
Abstract
Type 1 diabetes (T1D) is caused by low insulin production and chronic hyperglycemia due to destruction of pancreatic β-cells. Cell transplantation is an attractive alternative approach compared to insulin injection. However, cell therapy has been limited by major challenges, including life-long requirement for immunosuppressive drugs to prevent host immune responses. Encapsulation of the transplanted cells can solve the problem of immune rejection, by providing a physical barrier between the transplanted cells and the recipient's immune cells. Despite current disputes in cell encapsulation approaches, thanks to recent advances in the fields of biomaterials and transplantation immunology, extensive effort has been dedicated to immunoengineering strategies, in combination with encapsulation technologies, to overcome the problem of host's immune responses. This review summarizes the most commonly used encapsulation and immunoengineering strategies combined with cell therapy, which have been applied as a novel approach to improve cell replacement therapies for management of T1D. Recent advances in the fields of biomaterial design, nanotechnology, as well as deeper knowledge about immune modulation had significantly improved cell encapsulation strategies. However, further progress requires combined application of novel immunoengineering approaches and islet/β-cell transplantation.
Impact statement
Cell encapsulation shows promising potential in preventing host's immune responses and rejection of islets or β-cells by providing a selectively permeable barrier between the host and the transplanted cells. Innovative materials, conformal nanocoatings, and immunomodulation have provided promising approaches in the field of encapsulation technology. Novel nanocarriers have been synthesized to release and deliver immunosuppressive agents to islets/β-cells within the capsules in a controlled manner. The immunoengineering approach (immunosuppressive and immunomodulatory agents) could overcome the challenges of cell replacement therapy in type 1 diabetes.
Introduction
Insulin injection and blood glucose monitoring are the standard routine management for type 1 diabetes (T1D). Islet transplantation is an attractive alternative approach toward achieving insulin independence in T1D patients. In this approach, the extracted islet cells from the donor's pancreas, are transplanted to the T1D patient in a minimally invasive manner. 1 Results from a clinical trial in 2006 showed that insulin withdrawal following islet transplant was observed in 36% of T1D patients, while transplant failure occurred in 22% of patients. 2
Islet cell transplantation failure may occur due to islet loss, immediately following transplantation (transplant failure) or through the autoimmune-mediated cell rejection process. An efficient encapsulation device or membrane could provide a physical barrier between the donor's islet cells and the recipient's immune system. To this end, immunoengineering strategies using immunosuppressive or immunomodulatory agents have been studied to lower the recipient's immune reactions and prevent the formation of fibrotic tissue that yielded promising results. 3
This review provides a closer look at the concept of immunity in cell/islet transplantation and the complicated immune responses against transplanted cells/islets. Next, we focus on different cell encapsulation technologies and devices that have been applied using the immunoengineering approach to overcome the challenges of cell replacement therapies in T1D.
Immunity in Cell/Islet Transplantation
The two main immune-related challenges in islet/cell transplantation are allogeneic rejection through host's autoimmunity and subsequent foreign body reaction (FBR) against pancreatic insulin-producing cells. The instant blood-mediated inflammatory reaction (IBMIR) occurs as soon as the islets come in direct contact with the recipient's blood by transplantation through the portal vein. 4 IBMIR involves activation of the complement cascade and subsequent coagulation factors, which leads to islet disruption due to massive leukocyte infiltration. Islet disruption involves innate and adaptive immunity.
The innate immunity is responsible for early rejection of the transplanted islet graft, as the result of the accumulation of the innate immune cells (including neutrophils and macrophages) and subsequent inflammatory cytokine release at the site of transplant, leading to acute inflammation This process is accountable for 80% of transplanted islets failures. 5 During allogeneic rejection, soluble proinflammatory mediators (including tumor necrosis factor-alpha [TNF-α] and interleukin-1beta [IL]-1β) are released from the transplanted islets and activated immune cells, promoting further neutrophil and macrophage recruitment at the site of the transplant (Fig. 1).
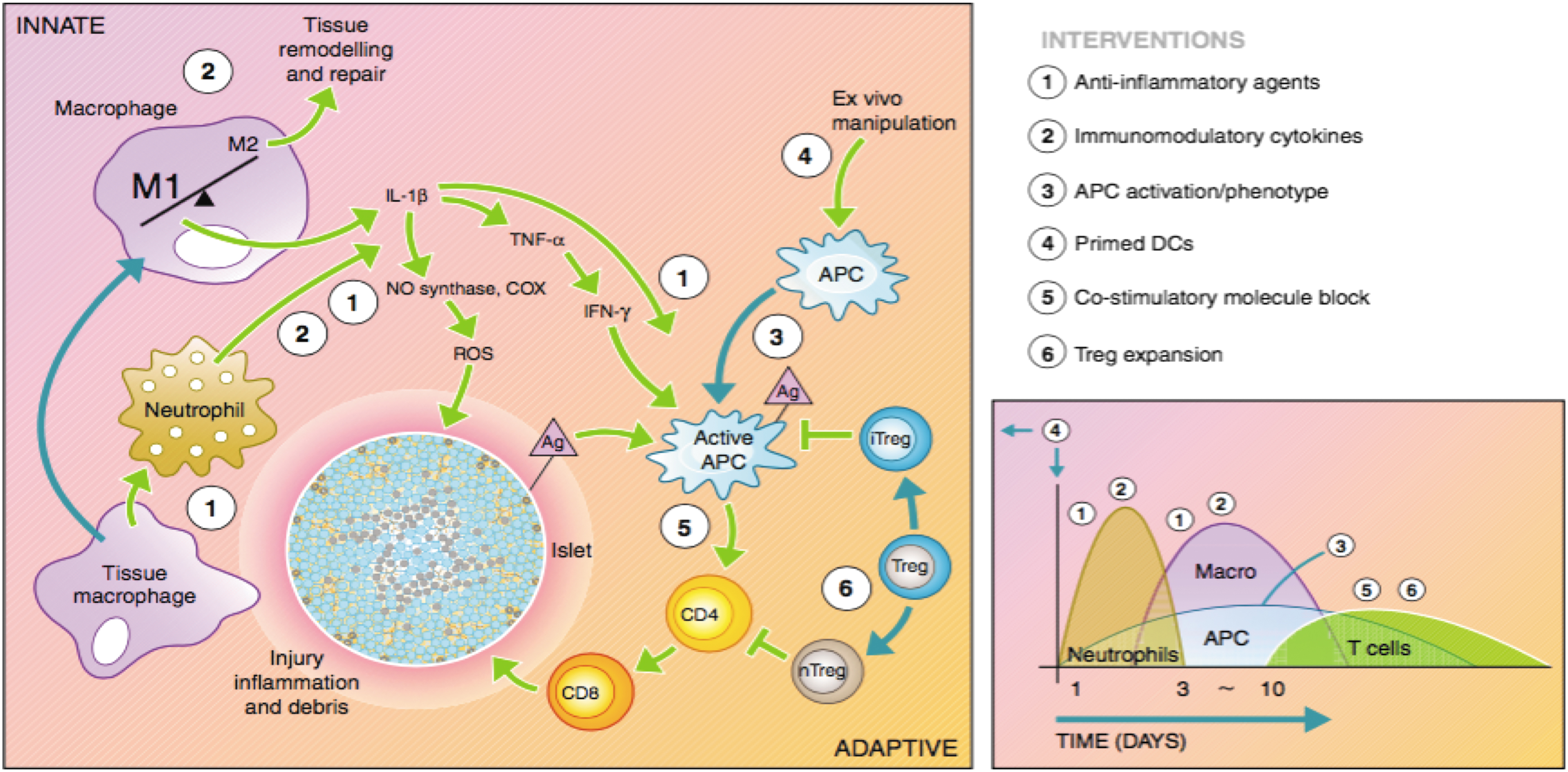
Immune responses to pancreatic islets after transplantation. The host's immune responses comprising the innate and adaptive immunity are presented in this figure. Activation of tissue macrophages and neutrophils following injury leads to subsequent release of inflammatory cytokines to activate APCs, CD4+ T, and CD8+ T helper and cytotoxic T lymphocytes. The diagram on the right shows the timeline and the types of penetrating immune cells at the site of xenograft transplantation. APC, activation of the protein C. Reprinted with permission from Gibly et al. 109 Copyright (2015), European Society of Endocrinology. Color images are available online.
The adaptive immune responses start within few days following islet transplantation and are the main cause of long-term disruption of the transplanted insulin-producing cells. Islet allograft expresses histocompatibility allogeneic antigens, which provoke the recipient's humoral and cellular immune reactions, as a foreign graft. Meanwhile, islet transplantation into a T1D patient can trigger autoimmunity. 6 The contribution of innate and adaptive immunity to islet/cell transplant rejection is illustrated in Figure 1. Activation of both alloimmune and autoimmune responses cannot be easily managed with routine immunosuppressive regimens, which highlights the importance of designing novel immunomodulating therapies.
Encapsulation Technology
Encapsulation provides a physical barrier that protects the transplanted insulin-producing cells from the recipient's immune responses, which in turn can eliminate the need for immunosuppressant drugs.7–10 Encapsulation of pancreatic islets is the most commonly used approach in this regard. 11 An ideal semipermeable barrier encapsulating the islet cells should have the following properties: (1) allows diffusion of nutrients, oxygen, glucose, insulin, as well as cellular waste; (2) prevents the transport of large immunoreactive cells 12 ; and (3) is biocompatible. 13
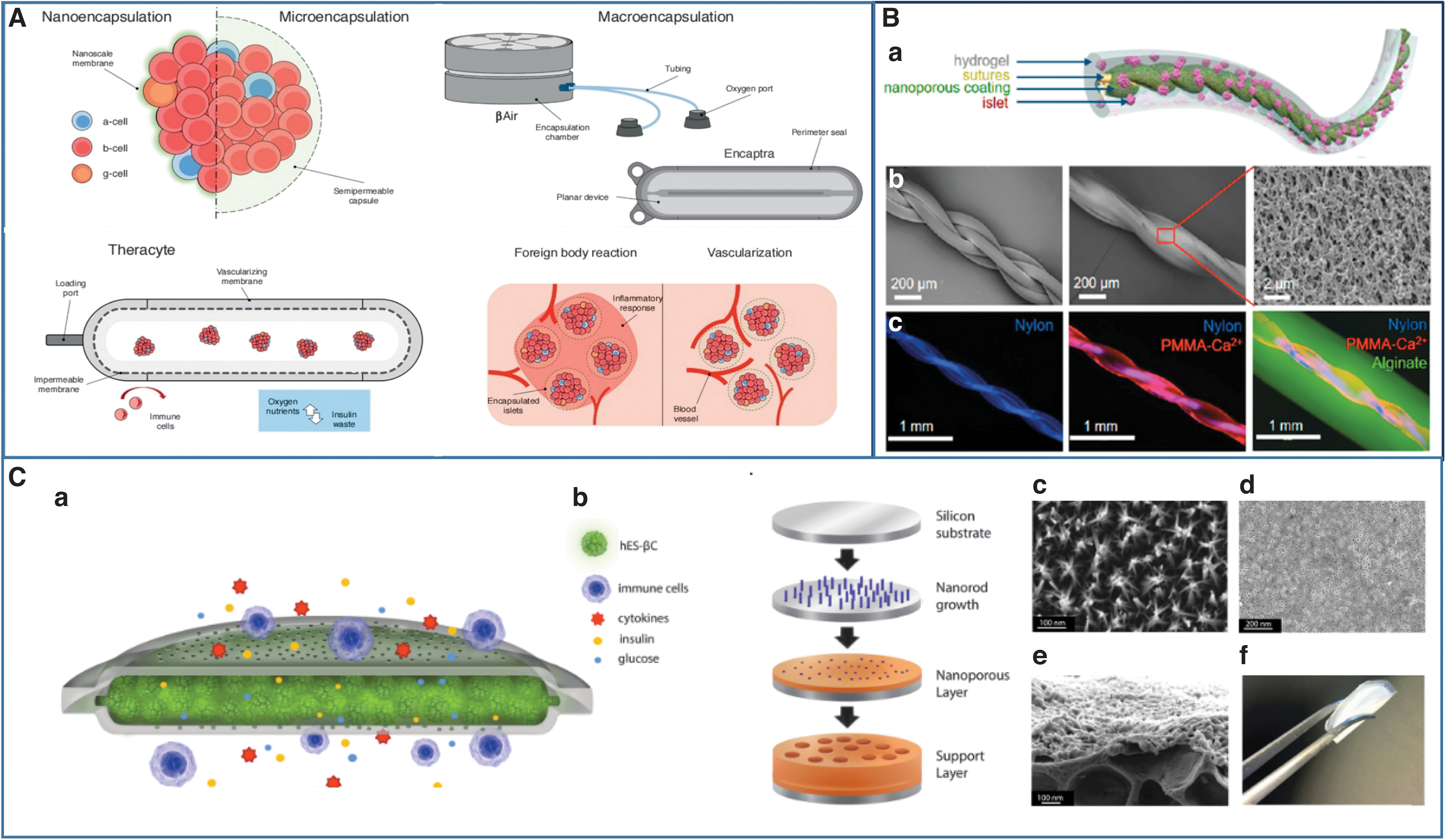
The encapsulation strategies are categorized into three groups: (1) macroencapsulation, (2) microencapsulation, and (3) nanoencapsulation or conformal coating (Fig. 2A). Unlike micro/nanodevices, macro devices are easy to access, are retrievable, and provide adaptable thickness, size, and porosity. However, due to their macrosize and reduced surface area to volume ratio, there are limitations in cell/islet oxygenation, as well as effective nutrient/insulin diffusion, which can be solved by using micro/nanoscale devices. 14
Macroencapsulation devices
Macroscale encapsulation devices incorporate more islets compared to microscale and nanoscale devices. 15 The macro devices include planner membranes, 16 hollow fibers, 17 and macrocapsules.18–20 The biomaterials used for developing these devices include alginate, polysulfones, agarose, and the copolymer of acrylonitrile and vinyl chloride. Macro devices can be used at different transplanted sites and are categorized into two groups: extravascular and intravascular. 21
Extravascular macro devices have no direct connection with the recipient's vasculature system and are transplanted in the peritoneal cavity, subcutaneously or at the omental poach. 22 In this case, the transplanted device becomes vascularized over time. Having no direct contact with the host's vasculature system is one of the main disadvantages of extravascular devices, which increases the risk of islet necrosis. 9 On the other hand, intravascular devices provide direct contact between the islet cells and the recipient's vascular system, but implantation of this device is also associated with greater risks because it can disrupt the vascular system in the transplant recipient due to the risk of clots and blockage of arteries, and the unsuccessful results of this type of device caused it to be no longer studied. 9
In the recent decade, great advances have been achieved in developing efficient macro devices and their commercialization. The device produced by Islet Sheet Medical is one of these examples, which is made of three layers of alginate. The middle layer consists of a mixture of islet cells and alginate, while the two external layers contain alginate alone. 23 Encaptra, a single-membrane system developed by ViaCyte started a clinical trial in 2015 by using human embryonic stem cells (hESC)-derived pancreatic progenitors 24 ; however, results have not yet been reported. Theracyte™ is another commercialized device (Fig. 2A) made of a thin polymeric chamber that could prevent hyperglycemia in animals. 25
Another clinical trial was performed on a 43-year-old diabetic patient who received islets in the BioHub system, a company with the approach of creating an engineered site in the body for the optimum survival and function of transplanted islets and insulin-producing cells, which resulted in normoglycemia for 12 months. 26 Weaver et al. studied islet encapsulation by a polyethylene glycol (PEG) hydrogel macro device. Encapsulated islets in this device showed high viability in vitro and significant vascularization around transplanted graft in vivo, which provided enhanced islet survival. 27 An et al. introduced a retrievable and scalable islet encapsulation device (Thread-reinforced alginate fiber for islets encapsulation [TRAFFIC]) that can be implanted in a minimally invasive manner and showed its mechanical strength, suitable mass transfer, and durability in different T1D animal models (Fig. 2B).
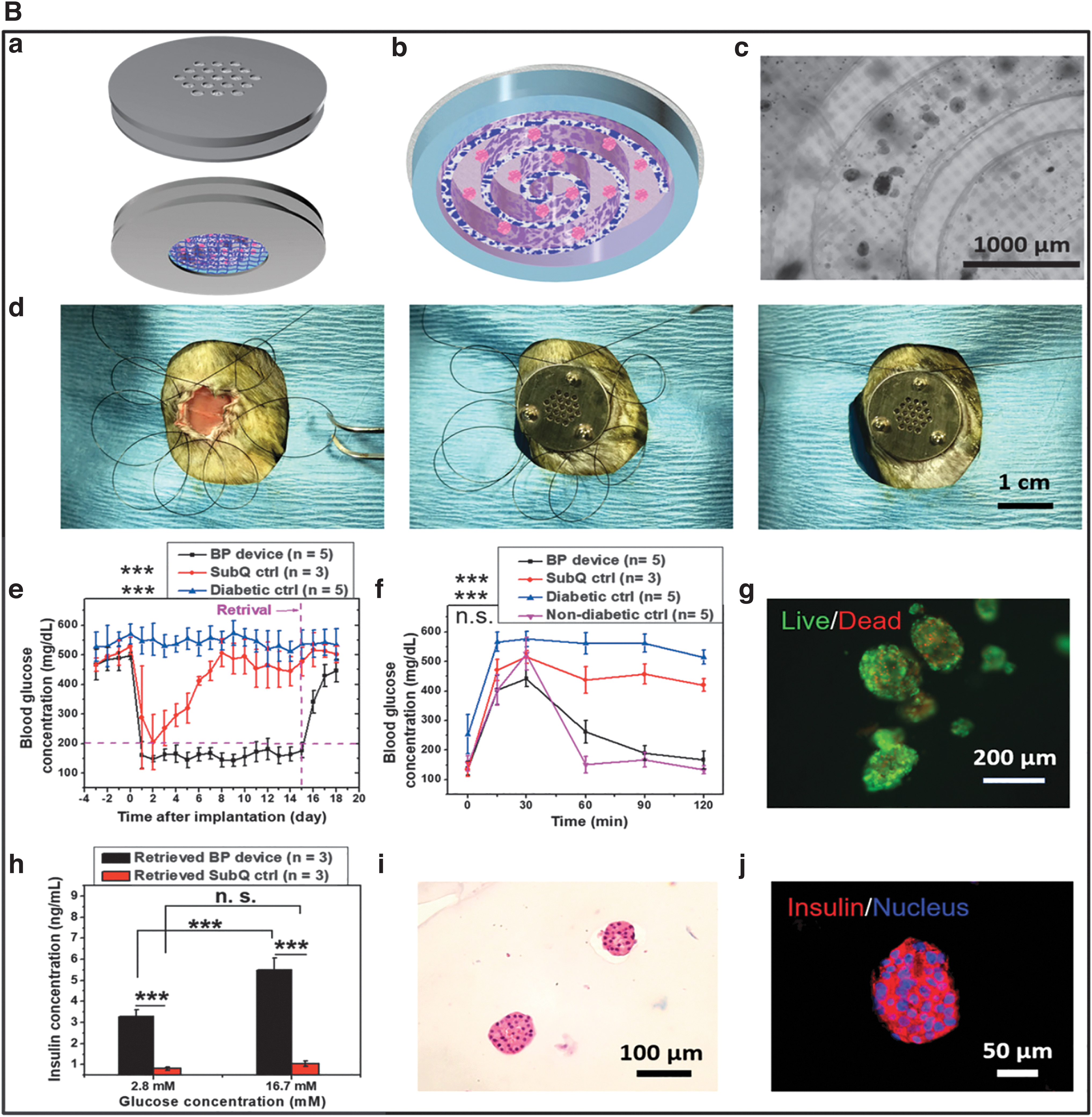
Also, transplantation of stem cell (SC)-derived β-cells by a nanoscale porous immune-protective device was evaluated in 2017 (Fig. 2C). Application of this macro device eliminated the host's immune responses, while allowing the proper exchange of oxygen and nutrients, and enhancing cellular viability and performance in vitro and in vivo. 28 Recently, encapsulation by elastomer-reinforced interconnected toroidal hydrogels was studied by Ernst et al. (Fig. 3A). Implanting this donut-shaped device in a diabetic mouse model for 12 weeks showed promising results for potential clinical application due to suitable mass transfer and complete retrievability. 29
Encapsulation of transplanted cells can overcome numerous shortcomings of current cell-based therapeutical approaches, including preventing the need for the administration of immunosuppressants. However, the challenge of low oxygen supply to the encapsulated cells has remained unresolved. 30 To address inadequate oxygenation, oxygen delivery from an external source can be incorporated. βAir from Beta-O2 Technologies contains (Fig. 2A) a chamber filled with islet and alginate, and provides an oxygen supply system for daily oxygenation of islets. 31 This system could normalize the blood glucose level in diabetic pigs for several months.32,33 A clinical trial started in 2012 using the βAir device in a 63-year-old patient and attained normoglycemia for 10 months. 34
A recent study by An et al. was performed using a modular transcutaneous biphasic cell delivery device for providing unlimited oxygen supply using a perfluorocarbon carbon oil-infused nanomembrane interface. The therapeutic potential and encapsulation efficiency of this cell delivery system were evaluated for islet transplantation in a diabetic rodent model (Fig. 3B). 35
Microencapsulation
In this approach, islets are individually encapsulated in a three-dimensional (3D) microcapsule with <1 mm diameter. 36 The biocompatibility of materials used to synthesize these devices is critical. Using poorly biocompatible materials leads to the formation of fibrosis around the microcapsules, which can disrupt the islets' oxygenation and nutrition supply leading to transplant failure. 37 Different biocompatible polymers, including chitosan, alginate, PEG, agarose, collagen, alginate, dextran, and hyaluronic acid, have been previously used for microcapsule fabrication. 38
Alginate-poly-
Nevertheless, different microencapsulation approaches have been used in animal models and clinical trials until today. Several studies in nonhuman primates (NHPs) have proved the efficacy of microencapsulated islets in controlling blood glucose levels.49,51,56 In a study by Soon-Shionget al., transplanted microencapsulated islet cells transplanted into a T1D patient could maintain normoglycemia for 9 months. 8 In another study, microencapsulated islets transplanted into four patients reduced exogenous insulin intake requirement. 53 More recently, Ca2+/Ba2+ alginate microcapsules containing islet cells (300,000 islet equivalent [IEQ] [an islet of diameter 150 μm]) were implanted into the omental poach of a diabetic female patient. Although no reduction in exogenous insulin uptake was observed, microcapsules remained fibrosis free. 54
Hydrogel encapsulation is another promising approach for providing immunoprotection in micro devices. Alginate has been the most commonly used biomaterial in hydrogel microcapsules for islet encapsulation, due to its low cost, simple preparation process, low toxicity, and high durability. 53 However, since alginate has a foreign origin, it can be the target of fibrosis, which will lead to transplant failure. In this context, native, biocompatible biomaterials with lower chance of fibrosis, as biomimetic scaffolds, have gained researchers' attention for islet transplantation. The extracellular matrix (ECM) components provide physical and biochemical support and are essential for maintaining cell survival and function. 57
Disruption of the ECM during cell transplantation has a negative impact on the graft's durability and performance, due to loss of cellular hemostasis, pathological ECM remodeling following cell transplantation, and host-triggered immune responses. It has been shown that islet cell survival and performance following transplantation are significantly dependent on the integrity of the ECM. 46 Type I collagen (COLI) is one of the main ECM components that becomes disrupted during islet cell isolation from the donor's pancreas.58–60
Different research groups have studied COLI-based hydrogels for islet transplantation in the recent years. Zbinden et al. reported on the benefits of co-culturing endothelial cells and β-cells with COLI on the improvement of cell survival and graft performance in post-transplantation hypoxic conditions. 61 Salamone et al. prepared a 3D COLI-based hydrogel incorporating adipose-derived microvascular fragments (ad-MVF) for induction of vascularization following islet transplantation in vitro. Their results showed that this hydrogel system improves cellular engraftment and vascularization. 62
In another recent study, a collagen-chitosan hydrogel was prepared and its angiogenic properties were evaluated in T1D mice following islet transplantation. According to their results, a significant increase in the levels of proangiogenic cytokines was observed 6 weeks following subcutaneous islet transplantation. 63 Primavera et al. 64 prepared a collagen-PDMS scaffold incorporating dexamethasone microplates. Collagen coating with PDMS improved scaffold's biocompatibility, while the sustained release of dexamethasone from the microplates reduced inflammation at the site of the transplant without affecting islet functionality and insulin release. Implanted T1D mice showed normoglycemia within 4 days following transplantation and the obtained glycemic control was maintained for 30 days.
Nanoencapsulation
Nanoscale polymer coatings have been recently applied for the encapsulation of individual islets (1–100 nm). The Layer-by-Layer (LbL) technique, which employs negatively and positively charged polymers, is the most commonly used nanoencapsulation approach for islet encapsulation. Minimized capsule's thickness, leading to efficient oxygen diffusion and increased islet viability, is the main advantage of this technique. Other advantages include reducing the total volume of islets22,65–67 and improved glucose/insulin exchange.68,69 However, in some cases, the islets are not fully protected from the recipient's immune cells, which may result in early rejection. 70 PEG, which is a common polymer used in the conformal coating of islets, stimulates insulin production in high glucose concentrations.71–73
In 2018, Syed et al. showed that chitosan and poly (sodium styrene sulfonate)-nanoencapsulated human islets could maintain long-term insulin production in the normal range in response to high glucose concentrations in diabetic mice. 74 Heparin nanoencapsulated islet transplantation in NHPs has been shown to significantly reduce inflammatory mediators of IBMIR in the blood. 75 However, a 6-month clinical trial carried out on two patients, who received nanoencapsulation islet transplants, did not result in normoglycemia and insulin injection withdrawal. 76 More recently, Stock et al. showed that nanocoated islets derived from SCs (SC islets) show similar functionality as of nonencapsulated SC islets in vitro. 77
Immunoengineering-Based Biomaterials for Modulating the Immune System
Although islet encapsulation can prevent immune responses against allograft antigens, the FBR induced by the host's immune reaction, against capsule biomaterials, is still a great challenge in the survival and performance of transplanted islets. 78 The formation of FBR around the encapsulated islets leads to inflammatory responses, which subsequently prevent oxygen and nutrient diffusion into the islet graft and result in transplant failure. A previous study has shown that the properties of the capsule's biomaterials play a key role in FBR formation. Indeed, the high purity and biocompatibility of these materials can reduce immune response's severity and FBR formation. 3
Recent advances in developing novel biomaterials and deeper insights into the host's immune responses have resulted in the development of immunomodulatory biomaterials with cell transplantation applications. The purpose of these novel materials, also known as immune-evasive biomaterials, is to modulate the host's immune responses. Immune-evasive materials are used for attenuating possible inflammatory responses against the implanted xenograft. Microalteration of the biomaterial's properties, including surface chemistry, topology, and geometry, was initially used for reducing the chance of immune-induced xenograft rejection by inhibiting protein accumulation and immune cell adhesion.
Despite the successful application of these materials, more research is required toward finding novel strategies to neutralize the immune system. 3 Functionalization of biomaterials with chemicals or ECM ligands, using immunosuppressive or immunomodulatory agents in combination with encapsulation, and other promising techniques are possible strategies that can provide biomaterial immune evasion, which is summarized in Table 1 and shown in Figure 4.
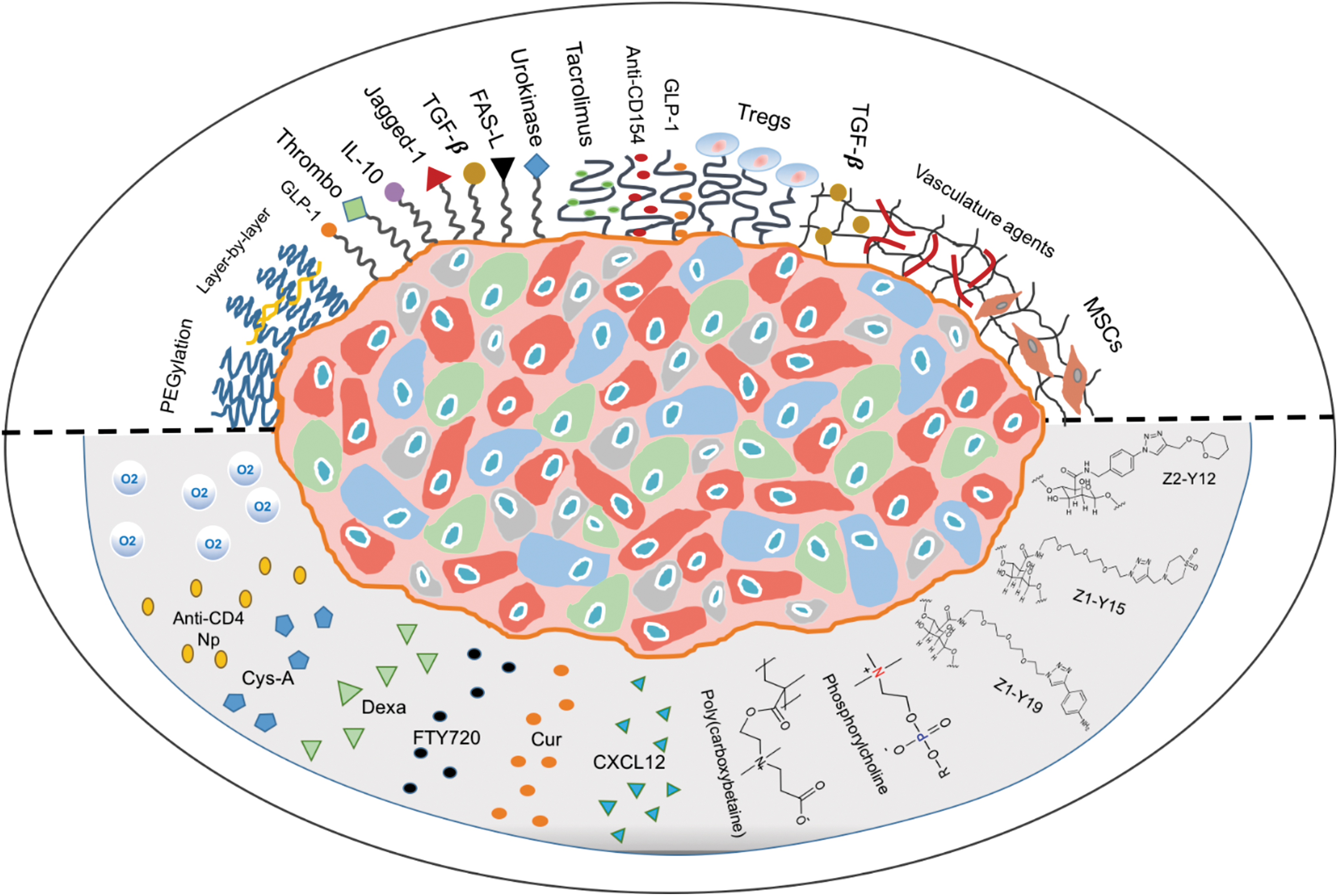
Schematic presentation of the immunoengineering approaches to mitigate the immune response following islet and β-cell transplantation; conformal coating of islets and β-cells (top of the line) with emphasis on designing an immunomodulatory biomaterial by functionalization of the coated surface with bioactive molecules, immunomodulatory agents and cells, immunosuppressive agents, and vasculature agents; chemical modification (down of the line) with three azide group-containing modifications, and zwitterionic polymers, loading of immunosuppressive and immunomodulatory agents into microcapsules, and oxygen generator or carrier that incorporated into the microcapsules. Color images are available online.
Immunoengineering-Based Biomaterials for Modulating the Immune System
IL, interleukin; PEG, polyethylene glycol; PEI, poly ethylene imine; TGF-β, transforming growth factor beta.
Materials that inhibit or modulate the immune system
Functionalization of biomaterials based on chemical modifications is commonly used for modulation of the immune responses against xenografts. Veiseh and colleagues 79 have modified ultrapure alginate using different chemical groups, including amines, alcohols, azides, and alkynes. Quantification of collagen density following subcutaneous implantation of microcapsules in rodents showed that among large combinatorial hydrogel analogs, three azide group-containing modifications (triazole-containing alginate analogs [Z2-Y12, Z1-Y15, and Z1-Y19] formulation) could significantly reduce FBR formation.
Recently, zwitterionic polymers with inherent antifouling properties, as biomaterial's coatings, have gained researchers' interest. Yesilyurt et al. 80 introduced a simple method to coat alginate microcapsules with zwitterionic phosphorylcholine polymer and pendant dithiol-containing co-monomers and performed the first in vivo biocompatibility assessment of the zwitterionic polymer-coated microcapsules (Fig. 5A). However, uncommon cross-linking procedures may limit the application of zwitterionic groups in islet encapsulation. A recent comprehensive study 81 introduced a mild, reproducible, and inexpensive approach for chemical modification of three ultrapure alginates (VLVG, SLG20, and SLG100) using three novel zwitterionic groups: sulfobetaine (SB) and two carboxybetaines (CBs) (Fig. 5B). While SLG100 zwitterionic modification did not affect alginate's physicochemical properties, it prevented cellular overgrowth (CO) in mice, dog and pig models in a long-term implantation period compared to SLG100 alone.

Zhang and colleagues 82 used poly ethylene imine (PEI), a cationic polymer, for preparing zwitterionically modified alginate instead of the chemical modification method. This strategy provides an eco-friendly synthesis process and avoids using chemical cross-linking and toxic reagents, which could disrupt cellular functionality. Their results proved that the prepared hydrogel platform's performance was comparable to other antifibrotic zwitterionic biomaterials since no increase in CO was observed for 4 weeks following alginate/PEI hydrogel implantation. Although using zwitterionic coatings for islet encapsulation has shown promising results, more research is needed on long-term functionality and survival of the encapsulated cell.
Cross-linking of alginate-based microbeads with calcium ions has gained the researcher's attention due to the high in vivo stability of the microbeads. Researchers have studied the chemical modification of alginate using methacrylation 83 and carbamate bond 84 (Fig. 5C). In this approach, the obtained high stability due to the dual cross-linking process improves graft isolation from the body's inflammatory responses. In addition, Bowers et al. 75 introduced a retrievable macroscale membrane that provides all the parameters necessary for the survival of prolonged encapsulation systems, including mechanical strength, vascularization, and immunomodulatory properties.
The outer membrane layer of poly(hydroxybutyrate-co-hydroxyvalerate)-poly(ϵ-caprolactone) (PHBV-PCL) electrospun-based nanofibers was loaded with FTY720, while the interior layer was made from the porcine decellularized dermis (Enduragen®). FTY720 showed immunomodulatory and proangiogenic roles and provided a suitable environment for islet cells' survival and function.
In a recent study by Jeon et al., PEG-dendron was sued for islet surface modification. 85 Based on their results, PEG-dendron modification did not affect islet morphology, survival, or performance, while inhibiting immune responses. They concluded that combinatorial application of PEG-dendron islet implants with low-dose administration of immunosuppressive drugs would provide higher functionality and survival for islet transplantation.
Immunosuppressive agents
Systemic administration of immunosuppressive agents is necessary, following islet cell transplantation to prevent graft rejection. Despite their high efficacy in suppressing the immune responses, their constant administration makes the patient highly susceptible to developing infectious diseases or cancer. An alternative approach to systemic immunosuppressant administration is local delivery of these agents at the site of transplantation. Cyclosporine A is a commonly used systemically administered immunosuppressive drug. 86 Several reports have evaluated the efficacy of polylactide nanoparticles as carriers for cyclosporine A delivery to encapsulated islet graft implantation site. The obtained results showed that continuous release of cyclosporine A could reduce T cell proliferation and inhibit production and secretion of inflammatory cytokines, which will enhance the islet graft's durability. 87
Similar promising results have been observed by using kaptoprofen-loaded islet graft microcapsules due to the immediate release of the immunosuppressive agent. 84 The synergistic effect of low-dose tacrolimus combined with a surface coating of 6-arm-PEG catechol with anti-CD154 monoclonal antibody (MR1) was assessed by Jee-Heon Jeong et al. Based on their results, the prepared formulation showed local inhibition against CD4+ T cells and was able to maintain normoglycemia for 50 days in vivo. 88
Co-encapsulation of anti-inflammatory agents is another promising approach for efficient local delivery of immunosuppressants. In a research study, pentoxifylline co-encapsulation significantly attenuated IL-2 expression in comparison with non-pentoxifylline encapsulation preparation. 89 Dang et al. studied the co-encapsulation of 16 different anti-inflammatory agents, from which dexamethasone and curcumin significantly inhibited local inflammatory responses in the islet graft's microenvironment. 90
Dexamethasone-loaded polydimethylene scaffolds for local immunosuppressants delivery could also diminish inflammation in the first week following islet graft transplantation, due to polarization of the anti-inflammatory phenotype of macrophages. 91 Other studies have shown that targeting colony-stimulating factor 1 receptor (CSF1R) with crystalline GW2580, a selective CSF-1R inhibitor, rendered 6 months of localized antifibrotic activity in mouse and primate models.92,93
Immunomodulatory agents
The higher specificity of immunomodulatory agents compared to immunosuppressive agents is encouraging for their application in encapsulation techniques. Regulatory T cells (Treg cells), which can modulate the innate and adaptive immune responses, are considered the key immunomodulatory agents. Gołąb et al. showed immunosuppression by islet coating with Treg cells. They also evaluated the effect of Treg coating on islet cells' function by glucose-stimulated insulin response (GSIR) assay. 94 According to their results, a direct relationship was observed between the number of islet-attached Treg cells and the intensity of GSIR. In other words, increasing the number of Treg cells has led to higher rates of insulin production and secretion from islet cells. It is well accepted that hindering the innate immune responses could be achieved by inhibiting dendritic cell maturation at the transplanted graft's microenvironment. 95
Co-immobilization of transforming growth factor beta (TGF-β) and IL-10 on the surface of hydrogel microcapsules can inhibit dendritic cell maturation. 96 In a recent study, TGF-β1-loaded poly(lactide-co-glycolide) (PLG) scaffolds could significantly reduce leukocyte infiltration at the site of transplantation. 97 CXCL12, a Treg-recruiting chemokine, was incorporated into ultrapure alginate microbeads, containing autologous islets, and were transplanted intraperitoneally in NHPs. 98 Based on the obtained results, a substantial reduction in foreign body response was observed for 1 month pos-implantation. 98
The co-delivery of Tregs by PLG scaffolds has led to euglycemia in mouse models. It was reported that the co-localization of Treg cells resulted in systemic tolerance in extra-renal implanted grafts. 99 Recently, a surface immunoengineering study was conducted for immobilization of Jagged-1 on PEG-coated islet surfaces (Fig. 5D), which showed increased Treg population as well as decreased proinflammatory cytokine concentrations in vitro, along with improved glucose regulation in vivo. 71
In addition to increasing the Treg population, many studies have reported on the downregulation of proinflammatory T effector (Teff) cells for increasing the likelihood of islet graft acceptance. In this regard, Headen et al. 100 prepared Fas ligand-presenting microgels, where Fas ligand is present on the surface of Teff cells as the death receptor. Fas ligand-presenting microgels were co-transplanted into the kidney capsule or epididymal fat pad of T1D mice. Rapamycin administration following the transplant significantly improved long-term graft survival and maintained blood glucose levels in the normal range during the 200-day follow-up period. Therefore, both of these strategies have been able to provide immune regulation at the transplantation site and improved islet survival.
Activated protein C contributes to the inhibition of inflammation by disrupting the production of inflammation initiating cytokines in the macrophages. Activation of the protein C (APC) is significantly prompted by thrombomodulin. Studies argue that immobilization of this agent on the surface of islets can significantly reduce inflammation at the transplant site.101,102 On the other hand, urokinase co-immobilization with thrombomodulin yielded life-long islet survival for xenografts. 103 Hydrogels functionalized with immunomodulatory peptides such as the IL-1 receptor recognition peptide have demonstrated significant protection against INF-γ, IL-1β, and TNF-α. 104 The addition of leukemia inhibiting factor with encapsulated PEG islets improved islet function compared to PEG encapsulation alone. Leukemia inhibiting factor induces Treg differentiation.
For targeted delivery of this factor, poly(lactic-co-glycolic acid) (PLGA)-based nanoparticles coated with anti-CD4 showed promising results. 105 Incorporation of TGF-β and IL-2 to the nanoparticles, combined with rapamycin administration, induced Foxp3+ Treg and had a significant protective effect at the graft site. 106 Hemoglobin-C is another immunomodulatory factor that can actively inhibit nitric oxide-induced cytotoxicity. Similarly, co-encapsulation with hemoglobin-C significantly increased islet viability and insulin secretion by the graft compared to the control group without hemoglobin-C. 107 In the same way, encapsulation in the scaffold immunomodulatory silk and its association with the release of IL-4 and dexamethasone have shown significant improvement in terms of reducing the immune responses to the transplanted islet graft. 108
Conclusion
In summary, cell encapsulation technology has shown promising results in overcoming the need for immunosuppressive drug consumption following cell transplantation. In this study, we have summarized current innovative immunoengineering strategies to protect transplanted cells from the host's immune system. We described islet encapsulation with a permeable barrier as a promising strategy for preventing the host's immune responses and subsequent rejection of islets or β-cells. However, despite significant recent advances in this field, many challenges remain to be addressed in the future.
Current works have focused on developing novel and highly biocompatible materials to encapsulate islet or β-cells. Although this technique has been successfully implemented in small animals, its clinical translation to larger animals and in humans is facing serious challenges, mainly due to the occurrence of encapsulating biomaterial-induced inflammation, thrombosis, and fibrosis. In addition, the absence of scalability for human applications to provide the ideal number of insulin-producing cells for clinical effectiveness is another important challenge. Innovative materials, conformal nanocoatings, and immunomodulating strategies have resulted in the development of novel encapsulation approaches. Another strategy for the effective local delivery of immunosuppressive agents is co-encapsulation of anti-inflammatory factors with islets/β-cells. Novel nanocarriers have been synthesized to release and deliver immunosuppressive agents to islets/β-cells within the capsules in a controlled manner.
Despite overcoming several challenges and demonstrating promising results, combined research in the fields of islet biology, material sciences, nanotechnology, and immunology are still needed for developing novel approaches to prevent immune responses and to increase graft's durability and performance in humans. Focus is now moving toward developing innovative tools and materials for controlling the immune system that can be used in large-scale clinical applications. Furthermore, introducing reliable, noninvasive approaches for determining the number of islet/β-cells, as well as their biodistribution, survival, and functionality in vivo, are crucial to further improve T1D cell-based therapy. By combining interdisciplinary specialties, the potential safety challenges of cell therapy can be addressed to further improve the effectiveness of this treatment approach for T1D patients.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: Z.I., M.R., and H.D.: conceptualization. S.S. and S.J.: investigation and G.B. and E.H.-S.: validation. H.D., F.J., H.D., Z.S., and H.K.: writing—original draft preparation. M.R., S.S.M. and Z.I.: writing—review and editing. Z.I. and M.R.: supervision.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This research has been financially supported by Kermanshah University of Medical Sciences (KUMS).