
Abstract
Adipose tissue-derived microvascular fragments (MVF) are functional vessel segments, which rapidly reassemble into new microvasculatures under experimental in vitro and in vivo conditions. Accordingly, they have been used for many years in microcirculation research to study basic mechanisms of endothelial cell function, angiogenesis, and microvascular network formation in two- and three-dimensional environments. Moreover, they serve as vascularization units for musculoskeletal regeneration and implanted biomaterials as well as for the treatment of myocardial infarction and the generation of prevascularized tissue organoids. Besides, multiple factors determining the vascularization capacity of MVF have been identified, including their tissue origin and cellular composition, the conditions for their short- and long-term storage, as well as their implantation site and the general health status and medication of the recipient. The next challenging step is now the successful translation of all these promising experimental findings into clinical practice. If this succeeds, a multitude of future therapeutic applications may significantly benefit from the remarkable properties of MVF.
Impact Statement
The present review provides a complete overview of the broad application spectrum of adipose tissue-derived microvascular fragments (MVF) in angiogenesis research and regenerative medicine. Moreover, it systematically describes factors determining their vascularization capacity. These factors may be used to further improve the remarkable properties of MVF in personalized medicine and to promote their rapid introduction as vascularization units into clinical practice.
Introduction
During the past few decades, it has become evident that adipose tissue is by far more than just an energy storage of the human body. In fact, besides its major function as an endocrine organ, 1 adipose tissue is meanwhile considered the greatest source for regenerative cells. 2 These cells can be harvested by enzymatic digestion of fat samples within ∼1 h, followed by several purification steps, which finally result in a single cell suspension, the stromal vascular fraction (SVF). 3
The SVF is a heterogeneous mixture of fibroblasts, endothelial cells, pericytes, macrophages, preadipocytes, endothelial progenitor cells, and mesenchymal stem cells (MSC) with a high regenerative and vascularization potential. 4 Accordingly, it is an attractive isolate for multiple therapeutic applications, including the treatment of wounds, bone defects, osteoarthritis, fistulas, and non-reconstructable peripheral vascular disease.5–9
A shorter enzymatic digestion of adipose tissue for only ∼10 min enables the isolation of microvascular fragments (MVF). 10 MVF are functional vessel segments with an intact arteriolar, capillary, or venular morphology (Fig. 1). Hence, they bear several advantages when compared with SVF single cells. In microcirculation research, they are used as nonartificial, native vessel segments to study basic mechanisms of angiogenesis. In tissue engineering and regenerative medicine, transplanted MVF are highly effective vascularization units, which are capable of forming new blood-perfused microvascular networks by their rapid interconnection with each other and the surrounding host microvasculature within 3–6 days.11,12
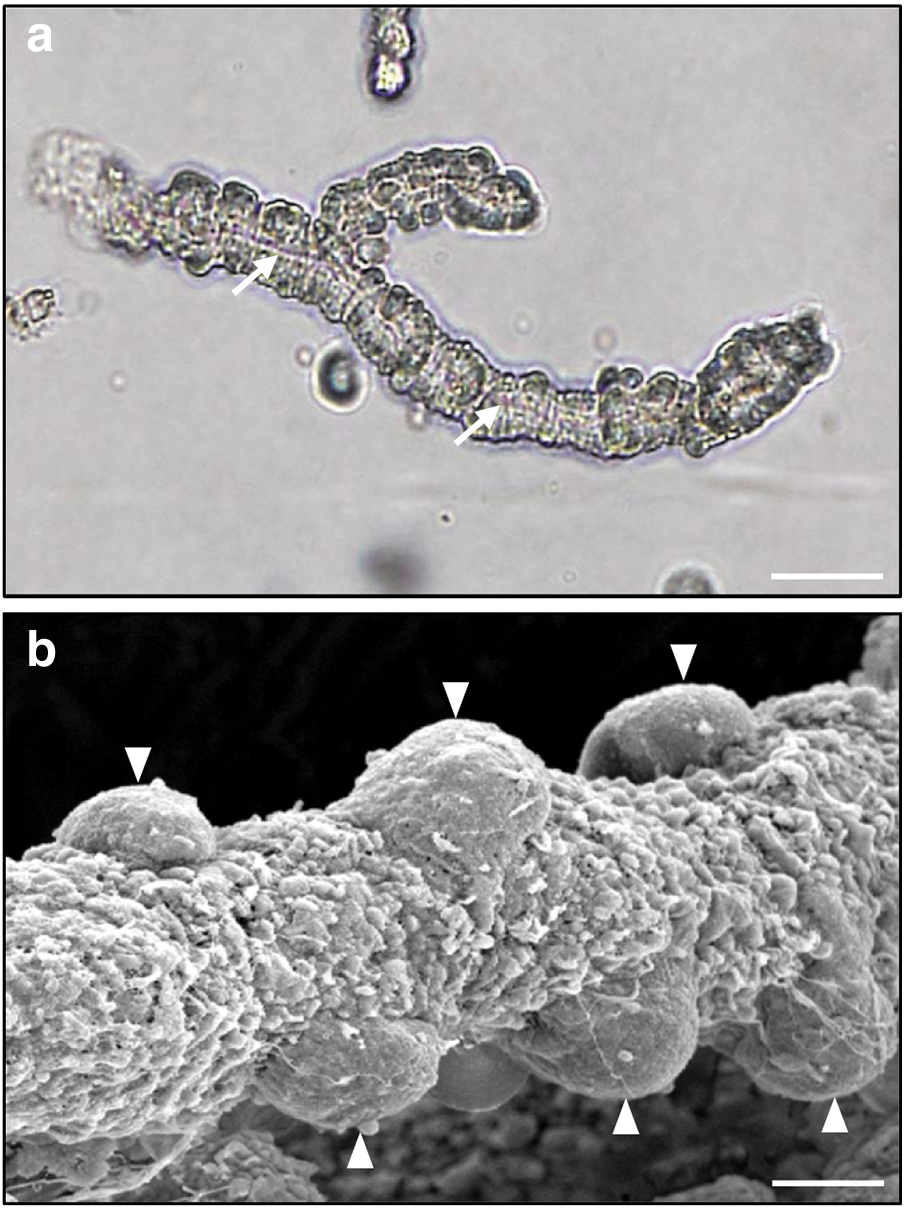
Morphology of MVF.
Accordingly, they markedly improve the vascularization of implanted scaffolds when compared with SVF single cells. 13 In addition, MVF contain resident MSC, which exhibit a higher differentiation capacity than single MSC most probably due to their localization in an intact physiological niche. 14 This offers the opportunity to use MVF as the sole source of biological material for the generation of well-vascularized tissue-specific substitutes, such as engineered adipose tissue. 15
Based on these unique properties, MVF have been increasingly used in basic and preclinical studies focusing on angiogenesis and tissue vascularization (Fig. 2). This deserves an up-to-date overview of the continuously expanding application spectrum of these native vessel segments and a look ahead to their potential use in future regenerative medicine.

Applications of adipose tissue-derived MVF in microcirculation research and regenerative medicine. In microcirculation research, MVF are used for the isolation of vascular cells, the co-cultivation with single cells, the 3D cultivation in collagen gels, and the in vivo implantation of these gels to study angiogenesis and microvascular network formation. Previous experimental studies indicate that in future regenerative medicine MVF may serve for the improvement of musculoskeletal regeneration and biomaterial vascularization as well as the treatment of myocardial infarction and the generation of prevascularized organoids. 3D, three-dimensional. Color images are available online.
MVF in Microcirculation Research
MVF as vascular cell source
MVF originally served as a source for setting up endothelial cell and pericyte cultures. Wagner and Matthews 16 cultured isolated capillary segments from rat epididymal fat pads on glass coverslips, which resulted in the outgrowth of capillary endothelial cells. In follow-up studies, these cells were then used to study micropinocytosis and endothelial cell–matrix interactions.17,18 Jeon et al. 19 separated pericytes from MVF by colony selection during cultivation and subsequently analyzed their secretion of basement membrane compounds. They found that pericytes synthesize substantial amounts of type IV collagen, which can be stimulated by ascorbic acid phosphate.
In addition, they secrete several laminin variants that are partly similar to those produced by aortic and pulmonary endothelial cells. 19 These findings indicate that pericytes crucially contribute to the formation of the basement membrane and, thus, to the regulation of endothelial cell migration and proliferation as well as organization of microvascular networks. Accordingly, angiogenesis assays involving both endothelial cells and pericytes may be most suitable to study basic mechanisms of blood vessel development. The use of MVF as cell source for such assays bears the advantage that, in contrast to immortalized cell lines, their vascular cells are in a physiological proliferation and differentiation state.
MVF/single cell co-cultures
Sato et al. 20 developed an in vitro model to investigate capillary growth by co-cultivation of MVF from rat epididymal fat pads with the surrounding single cells that are typically present in fresh MVF isolates. Initially, they called these single cells as myofibroblastic cells due to their intracellular microfilament patterns as well as their well-developed granular endoplasmic reticula and Golgi apparatus. Meanwhile, it is obvious that these cells were most probably MSC.
In fact, McDaniel et al. 14 reported that they express typical stem cell surface markers and exhibit a multilineage differentiation potential. Sato et al. 20 observed that they rapidly expand in culture and form a monolayer after 4 days. A few days later, the co-cultured MVF develop sprouts, which elongate, branch, and finally interconnect with each other to a new microvascular-like network on the monolayer. 20 Therefore, it was concluded that this in vitro co-culture system may be suitable for identifying factors stimulating or inhibiting angiogenesis.
Accordingly, the approach has been used to study the anti-angiogenic action of tumor necrosis factor and interferon-γ21,22 as well as the proangiogenic action of insulin,23,24 platelet-derived growth factor, 25 and norepinephrine. 26 Moreover, it served for assessing the effects of endurance training on angiogenesis. 27 For this purpose, MVF/single cell co-cultures were exposed to muscle extracts from rats, which were trained on a rodent treadmill for 9 weeks. This markedly promoted sprout formation and capillary growth, indicating that physical activity is a major trigger for blood vessel formation in skeletal muscles. 27
Three-dimensional MVF cultivation in collagen gels
Considering the importance of a physiological three-dimensional (3D) environment with a supporting extracellular matrix (ECM) for the process of blood vessel formation, Hoying et al. 28 introduced a novel 3D culture system by embedding freshly isolated MVF from rats in 3D collagen type I gels. These MVF-loaded collagen gels are cultivated for several days under static conditions 28 or under perfusion using a dynamic in vitro perfusion chamber. 29 Within the gels, MVF develop angiogenic sprouts and elongate.
This can be enhanced by endothelial cell growth supplement and the non-proteolytically active thrombin peptide TP508 and can be suppressed by transforming growth factor-β and hydrocortisone.28,30 Moreover, the embedded MVF actively modify the stiffness of the surrounding ECM. During their sprouting, they mainly express metalloproteinases with a strong proteolytic activity, resulting in an overall decrease in matrix stiffness. 31 This is followed by a phase of neovessel elongation with an elevated expression of genes encoding for ECM compounds, which leads to a re-stiffening of the collagen gel. 31 However, the properties of the ECM crucially determine the growth behavior of embedded MVF.
Higher collagen densities promote the formation of microvascular networks with shorter vessel lengths, less branch points, and reduced interconnectivity. 32 In addition, an artificially generated matrix interface, which can be achieved by embedding an inner MVF-loaded collagen gel into an outer MVF-free collagen gel, has been shown to act as a barrier to vessel growth, deflecting growing MVF parallel to the interface. 33 Of interest, in this study, the initial collagen concentration used to generate both the inner and outer collagen gel was 3 mg/mL. However, after the fabrication process, the inner gel and interface exhibited a significantly higher collagen density of ∼4–6 mg/mL when compared with that of the outer gel (∼3 mg/mL).
MVF/collagen gels are highly suitable to study the effects of mechanical forces on the formation and orientation of microvascular networks. For this purpose, the gels are exposed to a mechanical loading system consisting of a custom culture chamber, in which they polymerize around a fixed anchor post and a moveable actuating post to induce different stress and strain fields. 34
This approach revealed that growing MVF typically align parallel to the direction of stress/strain or internally generated traction, which is most probably regulated by the alignment of surrounding collagen fibrils. 35 Moreover, the angiogenic sprouting and branching of MVF is suppressed by an increasing constraint imposed on the boundaries of the cultured gel. 36 In the human body, similar mechanically mediated mechanisms may contribute to the formation of oriented vascular beds in native tissues, such as the parallelly arranged capillaries in striated muscle tissue.
Rhoads et al. 37 cultivated MVF/collagen gels over a monolayer consisting of rat skeletal muscle satellite cells. This co-culture approach showed a higher sprouting activity of MVF in the presence of the satellite cells. Additional mechanistic analyses revealed that this proangiogenic effect is mediated via hypoxia-inducible factor-1α-induced secretion of vascular endothelial growth factor (VEGF) by the myogenic cells. In a follow-up study, Rhoads et al. 38 used satellite cells from adult and aged rats or from muscular dystrophy X-linked mice developing Duchenne muscular dystrophy. Of interest, they found that MVF exhibit a reduced vascularization capacity when co-cultured with satellite cells from aged or dystrophic muscles. Hence, the functional deficits of these cells seem to directly impair their interaction with the surrounding microvasculature.
During the past two decades, the continuous application of 3D MVF/collagen gels has been accompanied by the development of sophisticated microscopy technologies as well as imaging processing and computational modeling tools. These include the combination of second-harmonic generation signals from fibrillar collagen with two-photon excited fluorescence and coherent transmission imaging of vascular cells for the visualization of collagen remodeling by MVF. 39 Smith et al. 40 used an automatic thresholding scheme to obtain volume measurements of growing MVF.
In addition, Utzinger et al. 41 developed a new time-lapse image acquisition procedure and morphometric analysis tools to quantify the elongation dynamics of MVF. Their analyses demonstrated that the physiological growth rate of microvessels is ∼5 μm/h. Guilkey et al. 42 described a modified material point algorithm enabling large-scale simulations of mechanical interactions between MVF and their surrounding collagen matrix. With the same objective, Edgar et al.43,44 introduced later a nonlinear finite element approach, which provides a flexible platform for in silico investigations of angiogenesis in complex and multifaceted mechanical environments.
In conclusion, these studies indicate that 3D MVF/collagen gels represent versatile in vitro systems to study basic principles of angiogenesis with particular emphasis on the interaction of microvessels with the ECM and associated mechanical forces.
In vivo implantation of MVF/collagen gels
MVF have not only been used for in vitro analyses in angiogenesis research but have also been implanted into recipient animals to study microvascular network formation under in vivo conditions. For this purpose, collagen gels have been used as vehicle (Table 1). These experiments demonstrated a rapid interconnection of the MVF with the host microcirculation, resulting in an early onset of blood perfusion within the gels during the first days after implantation. 45 Morphological, functional, and transcriptional analyses revealed that this process is associated with three distinct vascular phenotypes in the implants reflecting sprouting angiogenesis, neovascular remodeling, and network maturation. 46
Previously Used Vehicles for the In Vivo Administration of Microvascular Fragments
PBS, phosphate-buffered saline; PRP, platelet-rich plasma.
To enable the in vivo implantation of MVF-based neovasculatures with a clearly defined parallelly arranged topology, Chang et al. 47 introduced a direct-write bioprinting technique, which allows the dispensing of MVF/collagen gels into hydrogel molds for the generation of composite biohybrid constructs. After implantation of these constructs in the flanks of mice, the neovasculatures developed functional networks after 4 weeks, but lost their prepatterned architecture. 48 In another approach, MVF prepatterning was achieved by physically constraining MVF/collagen gels along an axis. 48
This also resulted in a parallel neovessel orientation. However, in this case, the maintenance of uniaxial physical constraints after the in vivo implantation of the gels produced stable microvascular networks with aligned microvessels. These findings indicate that the long-term network topology of implanted MVF/collagen gels is independent of the prepatterning approach but markedly influenced by a patterning stimulus in the phase of microvascular remodeling and maturation. 48
MVF in Regenerative Medicine
MVF in musculoskeletal regeneration
One of the first described applications of MVF in the field of tissue engineering and regenerative medicine was their autotransplantation into myocutaneous flaps. Nakano et al. 49 reported that this improves the survival of ischemic flap tissue by the rapid interconnection of MVF with the surrounding host vessels, particularly if MVF are co-transplanted with myofibroblasts. Stone and Rathbone 50 injected MVF in phosphate-buffered saline as vehicle in 10 × 3 cm random-pattern flaps on the back of rats at the time of surgery. Although this approach did not markedly improve the microvessel density and blood perfusion of the flap tissue over time, it significantly increased flap survival by 6.4% when compared with sham-treated controls.
MVF have been further evaluated as vascularization units for the treatment of volumetric muscle loss. For this purpose, tibialis anterior muscle defects in rats were filled with empty collagen gels or gels enriched with MVF or adipose tissue-derived stem cells. 51 The administration of both MVF and stem cells resulted in a higher microvessel density of the defects. However, the onset of tissue perfusion was markedly accelerated by MVF when compared with stem cells.
Li et al. 52 implanted MVF–myoblast-loaded collagen hydrogels into large volumetric defects in the rat biceps femoris muscle. Although this improved tissue vascularization, the healing defects were characterized by the formation of fibrotic tissue with adipose infiltration, poor volume maintenance, and little muscle regeneration. 52 These findings indicate that the regeneration of volumetric muscle defects is not solely driven by an adequate vascularization but is crucially dependent on other factors that should be identified in future studies.
As recently reported by Acosta et al., 53 this may be achieved by the establishment of vascularized tissue-engineered skeletal muscle models. They co-cultured muscle precursor cells with MVF and exposed them to adipogenic induction media to induce the formation of intramuscular adipose tissue like in skeletal muscles of patients with diseases, such as diabetes. Of interest, they found that adipogenesis within the constructs reduced the maturation and mechanical integrity of the muscle tissue as well as its myotube and vessel alignment.
As an alternative to the frequently used collagen gels, Orth et al. 54 used a thermoresponsive hyaluronan hydrogel for the delivery of MVF into bone defects. This biocompatible hydrogel is liquid at room temperature and exhibits a gel-like consistency at body temperature, which makes it an attractive carrier system for in vivo applications.55,56 In vitro, MVF incorporated in this hydrogel exhibited less apoptotic cells and a stable vessel morphology throughout a 7-day culture period when compared with non-incorporated controls. 54 Moreover, in vivo, they increased the early vascularization of murine femur defects.
However, this was not associated with an improved defect healing, but even impaired the bone formation process. 54 Similar results were obtained by Ruehle et al.,57,58 who did not detect a beneficial effect of MVF on the regeneration of internally stabilized defects in mid-diaphysis rat femurs with overlying full-thickness quadriceps defects. These unexpected results may be explained by the fact that the bone healing process is crucially dependent on an adequate spatiotemporal balance between angiogenic and osteogenic growth factors. 59 Hence, an overwhelming MVF-induced early vascularization of bone defects, which is associated with the downregulation of VEGF expression in the callus tissue, 54 may essentially disturb this fragile balance.
MVF as vascularization units for implanted biomaterials
In classical tissue engineering, artificial tissue constructs are generated by seeding different cell types on scaffold biomaterials. Dependent on the type of tissue to be generated, these scaffolds may markedly differ in terms of their chemical and physical properties.60,61 However, most of them share the common requirement that they should rapidly vascularize after in vivo implantation to guarantee the survival of the seeded cells.62,63 To achieve this goal, MVF can serve as native vascularization units. After their seeding onto nanosize hydroxyapatite particles/poly(ester urethane) scaffolds for bone tissue engineering, they have been shown to survive and rapidly develop dense microvascular networks inside the scaffold pores, resulting in a rapid in vivo vascularization. 64
For this purpose, freshly isolated MVF should be seeded onto the scaffolds immediately before implantation, because they lose their physiological vessel morphology when precultivated for several days onto the scaffold surface. 65 In addition, it should be considered that the scaffold architecture and pore size crucially influence MVF-based network formation. For instance, MVF have been shown to develop greater vessel loops inside hydroxyapatite scaffolds with 450 μm pores when compared with scaffolds with smaller pore sizes of 250–340 μm. 66
Bioengineered dermal skin substitutes are also a kind of scaffolds, which have been used for many years in plastic surgery in the initial treatment of extensive full-thickness skin defects. 67 They are directly implanted into the debrided wound bed for the provisional maintenance of the skin's physiological barrier function. After their vascularization and tissue incorporation, they are finally covered in a second step with split-thickness skin grafts. However, this approach bears the major disadvantage of extended patient hospitalization because the vascularization of dermal skin substitutes requires up to 3 weeks. 68 Moreover, there is an increased risk for infection during this critical time period. To overcome this problem, Frueh et al. 69 seeded Integra matrices consisting of cross-linked bovine collagen and shark glycosaminoglycan with freshly isolated murine MVF.
Compared with nonseeded matrices, seeding markedly accelerated and improved in vivo Integra vascularization after implantation into mouse dorsal skinfold chambers. The substitutes did not only contain more microvessels but also contained lymphatic vessels originating from the seeded MVF. This interesting observation opens the door for novel future applications of MVF in the fields of lymphatic tissue engineering and lymphedema therapy. 70 In a follow-up study, Frueh et al. 71 implanted MVF-seeded and nonseeded Integra into bradytrophic full-thickness defects on the skull of CD1 nu/nu mice. After 10 days, the matrices were covered in a second step with autologous split-thickness skin grafts.
Of interest, the survival of these grafts on MVF-seeded Integra was markedly improved after 5 days when compared with grafts on nonseeded control matrices (Fig. 3). Despite these highly promising results, it should be noted that the seeding of Integra with MVF is mainly limited to its surface due to its sheet-like structure with small pores. This offers the opportunity for further optimization. In line with this view, Später et al. 72 compared the in vivo vascularization of MVF-seeded conventional Integra with that of Integra flowable wound matrix. The latter one is a gel-like matrix, which allows the direct admixture of MVF during sample preparation.
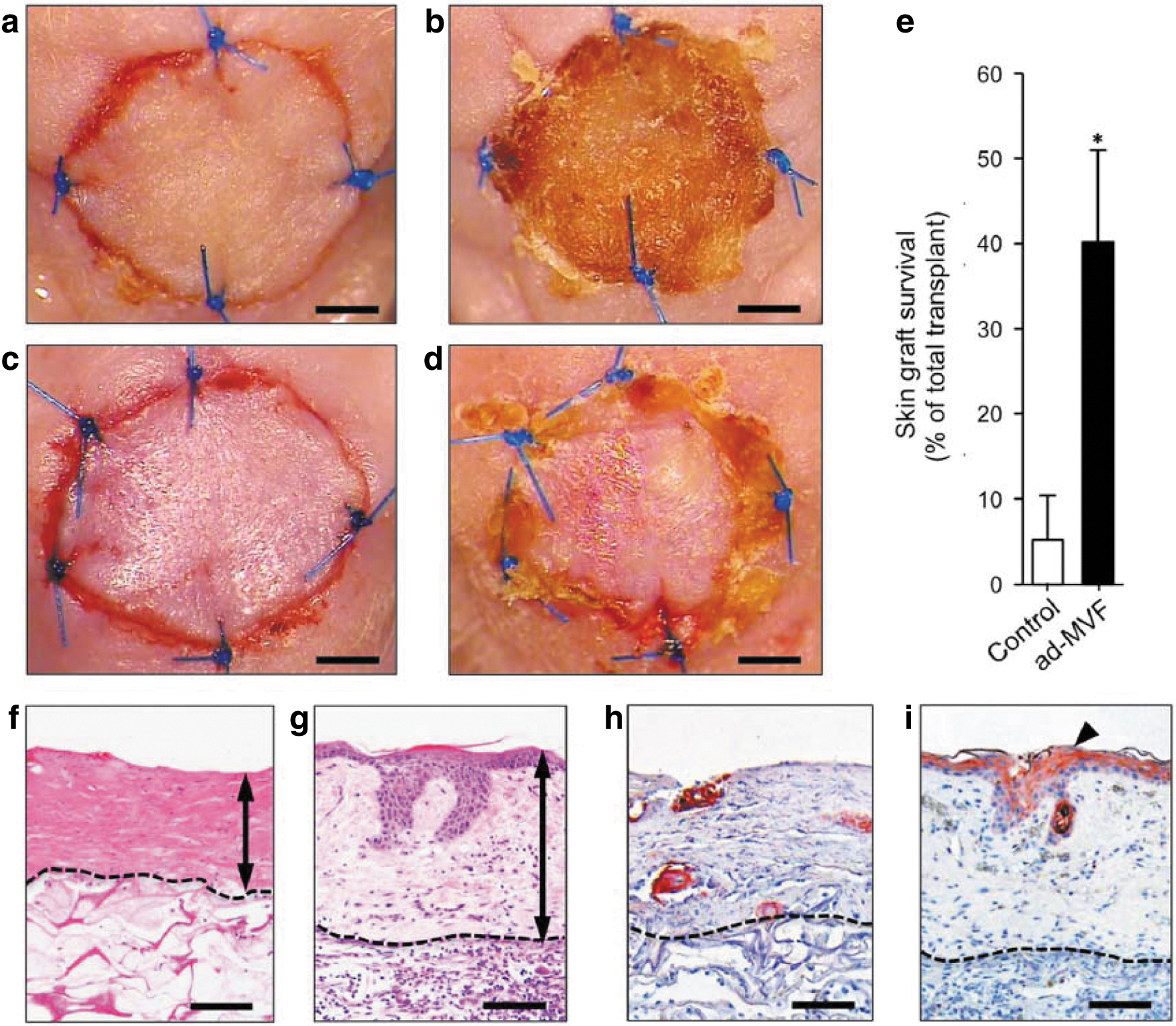
Successful autologous skin grafting by means of MVF-seeded Integra according to Frueh et al.
71
Accordingly, when using the identical seeding number of MVF, this matrix exhibited a more homogeneous MVF distribution directly after seeding when compared with conventional Integra. However, this did not result in an improved in vivo vascularization, because due to the more homogeneous MVF distribution the reassembly of MVF into new microvascular networks was prevented by an increased interfragment distance. 72
These findings confirm the results of another study 73 showing that a high MVF seeding density and, thus, a short interfragment distance is essential for a rapid vascularization, even if it is restricted to distinct implant regions. In fact, after the successful reassembly of MVF into blood-perfused microvascular networks, these regions can serve as starting points for a complete implant vascularization within a short period. For this purpose, it is necessary that the implant material exhibits a porous structure, which allows the continuous expansion of the MVF-based microvascular networks.
Finally, it is noteworthy to mention that strategies have been established for the MVF seeding of biomaterials with hydrophobic surfaces, which prevent adequate cellular and tissue attachment. To achieve this, Gruionu et al. 74 coated expanded polytetrafluoroethylene with MVF/collagen gels. This coating did not only promote the development of a vascularized granulation tissue but also reduced the number of activated macrophages surrounding the implants. Später et al. 75 suspended MVF in platelet-rich plasma (PRP) for the coating of porous polyethylene. PRP is a fraction of the blood plasma with platelet concentrations above baseline, which forms a solid gel after its activation. 76
Hence, it is an easily producible autologous product for the coating of alloplastic materials.77,78 MVF/PRP-coated implants exhibited an enhanced in vivo vascularization and tissue incorporation when compared with uncoated controls. 75 Moreover, they induced proangiogenic M2 macrophage polarization at the implantation site. Taken together, these findings indicate that besides their vascularization capacity, MVF coatings seem to have an immunomodulatory effect, which may serve to improve the integration of implanted biomaterials.
MVF in the treatment of myocardial infarction
In an early proof-of-principle study, Nakano et al. 79 injected MVF in combination with myofibroblasts into the superficial myocardium of rat hearts. Repetitive microscopic and histological analyses of the hearts proved the survival of the MVF for at least 49 days and their interconnection to the host's coronary microvessels. Accordingly, the authors concluded that MVF may promote the development of a new collateral microcirculation, which could be beneficial for the therapy of ischemic heart conditions.
Another promising approach for the treatment of such conditions is the transplantation of human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CM). 80 However, most of these cells do not survive after transplantation. 81 To overcome this problem, Sun et al. 82 recently co-transplanted them with MVF in collagen type I gels into infarcted heart tissue of rats. Notably, this resulted in a sixfold increase of hiPSC-CM survival and also enhanced the maturation of the cells. This indicates that MVF may significantly improve the functional outcomes in future cell replacement therapies.
MVF for the generation of prevascularized organoids
The incorporation of MVF into tissue organoids represents a very new type of application. Due to their 3D environment with intensive cell–cell contacts, organoids mimic the physiological conditions of native tissues much better and, thus, have been shown to exhibit an increased viability as well as an improved proliferation, differentiation, and metabolic activity when compared with conventional two-dimensional cultures.83,84 With this in mind, Strobel et al. 85 recently incorporated human MVF into organoids for the generation of both vascularized MSC and adipocyte organoids.
Under culture conditions, the MVF retained their vessel morphology and expanded via sprouting angiogenesis within the organoids and into surrounding collagen gels. Simultaneously, it was possible to differentiate the incorporated MSC into adipocytes, which showed a higher insulin receptor expression in the presence of MVF, indicating the close interaction of these cells with their adjacent microvasculature.
Salamone et al. 86 co-cultured MVF and pancreatic islets in 3D collagen type I hydrogels and observed the in vitro vascularization of the islets by ingrowth of angiogenic sprouts developing from the surrounding MVF. Hiscox et al. 87 demonstrated that subcutaneously implanted collagen-embedded pancreatic islets with a surrounding MVF/collagen gel exhibit an enhanced survival in recipient mice. These studies suggest that MVF may also be promising vascularization units to improve the outcome of islet transplantation for the therapy of type I diabetes. Developing further this strategy to the next level, Nalbach et al. 88 generated prevascularized islet organoids by direct fusion of MVF with pancreatic islet cells in a liquid overlay culture (Fig. 4).

Generation of prevascularized islet organoids by direct fusion of MVF with pancreatic islet cells according to Nalbach et al.
88
In vitro, these organoids secreted insulin and presented with a higher angiogenic activity when compared with freshly isolated and cultivated islets as well as non-prevascularized islet organoids. After transplantation, they vascularized more rapidly, resulting in an improved survival and, thus, a markedly lower number of grafts required to restore normoglycemia in diabetic mice. 88 These promising findings indicate that the approach of Nalbach et al. 88 may have also great potential to improve the engraftment and function of other tissue constructs, such as hepatic organoids.
Factors Determining the Vascularization Capacity of MVF
Tissue origin and composition of MVF isolates
The reassembly into new microvascular networks is a basic property of MVF, which is independent of their tissue source as long as they contain both endothelial and perivascular cells. 89 So far, MVF have been harvested from the brain and adipose tissue. These tissues are characterized by a rather loose tissue consistency, which facilitates their rapid enzymatic digestion, while guaranteeing the integrity of MVF. Microvascular networks originating from MVF of the brain cortex exhibit a higher microvessel density and are significantly less permeable to high- and low-molecular-weight molecules when compared with microvasculatures developing from adipose tissue-derived MVF. 89
This indicates that they retain the typical properties of the blood–brain barrier. Accordingly, brain-derived MVF are particularly promising tools for basic studies focusing on distinct molecular characteristics and cellular mechanisms of the blood–brain barrier, such as transcriptional profiles of brain vascular endothelial cells or functional transport processes.90,91 In contrast, adipose tissue-derived MVF offer the opportunity for direct clinical applications in tissue engineering, because fat tissue can be harvested minimal invasively in patients without causing severe side effects or complications.
Considering the fact that due to demographic change mainly elderly patients may profit from such applications in the future, it has been shown that adipose tissue-derived MVF from aged donor mice do not differ in their stem cell content, release of angiogenic growth factors, viability, and proliferation under hypoxic in vitro conditions when compared with MVF from adult animals. 92 However, their in vivo network forming ability is markedly reduced, which is particularly associated with an impaired vessel maturation. Accordingly, MVF from aged donors develop into microvascular networks with vessel wall irregularities and a significantly lower fraction of perivascular cells expressing α-smooth muscle actin and matrix metalloproteinase-9. 92
The composition of MVF isolates is another important determinant for their vascularization capacity. These isolates do not only consist of MVF but also of single cells of the SVF. Hence, they contain substantial amounts of macrophages, which are known to secrete various angiogenic growth factors, to act as guides for endothelial tip cells, and to be involved in the interconnection of individual angiogenic sprouts. 93 In line with these findings, the isolation and transplantation of MVF in macrophage-depleted mice result in the development of microvascular networks with a reduced density and vessel maturation. 94
This indicates that a further purification of freshly isolated MVF to separate them from surrounding single cells may not be recommended for their use as in vivo vascularization units. Moreover, it should be considered that variations in macrophage numbers and activity may directly affect the outcome of interventions involving MVF in individuals with an altered immune system.
Storage conditions
In an ideal future clinical setting, MVF are rapidly isolated from fat samples of a patient by means of an automated isolation system and directly retransferred into a tissue defect (Fig. 5). However, this may not always be feasible due to time-consuming and complex surgical interventions, which last many hours or even require a multistage procedure. In such cases, it may be necessary to store MVF under appropriate conditions. Experimental studies indicate that this is possible on non-adherent culture surfaces for at least 24 h without losing the physiological vessel morphology of MVF (Fig. 5). 95

Storage conditions for MVF. In an ideal future clinical setting, MVF are rapidly isolated from liposuctioned fat and directly retransferred into a tissue defect. However, experimental studies indicate that it is also possible to store them for hours to days under appropriate culture conditions or for longer time periods by means of cryopreservation. Color images are available online.
For this purpose, a subnormothermic cultivation temperature of 20°C should be preferred when using standard endothelial cell growth medium containing fetal calf serum, because this temperature better preserves the viability of MVF and even increases their proliferative activity and in vivo network formation when compared with 37°C. 95 However, MVF can also be stored for 24 h in University of Wisconsin solution at 4°C without affecting their vascularization capacity. 96 Particularly for clinical applications, the latter approach bears the major advantage of a xeno-free storage solution, which is already clinically approved and well established in the field of organ transplantation. 97
The short-term storage of MVF may not only solve logistic problems in clinical routine but also allows the improvement of their angiogenic activity by exposing them to stimulating compounds that can easily be added to different storage solutions. Recent studies demonstrate that such a proangiogenic effect on MVF can be achieved by means of erythropoietin, 98 insulin-like growth factor-1, 99 or high glucose concentrations. 100
Finally, there is the opportunity to cryopreserve MVF for their long-term storage (Fig. 5). 101 In a future scenario, this may be an option for patients undergoing elective liposuction. If required later on, their stored MVF could be autologously retransferred into a tissue defect without the need of an additional MVF isolation procedure. Cryopreservation does not affect the cellular composition and vascular morphology of MVF. However, it reduces the viability and overall number of transplantable MVF. Of interest, this is completely compensated by an increased angiogenic activity of the remaining MVF, which express significantly higher levels of angiogenic growth factors when compared with freshly isolated controls. 101
Characteristics of the implantation site and the recipient
The onset of blood perfusion in implanted MVF-seeded tissue constructs is crucially determined by the speed of their inosculation, that is, the functional interconnection between MVF and the host microvasculature. 102 The probability of such a successful interconnection, in turn, is dependent on the density of angiogenic sprouts growing from the MVF and the host vessels toward each other. Accordingly, it is obvious that a well-vascularized implantation site ideally supports the rapid vascularization of MVF-seeded tissue constructs.
If this is not the case, the exogenous angiogenic stimulation of the implantation site may be a possible strategy. Grässer et al. 103 demonstrated that this can be easily achieved by a single topical application of macrophage-activating lipopeptide-2. However, this toll-like receptor 2/6 agonist additionally induces apoptosis of the endothelial and perivascular cells within MVF, which markedly affects their in vivo vascularization capacity. 103 Hence, to avoid this detrimental side effect, more suitable proangiogenic compounds should be identified in future experimental studies.
Besides the implantation site itself, the general health status and medication of a patient may also determine the outcome of MVF-based vascularization approaches. For instance, it is well known that chronic diabetes mellitus induces severe microangiopathy, which markedly affects the functionality of microvessels throughout the entire body. 104 Altalhi et al. 105 found that the expression of hepatocyte growth factor (HGF) is downregulated within MVF/collagen gels that are implanted into streptozotocin-injected type I diabetic mice when compared with nondiabetic controls.
This reduced the angiogenic sprouting of the MVF, leading to their delayed interconnection with the surrounding host vessels. Of interest, the supplementation of HGF in the gels could restore the sprouting activity of MVF under these diabetic conditions. Hence, it is tempting to speculate that the susceptibility of MVF to distinct angiogenic stimuli allows the adaptation of their vascularization capacity to patient-specific needs. 70 In line with this view, Später et al. 106 recently demonstrated that systemic low-dose erythropoietin administration improves the vascularization of implanted MVF-seeded dermal substitutes.
However, for a broad implementation of MVF-based vascularization approaches, it should be also tested whether the reassembly of MVF to microvascular networks is affected by clinical routine procedures. In this context, the low-molecular-weight heparin (LMWH) enoxaparin, which is routinely used for thromboprophylactic therapy in clinical practice, 107 has already been shown to exert no effects on the in vivo network formation of MVF. 108
Conclusions
During the past two decades, MVF have been increasingly used in experimental studies focusing on microcirculation research, tissue engineering, and regenerative medicine. This may be particularly explained by the fact that they originate from the body's own microvasculature. Thus, in microcirculation research, 3D MVF/collagen gels are well-established tools that allow studying basic mechanisms of angiogenesis under realistic physiological conditions.
Currently, there is a trend toward the refinement of this approach by adding other cells or larger cell clusters for the generation of vascularized tissue-specific in vitro models, which can serve as future platforms for drug screening or the analysis of tissue-specific disease mechanisms.53,86 However, MVF exhibit the unique property to rapidly reassemble into new microvascular networks due to their retained vessel morphology and high angiogenic activity. Hence, they represent efficient vascularization units for a broad spectrum of future applications in tissue engineering and regenerative medicine.
However, the successful translation of MVF-based approaches into clinical practice still remains a major challenge. To achieve this goal, it will be necessary to develop systems for the automated intraoperative isolation of MVF and to establish adequate solutions for their short- and long-term storage according to good manufacturing practice conditions. Besides these technical aspects, additional studies are required to identify the factors determining the vascularization capacity of MVF under physiological and pathological conditions to optimally adapt their in vivo performance to the needs of individual patients in the sense of personalized medicine.
In light of the fact that MVF isolates also contain substantial amounts of stem cells and immune cells, it should be further clarified how these cells can be used to improve the functionality of MVF, to generate tissue-specific substitutes, and to positively modulate the immune system, while still fulfilling the strict safety requirements of cell-based therapy. If this succeeds, a multitude of future therapeutic applications may significantly benefit from the remarkable properties of MVF. Beyond the previously suggested applications described in the present article, these may include the improvement of nerve, tendon, or ligament regeneration, the treatment of ischemic conditions, such as stroke or peripheral vascular disease, as well as the vascularization of medical devices, including surgical meshes or vascular prostheses.
Footnotes
Acknowledgments
We are grateful for the excellent technical assistance of Wolfgang Metzger (Department of Trauma, Hand and Reconstructive Surgery, Saarland University) and Claudia Scheuer (Institute for Clinical and Experimental Surgery, Saarland University) in preparing the images of Figure 1. Moreover, we thank Servier Medical Art for providing access to designed medical elements (![]() ), supporting the generation of graphical items in this publication.
), supporting the generation of graphical items in this publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a grant of the Deutsche Forschungsgemeinschaft (DFG—German Research Foundation; Grant No. LA 2682/7-2).