
Abstract
Osteoarthritis is among the most prevalent of musculoskeletal disorders in the world that causes joint pain, deformity, and limited range of movement. The resulting osteochondral defect can significantly decrease the patient's quality of life, but current treatment options have not demonstrated the capacity to fully regenerate the entire osteochondral microenvironment. Structurally, the osteochondral unit is a composite system composed of three layers—articular cartilage, calcified cartilage, and subchondral bone. Collectively these distinct layers contribute to the distinct biomechanical properties that maintain the health and aid in load transfer during joint articulation. The purpose of this review was to examine the role of the osteochondral interface in tissue engineering. Topics of discussion include the biomechanics of the osteochondral unit and an overview of various strategies for osteochondral interface tissue engineering, with a specific focus on three-dimensional bioprinting. The goal of this review was to elucidate the importance of the osteochondral interface and overview some strategies of developing an interface layer within tissue engineered scaffolds.
Impact Statement
This review provides an overview of interface tissue engineering for osteochondral regeneration. It offers a detailed investigation into the biomechanics of the osteochondral unit as it relates to tissue engineering, and highlights the strategies that have been utilized to develop the osteochondral interface within tissue engineering scaffolds.
Introduction
Osteoarthritis is the most common joint disorder in the United States. 1 The resulting osteochondral defects can cause joint pain, impaired function, deformity, and limited range of motion that can be debilitating and significantly influence the patient's quality of life. 2 Full thickness osteochondral lesions can also result from traumatic injuries in young individuals, which can lead to joint pain and swelling in the absence of diffuse osteoarthritis. Although palliative and surgical treatments exist to mend osteochondral defects, these options have not demonstrated the capacity to fully regenerate healthy hyaline cartilage within the articulating joint. 3 As a result, tissue engineering strategies have been explored to fully regenerate osteochondral defects. 4
Structurally, the articular cartilage, calcified cartilage, and subchondral bone make up the osteochondral unit. This composite system possesses distinct biomechanical properties that facilitate the load transfer during joint articulation. 5 However, when the osteochondral unit is compromised by trauma or pathology, the cartilage and subchondral bone experience structural changes that lead to further mechanical instability within the complex. 6 Irreversible deterioration of this complex limits joint mobility and will perpetuate the onset of osteoarthritis that affects all structures within the region, which is characterized by structural changes such as joint space narrowing, osteophyte formation, and subchondral sclerosis. 7 In addition to the alterations to the chondrocytes and cartilage matrix, the subchondral bone undergoes changes early in the disease process, although the exact mechanism involved in the process is unknown. 8 Ultimately, the intricate balance between bone and cartilage influences biochemical and biomechanical changes experienced within the osteochondral unit. 9
Therefore, to design a biomimetic osteochondral scaffold, the layer-specific structural and biomechanical properties have to be recapitulated within the scaffold. Three-dimensional (3D) printing is an additive manufacturing strategy that has been available since the 1980s, and it has been increasingly utilized for osteochondral tissue engineering. 10 This fabrication strategy can replicate complex macroscale geometries using patient defect-specific scanning techniques with consistent microscale geometry while eliminating sample-to-sample variability. 11 Therefore, this approach allows researchers to easily produce scaffolds with the complex geometries without encountering inconsistencies that arise when manufacturing on larger scales. This review aims to investigate the function of the osteochondral interface within tissue engineering scaffolds. We will overview the structure and biomechanics of the osteochondral unit and overview various strategies that have been utilized for interface tissue engineering for osteochondral regeneration. A particular focus of the review will be on recent studies that utilize extrusion-based 3D bioprinting in the development of an interface within osteochondral scaffolds.
Methods
PubMed through NCBI was utilized to gather and examine all cited sources published until July 1, 2021. The keywords utilized in conducting the database searches were 3D printing, calcified cartilage, hybrid composites, mechanical interlocking, osteochondral interface, osteochondral tissue engineering, polymer interface, scaffold, shear strength, and tissue engineering. References included were gathered through primary searches, articles known to the authors, or from citation lists contained in other literature reviews.
Structure and Biomechanics of Osteochondral Defects
The osteochondral unit possesses a distinct ability to transfer loads during joint movement (Fig. 1A, B). 5 Because each layer of the osteochondral unit has its own unique hierarchical structure and biological properties, the composition, structure, and function of each layer has to be considered to design a biomimetic osteochondral scaffold.
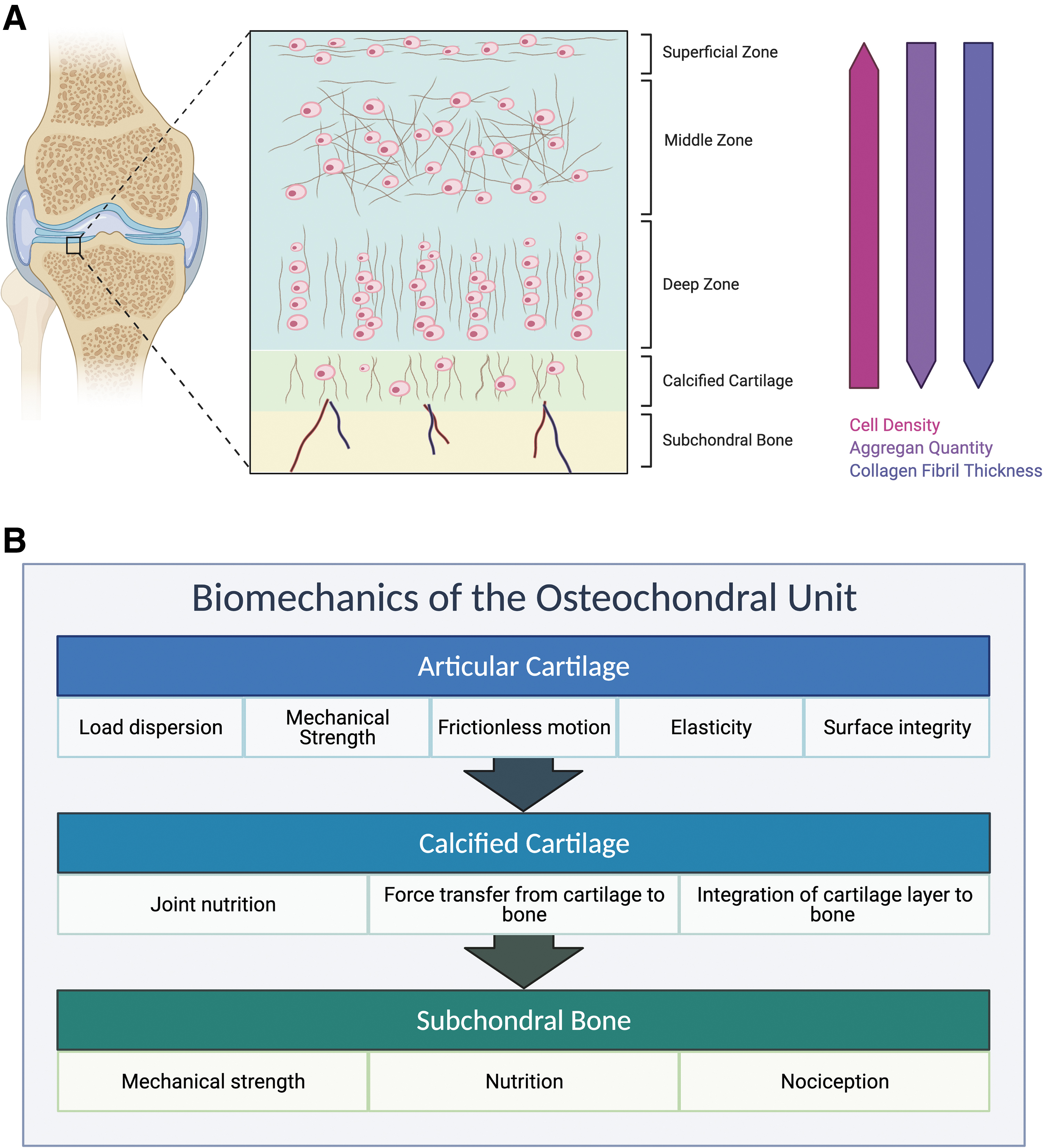
The principal function of articular cartilage is to enable low friction articulation and facilitate load transmission through the osteochondral unit. In addition to the lubricated surface, the articular cartilage also possesses unique viscoelastic properties to withstand high cyclic loads without degenerative change. 12 Its overall composition can be thought of as a biphasic medium consisting of a fluid phase and a solid phase owing to its compositional nature. 13 Two mechanisms have been identified to describe the viscoelasticity and mechanical behavior of articular cartilage.14,15 First, the flow-independent mechanism of viscoelasticity describes the viscoelastic behavior that arise from the collagen–proteoglycan interactions within the extracellular matrix (ECM). 16 Conversely, the flow-dependent mechanism depends on the interstitial fluid and frictional drag resulting from the fluid flow. 17
The flow-independent solid phase of articular cartilage consists of the porous and permeable ECM. 17 As a viscoelastic structure, the articular cartilage displays a time-dependent behavior upon constant load. 18 The boundaries of the osteochondral unit are designed to restrict mechanical deformation at the contact surface. When the articular cartilage is subjected to a constant compressive load, it demonstrates a creep and stress–relaxation response. 17 As the cartilage deforms and is held at a constant strain, the stress experienced by the structure reaches a maximum. Upon the removal of strain, the stress relaxes within the structure and reaches an equilibrium. Therefore, articular cartilage cannot be defined by a single Young's modulus as it generally stiffens with increasing strain. 19
The fluid phase of articular cartilage is mainly water that makes up to 80% of its wet weight. 13 When the diarthrodial joint experiences a load, the interstitial fluid flows out of the ECM because of the rapid buildup of pressure during function, which will eventually flow back in upon the release of the load. 20 The low permeability of articular cartilage slows down the interstitial fluid flow owing to the frictional drag resulting from the matrix. 21 Ultimately, the fluid pressure plays a significant role in stress reduction and structural support experienced by the entire complex upon load. In addition, in conjunction with the solid phase, negative electrostatic repulsive forces help resist the compressive forces as the proteoglycan aggregates of the matrix interact with the interstitial fluid. 22
The calcified cartilage serves as an interface layer to help adhere the articular cartilage to the subchondral bone. 23 This layer enables a gradual stiffness transition from cartilage to bone that ultimately facilitates the stress distribution. Because the vertically positioned collagen fibers extend from the calcified cartilage layer into the intermediate region of articular cartilage, delamination owing to horizontal shear stress would occur just above this region. 24 This specific matrix organization connects the relatively softer articular cartilage to the stiffer calcified cartilage and aids joint stress transmission throughout the osteochondral unit. 25
Finally, the subchondral bone is responsible for the dispersion of axial loads across the osteochondral unit while preserving the articular cartilage above it. 26 During regular joint movement, the subchondral bone dissipates the forces with ease because its capacity to deform is tenfold that of long bones. 27 When the articular cartilage is under duress, the various layers of the arthrodial joint work together to facilitate support and force distribution. Because the subchondral bone interfaces with the articular cartilage through the calcified cartilage layer, the forces are transferred to the subchondral bone and the shear stresses in the cartilage layer are minimized. 28 Accordingly, the trabeculae lying deeper within the subchondral bone helps dissipate the load across the layers of the joint.
Although subtle but detectable changes can be detected early on in subchondral bone, most osteochondral defects arising from the region are caused by pathologies causing significant lesions, such as osteosclerosis and osteochondritis dissecans. 29 Ultimately, the functional coordination among the different layers capably offsets the forces imposed on the joint. Because joint motion is anatomically restricted by the joint shape and attachments of various ligaments, the dissipation of the stresses through the subchondral bone follows a distinctive pattern. 30 As a muscle or tendon within the osteochondral unit contributes surface loads to the joint, they also proceed to neutralize the torque resulting from the ground reaction force that acts along the lever arm of the limb. 27 Because the lever arm associated with the limb is considerably longer than that of the tendon, the tensile force of the tendon is greater than the corresponding ground reaction force that amplifies the contact forces within the joint.
If these joint forces persist over the long term, the joint will adapt to the repetitive stresses by bone remodeling. 26 Although physiological loads help maintain joint homeostasis, abnormal joint loading resulting from obesity or trauma can precipitate the formation of osteoarthritis owing to heightened catabolic activity, chondrocyte apoptosis/necrosis, and damage to the surrounding collagen network. 29 When the osteochondral unit begins to deteriorate because disease or trauma, the normal process of mechanical load transfer is compromised. Anderson et al. indicated that the shear stress levels increase within the deepest layers of articular cartilage upon degradative change within the osteochondral unit. 31 The finite element data from the study suggested that the alterations in the juxtaarticular stress distribution could lead to concomitant cartilage thinning and subchondral bone thickening.
Current Treatment Options for Osteochondral Defects
Currently available treatment options for osteochondral defects are dictated by the severity of symptoms and defect size (Fig. 2). Initial treatment goals are palliative to manage pain, improve function, and control the structural deterioration of the affected joints. 3 Patients have traditionally been managed noninvasively with analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and weight loss exercise. 32 Intra-articular injections of glucocorticoids, hyaluronic acid, and recently platelet-rich plasma (PRP) can also provide symptomatic relief. However, because these palliative treatment methods do not replace large damaged portions of the osteochondral unit, more invasive treatments are often sought to replace symptomatic partial or full-thickness defects.
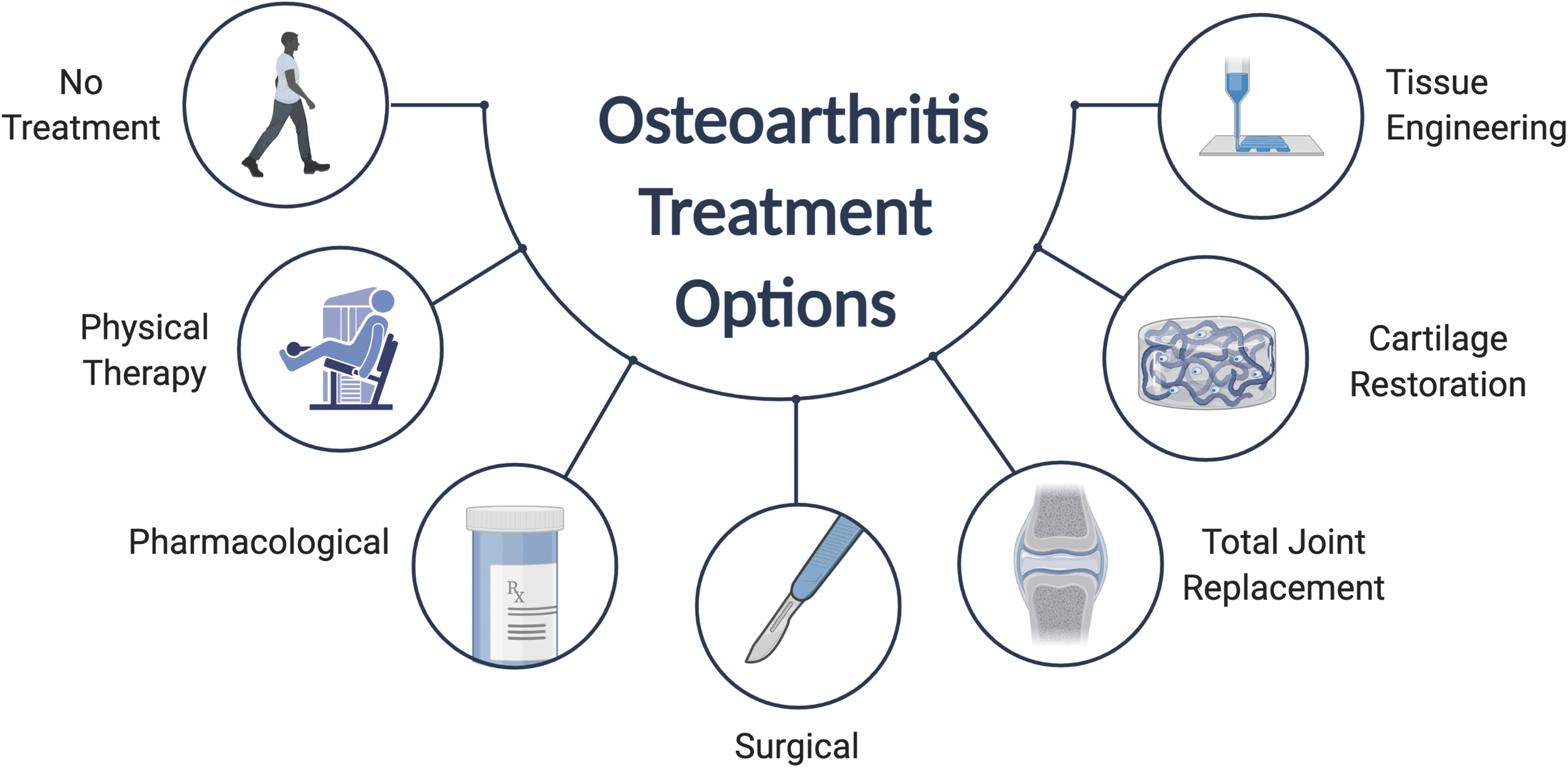
Treatment strategies for osteochondral defects depend on the severity of the defect. The treatment options for early-stage osteochondral defects are generally palliative to manage pain and control the structural deterioration of the affected joints. Noninvasive palliative strategies generally involve physical therapy, analgesics, and NSAIDs. However, late-stage osteochondral defects require reparative treatment options that can replace partial or full-thickness osteochondral defects. Microfracture or mosaicplasty is often the first surgical procedure considered to repair the defect site of <2 cm. Osteochondral allografts are generally attempted as a single-stage technique to address large osteochondral defects involving extensive subchondral bone loss. NSAIDs, nonsteroidal anti-inflammatory drugs.
Marrow stimulation techniques, such as microfracture, are often the first surgical procedures considered to treat smaller defects (<2 cm2). 33 Microfracture surgery is often considered for the initial intervention because it is minimally invasive, has a well-documented track record of success, and is relatively inexpensive compared with other surgical options. 34 This procedure first involves the removal of the damaged cartilage and calcified cartilage layer. Subsequent drilling into the subchondral bone allows bone marrow and blood to permeate into the osteochondral region, which ultimately promotes repair and regeneration. However, the procedure is contraindicated when there is global cartilage degeneration, an open defect that cannot maintain clot formation, and inability to comply with weight-bearing restrictions after the procedure. 35 Marrow stimulation is ideal for small, contained, and isolated osteochondral lesions.
Osteochondral autograft transfer is another well-established surgical technique to repair small to mid-sized cartilage defects. 36 The procedure involves transplanting cylindrical autologous grafts extracted from the nonweight-bearing areas of the knee joint. 37 Mosaicplasty is a similar surgical technique that implants multiple full-thickness “plugs” into a large-sized osteochondral lesion. As a one-stage procedure, mosaicplasty has demonstrated favorable success rates in treating full-thickness osteochondral defects of <2.5 cm2. 38 One 10-year clinical study demonstrated that patients experience a poor outcome 40% of the time, but a subgroup involving younger men with a defect size <3 cm2 experienced a failure rate of only 12.5%. 39 Hangody and Fules also observed good to excellent postoperative results in ∼90% of the patients who underwent femoral condyle or tibial plateau mosaicplasty for up to 10 years. 36 Nonetheless, the outcomes still varied greatly because of age, gender, and defect size, as the failure rates were higher among women, individuals older than age 40, and those with large defects. 39
Autologous chondrocyte implantation (ACI) is a surgical technique that harvests the patient's own chondrocytes to be implanted into osteochondral defects. Although this two-stage procedure is more surgically invasive and highly expensive, the first iteration of this procedure has demonstrated success in younger patients who possess a single defect exceeding 2 cm2. 40 One long-term follow-up study demonstrated that treating large, full-thickness cartilage defects with first-generation ACI significantly improved pain relief and functional rehabilitation within patients. 41 However, treatment complications, including periosteal hypertrophy, graft delamination, arthrofibrosis, and graft failure have led to a significant rate of reoperation after the initial procedure. 42 Advances in various regenerative strategies have prompted the development of enhanced ACI techniques. Unlike first-generation ACI, matrix-assisted autologous chondrocyte implantation (MACI) involves the expansion and placement of autologous chondrocytes on a matrix, which is implanted inside the defect to assist osteochondral regeneration. 43 The MACI procedure is technically easier to perform and has mostly replaced ACI in the United States. Although long-term data for MACI is still limited, Kreuz et al. recently demonstrated in a 12-year follow-up study that patients who received MACI exhibited significant increases in clinical outcome and function. 44 In addition, >70% of the patients within the study reached near normal values upon radiological evaluation, further suggesting that MACI has great potential as a long-term cartilage repair procedure. However, ACI and MACI cannot address any bone deficiency and may not be the ideal treatment for defects with significant osseous involvement.
Finally, allografts provide surgeons with the flexibility to treat larger defects when the defect size is exceedingly large or previous surgical repair attempts have failed. 45 Osteochondral allografts are generally attempted as an one-stage procedure to address large-sized defects and can also address extensive subchondral bone loss. 46 Levy et al. achieved a 82% graft survivorship at 10 years in patients who underwent osteochondral allograft transplantation of the femoral condyle. 47 However, the study also suggested that individuals younger than 30 years of age with no more than one prior surgical operation were the best candidates for allograft procedures. Old age, osteoarthritis, and bipolar allografts have all been suggested to increase the failure rate of these procedures.48,49 In addition, allograft transplantation have increased the risk of disease transmission from the allograft. 50 As allografts become more common as a restorative procedure to treat knee pathologies, more investigations will be needed to better determine their viability of an osteochondral restorative option.
Fabrication of the Interface Layer Within Multiphasic Osteochondral Scaffolds
Tissue engineering is a promising strategy that could offer potential solutions to regenerate the osteochondral complex that current treatment solutions cannot accomplish (Fig. 3A). Cells, bioactive signals, and scaffolds generally make up the foundation of most osteochondral tissue engineering approaches. 4 In general, most strategies are classified as either a scaffold-free strategy or a scaffold-based strategy.
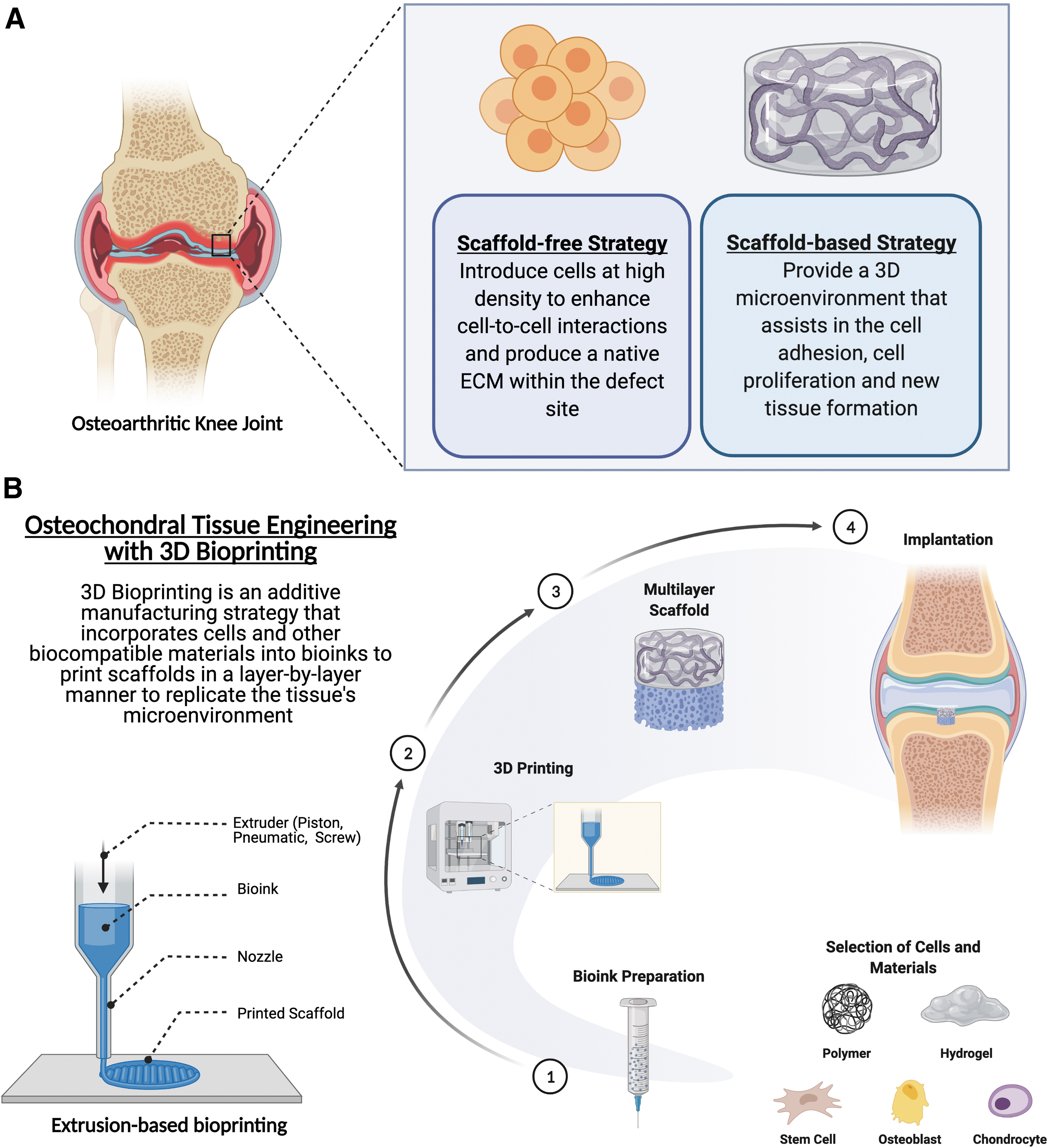
Scaffold-free osteochondral regeneration is an attractive option owing to minimal preparation procedures, optimized time and cost, and minimal risk of material rejection by the body. The essence of scaffold-free tissue engineering is to introduce cells at a high density as a cell sheet or spheroid to enhance cell-to-cell interactions and produce a native ECM within the defect site. 51 Nonetheless, this strategy is susceptible to failure because of decreased mechanical strength and instability. In addition, the inability for scaffold-free strategy to maintain a tight connection with the native tissue highlights the fact that proper fixation is critical to the success and proper load transfers between the cartilage and bone layers. 52
A scaffold-based tissue engineering strategy conversely provides a 3D microenvironment that assists in cell attachment and proliferation, cell differentiation, and new tissue development. The scaffold should ideally be porous and have interconnected pore structure for proper cell migration, growth, and nutrient/waste transport. 53 Table 1 provides a summary of scaffold-based interface tissue engineering strategies for osteochondral regeneration.54–75 Early design of osteochondral scaffolds was primarily monophasic and homogenous in makeup. 76 The porosity and structure within these scaffolds are uniform throughout the construct, but recent studies have demonstrated that these single-phase scaffolds cannot sufficiently regenerate the anisotropic and biomechanical properties of the osteochondral unit. 77 Because this complex exhibits depth-dependent mechanical heterogeneity throughout its ECM, the osteochondral scaffolds require up to three distinct layers—the articular cartilage, calcified cartilage, and subchondral bone layers—that guide the infiltrating cells through layer-specific mechanical stimuli. It has been well established in the literature that each tissue has a characteristic stiffness that affects tissue development by directing cell behavior and matrix protein production. 29 Furthermore, mesenchymal stem cells (MSCs) have been shown to be highly mechanosensitive and respond to stiffness and mechanical loading to influence signal transduction pathways dictating stem cell fate. 78 Therefore, coordinating the interplay of biomaterials and cells by varying the mechanical properties, such as material stiffness, could assist in the regeneration of the osteochondral unit.
Scaffold-Based Interface Tissue Engineering Strategies for Osteochondral Regeneration
μCT, micro-computed tomography; β-TCP, β-tricalcium phosphate; 3D, three-dimensional; ACECM, articular cartilage extracellular matrix; BG, bioactive glass; BMS, bone marrow stimulation; BMSCs, bone marrow stromal cells; CDA, calcium-deficient apatite; CHIT, chitosan; ECM, extracellular matrix; GAGs, glycosaminoglycans; hASC, human adipose-derived stem cell; Ica-HA, icariin-conjugated hyaluronic acid; MRI, magnetic resonance imaging; MSC, mesenchymal stem cell; PCL, polycaprolactone; PEG, polyethylene glycol; PHB, polyhydroxybutyrate; PLA, polylactic acid; PLGA, poly(lactic-co-glycolic acid); RCT, randomized clinical trial; ScB, subchondral bone; StarPEG, star-shaped poly(ethylene glycol); TIPS, thermal-induced phase separation.
More recent efforts to regenerate the osteochondral tissue have resorted to biphasic or multiphasic scaffolds. The multiphasic nature of an osteochondral implant has required the use of multiple materials or varied structural organization of the scaffold to replicate the complex architecture of the osteochondral unit. Kunisch et al. designed a bizonal cartilage scaffold utilizing a polyethylene glycol (PEG)/heparin-based hydrogel system.
66
The spaciotemporal design of the casted hydrogel system supported articular chondrocytes in the superficial layer and MSCs in the deep cartilage layer, which helped maintain the bizonal organization to match the cellular organization within articular cartilage. Jin et al. demonstrated the potential to regenerate osteochondral tissue utilizing stackable cell sheets precultured on an electrospun fibrous mesh.
71
Bone marrow MSCs were precultured on fibrous meshes consisting of poly (
3D Bioprinting the Interface Layer Within Osteochondral Scaffolds
The use of 3D bioprinting has recently received much attention as a potential strategy to fabricate osteochondral scaffolds (Fig. 3B and Table 2).79–87 This technique helps combine cells, growth factors, and biocompatible materials within a bioink, which then can be precisely laid down layer-by-layer into a biomimetic structure. 88 Therefore, 3D printing can more readily fabricate the complex zonal organization with distinct biomechanical properties of the osteochondral unit. Because numerous 3D printing strategies are available, the selection of a bioprinting strategy most suitable for osteochondral regeneration depends primarily on the processing conditions, material type, and scaffold design. 89
Three-Dimensional Bioprinting Strategies for Osteochondral Interface Tissue Engineering
ALG, alginate; AlgMC, alginate methylcellulose; BM-MSCs, bone marrow mesenchymal stem cells; CS-AEMA, chondroitin sulfate/2-aminoethylmethacrylate; CPC, calcium phosphate cement; GelMA, gelatin methacryloyl; hAC, human articular chondrocytes; HAMA, hyaluronic acid methacrylate; HAP, hydroxyapatite; hDZCs, human deep zone chondrocytes; MEW, melt electrowriting; PLGA, poly(lactic-co-glycolic acid); SC, sodium citrate; ZCC, zone of calcified cartilage.
Extrusion-based bioprinting, which utilizes pneumatic or mechanical force to precisely deposit material layer by layer, has demonstrated promise to create scaffolds with the distinct heterogeneous zonal architecture within the osteochondral unit. Guo et al. demonstrated that a multilayer cartilage scaffold, fabricated with poly(
Kosik-Koziol et al. utilized an extrusion-based bioprinter configured with a coaxial needle to engineer the calcified cartilage layer within a hydrogel scaffold system embedded with β-tricalcium phosphate (β-TCP) particles. 85 The composite alginate (ALG)/gelatin methacryloyl (GelMA) bioink optimized the gelation process for high-resolution printing and introduced the cell-binding motifs. The optimized hydrogel system consisting of 0.5% of β-TCP particles appeared to demonstrate the potential to modulate the bone marrow mesenchymal stem cells (BM-MSCs) toward the formation of calcified cartilage. Although the multilayered scaffold was not examined in this particular study, another group utilized a similar bioink formulation to recapitulate the different cartilage zones within a single construct. 84 The extrusion-based bioprinter was configured with a microfluidic device to help vary composition within each layer and induce heterogeneous differentiation of cells. The results demonstrated that the coculture of MSCs and chondrocytes appeared to yield a more hyaline-like phenotype than culturing MSCs alone.
To fully capitalize on the advantages offered by 3D printing for osteochondral regeneration, several technical challenges still need to be overcome. Some of these challenges include issues with incorporating multiple materials into the bioink, nozzle clogging, optimizing the bioink, and dealing with the sensitivity of bioinks to processing parameters. 91 You et al. utilized sodium citrate as a dispersant to evenly distribute HAP within ALG hydrogel. 82 This homogenous ALG/HAP composite hydrogel helped promote chondrocytes to exhibit greater amounts of collagen X, which is characteristic of calcified cartilage. The use of dispersant could ultimately improve the mineralization capability and 3D printing outcomes.
In addition, the integration between the osteal and chondral layers could be essential for the success of engineered osteochondral scaffold. Delaminated cartilage grafts have consistently compromised the outcome of the defect site repair on numerous occasions because of inadequate integration. 92 When it comes to biphasic osteochondral scaffolds, most have been integrated by suturing, gluing, or crosslinking.93–95 Although these integration strategies fail to fully satisfy the mechanical requirements of the osteochondral scaffold, they are still readily relied on to integrate the bone and cartilage layers. Therefore, more fabrication strategies have to be examined to improve the integration within biomimetic, multilayer osteochondral scaffolds. 79
Effectively integrating the cartilage and bone regions with an interface layer is critical for the success of osteochondral scaffolds, because engineered cartilage have been shown undergo delamination and ultimately jeopardize cartilage repair. 96 Although suturing, adhesives, and chemical crosslinking have been utilized to augment the integration within biphasic osteochondral scaffolds, these methods still fail to achieve the levels of integration necessary for osteochondral integration.93,97 Therefore, engineering an osteochondral interface requires a strategy that facilitates the load bearing and stress distribution experienced within this region.
Strategies to Enhance Biomechanics of Bioprinted Osteochondral Scaffolds
Adhesion can simply be described as the two-dimensional adherence of two materials to each other, and much of the insight pertaining to it comes from studying adhesives and adhesion bonds over the years. Although the interaction between adhesive and adherent layers within an adhesive system takes place at different levels of scale, most of these interactions act on the molecular or atomic level. 98 To date, there is still no consensus on the theories of adhesion or on the mechanisms involved. Conventional adhesion theories postulated that adsorption, diffusion, electrostatic reactions, and mechanical interlocking best described the mechanisms involved during adhesion. 99 However, additional theories of adhesion have gained traction in recent years to supplement the previous explanations to include wettability, chemical bonding, acid-base, and weak boundary layer theories. 98 All these mechanisms are essential to adequately describe an adhesive system, because no single mechanism can completely describe an adhesive system. In addition, the role each mechanism plays will vary within each adhesive system.
Although there is plenty of evidence that a modified contact surface improves adhesion, there are still questions as to whether mechanical interlocking can create strong bonds between the adhesive and adherent layers. Some have postulated that increasing the contact surface on a substrate can heighten other adhesion mechanisms through the formation of a clean reactive surface and increase in overall surface area. 100 These modifications consequently alter the physical and chemical properties of the substrate surface, such as wetting and chemical bonding, to increase the adhesion within the system. In 2006, Romito and Ameer engineered osteochondral scaffolds that could recreate the interfacial structure and biomechanics of articular cartilage. 101 The composite scaffold was created from a nonwoven PLLA mesh mechanically interlocked to a solid core at a microscopic level and seeded with bovine articular chondrocytes. The biochemical and histological analyses demonstrated that these constructs supported the development of a cartilage ECM for at least 6 weeks in vitro with improved adhesion strength, whereas a scaffold without the interface achieved <5% of this adhesion strength. These results suggested that mechanical interlocking should be utilized as an adhesive mechanism to engineer a multilayer osteochondral scaffold with synthetic materials.
Zhang et al. developed a biphasic osteochondral scaffold with enhanced interfacial integration by 3D printing PEG hydrogel on top of gel-casted β-TCP ceramic scaffold with a stereolithographic printer. 79 Microscopic and scanning electron microscope (SEM) characterization of the interfaces showed that the PEG hydrogels were tightly interlocked within the ceramic scaffold by extending into the pores. The interfacial shear strength of the biphasic scaffolds with a 30% pore area percentage exhibited a threefold improvement compared with that of 0% pore area scaffolds. In an alternative approach, Diloksumpan et al. utilized multiscale printing to integrate a hydrogel-based cartilage layer to a stiff osteo matrix. 86 By combining extrusion-based 3D printing with electrowriting, ceramic-integrated melt electrowriting (MEW) meshes were designed to protrude into the interface region of the composite hydrogel–ceramic scaffold. The interlocking features within these composite scaffolds enhanced structural stability during handling and implantation, as the interface adhesion strength and compressive properties were shown to be superior to the noninterlocking counterparts.
Other adhesive strategies for 3D bioprinted osteochondral scaffolds have been minimal to date. Li et al. designed a triphasic composite scaffold that simulated the full-thickness structure of the osteochondral unit. 81 The composite scaffold was formed utilizing a “dissolved-adhesion technology,” which involved spraying an organic solvent to the surface of the calcified cartilage and chondral phases. Once both surfaces underwent mild dissolution, the anisotropic chondral phase was gently applied onto the bony phase and eventually lyophilized to complete the osteochondral construct. Although the biomechanical tests demonstrated that these composite scaffolds possessed significantly stronger maximum tensile and shear strengths than scaffolds without the calcified cartilage structure, two different fabrication methodologies were utilized in this study, and the adhesive strategy utilized to conjoin the cartilage and bone layers involved manual intervention. Once again, the existing studies (Table 2) provide us with relatively few insights on how adhesive strategies can be utilized in bioprinted interface scaffolds for osteochondral scaffolds.
Conclusion
Both articular cartilage and subchondral bone contribute to the distinct biomechanical properties that maintain the health and aid in load transfer throughout the osteochondral unit. While preemptive treatment of osteochondral defects is essential to successfully manage their associated pathologies or traumatic injuries, existing nonsurgical treatment modalities are palliative in nature and generally just serve to slow down disease progression. In addition, current surgical treatment options present with an abundance of risks, limitations, and expenses. Tissue engineering offers promising solutions to regenerate the osteochondral complex that current treatment solutions cannot accomplish. 3D bioprinting especially has demonstrated the capability to create multilayered scaffolds with heterogeneous properties that recapitulate the native osteochondral architecture and composition. Most of the literature retrieved for this review demonstrates the potential to develop an osteochondral interface that enhances the biomechanics of the scaffold. Future studies will improve upon the interface layer that can improve the biomechanics within multilayered scaffolds for enhanced osteochondral regeneration.
Footnotes
Acknowledgment
Figures were created with Biorender.com
Disclosure Statement
No competing financial interests exist for all authors.
Funding Information
The authors acknowledge support by the NIBIB/NIH Center for Engineering Complex Tissues (P41 EB023833) and MPowers Graduate Fellowship program.