
Abstract
Tissue engineering (TE) was introduced almost 30 years ago as a potential technique for regenerating human tissues. However, despite promising laboratory findings, the complexity of the human body, scientific hurdles, and lack of persistent long-term funding still hamper its translation toward clinical applications. In this report, we compile an inventory of clinically applied TE medical products relevant to surgery. A review of the literature, including articles published within the period from 1991 to 2020, was performed according to the PRISMA protocol, using databanks PubMed, Cochrane Library, Web of Science, and Clinicaltrials.gov. We identified 1039 full-length articles as eligible; owing to the scarcity of clinical, randomized, controlled trials and case studies, we extended our search toward a broad surgical spectrum. Forty articles involved clinical TE studies. Among these, seven were related to TE protocols for cartilage applied in the reconstruction of nose, ear, and trachea. Nine articles reported TE protocols for articular cartilage, nine for urological purposes, seven described TE strategies for cardiovascular aims, and eight for dermal applications. However, only two clinical studies reported on three-dimensional (3D) and functional long-lasting TE constructs. The concept of generating 3D TE constructs and organs based on autologous molecules and cells is intriguing and promising. The first translational tissue-engineered products and techniques have been clinically implemented. However, despite the 30 years of research and development in this field, TE is still in its clinical infancy. Multiple experimental, ethical, budgetary, and regulatory difficulties hinder its rapid translation. Nevertheless, the first clinical applications show great promise and indicate that the translation toward clinical medical implementation has finally started.
Impact statement
The clinical use of a tissue-engineered windpipe in compassionate patients elicited euphoria in the media between 2010 and 2016: tissue engineering (TE) had proven to be no longer a fictional concept but a life-saving reality. However, most of the treated patients died, and the surgeon was convicted for scientific misconduct and aggravated assault. As of 2020, the authors had eight of their articles retracted and two received an expression of concern.1 These events have fueled skepticism among clinicians about TE: science or fiction?
Although TE is full of promises, it is not realistic yet to engineer a (vascularized) construct that thrives in a “hostile” clinical environment. Therefore, a realistic update of the current clinical outcomes and the promises of TE in human trials are essential.
Introduction
Langer and Vacanti define tissue engineering (TE) as “an interdisciplinary field that applies the principles of engineering and life sciences towards the development of biological substitutes that restore, maintain, or improve tissue function or a whole organ.” 2 As proof of principle, Vacanti et al. grafted a human auricle-shaped polymer-cell construct onto the back of a mouse in 1991. 3 They introduced TE into animal experiments using chondrocytes from newborn calf joints seeded on a synthetic scaffold for culture. 4 After these were cultured, the construct with cultured cells was implanted subcutaneously in nude mice. Their work demonstrated the fascinating possibility of creating new autologous cartilage on a synthetic scaffold in an animal model and marked the onset of the field of “TE.”
Subsequently, considerable efforts have been expended to implement TE in clinical practice. TE refers to methods used to synthesize tissue substitutes created with a matrix populated by autologous cells and their subsequent implantation in vivo. To provide this matrix, one can synthesize allogeneic tissue and perform an extensive decellularization process that results in an acellular matrix, which is then recellularized with autologous cells, commonly referred to as the “decell–recell” concept. 5 Alternatively, a matrix can be fabricated with synthetic or biological materials, which can then be seeded with autologous cells.
As documented by the number of hits that appear on the term “TE” in PubMed, interest has grown tremendously since the 1990s. 6 However, three decades since the first report of Vacanti et al., 3 clinical studies are very scarce and do not yet meet the expectations set 30 years ago. For tissues that do not need intrinsic vascularization, such as bone and articular cartilage, stability against clinical forces—traction, friction, and pressure—is mandatory, whereas for elastic cartilage flexibility and shape are essential. For tissues that require revascularization, the regeneration of neovascular networks within a three-dimensional (3D) matrix to distribute oxygen and other nutrients within the TE device is the major hurdle. It is very challenging to rebuild the capillary network within the TE organ. Preclinical models have shown that implanted TE construct get nutrients originally from tissue fluid permeation and secondarily from neovascularization originated from enclosed tissue. The center area of the TE construct experiences ischemia at the beginning of transplantation. Therefore, it is possible that a main part of the seeded cells would not survive and participates in degradation of the construct. In a clinical surgical setting, we can alter vascularization by prefabrication and prelamination strategies, which may lead to hybrid “ex vivo” approaches using principles of cell engineering and growth factor therapy,7–9 decellularization of scaffolds, and microvascular surgery.10–12 If intrinsically vascularized tissues do not rapidly receive a source of vascularization tissue necrosis occurs in a clinical setting.13,14
This review focuses on all clinical studies currently conducted with tissue engineered medical products in a clinical setting.
Methods
Data search protocol
In accordance with the PRISMA guidelines, a systematic search was performed using PubMed, Cochrane Library, Web of Science, and Clinicaltrials.gov to identify pilot clinical studies and reports from compassionate-use programs published since the first trial conducted by Vacanti on August 1, 1991 until the end date of the search in August 2020.
The Patient, Intervention, Comparison, Outcome (PICO) question was stated as: ((“Clinical Trial” [Publication Type] OR clinical-trial[tiab] OR intervention-study[tiab] OR “Clinical Study” [Publication Type] OR Clinical-study[tiab] OR “Clinical Trial, Veterinary” [Publication Type] OR ((“Patients”[Mesh] OR Patient[tiab] OR large-animal*[tiab] OR “Sheep”[Mesh] OR sheep[tiab] OR ovis[tiab] OR “Goats”[Mesh] OR goat*[tiab] OR “Swine”[Mesh] OR swine[tiab] OR porcine[tiab] OR pig[tiab] OR pigs[tiab] OR “Cattle”[Mesh] OR cattle[tiab] OR cow[tiab] OR bovine-animal[tiab] OR “Horses”[Mesh] OR horse*[tiab] OR equine-animal[tiab] OR “Dogs”[Mesh] OR dog[tiab] OR dogs[tiab] OR “Rabbits”[Mesh] OR rabbit*[tiab]) AND in-vivo[tiab] OR implant*[tiab]))) AND (“Tissue Engineering”[Mesh] OR tissue-engineer* [tiab] OR recell*[tiab]).
Endnote X9® (Clarivate Analytics, Philadelphia, PA) was used as reference manager. The selection of articles was conducted by two independent reviewers. Reference lists of included articles were hand-searched for possibly suitable articles. Inter-examiner conflicts were dissolved by discussion until a definitive list of eligible articles was composed.
Eligibility criteria
Studies meeting the following predefined criteria were included: (1) clinical trials in humans including randomized clinical trials, cohort studies, case–control studies, cross-sectional studies, and case series; (2) full text available in the English language; (3) TE 15 (macroscopic scaffold seeded with autologous cultured cells) was the main subject; (4) study subjects were patients treated with TE constructs; (5) studies published within the period from August 1, 1991 to August 1, 2020. Following criteria were used for exclusion from current review: (1) full-text not available; (2) non-English text; (3) in vitro studies; (4) systematic reviews, meta-analyses, and commentaries; and (5) studies on acellular grafts and with cellular implants without any graft or scaffold.
Data collection
Data extraction of included articles followed. These were analyzed and reported using MS Office Excel 2016. The data recorded were first author, year, study type, number of included patients, treatment technique, treatment materials, follow-up time, and outcomes. No statistical analysis was conducted, owing to the broad array of parameters.
Results
The complete full-search strategy is schematically summarized in Figure 1.

PRISMA flow diagram. PRISMA flow diagram used for scoping review. *Additional sources found by hand searching key journals for the topic of tissue engineering and searching table of contents, as well as reviewing reference lists form our selected articles and citing articles. Color images are available online.
This review referenced a total of 40 studies with different study characteristics and designs. Clinical studies in which TE was used for plastic reconstructive purposes were considered the most relevant (seven studies; Table 1). These studies covered the reconstruction of nose, ear, and tracheal cartilage with TE substitutes. Nine studies reporting articular cartilage TE were subjected to full-text screening and were reviewed in this survey (Table 2). Nine clinical studies reported the treatment of urological defects with TE (Table 3), seven clinical studies described cardiovascular TE (Table 4), and eight clinical studies focused on treatment of mucosal defects (Table 5).
Status of Clinical Translation of Tissue Engineering in Plastic Reconstructive Surgery
The in vitro cell-scaffold 3D culture.
BM-MNC, bone marrow–mononuclear cell; Y, years; M, months; W, weeks; D, days; pt, patients; FU, follow-up; hrEPO, human recombinant erythropoietin; TGF-β1, transforming growth factor β1; G-CSF, granulocyte colony-stimulating factor; MSC, mesenchymal stem cell; PRP, platelet-rich plasma; BMSC, bone marrow stem cell; P, passage; n.m., not mentioned; PLLA, poly
A Glance of Clinical Studies Using Tissue-Engineered Constructs for Articular Cartilage Reconstruction
The in vitro cell-scaffold 3D culture.
ACI, autologous chondrocyte implantation; MACT, matrix-associated chondrocyte transplantation; Y, years; M, months; FU, follow-up; n.m., not mentioned; pt, patients; RCT, randomized controlled trial.
Status of Translational Investigation in Urology Tissue Engineering
The in vitro cell-scaffold 3D culture.
Y, years; M, months; W, weeks; D, days; FU, follow-up; pt, patients; SMC, smooth muscle cells.
Status of Translational Investigation in Cardiovascular Tissue Engineering
The in vitro cell-scaffold 3D culture.
Y, years; M, months; W, weeks; D, days; FU, follow–up; pt, patients.
Status of Translational Investigation in Tissue-Engineered Skin and Mucosa
The in vitro cell-scaffold 3D culture.
Y, years; M, months; W, weeks; D, days; FU, follow-up; n.m., not mentioned; pt, patients.
Discussion
There are four essential elements of any TE approach to reconstruct a tissue or organ: a matrix, a cell source, mechanical and biochemical signals that enable new tissue formation, and for most of the tissues also the identification of a source for blood supply. The design protocols used to incorporate these four elements differ considerably in different organs and have to be adapted to specifically to the organ that is being replicated.
In addition, the standard TE technique has two distinct phases in a clinical setting: in vitro cultivation of 3D cell scaffolds, and the in vivo development and integration of the tissue-engineered medical construct in the real-time clinical wound environment.
Most translational advances of tissue-engineered medical products were reported in the reconstruction of elastic cartilage in reconstruction protocols of nose, ear, and trachea followed by studies with tissue-engineered articular cartilage. Clinical tissue-engineered constructs were also reported for the treatment of urological defects, cardiovascular defects, and mucosal defects.
Clinical Use of TE Elastic Cartilage
There is a substantial difference between the morphology and requirements of elastic and articular cartilage. 16 Large laboratory animal studies reporting tissue-engineered cartilage constructs were critically analyzed, and promising and challenging outcomes were identified (Table 6). TE constructs undergo degeneration, inflammation, fibrosis, and foreign body reaction after implantation.17–22 Furthermore, a critical factor that hinders translation is the worsened vascularization of large structures that initiates necrosis and poor cell expansion. 23 Cartilage tissue itself is avascular but it is enclosed by well-developed vascular networks. Preclinical models have shown that implanted tissue-engineered constructs obtain their nutrients primarily by tissue fluid permeation and secondarily by neovascularization originating from the enclosed tissues.24–26 The central area of the construct experiences ischemia at the beginning of transplantation, which triggers revascularization. This process takes multiple weeks. Therefore, a substantial part of seeded cells may not survive and will participate instead in the degradation of the construct.
Status of Large Animal Studies in Plastic Reconstructive Tissue Engineering
The in vitro cell-scaffold 3D culture.
Y, years; M, months; W, weeks; D, days; H, hours; FU, follow-up; bFGF, basic fibroblast growth factor; P, passage; BMSC, bone marrow stem cell; PET/PU, polyethylene terephthalate/polyurethane.
Malformation or injury of the cartilages of the ear, nose, and trachea necessitate complex surgical reconstructions to rebuild absent cartilage and bony support. The use of autologous cartilage obtained from the rib, auricle, or nasal septum is the gold standard for reconstructing craniofacial cartilage defects owing to their lack of immunogenicity. 27 However, disadvantages such as limited availability of graft tissue, donor site morbidity, and variable tissue quality remain. Furthermore, the inability to implant cartilage with growth potential in neonates and small children poses another limitation. In addition, rib fibrocartilage differs from flexible elastic cartilage and is subject to aging calcification. 28 Cartilage reconstruction with alloplastic implants is universally available as an alternative to autologous grafts. 29 Because of the consistent pre-established shape and straightforward surgical implantation procedure, some researchers prefer this reconstruction approach. However, the possibility of infection, lack of biocompatibility, extrusion, and unknown long-term sustainability are significant drawbacks.
TE protocols for tracheal replacement
To achieve a durable functional restoration of long-segment tracheal defects, a tissue-engineered substitute needs to have (1) extensive cartilage regeneration capability to prevent airway collapse, (2) stability, (3) effective prevascularization capacity to support cartilage viability and epithelialization, and (4) a functional epithelium to avoid infections and granulated hyperplasia. In contrast to other tissues, the purpose of TE for trachea is not to enhance malfunctioned tissue, but to replace a vital organ to save function and life.
In 2010, a 10-year-old boy with congenital tracheal stenosis and aorto-tracheal fistula received a tissue-engineered tracheal replacement. 30 Because of the urgent nature of the condition, the multidisciplinary team had to perform a direct protocol for the development of the construct. The epithelium was fully restored after 1 year. The question that arose was whether this epithelialization was induced by the epithelial patches or whether it originated from nearby healthy tissue. A 4-year follow-up report declared the good health of the boy. In decellularized tracheas, the reepithelialization process is extensive to preserve the construct and to save the graft from the fibroproliferative reaction of the recipient. 31 Disadvantages of decellularized scaffolds are size matching, demanding decellularization processes, and the need for allogeneic tissues. Elliott et al. successfully implanted a cell-seeded decellularized homograft in a 15-year-old girl with critical tracheal stenosis under compassionate-use license.30,32 According to the hypothesis that seeding a neovessel would inhibit graft stenosis,33,34 they seeded the graft with bone marrow stem cells (BMSCs). The graft was maintained for 2 weeks. The early results were promising and increased exercise tolerance by the host until the abrupt tracheal obstruction of the posterior wall. The long-term follow-up of these patients is unclear. It seems they were eventually treated with endotracheal stents that prevented collapse of the airway.35,36 This knowledge is essential because the use of stents elicits a strong inflammatory response, which may be a cause of hypergranulation and hence obliteration and collapse.
Tan et al. 37 developed an in vivo bioreactor for connecting the tissue-engineered airway construct with the external environment through two Port-a-cath® catheters. For 1 month, the bioreactor was perfused by Ringer's gentamicin fluid to prevent infection, keep the preseeded cells alive, and allow reseeding of the scaffold with BMSCs. The authors observed the secretion of several angiogenic growth elements, which confirmed the migration of the reseeded cells to the tissue-engineered construct.
The mechanical alterations of the constructs after transplantation in human trials are very evident but were not observed in earlier pig models. 19 This indicates that human trials are essential to identify the limitations and strengths of a tissue-engineered construct, as animal models cannot fully emulate the complex pathological processes in humans. 19 Furthermore, patients in compassionate-use programs are not treated as study subjects, and thus allow only the most necessary procedures to be performed. Therefore, both trials with compassionate patients as well as relevant in vivo studies need to be combined to establish a clear-cut study protocol for clinical trials that meets regulatory requirements.
The long-term outcomes of this sequence of clinical trials revealed apparent drawbacks in the used techniques and require transparent research in relevant in vivo models before clinical translation. The main complication of a tissue-engineered trachea is graft stenosis, which poses a primary barrier to clinical translation. Especially for the trachea, it is imperative that the hollow convexity is stably maintained to facilitate efficient ventilation.
The most common difficulty associated with the application of autologous cartilage in the reconstruction of the trachea is the absence of respiratory epithelium and subsequent lack of mucociliary clearance that causes mucous stagnation, graft stenosis, and chondromalacia. 38 Moreover, as the inner respiratory ciliated epithelium of the windpipe is the first defence mechanism against aggressive particles present in air, a well-vascularized inner epithelial lining is essential in all reconstructive procedures. It is striking that none of the previous trials developed a prevascularized trachea, as sufficient blood supply is crucial for the survival of the tissue-engineered implant. These particular features of the windpipe make a TE approach quite complex.7,12,39
For tracheal substitution, two other elementary approaches have dominated the field: tracheal allotransplantation and aortic homograft transplantation (Fig. 2). The complex capillary-based blood supply in the trachea discourages regular allotransplantation because the trachea lacks a detectable vascular pedicle. This key issue prevents efficient tracheal transplantation. Furthermore, the substitute should offer elasticity with sufficient stiffness and long-term efficacy alongside biological integrity to avoid rejection, dehiscence of the anastomosis, and weakening. Trachea transplantations with cadaveric allografts and aortic homografts fail to meet these conditions and require high-dose immunosuppression to prevent acute graft rejection owing to the antigenically active cells in the airway mucosa.7,11 These challenges, together with the heterogeneous presentation of tracheal conditions, make the production of an adequate tracheal replacement very difficult. Potential solutions to the complications and limitations associated with the aforementioned approaches may be found with TE techniques:

Tracheal allotransplantation. Upper row: Trachea allotransplantation to restore a long-segment defect of the trachea. A donor trachea is prelaminated in the vascularized fascia of the forearm and allogenic mucosa is replaced with recipient autologous buccal mucosa. This creates a chimeric construct that consist of autologous cell lining within an allogenic cartilaginous framework. This chimera strategy generates a certain degree of “tolerance”. Microvascular transfer to the defect occurs in a second stage after weeks. Immunosuppression can be tapered and stopped after control bronchoscopy.9,10 Lower row: currently the authors investigate in a preclinical setup the cultivation of autologous respiratory cells and gentle decellularization techniques on the allogenic trachea to diminish immunogenicity even further and to induce faster reepithelialization and angiogenesis.11,41 Color images are available online.
Cell cultures of ciliated epithelium seeded in a porous cartilaginous matrix or a decellularized allogenic trachea and banked on vascularized fascia for transplantation after “prefabrication,” may lead in future to an authentic trachea construct.
TE protocols for replacement of nasal cartilage
Fulco et al. 40 pioneered the first human trial of TE reconstruction of the alar lobe and recommended a safe functional and esthetic replacement approach for native cartilage. In vitro fabricated extracellular matrix (ECM) with characteristics of mixed hyaline and fibrous cartilage was implanted in vivo. After 6 months, it transformed into a mixture of fibrous connective tissue with muscle fibers and fat cells similar to alar tissue. This change is attributable to the lack of environmental cues required for the preservation and progression of the cartilaginous phenotype and the availability of other cues for the conversion of the cartilage that corresponded to the tissue at the site where it had been placed.
Given that platelet-rich plasma (PRP) is biocompatible and contains several growth factors, such as transforming growth factor β1 (TGF-β1), fibroblast growth factor 2 (FGF-2), and insulin growth factor 1 (IGF-1), it is a propitious cell carrier for TE. Based on successful results in recently published reports, Gentile et al.41,42 created a cartilaginous construct made of nasal chondrocyte micrografts mixed with PRP for subcutaneous injection in the nasal dorsum for the nasal alar reconstruction in 11 patients. They combined PRP with chondrocyte micrografts to prevent rapid contraction and degradation in vivo. In our experience, PRP neither maintains shape nor volume and therefore cannot serve as a 3D matrix that guides cells into the desired shape. 9 However, it induces angiogenesis and promotes healing by proangiogenic growth factor release,43,44 and can be used for other purposes.
The exploratory first-in-human clinical trial of Hoshi et al.45,46 indicated that the application of autologous tissue-engineered cartilage with poly-
In contrast to the research conducted on other tissues, there is an insufficient number of high-quality reports concerning TE strategies in rhinology. Apart from these three human studies, there are no reports on nasal TE in large animals.
TE protocols for replacement of auricular cartilage
Thirty years after the landmark study of Vacanti et al., 3 the first clinical trial of a tissue-engineered ear implant was published. The bench-to-bedside study described by Zhou et al. 47 is a pilot clinical trial for the reconstruction of the human ear with a human ear-shaped cartilage engineered in vitro. At present, the longest follow-up period described in this trial is 2.5 years. This certainly is a landmark study. The authors used autologous chondrocytes obtained from the remains of the microtia ear cartilage of the patients as the seed cell source. They used a prolonged in vitro precultivation period to diminish the postimplantation inflammatory response. The investigators used computer-aided design and computer-aided manufacturing to generate a patient-specific poly-glycolic-PLA scaffold for cartilage seeding, with a polycaprolactone center to ensure the mechanical strength of the scaffold. The five patients are currently in follow-up.
Translational hurdles for clinical application of TE elastic cartilage
The ideal scaffold is a nonimmunogenic, long-lasting, biocompatible construct with growth potential. This construct ideally must be individualized for instance with the help of CAD-CAM and 3D printing, making it applicable for the morphological and structural requirements of the recipient (see Fig. 3). Both preclinical and clinical outcomes indicate the difficulty of this mission. Biosynthetic scaffolds were synthesized to overcome the inherent limitations of decellularized scaffolds: they are commercially available, easily adjustable, and physiologically neutral. However, biocompatibility, immune response, and an unknown long-term fate of the scaffold in cartilage TE still are substantial obstacles that require further research. 48
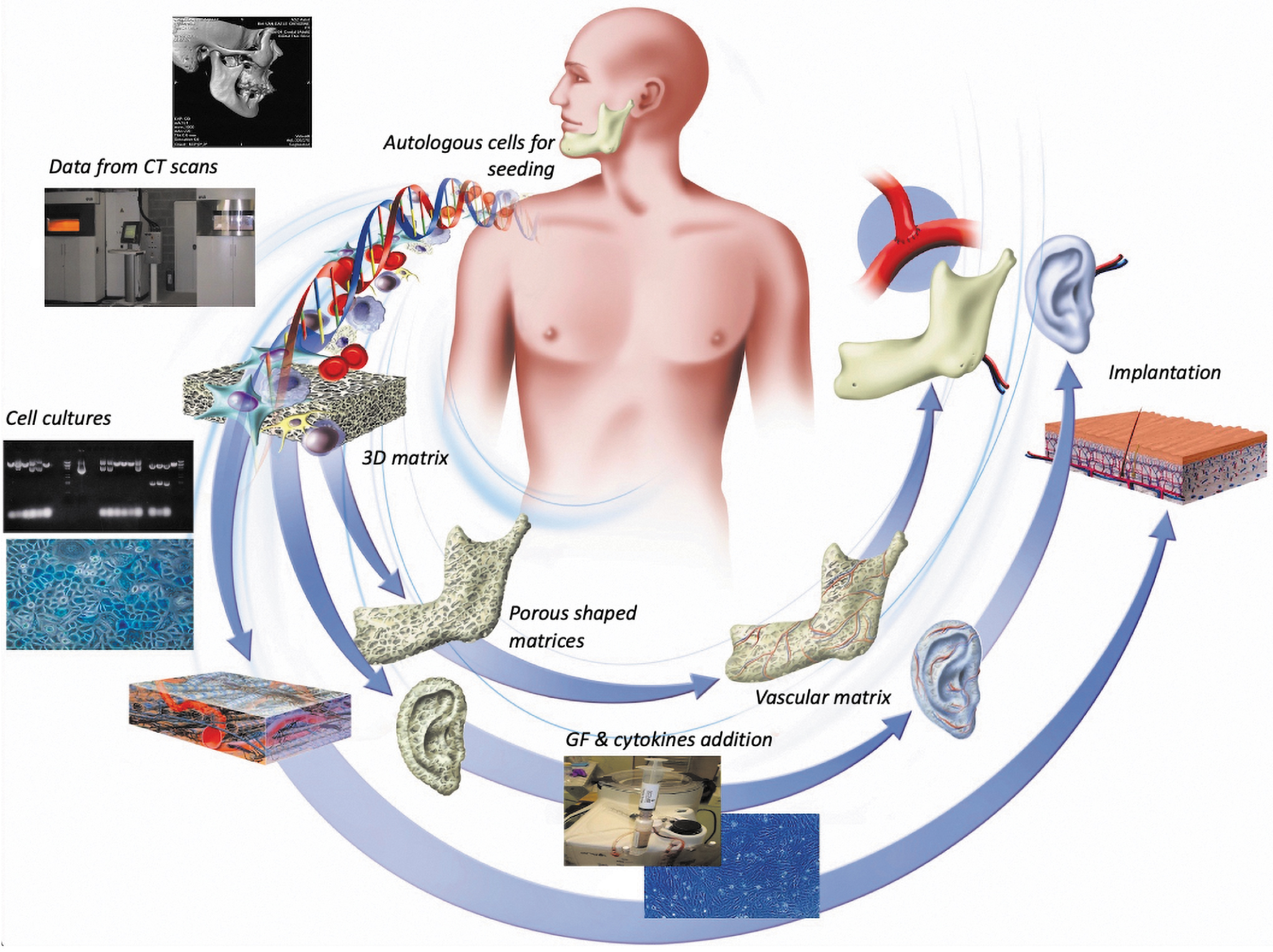
Clinical tissue engineering strategies. 1—(upper left) CT scan data of the required matrix are translated in DICOM format to a Virtual Surgical Planning software package where the required custom made matrix is designed. 2—After Computer-Aided Design (CAD), the 3D matrix subsequently is 3D printed by Computer-Aided Manufacturing. 3—(left) From autologous biopsies of the patient, cell populations are cultured within the matrix directly or ex vivo and transferred to the matrix in second stage. 4—(below) Proangiogenic growth factors and endothelial progenitor cells are integrated in the incubation environment to generate blood vessel networks. 5—(right) After generation of macroscopic blood vessels in the matrix, the 3D custom-made implant can be transferred into the clinical situation by microvascular transfer. Nb. Quasiavascular tissues such as “custom-made and shaped” cartilage and bone do not need steps 4 and 5. Color images are available online.
Second, auricular, septal, alar, and tracheal cartilage, have a shared embryonic origin, but display different cartilage subtypes. Following new evidence, the choice of the cell source is one of the most important factors for successful cell therapy.49–51 Chondroprogenitors found in articular cartilage and the perichondral structure of auricular cartilage are now considered as superior cellular components. 52 Adult autologous cells bear the disadvantage of poor growth and dedifferentiation potential in vitro.
For tissue reconstruction, cells are expanded in vitro to mature to secure an extensive cell population. Chondrocytes grown in monolayer cultures do not fully regain their original phenotype, 23 but the use of 3D structures for chondrocyte culture has been shown to maintain the differentiated chondrocyte phenotype. A highly chondrogenic microenvironment with growth factors and accurate cartilage ECM molecules is fundamental in assuring sufficient chondrogenesis and in the prevention of dedifferentiation. 53 Other reasons for TE failure include independent cell sources that cause overgrowth of immature new cartilages, which are likely to break and stiffen, eventually resulting in calcification. 54 Multidisciplinary groups are collaborating to improve the bioreactor technology for emulating the required conditions under which tissues can be engineered.
The implanted biodegradable cartilage scaffold with neocartilage formation can induce an active inflammatory response, which adversely affects chondrogenesis and encourages the resorption of autologous neocartilage. Inflammation is primarily induced by the degradation of biomaterials or scaffolds and elicits an immune reaction regardless of whether scaffolds are synthesized with biological or artificial biomaterials. The degree of maturation of the cultured chondrocytes also influences this immune reaction. Scientists have introduced “in vitro precultivation” to create mature cartilaginous tissue with improved neocartilage properties and the ability for an appropriate breakdown of scaffold materials and matrix accumulation before implantation. 55
Clinical TE Trials Other Than (Elastic) Cartilage
Tables 2–5 give an overview of clinical studies on TE principles and substitutes for the treatment of articular cartilage breakdown,56–60 urological defects,61–69 cardiovascular frailty,33,70–78 and mucosal defects.79–87
Clinical TE trials for articular cartilage
Matrix-induced autologous chondrocyte transplantation (MACT) is a technique used for the reconstruction of full-thickness articular cartilage defects and consists of a 3D cell carrier seeded with cultured autologous cells. Bone marrow mesenchymal stem cells are widely investigated in articular cartilage TE trials.88–90 Besides their immunoprivileged and immunomodulatory capabilities that make them convenient for application in inflammatory diseases, they also have a striking ability for multiplication and chondrogenesis. However, a major obstacle is the initiation of calcification and hypertrophy. 91 On the contrary, multiple studies have tried to culture mature chondrocytes, but owing to limited quantities of obtained chondrocytes, their utilization in clinical trials has been limited. However, growth factors and exogenous stimuli are proved to be a very important factor for the production of hyaline-like cartilage. Nasal chondrocytes, in contrast, are declared in some research protocols to be superior to articular chondrocytes with the production of higher quality hyaline cartilage.40,60
Given the numerous clinical studies describing articular TE, this review briefly lists some to compare different cell carriers (Table 2).
The results from the first phase III clinical study of an articular construct will soon be published to gain Food and Drug Administration (FDA) approval for the NeoCart® construct (NCT01066702). Mumme et al. 60 developed another technique subsequent to the publication of the results of the human trial that was used to rebuild the alar lobe with autologous nasal chondrocyte constructs. 40 They seeded nasal septum chondrocytes (Chondro-Gide®) for the reconstruction of articular cartilage defects in a phase I study with satisfactory outcomes resulting in the ongoing phase II multicenter clinical study (NCT02673905). Owing to the different primary endpoints and scoring scales, it is difficult to compare this novel MACT technique with existing methods and to demonstrate its superiority.
Clinical TE trials for bladder and urethra
The ultimate target of generating a long-lasting, functional tissue-engineered duct, as was expected after the achievement of the first in-human tissue-engineered cystoplasty 20 years ago by Atala et al., 61 has not been achieved yet. However, substantial technical and preliminary steps have been taken (Table 2). Phases I and II of a clinical trial achieved success in bladder substitution with a bioresorbable scaffold (Tengion®).66,67 A multicenter phase I clinical trial is currently being developed (NCT01087697). It should be noted that despite the progress in the field, the substitutes are very thin and do not have any functional features resembling those of a natural bladder. This lack of functionality and original shape is even more important in the case of the ureter. Almost all the substitutes produced so far have been developed for transplant in an onlay manner and only have partial thickness.61–69 Nonetheless, Raya-Rivera et al. 63 reported satisfactory long-term results of tubularized urethroplasty in five boys with complex posterior urethral defects. The grafts were composed of autologous muscle cells and epithelial cells seeded on PGA scaffolds.
Clinical TE trials for heart valves and myocardial tissue
The application of tissue-engineered heart valves with cell-seeded scaffolds in clinical practice has been suspended because of the unscalable nature, time-intensiveness, and high cost of the process, as well as its unavailability for emergencies. 92 However, TE approaches can be used for the development of biologically based ducts to address the need for vascular grafts (Table 4). The largest trial was an 11-year follow-up study in 42 patients. 72 The recurrence of asymptomatic vascular restenosis was the principal obstacle and was associated with tissue overgrowth at the suture site, for which the patients were treated with balloon angioplasty. 93 Seeding higher amounts of BMSCs on the graft and adding TGF-β to the medium is a potential realistic approach to supporting graft patency.
The electrical conduction and powerful contractile force of myocardial tissue make its substitution by TE extremely challenging. There have been proposals for the use of scaffold-free cell sheets, acellular grafts, and bioengineered recellularized scaffolds, but the literature includes only one TE trial.76,77 Chachques et al. 77 implanted a cell-seeded, biodegradable, 6-mm-thick 3D collagen type I patch in the epicardia of 10 patients with postischemic myocardial lesions. Although this has been described as a superior technique, no subsequent studies were conducted after this 2008 report.
Clinical TE for skin and mucosa
A substantial number of epidermal and dermal substitutes are commercially available and have been successfully applied in clinical practice. In burn wound care, dermal substitutes include a base layer that enhances the elasticity and pliability of the overlying thin skin graft. However, these substitutes only represent the superficial layer of the skin and do not incorporate hair follicles, apocrine glands, or sensory nerve buds.14,94 Such substitutes do not meet the criteria for TE. 43 However, for gingival augmentation and oral mucosa reconstruction, several case series studies have achieved a cell-seeded matrix (Table 5)79–87 and full-thickness mucosa. Long-term studies using larger sample sizes are essential to concluding the superiority of tissue-engineered gingival mucosa over currently used techniques such as grafting of autologous buccal mucosa.
Undoubtedly, a TE strategy for achieving full-thickness skin including the aforementioned elements is one of the most anticipated and clinically required therapeutic innovations.
Additional hurdles toward translation of TE medical products
There are numerous additional obstacles for the transition of TE medical products toward clinical practice. In first stage there is a critical need for early transdisciplinary collaboration and a shortage of sustained funding programs for multidisciplinary translational research.
Furthermore, large number of ventures fail to attract or retain investor funding, promotion, and clinical acceptance. Investigators often fail to accurately identify critical clinical adoption criteria because of their focus of improved patient outcomes. Other criteria such as ethical concerns, price, alternatives, and place in the workflow can result in a failure of the product.95–97
Moreover, market entry requires elaborate and expensive clinical trials to deliver high-quality clinical evidence analyzing safety, efficacy, and accuracy of the product. More than 80% of all clinical trials fail to result in Federal Drug Administration approval. By utilizing a bedside to bench and back again approach, investigators can improve the odds that their research will have a meaningful clinical impact.
Limitations of this review
Several important limitations are associated with this study and need to be acknowledged. The first limitation is the narrative nature of this study with its inherent subjectivity. We switched the focus from the comparison of the outcomes of published clinical studies to a conclusive reflection of the development and innovation of TE in clinical studies that have been published. Second, owing to the paucity of randomized controlled trials, many of the included studies were case reports and articles that described outcomes in compassionate patients. The evidence in these studies is minor; however, these studies are worth mentioning because the literature only offers a few high-quality studies that have examined TE in humans.
Conclusion
It is critical to determine the cues that are mandatory to preserve the stability of the regenerated tissue and ascertain if it is really possible to generate a tissue-engineered construct that can stimulate its growth and expansion. Additional important questions that need to be addressed include the determination of the angiogenic mechanisms that could improve neovascularization in the implanted constructs and whether use of detergents to extract cells from tissue biopsy is truly safe. These are only a few of the many important questions that further research should address in the domain of TE to deal with remarkable challenges and achieve progress in clinical practice.
This review listed individual strategies within the field of TE that have been published. To date, only two published clinical studies have reported functional, 3D tissue-engineered constructs.40,47 Accordingly, the need to combine diverse domains of expertise to facilitate the creation of a tissue-engineered organ for clinical application is emphasized. The diversity of procedures reported in the literature indicates that a durable tissue-engineered approach remains unavailable. These are the initial stages of what will subsequently evolve in a feasible, free-graft substitute for regenerative surgery in the future. Each model must be exposed to a thorough investigation along with the exploration of molecular and cellular processes that support new tissue generation. Merely mixing fundamental TE materials will not prove satisfactory for the accurate clinical translation of tissue-engineered constructs. It is of paramount importance that advancements in preclinical and clinical outcomes are extensively reported within predetermined metrics to homogenize information to enable protocol interventions and to assess procedural cost-effectiveness. There is a critical need for early transdisciplinary collaboration and sustained funding programs for multidisciplinary translational research.
Footnotes
Authorship Confirmation Statement
All co-authors have reviewed and approved the article before submission.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.