
Abstract
Regenerative engineering strategies for the oral mucoperiosteum, as may be needed following surgeries, such as cleft palate repair and tumor resection, are underdeveloped compared with those for maxillofacial bone. However, critical-size tissue defects left to heal by secondary intention can lead to complications, such as infection, fistula formation, scarring, and midface hypoplasia. This review describes current clinical practice for replacing mucoperiosteal tissue, including autografts and allografts. Potentially paradigm-shifting experimental regenerative engineering strategies for mucoperiosteal wound healing, such as hybrid grafts and engineered matrices, are also discussed. Throughout the review, the advantages and disadvantages of each replacement or regeneration strategy are outlined in the context of clinical outcomes, quality of life for the patient, availability of materials, and cost of care. Finally, future directions for research and development in the area of mucoperiosteum repair are proposed, with an emphasis on identifying globally available and affordable solutions for promoting mucoperiosteal regeneration.
Impact statement
Unassisted oral mucoperiosteal wound healing can lead to severe complications such as infection, fistulae, scarring, and developmental abnormalities. Thus, strategies for promoting wound healing must be considered when mucoperiosteal defects are incident to oral surgery, as in palatoplasty or tumor resection. Emerging mucoperiosteal tissue engineering strategies, described in this study, have the potential to overcome the limitations of current standard-of-care donor tissue grafts. For example, the use of engineered mucoperiosteal biomaterials could circumvent concerns about tissue availability and immunogenicity. Moreover, employment of tissue engineering strategies may improve the equity of oral wound care by increasing global affordability and accessibility of materials.
Introduction
Oral defects, such as clefts, oral cancer tumor resections, periodontal implant surgery, and traumatic injuries, afflict both the bone and overlying soft tissue, or mucoperiosteum. The mucoperiosteum is the full thickness of soft tissue that lines oral cavity bones, comprising periosteum, lamina propria, and oral lining mucosa, including squamous epithelial cells (Fig. 1). Although mucoperiosteal biology is relatively consistent across locations in the mouth, there are slight variations in elastin and collagen density, and the presence of keratinized mucosa between the alveolar, gingival, and palatal regions. 1 In some cases of acute mucoperiosteal defect, current practice is to permit healing by secondary intention (i.e., without intervention), which can result in adverse complications, including fistula formation, infection, scarring, and growth challenges, each of which is described in detail below.2–4
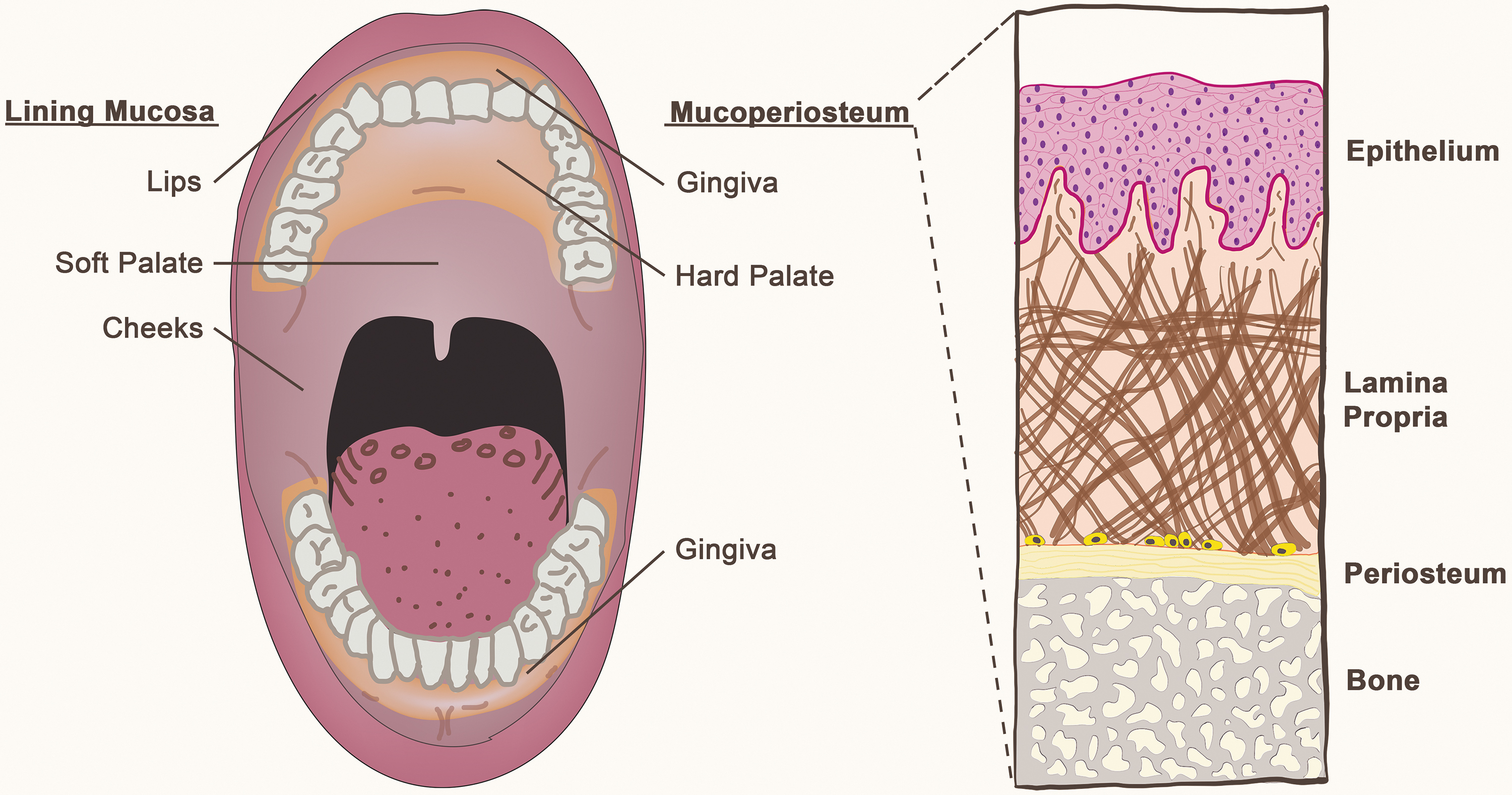
Sketch of the oral cavity (left), with mucoperiosteal tissues (gingiva and hard palate). A cross-sectional sketch of the mucoperiosteum (right), showing distinct tissue layers. Color images are available online.
After initial closure of a wound by secondary intention, excessive inflammation or fibroblast proliferation can lead to wound dehiscence (reopening), particularly for infected or poorly maintained wound beds. 5 The risk of wound dehiscence also increases when high degrees of tension are present at the wound, as often occurs when oral tissue is pulled, stretched, or moved from its original site during oral reconstructive surgery.5–8 In the case of mucoperiosteum, wound dehiscence can lead to an abnormal passageway (i.e., fistula) between the oral and nasal cavities. Oronasal fistulas are a particularly common consequence of mucoperiosteal defects; fistulas occur in up to 78% of palatoplasties and may also follow surgical procedures for periapical infection, oral trauma, and neoplasm.5,8 Complications of fistula include nasal regurgitation of food, hypernasal speech, and increased sinonasal and ear infections. In children, oronasal fistula can also impair speech development, and for adults, food caught in the fistula is difficult and embarrassing to remove and can result in halitosis. While clinical fistula management depends on its size and location as well as patient age, a second surgical procedure is often required, which further disrupts a patient's life and increases their care costs.
Because saliva flow is inherently reduced in an open wound or fistular passageway due to their recessed nature, bacteria and nutritive matter are more likely to accumulate, which can increase the risk of infection.9–11 However, overall, the infection rate of mucoperiosteal surgical sites is relatively low compared with other clean-contaminated sites, possibly due to higher numbers of innate lymphoid cells and greater blood supply compared with more distal sites. 12 While the infection rate following palatoplasty seems to be quite low in the United States, 13 one study found an aggregate 2.2% infection rate from 1988 to 2008 in developing areas of Southeast Asia. 14 In addition to fistula, the likelihood of infection is also dependent on risk factors such as being underweight or anemic, poor oral hygiene, tobacco and drug use, diabetes, and immune deficiencies. 15 Bacterial infection of a wound disrupts healing and tissue regeneration, and can result in systemic infection, which increases the likelihood of readmission, the risk of serious downstream complications, and health care expenses.
Healing by secondary intention can also alter tissue mechanical properties and decrease function compared with undisturbed mucoperiosteum, likely due to the absence of elastin and vasculature in scar tissue. 4 In cases of mucoperiosteal healing with underlying bone defects, aberrant scar tissue may grow into undesirable spaces and cause disruptions in healing and development. 4 Furthermore, mucoperiosteal wounds can interrupt craniofacial development in pediatric patients, independent of scarring. The most common example of this is in primary palatoplasty, which usually occurs between ages 6 and 18 months to support normal speech development in children born with a clefted palate. 16 Although the direct and definitive cause is not known, midface hypoplasia, a disrupted craniofacial growth condition, occurs in up to 50% of patients who undergo palatoplasty. 17 In a murine model, disruption of palatine bone sutures, as may occur by denudation of the palatal bone (a common practice during palatoplasty) directly contributes to midface hypoplasia. 18 Based on this and clinical observations, many surgeons believe that earlier palatoplasty results in more severe midface hypoplasia. However, if palatoplasty is performed too late, speech development is severely disrupted, requiring therapy and surgery to prevent lifelong challenges. These opposing constraints push the surgeon to operate earlier or later, with serious trade-offs required in either scenario. In addition, similar growth challenges can follow large mucoperiosteal repairs after pediatric trauma or cancer, especially in low resource settings. In any case, improved surgical adjunct therapies could permit an earlier reconstruction without craniofacial growth impact or postoperative complications.
Secondary intention of acute mucoperiosteal wounds, such as those formed trauma, tumor resection, periodontal implant, or cleft palate repair, has significant negative consequences. Yet, surgical best practices and regenerative strategies to promote mucoperiosteal healing are understudied compared with those for other craniofacial tissue types (e.g., bone). In this review, we discuss current approaches to mucoperiosteal repair and wound healing, including their advantages and disadvantages. We also present some mucoperiosteal repair tissue engineering technologies still in development and discuss their prospects for future clinical use.
Methods
Emerging technologies and general trends in the field were identified by general and targeted literature searches using the PubMed database. First, a general literature search with keywords, such as “mucoperiosteum” and “tissue engineering” or “biomaterials,” were used to identify three broad categories (autografts, acellular dermal matrix [ADM], and biomaterials) and their corresponding subcategories (Fig. 2), which were corroborated by our own expertise and exposure to general trends in the field. Next, each subcategory was used as a search term in combination with the terms “oral mucosa” or “mucoperiosteum” for a comprehensive search. At this stage, publications were excluded based on several logistical criteria: publication date before 2000 or full text not available (in English). Finally, an additional filtering step for relevance was performed manually (B.N.A. and Q.W.), with exclusion criteria being: (1) focus on irrelevant anatomy (e.g., intestinal mucosa) or chronic conditions (e.g., gingival recession); (2) case study with a single patient (i.e., n = 1); and (3) study involving an incomparable biomaterial (i.e., complex characteristics that could not be readily compared with the majority of other biomaterials in the literature pool). The number of publications in each subcategory before and after filtering are shown in Figure 2. For each publication, results are summarized in tables, while connections and our own qualitative analyses across studies are provided in each corresponding section of the text.

Graphical description of search methods. The box under each focused search term indicates the number of articles generated by the focused search term and oral mucosa/mucoperiosteum. The box underneath the filter indicates the number of articles in the preceding box that met the logical and relevancy criteria. ACS, autologous cell sheets; Ker, keratinocytes.
Current Practice: Autologous Cells and Tissue
Given the distinct drawbacks of secondary intention, tissue transplantation, either autologous or allogeneic, is frequently used in surgery when a mucoperiosteal defect is too large to close using only the immediate surrounding tissue. Insufficient amounts of tissue can result in excessive tension on the defect site, which can lead to fibrosis and its complications as discussed in the Introduction section.19,20 The use of autologous tissue, which is collected from a secondary site on the patient's body (Fig. 3A), is widely accepted and commonly utilized to supplement local mucoperiosteal tissue in children and adults with mucoperiosteal defects (Table 1). Transplanted tissues can be categorized into three broad groups: grafts, free flaps, and pedicle flaps. Grafts are tissues that are harvested and transplanted without connecting the donor vasculature to the host site. Thus, the survival of grafts is initially dependent on diffusion of nutrients into the tissue and requires neovascularization for long-term tissue survival. Due to the diversity of graft harvest sites, the long history of graft use in general reconstructive surgery, and the challenges associated with long-term graft survival, detailed information about the use of tissue grafts for mucoperiosteal repair are not included in this review. In contrast to grafts, if the vascularization of tissue is completely maintained (pedicle) or briefly disconnected and then reanastomosed (free) during the procedure, the tissue is known as a flap. 21 The inherent advantage of flaps compared with grafts is their extensive vascularization and thus greater success rate. However, flap procedures are more technically challenging than tissue grafting, and require longer operating times.
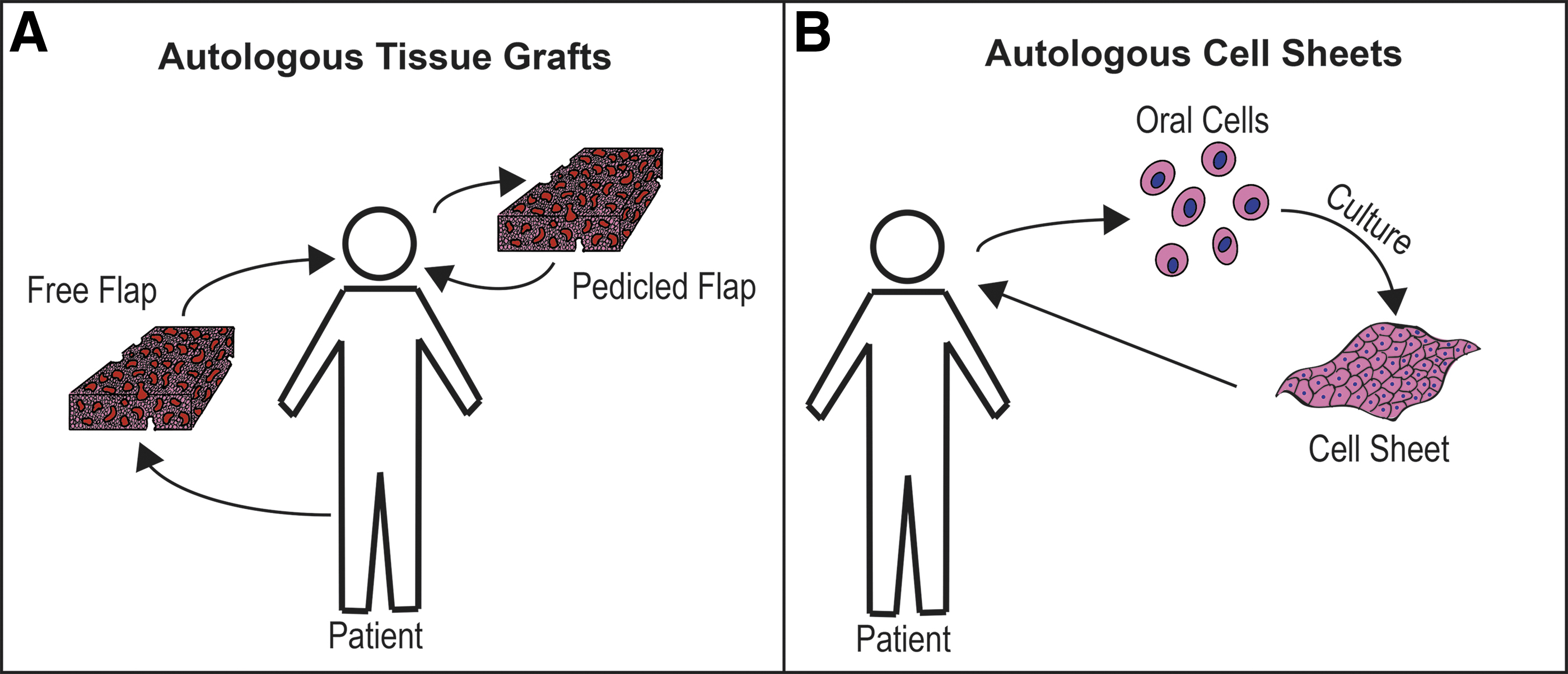
Schematic of autologous tissue grafts
Clinical Uses of Autologous Grafts for Repair of Acute Mucoperiosteal Defects, January 2000–May 2021
BFP, buccal fat pad; BMM, buccal myomucosal; F, female; FAMM, facial artery musculomucosal; M, male.
The type of tissue, or flap, selected for a particular procedure is also determined by the thickness, shape, and anatomical location of the defect. For example, within each broad category, flaps and grafts are further categorized based on which functional layers are included in the tissue. For example, a fasciocutaneous flap contains skin, subcutaneous tissue, and the underlying fascia. In general, flaps are carefully selected to match the host tissue structure and function as closely as possible. Other factors affecting flap choice include comorbidities that impact surgery and recovery time, desired esthetic and functional outcomes, and surgical training required for the technique.
Pedicle flaps must be sourced from local or regional tissue because they are constrained by the length of the blood supply. The angle of rotation to reach the defect must also be considered based on the flexibility of the blood supply. Thus, the location and size of the defect are critical factors in deciding which flap will provide the best outcome. Mucoperiosteal defects are commonly repaired with regional vascularized flaps, most commonly buccal myomucosal flaps,22–25 including facial artery musculomucosal flaps (FAMM),26,27 buccal fat pad flaps,28–31 or tongue flaps 32 (see details in Table 1). Tissue can also be harvested from seemingly distal sites such as facial skin and even calvarial (skull) bone and transplanted intraorally without disconnecting the vasculature.33,34 Rotation and transfer of mucoperiosteum from one site of the palate to cover another area is also a commonly employed technique in repair of palatal defects but was not included in this review since the donor and host tissue are anatomically and functionally analogous. Since pedicle flaps are mostly taken from regions of the oral cavity, there is greater likelihood (compared with a free flap) that the grafted tissue will esthetically and functionally blend with the host tissue. However, pedicle flaps are generally more size restricted than free flaps, as there is a limited amount of mucosal tissue in the mouth. Thus, substantial defects may require tissue from distant parts of the body, in which case free flaps are used.
Free flaps generally require longer operating times and are more technically challenging and thus more expensive to use than pedicled flaps. Additionally, free flaps have higher complication risks in patients with certain pre-existing conditions. For example, free flaps create a higher risk of severe bleeding, pneumonia, and cardiac arrest in patients with insulin-dependent diabetes compared with those without. 35 However, free flaps present a smaller chance of infection than certain pedicled flaps. 36 Because of their potentially large size compared with pedicle flaps, free flaps are frequently used for repair of severe problems like head and neck cancer, complicated craniofacial Tessier clefts, or serious trauma (Table 1), 37 and they are rarely used in pediatric oral mucoperiosteal repair due to overall tissue shortages and the risk of donor site tissue morbidity. Repair with free flaps is also undesirable if the flap contains skin tissue (e.g., fasciocutaneous flaps); skin does not have the same texture and function as mucoperiosteum, thus causing complications such as foreign body sensation, distorted sense of taste, and hair growth within the oral cavity. The technique of prelamination, wherein flaps are lined with oral mucosa before reconstruction of intraoral defects, has been developed to circumvent these issues. 38 However, this technique significantly increases operating time and sometimes requires two procedures. In addition, it requires advanced surgical skills and flap shrinkage often occurs, necessitating later surgical revisions.
The primary benefit of autografts is their low immunogenicity and thus minimal risk of rejection due to being harvested from the patient. Drawbacks include risks of infection and scarring at both the donor and recipient sites, and donor site morbidity. For either type of flap, surgery is technically challenging, requiring specialized training, and nursing care is needed to achieve acceptable outcomes. Additionally, autografts are limited in supply by the amount of tissue the patient can safely spare. Tissue supply is exceptionally limited in infants and children, posing substantial challenges for mandatory surgeries that occur at young ages, such as cleft palate repair. Furthermore, donor site morbidity is an especially critical consideration for sites where growth or development of the donor region may be challenged if disturbed. Growth alterations during these early stages have far-reaching physical and psychosocial consequences, including mobility, esthetics, and athletic potential. Thus, the development of alternative tissue engineering options for pediatric mucoperiosteal repair are particularly pertinent and important.
As an alternative to free tissue grafting, autologous oral cells can be isolated using punch or brush biopsies and cultured in vitro to form a monolayer of patient-specific epithelial tissue (Fig. 3B), supported with gauze.39,40 Two publications have reported results on autologous oral cell sheets in the last 20 years. In the first, large oral mucosal wounds (12 patients: 10 males and 2 females; mean age 51 years) were treated with cell sheets derived from either freshly biopsied or banked mucosal epithelial cells. Regardless of cell source, wounds were fully healed after 3 weeks, with no infection nor scarring noted. 41 In a following report from the same research team in which a similar procedure was followed (11 patients: 10 males and 1 female; mean age 52 years), cell sheets were fully adhered to the site after 1 week, and defects were fully healed and keratinized within 3 weeks. 42 Despite these promising results, the use of an autologous cell sheet requires the creation of a donor tissue defect and several weeks of culture in a sterile, tightly regulated good manufacturing practice facility, which increases cost and potential for contamination or mutation. Furthermore, cellular sheets alone are fragile, difficult to handle, and fail to prevent wound contraction and scarring in full-thickness skin wounds.43,44 Thus, epithelial sheets often require a support structure such as gauze during application, which then requires follow-up surgery for removal.35,45 Nonetheless, the concept of autologous oral cell transplantation has spurred investigation of degradable hybrid graft constructs that do not require later removal.
Contemporary Clinical Materials: Matrix Allo- and Xeno-Grafts
Allogeneic and xenogeneic matrices are increasingly common for mucoperiosteal tissue repair, since human donor and animal tissues are more readily available than autograft tissue, and patient donor site morbidity is avoided. Overall, foreign soft tissue grafts can improve mucoperiosteal regeneration and mitigate postoperative complications, such as fistula formation (Table 2)46–48 ; these findings are described in greater detail below.
Clinical and Exploratory Uses of Acellular Tissue Matrices for Repair of Acute Mucoperiosteal Defects, January 2000–May 2021
ADM, acellular dermal matrix.
ADMs are the most common type of foreign grafts for mucoperiosteum repair; they lack foreign, potentially immunogenic cells and noncollagenous proteins, but still provide a scaffold into which the patient's cells can grow (Fig. 4A). These matrices also allow the graft to esthetically blend into the patient's tissue more readily than autografts, which maintain the color and texture of the donor tissue. It has been estimated that up to 45% of surgeons use ADMs for primary cleft palate repair, including commercially available options, such as AlloDerm®, Mucoderm®, Allopatch®, SurgiMend®, and Epiflex®. 49

Schematic of allogeneic acellular dermal matrices
ADMs have been shown to enhance mucoperiosteal wound healing in animals and humans. For example, treatment with ADM significantly increased vascularization and epithelialization of mucoperiosteal wounds compared with those treated with iodoform gauze alone in rabbits. 50 In humans, there have been several successful clinical trials using ADMs to facilitate gingival growth after dental implant surgery.51–53 Furthermore, one clinical trial demonstrated that ADMs did not cause immune rejection nor infection, and effectively regenerated the mucoperiosteum in up to 94.5% of patients (n = 36). 54 However, mild graft contraction did occur in some patients that also had buccal or lip defects. Moreover, in patients with recurrent oronasal fistula, ADMs can prevent infection and fistula recurrence when used to fill nasal mucoperiosteal defects. 55 On the other hand, some evidence suggests that the long-term graft stability of ADMs is inferior to that of autografts. Specifically, in a clinical trial for peri-implant gingival regeneration, ADM-treated sites had higher gingival and plaque index scores and thinner mucosa compared with sites treated with free gingival grafts. 56 Furthermore, in a similar study, mucosal thickness significantly increased during the first month, but 23% of the new tissue volume was lost during the subsequent 11 months, with no additional growth observed. 52
The use of decellularized nondermal tissues has also found favor in the past two decades, primarily as an augmentation to ADMs. For example, xenogeneic bilayer matrices consisting of a dermis (ADM) layer and a peritoneum layer have also been used clinically for applications such as peri-implant gingival regeneration and fixing intraoral and palatal defects. The use of a bilayer matrix generally results in better esthetic outcomes, reduced surgery time, and less patient morbidity compared with free gingival grafts, with no difference in final keratinized tissue volume.52,57–59 Decellularized bovine pericardium has also been employed in a mucoperiosteal wound healing clinical trial, in which it facilitated tissue repair. 60 In addition, this membranous material is compatible with exploratory laser-initiated bioadhesives 61 ; altogether, these materials show promise for a clinically relevant, sutureless approach to mucoperiosteal wound healing.
Decellularized tissue matrices have several logistical drawbacks of their use in mucoperiosteal wound healing. First, they must be cut to fit the defect in the operating room, increasing procedure time. Matrices from human donors are also in limited supply, especially in developing countries. Xenogeneic matrices have more ample supply globally, but social and ethical factors must be considered when using animal tissue grafts in surgical settings. In either case (allo- or xenogeneic), heavy processing is required to reduce immunological risk while maintaining delicate tissue structures, adding to their expense. While most immunological risk is removed by this processing, a small amount may remain compared with autografts. In summary, acellular matrices can effectively regenerate mucoperiosteal tissue, but they may be time- and cost-prohibitive, and production is limited by the amount of donor tissue available. 48
Acellular matrices can be topped with a monolayer of oral keratinocytes in vitro or seeded with oral mucosal fibroblasts to form a hybrid autologous/allogeneic graft (Fig. 4B).45,48,62–68 Once matured, these hybrid materials have slightly thinner epithelium and underdeveloped basement membrane compared with native tissue, but similar protein expression.69–71 Matrix/cell grafts have been successful in some animal and clinical studies,72,73 although one canine study suggests that vascularization is too slow to supply nutrients to the cells within the graft. 74 Regardless of the scientific merits of the foundational studies referenced here, the feasibility of using a graft that contains autologous cells to treat mucoperiosteal defects is tenuous. Namely, safety, time, and resource limitations hinder the global relevance of a multilayered cultured graft approach in this context.
Emerging Approaches: Engineered Biomaterials
The extracellular matrix of the mucoperiosteum, which mostly lies within the lamina propria, is composed of type I collagen, type III collagen, and elastin. Thus, collagen, along with its denatured counterpart gelatin, is a popular material for biopolymer graft fabrication (Fig. 5). While gelatin is chemically similar to collagen, its immunogenicity is lower due to removal of cystines and reduction in a number of aromatic rings during the manufacturing process. 75

Schematic of engineered crosslinked biopolymers used for mucoperiosteal repair and in vitro modeling. ECM, extracellular matrix. Color images are available online.
In animal models, collagen scaffolding systems are compatible with mucosal tissue (Table 3) and can be used to release growth factors, like VEGF, IFN-γ, and FGF, which increase graft vascularization and cell density. 76 Overall, the wound healing and tissue regeneration outcomes of collagen with growth factors are generally better than collagen material alone. Furthermore, crosslinked collagen scaffolds can successfully integrate with palatal mucosa with minimal inflammatory response and foreign body reaction. These scaffolds can even guide the otherwise random formation of new collagen fibers. 77 Like ADM, in vitro and in vivo use of collagen scaffolds in engineered mucoperiosteum is also well established. Commercial products, such as EpiGingival®, which is a multilayered tissue mimic containing human cells, is marketed for use in dental product testing. Furthermore, some products, such as Bio-Gide® and CollaTape® (both comprising crosslinked collagen) have also obtained FDA 510(k) clearance for clinical use. Clinical trials using premarket approved collagen products in for mucoperiosteal repair have demonstrated their ability to achieve similar outcomes compared with free tissue grafts, with reduced surgery time and patient morbidity (Tables 3 and 4). In addition, compared with healing by secondary intention, collagen matrices reduce scarring and inflammation. 78 From an exploratory perspective, various in vitro oral mucosa tissue models have shown that in vivo structure and protein expression can be recapitulated in a dish, pointing to the promise of these materials for use in tissue engineering applications (Table 5).
Clinical and Exploratory Uses of Engineered Collagen Materials for Repair of Acute Mucoperiosteal Defects, January 2000–May 2021
bFGF, basic fibroblast growth factor; C6S, chondroitin-6-sulfate; FGF-2, fibroblast growth factor 2; IFN-γ, interferon-gamma.
Preclinical and Clinical Uses of Hybrid Tissue-Engineered Grafts for Repair of Acute Mucoperiosteal Defects, January 2000–May 2021
Human cells unless otherwise indicated: epithelial (typically keratinocytes) and/or fibroblasts. Y indicates presence of cell type indicated by the column title.
Exploratory Uses of Hybrid Tissue-Engineered Grafts for Mucoperiosteal Tissue Modeling or Defect Repair, January 2000–May 2021
Human cells unless otherwise indicated: epithelial (typically keratinocytes) and/or fibroblasts.
Glycosaminoglycan: chondroitin-4-6-sulfates.
Cells in this study were immortalized.
Human umbilical cord Wharton's jelly stem cells.
ECM, extracellular matrix; MSCs, mesenchymal stem cells.
Gelatin scaffolds are sparingly used in oral mucoperiosteum defect repair. In our literature search, one study used gelatin in combination with collagen to improve growth factor delivery 79 and another used a crosslinked gelatin hydrogel with encapsulated fibroblasts for oral mucosa tissue engineering. 80 Compared with a collagen hydrogel, the gelatin had less-viable encapsulated fibroblasts and lacked epithelial differentiation. However, this was an in vitro study only and included only limited assessments (e.g., cell viability and histology). Further studies using additional cell types for in vitro study, as well as animal studies, should be performed to assess potential use of gelatin in oral mucoperiosteum repair.
Despite their exceptional biocompatibility and tissue formation capabilities, there are a few challenges to clinical translation of collagen and gelatin materials. For example, as with ADMs, engineered collagen materials are poorly adherent to the wound site, causing premature graft sloughing. 81 Furthermore, loosely crosslinked collagen and gelatin-based biopolymers (i.e., hydrogels), which have better adhesion than collagen sponges, can pose immunogenicity risks, exacerbated by source variability. Moreover, hydrogel materials, while advantageous from a growth factor delivery and vascularization perspective, have limited mechanical properties, and their pore size is often difficult to control. 82
As an alternative to collagen, mucoperiosteal scaffolds commonly include fibrin because it has mechanical properties similar to the lamina propria and excellent mucoadhesion properties (Table 6). 83 Fibrin glue is frequently used to mend surgical wounds in place of sutures, and can help heal postsurgical mucoperiosteal wounds, preventing complications, such as infection and oronasal fistula formation.84,85 Platelet-rich fibrin (PRF) is especially useful because the material spontaneously gels (i.e., clots) with ease, and thrombocytes produce growth factors that promote bone and soft tissue regeneration and maturation. 86 PRF gels require less surgical skill to employ than free flaps 87 and have been used clinically to promote soft tissue growth around periodontal implants,88,89 within surgical lesions,90,91 and to close oronasal communication. 87 As such, several research groups have investigated fibrin's potential as a mucoperiosteal graft component (Tables 4–6). For example, in a series of studies, engineered mucoperiosteum was created by embedding oral mucosal fibroblasts in a fibrin/agarose gel and topping with a keratinocyte monolayer.48,92 When transplanted, these grafts improved palatal bone growth and maturation in a rabbit model by preventing the negative effects of healing by secondary intention. 48 Compared with fibrin/agarose gels, however, pure fibrin gels are more conducive to fibroblast proliferation and extracellular matrix production, two precursors to scarring. 93 Importantly, these studies suggest that the chemistry of a biopolymer matrix can modulate the wound healing mechanisms of the mucoperiosteum.
Clinical and Exploratory Uses of Engineered Fibrin Materials for Repair of Acute Mucoperiosteal Defects, January 2000–May 2021
PGA, poly(glycolic acid); PRF, platelet-rich fibrin.
Despite these advantageous properties, one clinical trial showed that split-thickness grafts resulted in better wound healing outcomes, based on oral cavity opening and speech intelligibility data. 83 To further improve wound healing, fibrin can be supplemented with growth factors such as basic fibroblast growth factor (bFGF). Several research teams have studied this hypothesis in animals (rats and dogs) by impregnating fibrin with bFGF or injecting bFGF into the wound site to accelerate mucoperiosteal growth, and potentially decrease midface hypoplasia.79,94
Chitosan is also a popular material choice for mucoperiosteal wound healing. This naturally derived polysaccharide is especially suited to mucoperiosteal repair because it is mucoadhesive,95,96 antibacterial,96–98 and when converted to a hydrogel form, could be tuned to mimic the physical properties of the mucoperiosteum. Fibroblast proliferation, hyaluronic acid synthesis, and blood clotting are all naturally facilitated by chitosan, which promotes wound healing and prevents scarring. Chitosan hydrogels encourage oral mucosal cell proliferation in vivo in canines 99 and rabbits 100 and are readily resorbable by native tissue. Another beneficial property of chitosan is its excellent drug delivery capabilities. Several researchers have studied chitosan to facilitate drug and antimicrobial delivery to the oral mucosa.97,101 However, chitosan does not have sufficient cell attachment regions to stand alone as a tissue engineering scaffold so it is often paired with collagen to promote cell attachment and improve mechanical properties.63,73
Conclusions and Future Directions
Acute mucoperiosteal defects, such as those created during periodontal implant placement, cleft palate repair, and tumor resection, are global challenges that can be treated with autologous tissue, allogeneic and xenogeneic extracellular matrix, and, if developed further and approved for use, tissue-engineered matrices, or combinations thereof. Compared with secondary intention, these grafts have the potential to prevent infection in the wound site, reduce fibrosis, and potentially decrease the risk of growth disruptions such as midface hypoplasia for pediatric patients.
Despite the preliminary success of tissue engineering approaches, several areas of opportunity lie ahead. For example, engineering approaches to date have not prioritized the site-dependent biomechanical properties of oral mucoperiosteum as opposed to oral mucosa. Thus, engineering strategies that are tailored to specific mucoperiosteal regions are underdeveloped. A recent study examining the mechanical properties of various intraoral tissues (n = 30 samples: 10 from each of 3 regions) helps to lay the groundwork for this future direction. 102 Specifically, despite the fact that attached gingiva and the hard palate are both classified as mucoperiosteum, the elastic modulus of gingiva is more than double that of the hard palate (37.4 ± 17.4 vs. 18.1 ± 4.5 MPa), and both are substantially stiffer than buccal mucosa (8.3 ± 5.8 MPa). Given the unique and demanding masticatory forces present in the oral cavity, these biomechanical differences are relevant considerations for site-specific mucoperiosteal tissue engineering.
In addition, none of the interventions described in this study is known to be rapidly deployable; each requires preparatory fabrication or culture time before surgery or time-consuming manipulation during surgery. Moreover, given the increasing costs of health care, and limitations to its access in some regions of the world, many of the engineering solutions described herein are not globally relevant.
For future studies, we recommend that researchers and clinicians clearly identify intended oral sites and tailor materials accordingly. Researchers should continue to determine which biopolymer chemistries and combinations are most conducive to mucoperiosteal wound healing, and the minimal required mechanical strength of such materials for appropriate duration in the oral cavity. For example, nanomaterials such as nanoparticles and nanofibers could be used to enhance the mechanical strength of mucoperiosteal materials, and may even boost integration between tissue and bone. 103 Furthermore, significant advancements in the fields of oral regeneration and repair could be catalyzed by fundamental research probing the role of micro- and nanostructure on mucoperiosteal function, healing, and the immune response.
Moreover, many of the strategies we reviewed in this study, involve the use of allogeneic or autologous cells to recapitulate the mucoperiosteum. As noted in each corresponding section of this article, there are salient ethical, practical, and financial limitations to using cell-based therapies for this application. As such, advancements in cell-free mucoperiosteal biomaterial approaches should continue to be developed. In addition to being appropriately robust mechanically, any candidate graft must also be sufficiently vascularized in vivo within a reasonable time. Ideally, use of the candidate material would also result in minimal scarring. Several studies reviewed here employed embedded growth factors to enhance vascularization and decrease scarring, with promising outcomes.79,94,104,105 As such, future work could include understanding the diffusion rate of growth factors from mucoperiosteal materials and mechanisms by which to elongate their active lifespan by sustained and controlled release. In addition, emerging strategies for stimulating vascularization and wound healing should also be considered as potential paths forward. For example, exosomes secreted from mesenchymal stem cells or mucosal epithelial cells promote healing and vascularization in skin and other tissues.106,107 Thus, future work involving the inclusion of exosomes in mucoperiosteal wound healing materials may represent a beneficial step forward for the field.
Ultimately, efficient and effective surgical approaches to deploy mucoperiosteal materials in the operating room must also be developed. Since mucoperiosteum overall is inflexible but the mucosa easily tears, the tissue is difficult to stretch and to suture. 61 Furthermore, given the space constraints within the oral cavity, sutureless solutions may be helpful for this application. Collectively, this knowledge will be critical for the equitable and affordable application of biopolymer-based mucoperiosteal wound healing strategies on a global scale.
Authorship Confirmation Statement
All authors substantially contributed to the acquisition of data, writing, or reviewing of this work. All authors agree to be held accountable for the integrity and accuracy of this article. This work has not been published and is not under consideration for publishing by any other journals.
Footnotes
Acknowledgments
This work was supported by the Roy J Carver Charitable Trust, University of Iowa Dean's Graduate Engineering Fellowship, the University of Iowa Old Gold Summer Fellowship, and the Paul N. Johnson Associate Professorship of Craniofacial Abnormalities.
Disclosure Statement
No competing financial interests exist.
Funding Information
Authors have no funding sources that would be financially impacted by the publication of this article.