-intensity pulsed ultrasound (LIPUS), and hyperbaric oxygenation (HBO) are able to stimulate the upregulation of proangiogenic growth factors, and, thus, the process of vascularization, osteogenesis, and bone formation.29–31
ESWT is based on the generation of shock waves that are focused on the diseased tissue area of the patient. The application of ESWT in orthopedics includes a large number of diseases, such as proximal plantar fasciitis, 32 lateral epicondylitis of the elbow, 33 calcifying tendinitis of the shoulder, 34 and, also, nonunion formation. In a clinical study, Cacchio et al. 35 compared the outcome of ESWT to surgical treatment in the management of long-bone nonunions. Radiological analysis revealed a healing rate of 70–71% in nonunions treated with ESWT and 73% in nonunions treated surgically. Of note, the short-term clinical outcome showed even better results after shock wave treatment when compared to surgery. 24 However, taking other studies into account, it should be noted that the success rate of ESWT shows a great variability, ranging from 50% to 89%.36–41 The exact mechanisms of the stimulatory activity of ESWT in the healing of nonunions are not fully understood. It is speculated that shock waves induce the growth and differentiation of bone marrow-derived osteoprogenitor cells. Interestingly experimental studies could demonstrate that these tissue responses trigger the release of vascular endothelial growth factor (VEGF),42,43 indicating a proangiogenic mode of action in shock wave therapy. Moreover, it has been reported that ESWT enhances the transmembrane current and the voltage dependence of Ca-activated and K channels, and thereby affects ion transportation and positively influences cell proliferation. 44
LIPUS represents another noninvasive technique to stimulate bone formation by applying ultrasound waves on the fracture site. In vitro studies revealed that LIPUS promotes the differentiation of periosteal cells and mesenchymal stem cells (MSCs) into the osteogenic lineage.29,45 Moreover, clinical studies showed an increased healing rate of delayed healing bones or nonunions in LIPUS-treated patients.46–49 In a clinical study, Zura et al. 50 reviewed the outcome of 767 patients with established nonunions from 1 to more than 10 years. Patients treated with LIPUS showed a promising healing rate of 86.2%. Similar to ESWT, the beneficial effect of LIPUS in nonunions is thought to be mediated by the release of proangiogenic cytokines, an improvement of microvascular blood perfusion, and the promotion of the transport of nutrition and enzymes, including calcium ion transport-related proteins.51,52 In contrast, in a recently published clinical statement, Poolman et al. 53 did not recommend the use of LIPUS in bone healing. This recommendation against the use of LIPUS was based on the negative findings of a systematic review of randomized controlled trials analyzing the outcomes of LIPUS on the healing of fresh fractures, in particular, operatively managed tibial and clavicle fractures. 54 In fact, Poolman et al. 53 stated that ‘if LIPUS on fresh fractures does not decrease the incidence of nonunions, it is unlikely to exert a beneficial effect in the conversion of nonunions into healed bones.’ Of interest, trials including patients with nonunions were either at high risk of bias or did not contribute sufficient outcome data to the systematic review. Thus, we feel that further appropriate clinical trials, studying LIPUS in nonunion healing, are necessary.
HBO defines the systemic application of pure oxygen in an elevated ambient pressure, resulting in a temporarily increased partial pressure (pO2) of oxygen within the tissue or organism. As early as 1966, Coulson et al. 55 could prove a favorable effect of HBO on fracture healing in a rat femur. These initial findings were supported by further in vitro and in vivo studies exploring the impact of HBO on bone regeneration. Wu et al. 56 reported an increased alkaline phosphatase activity in human osteoblasts treated with HBO, which was associated with enhanced mineralization, bone nodule formation, and calcium deposition. In vivo, animal studies showed beneficial effects of HBO on bone mineral density and bone formation in distraction osteogenesis and critical-size defects.57,58 Furthermore, hyperoxia is known to trigger tissue vascularization and improve bone repair in ischemia-induced delayed healing, indicating beneficial effects in the treatment of nonunions. 59 These results were confirmed by others in the treatment of bone defects, using a combination of autologous bone grafting and HBO without or with platelet-rich plasma (PRP). HBO resulted in a significantly enhanced angiogenesis, which was associated with an improved bone formation.31,60 However, data on HBO treatment in clinical trials are sparse. Two Cochrane data base reviews analyzed the outcome of HBO treatment on osteonecrosis of the jaw and found no convincing evidence for beneficial effects of HBO. This may be due to a suboptimal reporting and insufficient sample sizes of the included studies. Hence, one of the major challenges will be the development of well-designed and conclusive clinical trials to prove the efficiency of HBO treatment in bone regeneration.61,62 Moreover, HBO is associated with severe side effects, including visual changes, nausea, dizziness, convulsion as well as the formation of free oxygen radicals, which may have cytotoxic effects on cells and tissues. 63
Electric stimulation (EStim) is another biophysical application, which is used in the field of bone regeneration. In the clinical setting, EStim is administrated by using three different approaches: (1) direct current (DC), (2) pulsed electromagnetic field (PEMF), and (3) capacitive coupled (CC). 64 DC EStim is applied by a surgically implanted power source, which generates dosages between 10 and 100 μA. PEMF and CC, on the other hand, are both applied externally. PEMF current-carrying coils, placed on the skin over the fracture site, generate a PEMF ranging between 3 and 10 V peak-to-peak. EStim by CC generates an electrical field of 0.1–20 G by using an alternating voltage to cutaneous electrodes placed on the opposite site of the fracture. 64 For decades, the effect of EStim on bone regeneration has been studied in preclinical and clinical practice. Recent in vitro studies indicate that EStim promotes bone healing by influencing behavior and function of bone-forming stem cells, including migration, proliferation, differentiation, and mineralization. 65 In addition, Leppik et al., 66 demonstrated that the combination of EStim and bone tissue engineering successfully promotes bone repair of large bone defects in a rat model. Moreover, the authors found an increased blood vessel formation in bone defects treated with EStim. This proangiogenic effect of EStim is most likely mediated by stimulating angiogenic responses of vascular endothelial cells and selectively regulating growth factors and cytokines, which are vital for angiogenesis through a VEGF receptor-dependent feedback loop. 65 In clinical practice, a variety of studies have shown the beneficial effect of EStim on bone healing, including the treatment of delayed healing and nonunions. Despite these positive results, EStim has not become a widespread, universally used clinical treatment approach in orthopedic surgery. This may be not only due to the considerable number of complications, such as damage or disconnection of the implanted stimulators, but also due to the great variations of application and the high costs associated with EStim.
Taken together, biophysical applications stimulate bone regeneration by triggering proangiogenic pathways and, thus, vascularization. Application of ESWT and LIPUS represents a noninvasive and practical alternative to the use of bone allografts in revision surgery; however, the success rates reported are highly variable between the different clinical studies. The promising results of HBO make this approach an appealing stand-alone treatment as well as a potential adjuvant therapeutic option in combination with autologous bone grafting. Nonetheless, the amount of existing data is limited to experimental studies, while data from clinical trials are still lacking. EStim has proven its efficiency in bone regeneration in preclinical and clinical trials, but its use is yet limited due to financial hurdles and the vulnerability of the applied stimulators and implants.
Systemic Pharmacological Treatment
Systemic pharmacological treatment to promote the process of vascularization in bone regeneration bears the advantage of being feasible and easy to perform. Erythropoietin (EPO) is the primary regulator of erythropoiesis, but may also be a promising candidate for the improvement of angiogenesis and vascularization in delayed bone healing and nonunion formation. EPO has been shown to exert cell protective, proangiogenic, and regenerative actions in a variety of tissues.67,68 For instance, experimental studies in the dorsal skinfold chamber model reported that EPO successfully protects musculocutaneous tissue from ischemic damage and improves and accelerates skin wound healing.69–71 In bone, EPO is capable of stimulating endochondral ossification and fracture repair.72–74 In addition, Holstein et al. 75 could demonstrate that EPO promotes cell proliferation, angiogenesis, and bone formation in a nonunion model in mice. Their microcomputed tomography (μCT) and histomorphometric analysis revealed a significantly increased bone volume and bridging rate in EPO-treated animals. This was associated with a higher expression of VEGF and an increased density of blood vessels in the early phase of bone defect healing when compared to controls. 54 Therefore, it may be speculated that the improved bone regeneration observed in EPO-treated animals in this nonunion model is caused by an EPO-induced stimulation of vascularization. These findings were confirmed in subsequent experimental studies, revealing that both systemic as well as local EPO treatment trigger angiogenesis and promote bone regeneration in critical-sized bone defects.76,77
Another systemically applied substance that may support bone healing is granulocyte colony-stimulating factor (G-CSF). G-CSF, an important mediator of granulopoiesis, can be used in the treatment of diseases, involving impaired vascularization78–80 by mobilizing endothelial progenitor cells (EPCs) into the circulation.81,82 Herrmann et al. 83 analyzed the effects of G-CSF treatment in a critical-size segmental femoral defect model in rats. Interestingly, they found an enhanced bone formation and a reduced gap size in G-CSF-treated animals, most likely caused by the induction of early neovascularization. 62 These results are supported by Ishida et al., 84 who found an increased capillary density in bone defects after local and systemic G-CSF treatment. Therefore, G-CSF represents a promising compound to enhance vascularization in bone regeneration.
Human parathyroid hormone (hPTH) (1–84) and the shortened recombinant peptide teriparatide (parathyroid hormone [PTH] 1–34) are main regulators of calcium metabolism. These days, PTH is the sole clinically approved drug with osteoanabolic properties and, thus, is well established in the treatment of osteoporosis.85,86 Furthermore, PTH treatment is known to accelerate fracture healing87–90 and to promote bone formation in segmental bone defects.91,92 Of interest, the impact of PTH on vascular regeneration and proliferation may contribute to its anabolic properties in bone regeneration applications. Bone endothelial cells respond to PTH treatment by stimulation of cyclic adenosine monophosphate (cAMP)-related signal transduction 93 and, thereby, influence pathways regulating gene expression in cell proliferation and differentiation. 94 In addition, PTH enhances the migration of proangiogenic C45+/CD34+ cells as well as the upregulation of VEGF-A mRNA, resulting in an increased neovascularization and cell survival. 95 An experimental study by Xie et al. 96 demonstrated that systemic teriparatide treatment facilitates neovascularization, bone formation, and degradation of β-tricalcium phosphate (TCP) in critical-size bone defects. Moreover, teriparatide modulates angiogenesis in bone allografts, resulting in a higher number of blood capillaries, and, simultaneously, narrows blood vessel diameters, indicating a matured capillary network. 97 These findings support the view that PTH stimulates the process of bone regeneration by inducing new blood vessel formation.
The systemic pharmacological treatment with EPO, G-CSF, and PTH fosters bone regeneration by increasing the expression of proangiogenic factors as well as the mobilization of EPCs and immune cells in the circulation, resulting in an enhanced vascularization. EPO and PTH have even the advantage of acting both proangiogenic and pro-osteogenic. Hence, these compounds represent promising and simply applicable treatment strategies during a critical course of fracture healing to prevent nonunion formation. In contrast, VEGF, which is one of the most potent angiogenic factors and which may act also pro-osteogenic, may not be used for the systemic pharmacological treatment. This view is based on the fact that it is a key mediator of angiogenesis in cancer in which it is upregulated by oncogene expression. 98 Therefore, local as well as systemic treatment with VEGF may likely induce and promote malignant transformation.
Indeed, it has to be taken into account that all types of pharmacological treatment bear the risk of potential side effects. For instance, EPO increases systemic hematocrit levels, elevating the risk of thromboembolic events,99,100 whereas possible side effects of GCS-F treatment include the promotion of tumor metastasis. 101 Systemic PTH treatment may lead to a disturbance in calcium metabolism and high levels of PTH may even cause bone resorption, resembling the symptoms of hyperparathyroidism. 102 Thus, despite the promising data achieved from experimental studies, systemic pharmacological treatment has to be carefully monitored when applied in the clinical setting.
Tissue Engineering
Scaffold-based vascularization strategies
Scaffolds for bone regeneration applications should (1) promote cell viability and proliferation, (2) exhibit osteoinductive and load-bearing properties, and (3) induce an angiogenic tissue response with ingrowth of newly developing microvessels. During the last decade, a variety of biomaterials was carefully investigated, including bone grafts, polymers, calcium phosphates, and ceramics. Each of these materials has a specified biocompatibility, osteoinductivity, and bioresorbability. 103 Besides these chemical characteristics, the three-dimensional (3D) architecture of the scaffolds is of major importance for the development of a suitable bone graft substitute. Porous architecture is a widely used scaffold design, because it mimics the natural structure of bone and allows the infiltration of osteoblasts and endothelial cells, thereby promoting vascularization and bone formation within the scaffold. 104 Interestingly, vascularization and bone formation are dependent on the scaffolds' pore size. In scaffolds with a pore size <100 μm, vascularization and bone formation are restricted to the border margin, resulting in a low perfusion of oxygen and nutrients throughout the material. 105 In contrast, scaffolds with a pore size >200 μm enable a high osteoinductivity and vascularization throughout the entire scaffold structure.106,107 As an alternative to a porous architecture, several studies propose a tubular scaffold design to imitate the tubular structure of native bone with potential benefits on neovascularization and bone tissue infiltration.108,109 Feng et al. 110 compared β-TCP scaffolds with different porous and tubular architectures in a radius bone defect model in rabbits and found an enhanced neovascularization, mechanical strength, and defect healing in tubular scaffolds, indicating their superiority in bone tissue engineering applications.
Bioactive glass represents a promising compound for bone tissue engineering, as various studies demonstrated its proangiogenic111–113 and pro-osteogenic properties. 114 Scaffolds made of bioactive glass induce proliferation and cell growth of MG-63 osteoblast-like cells. 115 Its potential to improve neovascularization and bone regeneration was confirmed in vivo by an experimental study using calvarial defects in rats. 116 In clinical practice, however, it has received little attention as bone scaffold material, despite the excellent biological performance. This may be due to the limitations of the original 45S5 Bioglass® to develop into porous constructs.117,118 Of interest, this problem can be overcome using bioactive glass fabricated by 3D printing, which can be easily densified by viscous flow sintering to achieve a biomechanical strength similar to that of human cortical bone. 119 Moreover, Jia et al. 120 demonstrated that bioactive glasses, consisting of silicate and borosilicate, induce a bridging rate and a mechanical function in bone defects comparable to those treated with autologous bone grafts. Of note, the borosilicate composites even showed an enhanced number of blood vessels 3 months after implantation, proving the competence of bioactive glass to induce vascularization at an early stage of defect repair. The ability of bioactive glass to promote angiogenesis was further confirmed in an in vitro study by measuring elevated VEGF levels in a MC3T3-E1 line of murine preosteoblastic cells seeded on glass scaffolds. 121 In a recent study, Wu et al. 122 developed an injectable hydrogel with copper-containing bioactive glass nanoparticles. The resulting gel triggered the growth of seeded MC3T3-E1 cells and human umbilical vein endothelial cells, and fully restored bone defects with the formation of vascularized bone tissue in a critical-size rat calvarial bone defect model. 122 This underlines the potential of bioactive glass as a tool to promote vascularization in bone regeneration. By changing the bioglass composition and by addition of therapeutically active ions, such as boron, the biological characteristics of the bioglass scaffolds can be tailored toward specific needs and areas of application. This allows to further ameliorate the proangiogenic and pro-osteogenic properties of bioglass and develop innovative and powerful bone tissue engineering constructs. 123
The vasculature of the periosteum controls the blood perfusion of the bone. Bone defects caused by high-energy trauma are often associated with severe damage to the periosteum, leading to an increased risk of nonunion formation due to alteration of blood perfusion. Therefore, the generation of an artificial periosteum, which provides a sufficient microvascular network to deliver nutrients for osteogenesis, represents an interesting, but ambitious novel treatment strategy.124,125 Xin et al. 126 designed a novel gelatin hydrogel membrane by an inorganic and organic co-cross-linked network, consisting of mesoporous bioactive glass nanoparticles and a photo-cross-linkable gelatin derivative. This hydrogel membrane demonstrated a considerable capacity to induce vascular regeneration and osteogenesis in a rat calvarial critical-size defect model, making it a promising approach in bone tissue engineering.
Current progress in nanotechnology also directs the attention on nanohydroxyapatite (nHA) for bone tissue engineering. Its chemical structure and size resemble native bone mineral crystals. Porous nHA presents with osteoinductive and osteointegrative properties, however, lacks a proangiogenic potential. 127 To overcome this limitation, that is, to enhance the vascularization potential of nHA scaffolds, the cell- and growth factor-free supplementation with trace elements like strontium (Sr), iron (Fe), and silicon (Si) represent an interesting and cost-effective approach. Nowadays, Si-substituted hydroxyapatite (HA) is approved in clinical practice and commercially available (Actifuse®; Baxter GmbH, Unterschleißheim, Germany). In the attempt to mimic the needle-/rod-shaped structure of native bone, Anitha et al. 128 developed a nanocomposite matrix containing HA-silica core-shell nanorods. This improved (1) the viability, functionality, and proliferation of endothelial cells in vitro, (2) induced new blood vessel formation and vascularization in vivo, and (3) promoted new bone formation in a femoral critical-size defect in rats. 99
Other new nanomaterials, which are capable of stimulating angiogenesis and enhancing bone formation in critical-size defect models, include europium-doped mesoporous silica nanoshperes, 129 silicon oxynitrophosphide, 130 and collagen scaffolds incorporated with strontium-graphene oxide nanocomposites. 131 These studies reflect the tremendous potential of sophisticated nanofabricated scaffolds as tools to increase the vascularization capacity in bone regeneration applications.
Local growth factor-based vascularization strategies
A powerful strategy to promote vascularization in bone defect healing is the use of scaffolds as growth factor delivery system (Table 1). Growth factors, such as VEGF, bone morphogenetic proteins (BMPs), and basic fibroblast growth factor (bFGF) regulate the various stages of angiogenesis and osteogenesis in the process of bone regeneration.132–136
Local Growth Factor-Based Vascularization Strategies
α-CGRP, alpha-calcitonin gene-related peptide; bFGF, basic fibroblast growth factor; BMP-2, bone morphogenetic protein-2; BMP-7, bone morphogenetic protein-7; COMP-Ang1, cartilage oligomeric matrix protein-angiopoietin 1; DMOG, dimethyloxalylglycine; DNA, deoxyribonucleic acid; HGF, hepatocyte growth factor; IGF-1, insulin-like growth factor-1; microRNA, microribonucleic acid; NELL-1, Nel-like protein-1; OP-1, osteogenic protein-1; S1-P, sphingosine 1-phosphate; SAG, smoothened agonist; SDF-1, stromal cell-derived factor-1; siCkip-1, casein kinase 2 interaction protein-1; siFLT-1, soluble VEGF receptor-1; VEGF, vascular endothelial growth factor.
A considerable number of experiments studied the delivery of single growth factors, providing a distinct insight in their potential to promote angiogenesis in bone regeneration. VEGF, the most potent angiogenic factor, is well known to stimulate the formation of new blood vessels. Its local application in bone defects has already been shown to successfully increase vascularization and bone formation.133,137–141 BMP-2 on the other hand, despite its ability of inducing bone formation, 142 lacks the capacity to initiate angiogenesis. 143 However, another protein from the BMP family, BMP-7, induces early graft remodeling by stimulating blood vessel formation and osteoclastic activity, as well as the expression of angiogenic and inflammatory cytokines.134,144 Furthermore, proangiogenic growth factors and compounds, which may be used in bone tissue engineering applications, are insulin-like growth factor-1, 145 hepatocyte growth factor, 146 sphingosine 1-phosphate 147 and its receptor agonist FTY720,148,149 angiopoietin-2, 150 plasma factor XIII, 151 G-CSF, 84 the glycoprotein fibrinogen, 152 and PRP, which contains a variety of cytokines (i.e., platelet-derived growth factor, TGF-β, and epidermal growth factor).153–156 Of note, the local application of clinically approved drugs at the bone defect site, such as simvastatin,157,158 rosuvastatin, 159 desferrioxamine,160–163 and even antibiotics like minocycline, 164 has also beneficial effects on vascularization and bone formation.
The technique of the local delivery of those substances ranges from the direct injection into the fracture area, 140 the coating of scaffolds and bone allografts with growth factors,134,135 the application of hydrogel formulations, microspheres, and microparticles loaded with specific cytokines137–139,157,165 to the transfection with proangiogenic gene vectors.166–169 The gene-activated matrix concept, for instance, involves the preloading of matrices with gene vectors to guarantee a sustainable release of DNA to ingrowing cells at the fracture site. 170
Alpha-calcitonin gene-related peptide (α-CGRP), a 37-amino acid peptide transcribed from the same gene locus as calcitonin, has been shown to play a significant role in bone development and metabolism. 171 Moreover, α-CGRP is known to possess a strong vasodilatory activity and to stimulate the proliferation of endothelial cells. 172 Therefore, α-CGRP may be a promising candidate to regulate and promote bone regeneration and vascularization in preclinical and clinical applications. In fact, a variety of studies could demonstrate that α-CGRP induces the osteogenic differentiation of MSCs in vitro,173,174 most likely by affecting a Hippo-Yes-associated protein (YAP) pathway. 175 In addition, in vivo animal studies suggest that α-CGRP induces angiogenesis and osseointegration of titanium implants,171,176 as well as new blood vessel formation and bone regeneration at the defect site of a distraction osteogenesis model. 177 Interestingly, the pro-osteogenic effect of α-CGRP can be stimulated by magnesium-based implants, highlighting the significance of the interaction between specific materials and growth factor-mediated tissue regeneration. 178
Natural bone regeneration is a highly organized and complex process that requires the strict coordination of multiple growth factors influencing various cell types, which arrange the fracture callus and eventually resolve the callus, resulting in successful bone healing. Accordingly, just the release of individual proangiogenic growth factors from scaffold materials might be an oversimplified and, thus, insufficient approach to stimulate the regeneration of bone. In fact, several studies demonstrated that solely delivering angiogenic factors leads to an inability for controlled bone regeneration.143,179 Therefore, it has been proposed to incorporate both an osteogenic factor, most commonly BMP-2, and an angiogenic factor, such as VEGF, into the scaffold material. The simultaneous release of two growth factors may have the advantage of mimicking the natural bone healing process more accurately. Indeed, several studies report the successful application of dual growth factor delivery to induce angiogenesis and bone formation.180–185 Using a critical-size defect model, Ratanavarporn et al. 186 revealed that the dual release of stromal cell-derived fator-1 (SDF-1) and BMP-2 has superior effects on bone regeneration when compared to the application of BMP-2 alone. This is most probably due to a synergistic effect of SDF-1 to enhance angiogenesis as a result of the recruitment of hematopoietic stem cells and the BMP-2-induced differentiation of osteoprogenitor cells. Another study by Su et al. 187 explored the effects of the delivery of BMP-2 and fibroblast growth factor (FGF) in large-size mandibular defect regeneration in rabbits. Noteworthy, the authors observed a significant increase in bone formation after implantation of scaffolds loaded with BMP-2 and FGF when compared to scaffolds loaded with either BMP-2 or FGF alone.
As an alternative to growth factor delivery, some studies recently proposed the delivery of small molecules to induce bone regeneration.188,189 Small molecules induce specific cellular responses by triggering signaling cascades. It is assumed that small molecules may avoid the potential side effects of high-dose growth factor delivery, while easily maintaining bioactivity in a biological environment. Woo et al. 190 examined the combined application of angiogenic and osteogenic small molecules on bone regeneration with α-calcium sulfate. The in vivo results in a critical-size bone defect model in rats showed a synergistic effect on blood vessel formation and bone regeneration, 190 highlighting the potential of small molecules as alternative to common growth factors.
Despite these promising results, there are also studies reporting that the dual delivery of growth factors fails to improve long-term results. By analyzing the impact of VEGF and BMP-2 delivery in rabbit femoral and cranial defects, experimental studies showed initial benefits on bone formation; however, at later time points, there were no significant differences between animals receiving two growth factors when compared to animals receiving BMP-2 alone.179,191 These findings indicate that, although VEGF initially increases vascularization and tissue formation, a dual delivery in combination with BMP-2 does not always lead to a satisfying long-term outcome. Hence, efforts have to be made to fully understand the interaction of growth factors with the multiple cell types at the fracture site and to determine ideal release doses, time points, and kinetics of each individual factor.
To engineer delivery systems that allow the application of multiple growth factors, scaffold material properties and mechanisms of protein release are of utmost importance. Polymer encapsulation scaffolding allows distinct release profiles of growth factors by using polymers with different degradation behaviors. This method also includes growth factor-coated microspheres encapsulated within a second scaffold material. 132 As an alternative, core-shell and layer-by-layer scaffolding offer the possibility to control the local spatial separation of growth factor release. In these scaffold architectures, growth factors are spatially separated into different layers of physical material to govern their individual release.132,192 The next generation of bone scaffolds must address the incredible complex spatial and temporal growth factor presentation in the process of bone healing, while keeping in mind that the appropriate scaffold material should also provide the necessary mechanical properties and adjustable fabrication qualities.
Cell-based vascularization strategies
A further approach to improve vascularization in the prevention of nonunion formation represents the seeding of scaffolds with blood vessel-forming cells. 193 In a clinical setting these cells (1) should be easy to harvest with minimal risk for the donor, (2) should induce the generation of new blood vessels within the bone scaffold and its surroundings to allow an adequate vascular supply, (3) should have a low potential of an immunogenic response, and (4) should not induce malignancies. During the last decade, a variety of different cell-based vascularization strategies have been studied in the field of bone tissue engineering, ranging from EPCs to complex tissue constructs with an architecture similar to that of the periosteum (Table 2).
Cell-Based Vascularization Strategies
ADSCs, adipose-derived stem cells; BFP-1, bone forming peptide-1; BMP-4, bone morphogenetic protein-4; Cbfa1, core-binding factor a1; CD, cluster of differentiation; E-EPCs, early endothelial progenitor cells; EPCs, endothelial progenitor cells; L-EPCs, late endothelial progenitor cells; MSCs, mesenchymal stem cells; PBMNCs, peripheral blood mononuclear cells; PRF, platelet-rich fibrin; PRP, platelet-rich plasma; PVCs, perivascular cells; QQ, quality and quantity; SVF, stromal vascular fraction.
Endothelial progenitor cells
EPCs are bone marrow-derived cells that can be isolated from peripheral adult human blood and the umbilical cord. 194 They have a highly clonogenic potential and can, therefore, be rapidly expanded for use in patients. EPCs represent a somewhat heterogeneous cell type that is classified in early- and late-outgrowth EPCs, which differ in their culture times, proliferative potential, and gene expression. 195 Rozen et al. 196 implanted early-outgrowth EPCs locally within the fibrous scar tissue of a critical-size defect in sheep tibia and observed a significantly improved bone healing and defect bridging in most of the animals treated with EPCs, whereas the nontreated controls only showed minimal bone formation. In two similar studies, Atesok et al. 197 and Li et al. 198 transplanted a gel foam loaded with early-outgrowth EPCs within segmental bone defects in rats. The authors found an increased callus formation, a higher torsional strength, and stiffness in the EPC group when compared to controls. The local delivery of EPCs can be achieved by a variety of scaffold materials, including collagen sponges, ceramic scaffolds, and bioglasses.199–201 In further experiments, Li et al.202,203 demonstrated an elevated VEGF and BMP-2 expression in early-outgrowth EPC-treated bone defects. This indicates a paracrine mechanism of action in EPC therapy. Interestingly, these results are contradictory to the findings of Smadja et al., 204 who observed BMP-2 and BMP-4 expression selectively in late-outgrowth EPCs. Analysis of the therapeutic efficacy of early- and late-outgrowth EPCs showed an increased bone union and callus formation in animals treated with early-outgrowth EPCs when compared to animals treated with late-outgrowth EPCs and untreated controls. 205 These findings indicate a superiority of early-outgrowth EPCs over late-outgrowth EPCs for the treatment of nonunions.
Apart from the type of cells, the timing of the intervention is thought to play a crucial role in the efficacy of cellular therapy of nonunions. 206 In clinical practice, treatment of delayed unions or nonunions is indicated at late time points when final diagnosis is made. In contrast, most experimental studies apply EPCs, engineered tissues, or other types of treatment directly after creation of the bone defects. To more appropriately mimic the clinical situation in the design of the experimental study, Bates et al. 207 evaluated the potential of a delayed EPC delivery in a segmental bone defect model. They found that EPCs enhance radiographic and morphometric bone repair when applied 3 weeks after the creation of a bone defect. Noteworthy, the healing response did not differ from the acute treatment with EPCs, indicating the potential of delayed onset of EPC treatment in bone defect healing.
To further expand the proangiogenic potential of EPCs, the combination with vessel-forming growth factors seems to be a promising approach. In the attempt to construct vascularized bone grafts, Wang et al. 208 added EPCs to a β-TCP scaffold loaded with bone forming peptide-1 (BFP-1). Micro-CT analysis revealed a synergistic and vigorous effect of EPC- and BFP-1-loaded scaffolds not only on blood vessel formation but also on bone healing in segmental bone defects in rabbits. These findings indicate the potential of a combined cell- and growth factor-based therapy to promote vascularization in tissue-engineered bone.
Peripheral blood cells
Adult CD34+ human peripheral blood cells have been reported to contain a large number of EPCs and hematopoietic stem cells. 194 Accordingly, this cell population is capable of promoting vasculogenesis and participating in neovascularization.209,210 Moreover, Matsumoto et al. 211 demonstrated that intravenously injected CD34+ cells result in morphological and physiological healing of nonunions in rats. The enhanced bone healing was associated with an increased neovascularization and an improved blood perfusion within the fracture area. This makes CD34+ cells a potent cell population for therapeutic vasculo-osteogenesis in the healing of nonunions. In contrast to CD34+ cells, peripheral blood mononuclear cells (PBMCs) represent a more mixed cell population, also containing lymphocytes and monocytes. 212 Therefore, their isolation does not require magnetic cell sorting, and can be performed in a shorter time and at a lower cost. Fukui et al. 213 treated nonhealing fractures in rats with the local transplantation of PBMCs and found an increase of angiogenesis and osteogenesis. However, in direct comparison to peripheral blood CD34+cells, PBMCs were less effective in promoting the healing of nonunions. To overcome this problem, Mifuji et al. 214 applied a so-called ‘quality and quantity culture’ (QQ-culture) to PBMCs, which increases the angiogenic cell fraction by adding cytokines and growth factors, like VEGF, interleukin-6. and thrombopoietin. As a result, the authors found an enhanced endochondral ossification and bridging rate in animals treated with QQ-cultured PBMCs, indicating an augmentation of the therapeutic potential of PBMCs.
Mesenchymal stem cells
MSCs are a multipotent cell type, which derives from numerous tissues in the body. They represent the precursors of bone-forming osteoblasts and are, therefore, a powerful tool to induce bone formation in critical healing conditions. 12 Besides, they can participate in the vascularization of tissues by various pathways. 215 Like any other cell line, MSCs suffer from hypoxia within scaffolds during the initial phase after implantation. This in turn leads to the expression of proangiogenic cytokines, such as VEGF and the hypoxia-inducible transcription factors, resulting in the stimulation of angiogenesis in the surrounding tissue. 216 In addition, multipotent MSCs are capable of differentiating into endothelial cells, which are directly integrated in the newly formed blood vessels.217,218 In fact, Zou et al. 219 analyzed the efficiency of various stem cell-derived osteoprogenitor cell populations in healing nonunions in vivo and found that the cells' capabilities to stimulate fracture healing are directly dependent on their proangiogenic activity. These findings highlight the predominant role of the cell populations' proangiogenic potential when applied in cell-based bone tissue engineering.
MSCs are commonly isolated from adipose tissue216,220–222 and bone marrow,223–227 but also from various other tissues, including fetal tissue, 228 placental tissue, amniotic fluid,229,230 the umbilical cord, cord blood, and the periosteum.231,232 Adipose-derived stem cells (ADSCs), which are of special clinical interest, are easily accessible with a low donor site morbidity and allow the isolation of a vast amount of stem cells. 233 However, ADSCs require a time-consuming in vitro culture and purification before they can be applied in vivo. Therefore, several studies investigated the potential of the freshly isolated stromal vascular fraction (SVF) from adipose tissue. The SVF consists of a heterogeneous cell population, including circulating blood cells, adipocytes, fibroblasts, macrophages, pericytes, and endothelial cells. Unfortunately, the SVF shows only minor bone formation and an inferior healing capacity when compared to cultured ADSCs,234,235 indicating that without any in vitro procedures, additional pro-osteogenic stimulation is needed to significantly stimulate bone formation.
To gain an alternative source for cell-based tissue engineering, James et al. 236 successfully purified the SVF and isolated perivascular stem cells (PSCs). This cell population can be found in every vascularized organ and is capable of inducing osteogenic differentiation and bone formation. Moreover, PSCs have been shown superior in bone healing of critical-size defects in mice when compared to animals treated with nonpurified SVF. 237 Furthermore, Kargozar et al. 238 seeded strontium- and cobalt-substituted bioglass with perivascular cells derived from the umbilical cord and found an enhanced expression of proangiogenic genes, resulting in an improved bone healing. These results underline the vast potential of combining advanced biomaterials with cell-based tissue engineering to generate vascularized bone substitutes.
Another source for cell-based tissue engineering represents pericytes. These cells surround the endothelial cells of capillaries and other microvessels and contribute to the stabilization and maturation of these blood vessels.239,240 In addition, it has recently been shown that pericytes possess multilineage differentiation capacities similar to MSCs. 241 By injecting pericytes percutaneously into the fracture gap of an atrophic nonunion model in the rat tibia, Tawonsawatruk et al. 242 demonstrated that pericytes are capable of rescuing fractures from nonunion formation. These findings were supported by a study from Supakul et al., 243 which verified the ability of pericytes to differentiate into osteoblasts and osteoclasts, thereby contributing to the process of fracture healing (Fig. 2). In contrast to MSCs, pericytes can be abundantly isolated from adipose tissue without the need for culture expansion, making them an attractive alternative in cell-based bone tissue engineering.
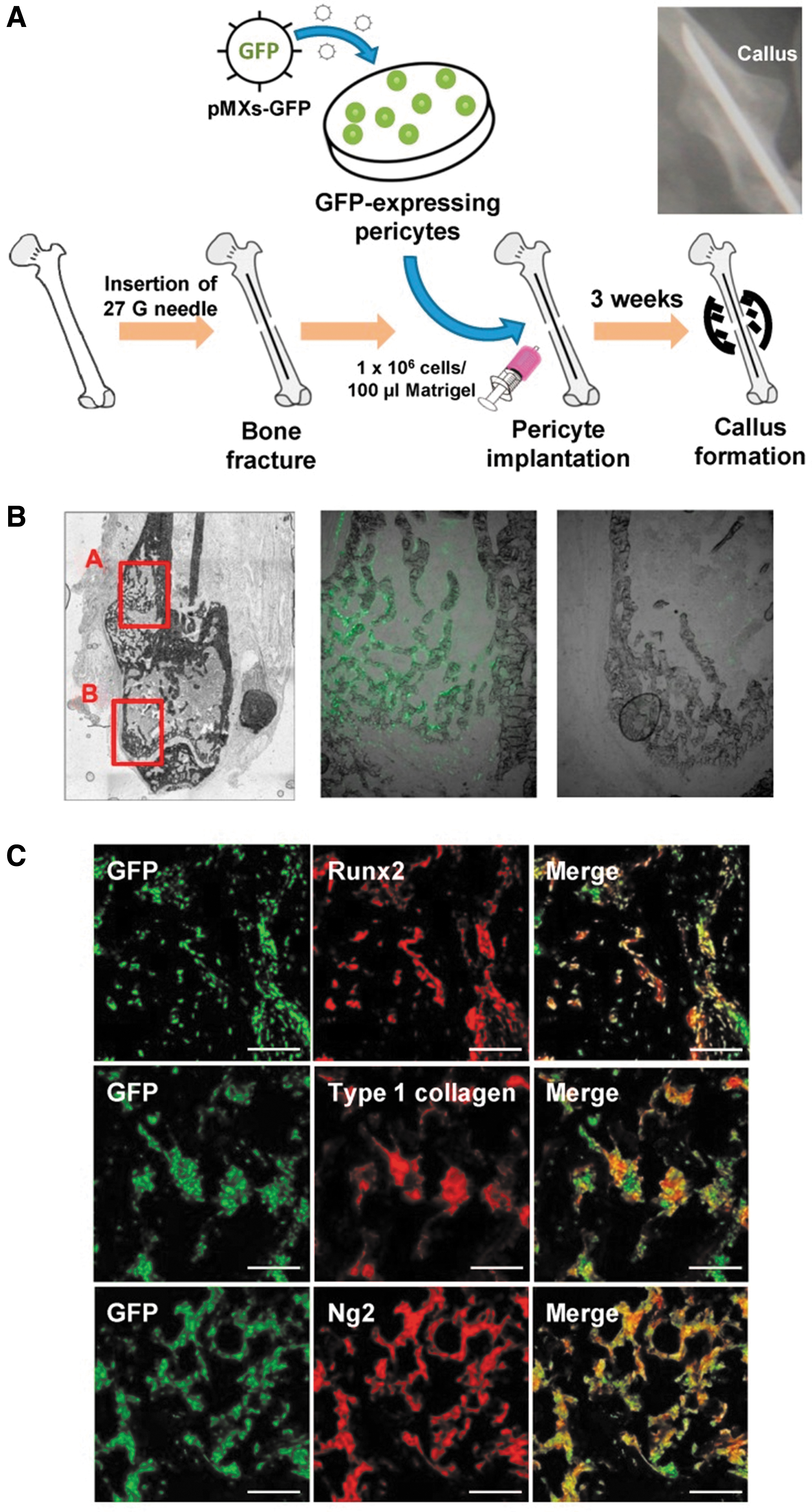
Contribution of implanted pericytes to callus formation during bone healing according to Supakul et al.
206
The proangiogenic properties of MSCs may be further optimized by the combination of MSCs with growth factor delivery systems. Several studies describe promising results of this synergistic approach. Growth factors can be delivered by local application, 244 by the incorporation within scaffold materials245–251 or by genetically modified MSCs, which all provide a sustained release and concentration of growth factors within the bone defect.252–260 Kumar et al. 253 used an ex vivo approach to create genetically engineered MSCs expressing both VEGF and BMP-2 and transplanted them in a segmental bone defect in mice tibia. Animals treated with genetically modified MSCs showed an increased vascularity, osteoblastogenesis, and bone formation. However, despite these promising results, it should be kept in mind that gene therapy is associated with the risk of heterotopic bone formation and even of malignancies.
Combined cell-based therapy
Combined cell populations for vascularized bone tissue engineering allow the accumulation of proangiogenic and pro-osteogenic cell lines to facilitate bone formation in critical bone healing. Common combinations of cell types include endothelial cells and osteoblastic cells,261–263 CD34+ peripheral blood cells and bone marrow-derived MSCs, 264 pericytes, and adventitial cells, 265 as well as EPCs and undifferentiated MSCs.266–270 Moreover, Amini et al. 269 established a double-tracked approach for bone regeneration in large defect areas in vivo, involving oxygen-controlled matrices and an optimal cell combination of MSCs and EPCs, which increases oxygen tension levels and cell viability. Scaffolds were co-cultured with MSCs and EPCs for 2 days and subsequently implanted in nude mouse subcutaneous tissue and a rabbit ulnar defect model. Interestingly, the authors found a ratio of 1:1 MSCs:EPCs as the most effective progenitor cell ratio to induce vascularized bone regeneration. These results indicate that not only the type of cells but also their ratio determines the success of inducing vascularization in segmental bone defects.
Periosteal substitutes
The periosteum is a highly vascularized tissue, being an essential factor in successful long bone repair by providing the cortical blood supply. 271 Moreover, it serves as a reservoir for osteoprogenitor cells, comparable to bone marrow-derived MSCs. 272 Therefore, a viable periosteum is a prerequisite to prevent nonunion formation. Masquelet et al. 273 used a bioactive induced membrane (IM) as a novel concept for guided bone regeneration. The implantation of a cement spacer inside the critical-size defect induced a biological membrane surrounding the spacer. Subsequently, the spacer was removed with the remaining IM serving as a conduit for cells and bone grafts (Fig. 3). This biomembrane expressed genes critical for bone development and formation, including BMP-2, BMP-6, VEGF, and RUNX-2, an important regulator of osteoblast differentiation. Additional analyses of the cellular and molecular composition of the IM revealed a similar cellular and vascular architecture, as well as growth factor expression when compared to native periosteum. This includes the number of colony-forming unit-fibroblasts, the osteogenic potential of the expanded MSCs, and the histological composition of both tissues. 274 As a result, the regenerative capacity of these tissues is most likely comparable and the IM may also be described as an “induced periosteum.” 275 Of interest, Henrich et al. 276 demonstrated the highest osteogenic and angiogenic activity of IMs at an early time point (2–4 weeks) after spacer implantation. To maximize bone regeneration, they proposed an early replacement of the spacer by an appropriate bone graft. 244 The disadvantage of this approach is the necessity of two surgical interventions, increasing the risk of complications and elevating the costs. In contrast, the implantation of a bioresorbable scaffold that induces membrane formation without the need of removal later on may minimize patient morbidity and economic burden.
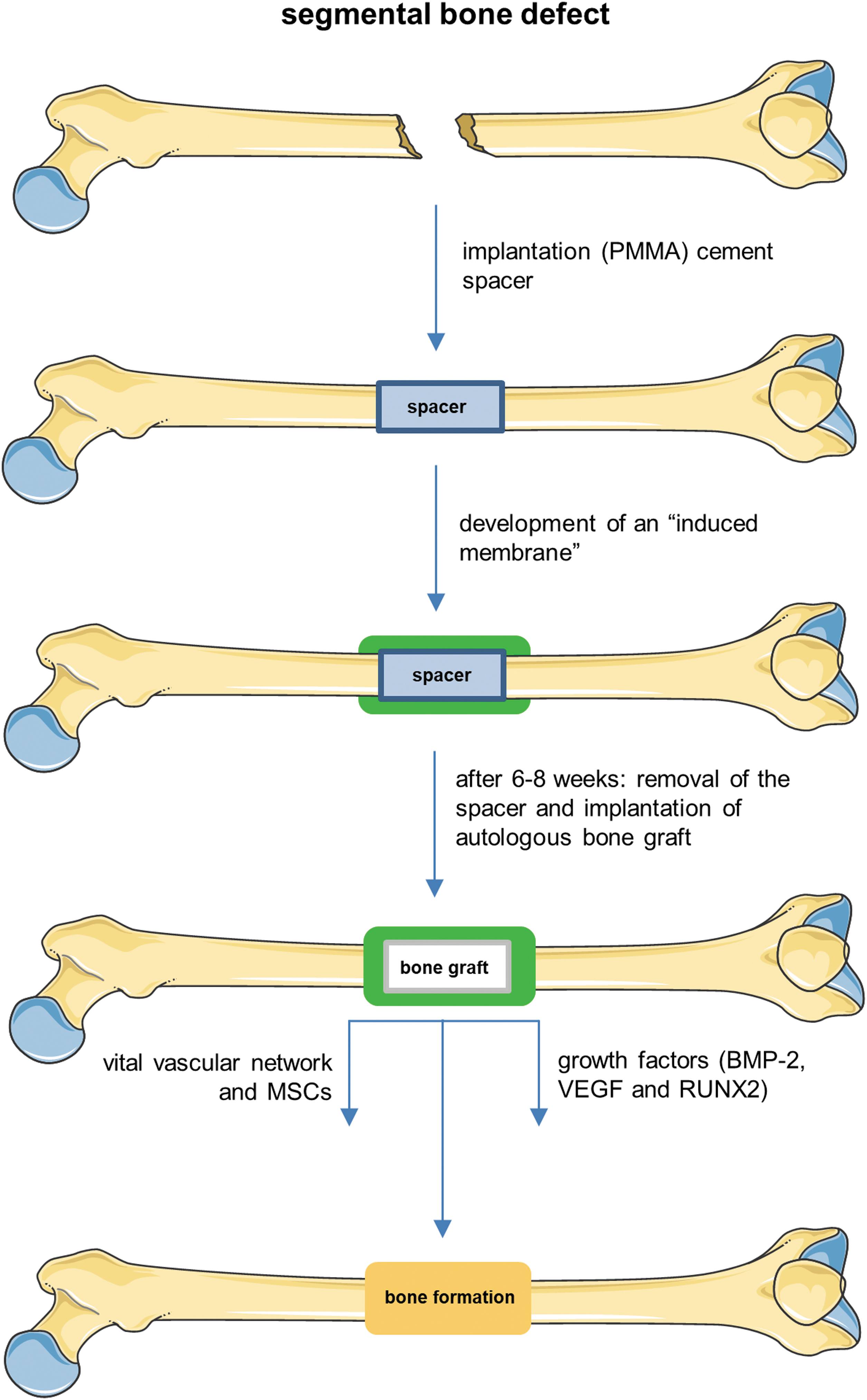
The IM technique for the healing of large bone defects as described by Masquelet et al. 241 In a first step, the fracture site is debrided and a PMMA cement spacer is implanted. This leads to the development of an IM, which surrounds the spacer. After 6–8 weeks, the spacer is removed and replaced by an autologous bone graft. The membrane provides a vital vascular network, MSCs, as well as growth factors like BMP-2, VEGF, and RUNX2 to facilitate bone healing and union formation. BMP-2, bone morphogenetic protein-2; IM, induced membrane; PMMA, polymethyl methacrylate.
An even more sophisticated approach to facilitate bone repair represents the construction of artificial cell-based periosteal substitutes. Suggested materials for tissue-engineered periosteum are synthetic polymers,277,278 ceramics, 279 and polysaccharides. 280 Recent advancements in nanotechnology allow the fabrication of electrospun nanofiber sheets to mimic the highly organized architecture of the periosteum 281 (Fig. 4). To further improve the angiogenic potential of the periosteal substitutes, several studies also propose the addition of growth factors278,280 and MSCs.277,281,282 Moreover, the design of cell sheets consisting of MSCs and endothelial cells, which mimic the physiological architecture of the native periosteum, shows great potential in promoting vascularization in experimental studies.283,284 Kang et al. 284 developed a biomimetic periosteum, which contains a mineralized MSC-seeded cell sheet, resembling the cambium layer of native periosteum and a second vascularized cell sheet seeded with human umbilical endothelial cells and MSCs, mimicking the outer fibrous layer of the periosteum. This cell-engineered periosteum successfully promoted angiogenesis and ectopic osteogenesis of β-TCP scaffolds at a subcutaneous transplantation site in mice. These promising results have now to be transferred into the clinical setting.
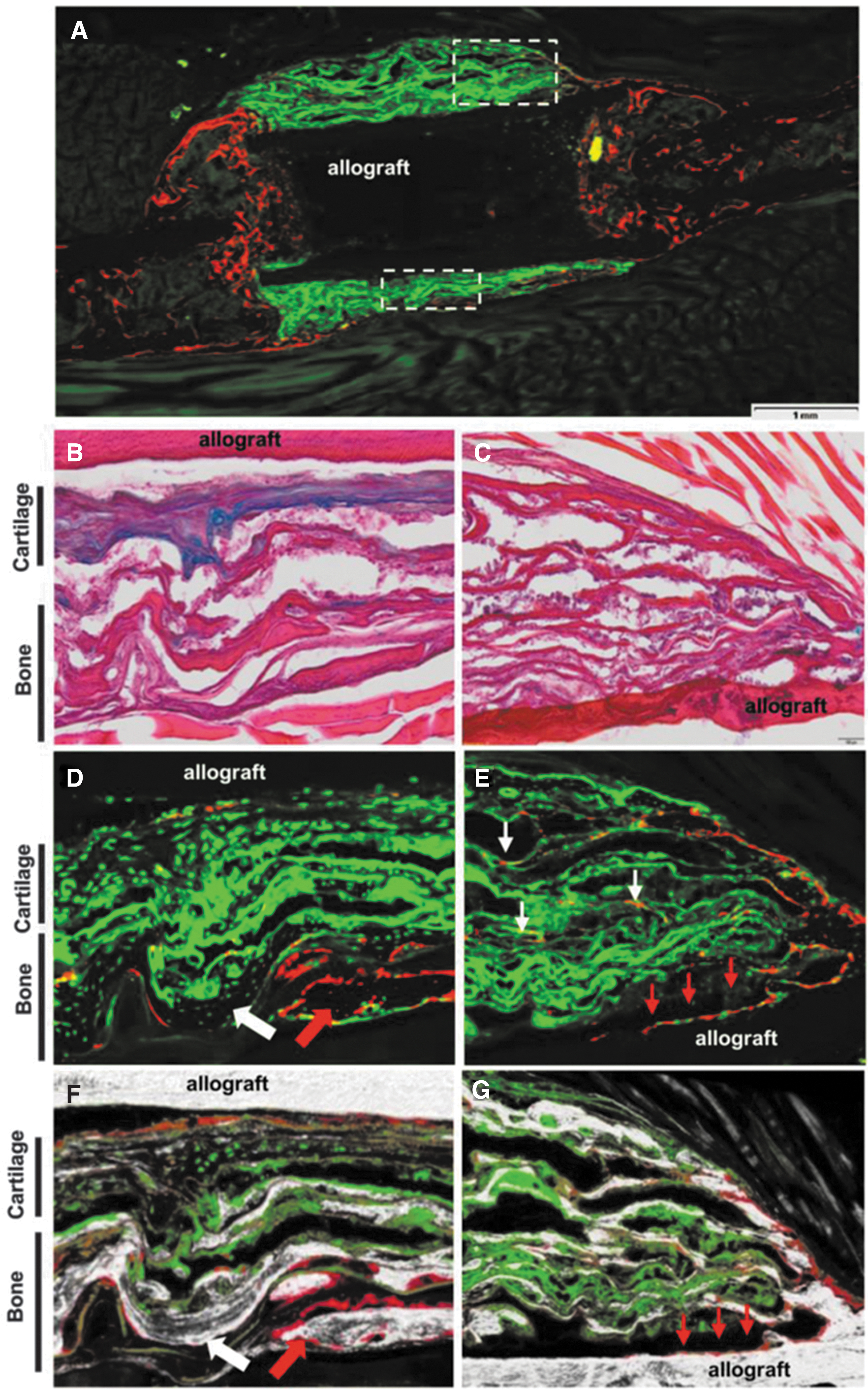
Donor/host contribution to engineered periosteal callus in femoral allograft healing published by Wang et al.
249
GFP-positive BMSC-seeded tissue-engineered periosteum was implanted into an immunodeficient NOD-OSXRFPcherry mouse. Representative fluorescent images of the grafted femur at 7 weeks postimplantation
Surgical approaches for vascularized bone tissue engineering
The principle of surgically delivered vascularization in bone tissue engineering is a promising approach to improve bone regeneration and to overcome nonunion formation. The common surgical technique for this purpose is the transplantation of vascularized bone grafts from unharmed areas of the body, including fibula, iliac crest, and radius, into the defect site. However, this procedure is associated with a considerable donor site morbidity such as pain, sensory abnormalities, and loss of function. 285 Experimental approaches such as the implantation of scaffolds in combination with vascular bundles286,287 or vascularized periosteal flaps288–290 avoid these complications. In these scaffolds, the sprouting of a capillary networks can help to increase the initial survival and engraftment of transplanted MSCs, resulting in an improved blood vessel and bone formation.
The arteriovenous (AV)-loop model represents an even more sophisticated strategy. A superficial artery and vein are anastomosed to create the AV-loop. This AV-loop generates axially vascularized tissue by using the own body as a bioreactor. This allows the prevascularization of materials, scaffolds, and cell constructs. Subsequently, the prevascularized tissue can be transplanted with its vascular axis into the defect site, that is, large bone defects. 291 Mian et al. 292 were among the first to describe the AV-loop technique and designed an isolated chamber with highly vascularized fibrous tissue in rats suitable for microsurgical transplantation. During the last two decades, the AV-loop model was further developed, including the prevascularization of solid porous matrices 293 as well as the combined application with growth factor- and cell-based strategies.285,294
In 2018, Arkudas et al. 295 successfully applied the AV-loop technique in a critical-size femoral defect model in rats by transplanting axially vascularized bone constructs into the defect site. The authors observed an increased vascularization and bone formation, leading to bone union in the long term. To pave the way toward clinical application, the function of AV-loop technique was tested in large animal models. These experiments demonstrated an axial prevascularization of bone substitutes and the successful formation of transplantable bone tissue.296,297 In fact, experiments in large animals were the necessary step for the translation of those techniques into clinical practice. 298
In 2004, Warnke et al. 299 were among the first performing a successful human application of surgically delivered bone tissue engineering. To repair an extended mandibular discontinuity defect in an adult male patient, they grew a custom-made bone transplant inside the latissimus dorsi muscle. Seven weeks later, this bone transplant was transferred as a free bone-muscle flap into the mandibular defect site. Computer tomography and skeletal scintigraphy showed bone remodeling and mineralization inside the mandibular transplant both before and after transplantation. 299 In a more recent study, Horch et al. 300 demonstrated successfully axially vascularized in situ tissue-engineered bone regeneration within large bone defects in a clinical setting by using the AV-loop model. For osseus reconstruction, AV-loops were created as vascular axis and placed in the bony defects. Long-term follow-up showed patent AV-loops, completely healed bone defects with osseus regeneration as well as a satisfying clinical outcome without the creation of a significant donor site morbidity. Taken together, surgical approaches for vascularized bone tissue engineering, especially the AV-loop technique, have an enormous potential to successfully treat bone defects and established nonunions. In future, these techniques may set new standards in reconstructive surgery and open the door for custom-made prevascularized bone constructs in clinical practice.
Current clinical tissue engineering approaches
In clinical practice, the reconstructive treatment of established nonunions most frequently include the use of autologous bone grafts, bone allografts, and/or synthetic biomaterials. Autologous bone grafts, mostly harvested from the iliac crest of the patient, are still the gold standard for the treatment of nonunions. They provide ideal osteogenic, osteoinductive, and osteoconductive properties without the risk of viral transmission. Still, major drawbacks of this approach are the necessity of two surgical sites and the limited amount of graft material. 301 Bone allografts, harvested from living donors during joint replacement or from cadavers, may overcome these problems. They are immediately available in different sizes and shapes 302 and are especially suited for large bone defect reconstructions after nonunion resections. 301 On the other hand, allografts present a lower osteogenic potential compared to autografts 303 and bear the risk of immune rejection and disease transmission. 301 The use of synthetic bone tissue substitutes represents another strategy in the clinical treatment of nonunion formation and bone reconstruction. Among the most common materials are biphasic calcium phosphate (BCP), TCP, calcium HA, and bioactive glass. These synthetic bone substitutes represent an excellent alternative to biological grafts in small bone defects. 301 However, due to their insufficient biomechanical strength and neovascular ingrowth, they are limited in the daily clinical use. 304
Cell-based tissue engineering therapies may further improve the outcome of autograft, allograft, or synthetic biomaterial treatments. In recent years, substantial efforts have been made to understand the fundamental biological, material, and physical requirements of cell-based tissue-engineered bone substitutes. However, only a few approaches have successfully progressed from preclinical research to clinical trials. 305 In a pilot study, including eight patients, Gianotti et al. 306 implanted osteogenetically differentiated MSCs with a fibrin clot in nonunions of upper limb extremities after re-osteosynthesis. After an average follow-up of 6 years and 3 months, all patients showed radiological healing and recovered limb function with no evidence of tissue overgrowth or tumor formation. Although these results are encouraging, the study suffers from a limited number of cases and the lack of an appropriate control group. ORTHO-1, a European, multicentric clinical trial, 307 has only recently proven in patients with long bone nonunions the safety and feasibility of the surgical implantation of commercially available BCP bioceramic granules in combination with mesenchymal stromal cells expanded from bone marrow. Moreover, the study demonstrated radiologically healing in 26 out of 28 treated patients. Future studies have now to determine the efficacy and the potential of this cell-based tissue engineering approach in comparison to the gold standard procedures with bone autografts and allografts.
Conclusion
During the last decade, there has been major progress in the development of novel vascularization strategies to prevent and treat nonunion formation. These include biophysical applications, systemic pharmacological interventions, and scaffold-, growth factor-, cell-, and periosteum-based techniques, as well as surgical tissue engineering approaches. To further improve the efficiency of these vascularization strategies, additional research should focus more detailed on their particular spatial and temporal requirements. Indeed, it has to be considered that in nonunions, the process of bone healing may only be supported ideally, if the vascularization is stimulated in the right dose to the right place at the right time. The major challenge for the future will then be the translation of these strategies into clinical practice to make them accessible for the majority of patients.
Footnotes
Acknowledgments
The authors thank Servier Medical Art for providing access to designed medical elements, supporting the generation of graphical items in this publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.