
Abstract
With the recent developments in tissue engineering, scientists have attempted to establish seed cells from different sources, create cell sheets through various technologies, implant them on scaffolds with various spatial structures, or load scaffolds with cytokines. These research results are very optimistic, bringing hope to the treatment of patients with uterine infertility. In this article, we reviewed articles related to the treatment of uterine infertility from the aspects of experimental treatment strategy, seed cells, scaffold application, and repair criteria so as to provide a basis for future research.
Impact statement
Tissue engineering is a new emerging and viable therapeutic method to be contained within repairation of organ injury strategies. So far, there is no review article summarizing and organizing the treatment strategies, application effects, and current research progress of tissue engineering in the treatment of damaged uterine tissue. Therefore, this article focuses on the application of tissue engineering materials, seed cells, and active factors in the repair of uterine injury, aiming to provide theoretical reference for the development of new strategies for treating infertility caused by uterine injury.
Introduction
The uterus is an essential reproductive organ for women, as it undergoes cyclic changes—producing menses monthly—and provides an acceptable location for embryonic implantation and fetal development. Absolute uterine factor infertility refers to the absence of a functional uterus due to both congenital (e.g., uterine dysplasia, uterine malformations) and acquired conditions (e.g., caused by hysterectomy, benign conditions, including leiomyoma and adenomyosis, postpartum hemorrhage, uterine adhesions). Despite considerable progress in reproductive medicine, infertility due to uterine factors continues to exist. Uterine transplantation (UTx) or surrogacy is one of the ways to resolve this problem—but ethical, social, legal, technical, security, and tissue rejection issues remain great challenges.1,2 Treating uterine infertility with novel modalities is therefore a significant task to be undertaken by medical scientists.
In recent years, the continual development of material science and tissue engineering provides the technical means for uterine tissue regeneration. The main goal of tissue engineering is to use life science and engineering methods to manufacture biological substitutes that can maintain, improve, or rebuild the structure and function of entire organs or tissues. 3 Tissue engineering has been accepted for generating tissue in vitro for clinical applications, such as displacing injured tissues or damaged organs.
The application of tissue scaffolding—with the development of material science—enables the generation of complex multichamber tissues and tissue structures, is convenient to use, avoids opening a second surgical area, possesses unlimited sources and good biocompatibility, and achieves desirable tissue repair by promoting the regeneration of body tissue. This technology therefore provides a promising solution in regenerating and reconstructing bioartificial uterine tissue for uterine infertility therapy. The three components of tissue engineering, namely scaffolds, seed cells, and signaling factors, could be used individually or in combination through the experimental research methods used in life sciences and engineering to better exert their biological effects. 4
It is well known that scaffolds are functional structures made of natural or synthetic materials, simulating the space and microenvironment where extracellular matrix (ECM) production and degradation, cell proliferation, cell response, and signaling factors play biological functions. By engineering them, scaffolds can be used to provide a microenvironment for cellular growth in vivo and in vitro. Using life science research methods, investigators have uncovered specific cells that can be cultured into target tissues or organs in vitro and in vivo. Then, by detecting the alterations to moleculars of newly regenerated tissue, scientists can verify whether the scaffolds could support and guidance cells proliferation well.
This review article provides a detailed overview of the information at the current level of technology with respect to cells and active factors, and tissue engineering scaffolds and applications of these scaffolds in uterine tissue regeneration. We herein analyze various aspects that involve different cell sheets, scaffolding species, composition, structure, effects on cellular engineering strategies, and scaffolds (Fig. 1). In addition, we discuss the advantages and disadvantages or limitations of disparate bioen ECM, and support and stimulate proliferation and organization. Finally, our review concludes with the challenges remaining in the application of scaffolds to uterine tissue regeneration engineering, and future perspectives regarding improving the properties and applications of these scaffolds.
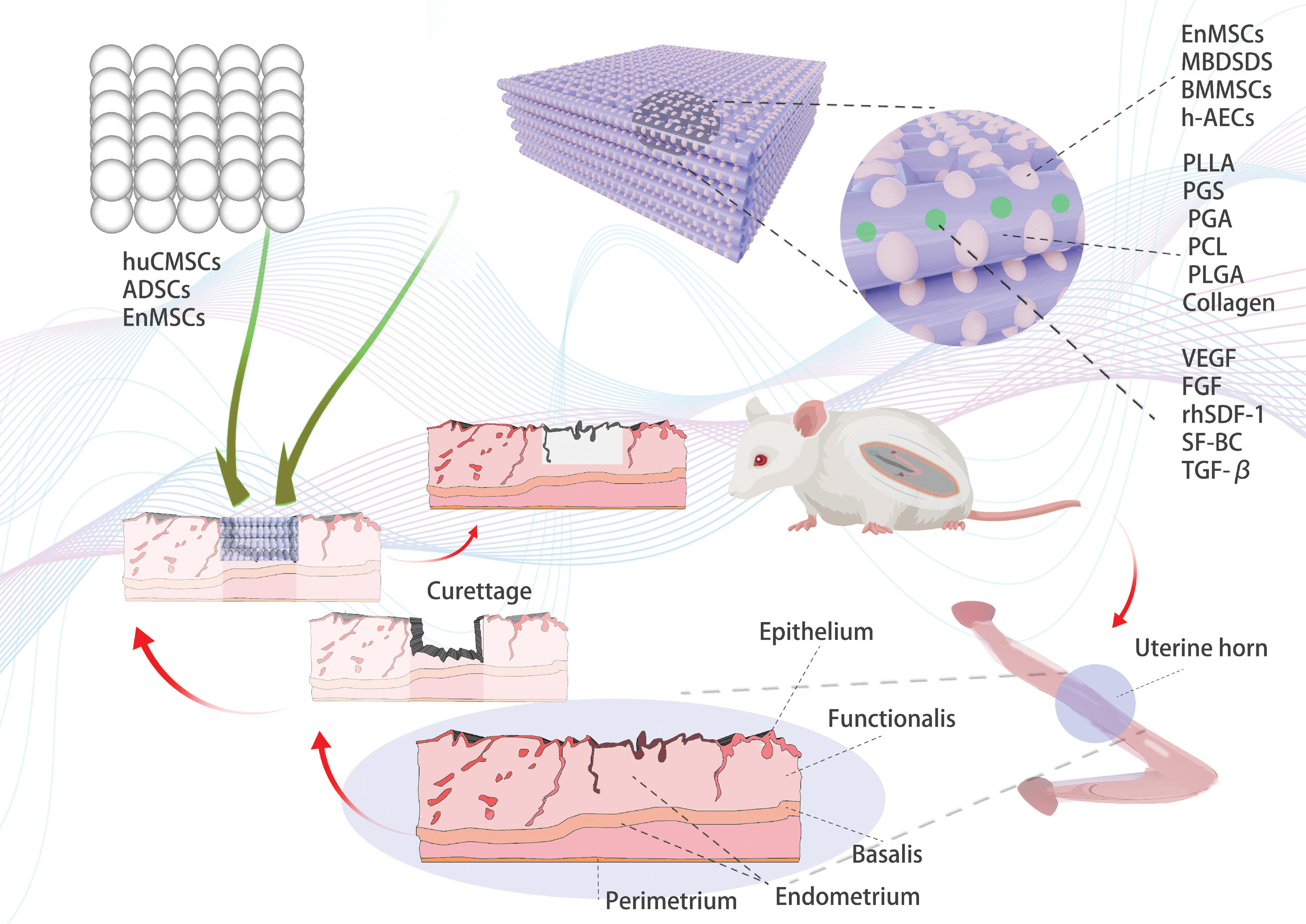
Uterine tissue engineering strategies: biomaterial scaffold, seed cells, and active factors. Color images are available online.
Strategies for Uterine Regeneration
Cell sheet engineering
Cell sheet engineering (CSE), an innovative technology that implants cell sheets obtained using cell sheet fabrication techniques into the injury site, thereby promoting the regenerative repair of injured tissues, has exhibited great potential in the field of tissue regeneration (Table 1). The CSE technique refers to growing cells as dense sheets of cells on a Petri dish capable of thermal response, which is isolated when the temperature is lowered by adjusting the temperature (Fig. 2). Cell sheet technology was invented in 1993 by Yang J, 5 and the advantage of cell sheets is that ECM proteins and a large number of cytoactive factors are retained. 6
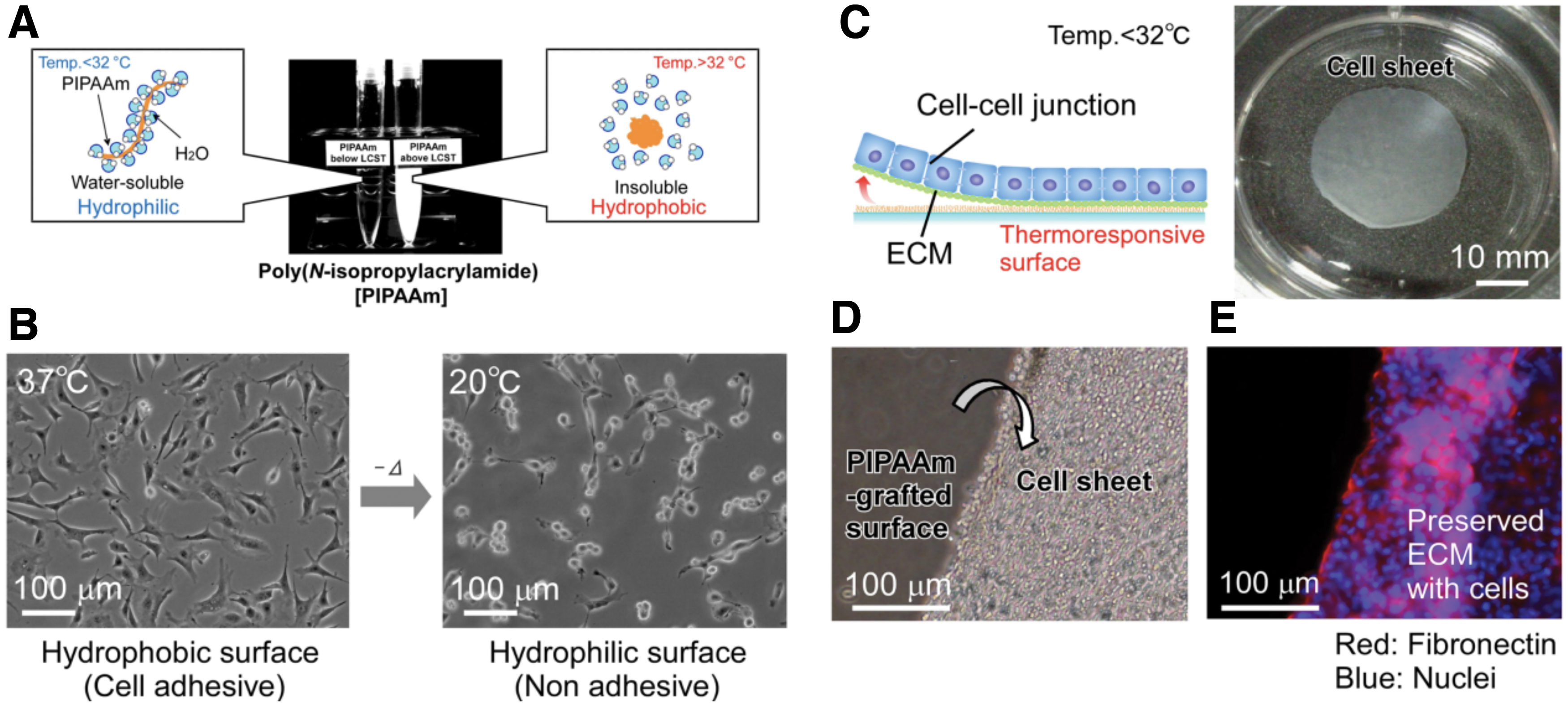
Fabrication process of cell sheets by thermoresponsive technique.
The Application of Cell Sheet Engineering in Uterine Tissue Regeneration
ADSC, adipose tissue-derived stem cell; EnMSC, endometrial mesenchymal stem/stromal cells; hUCMSC, human umbilical cord mesenchymal stem cell.
To date, three types of cells have been made into cell sheets for the repair of adhesions in the uterine cavity: human umbilical cord mesenchymal stem cells (hUCMSCs), 7 endometrial mesenchymal stem/stromal cells (EnMSCs), and adipose tissue-derived stem cells (ADSCs). A hUCMSC sheets by culturing hUCMSCs on thermoresponsive cell culture plates, and when transplant hUCMSC sheet into uterine injury site, it can significantly come out with smaller fibrotic-to-normal myometrial ratios, and the mean number of fibroblasts–demonstrating that stem cell sheets transplanted to hysterotomy sites promoted myometrial regeneration and reduced fibrotic tissue formation. 7 And primary endometrial cell sheet transplantation restored regeneration of endometrial tissue with histological structure and physiological function that support pregnancy in a manner similar to that with normal endometrial tissue. 5
It has been demonstrated that the migration rate of EnMSCs in the intrauterine adhesions (IUA) women was significantly lower than that in normal healthy women without IUA. Wound healing and transwell chamber assays were used to assess the migratory and invasive capabilities of the EnMSCs in IUA patients and normal healthy women, revealing that these capabilities were attenuated in IUA patients, and that tube formation and immunosuppressive abilities of the EnMSCs were lower in the IUA patients. 8 These differences provide a basis for the treatment of endometrial adhesions with EnMSCs cells.
Although thermoresponsive technology is more applicable, using it to fabricate cell sheets is rather time consuming due to the technical complexity, 8 and the fabrication consumables used in the fabrication process are also expensive.9,10 Therefore, researchers have endeavored to explore new ways to simplify the cell sheet fabrication process and reduce the fabrication cost. The investigators found that cell sheets were obtained during cell culture by adding a specific amount of ascorbic acid instead of the thermoresponsive technique.9–12
The addition of ascorbate during cell culture has the effect of stimulating ECM production, at the same time, it can promote cellular DNA synthesis and thus promote rapid cell proliferation.13–15 In addition, ascorbate supplementation was also found to help maintain stem cell properties when making stem cell sheets. 16 ADSCs treated with the addition of ascorbate are more proliferative. 17 ADSCs maintain self-renewal by proliferation on the one hand and differentiation into adult stem cells with multiple differentiation potentials on the other hand.18–20 Otherwise, ADSCs have immunosuppressive properties and low immunogenicity, secrete bioactive factors during proliferation, and are currently the most seemingly ideal cell type in regenerative medicine.21,22
Therefore, researchers have successfully constructed ADSC sheets by adding ascorbic acid and evaluated the effect of cell sheets to promote regeneration, and found that the regeneration promoting effect was significant. 23 Instead of using thermoresponsive techniques, ascorbic acid was added to form cell sheets during ADSC culture, the formed cell sheets transplanted into the injured uterine site can promote the repair of injured myometrium, and the repaired uterine tissue is lined with columnar epithelium, with the myofibers arranged more closely to the normal myofiber arrangement. 9 This demonstrates that ADSCs can be one of the cell types used to treat uterine infertility and that the addition of ascorbic acid to create the cell sheets can be an alternative to replace touch fever technology in the process of making cell sheets (Fig. 3).
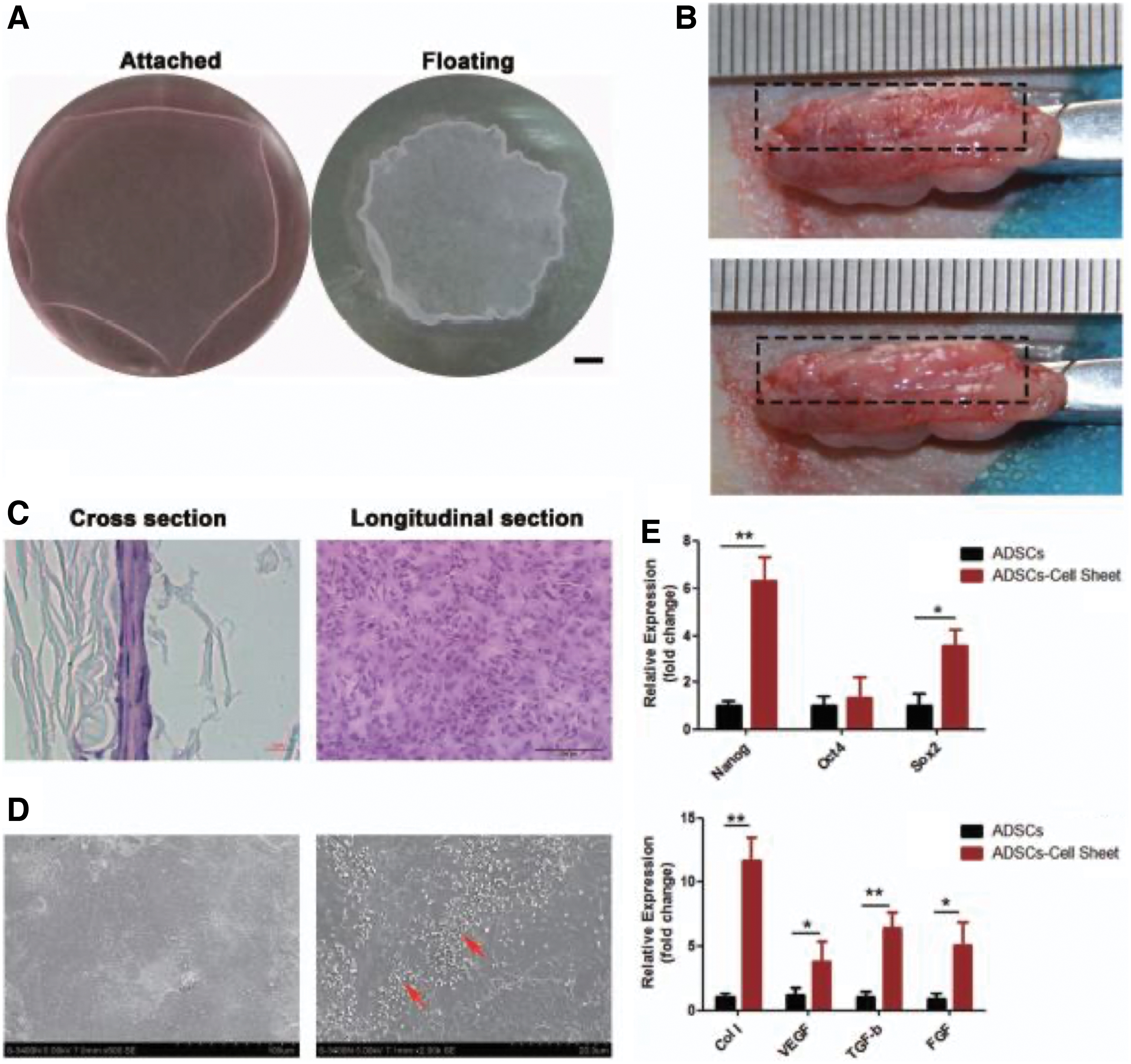
Configuration of a 3D ADSCs sheet.
Scaffolds
Commonly used scaffolding materials for tissue engineering primarily include two major categories, natural and artificial. Natural scaffold materials include ECM proteins, polysaccharides, and silk fibroin-like materials such as collagen, gelatin, hyaluronic acid, and adhesins—among others. There are many sources of collagen, and these are widely distributed in the connective tissues of humans and animals. Gelatin is a degradation product of collagen, which after proper cross-linking improves its physicochemical characteristics; and the use of gelatin in the field of uterine tissue regeneration engineering has been studied extensively.24–29 Hyaluronic acid belongs to the polysaccharide class of substances that shows favorable biocompatibility as a neural tissue scaffold material, and can be degraded into nontoxic products. 30
The synthetic scaffolds include silica gel, poly(levo-poly
The Application of Scaffolds in Uterine Tissue Regeneration
b-FGF, basic-fibroblast growth factor; BDMSC, bone marrow-derived mesenchymal stem cell; ES, embryonic stem cells; MSC, mesenchymal stem cell; PGA, poly(glycolic acid); PGS, poly(glycerol sebacate); PLGA, poly (lactic co glycolic acid); rhSDF-1α, recombinant human stromal cell-derived factor-1α; SF-BC, silk fibroin-bacterial cellulose; SIS, small intestine submucosa; VEGF, vascular endothelial growth factor.
Decellularized scaffold is a perfect ECM material, which has been extensively concerned in tissue engineering and regeneration medical science in recent years.35,36 At present, decellularized scaffolds used for uterine tissue regeneration and repair come from tissues and organs, such as uterus37–39 and small intestinal submucosa. 40 Using physical and chemical methods to remove the original cells in tissues and organs to obtain ECM scaffolds without primitive cells, which showed excellent ability in providing favorable microenvironment, retained the physical scaffolds and biochemical signals from primitive tissues/organs, and was more conducive to the adhesion, growth, and proliferation of transplanted cells.
In in vitro experiments, endometrial cells and uterine smooth muscle cells were co-cultured with the acellular scaffold by cell covering and injection technology. Hematoxylin–eosin staining and immunofluorescence staining of vimentin, cytokeratin, a-smooth muscle actin, and CD31 confirmed the recellularization. In vivo animal experiments have confirmed that porcine small intestine submucosa-loaded UCMSCs are beneficial to uterine tissue regeneration and repair. 40
Another improvement is to obtain the cell matrix skeleton after the uterus is completely decelled, grind it into powder, remake ECM gel membrane, and inject mesenchymal stem cells (MSCs) (Fig. 4). And when implant ECM membrane with MSCs grow well into the damaged uterus and uterine cavity, effectively stopping uterine adhesions, and promoting endometrial regeneration and muscle collagen reconstruction. By establishing physical barriers and secreting cytokines, wound healing is accelerated, achieving effective recovery of the uterus. The damaged uterus is almost completely recovered (Fig. 5). It is similar to the normal function of the undamaged uterus. It can be used for normal pregnancy and support fetal development and live birth. 38 In general, decellularized scaffold is a promising application material for uterine tissue engineering and regenerative medicine, which deserves more in-depth research.
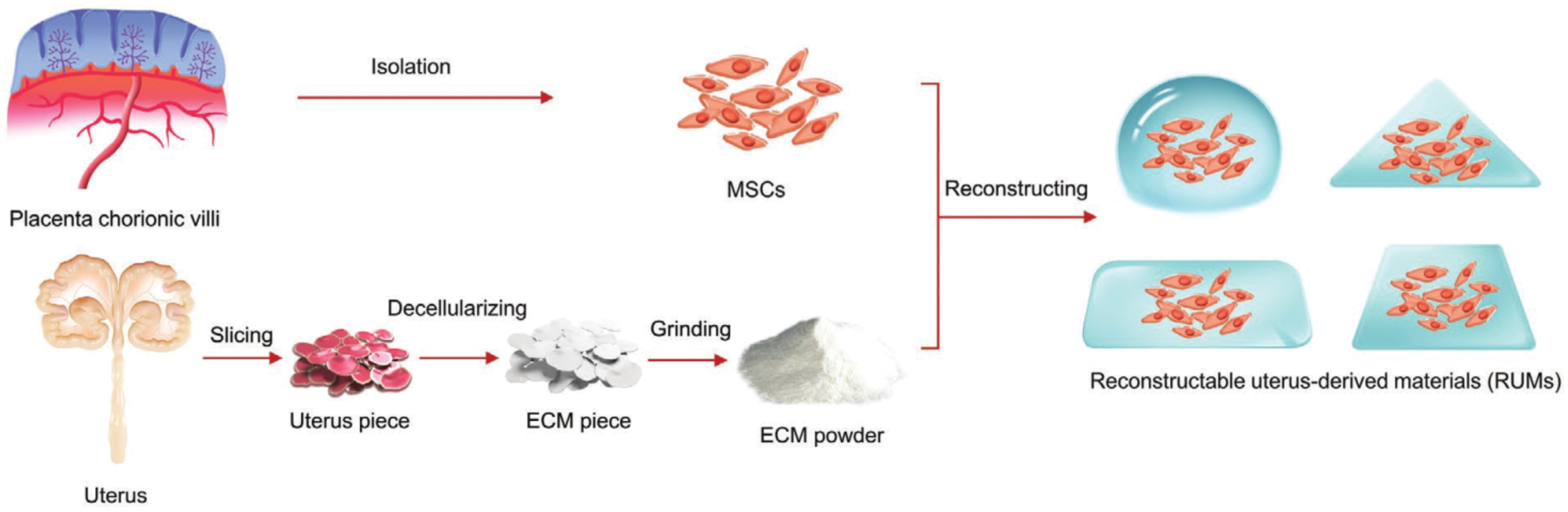
Construction of RUMs for uterus recovery. MSCs were isolated from human placental chorionic villi, which were subsequently seeded into ECM, allowing the formation of RUMs. 38 MSC, mesenchymal stem cell; RUMs, reconstructable uterus-derived materials. Color images are available online.
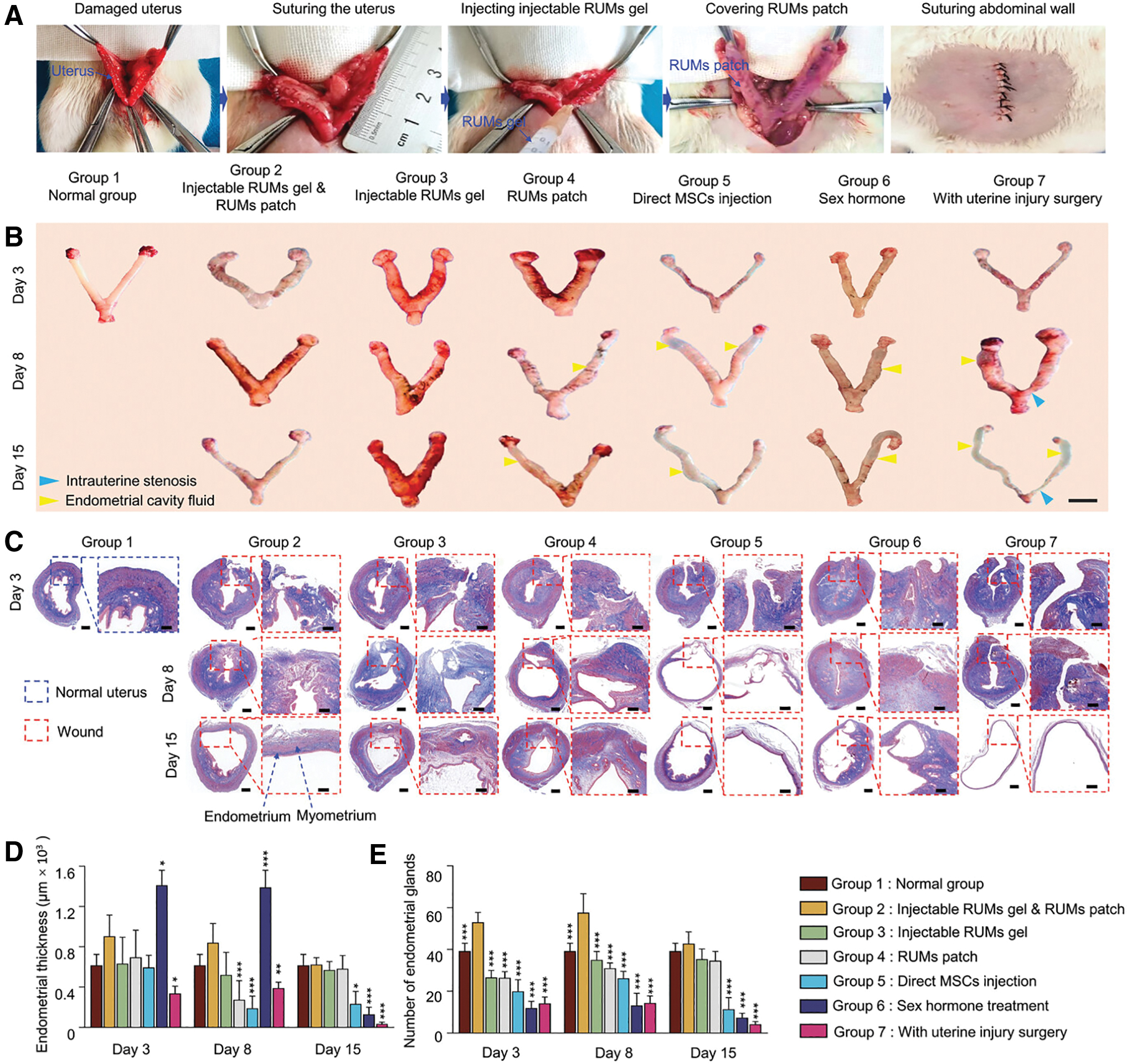
The treatment assessment of rats with severe uterine injury at different interventions.
The key elements of tissue engineering are materials; collagen is the earliest natural material used by researchers to perform tissue engineering studies, and fabrication of collagen into scaffolds with porous spatial structures could provide ideal space support and chemical microenvironment for transplanted stem cells as well as other seeded cells to adhere and grow. Constructs composed of biomaterials loaded with active seeded cells have also recently been tried for application in the treatment of uterine tissue damage. It was confirmed in an in vitro study that hUCMSCs could promote endometrial regeneration, and collagen scaffold (CS)/hUCMSCs facilitated endometrial stromal cell (ESC) hyperplasia and inhibited cell apoptosis through a paracrine mechanism effect.
The implanted CS/hUCMSCs could maintain the regular spatial structure of the uterine lumen and promote endometrial regeneration and regenerative tissue remodeling. And the new growing endometrial cells were able to express estrogen receptor (ER)-α and progesterone receptor (PR), which allow zygote implantation and support embryonic development. 28 These results were similar to those of the proliferation-promoting effect of CS-loaded bone marrow-derived mesenchymal stem cells (BDMSCs).25,41 Collectively, a strategy using CS/hUCMSCs 29 or CS/BDMSCs could encourage the reestablishment of endometrial structure and support pregnancy ability.
PGA and PLGA biomaterials have unique physical and chemical properties and are used in the field of tissue engineering. These excellent properties include high porosity and good pore interconnection, providing larger area per unit volume, good physical and chemical properties, and high biocompatibility. 13 Biofilm scaffolds composed of PGA and PLGA have been used for repairing urethral injuries in human patients, 41 and the combination of PGA and collagen has also achieved satisfactory results in bladder engineering. 42 The polymer scaffold composed of PLGA and PGA was seeded with cells from primary uterine tissue to form a complex and was implanted into the uterine cavity; the engineered uterine tissue formed a regular uterine cavity, forming an anatomical structure similar to normal uterine tissue for the regenerated endometrium and myometrium, and supporting the implantation of zygote and embryonic development. 43
PGS, a biodegradable biomaterial developed in recent years, which has biocompatibility and good compliance, has been used as a scaffold material or carrier for seed cells to achieve good results in regeneration of tissues other than uterine tissue.42–45 Therefore, researchers believe that using PGS as a carrier to transport seed cells into the uterine cavity for the treatment of damaged endometrium is expected to achieve good results. The advantage of PGS is that compared to collagen or PLGA, the mechanical characteristics of PGS scaffolds are closer to the mechanical characteristics of the uterus, indicating that PGS scaffolds better match the mechanical characteristics of the uterus than collagen or PLGA. 46
The good compliance of PGS stent can maintain the dynamic environment of mechanical changes in the process of uterine tissue regeneration. Because PGS has good histocompatibility, it will not produce mechanical stimulation to surrounding tissues. In contrast, PLGA and collagen have poor elastic strain compliance and cannot recover from deformation, thus providing less space for dynamic mechanical changes required for uterine tissue regeneration. When researchers created PGS/BMMSC, PLGA/BMMSC, and collagen/BMMSC constructs to compare the effectiveness of PGS, PLGA, and collagen biofilms or scaffolds in preventing IUA during the treatment of injured uterus, they found that PGS scaffolds exhibited mechanical characteristics similar to natural uterine tissue and could provide good adhesion and growth of BDMSCs. Compared with PGS, PLGA and CS have been proven to have characteristics similar to plastic, such as hardness and poor compliance.
Second, in vivo bioluminescence imaging showed that compared with direct intrauterine injections of BDMSCs, PLGA, and CS, the PGS scaffolds notably extended the survival time of BMMSCs at the injury site. BMMSCs in scaffolds implanted with PGS/BMMSCs migrated to the mucosal basal layer of the endometrium, and pathological examination confirmed more active local endometrial stromal cell proliferation compared with PLGA/BMMSCs or collagen/BMMSCs. What is more important, only the BMMSCs transplanted using the PGS/BMMSC construct could directly differentiate into endometrial stromal cells, whereas those transplanted using the PLGA/BMMSC construct or the collagen/BMMSC construct could not.
This illustrates that PGS is more suitable for guiding BM cells toward uterine tissue differentiation. The transplantation of PGS/BMMSCs can also better restore the spatial and tissue structure of the damaged uterus than PLGA/BMMSC or collagen/BMMSC transplantation. PGS/BMMSCs are equivalent to collagen/BMMSCs in promoting fertility recovery. Although PLGA/BMMSC transplantation can also promote fertility recovery, the effect is not as good as PGS/BMMSC and collagen/BMMSC transplantation.
In some studies, only transplanting PGS without loading any seed cells can significantly improve the pregnancy rate after uterine injury (Fig. 6). After implantation of PGS biofilm scaffold, pregnancy function only partially recovered. This can be achieved through manufacturing technology by adjusting the spatial structure and pore size of PGS scaffold to optimize its mechanical performance, which is expected to better promote the repair of damaged uterine tissue structure and functional recovery. 32 In conclusion, after various biological performance evaluations, PGS stent has clear composition, mature manufacturing process, and wide application in the field of regenerative medicine. The use of PGS/BMMSC is a promising method for clinical treatment of uterine infertility. 32
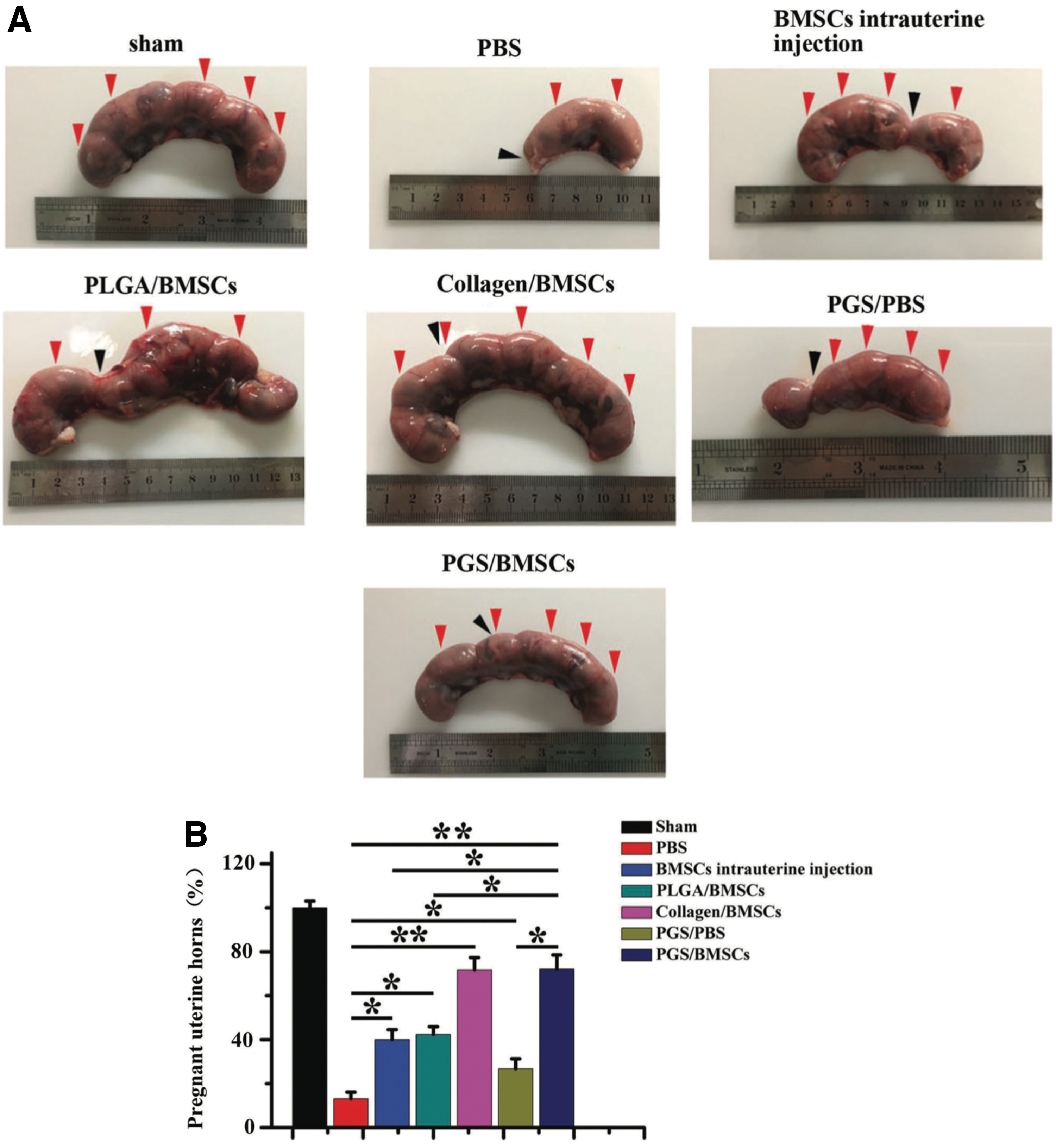
Pregnancy function test.
The CS structure of multiaperture space could provide good physical support for the attachment and hyperplasia of hUCMSCs.28,32 The scaffold surface with a porous spatial structure is more beneficial to the diffusion of oxygen and nutrients, thereby accelerating cell adhesion and hyperplasia. The biomechanical properties of scaffold materials can also exert a modulatory effect on the differentiation of stem cells, making it possible to manage the cells. Steinberg 47 studied the promotion of epithelial tissue formation by microstructural and mechanical properties of scaffold materials by culturing epithelial cells on various nanogelatin, nonwoven fibrous elastomers. Although the aforementioned studies provided favorable pregnancy outcomes, cellular survival upon implantation was still limited. 48 In addition, manufacturing methods previously used in tissue engineering faced difficulties in reconstructing organ ultra microstructure and enlarging for feasible use in total uterine regeneration.
Nevertheless, in pace with 3D bioprinting, a more advanced biological manufacturing technology, these problems have gradually been solved. Three-dimensional bioprinting technology49,50 has made significant progress and can now create various organizational structures. By optimizing the bore diameter porosity, and mechanical properties of the scaffold, it is expected to achieve more ideal results. From microscale CSE and cell-seed biological scaffolds to nanoscale extracellular vesicles and transfer of bioactive molecules, biomimetic endometrial interfaces not only emulate a physiological multilayer structure but also restore the proper nutritional microenvironment by increasing vascularization and reducing immune response. 34
Scaffold loading with seed cells
Tissue engineering scaffolds could provide an architectural microenvironment that is similar to the original 3D tissue. However, in vivo and in vitro experiments have confirmed that the combination of scaffolds and functional cells can better exert the biological effects of scaffold materials (Tables 2 and 3).
The Application of Bioactive Cells in Uterine Tissue Regeneration
h-AEC, human amniotic epithelial cell.
Functional cells would produce the growth factors necessary to produce the microenvironment provided by engineered scaffolds analogous to that required for cellular regeneration of target organs and tissues. MSCs are able to differentiate into different types of histiocyte, and have the characteristics of rapid proliferation and immune regulation ability, 51 and are considered to be the ideal seed cell type to promote tissue regeneration and repair. There are several reasons for scientists to use human MSCs (hMSCs) for recellularization. First, because of their self-renewal capacity, multilineage tissue differentiation potential, and easy acquisition, hMSCs are often used as seed cells in attempts to apply them in regenerative medicine.52–55 Studies have found that stem cells characteristic of hMSCs exist in endometrial stromal and epithelial cells. 56 Second, hMSCs, on the one hand, have low immunogenicity and, on the other hand, could play an immunomodulatory role during tissue injury repair.47,57–59
Researchers have also demonstrated that hMSCs with CS constructs are able to promote repair of injured uterine tissue. 29 These stem cells with multiple differentiation potentials move to the site of injury to play a significant role in the process of tissue healing and remodeling of tissue architecture by releasing active factors and producing ECM proteins. 60 Therefore, the use of several stem cell types has been considered, including embryonic stem cells (ES),61,62 BMMSCs,25,32,63 hUCMSCs,29,64–66 EnMSCs,66,67 and menstrual blood-derived stem cells (MBDSCs),68–70 and BMMSCs have been approved for clinical use. These are currently widely applied to the field of uterine regenerative medicine research.
Human amniotic epithelial cells (h-AECs) are also good candidates for tissue regeneration.71–74 Due to the proven ability to promote endometrial regeneration through MSC transplantation, h-AECs have been shown to possess stem cell characteristics and therefore have the potential to serve as seed cells for tissue engineering, 75 and both direct uterine injection of h-AEC or tail vein injection of h-AEC could promote endometrial thickening, stimulate glandular and vascular regeneration of the endometrium, decrease endometrial fibrosis, and ultimately produce new functional endometrium at the damaged site, thereby improving the recovery of pregnancy function in IUA model rats. 74
EnMSCs with the characteristics of MSCs were characterized on EnMSCs harvested from the endometrium of women. Endometrial tissue is periodically remodeled and therefore easily accessible, and the development of minimally invasive gynecological surgery in recent years has made endometrial tissue sampling more convenient. The female endometrium brings a new way to get stem cells for regenerative medicine. 76 Menstrual blood-derived stem cells (MBDSCs) have characteristics and biological differentiation potential similar to that of EnMSCs.77–81 There are several reasons for using hMSCs for recellularization. First of all, the endometrium contains MBDSCs and EnMSCs with endometrial menstrual blood origin, and EnMSCs have similar property potentials to BDMSCs82–84 and dental pulp MSCs. 85 Studies on the regenerative potential of MBDSCs and EnMSCs demonstrated that MBDSCs and EnMSCs have multiple differentiation potentials and can differentiate into endoderm, mesoderm, and ectoderm tissues.26,86–91
Second, MBDSCs and EnMSCs could be isolated either by collecting menstrual blood or from endometrium obtained by diagnostic curettage, neither causing great trauma to the organism nor involving ethical issues. 92 Last but not least, both MBDSCs and EnMSCs are characterized as MSCs with higher proliferative activity and speed comapred with BDMSCs and dental pulp stem cells 93 or umbilical cord stem cells,81,94 and even after 20 months of continuous culture, MBDSCs and EnMSCs still maintain strong proliferative activity and colony-forming ability, 95 and could retain their normal karyotype and angiogenic ability after 34 consecutive passages. 96 Even EnMSCs harvested in the postmenopausal endometrium retain their stem cell properties. 97 However, these two cellular sources are only employed in animal experiments, and thus, these sources remain an issue for clinical patients.
In addition, there are also some investigators who do not advocate the application of endometrial origin stem cells as seed cells for regenerative medicine, as their findings suggest that BDMSCs better promote tissue regeneration repair compared to endometrium-derived stem cells.12,13 The technology of stem cell acquisition has also recently undergone a developmental breakthrough. In early studies on uterine tissue engineering for the treatment of uterine infertility, the convenience of cell acquisition was not the primary issue in whether the research would be successful, but rather the issues relate to the exploration of the molecular mechanism(s) underlying uterine tissue regeneration and the need to find seed cells.
Scaffold loading with active cytokines
As mentioned previously, collagen is currently the most commonly used scaffold materials for natural tissue engineering due to its unique characteristics.98,99 Scientists have developed a chemotactic composite scaffold by incorporating recombinant human stromal cell-derived factor-1α (rhSDF-1α) into a silk fibroin-bacterial cellulose (SF-BC) membrane carrier. 96 SF-BC scaffolds loaded with rhSDF-1α significantly encouraged endometrial regeneration and angiogenic capacities of the injured uterus and improved pregnancy outcomes, thus demonstrating that this strategy can contribute to functional uterine repair and impaired endometrial regeneration. It was suggested that SF-BC membrane carries the necessary good physicochemical properties and biocompatibility for bioactive materials. 96
The structural collagen-binding domain (CBD) can bind to the N-terminus of basic fibroblast growth factor (b-FGF) molecules, so CS materials are suitable materials for producing targeted delivery systems that target b-FGF to injury sites. After transplanting the CS/b-FGF construct to the injured site, b-FGF produces a marked effect in encouraging cell multiplication and neovascularization at the injured site. As the CS is completely degraded and absorbed by the body, the implanted site is gradually replaced by regenerated endometrial tissue and uterine smooth muscle tissue (Fig. 7). The implantation of collagen/CBD b-FGF complex in the uterus supports normal implantation development of embryos, just like normal and undamaged uterine tissue (Fig. 8). Therefore, CS loaded with vascular endothelial growth factor (VEGF) could promote the repair of damaged uterine tissue structure and the recovery of pregnancy function. 27
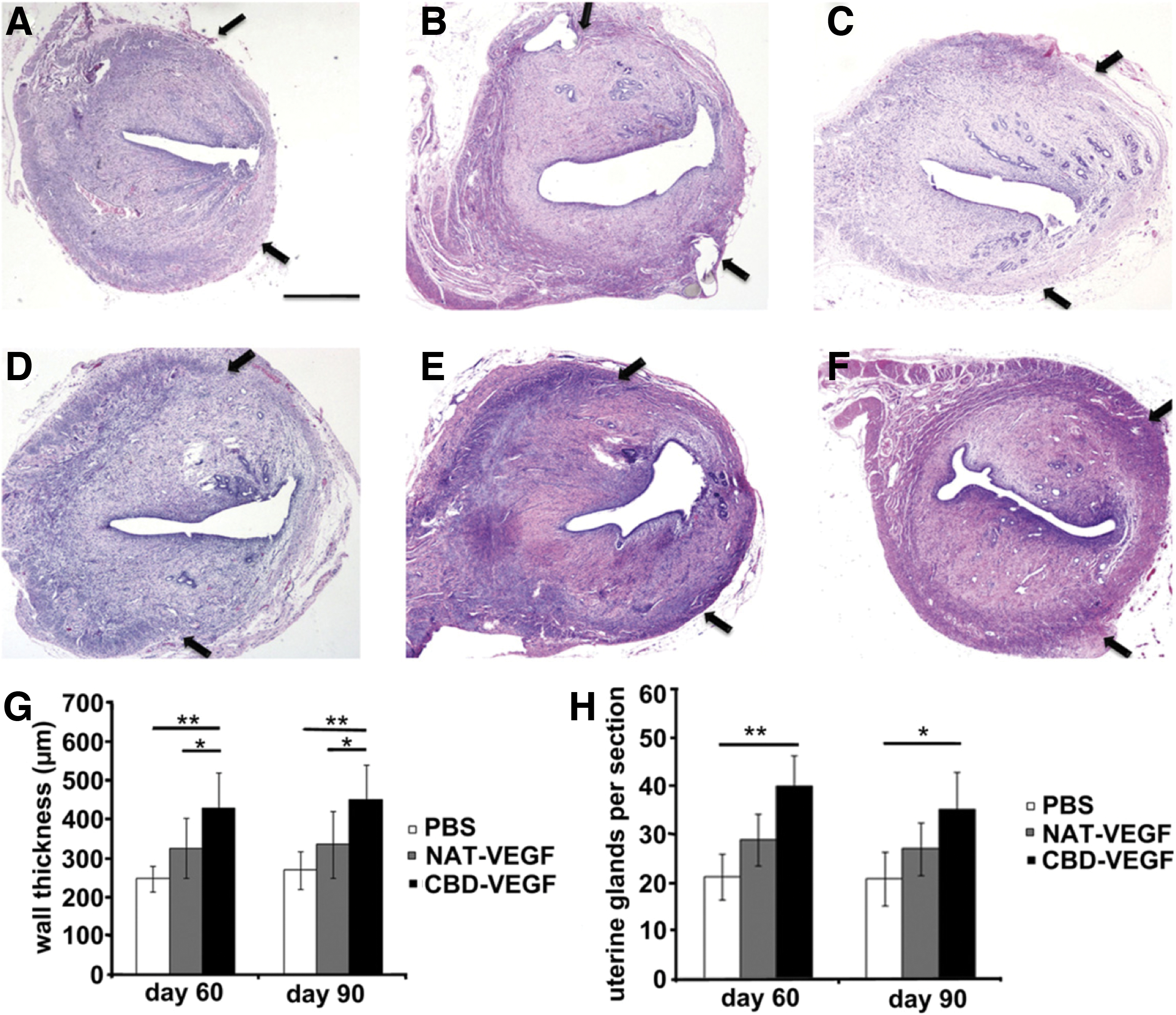
Histological changes by H&E staining in the cross-sections of uterine horns. Sixty days
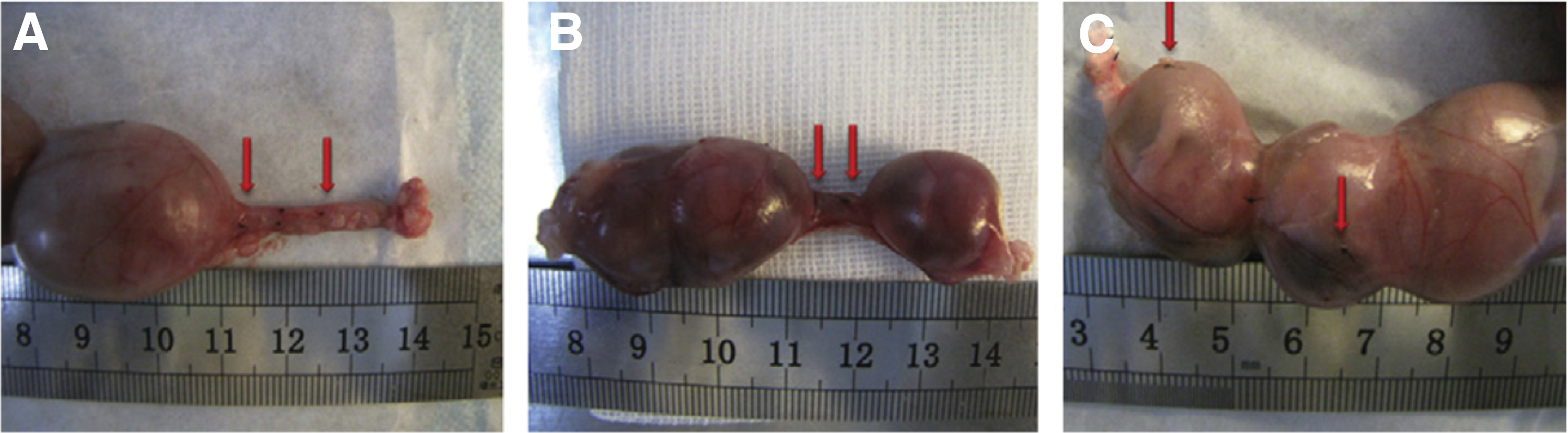
Pregnancy in uterine horns of female rats mated 90 days after injury. The embryos implanted in areas of normal uterine tissue, but not in the scar tissue in PBS group
The CB domain of collagen can also be fused with the N-terminus of natural VEGF to construct a CS/VEGF binding body, and after transplantation into a scarred uterus model, the effect was verified. It was found that CS targeting VEGF not only promotes the remodeling of the scarred uterus but also promote the regeneration of endometrial cells, uterine smooth muscle cells, and blood vessels, which is beneficial for improving pregnancy outcomes. 100 Therefore, the growth factor family could stimulate vascular regeneration and epithelialization of the damaged tissue endometrium, and also proved that gelatin scaffolds can provide a microenvironment where growth factors exert appropriate biological functions in tissue repair (Table 2).
Other Strategies for Uterine Regeneration
Injecting stem cells into hydrogels suitable for cell growth and reproduction is also one of the strategies currently used in uterine regenerative medicine. Research on injecting BMMSCs and hUCMSCs or ADSCs 65 into hydrogels has achieved good results. 101 It is worth mentioning that BMMSCs can be automatically transplanted without immune rejection, demonstrating advantages in tissue and organ repair and recovery. 102
Molecular Modulation of the Uterine Repair Procedure
To tease apart the currently available studies that entailed uterine tissue engineering to repair uterine tissue damage, and to ascertain whether to use hUCMSCs,64,103 ADSCs,23,28 or h-AECs96 as seeds, a uterine tissue injury model to regenerate, repair, and restore pregnancy competence comparable to that previously shown must be accompanied by the elevated presence of VEGF-A, transforming growth factor-β (TGF-β), and fibroblast growth factor (FGF). 23 These bioactive factors act to promote growth and development and tissue differentiation by promoting local cell proliferation and inhibiting apoptosis.104–106
VEGF is crucial for endometrial cell hyperplasia and endometrial angiogenesis, 103 and studies have shown that combining VEGF with collagen alone can remodel full-thickness uterine injury.64,100 Fibroblasts, vascular endothelial cells, and smooth muscle cells proliferatively differentiate during tissue repair, and b-FGF has biological effects that stimulate the proliferation of these cells, bringing into play functions in the repair process to facilitate cell survival, migration, and cell matrix production, as well as degradation. 107 Transplanting CS loaded with FGFs into the uterine cavity can promote the regeneration and repair of damaged endometrium. 27 TGF is involved in regulating cytodifferentiation, tissue repair, and inflammatory processes. 108
Seed cells with stem cell activity transformed by paracrine action and production of TGF-β1 may promote tissue repair—participating in creating a favorable tissue-regenerating microenvironment, with subsequent rapid deposition of ECM. 109 TGF-β acts to induce endometrial proliferation and modulate immune responses.110,111 Meanwhile, TGF-β1 positively affects uterine regeneration by reducing apoptosis, inflammation, and immune responses.112–115 Although multiple components comprise the ECM, its defining component is Col 1. 116
A variety of components constitutively contribute to the ECM in the animal models showing successful repair and regained pregnancy capability; for example, increased matrix metalloproteinase-9 expression, 29 decreased platelet-derived growth factor (PDGF), and connective tissue growth factor (CTGF) expression are often observed to reduce collagen deposition, 74 thus altering the tissue and cellular mechanisms of proliferative repair.
Studies have confirmed that PDGF-C may be an initiating factor of fibrosis when its overexpression could activate multiple profibrotic genes and activate fibrosis-related signaling pathways, leading to ECM deposition and thus tissue fibrosis.117–119 PDGFs accelerate stromal cell hyperplasia through autocrine action during the cell multiplication phase.105,120 THBS1, an in vivo TGF-β of major endogenous activators, has been confirmed as a profibrotic cytokine that could regulate fibrillar collagen expression121–124 and obstruct the hyperplasia and angiogenesis of human endometrial cells. Therefore, THBS1 is an adverse factor for tissue regeneration and repair.125–128 CTGF is a TGF-β-induced multifunctional stromal cell protein involved in TGF-β-downstream mediators of fibrosis promoting effect. 83 The overexpression of CTGF in endometrial tissue is an effective therapeutic indicator for combating endometriosis. 129
The repair of uterine tissue using tissue engineering is still in its nascency, and its underlying mechanisms are currently under intense study. We need to generate more models of complete repair of uterine tissue defects in animal models; and we need to uncover variously seeded tissue engineering scaffolds loaded with cells or growth factors. The mechanisms subserving complete uterine repair also require elucidation so as to apply them effectively.
Criteria for Repair Adjudication
Due to the lack of research on uterine repair and the brief period of time researchers tried applying tissue engineering to uterine regeneration, a standardized scheme has not yet been formed to test the reparative effects of various extant strategies. In the currently available literature, cell proliferation markers and mature-cell antibody formation comprise the molecular means by which to detect reparative effects. Ki67 immunostaining has also been used to evaluate the proliferative effect 130 —as have pan-cytokeratin, ER, and PR—after any kind of transplantation. The regeneration of blood vessels and endometrial cells is an important indicator in evaluating endometrial tissue repair.23,27
However, supporting embryo implantation, growth, and development is the most important criteria for evaluating the function of regenerated endometrium, and therefore all studies must meet this fertility test. No matter the type of animal model selected, or the kind of strategy used for uterine tissue repair, the ultimate goal is successful completion of pregnancy in the repaired uterus. Therefore, research on tissue engineering for uterine repair should cover the spectrum from phenomenologic to mechanistic and confirm effective uterine repair so as to achieve pregnancy, and researchers should also attempt to elucidate the mechanism(s) governing molecular repair of the uterus.
Summary
Although multiple strategies have been applied to treat damaged uterine tissue and promote repair, most studies have only stayed in the experimental animal research stage. More research is needed to use existing research methods to treat larger uterine tissue injuries and defects, and further apply them to clinical feasibility. In terms of current research results, bioengineering strategies have shown great advantages as potential treatment methods and therapies for female infertility, and the clinical transformation of tissue engineering strategy technology is undoubtedly imminent.
In this report, we reviewed the relevant articles on uterine regeneration, searching PubMed with a combination of key words that primarily concerned rat models and one rabbit model. Although these studies included differing methodologies, the injured uterus recovered well morphologically and functionally in every study. However, UTx precipitates many problems in the medical, ethical, and social fields. Although the term “artificial uterus” was also searched and some improvements in this technology were reported, some time is required for the technology to reach a clinically applicable stage, and thus, further human studies and trials are warranted. 131
Footnotes
Acknowledgments
Thanks to the magazine editors for their guidance and help in the process of publication. Special thanks to Professor Changzhong Li for his help and support in the writing process and to all the authors for their dedication and help. We thank LetPub for its linguistic assistance and scientific consultation during the preparation of this article.
Authors' Contributions
D.H., J.L., J.Y., C.Y., X.W., and T.D. contributed to conceptualization; D.H., J.L., and J.Y. contributed to constructing search strategy; D.H., J.Y., and T.D. performed investigation; D.H. and X.W. contributed to data acquisition; D.H. performed visualization; D.H., J.Y., and C.Y. contributed to writing of the original draft; D.H., J.L., J.Y., C.Y., T.D., and T.S. contributed to writing-review and editing; F.W., C.L., and T.S. performed supervision; F.W. contributed to project administration; and C.L. and F.W. performed funding acquisition. All authors have read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Rongxiang Regenerative Medicine Foundation of Shandong University [Grant No. 2019SDRX-21] and the Jinan Science and Technology Program [Grant No. 202019161].