
Abstract
Tendon injuries disrupt the transmission of forces from muscle to bone, leading to chronic pain, disability, and a large socioeconomic burden. Tendon injuries are prevalent; there are over 300,000 tendon repair procedures a year in the United States to address acute trauma or chronic tendinopathy. Successful restoration of function after tendon injury remains challenging clinically. Despite improvements in surgical and physical therapy techniques, the high complication rate of tendon repair procedures motivates the use of therapeutic interventions to augment healing. While many biological and tissue engineering approaches have attempted to promote scarless tendon healing, there is currently no standard clinical treatment to improve tendon healing. Moreover, the limited efficacy of systemic delivery of several promising therapeutic candidates highlights the need for tendon-specific drug delivery approaches to facilitate translation. This review article will synthesize the current state-of-the-art methods that have been used for tendon-targeted delivery through both systemic and local treatments, highlight emerging technologies used for tissue-specific drug delivery in other tissue systems, and outline future challenges and opportunities to enhance tendon healing through targeted drug delivery.
Impact statement
Tendon injuries heal in a scar-mediated manner, which lead to numerous complications. However, there is currently no pharmacological approach to augment the tendon healing process. This can be attributed to the lack of targeting modalities within the tendon to which drug carriers can be directed, as well as the lack of effective therapeutic molecules. In this review, we identify promising approaches that are currently used in other tissues, which can be leveraged to promote effective, tendon-targeted drug delivery and provide our perspective on the key considerations for tendon-targeted drug delivery, and the challenges and opportunities that exist in this space.
Introduction
Tendons are dense, fibrous connective tissues primarily composed of Type I collagen that transmit mechanical forces from muscles to the bone. 1 While there is diversity in tendons, such as size, location, and structure, there are several conserved means through which tendon homeostasis is disrupted. More specifically, tendons are susceptible to tendonitis, tendinopathy, age-related degeneration, sprains, and acute rupture or traumatic injury.2–6 Nearly half of all musculoskeletal injuries reported in the United States involve tendons and ligaments, and these disorders lead to many complications and challenges. 3 The most common complications that occur with tendon injuries include re-rupture due to an insufficient initial healing response, excess postoperative scarring, joint contracture, and infections.1,2,4,7–12
Collectively, these complications result in a lengthy rehabilitation process and unsatisfactory healing outcomes that substantially impair the restoration of quality of life and impact patients' ability to meet their recreational, occupational, and physical function goals. 11 Moreover, as the human population ages and life expectancy increases, it is estimated that 25% of all adults will suffer a tendon-related injury due to a combination of disrupted tendon homeostasis and an impaired healing response after injury, which will further burden the health care system financially, and thus increase the need for therapeutic interventions.5,7,10,11,13
Current approaches to treat tendon disorders and their associated complications can be broadly classified as either operative or nonoperative (conservative) treatments. Operative treatments include surgery with or without a tendon transplant, usually followed by lengthy periods of rehabilitation and nonsteroidal anti-inflammatory drugs (NSAIDs) to manage pain. 14 Alternatively, conservative treatment methods such as ultrasound, laser, and shock wave therapy are also effective in managing pain. However, growing evidence from randomized controlled trials and observational studies suggests that these conservative treatments are only beneficial when used in combination with other interventions like exercise, which increases loading and helps to stimulate healing.15,16
In addition, surgical and conservative treatment approaches have also incorporated adjuvant approaches, including biomaterials such as chitosan, poly(lactic acid) (PLA), and hyaluronic acid as mechanisms to deliver therapeutics to resolve inflammation, promote matrix remodeling, and increase mechanical integrity. However, to date, there is no consensus on standard biomaterial treatment that restores preinjury tendon structure and function. In particular, the lack of effective therapeutic strategies to improve tendon healing can be attributed to the paucity of fundamental cellular and molecular understanding of tendon cell biology and the mechanisms underlying tendon pathophysiology.
This gap in knowledge limits the identification of possible targets that can be leveraged for improved tendon healing and function. Collectively, the successful therapeutic approach(es) to facilitate tendon healing requires a complete understanding of the anatomy, and molecular basis of healing of tendons in different anatomical locations and their potential complications and outcomes, 5 to facilitate the successful restoration of function, minimize disability, and reduce the risk of complications.
In this review, we discuss tendon-targeted and systemic approaches to deliver drugs to the tendon to promote healing and the advantages and disadvantages associated with each method. In addition, we provide our perspective on targeting approaches that can be leveraged in the tendon to control drug delivery. Since most studies employing nanotechnology in the tendon use mid-substance injuries as experimental models compared to other injury models like tendon-bone injuries, we have chosen to primarily focus this review on acute mid-substance injuries. While we do not explicitly discuss tendon-bone injuries due to the unique challenges and opportunities associated with this tissue interface, we provide a few examples of how nanotechnology can be used in this setting in our comprehensive tables. We also briefly discuss other tendon injuries, including tendonitis and degeneration, within our comprehensive tables and future perspectives section.
Systemic Versus Local Drug Delivery
Drugs can be delivered to the tendon by two major approaches: systemically or locally. Local delivery refers to using biomaterials, synthetic or natural, to deliver a minimal amount of drug locally to the affected tissue. Local delivery can be classified into noninjectable/preformed solid implants (preformed hydrogels, films, sponges, stents, and fibers) and injectable implants (in situ cross-linkable hydrogels and nanoparticles/microparticles). 17 Alternatively, systemic delivery refers to a route of delivery directly into the bloodstream to reach all areas of the body. It can be achieved through intravenous injection, intramuscular injection, subcutaneous injection, and oral delivery. 18
Both systemic and local delivery approaches have unique context-dependent strengths and weaknesses that must be considered in designing an efficient drug delivery system. For example, the properties of the drug (e.g., size, surface modality, etc.), the desired therapeutic window, and the location of the injury all need to be considered. To leverage therapeutic efficacy, while reducing side effects such as cytotoxicity, drugs can be administered directly to the diseased site (i.e., local delivery) or delivered systemically based on the considerations. In the tendon, localized drug delivery mechanisms have dominated the field due to the ease of administration and the lack of tendon-targeted drug delivery methods for systemic treatments.19,20
Local drug delivery modalities include natural and synthetic scaffolds, fibers, sponges, and stents. 12 The primary advantage of local delivery consists of the immediate supply of a therapeutic to the injury site, while minimizing off-target tissue exposure. Furthermore, biomaterials used to deliver drugs locally can also be engineered to provide relevant cues to dictate specific aspects of cell function. However, these local delivery approaches have pitfalls. For example, it can be difficult to control the degradation rate of biomaterials at the injury site, which can cause an increased inflammatory response, impact the metabolic activity and extracellular matrix (ECM) deposition capacity of tenocytes, and cause cytotoxicity.12,21
Furthermore, drugs and growth factors delivered locally with biomaterials are typically released and cleared rapidly due to suboptimal loading capacity and release kinetics. In addition, inadequate binding affinity (e.g., how tightly a drug binds to the scaffold) is a crucial consideration as the binding affinity must be low enough to ensure the release of the drug, but high enough to prevent drug dumping and toxicity. 22 Furthermore, using biomaterials to deliver drug depots to the tendon ensures site-specific drug delivery; however, this approach requires invasive procedures, which may disrupt the physiological healing response.12,20,22–26 Even with the intraoperative application, embedding foreign materials at the repair site may cause additional complications, such as sustained inflammation. 26 In addition, local injection of drugs directly into the tendon may reactivate the inflammatory response and can result in drug dumping, leading to rapid local clearance and off-target effects.9,27,28
Systemic drug delivery approaches such as nanotechnology have been employed to combat the disadvantages of local drug delivery. Nanotechnology enables the controlled delivery of drug payloads, and this approach has primarily been used to target immune and reparative responses after injury. 29 Due to their small size and surface properties, nanoparticles (NPs) can reach all tissues, which can be disadvantageous if drugs are distributed to unintended tissues. 30 However, nanotechnology modalities are attractive because they can be designed to have high specificity, ensure the stability of the loaded drug, have high loading capacity, and, perhaps most importantly, be biocompatible.31,32
Biomaterials for Local Drug Delivery
Coated sutures
Acute tendon injuries are common and often require surgical intervention. However, postoperative healing is often associated with an increased risk of re-tear, especially during early postoperative mobilization protocols. 33 High re-tear rates are attributed to the weakened tendon tissue around the suture, which allows the suture to cut through the tissue after exposure to tensile stresses. To overcome these complications, exogenous cross-linking agents, growth factors, and cells can be applied to the surgical site to augment healing and increase the mechanical integrity and prevent repair failure.33–41
While the primary purpose of sutures is to reduce gap formation and promote mechanical stability after tendon rupture, sutures can also be leveraged as drug carriers to reduce re-tear rates and/or minimize scar tissue formation. For example, Pasternak et al investigated the effects of doxycycline-coated sutures on the suture-holding capacity of repaired rat Achilles tendon (AT). 33 This study used a 3–0 polybutylester monofilament suture treated with radiofrequency plasma and coated with doxycycline, a matrix metalloproteinase (MMP) inhibitor, to repair an AT transection. The doxycycline-coated sutures inhibited degradative processes associated with surgical re-tears, thereby improving the suture-holding capacity. 33
Moreover, Chamberlain et al used BMP-12-releasing sutures to repair AT ruptures and demonstrated reduced adhesion formation relative to tendons that were fixed with untreated mineral sutures. 34 Several other studies have reported the beneficial effects of sutures as drug carriers on tendon healing (Table 1). Coated sutures are advantageous as drug vehicles because they are close to the tendon and therefore do not require biomaterial drug vehicles. However, a significant disadvantage is that they can only be used to deliver extremely small amounts of the drug (nanograms—micrograms) because only a few centimeters of the suture is typically required for surgical repair. Drug-laden sutures also have no sustained release characteristics, which limits therapeutic efficacy.
Summary of Coated Sutures in Tendon Healing
AT, Achilles tendon; bFGF, basic fibroblast growth factor; EDC, 1-ethyle-3-(3-dimethylaminopropyl) carbodiimide; FDL, flexor digitorum longus; PDS, polydioxanone; rhPDGF-BB, recombinant human platelet-derived growth factor-BB; VEFGA, vascular endothelial growth factor A.
Furthermore, since the sutures used for tendon repair are usually only administered intraoperatively, the drugs loaded onto the sutures are only available during the early phases of tendon healing. They therefore have limited ability to modulate later stages of the healing process. Finally, sutures are suboptimal carriers for growth factors, given the rapid degradation of growth factors by proteases in the healing environment. Hence, more recent studies are focused on using nanocarriers/plasmid complex-coated sutures to facilitate sustained release. 41
Polymeric scaffolds
To date, numerous biopolymers have been assessed for tendon repair, with variable degrees of efficacy.12,19,20,22–26,36,42–48 Advancements in polymer chemistry and biotechnology have increased the availability of technologies to fabricate hierarchical three-dimensional scaffolds. The scaffolds can be customized to closely imitate native tendon architectural features, while enabling localized and sustained delivery of therapeutics. These scaffolds come in various forms, including electrospun fibers, composite hydrogels, and cell sheets

Approaches to promote tendon healing. Current approaches to promote tendon healing include tissue engineering approaches mediated by use biomaterials such as scaffolds and NPs. Scaffolds, including
Synthetic polymers allow a high degree of customization, which facilitates broad biological application. For example, synthetic polymer scaffolds such as PLA, poly(glycolic acid) (PGA), poly-ɛ-caprolactone (PCL), and poly(lactic-co-glycolic acid) (PLGA) are commonly used in preclinical models of tendon injury as they can provide a high degree of mechanical stabilization.48,50,51 However, synthetic polymers have several disadvantages. Most synthetic polymers have very low biodegradability and must therefore be eliminated through renal excretion. As such, the molecular weight of polymers is a key consideration to ensure successful excretion.22,46,49,52,53 Because of this, polymer scaffolds are primarily used for the repair of minor injuries that require relatively small scaffolds. For example, a controlled-release scaffold for the delivery of Ibuprofen was developed in a previous study by Hu et al, which revealed that electrospun fibers loaded with Ibuprofen were effective in minimizing adhesion formation in a chicken flexor tendon model.
Specifically, poly(lactic acid) (PLA) fibers synthesized by a co-solvent method were loaded with mesoporous silica nanoparticles (MMS) containing Ibuprofen and electrospun to form composite fibrous membranes. Following transection and repair of the flexor digitorum profundus tendon, ibuprofen-loaded fibrous membranes were wrapped around the repair site. Histological analysis of harvested tendons 4 weeks postinjury revealed that the PLA-MMS-Ibuprofen fibrous membranes were effective in reducing tissue adhesion and inflammation. Although no significant improvement in mechanical properties was observed, the PLLA-MMS-Ibuprofen membrane demonstrated controlled release of the loaded drug over a long period of time (8 weeks). 54
Natural polymers (e.g., chitosan, chondroitin sulfate, alginate, and hyaluronic acid) are broadly used to treat tendon injuries because they provide important biochemical cues and facilitate cell adhesion. 55 Natural polymers also overcome many challenges of synthetic polymers due to uncontrolled cell-dictated degradation. However, natural polymers lack the mechanical stability of synthetic polymers, and often lack the desired topographical properties, matrix stiffness, alignment, and fiber pore size required to influence the proper function of immune cells and tendon cells, including enabling these cells to contract and migrate as needed to phagocytose debris and dead cells, as well as deposit and remodel the matrix.12,22
Furthermore, natural scaffolds depend on basic diffusion and desorption to release drug depots. 56 As such, natural scaffolds result in an initial, uncontrolled burst release of the loaded drug, which may be followed by a first-order release depending on the material properties of the scaffold. This burst release exposes cells to high levels of drug soon after polymer delivery, which may be undesirable for proper healing, and can lead to high cytotoxicity.
Therefore, further studies are needed to identify the properties required for these engineered scaffolds to serve as optimal drug carriers, to promote tendon healing. 57 To investigate the potential of a small molecule drug delivered in a controlled-release manner, a hydrogel-based scaffold comprising hyaluronic acid was applied in a chicken flexor tendon model to deliver rhynchophylline (Rhy). Rhy is a small molecule drug which can act by downregulating TGF-β1 to reverse tenocyte dysfunction, and has been proven effective in minimizing abdominal adhesions. Biomechanical analysis of harvested tendons 6 weeks postinjury revealed that Rhy-loaded hydrogels inhibited tendon adhesion formation and improved gliding compared to the control group. 58 This study established the benefit of using PEG diacrylate as a cross-linker to enable sustained, controlled release of small molecule drugs from hydrogels.
In summary, polymeric scaffolds have several benefits including extended bioavailability to increase the duration of drug action, minimizing the frequency of drug administration, and subsequently reducing possible drug side effects. In addition, polymeric scaffolds improve drug utilization by minimizing premature drug degradation and loss and require lower drug doses due to the benefits of local administration12,20,22,23,26 (Table 2). However, a major pitfall of polymeric scaffolds for localized drug delivery is the necessary surgical intervention to either administer or remove the scaffold when needed, which may lead to further complications such as excessive scarring, and can lengthen the recovery and rehabilitation process. 12 In addition, maximizing drug utilization is a key consideration for polymeric scaffold design.
Summary of Drug-Loaded Polymeric Scaffolds in Tendon Healing
GDF-7, growth and differentiation factor 7; HBDS, heparin-based delivery system; PDGF-BB, platelet-derived growth factor-BB; PLGA, poly(lactic-co-glycolic) acid; PPLA, poly-l-lactic acid; TGF-β1, transforming growth factor β1.
More specifically, polymeric scaffolds must allow uniform drug distribution throughout the entire scaffold, permit drug release at a pre-established rate, possess sufficiently low drug binding affinity to ensure drug release at physiological conditions (i.e., pH, temperature), and must possess stable chemical structure, biological activity, and physical dimension over an extended duration. However, the design and manufacturing of polymeric scaffolds that meet these criteria represent a key technical hurdle.22,59 Some of these hurdles include reproducibility (scale-up), sterilizability, and physicochemical stability of drug during scaffold manufacture and processing. 59 Studies in other tissues such as the bone and heart have addressed some of these challenges. In bone tissue engineering, approaches to sustain drug release has been an area of intense interest. These include incorporating mechanisms to decouple the drug release mechanism from the intrinsic degradation kinetics of the scaffold to promote longer drug retention. 60
Furthermore, mechanisms to modify the degradability or electrochemistry of polymers by incorporating counter-ion charged agents and alternating the rows of charged polymers to extend the span of drug release have been investigated.60,61 As an approach to ensure drug stability during manufacturing, as well as promote sustained drug release, other studies have encapsulated drugs in nanospheres/microspheres embedded in hydrogels. This mechanism is attractive because the encapsulation system can be made from a different material than the scaffold, thus allowing several possible combinations of polymers to promote effective scaffold synthesis.62–64 Furthermore, encapsulating the drug in a nanocarrier/microcarrier establishes the presence of a second physical hindrance to minimize premature drug loss. 65
Tissue-Targeted Systemic Treatment: Current Approaches and Opportunities
Systemic delivery refers to direct drug delivery to the bloodstream, resulting in broad release to most areas of the body. These routes include intravenous injection, intramuscular injection, subcutaneous injection, and oral delivery. 80 Despite the relative success of systemic delivery, it is a challenge to avoid burst release at the time of administration followed by subsequent drops to subtherapeutic drug levels, and difficulty controlling drug levels over extended periods of time. 81 Recently, new strategies have been developed that enable precise control over multiple properties to enhance treatment performance, including improved tissue-specific delivery.62,82,83 Therefore, the advantages of current systemic drug delivery approaches over local delivery include the ability to deliver a drug more accurately with less frequent dosing, the ability to engineer carriers that enable reduced variability in systemic drug concentration, and reduced toxicity. 49
NPs for systemic drug delivery
NPs have been employed in systemic drug delivery approaches because of their high tunability. NPs can be engineered with specific properties that are required for effective drug delivery,29,31,32,84,85 which lower possible side effects of the drug payload in nontarget organs and tissues. NPs can also be designed to control drug release mechanisms and kinetics once at the target site through physiological or chemical triggers. 53 Hence, NP-based drug delivery technology can overcome many limitations of traditional delivery, including issues related to biodistribution and intracellular trafficking, can effectively prolong circulation time of drug payloads to increase efficacy, enhance the solubility and stability of drugs, and promote transport across membranes.29,31,32,86
Although the field of targeted drug delivery systems has seen significant growth within the last decade, only a few studies have attempted to use these approaches to enhance tendon healing (Table 3). For example, a collagen hybrid peptide (CHP) was used to modify the surface of PLGA NPs, which were used to deliver rapamycin to injured tendon sites by subcutaneous injection. 86 The targeting of denatured collagen chains facilitated accurate positioning and integration of the PLGA into the injured tendon rather than adjacent healthy tendon and resulted in sustained release of rapamycin and inhibition of endochondral ossification. 86 The PLGA NPs were synthesized using oil/water emulsion-solvent evaporation technique and were subsequently conjugated to the CHP by covalent bonding with glutaraldehyde as a cross-linker. 86
Summary of Drug-Loaded Nanotechnology in Tendon Healing
CHP, collagen hybrid peptide; COX, cyclooxygenase; DMAEMA, dimethylaminoethyl methacrylate; GelMA, gelatin-methacryloyl; LF/Hep-PLGA NPs, lactoferrin-immobilized, heparin-anchored, poly(lactic-co-glycolic acid) nanoparticles; NPs, nanoparticles; PEG, poly(ethylene glycol); PPZ, poly (organophosphazene).
Collectively, this study demonstrated the potential of CHP-PLGA NPs as an effective drug delivery system with targeted binding, sustained-release ability, and retention of drug bioactivity to treat tendon disease. However, while PLGA has been shown to produce acidic byproducts, which can result in inflammation, 86 no study was conducted to investigate the inflammatory response of cells in the tendon to these NPs, which will be an important consideration for future studies. In another study, siRNAs complexed with cationic NPs facilitated intracellular delivery of Serpine1 silencing siRNAs. 87 Diblock copolymer NP with cationic corona blocks of dimethylaminoethyl methacrylate (DMAEMA) and pH-responsive hydrophobic core blocks of DMAEMA, butyl methacrylate, and propylacrylic acid (PAA) were synthesized through reversible addition-fragmentation transfer.
While the cationic corona blocks of DMAEMA enabled complexing to, and protection of the siRNA, the pH-responsive hydrophobic core blocks enabled endosomal escape after protonation, ensuring cytocompatibility and effective gene silencing. Following flexor tendon injury, NP-siRNASerpine1 labeled with Cy-3 dye was subcutaneously injected into the laceration site. Live animal imaging showed that, although NP-siRNASerpine1 was localized to the injury site, it was rapidly cleared after 24 h. Nevertheless, Serpine1 gene expression in the treated tissues was significantly reduced compared to controls, resulting in reduced MMP activity. 87 Hence, this study demonstrates the potential of polymeric NPs as siRNA carriers for controlled-release drug delivery in the tendon.
To leverage the beneficial properties of NP drug delivery systems, while overcoming limitations of polymeric scaffolds as drug carriers, other studies have incorporated NPs into porous scaffolds to overcome issues relating to drug loading and release kinetics (Table 3). For example, Liu et al, used electrospun fibrous membranes loaded with basic fibroblast growth factor (bFGF) to prevent peritendinous adhesions in the AT. In this study, preformulated dextran glassy NPs were loaded with bFGF and then electrospun into a poly-L-lactic acid (PLLA) copolymer fiber as a mechanism to secure the bioactivity of bFGF in a sustained manner.
Following complete transection and repair of the AT, the electrospun bFGF/dextran glassy nanoparticles (DGNs)-PLLA fibrous membrane was wrapped around the repaired tendon. Histological and biomechanical assessments of the injured tendon revealed that the bFGF/DGNs-PLLA membrane was effective in minimizing adhesion formation and exhibited better tendon healing compared to control groups, thus establishing a promising, controlled-release mechanism to deliver therapeutics to the tendon. 43
Altogether, most attempts to improve tendon healing using NP delivery systems involve either injecting the drug directly into the tendon or incorporating the NPs within a scaffold (Table 3). Although these mechanisms are effective, they can result in high toxicity due to rapid clearance; hence, more effective tendon targeting strategies need to be developed to reduce these undesired occurrences. In the next section, perspectives will be offered on potential strategies to promote systemic targeting of the tendon.
Future Perspectives and Benefits of Tissue-Targeted Systemic Therapies
NPs are attractive drug delivery mechanisms due to their high tunability and sustained delivery properties. However, NPs have low tissue specificity, and must, therefore, be delivered in large amounts to ensure maximum drug utilization at target sites, which can lead to adverse side effects, including increased collateral damage to other tissues like the liver and brain.84,102 Alternatively, systemic delivery of drugs or drug-loaded polymers functionalized with tissue-specific targeting mechanisms (i.e., tissue-targeted systemic drug delivery) provides a noninvasive approach for localized therapeutic delivery.64,103 Moreover, tissue-targeted systemic drug delivery does not require intraoperative administration and facilitates the treatment of conditions that may not require surgical intervention, such as tendonitis and age-related tendon degeneration. Despite these advantages, there is a lack of tendon-targeting systemic drug delivery methods, which is primarily attributed to the lack of an identified targeting mechanism within the tendon to which the NPs can be directed. 104
Opportunities for targeting the tendon include exploiting stimuli in the healing milieu such as pH, redox potential, lysosomal enzymes, and glucose, or to external stimuli such as temperature, light impulses, magnetic field, or ultrasound, or to a combination of both internal and external stimuli (dual response/multiresponse NPs)

Stimuli-responsive NPs for controlled drug delivery.
Mechanisms to target the tendon during the inflammatory phase of tendon healing: Hypoxia
Following injury, the tendon immediately progresses through a short inflammatory phase, which lasts for a few days. 1 During this period, there is an increase in vascular permeability, correlated with an increase in expression of growth factors such as vascular endothelial growth factor (VEGF) and bFGF. 9 There is also an influx of inflammatory cells, including neutrophils, monocytes, and erythrocytes, which stimulate and regulate expression of inflammatory cytokines and growth factors including IL-6, IL1-β, IGF-1, TGF-β, and PDGF.1,9,141 The expression of these various cytokines and growth factors promotes chemotaxis and proliferation of macrophages and resident tendon fibroblasts.7,13,27
As in other tissues, hypoxia has been identified as an inducing factor of angiogenesis and an essential factor to obtain physiological healing during tendon injury.143–146 Various studies have shown that angiogenesis results from the activation of hypoxia-inducible factor, which modulates hypoxic effects and eventually leads to upregulation of several genes, including VEGF.143–147
Furthermore, hypoxia has been shown to promote the expression of various proinflammatory cytokines like IL–1β, IL-6, and IL-10.143,144 A study by Sivakumar et al also demonstrated the role of hypoxia in promoting and maintaining inflammatory responses in rheumatoid tendon disease by neovascularization.
145
These studies establish the presence and role of hypoxia in tendon disease and present a targeting opportunity for systemic delivery. Specifically, internal stimuli-responsive NPs that respond to hypoxia/redox can be employed to ensure self-controlled drug release because of the presence of glutathione (GSH) in the hypoxic environment. GSH is a reducing agent that can cleave redox-responsive bonds such as nitroimidazole, azo, and disulfide bonds on polymers
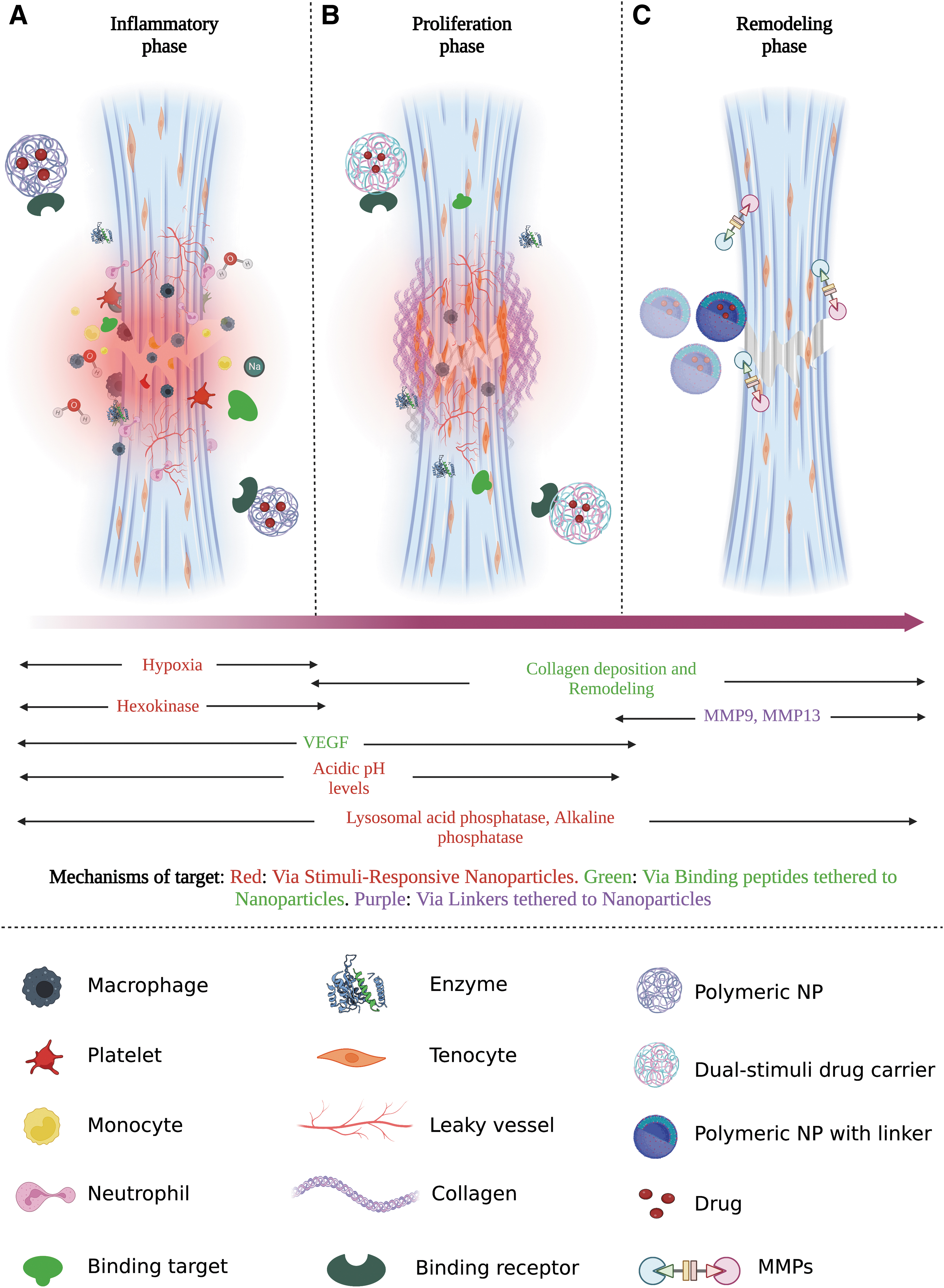
The tendon healing cascades associated enzymatic, biological, and physical changes, which can be leveraged for targeted drug delivery.
For example, Cheng et al developed redox-sensitive drug release poly(ethylene glycol)–poly(acrylic acid)–poly(N-isopropylacrylamide) (PEG-PAA-PNIPAAM) triblock copolymers through carbodiimide chemistry. Although the polymersomes were robust in physiological conditions, they rapidly dissociated upon uptake by MCF-7 breast cancer cells, resulting in the release of exogenous proteins due to redox-triggered de-cross-linking and disruption of the polymersome, thus enhancing drug accumulation at the tumor site, while reducing premature drug release. 149
In another study by Dai et al, highly packed interlayer-cross-linked micelle (HP-ICM) comprising a PEG corona and a disulfide-cross-linked interlayer was synthesized and loaded with doxorubicin. When the reducing agents, GSH or dithiothreitol, were added to the micelle solution, the HP-ICM micelles disassembled, indicating that the disulfide bonds had been broken, with the polymer chains completely dissolved as detected by dynamic light scattering and transmission electron microscopy. 115 In summary, current literature reports that the occurrence of hypoxia after tendon injury induces angiogenesis, promotes and maintains inflammatory responses, and modulates Hedgehog signaling, resulting in cell differentiation, proliferation, and vascularization.143–146,148,150,151
Furthermore, previous studies report increased levels of GSH due to hypoxia and oxidative stress within the tendon after injury.150,152,153 However, since these redox-responsive NPs have not yet been leveraged for use in the tendon, it cannot yet be determined whether the levels of GSH in the tendon are sufficient for localized drug delivery after systemic treatment or not. Hence, further studies are needed to investigate the peak GSH levels and durations in the tendon to ensure more effective therapies.
Mechanisms to target the proliferative phase of tendon healing: Collagen
During the proliferative phase of healing, there is an expansion of macrophages and recruitment of various Scx+/S100a4+ fibroblast populations, which start to proliferate and create a matrix primarily composed of collagen type 3.1,5,7,13,43 This process is mediated by the expression of a variety of growth factors involved in cell proliferation, collagen synthesis, ECM composition, and cell–matrix interactions. These growth factors include IGF-1, PDGF, TGF-β, bFGF, BMP-12, BMP-13, BMP-14, GDF-5, GDF-6, and GDF-7. 1
Depending on the organism, injury type, specific tendon, and treatment regimen, the proliferative stage can last a few days to weeks. 13 During this phase, the denatured collagen can be employed as a binding target to deliver drugs systemically. A collagen-binding domain peptide derived from Clostridium histolyticum can be used as a synthetic extension of a peptide-functionalized drug-loaded polymer. 154 This collagen-binding domain peptide specifically binds to the undertwisted triple-helical regions of collagen, with binding affinities in the micromolar range. It has been shown to preferentially bind bone and skin within 12 h of delivery and successfully localize drug payloads to sites of injury.154–156 Alternatively, a collagen mimetic peptide that specifically targets denaturing collagen can also be employed during this phase (Fig. 3b).86,157,159
Mechanisms to target the remodeling phase of tendon healing: MMPs
The final stage of tendon healing is the remodeling phase, which lasts from weeks to months and is characterized by the termination of cell proliferation and decreased vascularity. During this phase, there is high turnover of collagen and ongoing ECM remodeling. Furthermore, there is an increase in collagen type I synthesis, mediated by expression of various growth factors such as TGF-β, BMP-12, and BMP-14.1,52 During this phase, MMPs (e.g., MMP2, MMP9, MMP13) are secreted as inactive proteins and are activated when cleaved by extracellular proteinases, leading to upregulation of these MMPs.
Several MMPs are involved in collagen degradation,159–161 and this function can be leveraged for systemic drug delivery. Specifically, peptides for MMP2 (TLTYTWS/CTTHWGFTLC) and MMP9 (CRRHWGFEFC) have been identified through phage display. 161 Hence, binding peptides that have an affinity for these targets can be synthesized and conjugated to drug-loaded polymeric NPs for drug delivery. Alternatively, MMP cleavage can be used to cleave labile linkers between a drug and a carrier. These MMP-sensitive linkers can be introduced to polymeric drug carriers to ensure selective release at the injury site (Fig. 3c).
Mechanisms to target the tendon at all healing phases: Enzymatic changes and binding peptides
Drastic enzymatic changes occur during the inflammatory, proliferative, and remodeling phases of tendon healing, which can be leveraged to deliver enzyme-sensitive NPs. 162 During the first 12–72 h following tenotomy, glycolysis and release of citric acid cycle enzymes occur immediately throughout the tendon, with the most significant changes observed in the levels of lysosomal enzymes.52,163
Lysosomal acid phosphatase (LAP) enzymes are generally responsible for hydrolyzing organic phosphates at acidic pH,
164
and are expressed in monocyte/phagocyte lineage cells. Within 12 h of injury, LAP activity is significantly upregulated. However, peak activity does not typically occur until the beginning of the proliferative phase, followed by a decline during the remodeling phase of healing.
165
In addition, the expression and activity of several other enzymes change drastically during healing. They can therefore be employed for tendon-targeted systemic delivery, including alkaline phosphatase, glucose-6-phosphate dehydrogenase, and hexokinase (Fig. 3
Specifically, enzyme-responsive NPs can either be designed to have their exterior scaffold contain enzyme-sensitive materials that disintegrate when in contact with enzymes or can have the drug payload conjugated to the nanocarrier through electrostatic interactions or enzymatically biodegradable bonds (e.g., ester).62,64,82,83,103,166,167 Enzyme-responsive NPs have been used in various applications, including cancer therapy, 168 arthritis, 166 myocardial infarction, 169 diabetes, 170 and bacterial infections. 171 They may therefore be used as a reliable drug delivery system in tendon diseases.
To further fine-tune drug release and increase the therapeutic efficiency of drug-loaded NPs, sophisticated polymeric NPs that are responsive to more than one stimulus, such as pH/redox and enzyme/redox, and a combination of internal and external stimuli, such as temperature/enzyme and temperature/pH/redox, have been pursued. These dual stimuli and multistimuli responsive NPs offer extraordinary control over drug release and facilitate NP synthesis and drug loading under mild conditions in tissues such as the heart, lung, bone, muscle, and brain.20,102,105,108–116,118,119,121,122,133,137,140,150,172–175 Alternatively, high-affinity peptides and aptamers can be designed to specifically bind target proteins, molecules, or cells in the tendon. Through phage display, studies have identified peptides that bind to tartrate-resistant acid phosphatase, 176 LAP, 177 collagen, 154 and VEGF. 161 These binding peptides can be incorporated onto drug-loaded NPs and delivered systemically to the tendon.
Translational potential of systemically delivered tendon-targeted NPs
Recent advances in surgical repair techniques and suture material have improved healing outcomes of tendon injuries.178–181 However, successful tendon repair remains challenging due to the high potential for gap formation, repair failure, and adhesion formation. Moreover, adhesion formation, particularly in the flexor tendon, often necessitates tenolysis, or scar removal surgery, in an attempt to restore function.5,10,11,28,180,181 Hence, the primary goal of these procedures is to provide sufficient tension between the two tendon ends, minimize bulkiness, and provide as much range of motion as possible during and after the procedure.28,178,180 To successfully achieve all these outcomes, sutures can be coated with nanomaterials encapsulating drug payloads, especially for use in areas like Zone 2 of the flexor tendons, which are relatively anatomically constrained.
Currently, core sutures used for Zone 2 repairs range between 0.7 and 1 cm in length at minimum.178,180 Thus, NP-coated sutures can therefore be used to deliver a moderate amount of growth factors, 182 gene therapy, 41 and small molecules like mitomycin-C, 79 a chemotherapy agent with the ability to reduce postoperative scarring, 79 in a sustained delivery manner to strengthen the tendon ends and minimize adhesion formation, while minimizing bulk at the repair site. Furthermore, composite scaffold implants containing drug-loaded NPs can be applied in load-bearing tendons such as the AT after suture repair to provide mechanical strength, while promoting regenerative tendon healing.
Chronic pathological changes to the tendon can result from overuse and/or age-related tendon degeneration, and subsequently alter the mechanical and material properties of the tendon, negatively impact quality of life, and increase the potential for acute tendon rupture. Since these chronic pathologies do not require surgical intervention, it is impractical to use scaffold implants that require invasive procedures.
Furthermore, direct injection of NSAIDs such as Ibuprofen, corticosteroids, or other biologics (e.g., platelet-rich plasma) has not improved functional or material outcomes in clinical studies of rotator cuff pathology and tendinopathies.16,25,183–186 Furthermore, these injections can have deleterious effects on the tendon (e.g., decreased mechanical and material properties), increase the risk of infection and inflammation, increase the chances of needing a revision surgery, and require multiple treatments.25,184–186 Alternatively, nanotechnology can be used systemically to safely deliver biologics intravenously to facilitate controlled release and increased circulation time of drug payloads, which can subsequently improve material quality and functional outcomes of the tendon without the risks associated with classic treatment approaches.
Although tendon healing using nanotechnology has not yet reached clinical trial stages, investigations using NP-mediated drug delivery approaches to promote healing of acute tendon injuries,29,41,86,90,94,100,182 tendonitis,29,90,93,98 and bone-to-tendon injuries47,66,71,74–76,78 are emerging.
Conclusions
Despite the severity and frequency of complications associated with tendon injuries, there is no pharmacological approach to promote tendon regeneration. Although current approaches have focused on using scaffolds as carriers to deliver growth factors and therapeutics, these approaches can only be applied intraoperatively before knowing how healing will progress, thus limiting the potential for individualized care. Moreover, several complications associated with intraoperative procedures can arise, including exacerbation of tissue fibrosis. Hence, there is a need to develop personalized and customizable approaches that promote high specificity targeting of the healing tendon. NPs offer precise control over drug loading and release kinetics and are therefore an attractive translational platform that can deliver therapeutics without invasive procedures.
Moreover, advances in nanotechnology for tendon regeneration can be combined with stimuli-responsive polymers tailored for individual tendon injuries and the stage of healing that needs to be modulated. In this review, we have discussed various targeting opportunities that can be leveraged at different phases of recovery, based on the unique microenvironment that characterizes the tendon-healing cascade. By optimizing the targeting specificity of NP delivery systems, the outcomes of precision medicine therapeutics can be enhanced to improve patient outcomes, thereby reducing complications associated with tendon injuries, including disability, risk of reinjury, and increased socioeconomic burden.
Footnotes
Authors' Contributions
Conceptualization (A.E.L. and E.A.-S.), writing (E.A.-S.), and editing (A.E.L., E.A.-S., and D.S.W.B.). All authors have read and approved the final version of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, by NIH/NIAMS R21 AR081063 (A.E.L. and D.S.W.B.), and The University of Rochester Clinical and Translational Science Institute Trainee Pilot Award UL1TR002001 from the NIH (E.A.-S.).