
Abstract
Reconstruction of peripheral nerve injuries (PNIs) with substance loss remains challenging because of limited treatment solutions and unsatisfactory patient outcomes. Currently, nerve autografting is the first-line management choice for bridging critical-sized nerve defects. The procedure, however, is often complicated by donor site morbidity and paucity of nerve tissue, raising a quest for better alternatives. The application of other treatment surrogates, such as nerve guides, remains questionable, and it is inefficient in irreducible nerve gaps. More importantly, these strategies lack customization for personalized patient therapy, which is a significant drawback of these nerve repair options. This negatively impacts the fascicle-to-fascicle regeneration process, critical to restoring the physiological axonal pathway of the disrupted nerve. Recently, the use of additive manufacturing (AM) technologies has offered major advancements to the bioengineering solutions for PNI therapy. These techniques aim at reinstating the native nerve fascicle pathway using biomimetic approaches, thereby augmenting end-organ innervation. AM-based approaches, such as three-dimensional (3D) bioprinting, are capable of biofabricating 3D-engineered nerve graft scaffolds in a patient-specific manner with high precision. Moreover, realistic in vitro models of peripheral nerve tissues that represent the physiologically and functionally relevant environment of human organs could also be developed. However, the technology is still nascent and faces major translational hurdles. In this review, we spotlighted the clinical burden of PNIs and most up-to-date treatment to address nerve gaps. Next, a summarized illustration of the nerve ultrastructure that guides research solutions is discussed. This is followed by a contrast of the existing bioengineering strategies used to repair peripheral nerve discontinuities. In addition, we elaborated on the most recent advances in 3D printing and biofabrication applications in peripheral nerve modeling and engineering. Finally, the major challenges that limit the evolution of the field along with their possible solutions are also critically analyzed.
Impact statement
Complex nerve injuries, including critical-sized gaps (>3 cm loss of substance), gaps involving nerve bifurcations, and those associated with ischemic environments, are difficult to manage. A biomimetic, personalized peripheral nerve tissue surrogate to address these injuries is lacking. The peripheral nerve repair market currently represents a multi-billion-dollar industry that is projected to expand. Given the clinical and economical dilemmas posed by this medical condition, it is crucial to devise novel and effective nerve substitutes. In this review article, we discuss progress in three-dimensional printing technologies, including biofabrication and nerve computer-aided design modeling, toward achieving a patient-specific and biomimetic nerve repair solution.
Introduction
The surgical management of peripheral nerve injuries (PNIs) remains a major clinical challenge with suboptimal clinical outcomes.1,2 PNIs cause devastating functional disabilities in patients, leading to impaired quality of life. Annually, more than 1 million people suffer from PNIs worldwide, with ∼200,000 patients in the United States and 300,000 in Europe requiring surgical repair.3,4 Moreover, an increasing incidence of PNIs is reflected by the forecasted growth in the peripheral nerve repair market, which is expected to exceed $10 billion by 2022. 5 Traumatic nerve injuries secondary to road traffic accidents, fractures, lacerations, and traction injuries represent the most common entity of PNIs encountered in reconstructive practice. According to the largest published clinical series, the prevalence of PNIs in polytrauma victims is approximately 1–3%.6–8 Other important and under-reported causes of PNI and nerve discontinuity include iatrogenic nerve injuries, most often complicating operative orthopedic interventions,9,10 and oncologic resection of nerve sheath tumors such as schwannomas and neurofibromas, which could potentially be complicated by a nerve gap that requires reconstruction.11,12
Peripheral nerve repair and current therapeutic options
Depending on the severity of the nerve injury, guided by the Seddon-Sunderland classification system, the functional recovery and treatment strategy can be initially established (Table 1).13–15 In grade IV and V, surgical intervention is inevitable and the choice of technique is, essentially, contingent on the presence of scarring, nerve substance loss, and size of any nerve gap. 16 Currently, primary repair in the form of tensionless end-to-end neurorrhaphy is the gold standard for nerve reconstruction, where gap size is <2 cm.17,18 It is critical that any nerve repair should not be performed under tension, which could otherwise compromise microvascular blood flow and impair nerve regeneration. 19 Unfortunately, in several instances, initial injury can cause significant substance loss resulting in long gaps (>2 cm), or, due to the loss of biotensegrity, transected nerves may undergo retraction that makes tension-free repair surgically infeasible. 20
Seddon-Sunderland Classification of Peripheral Nerve Injuries
Reproduced from Taniguchi et al. 252 Color images are available online.
The nerve autograft
In the presence of irreducible nerve defects, an interposition human autograft, usually the sural nerve, represents the optimal approach to restore nerve continuity. 21 Autografts have the advantages of providing the inherent nerve extracellular matrix (ECM) and cellular components, including Schwann cells (SCs), thus offering the most physiologic solution to nerve replacement. However, this procedure often results in donor-site morbidity secondary to neuroma formation that presents as tingling, numbness, and pain in the dermatome supplied by the sacrificed nerve. 22 In addition, low success rates can occur due to unpreventable size and fascicular mismatch and scarring in the graft bed. Other limitations of this procedure also include the sparse amount of donor tissue available and creation of additional surgical sites for nerve harvesting. 23
Further, it is critical to emphasize the importance of vascularization in maintaining the longevity of the transplanted autograft and increasing the rate of axonal regrowth. 24 Theoretically, the presence of adequate perfusion to the graft tissue provides an optimal nutritional milieu permissive for nerve regeneration via the following mechanisms: (1) supporting the viability of SC population, (2) reducing fibroblastic invasion and endoneurial scarring, (3) stimulating axon remyelination, and (4) accelerating the process of Wallerian degeneration and elimination of myelin debris.25–27
Traditionally, the classic nerve autograft has no vascular supply, and on implantation, the graft initially survives by plasmatic imbibition during the first week. 28 Later, nerve graft revascularization from the recipient bed capillaries and neighboring reconstructed nerve stumps occurs in the subsequent weeks postoperatively.29,30 This physiological initial delay in the angiogenesis induction of graft tissue makes it liable to local ischemia that could impair nerve regeneration, particularly across wide gaps. To achieve prompt and continuous revascularization of the transplanted neural tissue, a vascularized nerve graft (VNG) represents a clinically promising alternative. 31
First described by Taylor and Ham in 1976, the free VNG has a dominant arterial pedicle that can be anastomosed to vessels of the recipient bed using microsurgical techniques.25,32 Experimental and clinical evidence has demonstrated the superiority of VNGs over conventional nerve autografts in supporting nerve regeneration and achieving better outcomes in scarred, ischemic beds and long gaps (>6 cm).24,33,34 Moreover, VNGs are commonly indicated in proximal nerve lesions, for example, brachial plexus injuries to mitigate denervation atrophy of hand muscles.31,35,36
Nerve conduits or tubulization
Alternatively, nerve conduits can also be used in the repair of PNIs to obviate the complications of autografting. Nowadays, the Food and Drug Administration (FDA) has approved several polymeric nerve conduits, wraps, and decellularized allograft tissues to bridge nerve discontinuities (Table 2). However, they are mainly indicated for small gaps (<3 cm) and fail to outperform the clinical standard. 22 Nerve guidance conduits (NGCs), also referred to as tubulization, are synthetic or biological hollow tubes that aim at apposing the proximal and distal transected nerve stumps in an enclosed chamber. Through the creation of this secluded milieu, NGCs are hypothetically anticipated to support nerve regeneration by, first, reducing the loss of neurotropic cues and neurotrophic growth factors (NTFs) to the surroundings, thereby establishing a conductive microenvironment for axonal regrowth and guidance. Second, conduits act as a barrier against myofibroblast invasion and fibrosis formation, which can undermine axonal regeneration. 37 Third, they are expected to promote proper migration of sprouting axons to the distal nerve stump and prevent collateral sprouting/axonal misdirection that can lead to neuroma formation. 38
Food and Drug Administration-Approved Nerve Substitutes
dECM, decellularized extracellular matrix; ECM, extracellular matrix; PGA, poly (glycolic) acid; PLCL, poly (
Reproduced from Taniguchi et al. 252
Despite the wide variety of synthetic conduits available commercially, clinical studies that have compared the outcomes of conduits with nerve autografts are a few, unreliable (no double-blinded randomized controlled trials) and show unpredictable performance in gaps above 4 mm.39–41 Further, NGCs fail remarkably to promote nerve functional recovery over gaps exceeding 3 cm due to the lack of SCs, ECM skeletal framework, and adhesion molecules that provide trophic and mechanical support to migrating axons over this critical distance (Fig. 1). These factors have limited the use of conduits to the repair of short gaps (<3 cm) occurring in small diameter non-critical sensory nerves. 22 In addition, biological conduits such as vessels, most commonly veins, and muscle grafts have also been used for peripheral nerve repair.42,43 The therapeutic basis of venous conduits in nerve regeneration is believed to be mediated by the venous endothelial lining, which secretes nerve growth factor (NGF) and contains laminin-rich basal lamina that facilitates SC migration and proliferation.44,45 Likewise, skeletal muscle grafts provide longitudinally arranged basal lamina that can help directing the growth cone of regenerating axons. 42
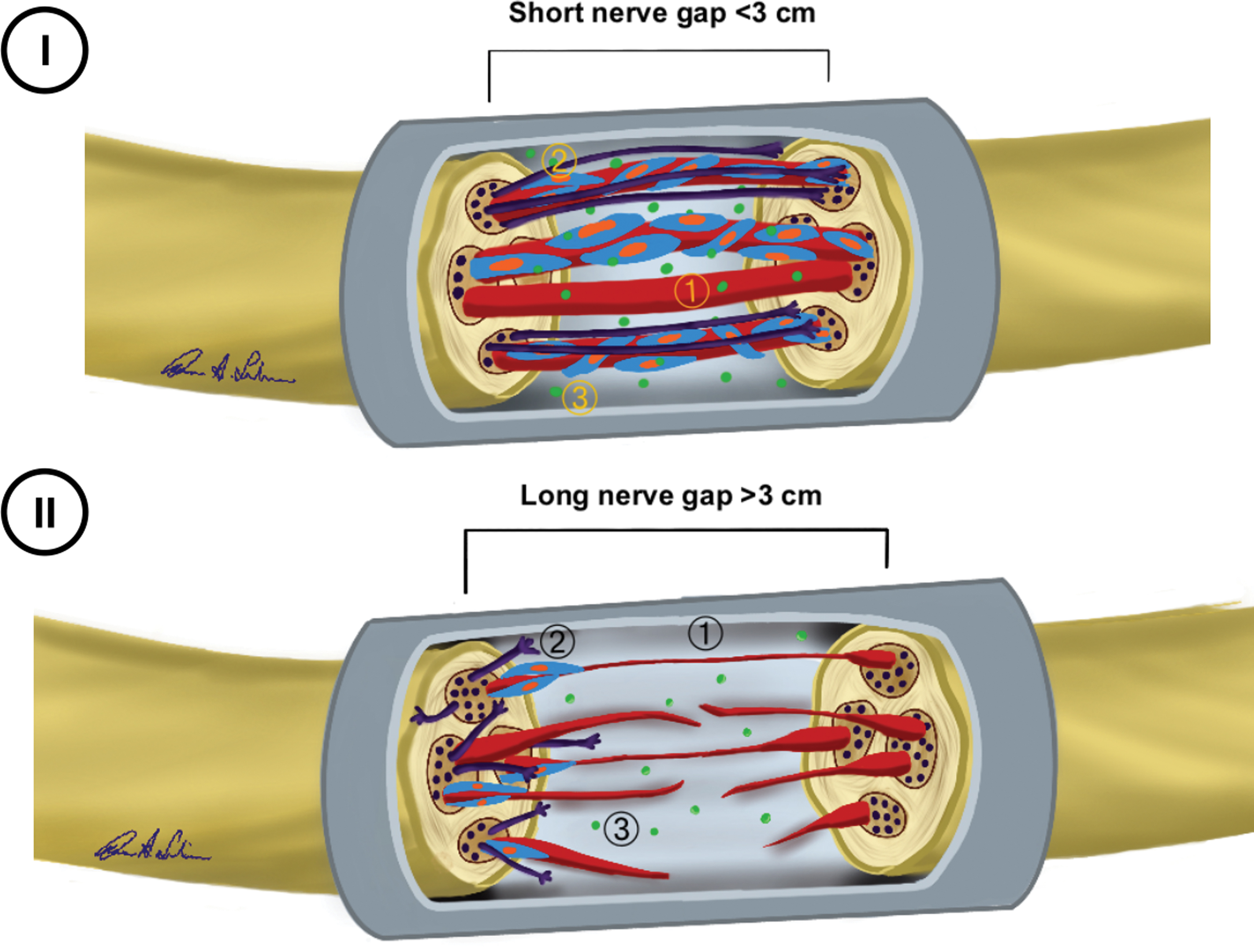
Conduit failure mechanisms in regeneration of long nerve gap.
The nerve allograft
Another nerve surrogate becoming widely adopted in nerve repair is the acellular allograft, commercially available off-the-shelf under the trade name Avance® (Axogen, Inc.). 46 Nerve allotransplantation has been used in cases where autograft tissue might be inadequate to bridge nerve discontinuities. 47 However, unprocessed nerve allotransplants expose the patient to risks of systemic immunosuppression-related complications. Therefore, decellularized allogeneic nerve tissue was developed to preclude the need for post-transplant immunosuppressive therapy. Decellularization attenuates the allograft antigenicity by eliminating intrinsic cellular elements (SCs, endothelial cells, and fibroblasts), which mediate the rejection mechanism via harboring the major histocompatibility complex. Concomitantly, the inherent nerve architecture together with ECM proteins and basal lamina tubes can be preserved to provide mechanical guidance for the regenerating nerve fibers and scaffolding for native SCs for migration. Decellularized cadaveric peripheral nerve tissues using chemical processing (detergents), 48 cold preservation, 49 freezing and freeze-thawing, 50 and irradiation 51 have been used. However, acellular allografts lack SCs and have an internal microarchitecture that does not match that of the recipient nerve, hence failing to restore optimal neural regeneration.
Irrespective of the type of repair, the prognosis of long gap PNIs is unsatisfactory. This is, essentially, the result of erroneous target innervation secondary to the inadvertent axonal misrouting that happens as nerve fibers traverse the critical interphase between the proximal and distal nerve stumps.52,53 The field of peripheral nerve surgery lacks an anatomically analogous nerve replacement that clinically matches or surpasses the autograft. This is partly due to complex regulatory barriers and, most importantly, the failure of conventional tissue engineering (TE) strategies to reproduce the anatomical intricacy of the peripheral nerve architecture in terms of the cellular network, native tissue ECM composition, mechanical properties, and the fascicular topography.
Scope of three-dimensional additive manufacturing technology
To address these shortcomings, additive manufacturing (AM) technologies have been leveraged to create complex three-dimensional (3D) tissue constructs in a layer-by-layer fashion from predefined computer-aided design (CAD) models. Recently, three-dimensional printing (3DP) and bioprinting have emerged as powerful advanced fabrication tools due to their ability to develop personalized, immunocompatible replacement therapies and implants with high precision.54–56 Further, 3D bioprinting could potentially offer control over the spatial organization of cellular components and biological guidance cues, which would allow researchers to devise a biomimetic fascicular pathway to enhance nerve regeneration. Since the recovery of nerve function is contingent on the correct matching of motor and sensory fibers to their respective motor endplates and sensory receptors, in addition to precisely matching the fascicles in both nerve segments, these technologies should, ultimately, allow the development of patient-specific nerve alternatives that achieve this desired fascicle-to-fascicle regeneration. 23 However, before proceeding with the recent developments in the field, a summarized outline of the peripheral nerve ultrastructure is described to understand the target tissue.
Gross and Histological Features of the Peripheral Nerve
The peripheral nervous system (PNS) is anatomically composed of the cranial nerves III to XII and spinal nerves that emanate directly from the brain (including the brainstem) and spinal cord, respectively. 57 Peripheral nerves travel throughout the body, relaying neural signals and commands from the central nervous system. Individual nerve bundles consist of motor, sensory, and/or autonomic fibers, which have distinctive conduction velocities, functions, and diameters.58–60
Connective tissue layers
Cross-sectionally, a peripheral nerve is composed of connective tissue with three distinctive layers: the epineurium, perineurium, and endoneurium (Fig. 2). Dissecting the polymeric and cellular compositions of these layers influences the choice of biomaterials and cells for fabricating nerve guides or tissue-engineered nerve alternatives (Table 3). The epineurium forms the outermost collagenous layer, investing multiple fascicles and the intrinsic neural vasculature. Each single fascicle is wrapped by concentric layers of cellular ensheathment called the perineurium, which consists of flat perineurial cells separated by collagen fibers. 65 The innermost layer is the endoneurium, which wraps and protects the SC-axon complexes. This layer contains highly anastomosing networks of fine microcapillaries that provide oxygenation and nutrition to the intra-endoneurial structures. 66

Anatomy of the peripheral nerve. Color images are available online.
Composition and Function of Connective Tissue Layers of Peripheral Nerves
BNB, blood-nerve barrier; EFLC, endoneurial fibroblast-like cell; SC, Schwann cell.
The endoneurial microvessels are formed of endothelial cells that share their basement membrane lining with pericytes. In addition to the intercellular tight junctions between the perineurial cells, the endoneurial microvasculature collectively forms a dynamic anatomical and physiological diffusion barrier known as the blood-nerve barrier (BNB) or the blood-nerve interface (BNI). 66 The BNI maintains the homoeostasis of the endoneurial microenvironment by stringently regulating the entry of electrolytes, water, and other small molecules into this isolated milieu. This restrictive permeability of the BNB prevents drastic changes in ion concentration and endoneurial fluid pressure due to variations in the blood pressure and volume, which could impair efficient action potential transduction.67,68 Therefore, when engineering artificial biomimetic neural tissues, it is important to ensure that these highly controlled microenvironments are meticulously replicated and maintained.
Cellular components
Peripheral nerves are composed of multiple cell types with distinctive functions. SCs are the primary neuroglial cells of the PNS that provide metabolic and trophic support to axons. In mature, adult peripheral nerves, two major SC phenotypes are identified: myelinating and non-myelinating (Remak) SCs (Table 4). Myelinating SCs are most abundant in the PNS and produce lipid-rich myelin, which provides electrical insulation for axons that permit fast, saltatory conduction of action potentials across the long distance spanned by peripheral nerves. 76 Interestingly, SCs may also exhibit motor and sensory phenotypes that are associated with modality-specific axonal regeneration.
Major Schwann Cell Phenotypes Existing in Peripheral Nerve Tissue
GFAP, glial fibrillary acidic protein; L1-CAM, L1 cell adhesion molecule; MAG, myelin associated glycoprotein; MBP, myelin basic protein; MPZ, myelin protein zero; NCAM, neural cell adhesion molecule; p75NTR, p75 neurotrophin receptor.
The SCs that are coupled to the sensory nerve fibers express high levels of NGF (NGF-β), insulin like growth factor (IGF-1), and erythropoietin (Epo). On the contrary, SCs associated with motor axons produce glial cell line-derived neurotrophic factor (GDNF) and pleiotrophin. 77 Thus, it is apparent that SCs may undergo phenotypic modulation to best support the axonal systems with which they are associated. 76
In addition, other cell types within the peripheral nerves include perineurial cells, endoneurial fibroblast-like cells (EFLCs), mast cells, pericytes, macrophages, and vascular endothelial cells. Perineurial cells, which render elasticity to the perineurium, are specialized myoepithelial fibroblasts. These cells physically contribute to the formation of the perineurial barrier that separates the epineurial and endoneurial interstitial fluid compartments. 78 In the endoneurium, EFLCs are spindle-shaped cells that represent approximately 2–9% of endoneurial cells. EFLCs typically possess irregular basal lamina and extended, angular cytoplasmic processes, which make them distinct from other endoneurial cells. The role of EFLCs has long been debated; however, they might be involved in myelin phagocytosis, immune surveillance, and mediating the inflammatory response after nerve injury. 79 Other endoneurial cells include pericytes, which are specialized smooth muscle cells that control the response of the endoneurial microvasculature to abrupt changes in blood volume and pressure.
The interplay between the various heterogeneous cell populations existing in peripheral nervous tissue is critical for recreating the microenvironment supportive of axonal regeneration after injury.80,81 For instance, resident and circulating macrophages have been shown to play instrumental role in peripheral neural repair. 82 In case of an injury, macrophages are typically the first cells to get recruited and remove the degenerated myelin and fragmented cell and axonal segments. 83 Vascular endothelial growth factor-A (VEGF-A), released by the macrophages, leads to the formation of polarized microvasculature within the regenerative cords of the proximal and distal nerve segments. 84 These vessels were shown to be crucial in guiding SC migration. Although it may seem counterintuitive, nerve fibroblasts might also promote nerve regeneration via favoring the mature SC phenotype and promoting basal lamina deposition. 85 One study explored the effect of nerve regeneration in a 5 mm sciatic nerve gap by transplanting a co-culture of mice nerve fibroblasts and SCs in rodent model. 86 Results revealed that a 1:2 ratio of fibroblasts and SCs enhanced the process of nerve regeneration significantly, resulting in superior functional recovery compared with SCs only. Therefore, these findings underscore the importance of multi-cellular engineered living systems when considering cell-based therapies, including biofabricated neural tissues for peripheral nerve regeneration.
Differential Regenerative Ability of Motor and Sensory Axons
As previously illustrated, accurate and specific target (skin and muscle) reinnervation is central to meaningful functional recovery after nerve transection. The misrouting of motor and sensory nerve fibers during nerve repair could explain the poor recovery seen in patients, for instance after mixed nerve injury. 87 Therefore, elucidating the molecular cues during the course of regenerating axons could facilitate engineering of modality-specific trajectories and cell-selective biomaterials. 88 Eventually, the misdirection of nerve collaterals and inappropriate reinnervation could be prevented.
Basic science research has demonstrated that specific cell adhesion molecules (CAMs) and neurotrophic factors are implicated in the selective regeneration of motor and sensory axons after nerve injury, although exact mechanisms remain unclear. 89 In addition, differential gene expression patterns have been observed in motor and sensory SC phenotypes to support selective axonal reinnervation.90,91 Accordingly, strategies that overexpress proregenerative genes and trophic signals can be employed to modulate or enhance neural functions such as myelination and axonal growth cone motility.92,93
Cell adhesion molecules
Accumulating evidence indicates the involvement of various CAMs in axonal growth cone pathfinding, cell survival, and migration during neural repair.94–96 Essentially, CAMs belonging to the immunoglobulin (IgG) superfamily, commonly known as IgCAMs, are highly expressed in the PNS and impact neuron cellular function post injury. 97 IgCAMs are transmembrane glycoproteins composed of extracellular and intracellular domains. The latter is attached to cytoskeletal elements such as actin and microtubules and mediate intracellular signaling pathways. By impacting the polymerization and disassembly of the cytoskeletal molecules, IgCAMs can influence axonal outgrowth and neuronal cell motility. The most notable IgCAMs implicated in peripheral nerve regeneration include neural cell adhesion molecules (NCAMs), L1-CAM (L1 cell-adhesion molecule), and the close homolog of L1 (CHL1). 97
The NCAMs have been shown to contribute to preferential motor reinnervation (PMR). The PMR refers to the intrinsic ability of regenerating motor axons to selectively reinnervate muscle targets. 98 Mixed nerves usually give off branches carrying purely somatosensory or motor supply. Thus, it is critical that after nerve transection, axons of the proximal stump do not intermingle along their regeneration course and selectively resupply their normal peripheral targets through recognition of appropriate growth substrates. 99 In this regard, Franz et al. demonstrated that the expression of polysialic acid (PSA) moiety of NCAM, a negatively charged glycan, by axons was essential for selective muscle reinnervation. 100 The proposed mechanism by which PSA promotes PMR is believed to be due to direct attenuation of cell–cell adhesive interactions. This effect is believed to enhance the response of sprouting motor axons to specific, instructive guidance ligands expressed in motor pathways.
Moreover, a recent study established the role of CHL1 molecule in the guidance of regenerating motor fibers, thereby promoting PMR. 101 The authors hypothesized that PMR facilitated by CHL1 is mediated via semaphorin 3A and neuropilin 1/2 signaling. In contrast, the L1 adhesion molecule was found to be critical in sensory axon regeneration. In L1-deficient mice, SCs become malformed and fail to ensheath sensory axons and axon survival is impaired.102,103 These findings emphasize the importance of exploiting cell adhesion signaling toward establishing novel pathways that enable modality-specific axonal regeneration across nerve gaps.
Trophic signals
Similarly, SCs from motor and sensory axons overexpress and secrete distinct types of NTFs after axotomy. 104 This differential response might also contribute to the selective regenerative capacity of axons toward their relevant pathways. Several in vitro and animal studies have demonstrated that NGF and neurotrophin-3 (NT-3) have a preferential sensory profile.105–107 In dorsal root ganglia (DRG) organotypic cultures, NT-3 was found to exert oriented, organized, and linearly direct axonal growth of DRG neurites, unlike NGF. Further, both growth factors can act synergistically, when combined together, to promote the guidance of DRG sensory axons over longer distances. 108 Cao and Shoichet demonstrated that combined concentration of NGF/NT-3 of 80 ng/mm/mL each results in 12.5 mm guided distance of axon elongation compared with 7.5 mm when NGF is used alone. 108 Both neurotrophins were shown to mediate their effect on axonal elongation via activation of tyrosine kinase (Trk) receptors and STAT3 (signal transducer and activator of transcription 3) signaling. 109
Other members of neurotrophins such as brain-derived neurotrophic factor (BDNF) and GDNF were reported to be neuroprotective to motor neurons and play a role in PMR.110,111 A study by Santos et al. demonstrated a dose-dependent effect of BDNF on the regeneration of motor axons both in vitro and in vivo. 110 The authors showed that a high dose of BDNF (50 ng/mL) significantly stimulated the outgrowth of motor neurites from organotypic spinal cord slices significantly compared with low concentrations (5 and 10 ng/mL). In comparison, the same high BDNF dose did not result in sensory axonal elongation from DRG cultures. Similarly, in vivo administration of BDNF in a rat nerve gap model resulted in significantly increased number of regenerated motor neurons in all treated groups compared with controls. However, only a low concentration (1 μg/mL) of BDNF resulted in a higher number of regenerated sensory neurons, which confirm the selective motor regenerative property of BDNF through dose manipulation.
Despite these findings, molecular mechanisms underlying axonal cone guidance remain complex and require further investigation. Eventually, detailed knowledge of the guidance cues and signaling pathways would allow researchers to immobilize well-defined gradients of trophic signals on various scaffolds to stimulate the effective migration of sprouting nerve fibers to their distal targets. Moreover, the spatiotemporal delivery of trophic signals to a confined nerve gap is challenging, which creates an unmet demand for advanced drug delivery systems that release neurotrophic factors at appropriate timing and dosage. 112
Gene expression profile
The pattern of gene expression also differs between motor and sensory SC phenotypes. Using gene chip analysis, Jesuraj et al. demonstrated upregulation of neurofilament light polypeptide (NEFL) and protein kinase C iota (PRKCI) genes in the motor pathways of rat femoral nerves. 113 Both NEFL and PRKCI gene products regulate SC-axon intercellular signaling, and motor neuron myelination and growth. In comparison, myelin basic protein (MBP) and neuroligin-1 (Nlgn1) genes were found to be upregulated in the sensory branches. Both MBP and Nlgn1 genes are hypothesized to play a role in neural myelination and synaptic transmission across the sensory nervous system. 113
State-of-the-Art Bioengineering Strategies for Peripheral Nerve Repair
Based on the anatomical complexity, reproducing the native peripheral neural tissue architecture is difficult. Historically, the focus of research for bridging nerve gaps relied on protecting the endogenous reparative mechanism by using conduits, as described earlier. Now, research tends toward developing biomimetic alternatives to the nerve autograft. Further, as health care delivery is shifting toward personalized therapy, it will be of paramount importance to tailor nerve repair solutions that would take into account the patient's specific nerve anatomy as well as unique disease condition. Herein, we review the three key bioengineering schemes currently being investigated in this field. In an increasing order of complexity, a biomaterials-based, a conventional TE-based, and AM-based approaches exist for replacing nervous tissue (Fig. 3). Although an overlap may exist between these different paradigms, it is crucial to elucidate the distinctions between them, as each strategy will eventually have different regulatory paths and translational challenges.

State-of-the-art bioengineering strategies.
Biomaterials-based approach
Recent progress in materials science and polymer synthesis technologies has made huge leaps in the design of artificial nerve guidance devices. A biomaterials-based approach involves, essentially, devising innovative nerve conduits by using advanced biomaterials with neuroregenerative capacity. 3 In addition, this approach focuses on optimizing the conduit's interior architecture to facilitate the formation of robust fibrin cables, which can enhance axonal migration. Generally, an ideal biomaterial candidate for the fabrication of peripheral nerve conduits should exhibit the following criteria 114 : (1) Biocompatibility should not elicit an immunological or allergic reaction once implanted in the host; (2) biodegradability with non-toxic degradation byproducts should eliminate the need for a secondary surgery; (3) neuroinductivity should be able to induce neuronal and glial cell differentiation; (4) neuroconductivity should be capable of transmitting neural impulses from proximal to distal nerve segments; (5) porosity should allow for vascular infiltration and tissue remodeling; (6) semi-permeability should permit gaseous exchange and nutrient transport for supporting cell survival; (7) flexibility should be more relevant for repairs across joint sites; and (8) suturability and mechanical robustness should withstand shear stress and compressive pressure from surrounding tissue. 115 In this regard, several natural, synthetic, and hybrid biomaterials have been exploited for the design of novel nerve conduits, each possessing their own advantages and limitations (Table 5).
Most Commonly Used Biomaterials in Peripheral Nerve Conduit Design
Chitosan nerve conduits (Reaxon®; Medovent GmbH, Mainz, Germany) are authorized and CE-certified for sale in Europe.
FB, foreign body; FDA, Food and Drug Administration; MMPs, matrix metalloproteinases; NGC, nerve guidance conduit; PHB, poly-3-hydroxybutyrate; PLGA, poly (lactic-co-glycolic acid).
Several fabrication processes have been applied for manufacturing NGCs, including injection molding, 133 solvent casting (with or without particulate leaching), 134 phase separation, 135 freeze-drying, 136 and electrospinning. 137 Among these, injection molding and electrospinning are the most commonly utilized techniques for developing NGCs. 138 However, electrospinning results in highly disordered and random fibers, whereas solvent casting uses toxic organic solvents during the fabrication process, which could produce scaffolds with traces of these harmful chemicals. Nevertheless, they are all limited by the lack of reproducibility, inability to control the porosity, pore size, and interconnectivity of the scaffolds. 139 Further, the fabrication of complex patterns such as multi-lumen conduits by using these techniques is technically challenging.
Single-lumen hollow NGCs dramatically fail to induce neural regeneration across critical-sized nerve defects (∼30 mm in rabbits and humans, ∼15 mm in rats). Thus, research is directed toward modifying their interior architecture and incorporating intrinsic structural frameworks, which are pivotal for effective axonal regrowth across these critical gaps. In preclinical testing, most of these modifications have increased the size of gap that can be repaired in rat sciatic nerve models from 10 to 15–20 mm. 114 A few clinical case reports have demonstrated the potential efficacy of poly (glycolic) acid (PGA) filaments, collagen sponges, and other intrinsic structural frameworks in achieving motor and sensory recovery in long gap nerve defects.140,141 For more comprehensive reviews on the latest progress in conduit design, please refer to articles by Wang and Cai, 142 Daly et al., 3 and Vijayavenkataraman. 143
Conventional TE-based approach
The sole use of biomaterials, however, represents a passive approach for restoring nerve integrity. Being completely reliant on the healing capacity of the patient's body and, eventually, the severed nerve regenerative potential, nerve repair using conduits only, could be insufficient for inducing functional neural recovery. 144 This becomes important in the presence of critical gaps that exhibit extremely limited nerve regeneration as a result of poor ECM formation, diminution in the neurotrophic support, and limited SC migration and proliferation. Accordingly, topographical or molecular modifications of nerve conduits have been coupled with the presence of an active biological neuroregenerative component such as cells or biological cues to augment the physiological neural repair process. Conventional peripheral nerve tissue engineering (PNTE) strategies apply the classic TE triad that combines (1) scaffolds, (2) cells, and (3) growth factors to develop more robust regenerative templates with desirable mechanical properties mimicking the native nerve.145–147 To this end, cell supplementation of polymeric NGC or decellularized allografts has been pursued as a viable strategy to augment the regenerative cellular response to PNIs. 148
Being the primary supporting cells in the PNS that orchestrate endogenous reparative mechanisms after PNIs, SC transplantation in combination with nerve scaffolds has been widely investigated, particularly across critical nerve gaps. 149 In comparison to hollow conduits, scaffolds loaded with SCs, in vivo, demonstrated superior nerve repair and functional recovery. 3 The SCs mediate neural repair through deposition of their own basal lamina, promoting re-myelination of regenerating axons, and more importantly, help in creating cell-secreted chemotropic gradients that are critical for directing the growth cone of nerve fibers, a phenomenon known as growth cone chemotaxis. However, the invasive extraction methods of SCs necessitating the sacrifice of a healthy nerve and prolonged culture period are major drawbacks of SC transplantation. 150 This has motivated researchers to consider alternative cell types and sources. Cell-based therapies utilize the potential of autologous stem cells, adipose-derived and bone-derived mesenchymal stem cells (MSCs), for peripheral nerve repair because of their abundance, plasticity, relatively facile isolation, and culture techniques.151–153 Although they have a different embryological origin, MSCs trigger the process of peripheral nerve regeneration via paracrine mechanisms through the release of NTFs such as NGF, GDNF, and BDNF. 154 Besides, the immunomodulatory properties of MSCs could potentially reduce infiltration of collagen and scar tissue formation in the conduit. 155 Other slightly lesser explored sources of stem cell investigated for PNTE are induced pluripotent stem cells (iPSCs), dental pulp stem cells, hair follicle stem cells, and neural stem cells.156,157
Cells have been introduced into nerve conduits by using different techniques, including suspension cultures encapsulated within intraluminal hydrogels, 158 seeding prefabricated scaffolds or intraluminal guidance structures in culture, and intraluminal injection.151,159,160 However, these conventional methods have significant limitations. First, simple encapsulation of cells in a hydrogel or top seeding on scaffolds is time-consuming and often leads to heterogeneous distribution of cells within the 3D structure. This leads to a lack of precise control over the cell density arising from non-uniform cell attachment. In addition, weak cell-matrix compliance can potentially result in cell detachment when implanted in vivo. Cell leakage and migration out of the conduits are also possible complications of luminal cell injections and seeding. 161 These shortcomings have resulted in the inability of these scaffolds to effectively generate and harness the complete potential of cell-secreted neurotrophic gradients.
In addition, NTFs, including NGF, 162 GDNF, 163 BDNF, 164 NT-3, 165 and VEGF, 166 have also been employed in peripheral nerve regeneration as they play a vital role in promoting SC proliferation and migration, guiding neurite outgrowth, and inducing neuroprotection.37,167 Besides, the presence of spatiotemporal and concentration gradients of chemokines and growth factors are crucial for tissue development, especially for directionally oriented tissues such as peripheral nerves. 168 By creating scaffolds with true biochemical, directional gradients of one or multiple growth factors, the process of driving the migration of SCs into the regenerating nerve bridge and axon elongation could be facilitated. Traditionally, the delivery of NTFs from the nerve conduit wall has been achieved by either tethering or physically adsorbing the proteins to the wall material. Several attempts have been made to optimize release kinetics and prolong localized availability of bioactive molecules. These include protein entrapment in hydrogel matrix loaded into the conduit lumen or encapsulation in microspheres embedded in the conduit wall. 169 Nevertheless, problems related to initial burst release, loss of bioactivity, and poor bioavailability remain unresolved. More importantly, theses growth factor presentation strategies do not sufficiently reproduce the complexity of the ECM microenvironment, which is pivotal for inducing satisfactory nerve regeneration over critical gaps. Accordingly, advanced fabrication strategies such as 3D bioprinting are needed to effectively engineer these spatially controlled niches and gradients.
AM-based approach
With major shortfalls associated with classical biomaterial and TE fabrication methods, there is an immense demand for designing scaffolds that can be fabricated with superior resolution, flexibility, speed, and scalability for regenerating complicated nerve gaps. Recently, sophisticated, cost-effective industrial systems such as rapid prototyping (RP), including AM, have been utilized in the health care arena. AM-based strategies are centered on the automated and timely production of 3D structures with predefined geometries using computer-aided modeling. Structural assembly is then achieved via sequential and precise placement of materials in a layer-by-layer fashion to yield geometrically complex shapes, which could not be produced by other techniques such as subtractive manufacturing. 170 AM-based processes are also widely exploited in pharmaceutical delivery, preoperative surgical planning, and surgical education.
AM is currently being explored to develop personalized nerve substitutes, in vitro models for peripheral nerve research, and advanced tissue engineered peripheral nerve solutions. A typical additive manufacturing or 3DP workflow can be broken down into three steps: (1) image acquisition and segmentation, (2) mesh model creation, and (3) 3DP. The first step involves capturing images of the organ of interest by using tomographic medical imaging such as computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography studies. It is critical to highlight that “diagnostic” imaging modalities are certainly not the best study for optimal 3D print generation, particularly in tissues where minute morphological details are vital. For instance, magnetic resonance neurography (MRN), although being an advanced neuroimaging technique, is not optimal for depicting detailed fascicular anatomy, including the endoneurial tubes. Nevertheless, Hu et al. used MRN as a proof of concept to reconstruct a patient's sciatic nerve and generate an NGC conduit model for indirect 3DP. 171 Generally, scan parameters that allow the accurate visualization of the desired anatomic tissue will be similar to those used to generate the 3D-printed structure. After image acquisition, the organ of interest needs to be segmented. Image segmentation involves isolating the target structure from the rest of the scanned anatomy and delineating boundaries between various tissues in images to generate patient-specific, highly accurate models of the desired organ. Segmentation can be done by using commercially available resources such as Osirix MD, 3D Slicer, or Materialise Mimics Imprint.
In the second step, postprocessing of the segmentation into a 3D printable mesh is performed and an .STL (Standard Tessellation Language) file is created from the segmented anatomy by using CAD tools. This step involves further manipulation to eliminate flaws and correct errors and discontinuities in the segmented model that arise during the processes of image segmentation or exporting. After mesh refinement, the final step involves exporting the refined 3D model to the printer by using different file formats. The most commonly used file formats for AM are STL, VRML (Virtual Reality Modeling Language), and the .OBJ formats. 172 Several techniques can be utilized for non-biological 3DP or bioprinting of the designed structure, each with their own advantages and limitations. In this section, we will elaborate more on these processes and their most recent applications to develop personalized nerve conduits and bioprinted constructs for peripheral nerve regeneration.
3DP of NGCs
Non-biological 3DP has been used in clinics to generate anatomical models and bespoke implants for preclinical education and therapeutic applications, respectively.173–175 Generally, this subtype of AM is predominantly focused on hard tissue regeneration such as bones and teeth owing to the inherent rigidity of the majority of used biomaterials. 176 Nevertheless, this technology has found further applications in the research field of peripheral nerve surgery through the development of customized 3D-printed nerve guides. This could potentially enable repairing injuries involving complex injuries involving nerve bifurcations that are surgically irreparable by using currently available nerve conduits (Fig. 4). From a technical perspective, 3DP offers also more versatility over controlling the internal structure of the fabricated scaffold, including the ability to modulate porosity, pore size, and mechanical properties, unlike conventional approaches.

3D printing for bridging complex nerve pathways (Adapted from Johnson et al.
180
).
To date, several advanced multi-functional NGCs have been additively manufactured by using various 3DP approaches and polymers. Technically, 3DP methods can be classified into stereolithography apparatus (SLA), digital light processing (DLP), fused deposition modeling (FDM), and inkjet 3DP. Each printing modality is associated with unique merits and drawbacks, and more importantly, it uses different types of printable biomaterials. A summary of the biomaterials most recently used for fabricating NGCs using 3DP techniques and salient design features and in vitro and in vivo findings can be found in Table 6. Herein, we will delineate and contrast the different techniques that have been utilized in the 3DP of nerve guides.
Most Recently Reported Three-Dimensional Printed Nerve Guides
μSL, micro-stereolithography; 3D, three-dimensional; 3DDCs, 3D-printed drug releasing conduit; 3DG, 3D printable graphene; ADSCs, adipose derived stem cells; BDNF, brain-derived neurotrophic factor; CMAP, compound muscle action potential; DLDM, double nozzle low-temperature deposition manufacturing; DLP, digital light processing; DRG, dorsal root ganglia; EHD, electrohydrodynamic; EHS, Engelbreth-Holm-Swarm; GDNF, glial cell line-derived neurotrophic factor; GelMA, gelatin methacrylate; hMSCs, human mesenchymal stem cells; ID, internal diameter; MAP2, microtubule-associated protein 2; mPEG, methoxypoly(ethylene glycol); NCV, nerve conduction velocity; NGF, nerve growth factor; OD, outer diameter; PAA, polyacrylic acid; PC12, pheochromocytoma-derived neuronal cell line; PCL, polycaprolactone; PDA, poly (dopamine); PEG, polyethylene glycol; PEGDA, polyethylene glycol diacrylate; PLA, poly (lactic acid); PGSm, poly (glycerol sebacate) methacrylate;; PPy, polypyrrole; PU, polyurethane; rGO, reduced graphene oxide; SA, surface area; SCs, Schwann cells; SFI, Sciatic Functional Index; SL, stereolithography; SLA, stereolithography apparatus; TCP, tissue culture polystyrene; XMU-MP-1, 4-((5,10-dimethyl-6-oxo-6,10-dihydro-5H-pyrimido[5,4-b]thieno[3,2-e][1,4]diazepin-2-yl)amino) benzenesulfonamide.
Stereolithography apparatus 3DP
The SLA is regarded as the earliest and most mature RP technique available nowadays.193,194 The NGCs developed by using SLA exhibited excellent mechanical performance and advanced structural features such as intraluminal topographical guidance cues concurrently (Table 6). The SLA is essentially a liquid-based technology that converts liquid polymer resins to complex and multi-functional solid architectures in a cost-effective and scalable fashion. The method is based on photopolymerization reactions that proceed under visible or ultraviolet (UV) light in the presence of a photosensitive system of unsaturated prepolymers and photoinitiators (PIs). 195 Light irradiation controlled by CAD releases initiating species (e.g., radicals or cations) from the PIs, which then attack the electron-poor carbon-carbon (C = C) double bonds of monomers or oligomers to form covalent bonds between monomeric units leading to liquid–solid phase transition of the resin. Traditionally, an SLA system consists of three components: (1) a bath (vat) of photocrosslinkable resin, (2) a mobile platform residing inside the vat, and (3) a UV laser source to cure the resin in layers as the platform descends deeper into the vat. The solidification of the resin continues on a slice-by-slice basis until the entire solid 3D object is generated.
An interesting feature of SLA is the ability to control the pattern formation of each individual layer by moving the laser beam, which permits the facile printing of large volume models with intricate designs. Compared with other 3DP methods, SLA produces constructs with high resolution, up to 20 μm, and smooth surface finishes. 196 However, one major disadvantage that could restrict the utility of this technique is the paucity of candidate printable materials; currently, only photopolymers such as acrylates, methacrylates, and epoxy resins are compatible with SLA-based platforms. 197 In addition, neural scaffolds produced by using SLA might not represent a good cytocompatible option for postprinting cell seeding or supplementation. Although most polymers employed in SLA for medical applications are biocompatible such as polyethylene glycol (PEG), fabricated scaffolds might contain residual free radicals that are carcinogenic, toxic byproducts of the photocrosslinking reaction, and unreacted monomers. Unless robust quality control systems are implemented to achieve acceptable safety standards, these factors might potentially undermine the viability of cells transplanted onto these scaffolds and would require long-term monitoring to exclude possible mutagenic effects.
Digital light processing 3DP
Another vat polymerization technique similar to SLA that uses laser beam is DLP 3DP. 198 Unlike SLA, which is a bottom-up printing approach, DLP is a top-down process. The DLP uses a digital projector to project an image, composed of squared voxels, of the two-dimensional (2D) cross-section of the desired structure into a photocurable liquid resin. 194 The printing process in DLP uses a digital mirror device (DMD), which is an array of micro-mirrors, to control the curing laser beam (Fig. 5IV.a). By using a DMD, a complete layer of the resin can be cured at once, making DLP relatively faster than SLA. 198 Despite the high resolution achievable by DLP-based printers, only small-sized objects can be printed, as a limited projection size is mandatory to achieve this high precision. In addition, DLP systems are very expensive and produce a characteristic “boxy” surface finish due to its squared voxel. Although the technique uses photosensitive polymers, nerve conduits produced using DLP were flexible and had high compressive moduli (Fig. 5IV.d, IV.e). In addition, they have been shown to support very high cell survival rates in vitro and promoted human SCs proliferation. 191
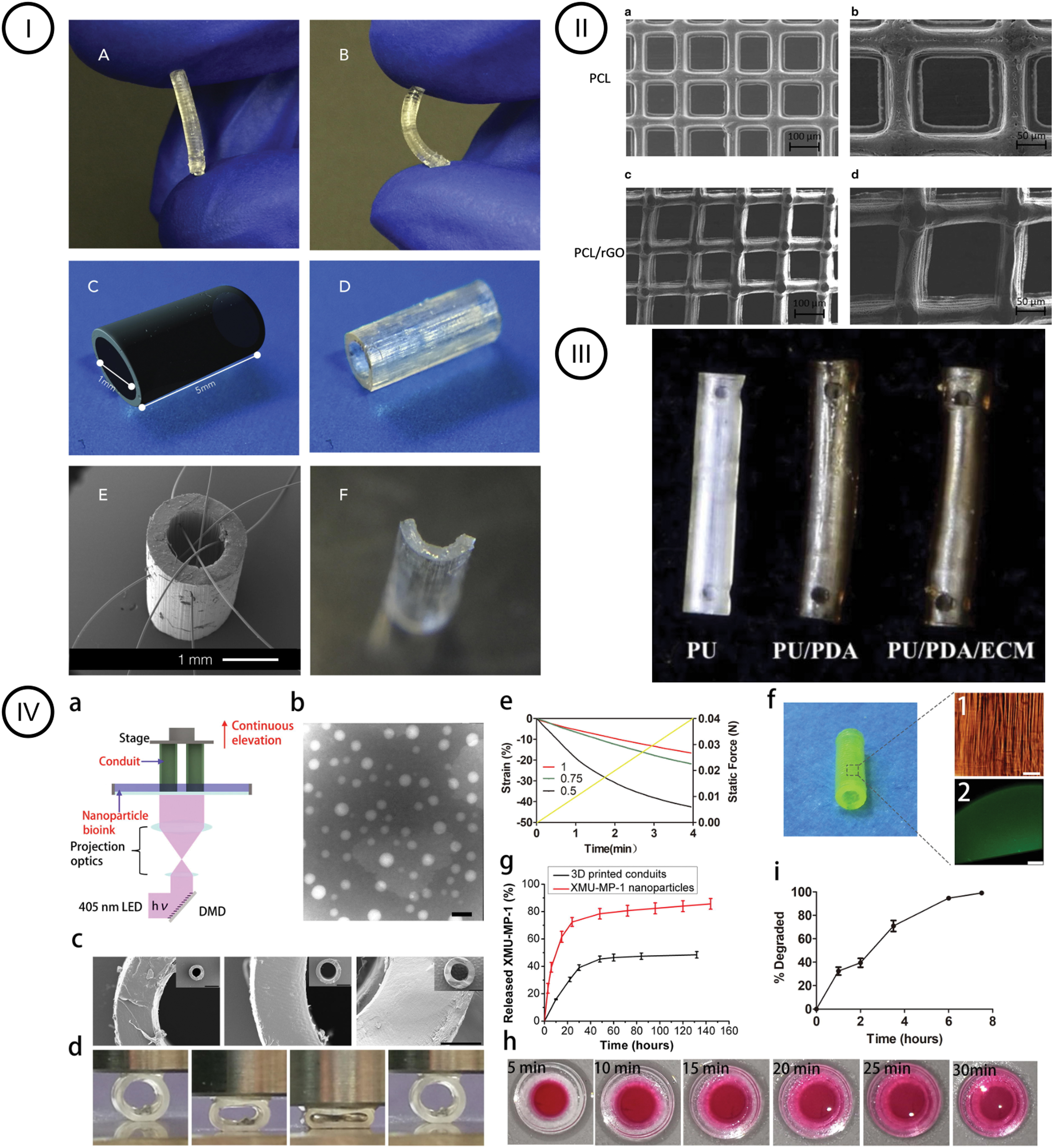
3D printing of nerve guides.
FDM or extrusion 3DP
FDM or extrusion 3DP offers a more affordable option for customized 3D scaffold fabrication compared with light-based 3DP approaches. The FDM is based on the hot melt extrusion technology. This technique uses a polymer filament of thermoplastic material such as poly (lactic-co-glycolic acid) (PLGA), poly (lactic acid) (PLA), or polycaprolactone (PCL) to build objects in a layer-by-layer fashion. Essentially, the polymer is fed into a heated metal cylinder, liquefied, and then extruded into the printing bed via a nozzle of predetermined size along with a computer-controlled path.199,200 Although the neural regenerative potential of FDM-manufactured nerve guides remains unexplored, FDM was employed to create a nerve graft model using PLA with a simulated nerve defect in a recent study. The authors investigated the feasibility of printing a customized nerve graft by using 3D reconstruction data from micro-MRI scans of human tibial nerve samples. Interestingly, the 3D-printed model demonstrated appreciable similarity to the original nerve fascicles, and matched with the proximal and distal segments of the nerve defect (Fig. 6II.a–II.e). FDM 3DP offers a great advantage in the field due to the ability to create personalized NGCs from currently available FDA-approved thermoplastics such as PGA and poly (
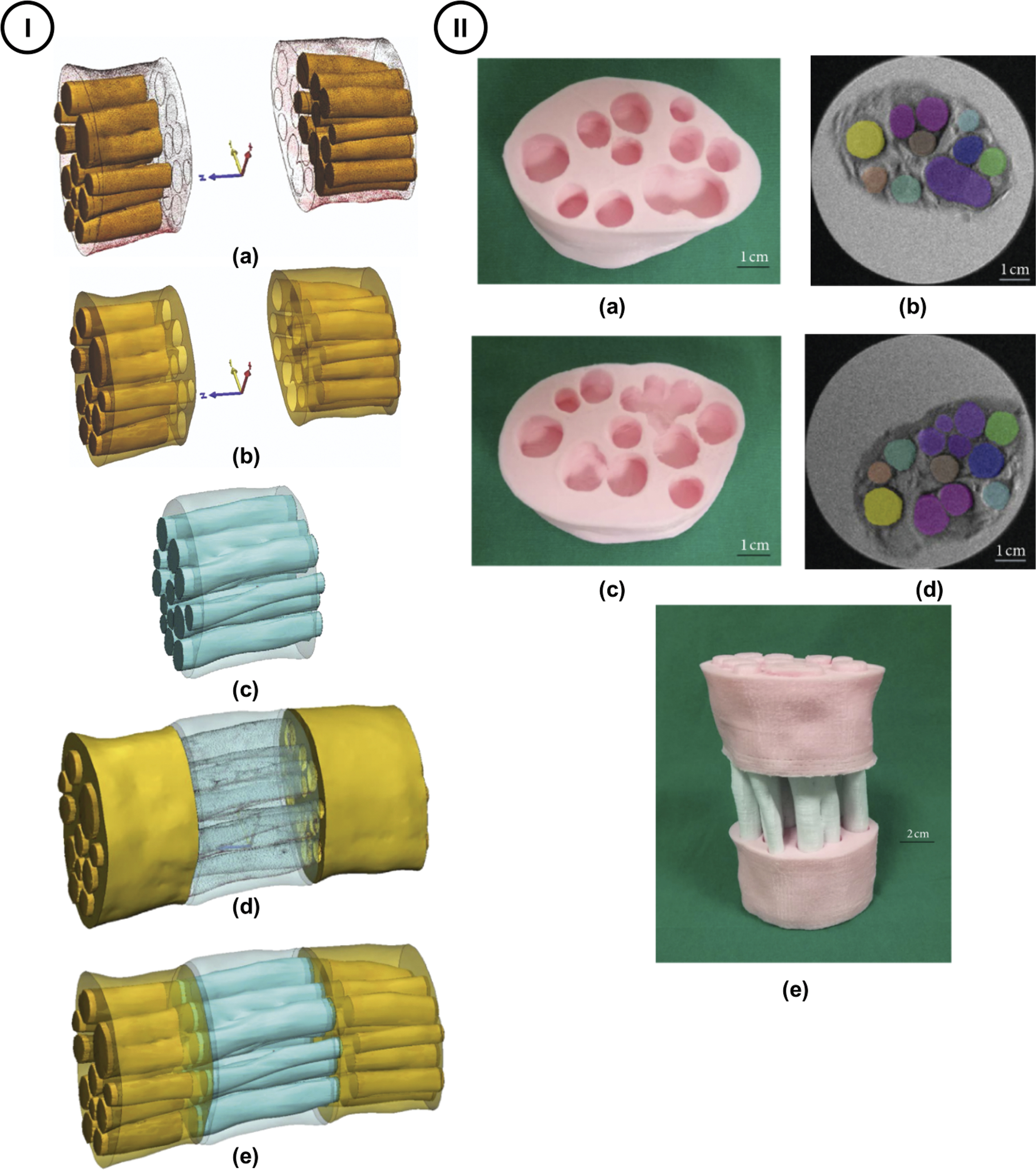
Using micro-MRI scans 3D reconstruction as a proof-of-concept to develop 3D-printed customized nerve graft (Adapted from Yao et al.
275
).
However, FDM 3DP has some serious constraints. The application of heat in FDM to melt the polymer can have undesirable effects on resultant material properties, and it strictly limits this technique to printing synthetic thermoplastic materials only. The high operating temperature of this system limits their application for biological supplementation with cells and biomolecules during printing. These materials possess Young's moduli different than living tissues and lack biologically active motifs, which make them unfavorable for soft TE. 201 Alternatively, a lower temperature-cooling platform called Low Frozen Deposition Manufacturing (LFDM) was developed to overcome these shortfalls. 198 In LFDM, the extruded ink immediately freezes as it comes into contact with the low temperature plate, thus the structure does not collapse during printing. The LFDM was used by Cui et al. to fabricate an integrated double-layered conduit of outer polyurethane (PU) and inner collagen filament layer. 190 The resulting porous conduits supported SC adhesion and proliferation in vitro compared with PU-only conduits. Nonetheless, there will be a need for more innovative approaches to augment the bioactivity of future FDM fabricated nerve guides such as using intraluminal hydrogel coatings or biofunctionalization with ECM molecules.
Inkjet 3DP
Inkjet 3DP is a non-contact printing method that involves ejecting controlled volumes of ink droplets through a printhead orifice to predefined locations on a collecting plate. Inkjet printing can be broadly categorized into: continuous-inkjet 3DP and drop-on-demand inkjet 3DP. 202 The latter will be reviewed within the context of 3D bioprinting. The printing principle of inkjet techniques is fundamentally centered on binder jetting technology. This process involves the dispensing of precisely controlled droplets of a liquid binder solution onto a powder bed of the desirable material (e.g., polymers, ceramics, etc.). The release binder induces fusion of powder particles to create an agglomerated 3D object. T Inkjet-based 3DP has the combined advantage of achieving cost-effective and high-resolution (approximately 20–50 μm) printing in both the x and y-axes. The printing process can also be expedited through using multi-nozzle systems. 203 However, inkjet platforms are capable only of printing low-viscosity solutions (<10 mPa/s) and result in low cell densities if employed for biofabrication.
A recently emerging subtype of inkjet 3DP that was investigated in NGCs fabrication is electrohydrodynamic (EHD) jetting (Fig. 5II). In principle, EHD printing uses an electric field, resulting from the electrical potential difference between the printhead and substrate, to pull a stream of ink droplets through the nozzle rather than pushing out as seen in the conventional inkjet systems. Advantages of EHD jetting include the ability to manufacture high-resolution, complex scaffolds in addition to allowing for precise control of the pore size, porosity, and fiber diameter and alignment using computer-controlled software. Vijayavenkataraman et al. constructed a library of PCL-based nerve conduits with tunable degradation rates using EHD-jet 3DP. 139 PCL scaffolds of five different pore sizes (125–550 μm) and porosities (65–88%) were fabricated. It was reported that ultimate tensile strength of NGCs with pore sizes of 125 and 215 μm mimicked those of the native peripheral nerve (6.5–11.7 MPa). Further, the EHD 3D-printed scaffolds supported neuronal tissue differentiation on incorporation of electrically conductive polymers such as reduced graphene oxide (rGO) and polypyrrole (PPy) in related studies.182,183
3D bioprinting of peripheral nerve tissue
Although non-biological 3DP could support anatomically complex geometries for injured nerves, they are limited in functional restoration. Thus, this paves the way for personalized grafts with cellular and biological components via 3D bioprinting. 3D bioprinting, also referred to as biofabrication, is another rapidly progressing domain of AM that has been recently exploited in advanced PNTE. This automated paradigm offers user-driven spatial positioning of the encapsulated bioactive substrates with the ability to create complex structures toward developing biologically inspired functional tissue constructs. For peripheral nerve repair, biofabrication offers the ability to develop patient-specific engineered nerves containing exogenously fabricated bands of Büngner, which recapitulate the physiological nerve regeneration process. After nerve injury, regenerative tracks, referred to as the bands of Büngner, comprising longitudinally arrayed columns of SCs and fibrin cables are formed. 204 These pathways are critical for selectively guiding regrowing axons to the target sites of innervation. Conventional strategies focus on inducing the formation of these regenerative corridors through the addition of topographical and biological cues to synthetic conduits, without actively constructing this complex microenvironment. 204 It is speculated that biofabrication technologies could allow more versatility and precision regarding the placement of neurotrophic factors and cells within the 3D space, thus enabling the development of patient-specific biomimetic fascicle pathways.
In addition to potential therapeutic applications, bioprinted nerve grafts and nerve organoids composed of patient-derived cells could serve as in vitro 3D tissue models for neuropathic disorders, for example, demyelination and neurodegenerative conditions, drug screening, and toxicology studies. Conventional in vitro assays for studying peripheral nerve disorders and regeneration are relatively simple and based solely on 2D monolayer neuronal cultures or nerve explants. 205 However, they fail to echo the complex 3D characteristics of living tissues, providing unreliable data of neuronal function. To circumvent this, Khoshakhlagh et al. fabricated a physiologically relevant 3D model of the myelinated peripheral nerve using micro-photolithography. 206 This in vitro model consisted of a photocurable dual hydrogel system comprising a cell-restrictive component and a cell-permissive component. The cell-restrictive part was formed of PEG diacrylate and served as a hydrogel micro-mold, whereas, the cell-permissive hydrogel component consisted of either methacrylated dextran or heparin that supported rat neuronal cell culture (Fig. 7A.I). This 3D configuration promoted both linearly directed neurite outgrowth from rat DRG explants and myelin deposition by rat SCs. The final hydrogel construct mimicked the myelinated axonal tracts of the native PNS tissue. In addition, myelin formation was identifiable on histology and the characteristic spiral, compact structure of the myelin sheath was demonstrated on transmission electron microscopy (TEM) imaging (Fig. 7A.II).
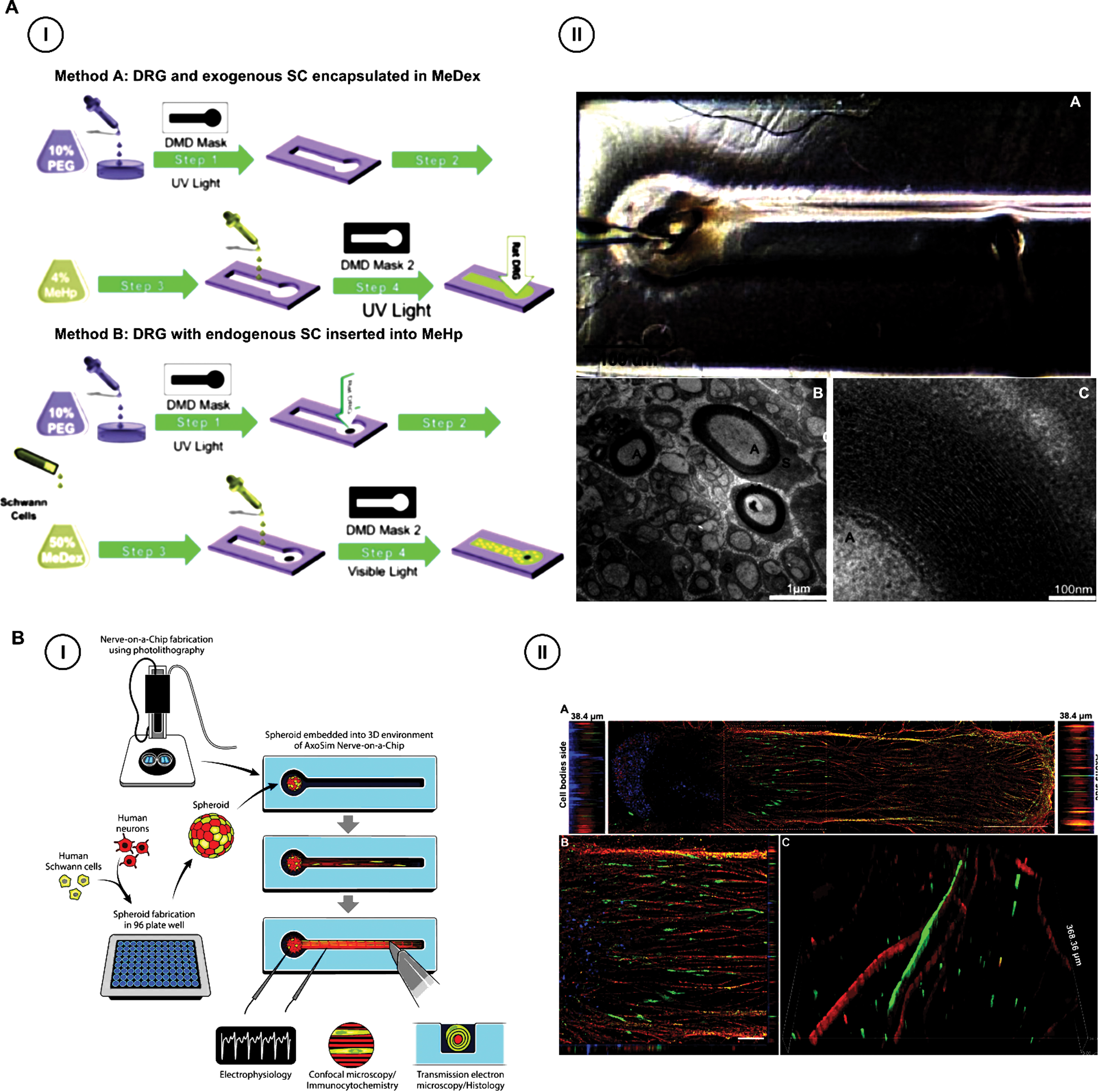
Engineering nerve-on-a-chip models.
Moreover, Sharma et al. took a step further and developed the first human biomimetic myelinated peripheral nerve organ-on-a-chip model, using a similar photolithographic approach. In their study, the authors developed an innovative 3D peripheral nerve model utilizing spheroidal co-cultures of human primary SCs and human iPSCs-derived motor neuronal cells (Fig. 7B.I). 207 Interestingly, this novel co-culture of SCs and human motor neurons was not only deemed viable (∼4 weeks) but also supported extensive neurite outgrowth (∼5 mm in vitro) and effective myelination of the motor neurons by human SCs (Fig. 7B.II). Besides, such microengineered nerve models permitted the measurement of clinically significant electrophysiological metrics such as nerve conduction velocity and compound action potential, which objectively evaluate neuropathological conditions. In addition, the cardinal histomorphometric parameters of peripheral nerves, usually obtained from in vivo studies, such as axonal diameter, myelin thickness, and g-ratio (ratio of inner axonal diameter to the diameter of the whole nerve fiber, including myelin sheath), were analyzable from TEM of these 3D functional nerve models. These 3D systems should potentially offer more representative models, thereby reducing burden on animal testing, resolving the associated ethical dilemmas. 208
Currently, peripheral nerve tissue bioprinting is in its infancy, focusing toward standardization of bioinks for printing, spatio-temporal cell alignment in the bioprinted constructs, in vitro neurite outgrowth assays, and in vivo biocompatibility. This section aims at summarizing the principles of scaffold-based and scaffold-free bioprinting techniques and recent advances in the field to develop biomimetic peripheral nerve tissues.
Scaffold-based peripheral nerve tissue biofabrication
Bioinks
Bioinks are the cornerstone of scaffold-based approaches for the biofabrication of living tissues with preprogrammed geometries. Although a consensus on bioink definition is currently lacking, the term usually encompasses materials that enable the 3DP of cells and biologics, including signaling molecules and growth factors. Bioinks generally include cell-encapsulating hydrogel precursor solutions and ECM-based materials.209,210 Hydrogels possess various favorable features that make them the material of choice for bioprinting cell-laden constructs, including peripheral nervous tissue. 211 Along with their biocompatibility, hydrogel-based bioinks are highly hydrated, tunable networks that can be formulated from a diversity of natural and synthetic multi-functional biopolymers. 212 The high-water content makes hydrogels inherently porous and permeable. These features permit the prompt diffusion of oxygen and nutrients throughout the scaffold, which is necessary for maintaining survival of the encapsulated cells. The porosity of hydrogels also facilitates cell migration and remodeling of the surroundings. Finally, advances in gelation mechanisms enable cell-friendly crosslinking of hydrogels into solid stable structures while minimizing the physiological stress on printed cells. Thus, these specifications allow hydrogels to closely mimic the native microenvironment of cells. A downside of hydrogel bioinks, however, is their inherent fragility. They often fail to maintain their designed shape. Notwithstanding, different reinforcing strategies have been researched to buttress these mechanically unstable printable materials while retaining their favorable biological properties. These include the use of hydrogel composites as printable materials, supramolecular bioinks, double network bioinks, and co-printing thermoplastic reinforcement. 211
The printing fidelity of bioinks can also be enhanced by either in-process or postprocess crosslinking approaches. 212 Examples of in-process crosslinking polymers are alginate and fibrin. To induce crosslinking of the hydrogel precursor during the printing process, a coaxial printhead can be used to simultaneously extrude both the bioink and crosslinker, thereby enabling instantaneous stabilization of the printed structure. On the contrary, postprocess crosslinking methods provide structural fidelity once the entire structure is fully deposited onto the printing bed. Although the method could pose cytotoxicity, curing the printed tissue using UV or light is typically used to achieve postbioprinting crosslinking. Recently, the deposition of hydrogel bioinks within a temporary sacrificial support material has also proven a viable technique to fabricate intricate-shaped structures, at scale, to date not feasible to generate with conventional 3DP methods.213,214 Further details on bioink designs and crosslinking schemes are beyond the scope of this review.
Bioinks ideal for the 3DP of neural tissue must render adequate biocompatibility to allow the encapsulation of neural cells and NTFs, and offer prolonged viability and differentiation. Bioinks must possess functional motifs that support cell adhesion, spreading, differentiation, and can induce basal lamina deposition by SCs. In addition, bioinks must produce scaffolds that are mechanically analogous to native nerve tissue (∼6.5 MPa) by having controlled degradation in synchronization with axonal regeneration. Another important consideration for nozzle-dependent biofabrication (microextrusion and inkjet-based techniques) is that optimal bioinks should display viscoelasticity as well as shear-thinning (or thixotropic) properties, that is, the viscosity correspondingly decreases under increased shear stress. 215 The shear-thinning property of extrudable bioinks aids in alleviating the printing-induced stress caused to the cells, and it enhances the printing fidelity. In addition, to produce multi-layered 3D structures with high resolution, extrusion-based biofabrication also utilizes self-healable bioinks. A self-healing hydrogel ink is capable of restoring its functionalities, morphological and mechanical integrity after cessation of the extrusion shear stress. 216 Self-healing mechanisms are essentially based on dynamic or reversible covalent bonding and non-covalent physical interactions (hydrogen bonding, hydrophobic interactions, electrostatic interactions). Postprinting, the self-healable bioink should also harden, in a cytocompatible fashion, to conserve the structural stability.217,218
Identifying the optimal cell-laden bioink formulation is the keystone step toward realistic, successful nerve bioprinting. Despite the variety of constituent materials present, an overwhelming challenge facing the field is the significantly limited amount of bioinks suitable for neural biofabrication meeting the criteria above. 219 Polymeric bioinks derived from natural sources, such as gelatin, hyaluronic acid, alginate, and fibrinogen, are generally used in biofabrication owing to their ubiquity, low cost, biodegradability, and bioactivity. However, the sole use of natural bioinks could not be adequate for fabricating self-standing structures and it is exceedingly troublesome to obtain regulatory permission for biological therapies. 220 Besides, natural polymers are associated with quality control issues and batch-to-batch inconsistencies. Thus, the addition of synthetic polymers should be considered. Biomaterials such as PEG, Pluronic, and polyvinyl alcohol (PVA) offer the benefits of bestowing mechanical strength, tunability, pH, and temperature responsiveness. In addition, synthetic bioinks lack manufacturing heterogeneities typical of their natural counterparts such as collagen, chitosan, and silk. Despite that, synthetic bioinks are inert to cellular activities such as adhesion and proliferation. Therefore, it is often mandatory to functionalize synthetic bioinks with cell–cell adhesive motifs, such as RGD (Arg-Gly-Asp) tri-peptide and IKVAV (Ile-Lys-Val-Ala-Val) fragments, or with incorporated growth factors for improving the cell–matrix compliance, necessary for facilitating cell attachment and survival.
Most of the present bioinks designed for PNTE, typically in the form of SC-laden constructs, are simply formulated by blending cells of interest with hydrogels. This approach is, however, an oversimplification of the hierarchal alignment of native neural tissues, which is characterized by a multiscale modular design. 221 Essentially, these modules describe the spatial organization of cells and ECM as repeated units of 3D building blocks. Modularity allows uncoupling of the cellular and tissue micro- and macroenvironments, which is pivotal for achieving the multifunctionality that is a prerequisite for proper tissue performance. 222 In its simplest form, modularity aims at developing 3D biomimetic scaffolds that recapitulate the smallest living functional units, that is, cells coated by CT matrix. A commonly exploited technique to implement modular bioinks is via encapsulation of cells in microgels, which are micrometer-sized hydrogels.
Recently, Chen et al. hypothesized a multiscale modular bioink for PNTE using hydrogel microspheres (Fig. 8I). In their design, they combined PC12 (a pheochromocytoma-derived neuronal cell line) laden microgels and rat SCs (RSCs; RSC96 cells) laden gelatin methacrylate (GelMA) hydrogel to assemble the 3D composite scaffolds using extrusion bioprinting. 223 The hydrogel microspheres were fabricated from chitosan and GelMA (GC-MS) using a microfluidic chip. Results demonstrated that GC-MS provided a suitable surface microenvironment for PC12 cell adhesion and growth. GC-MS were also shown to stimulate neurite outgrowth and elongation of PC12 cells when loaded with NGF. Interestingly, bioprinting of the modular composite scaffold revealed uncoupling of the cellular microenvironments on confocal microscopy in which RSCs were homogenously distributed throughout the bioink and PC12 cells were found to be adherent and proliferating on the microspheres (Fig. 8III.g, III.h). This 3D environment mimicked the anatomical organization of SCs wrapping the neuronal axons observed in mammalian nerves.

Effect of bioprinting speed on regulating the alignment of SCs and laminin. (Reproduced from Ning et al.
228
).
3D bioprinting techniques
According to the technique characteristic, the common categories of biofabrication include microextrusion, inkjet, and laser-assisted methods.224,225
Microextrusion bioprinting
Microextrusion-based bioprinters currently represent the most commonly utilized platform for biomanufacturing SC-laden constructs (Table 7). This technique utilizes pneumatic or mechanical (piston-driven or screw-driven) extruding pumps to continuously dispense filaments of cell-laden viscous bioinks onto a predefined location on receiving substrates such as a culture dish, growth medium, or support gel. 232 The instrumentation simplicity, low cost, and ability to eject bioinks with high cell densities are some apparent advantages of extrusion bioprinting that accounted for its extensive popularity. 233 Moreover, the resolution of the final bioprinted structures can be easily modified by manipulating printing parameters such as extrusion pressure, nozzle diameter, printing speed, path interval, etc. 234 To identify the appropriate extrusion conditions, rheological studies of bioinks are usually conducted to compute ink's viscosity and complex modulus.
Peripheral Nerve Tissue Engineering Using Scaffold-Based Bioprinting
2D, two-dimensional; 40FAH, 40% fibrinogen, alginate, and hyaluronic acid; FRAH, fibrinogen, RGD-modified alginate, and hyaluronic acid; GC-MS, gelatin methacrylate/chitosan microspheres; PC12, pheochromocytoma-derived neuronal cell line; PDGF, platelet derived growth factor; RGD, Arg-Gly-Asp; RSCs, rats Schwann cells.
Reproduced from Taniguchi et al. 252
Bioinks printable using extrusion-based techniques tend to have high viscosities (up to 6 × 107 mPa/s), as they better maintain their structures. 217 However, the high viscosity prerequisite could lead to nozzle tip obstruction and comes at the expense of compromising cell survival due to the resultant shear and extensional stresses involved. 235 Nonetheless, Ning et al. used extrusion-based printing to fabricate cell-dense, rat SC-laden tissue constructs, using an RGD-modified alginate, fibrinogen, and hyaluronic acid bioink. 228 Cell-laden scaffolds printed at 6 mm/s by a steel needle with 200 μm internal diameter were associated with ∼90% SC survival rates on day 10 post printing. Further, the study demonstrated the feasibility of bioprinting speed in altering rat SC alignment within the scaffolds to replicate their native linearly arrayed end-to-end orientation in peripheral nerves, necessary for achieving nerve regeneration (Fig. 9I).

3D bioprinting a multiscale modular bioink for peripheral nerve tissue engineering (Adapted from Chen et al.
223
).
Inkjet bioprinting
Inkjet or drop-on-demand bioprinting involves ejecting controlled volumes of hydrogel ink to predefined locations on a receiving substrate. Ink droplets can be created by either thermal or piezoelectric approaches. 236 In thermal-based inkjet systems, heat is used to nucleate an air bubble in the print head or nozzle that provides pressure pulses to eject ink droplets of varying sizes of ink drops. Typically, the volume of the drop ranges between 10 and 150 pL and is dependent on several factors, including applied temperature gradient, viscosity of the ink, and frequency of current pulse. On the contrary, piezoelectric-based systems rely on the generation of acoustic waves using polycrystalline ceramic actuators. The acoustic wave creates transient pressure that disrupts the bioink at regular intervals. Inkjet bioprinting is capable of producing high-resolution scaffolds (50 μm) with rapid printing speeds, affordable setups, and acceptable cell viabilities (up to 90%). However, the technique is limited to low-viscosity materials and does not achieve high densities. 237
Laser-assisted bioprinting
Laser-assisted bioprinting (LAB) is a printing technique that is typically nozzle-free. The technique is broadly divided into laser-induced forward transfer (LIFT) and laser-guided direct writing. LIFT is the most prevalent form of LAB. Essentially, the technique uses a pulsed laser beam, focused on an absorbing layer called the donor film, which is composed of a layer of cell-encapsulating bioink. The incident laser pulse increases the pressure of the bioink by generating sufficient energy that propels hydrogel droplets from the donor film onto a support stage. 238 The fallen bioink is then immediately crosslinked. Unlike other biofabrication technologies, LAB has unique advantages. First, the technique is a non-contact printing, thereby eliminating potential sources of contamination. In addition, highly viscous materials, up to 300 mPa/s, can be employed and the technique results in satisfactory cell viabilities (up to 85%). 237 Moreover, LAB is also capable of producing cell-level resolution (10 μm) by using rapid printing speeds. 239 Despite these benefits, LAB is associated with high system costs, and laser energy could result in increased cell fatalities. 217 For these reasons, LAB has not been investigated extensively for biofabrication applications and, to date, this technique has not been explored in printing peripheral nervous tissue.
Scaffold-free (cellular) bioprinting
To address the challenges related to unpredictable biodegradation and cytotoxicity of biomaterial-based 3DP, cellular or scaffold-free biofabrication is a viable alternative. 240 The rationale for this “bottom-up” method is based on the premise that replacement tissues and organs can be printed solely by using autologous cells. Taking inspiration from the embryonic organogenesis process guiding self-assembly of resident cells, scaffold-free bioprinting strategies depend on the juxtacrine signaling of cells for ECM secretion to generate patient-derived 3D tissue constructs for clinical applications. The approach is cell-friendly and typically generates macroscale tissues with high cell densities and long-term viability by printing spheroidal aggregates. Compared with their classical scaffold-dependent counterpart, cells are not exposed to xenogenic materials or harsh processing parameters, including shear stresses, UV, or chemical crosslinkers that compromise their resultant viability. 241 Further, cellular bioprinting fosters intercellular interactions of both homotypic and heterotypic nature, to guide the process of cell maturation and tissue morphogenesis.
Spheroids are typically formed by culturing cell lines under non-adhesive conditions, where they cluster to generate cellular aggregates.242,243 Although they could arguably be classified as bioinks, spheroids constitute the basic building blocks of bioprinted tissues in a biomaterial-independent approach. The dynamic 3D spheroids comprise multicellular organizations, facilitating the complex interplay between cell–cell and cell–ECM interactions, resembling native tissue architecture, which is impossible to achieve by using 2D monolayer cultures. Moreover, spheroidal stem cell cultures express pluripotency markers such as Oct-4 and Nanog, and they secrete higher levels of proangiogenic factors and signaling cytokines that promote cellular processes and viability compared with monolayer cultures. 244 Different approaches have been utilized to generate such 3D tissue spheroids in vitro; using hanging drop, 245 spinner culture, 246 rotating wall vessel, 247 microfluidic culture, 248 pellet culture, 249 and liquid overlay techniques. 250 Recently, fabrication of biomimetic nerve bioconduits using 3DP of spheroids has become increasingly popular.
Spheroidal aggregates are frequently assembled by using the famous “Kenzan” technique (Fig. 10II), using an automated printing strategy, which has so far been applied to bioassembly of blood vessels, 251 trachea, 252 cardiac patches, 253 and nerve conduits 254 (5 in Fig. 10II). The approach relies on cellular organization on stainless steel microneedles at micron-level precision that provides a temporary bolster to allow maturation and fusion of spheroids, instead of the hydrogel systems. 242 Preformed spheroids are robotically aligned on micro-needles by predefined CAD models using a commercial platform, Regenova® (Cyfuse, Tokyo, Japan). Needle arrays can be available in square (9 × 9 and 26 × 26 needles) and circular formats. After placement of the 3D spheroids in the micro-needles, they are incubated in a perfusion bioreactor system for allowing cell maturation to form macroscale tissues. Once the cellular tubes “conduits” are mechanically stable, they are then detached and become available for implantation. In Table 8 given next, we have highlighted some recent research within the domain of nerve bioconduit fabrication by employing Kenzan technique. In spite of the several advantages associated with the Regenova system, the tubular nerve conduits generated so far were simple, lacking some of the key features of the fascicle tracts. Nevertheless, pilot studies on neural regeneration conducted in vivo using these nerve bioconduits have provided meaningful results. However, their application in critical-sized gaps (e.g., >15 mm in rats) needs to be further explored for evaluating their clinical potential in long gap nerve regeneration in humans.

Scaffold-free bioprinting of nerve 3D bio conduits.
Scaffold-Free (Cellular) Bioprinting of Nerve Three-Dimensional Bio Conduits and In Vivo Testing
BM-MSCs, bone marrow derived mesenchymal stem cells; GMSCs, gingival mesenchymal stem cells; MNCV, mean nerve conduction velocity.
Reproduced from Taniguchi et al. 252
Another extrusion-based bioprinting technique for developing functional nerve grafts utilizing the principles of spheroidal assembly is NovoGen MMX Bioprinter™ (Organovo). 259 The bioprinter is equipped with dual dispensers: The first one is used for printing the cellular material by using predefined user settings, and the other concurrently prints an inert sacrificial hydrogel such as agarose or alginate to act as a temporary support (Fig. 10I.A–I.E). Similar to the Kenzan technique, tissue spheroids are then allowed to fuse together to attain structural integrity before the fugitive gel can be removed later. As a proof of concept, Owens et al. fabricated a multi-luminal nerve graft composed of an outer ring of bone marrow-derived mesenchymal stem cells (BM-MSCs) that circumscribed an inner core of alternating multicellular cylinders (90% of bone marrow-derived mesenchymal stem cells and 10% SCs) and agarose rods. 258 The whole structure was supported by agarose rods on the exterior, which were removed afterward following self-assembly of the spheroids to form three internal channels mimicking the nerve fascicles (Fig. 10I.G). Interestingly, the fully cellular nerve graft was able to perform on par with the nerve autograft when evaluated in an in vivo model of nerve gap.
Despite the merits of spheroid-based bioprinting, the approach has several limitations. Essentially, 3D cell culture techniques are expensive, labor-intensive, time-consuming, and require extensive experimental experience. This could potentially be associated with enormous manufacturing overheads when considering scaling up this technology for clinical translation. Although the procedure generates superdense cellular aggregates, spheroid 3DP poses technical challenges, as they are prone to premature aggregation that could easily clog the nozzle tip. Further, the biomechanical performance of spheroids is less predictable compared with using predetermined materials such as hydrogels. Poor and inconsistent ECM production could yield unstable structures that are not feasible for clinical implantation. 241 It is also critical to maintain the size of cell aggregates for scaffold-free bioprinting. Spheroids with diameters exceeding 400–500 μm are vulnerable to hypoxia of the central core, due to mass transport limitations, leading to ischemic cell necrosis. 260
For these reasons, proponents of scaffold-based bioprinting argue that this method offers greater versatility in terms of bioink composition and enables the fabrication of more complex structures mimicking native ECM. In addition, hydrogel-based bioinks can be printed by using various techniques and cross-linked via multiple physical and chemical interactions; therefore, the mechanical properties of the bioprinted construct can be tuned to match that of the desired tissue. In addition, the incorporation of polymers with pendant chemical groups bestows multi-functionality to the scaffold, which could allow the conjugation of neurotrophic factors and establishing gradients of guidance cues that might help directing the growth cone of regenerating axons.
Challenges of AM Processes in Peripheral Nerve Engineering and Potential Solutions
As the research field of nerve repair is currently trending toward personalized nerve guides and tissue constructs, it is of paramount importance to identify the major potential roadblocks facing this technology and coin effective solutions that could be instrumental in overcoming these obstacles.
Patient-specific nerve CAD modeling
Non-invasive conventional imaging such as the CT scan and MRI have been indispensable in the 3DP of complex anatomical models and fabrication of customized cell-laden scaffolds for repairing body tissue, including cartilage or bone defects.261,262 Unfortunately, these modalities along with contemporary clinical neuroimaging systems, including MRN, are far from optimal in delineating intraneural structures and fascicular orientation with high resolution. This makes generating patient-specific 3D nerve CAD models for biofabrication extremely challenging. Compared with the aforementioned tissues, the peripheral nerve anatomy is relatively intricate due to, primarily, the heterogeneity in fascicular topography throughout the nerve pathway, and, second, the presence of bifurcations and undulations along the anatomical course of the nerve.263,264 Therefore, there is a need for more advanced imaging platforms and protocols that could allow the complexity of the fascicular anatomy to be appreciated. This is critical for reconstructing personalized biomimetic nerve pathways that are anticipated to significantly enhance neural regeneration over longer gaps.
Ideally, an optimal nerve scanner should be capable of mapping the individual fascicle bundles up to the endoneurial tubes and accurately delimiting the normally occurring fascicular splitting and merging. 265 Moreover, in the context of PNIs, a reliable imaging protocol should involve the in situ scanning of the proximal and distal severed nerve stumps followed by extrapolating the lost segment to match the original nerve structure. Alternatively, a digital library of peripheral nerve scans could be constructed from cadaveric donors or individuals with various demographic backgrounds that would assist in the 3D modeling of a nerve graft homologous to the nerve of interest. Another more realistic and technically feasible option to pursue could also involve scanning the contralateral unaffected nerve of the same patient to aid in 3D modeling of the lost nerve segment in the affected limb. 266 In this regard, emerging imaging methods have been applied to reverse engineer the native fascicular pathway such as microfocus computed tomography (micro-CT) and micro-MRI. These tools might represent promising solutions that could capture the internal morphological details of the peripheral nerve with high fidelity.
Micro-CT is a powerful sub-micron scanning modality that can generate very high-resolution 3D images, with voxel sizes in the micrometer range, which could be useful in designing more anatomically precise nerve CAD models for biofabrication. 267 In addition, nanotomography, the most recent innovation in micro-CT-based platforms yet to be applied in 3DP, could open new frontiers for 3D nanoprinting and expand resolution limits. 268 Although micro-CT has now well-established applications in analyzing the microstructure of mineralized tissues and morphologic characterization of engineered scaffolds, it is not widely utilized in the evaluation of soft tissues, including peripheral nerves due to their inherently low X-ray attenuation coefficients.269–271 Nevertheless, iodine staining and freeze-drying have been used as viable solutions to enhance the contrast of peripheral nerves and allow for the 3D reconstruction of the intraneural fascicular topography.271,272 As a proof of concept, Zhu et al. successfully scanned lyophilized decellularized human nerve allografts by using micro-CT and produced high-resolution images of the nerve microstructure with visualization of the distinctive connective tissue layers, including the endoneurial tubes. 273 Moreover, the authors demonstrated the feasibility of 3DP a nerve model with visibly delineated fascicles by using 2D scans of the freeze-dried nerve sample. Despite the advantages of micro-CT, the higher resolution of tissues is currently achievable by using ex vivo imaging systems. 274
Another soft tissue-sensitive imaging is the micro-MRI that has been investigated by Yao et al. to 3D reconstruct nerve fascicles of the lower extremity nerves with high resolution (50 μm). 275 Using the database generated from the 3D reconstruction of nerve scans, 3D models clearly delineating the individual nerve fascicles of the tibial, common peroneal, and sciatic nerves could be designed with high accuracy (Fig. 11I–III). In contrast with micro-CT, micro-MRI lacks exhaustive sample preparation and samples can be recycled for use in later experiments, which makes it a more convenient non-destructive tool. Despite the enormous leap created by these innovative imaging technologies in the study of fascicular microstructure, both techniques are limited by their inability to perform in situ scanning of peripheral nerves. This ex vivo imaging nature makes the practicality of these scanning methods from the clinical perspective questionable. Another drawback of high-resolution microscale imaging is the laborious segmentation and time-consuming 3D reconstruction of multiple scans, which could limit the length of the nerve scanned.

3D reconstruction of the lower limb nerve fascicles using micro-MRI imaging (Reproduced from Yao et al.
275
).
Peripheral nerve biofabrication hurdles
The biofabrication of a fully functional nerve graft is at a primordial stage, and several milestones need to be achieved for clinical intervention. Constraints in the manufacturing technology, bioink material properties, and postprocessing maturation of the viable, printed tissue are among some of the most critical factors limiting the biofabrication of centimeter-scale constructs. 235 The layer-by-layer stacking technique of AM biofabrication methods is generally associated with relatively extended processing times. 276 Due to this, cells are left outside optimal culture conditions for prolonged durations, thereby inducing cellular stress and jeopardizing the viability of the encapsulated biologics. Moreover, the time of fabrication could also extend if single-cell resolution and inherently low-throughput technologies such as micro-stereolithography or two-photon polymerization (2PP) are opted for bioprinting human-scale nerve grafts. 277 Thus, it might be difficult to ensure the viability of bioprinted cells with the application of these processes. Eventually, the production of clinically relevant graft constructs would likely involve advanced bioprinting platforms that merge different modalities to leverage their advantages and simplify parts of the biofabrication protocol.
Another formidable challenge, especially in extrusion-based methods, is the fidelity of the 3D bioprinted constructs. The 3D neural scaffolds and nerve bioconduits fabricated to date are rather simple in design and far away from the desirable level of architectural complexity of nerve biomimicry. High-resolution scaffolds are prerequisite to satisfy the overall aim of biofabrication in achieving nerve biomimicry. In addition, they would facilitate elucidating the influence of micro-topography on cellular behavior and functions such as survival, differentiation, and migration.278,279 Compared with the printing of hard polymers, hydrogel-based bioinks mainly employed in biofabrication have limited the spatial resolution of the printed living tissue because they are prone to structural collapse and spreading postprinting. Apart from the narrow choice of materials, other factors that could also influence the resolution of the 3D bioprinted structure include bioink physicochemical properties and composition, technical features of the bioprinter system, for example, nozzle size, printing speed, etc., and crosslinking mechanisms. Thus, it is imperative to mention that manipulating one of these printing parameters to achieve a higher resolution could compromise another critical feature, which makes the process of optimization a challenging task. For instance, using a larger gauge needle might yield structures with high resolution, in turn compromising the cell viability. 280 Recently, volumetric bioprinting (VBP) has emerged that permits rapid fabrication, typically within a time frame of seconds, of clinically relevant 3D structures with preserved cell viabilities. Briefly, VBP uses cytocompatible visible laser light to cast multiple differential 2D projections onto a photocurable cell-laden resin to generate complex patient-specific biomimetic architectures with high resolution. 276 This technological advancement could open new frontiers in nerve biofabrication.
Another fundamental obstacle for the scaling-up of bioprinted tissues is mass transfer limitations. Vascularization of a bioprinted nerve graft is crucial for functionality of cells and axons, as it ensures the timely delivery of nutrients and oxygen and removal of metabolic waste products, thereby maintaining the longevity of the product. Current technology fails to maintain adequate mass transport conditions that are protective against hypoxic necrosis of cells in the inner core of the engineered tissues, and it is unable to replicate the hierarchical intraneural vascular plexus spanning arteries and veins down to capillaries. Thus, a logical future target to aim for in the scaffold-based bioprinting of peripheral nerves would involve simultaneously integrating interconnected vasculature. However, this task might be challenging considering the differential culture media requirements of the nerves and the vasculature. Further experiments need to be conducted to assess co-culturing conditions of these tissues simultaneously. 281
Several approaches have been investigated to bioprint tissues embedding synthetic vasculature, including the use of microfluidics and indirect bioprinting of fugitive bioinks, which can be thermally de-crosslinked leaving behind perfusable microchannels that can be infused later with vascular endothelial cells.282–284 Using these techniques, several groups have printed hollow vascular structures, diameters ranging from micro- to milli-meter scale, with the inner wall incorporated with endothelial cells.282,283 However, generating vasculature on a smaller scale to produce anatomically relevant dimensions demands fine tuning several aspects of the printing process, including resolution, nozzle diameter, and mechanical properties of the material and bioink to build free-standing hollow structures, among others. 281 Another caveat here is that the design of a bioprinted intrinsic vascular network should ensure its connection to a larger feeding vessel that can be anastomosed to the recipient vasculature; thus, graft perfusion can be resumed once the engineered nerve is implanted in the patient. 235
Further, most of the research attempts in biofabrication involve the use of a single material bioink to print cell-laden structures. This, however, does not accurately emulate the complex structural heterogeneity and composition of living tissues, including peripheral nerves. In the future, advances in multi-material and multi-cell bioprinting could help address the complexity of nerve engineering where a single representative biofabrication session would typically involve the use of sacrificial bioinks for vascularization, multiple tissue bioinks, and scaffolding polymers to generate heterocellular structures integrating intricate perfusable vascular networks with peripheral cellular networks.285,286
Regulatory, ethical, and cost concerns of personalized nerve repair solutions
Country-specific regulatory bodies have different rulings on additively manufactured medical products.287–289 Even though the FDA has set guidelines for the bulk manufacturing (mass production) of medical devices or drugs using 3DP, clear regulatory frameworks or specific legislative guidance pertaining to the AM of personalized therapeutics largely remain unaddressed. Robust and lucid regulatory measures to ensure CGMP (Current Good Manufacturing Practice) standards are integral to maintaining quality control and avoiding faulty products that could impair the healing process in patients. The AM processes are also associated with unclear legalities that need to be addressed. The fabrication of custom-made devices or biological tissues will require individual patient data at one stage, which might require the patient's data to be included in the care plan. 287 Besides, intellectual property disputes and privacy concerns may arise since the ownership of medical scans, CAD model design, and final printed products are not yet known. Without identifying proprietary rights, it might become problematic to determine the individual's responsibility for any serious harm that occurs in the patient and legally challenges the culprit. 290
Although biofabrication is a subtype of AM, more sophisticated regulatory considerations are associated with 3D bioprinting compared with non-biological printing. Biofabrication intersects with the fields of cell therapy and stem cell research, therefore the inherent risks and translational hurdles of those disciplines will pass over to 3D bioprinting. In addition, several factors will require evaluation, including the effect of the manufacturing process on cell viability and function and postprinting integrity of the biological product. Moreover, devising appropriate testing and techniques to ensure the maintenance of aseptic printed parts will be necessary. The consistency of the printing process will also need careful assessment. Parameters such as the cell distribution, construct dimensions, and mechanical and physicochemical properties could potentially help in evaluating the reliability of the biofabrication technique. 291 Eventually, researchers will need to integrate nondestructive in-line quality-control systems in AM processes to ensure that the aforementioned quality attributes of the biomanufactured clinical products are well defined, characterized, and conform to regulatory standards. 292 Taking these factors into account, a longer translational time frame is anticipated, before a bioprinted nerve graft is fabricated in contrast with 3D-printed nerve guides. Ultimately, as research on nerve graft biofabrication and 3DP continues to surge, policymakers in regulatory bodies, such as FDA, need to articulate more effective validation tools and tailored legislation in a commensurate pace.
Moreover, as therapies become more individualized, the reliability of clinical outcomes might be undermined due to difficulties in standardization of the study design. In addition, the personalized nature of biofabrication raises ethical dilemmas on the clinical testing of these patient-specific products in otherwise normal human subjects. It is certainly unethical and of questionable clinical value to prove the safety and efficacy of 3D bioprinted organs constructed from the cells of a specific patient with unique pathology in disease-free individuals. At the end, the aim of AM is to tailor treatment to individuals and not to develop a universal technology that can be tested on other groups. 293 Thus, there is a need to develop new models to test the effectiveness and safety of personalized regenerative medicine therapies; otherwise, the patient will serve as his/her test subject, which is ethically controversial.
In the future, it might be also crucial to evaluate the process of the 3D fabrication of nerve grafts from an economical standpoint. Nerve conduits currently available in the market are expensive, with some exceeding the $1000 unit price and their functional outcomes still remain controversial. 294 Given the long chain of production of any custom-made bioprinted nerve graft, the technology will definitely be associated with exorbitant manufacture costs and high-priced solutions, which could limit the accessibility of financially disadvantaged patients to these novel treatments leading to what has been referred to as the “social stratification of bioprinting.” 208 Therefore, conducting a cost–benefit analysis will be imperative in the future in such scenarios to weigh the benefits of such technologically and economically demanding innovation against the cost. A bioprinted nerve graft that could fully mitigate the debilitating functional deficits in those diagnosed with intractable PNIs, restore the patient's productivity, and offer equal access to treatment would prove itself as a worthwhile investment.
Conclusion
Repair of nerve injuries remains a surgical challenge. Despite the advances in microsurgical techniques and nerve substitutes, failure rates are high with suboptimal nerve regeneration outcomes. There is an unmet demand for a fully functional 3D engineered nerve graft that can recapitulate the native nerve microstructure, and allow for patient-specific fascicle-to-fascicle regeneration. Apparently, optimizing the design of commercially available nerve surrogates or supplementing them with patient cells appears a pragmatic solution to enhance nerve regeneration over long gaps in the shorter timeframe. However, they do not offer personalized therapies, and might not achieve the expected functional recovery as a result of the ineluctable fascicular mismatch. Automated fabrication methods such as 3DP are speculated to create a paradigm shift in the field of peripheral nerve surgery. Essentially, they offer spatial control over the deposition of materials and biologics, and thus could allow the creation of a biomimetic fascicle pathway relevant to the patient's anatomy. Although replicating the intraneural microstructure might not be a conceivable goal with the present technology, several milestones must be accomplished to prevent this research field from stagnation and accelerate the reaping of attainable gains. These include, but are not limited to, utilizing high-resolution imaging and developing 3D scanning protocols for patient-specific nerve modeling, incorporating interconnected vascular networks within bioprinted scaffolds, developing more versatile multi-functional bioinks for nerve biofabrication, and validating regulatory paths for the translation of additively manufactured nerve grafts.
Footnotes
Authors' Contributions
O.A.S.: conceptualization, visualization, methodology, investigation, formal analysis, software, writing-original draft preparation, writing-review, and editing. S.L.: writing-review and editing. S.M.: writing-review and editing, supervision. D.M.K.: writing-review and editing, supervision, and project administration. A.M.: writing-review and editing, supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding source to disclose.