
Abstract
Bone marrow stromal cells (BMSCs) and periosteum-derived cells (PDCs) represent promising skeletal stem cell sources to treat critical-size bone defects. However, the large number of preclinical tests with a variety of in vivo data complicates the selection of cells for further clinical translation. This systematic review aims to analyze the in vivo bone-forming efficacy of BMSCs- and PDCs-based approaches in all published preclinical experiments until November 2020. For this purpose, four databases (PubMed, Embase, Cochrane Central Register of Controlled Trial, and Web of Science) were searched for eligible literature, which yielded a total of 94 full-text articles for systematic review. This review generated an evidence-based list of BMSC- or PDC-based approaches, which have been evaluated for bone formation in different animal models. Among them, 74 studies were included for pairwise and network meta-analysis. The results revealed that both PDC and BMSC had beneficial bone-forming efficacy compared to bare scaffold. In addition, BMSC- and PDC-based approaches had no significant difference regarding in vivo bone-forming efficacy. However, BMSC-based approach had a higher probability to be ranked better than PDC-based approach. Furthermore, the review discusses (i) the possible risk of bias of the in vivo evaluation of cell-based approaches, (ii) the difficulty in replication of such experiments due to frequent poor reporting of the methods and results, and (iii) the clinical relevance of the currently utilized BMSC- and PDC-based approaches. Systematic review registration: The study was prospectively registered in PROSPERO, Registration No. CRD42021270922.
Impact statement
Bone marrow stromal cells (BMSCs) and periosteum-derived cells (PDCs) represent promising skeletal stem cell sources to treat critical-size bone defects. However, a large number of preclinical tests with a variety of in vivo data complicate the selection of cells for further clinical translation. This review goes beyond summarizing the existing experimental evidence of BMSCs and PDCs by systematically evaluating their performance in bone formation in different defect models. This evidence-based list of well-documented preclinical evaluations will serve as a practical guideline in future research on cell-based therapies for bone repair and reconstruction.
Introduction
Bone tissue possesses regenerative potential, however, bone defects that exceed critical sizes still cannot heal through the natural healing. 1 Hence, the reconstruction of large bone defects caused by trauma, congenital diseases, and tumor section has been a great clinical challenge.2,3 Nowadays, the gold standard to treat complex large bone defects involves transplantation of autogenous or allogenous bone grafts, which can be harvested from the iliac crest, fibula, scapula, or radius. 4 However, the inherent limitations of this approach, including insufficient autogenous resources and donor-site morbidity, 5 strongly urge clinicians and researchers to explore alternative treatment options.
Cell-based approach arises as a promising strategy to treat complex and large bone defects, especially in compromised conditions. It is envisioned that the stem/progenitor cells with the ability to self-renew and differentiate are the key factors in steering bone formation and integration, subsequently leading to the successful healing of the defect.6,7 Therefore, recent research has been focused on the development of cell-based approaches for bone regeneration to overcome the limitations of the existing treatments.
Among various cell types for bone regeneration, bone marrow aspirate and periosteum represent two reliable tissue resources to harvest skeletal stem/progenitor cells with convincing evidence of differentiation capacity both in vitro and in vivo.8–13 Although the bone marrow stromal cells (BMSCs) and periosteum-derived cells (PDCs) shared similarities in trilineage differentiation capacity and surface markers,9,14 they showed different in vitro and in vivo biological performance. For instance, the in vitro proliferation and differentiation capacity of BMSCs diminishes as aging, 15 and after implantation in vivo, BMSCs have been shown to exclusively contribute to fracture healing by intramembranous ossification. 16 On the contrary, PDCs showed a stable in vitro differentiation capacity after several passages, regardless of the donor age. 17 Furthermore, PDCs contributed to the majority of cartilage callus in the defect site,9,16 which is an essential process for the natural healing of bone fracture. 18
Despite numerous studies in both preclinical and clinical settings,8,11,12,19–26 the efficacy of cell-based approaches for bone regeneration remains controversial. Some studies showed that BMSCs-based approaches had a favorable effect on bone formation compared to their controls (e.g., bare scaffold group when the bare scaffold was applied,27–29 while other studies draw the opposite conclusions 30 or reported that there was no significant difference between experiments with or without BMSCs.31,32 The conclusions regarding the efficacy of PDCs also varied. Some studies proved that PDC-based approaches had better efficacy at new bone formation than bare scaffold,33,34 while others demonstrated no significant difference 20 or the opposite. 22 Furthermore, different opinions exist regarding the choice of cell types. Zhu et al 35 reported that PDCs-based approaches showed a superior subcutaneous bone formation compared to BMSCs-based approaches, while other studies showed different conclusions.21,33,36–38
To increase the value of animal experimental work as proofs-of-concept before entering new trials, it is worthwhile to perform a systematic analysis of all preclinical data to determine their potential translational value for human application. Consequently, the purpose of this work was to perform a systematic review and meta-analysis regarding BMSCs- or PDCs-based approach for bone regeneration to obtain more clarity on their in vivo bone-forming efficacy.
Materials and Methods
This review was designed and conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for systematic review incorporating the network meta-analysis. 39 The protocol was registered in the PROSPERO database (CRD42021270922).
Search strategy
Electronic bibliographic databases of MEDLINE/PubMed, EMBASE, Cochrane Central Register of Controlled Trial, and Web of Science were searched from the inception of each database to November 2, 2020. Literature concerning PDC and BMSC was separately searched. The full search strategy was based on four search components: “periosteum-derived cell” (or “bone marrow stromal cell”), “bone regeneration,” “tissue engineering,” and “bone.” Detailed search strategies for PubMed are displayed in Table 1 (the adapted strategies for the other three databases can be found in Supplementary Table S1). No language restrictions were imposed. A manual search was also conducted by searching the major journals of the same field by hand. Bibliographies of selected studies and review articles on the same topic were checked for cross-reference. Unpublished data were searched on OpenGrey.
Search Strategy for PubMed
BMSC, bone marrow stromal cells; PDC, periosteum-derived cell.
Screening and selection of articles
Studies were included when they fulfilled all the following criteria: (1) Preclinical experiments that involved transplantation of BMSC- or PDC-based approaches; (2) Outcome data were presented as quantitative new bone formation (%) after the local application of BMSC- or PDC-based approaches; and (3) Full-text original article. Studies that fulfilled the following criteria were excluded: (1) Models with orthopedic disorders; (2) Coculture of different cells; and (3) Cells were genetically modified or not isolated from the original tissue.
The selection of eligible studies was done in duplicate by two independent reviewers (J.Z. and J.X.) based on the abovementioned inclusion and exclusion criteria. Initial screening was conducted on the titles and abstracts. Eligible studies based on the initial screening were reassessed in the full-text screening for eligibility for inclusion. Any disagreement during these two phases will be resolved through discussion or consulting the third reviewer (W.J.).
Study characteristics and data extraction
The following study characteristics were extracted: the number of animals/defects, animal species, animal sex, implant site, defect size, scaffold material, cell loading number, cell source, healing duration, first author, year of publication, and any other reported adverse events.
The new bone formation (%) measured through histomorphometry was quantified as the outcome measurements used for the meta-analysis. Due to the limited number of the included studies, the results measured by micro-computed tomography (CT) were not used for meta-analysis.
The mean of new bone formation percentage, standard deviation (SD) or standard error of the mean (SEM), and the number of defects per group (n) were recorded or recalculated. If the new bone formation is displayed graphically, data were extracted using ImageJ (1.53a, National Institutes of Health, USA) when possible. 40 If SEM was reported, the SEM was converted to SD. Independent experiments within one article were extracted separately.
Risk of bias assessment
The risk of bias of the included studies was assessed by two reviewers (J.Z. and J.X.) independently using an adapted version of SYRCLE's risk of bias tool. 41 “1. Was the allocation sequence adequately generated and applied? 2. Were the groups similar at baseline or adjusted for confounders? 3. Was the allocation adequately concealed? 4. Were the animals randomly housed during the experiment? 5. Were the caregivers and/or investigators adequately blinded? 6. Were animals selected at random during outcome assessment? 7. Was the outcome assessment adequately blinded? 8. Were incomplete outcome data adequately addressed?” For each item, the risk of bias in the included studies was rated as “high,” “low,” or “unclear.” In item 4, the risk of bias was considered low if the animals were housed singly.
To avoid too many items being rated as unclear due to the poor reporting quality of animal studies, two more questions were added: “(a) Was it stated that the experiment was randomized at any level? and (b) Was it stated that the experiment was blinded at any level?” 42
Data synthesis and statistical analysis
First, a DerSimonian–Laird random-effect pairwise meta-analysis was performed on the outcome measures by computing the standardized mean difference (SMD). Data were analyzed with Stata 16 (StataCorp. 2019). 43 If one reference studied the bone-forming efficacy of two types of cell-based approaches or at various cell seeding densities in different groups of animals, these groups were analyzed as independent experiments. If one control group served more than one experimental group, the number of defects in the control group was divided by the number of experimental groups it served. When several time pointes were assessed, the data at the last time point were extracted.
Subgroup analysis was divided based on the animal model species. Then, the combined effect size (ES) and variance were calculated. Individual and weighted overall ES was displayed using a forest plot. Data were presented as Hedges'g and 95% confidence intervals (CIs). The heterogeneity in the estimates across the different studies was assessed using the Cochrane test for heterogeneity and the I2 statistic. Potential publication bias was assessed by using Egger's linear regression test and funnel plots.
Next, a frequentist random-effect network meta-analysis was performed using the network commands package in Stata.43,44 Inconsistency between the direct and indirect evidence obtained from network meta-analysis was assessed by using the global inconsistency evaluation and loop inconsistency model. Heterogeneity was represented with I2 statistics. Odds ratio (OR) and 95% CI were calculated to compare the effect between groups. The surface under the cumulative ranking (SUCRA) probabilities was then used to rank different treatments.
Results
Description of the included studies
The search strategy described in Table 1 and Supplementary Table S1 retrieved 9838 records, including 1121 and 8717 for PDC- and BMSC-related studies, respectively. After removal of duplicates and initial screening based on titles and abstracts, 513 records (78 and 435 for PDC- and BMSC-related studies, respectively) were included for full-text analysis (Fig. 1), of which 101 records (12 and 88 records for PDC- and BMSC-related studies, respectively) were eligible for systematic review. A total of 94 records were retrieved after removing the 6 duplicate references that involved both PDC and BMSC. Among them, 85 studies compared the BMSC-based approach with a bare scaffold; 9 studies compared PDC-based approach with a bare scaffold. Only 3 studies compared all the three approaches (BMSCs, PDCs, and bare scaffold) in one study.
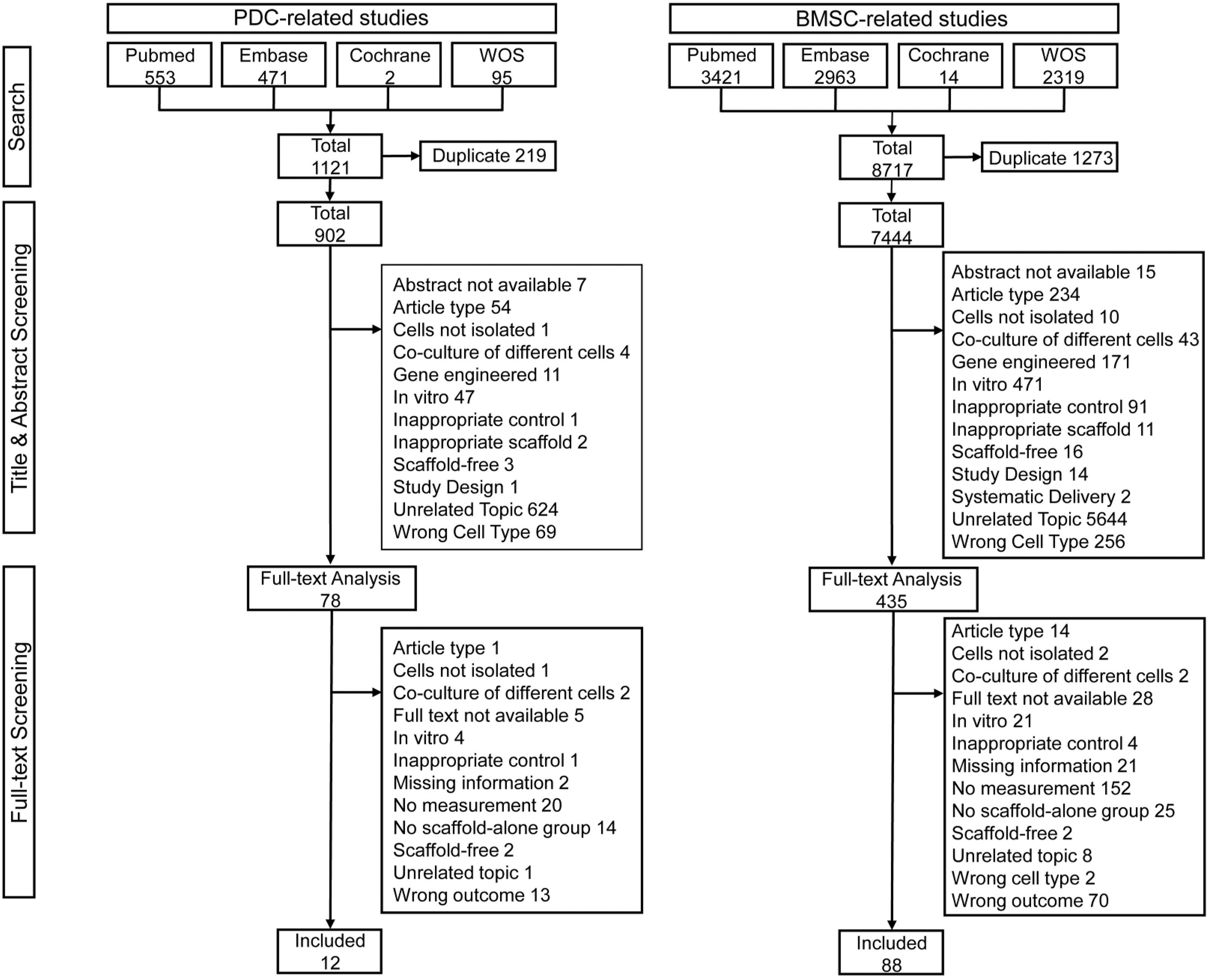
Flowchart of the screening process and study selection. The number of studies in each exclusion category were indicated behind each item. WOS, World of Science.
As shown in Tables 2–4, the characteristics of the included studies varied substantially. Nine different species were used for cell harvest: 26 studies were performed with rats, 21 with rabbits, 15 with humans, 13 with dogs, 7 with goats, 4 with sheep, 4 with mice, 2 with pigs, and 2 with minipigs. The bone marrow aspirates were documented from 5 different tissue origins: 38 studies used femur/tibia, 24 studies used ilium, 2 studies used humerus, 1 study used sternebra, and 23 studies did not specify the origin. In contrast, PDCs were mainly isolated from femur/tibia (8 studies), jaw (3 studies), and calvarium (1 study). Multiple types of cell carriers or biomaterial scaffolds were used, including natural (e.g., collagen and platelet-rich plasma) and synthetic biomaterials. The included synthetic biomaterials were ceramics (e.g., hydroxyapatite, tricalcium phosphate), polymers (e.g., polyglycolic acid), and composites (e.g., apatite-coated silk).
Characteristics of the Included Studies that Compared Bone Marrow Stromal Cells-Based Approach with Bare Scaffold
p < 0.05.
BCP, biphasic calcium phosphate; CAH, chitosan/alginate/HA complex scaffold; CDHA, calcium-deficient hydroxyapatite; CPC, calcium phosphate cement; DBM, demineralized bone matrix; DCPD, dicalcium phosphate dehydrate; GO, graphene oxide; GSB, Gu-Sui-Bu; HA, hydroxyapatite; MMP, matrix metalloproteinase; N, not mentioned; NS, no significant difference; PA6, polyamide 6; PCL, polycaprolactone; PEKK, polyetherketoneketone; PLGA, poly(lactide-co-glycolide); PPF, poly(propylene fumarate); TCP. tricalcium phosphate; “>” or “<” represents that the bone-forming efficacy of BMSC-based approach is higher or lower than bare scaffold.
Characteristics of the Included Studies that Compared Periosteum-Derived Cells-Based Approach with Bare Scaffold
p < 0.05.
Characteristics of the Included Studies that Directly Compared Bone Marrow Stromal Cells-Based with Periosteum-Derived Cells-Based Approach
p < 0.05.
The total cell-loading number ranged from 105 cells to 4 × 107 cells per scaffold, and the cell-loading density ranged from 0.13 × 104 to 10 × 104 cells/mm3 (if the volume of the scaffold was mentioned). The obtained cell-laden constructs were evaluated for bone formation via either ectopic or orthotopic implantation. The ectopic evaluations were mainly performed in subcutaneous pockets (8 studies) or muscles (1 study). The orthotopic evaluations were performed on a variety of defects, including the calvaria defect (40 studies), jaw defect (16 studies), femoral/tibial defect (16 studies), radial/ulnar defect (6 studies), iliac defect (2 studies), and sternal defect (1 study). The orthotopic defects were categorized as bicortical (49 studies) if they penetrate both layers of cortical bone. Otherwise they were categorized as monocortical (28 studies).
The animal models used for evaluation included rat (31 studies), rabbit (22 studies), dog (13 studies), mouse (11 studies), goat (7 studies), pig (4 studies), and sheep (4 studies).
Regarding the outcome measures, both histomorphometry and microCT were used to quantify the bone-forming efficacy, and the results of individual documentation varied (Table 2–4). Notably, 29 out of 85 studies compared BMSC-based approach with the bare scaffold based on microCT analysis, and 21 of them showed a significant superiority of BMSC-based approach over the bare scaffold (Table 2). In comparison, only one study compared PDC-based approach with the bare scaffold using microCT, and no significant difference was observed (Table 3). Furthermore, no studies used microCT as outcome measurements to directly compare BMSC with PDC-based approach.
Hence, only histomorphometric new bone formation outcome measurement was chosen for further meta-analysis. Based on histomorphometry, 52 out of 66 studies demonstrated a significant superiority of the BMSC-based approach over the bare scaffold group (Table 2). Five out of eight studies showed a higher bone-forming efficacy of the PDC-based approach compared with the bare scaffold group (Table 3). Notably, among the six studies that directly compared the PDC-based approach with the BMSC-based approach, four studies showed no significant difference between these two types of cells, whereas the other two studies revealed the superiority of either BMSCs or PDCs over their counterpart (Table 4).
Risk of bias and quality of reporting
Figure 2 shows the overall results of the risk of bias assessment of the 94 studies included in this systematic review. Regarding the selection bias, 59.57% of the included studies reported randomization across the experiment. However, only 18.09% stated the application of allocation sequence, and only 8.51% mentioned allocation concealment. Of the included studies, 72.34% stated similar baseline characteristics between experimental and control groups. In addition, 68.08% and 89.36% of the included studies were scored as under unclear risk of bias concerning the performance bias items “random housing” and “blinding,” respectively.

Risk of bias evaluated using an adapted version of SYRCLE's risk of bias tool. The risk of bias of each study was rated as “high,” “low,” or “unclear.” Color images are available online.
For the detection bias item “random outcome assessment,” 100% of the included studies were scored as low risk of bias, because the outcome of invention and control groups were assessed at the same time points. Only 21.28% of the studies reported that outcome assessment was blinded based on item 7. For attrition bias, 95.74% of the studies were scored as low risks of bias, as they adequately addressed incomplete outcome data.
Pairwise meta-analysis of outcome measures
A total of 66 studies were included for a pairwise meta-analysis of the BMSC-based approach vs the bare scaffold group. BMSC-based approach showed significant higher efficacy (SMD and 95% CI: 2.59 [2.11–3.07]; I2 = 87.26%, p < 0.001) than the bare scaffold group (Fig. 3). Subgroups analysis showed a beneficial effect of BMSCs in all animal species model except sheep. Interestingly, the SMDs in dog and mouse subgroups were higher than in other groups. Regarding PDCs, the pairwise meta-analysis revealed no statistically significant difference between PDCs and a bare scaffold on the basis of a total of 8 studies (SMD and 95% CI: 0.48[−0.16 to 1.13]; I2 = 75.42%, p < 0.001) (Fig. 4).
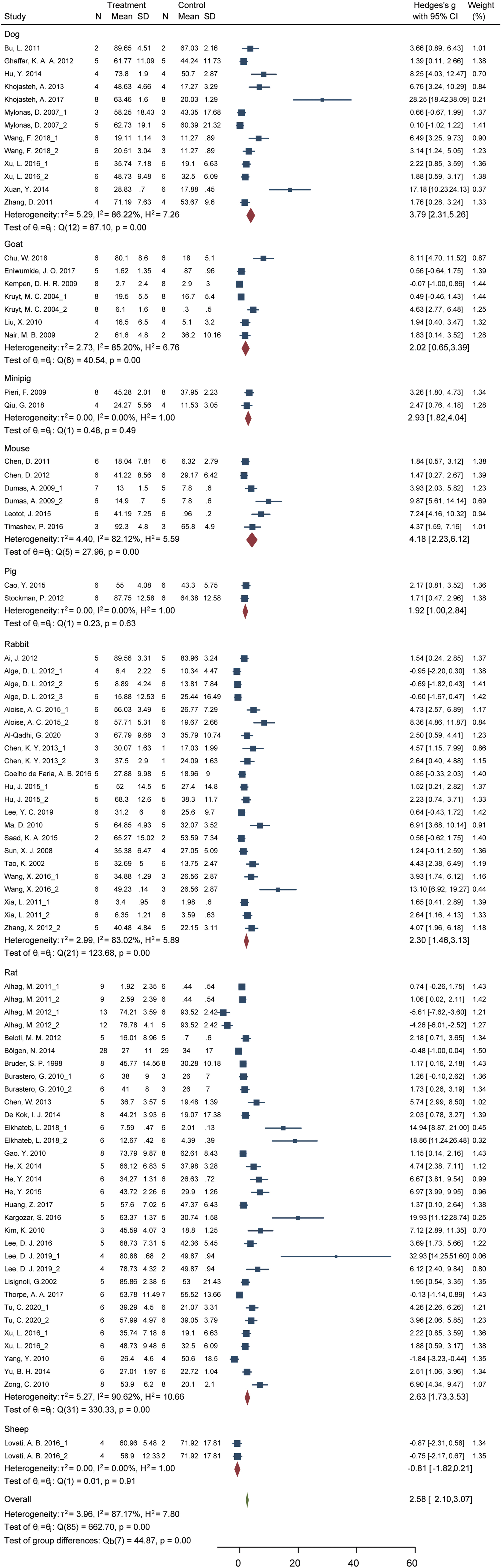
Forest plot of the studies that compared BMSC-based approach with bare scaffold group in the pairwise meta-analysis. The forest plot displays relative weight of individual experiments, the SMD, and 95% CI. The diamond indicates the global estimate and its 95% CI. BMSC, bone marrow stromal cells; CI, confidence interval; SMD, standardized mean difference. Color images are available online.

Forest plot of the studies that compared the PDC-based approach with the bare scaffold group in the pairwise meta-analysis. The forest plot displays relative weight of individual experiments, the SMD, and 95% CI. The diamond indicates the global estimate and its 95% CI. Color images are available online.
It is noted that substantial variation of the results existed in different animal models. Favorable effects of PDCs were only observed in mouse and pig models. We further performed a pairwise meta-analysis of the six studies involving a direct comparison between the PDC-based approach and the BMSC-based approach. Given the small number of studies, there was no significant difference between these two groups (SMD and 95% CI: −0.79[−2.76 to 1.18]; I2 = 95.57%, p < 0.001; Fig. 5). Furthermore, slight favorable effect of the PDC-based approach showed over MSC-based approach was observed in dog models.
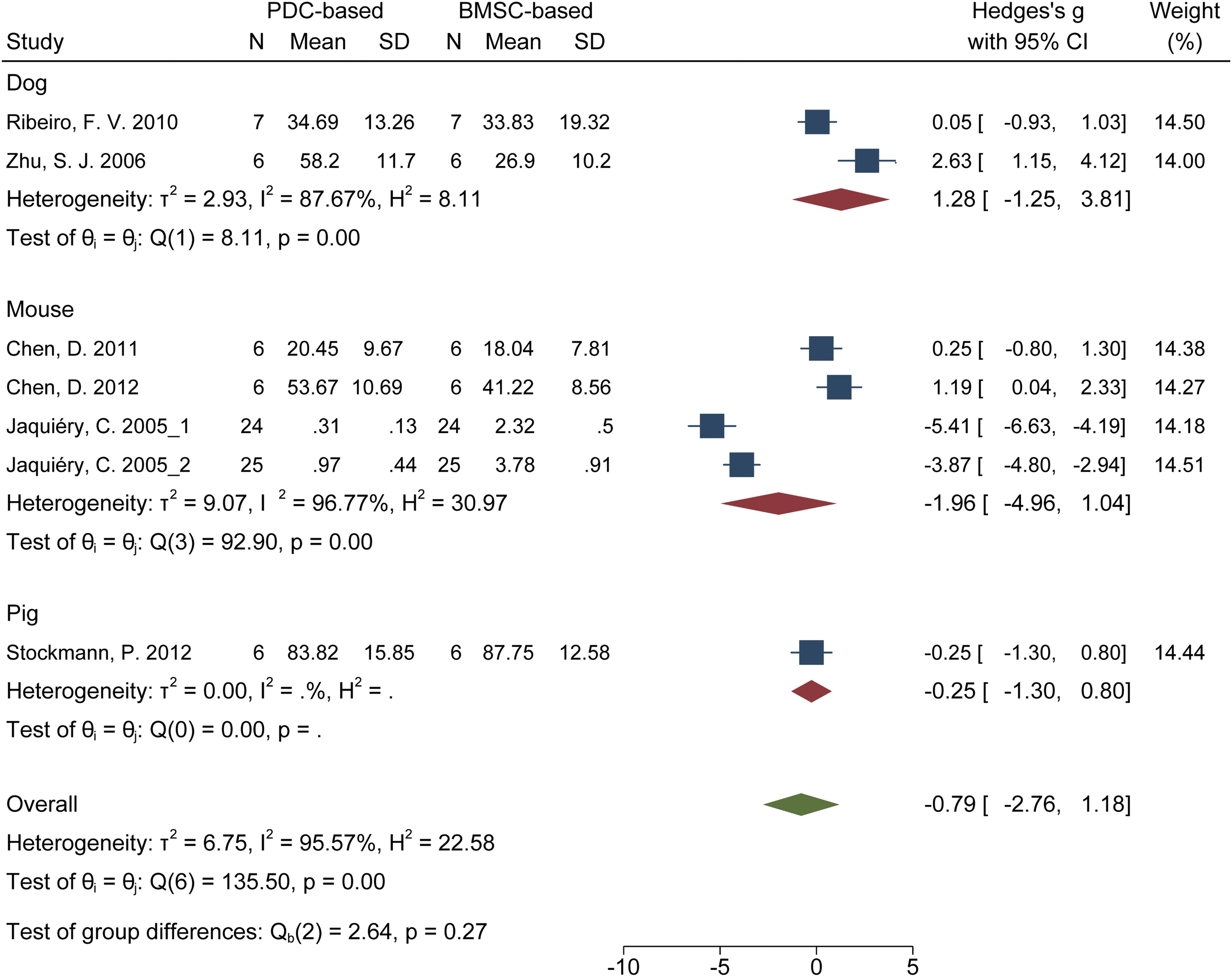
Forest plot of the studies that directly compared the PDC-based approach with the BMSC-based approach in the pairwise meta-analysis. The forest plot displays the relative weight of individual experiments, the SMD, and 95% CI. The diamond indicates the global estimate and its 95% CI. Color images are available online.
Among the funnel plots of the three pairwise meta-analyses, the studies that compared the BMSC-based approach with bare scaffold showed obvious underrepresentation of the small, negative studies (Supplementary Fig. S1a). The funnel plots of the other two pairwise meta-analyses appeared to lack studies of large sample size (Supplementary Fig. S1b, c).
Network meta-analysis
To address the issue of a lack of sufficient studies with direct evidence, the network analysis was further performed to compare the BMSC-based approach to the PDC-based approach, which consisted of three arms, namely: the BMSC-based approach, the PDC-based approach, and the bare scaffold group (Fig. 6a). By doing this, an indirect comparison between BMSC-based and PDC-based approaches can be achieved through the common comparator “the bare scaffold group.”45,46 Furthermore, network meta-analysis can combine direct evidence (studies that directly compared BMSC-based and PDC-based approaches) with indirect evidence (studies that compared them via “the bare scaffold group”) to calculate a mixed effect size, hence facilitating an increased amount of evidence. 46

Results of network meta-analysis.
Our results suggested that no obvious heterogeneity (I 2 = 0.4%) and no obvious publication bias (Supplementary Fig. S2) were detected between comparisons. Furthermore, no significant inconsistency in our analyses was detected based on the results of consistency test using global inconsistency and loop inconsistency model (Supplementary Tables S2, S3).
Our data revealed that compared with the bare scaffold group, both the BMSC-based approach (OR = 13.32, 95% CI: 10.40–16.25) and the PDC-based approach (OR = 10.88, 95% CI: 3.65–18.11) significantly enhanced new bone formation (Fig. 6b). However, no significant difference was found between these two types of cell-based approaches (OR = −2.452, 95% CI: −9.84 to −4.85), which was consistent with the aforementioned pairwise meta-analysis in Result 3. Furthermore, SUCRA values showed that the BMSC-based approach was most likely (74.2%) to be ranked the best among all the three interventions, while the probability to be ranked best of PDC-based approach and bare scaffold were 25.8% and 0.0%, respectively (Fig. 6c–f).
Discussion
This review aimed to systematically evaluate the bone-forming efficacy of the BMSCs- and PDCs-based approaches. The result of this systematic review and pairwise meta-analysis revealed that the BMSCs-based approach had a favorable effect on new bone formation, as displayed by the positive effect on histomorphometric analysis. However, BMSCs-based and PDC-based approaches had no significant difference. Network meta-analysis was further conducted to increase the amount of evidence to compare these two cell-based approaches. The results suggest that both BMSC and PDC can improve new bone formation compared with the bare scaffold. Although OR and 95% CI showed no significant difference between BMSC and PDC, SURCA ranking suggested that BMSC had a higher probability to be ranked better than PDC.
The currently used approach of systematic review allowed the inclusion of a sufficient number of studies, which involved BMSCs- or PDCs-based approaches for bone regeneration. By doing this, we could perform the meta-analysis and explore the effect in different subgroups. However, there are some potential limitations related to this approach. First, due to the nature of animal studies, experimental variabilities existed regarding the animal species, tissue origin of seed cells, animal model species, implant site, defect type and size, and so on, which, not surprisingly, leads to substantial statistical heterogeneity.47,48 To account for the expected heterogeneity, a random effect model was used in the pairwise meta-analysis. Also, subgroups analyses regarding animal model species were performed to explain the heterogeneity.
However, the subgroup analyses did not notably reduce the heterogeneity except in the PDC-based approach vs bare scaffold. Notably, as shown in funnel plots, pairwise meta-analyses were subject to publication bias, which can be caused by either nonpublication of negative results, small sample size, or other factors, including true study heterogeneity or differences in study quality. 49 Finally, the study quality assessment revealed poor reporting quality of animal studies existed in the evaluation of cell-based approaches. Most items in the assessment were rated as unclear because they were not mentioned in the articles. 41 To avoid bias, randomization and blindness are strongly suggested for preclinical and clinical studies. However, only 18.08% of studies reported the generation of a random allocation sequence. Also, only 21.2% of the studies reported blindness across the experiment. Therefore, the results of our systematic review and meta-analysis might cause overestimates of certain interventions.
Despite these limitations, the combined analysis of the included studies still generated extra and valuable information that could not be derived from individual studies.
One of the most important issues for the clinical application of cell-based approaches is the type of cell used. As shown in this systematic review, BMSCs have been explored extensively in both preclinical evaluations for bone regeneration, while the studies that explored PDCs-based approaches are rather limited. Currently, many systematic reviews were conducted focusing on the bone regeneration capacity of BMSCs or bone marrow aspirates,50–54 most of which showed promising results of BMSC-based cell therapy in treating long bone reunions, 50 osteoporosis, 53 and osteoarthritis. 54 However, these studies either included a variety of bone marrow-derived products50,51 or only evaluate in a certain disease model.53,54 No systematic review and meta-analysis of the bone regeneration capacity of BMSC-based approach in bone defects was conducted.
Meanwhile, PDC was an emerging source for bone tissue engineering, and there is currently no systematic review regarding its bone-forming efficacy, let alone the comparison between BMSCs and PDCs. In our systematic review, 64 out of 85 studies reported a positive effect of BMSCs on bone formation. For PDCs, five out of nine demonstrated a statistically significant improvement in new bone formation. The result of the meta-analysis revealed that BMSC-based approach had significantly higher bone-forming efficacy than the bare scaffold. However, no significant difference was found between the PDC-based approach and bare scaffold and the PDC-based approach and bare scaffold. This result is probably due to the limited study number and the obvious heterogeneity (I 2 = 75.42%, p < 0.001; I2 = 95.57%, p < 0.001) within the included studies.
To assess the possible influence of variables on cell-based approach, subgroup analysis regarding animal model species was performed. For BMSC-based approach, rabbit and rat were the most frequently used models, which both showed similar results with the overall effect. Interestingly, studies using mouse as animal model showed higher SMD than other species, which suggested that caution must be taken before scaling preclinical studies up to large animal models because mouse model might overestimate the bone-forming efficacy of cell-based approach. Similar implication can also be obtained from the subgroup analysis of PDC-based approach versus bare scaffold.
To compare the bone-forming efficacy between BMSCs and PDCs, we performed a network analysis to minimize the bias that caused by the limited number of PDCs-related studies.45,46 Network meta-analysis can integrate the effect size of both direct and indirect evidences, providing more comparisons between interventions. 45 Currently, this powerful tool has been used to compare of tissue regeneration capacity between different stem cells. 55 The result of heterogeneity assessment and inconsistency evaluation suggested the successful establishment of the network meta-analysis model. Our network meta-analysis showed that both BMSCs and PDCs showed a comparable positive effect on new bone formation, although BMSCs had a higher ranking probability than PDCs. Therefore, our results indicated that both BMSCs- and PDCs-based approaches can be applied for bone regeneration, and their actual implementation in clinical practice could be based on the specific condition of each individual patient (e.g., accessibility of cells and health condition of donor tissues). 56
Conclusion
The current systematic review and meta-analysis indicate that both BMSCs- and PDCs-based therapies have a positive effect on in vivo bone formation compared to scaffold-only therapies. Moreover, there is no statistically significant difference between BMSCs and PDCs regarding in vivo bone-forming efficacy, although BMSCs have a higher probability to be ranked better than PDCs. These results provide important information for the implementation of cell-based approaches in clinical practice as a routine treatment in the future.
Footnotes
Acknowledgments
The authors thank Professor Yukang Tu from National Taiwan University and Professor Fang Hua from Wuhan University for their kind help in the methodology of this research.
Authors' Contributions
J.Z.: Methodology, Formal analysis (equal), Investigation (equal), Data curation (equal), Writing—original draft, and Visualization (equal). J.X.: Formal analysis (equal), Investigation (equal), Data curation (equal), Draft editing, and Visualization (equal). W.J.: Conceptualization, Methodology, Writing—Review and Editing, Supervision, Project administration, and Funding acquisition.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is funded by the National Natural Science Foundation of China (No. 82170931), the Natural Science Foundation of Hubei Province (No. 2020CFB618), and the Fundamental Research Funds for the Central Universities (No. 2042022kf1172).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.