
Abstract
Dentin is a bone-like matrix that forms the bulk of the tooth. By fabricating dentin with protocols involving demineralization, sterilization, and preservation, treated dentin matrix (TDM)/demineralized dentin matrix (DDM) could be obtained, which is considered as a useful tool for bone and tooth–tissue regeneration. Non-negligible inflammatory and immune responses are reviewed in this article of autogenous, allogeneic, and xenogeneic TDM/DDM for the first time. Both autogenous and allogeneic TDM/DDM showed good biocompatibility in original and clinical studies, while a few cases reported the observation of inflammatory cells around tissue samples. As for xenogeneic TDM/DDM, multiple immune responses were revealed. Immune cells, including eosinocytes, macrophages, lymphocytes, mutinucleated giant cell, M1/M2 macrophages, and Th1-type CTL responses were involved. To avoid these adverse inflammatory responses caused by TDM/DDM implantation, some of the effective fabricating methods are discussed to reduce host immune responses to TDM/DDM.
Impact statement
This review aims to first narratively summarize the in vivo and human immune responses during implantation of autogenous, allogeneic, and xenogeneic treated dentin matrix (TDM)/demineralized dentin matrix (DDM)-guided bone/dental regeneration, and xenogeneic TDM/DDM is found to induce the most severe host immune responses. Also fabricating protocols for host response reduction of related tissue engineering are discussed. We consider that the lessons learned could contribute to the push toward bone/dental regeneration and future clinical practices.
Introduction
Given that the human body is considerably impossible to heal on its own under severe injuries or defects, regenerative strategies are developed to remodel or induce healing of tissue and organs. 1 Extracellular matrix (ECM), the natural 3D microenvironment around cells, is mainly made up by collagens and non-fiber-forming proteins,2,3 and could activate cellular processes involving proliferation, differentiation, and migration. Teeth are considered as highly specialized organs and are essential for overall health and wellbeing of human. 4 Currently used therapies regarding tooth damage and loss repair mainly rely on synthetic materials. 4 But these materials serve rare biological functions, such as promoting blood and nerve supplies, leading to poor clinical restorative outcomes and prognosis.4–6 Hence, the field of tissue engineering and regenerative medicine in dentistry is promoted for tooth regeneration. Among strategies for tooth regeneration, treated dentin matrix (TDM)/demineralized dentin matrix (DDM)-oriented technique has been a growing interest of original studies and clinical reports in recent years.7–9
Generally speaking, clinical outcomes of TDM/DDM-oriented regeneration varied. Processing methods, and the host immune response to these autogenous, allogeneic, and xenogeneic materials may contribute to this disparity. Harvest of dentin matrix mainly rely on vital and nonvital human permanent teeth, and were produced mainly in various shapes, including sheets, slices, chips, and root shaped. 7 TDM/DDM were mainly fabricated by demineralization, sterilization, and preservation. Addition of atelopeptidization, 9 cryopreservation, 10 lyophilization, 11 N-acetylcysteine (NAC), 12 recombinant human bone morphogenetic 2 (rh-BMP 2), 13 and tert-butyl-hydroquinone (tBHQ) 14 could also facilitate TDM/DDM-guided regeneration.
The focus of this review, is the host immune response to autogenous, allogeneic, and xenogeneic TDM/DDM, which is also a prominent influencing factor to the clinical outcome. Each source of biomaterial has its own advantages and disadvantages. 15 Autogenous TDM/DDM refers to the biomaterial originating from the individual itself with ideally excellent biocompatibility, but additional surgery is needed, which may cause complications.16–18 Allogeneic TDM/DDM is definite as the biomaterial taken from the same species as the recipient with genetical dissimilarity, it has relatively wide access and antigenicity.16,19 Xenogeneic TDM/DDM is not only derived from a genetically different species compared with the recipient with high volume but also high antigenicity and high risk of spreading disease. 16 Implantation of biomaterials may generate host reactions, which include injury, acute inflammation, and chronic inflammation, which may lead to both constructive remodeling outcome and unfavorable outcome. 20
Hence, the present review describes various aspects of the host response to autogenous, allogeneic, and xenogeneic TDM/DDM-oriented dental/bone regeneration and the factors that affect this response.
Definition of TDM/DDM
There exist various sources of TDM/DDM. The majority of the reported studies relied on human nonfunctional third molars, and maxillary and mandibular premolars extracted for orthodontic requirements. Permanent teeth from rats, dogs, rhesus macaque, porcine, bovine, and goats all contributed to fabricating TDM/DDM (Fig. 1).7,21–23 According to a previous systematic review, despite the authors' proposal that the term DDM be used for regenerative purposes, while the term TDM be used for physical treatments, there still existed articles of TDM-oriented tooth regeneration. 7
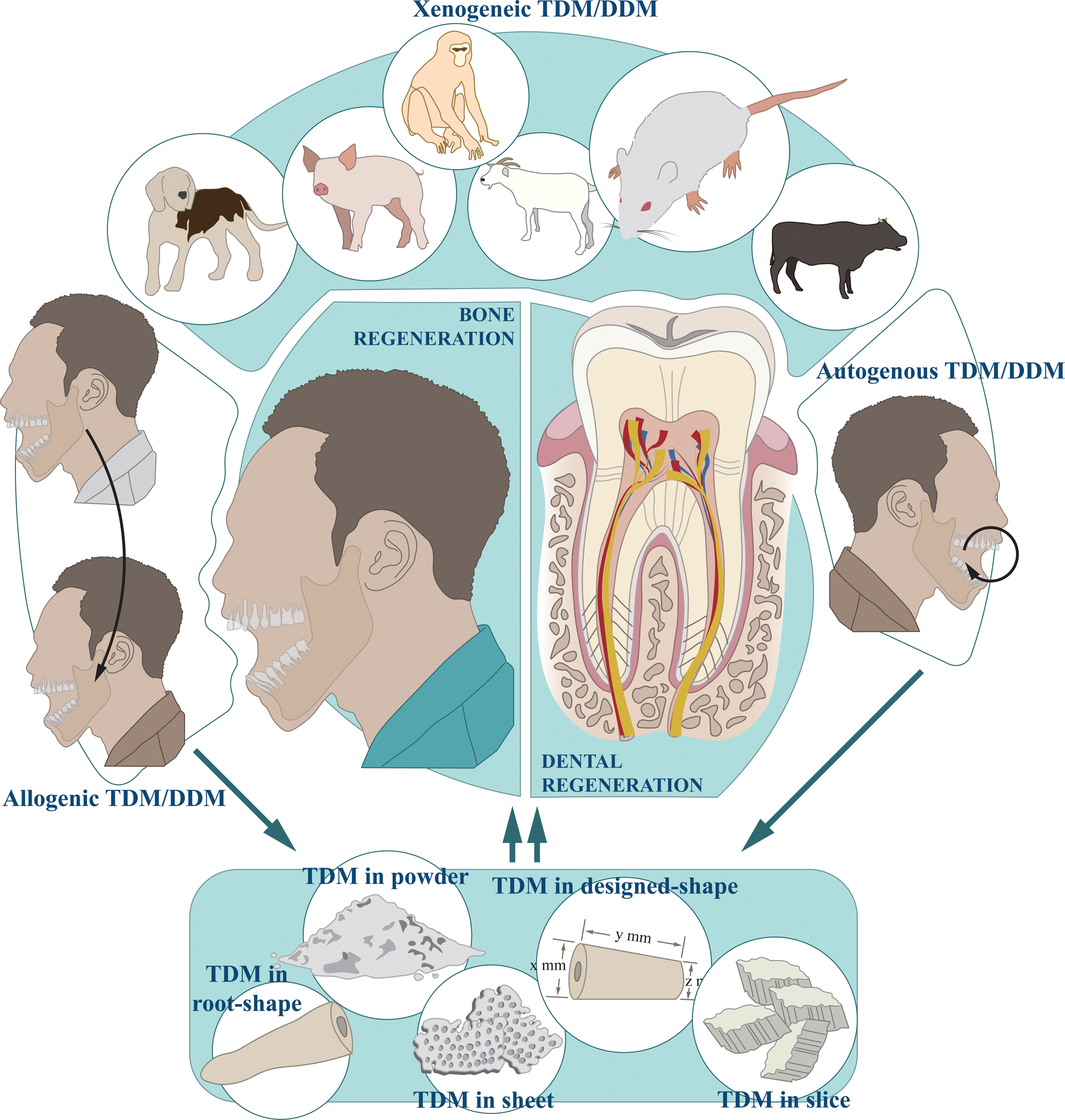
Source and fabricated shape of TDM/DDM during tissue regeneration. Autogenous, allogeneic, and xenogeneic TDM/DDM are fabricated for tissue regeneration. Autogenous TDM/DDM refers to the biomaterial originating from the individual itself. Allogeneic TDM/DDM is the biomaterial taken from the same species as the recipient with genetical dissimilarity, and xenogeneic TDM/DDM is derived from a genetically different species compared with the recipient. TDM/DDM is further fabricated into root shape, powder, sheet, slice, and designed shape. TDM/DDM, treated dentin matrix/demineralized dentin matrix. Color images are available online.
From our perspective, “D” in “DDM” is short for “demineralization”, which is a process to decrease antigenicity, facilitate exposing organic substances, lower the ratio of inorganic content, and enhance cell adhesion using various concentrations of ethylenediaminetetraacetic acid (EDTA
However, as the number of articles increased and the design became more complex, variants of both terms were created. One is to prefix the term with the initials of the source species. For instance, pTDM is short for porcine TDM, 27 hTDM is short for human TDM, 28 and rTDM is short for rat TDM. 12 The other is to prefix the term with special process during the protocol. For instance, PDDM is short for partially demineralized dentin matrix, 29 HDDM is short for homogenous demineralized dentin matrix, 30 LTDM is short for low-speed hTDM, and HTDM is short for high-speed hTDM. 31 Hence, for ease of understanding, we will use “TDM/DDM” throughout this review to refer to the above and related biomaterials, which should be defined as: TDM/DDM is (1) a kind of biomaterial of all species' origin and (2) dentin matrix/graft that is demineralized by any means, without other dental structure such as enamel and cementum.
The Host Immune Response to Autogenous, Allogeneic, and Xenogeneic TDM/DDM
Autogenous TDM/DDM
Compared with other types of TDM/DDM, autogenous TDM/DDM possesses good biocompatibility but request obtaining additional surgery. 16 It has been widely used for promoting the bone regeneration process during extraction, socket preservation, ridge augmentation, sinus bone graft, and guided bone regeneration (GBR) for implant site development with the advantage of induction of rapid healing without immune rejection.13,23,26,32
Histomorphometrical analysis in the majority of studies, including randomized controlled clinical trial and case reports, revealed that autogenous TDM/DDM is compatible with the host tissues without any notable inflammatory reaction, and no clinical signs of significant infection were reported.26,33 While a few cases reported the observation of inflammatory cells around tissue samples. In a case where the extracted 1st molar of a 61-year-old female was fabricated into autogenous TDM/DDM for GBR, inflammatory cells and hemorrhage findings were shown around the tissue samples after 2 months after the surgery. 34 In another case using autogenous partial TDM/DDM for alveolar bone regeneration, very few multinucleated osteoclastic cells were observed on the surface of TDM/DDM 32 ; but the immune response in both cases did not affect the outcome. Hence, it could be concluded that the mild inflammatory response after implanting autogenous TDM/DDM could promote tissue regeneration.
The molecules contained in autogenous TDM/DDM may also contribute to its good biocompatibility, as it includes various immune-related molecules. For instance, transforming growth factor-β1 released from dentine could achieve anti-inflammatory response, 35 and by regulating interleukin-1β production, osteopontin may be a critical component of the antibacterial immune response. 36 To note, there existed a wide use of TDM/DDM combining rhBMP-2 since the approval by the United States Food and Drug Administration in 2017. 13 Although the enhanced osteoinductive bone formation at an early stage of the combination has been reported, its immunity-inducing capability compared with TDM/DDM remains to be studied, as high concentration of rhBMP-2 could induce inflammatory side effects by increasing osteoclastic activity in a cancellous bone environment.
Allogeneic TDM/DDM
Although autogenous TDM/DDM has its promising clinical results for tissue regeneration, it has limitations such as insufficient quantity and patient preference. Allogeneic TDM/DDM has been considered as an alternative.15,16 Compared with the millions of cases of biological scaffolds composed of allogeneic ECM implanted during the past decades worldwide, 15 studies of allogeneic TDM/DDM targeting tissue regeneration are relatively lacking.
Allogeneic TDM/DDM has been proved to guide both bone and dental regeneration without a severe inflammatory response by the host.8,30,37,38 Antigenicity by immunologic reaction was assessed after synthesizing all allogeneic TDM/DDM-related studies, such as higher mean white blood cell count compared with the control group. However, studies related to inflammation and immune mechanisms caused by allogeneic TDM/DDM are still lacking.
Xenogeneic TDM/DDM
Xenografts and xenogeneic matrices have high volume compared with other biomaterials. 15 When it comes to clinical practice, the primary determinant of outcome of the xenogeneic scaffolds, such as xenogeneic TDM/DDM, is the response of the host to the materials, and the balances, including the innate and acquired host immune responses between the materials is essential for a successful outcome.
Despite most studies implanting xenogeneic TDM/DDM showed no inflammatory cell infiltration in the area surrounding the material, proving its excellent histocompatibility, proper host responses that accelerate the healing process and enhancing tissue regeneration was also observed.24,27,39 At 2 weeks after implanting human TDM/DDM into rabbit calvaria, infiltrated multinucleated giant cells, lymphocytes, eosinocytes, macrophages, and bleeding were exhibited. 21 At 4 weeks after the surgery, lymphocytes, macrophages, and a few multinucleated giant cells could still be observed, while plasma cells and slight inflammatory response with macrophages, lymphocytes, and eosinocytes presented at 8 weeks after the surgery. 21 In another study implanting human TDM/DDM into tooth sockets of the rat model, scattered inflammatory process was observed in the apical portion of the socket 3 days after the surgery, showing an advanced healing process, and no neoformed capillaries (granulation tissue) were found. 40
Similarly, by implanting human TDM/DDM into subcutaneous tissues of rats, moderate inflammation with predominant macrophages was observed after 3-, 7-, and 15-day periods, and the inflammatory responses reduced to mild after 30 days. 41
All of these findings suggest that xenogeneic TDM/DDM could stimulate a mild-to-moderate inflammatory response in the host to accelerate the process of tissue healing and regeneration.
It is worth exploring the immune responses behind the satisfied regenerative outcome guided by xenogeneic TDM/DDM, and the in-depth mechanism has been studied in the context of both bone and dental regeneration.
During bone remodeling, osteoclasts (OCs) are the only cells to degrade bone by the polarized secretion of proteolytic enzymes. 42 Immune and bone systems share a variety of molecules, including cytokines, chemokines, transcription factors, and signaling molecules. In many acute and chronic inflammatory conditions, excessive OC activation could lead to bone resorption and loss, which is defined as osteoimmunology. 43 In xenogeneic TDM/DDM-guided bone regeneration, activation and abnormal activities of multinucleated OCs were observed. To ensure the feasibility of clinical application, tBHQ, an anti-inflammatory antioxidant, was found to relieve the unfavorable process of OCs. 44 Apart from inducing heme oxygenase-1 (HO-1), a negative regulator of inflammation, 45 tBHQ could inhibit the release of high-mobility group box1 (HMGB1), which is a contributor to oxidative stress. 46
Further investigation suggested that compared with the group treated by xenogeneic TDM/DDM only, osteoclastogenesis-related molecules, including HMGB1, its receptor for advanced glycation end products (RAGE), cathepsin K (Cath-K), receptor activator of nuclear factor kappa-B (RANK), and nuclear factor kappa-B p65 (NF-κB p65) were all remarkably decreased, whereas HO-1 was increased in the tBHQ-added group. 14 It then demonstrated that xenogeneic TDM/DDM could stimulate the osteoimmunological response, the antioxidant tBHQ could suppress the induced osteoclastogenesis.
Xenogeneic TDM/DDM could trigger host M1/M2 macrophages' polarization and secretion when inducing dental regeneration. The polarization of macrophages and its secreted factors have been intensively studied.27,47 Among the five different phases of foreign body reaction, macrophages are known to participate in acute inflammation, chronic inflammation, foreign body giant cell formation, and fibrosis, and they were initially believed to have a complete negative effect on biocompatibility. 48 But recent studies revealed that both M1 macrophages that promote inflammation and M2 macrophages with diverse regulatory subtypes were indispensable for integration of biomaterials and replacement of degradable biomaterials. 48
By implanting porcine TDM/DDM into mandible defects of rats, CD68+CD163+M2 macrophages and CD68+iNOS+M1 macrophages were both observed, and a relatively balanced expression of M1 and M2 macrophages at 1 month after surgery was shown. 39 Compared with the less expression of CD163 and more expression of NOS2 at the early stage, the CD163+/NOS2+ ratio was greater than 1 at 1 month, indicating the host response might be mediated by xenogeneic TDM/DDM in the later stage.
Expression of TGF-β1 and IL-1β was also revealed. 39 Extensive bone resorption with positive OC differentiation took place on the xenogeneic TDM/DDM surface, where quantification analysis of xenogeneic TDM/DDM survival rate showed as low as 20%. Interestingly, the authors also found xenogeneic TDM/DDM could serve as a natural drug carrier for rosiglitazone (RSG). 39 RSG has the probability of creating an anti-inflammatory environment through activating peroxisome proliferators receptors-γ (PPAR-γ), hence, promoting tissue repair. 49 By loading RSG, the TDM/DDM/RSG complex could activate the PPAR-γ-NF-κB axis; more CD68+ CD163+ M2 macrophages were expressed; and levels of reactive oxygen species (ROS) and its related markers, including 8-hydroxydeoxyguanosine (8-OHdG), 3-nitrotyrosine (3-NT), and malondialdehyde were also found downregulated. 39 As a result, M2 macrophage polarization was promoted, inflammation was relieved, regeneration of periodontal ligament was promoted, and inhibited the formation of OC (Fig. 2a, b).
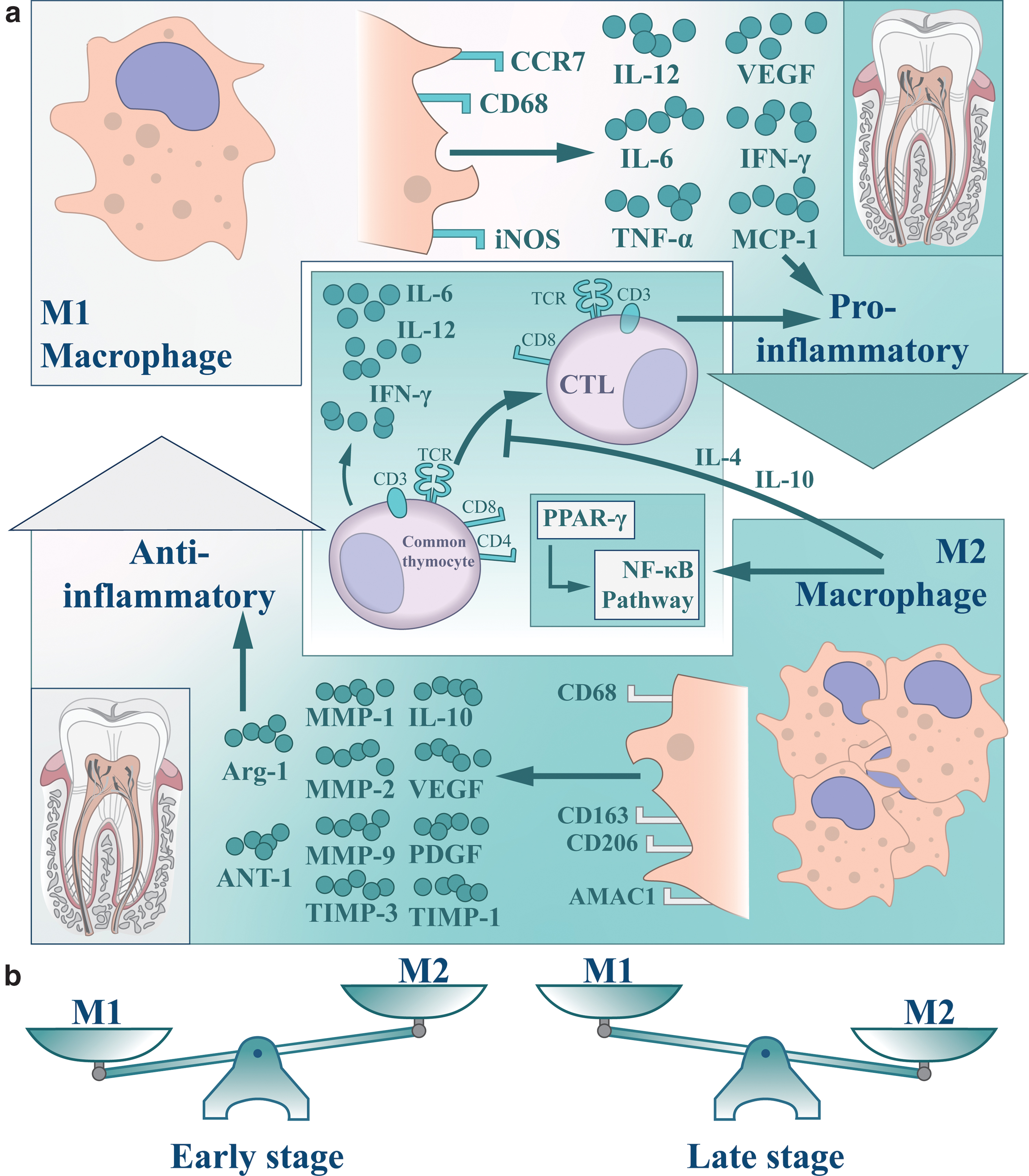
The host response of xenogeneic TDM/DDM-guided tissue regeneration.
To further investigate phenotypes and expression patterns of macrophages, gene expression assays were performed. Compared with normal tissue that only highly expressed CD68, xenogeneic TDM/DDM induced higher expression of IRF5, CD206, TGFβ1, MMP2, TIMP1, and TIMP3 in most groups. 27 Except for biomarkers of M1/M2 macrophages, MMPs are known to regulate equilibrium during fibrogenesis through interactions with TIMPs. MMPs also participate in tissue remodeling and degrading ECM, indicating xenogeneic TDM/DDM may perform a positive impact on promoting tissue reconstruction through balancing expression patterns of M1/M2 macrophages. 27 Nevertheless, it was also noticed that TIMP1, MMP1, MMP2, and MMP9 were reported as downregulated in other studies. 47
Th1-type CTL response targeted by xenogeneic TDM/DDM implantation could be further regulated by macrophages. 47 Further analysis of heatmap revealed that higher expression of proinflammatory cytokines, including IFN-γ, IL-6, IL-10, IL-12, and HGF indicated an accompanied Th1 response, while indiscriminate expression of IL-4 suggested mere Th2 responses. Under the same condition, a subtype of M2 named PPARγ-primed CD68+CD206+ M2 phenotype (M2γ) was found with anti-inflammatory properties; upregulated expression of TGF-β1, IL-4, IL-10, VEGF, and PDGF; and downregulated expression of IL-1β, IL-6, IL-8, and TNF-α. 47 Through the M2γ, triggered CD3+ T cell and CD3+CD8+ CTL lymphocytes were both significantly reduced by IL-4, TGF-β, and IL-10. 47 This regulatory mode eventually facilitated tooth root/tissue regeneration.
Fabricating protocols for host response reduction of TDM/DDM implantation
To avoid the adverse inflammatory responses caused by TDM/DDM implantation, the importance of effective possessing cannot be overstated, whether the source is autogenous, allogeneic, or xenogeneic.
TDM/DDM of different particle sizes, demineralization degrees, and methods of sterilization and preservation could all influence host response after implantation. By processing into 0.25- to 1.0- mm and 1.0- to 2.0- mm particles, TDM/DDM with smaller particle size and sparser space of 200 μm showed fewer infiltration of macrophages and higher rate of new bone formation. 21 Although no statistical significance was observed compared with other groups, such findings could still assist the design of clinical applications.
The effect of demineralization on organ regeneration medicine has been widely studied. Compared with 1-day demineralized and 7-day demineralized TDM/DDM for dentin/pulp tissue regeneration, the 13-day demineralization showed lower aggregation of neutrophil, lymphocyte, and macrophages. 9
Sterilization processes are commonly added to inactivate microbial contaminants and eliminate immunologic risks while maintaining the biological characteristics. Various ways of sterilization of TDM/DDM were mentioned, 7 but some researchers doubted if there was still a risk of an immune response and infection in patients. 38 Hence, autoclaving, a new approach, was introduced, since it has become an established method in reconstructive surgery for bone tumors, and contributes to microbiological safety. 50 Steam sterilization for TDM/DDM was performed at 121℃ and 1 bar for 15 min. 38 No toxic side effects were exhibited, and the autoclaved TDM/DDM could support stem cells differentiating into dentin-like tissue without immunogenicity, suggesting the rapid autoclaving protocol may have the potential for clinical application and enhance tissue regeneration. 38
TDM/DDM containing other molecules or cells could induce better regeneration outcome, and some of these molecules have been proved to regulate host response to TDM/DDM.
NAC, a small molecule, is a precursor of glutathione (GSH) and an ROS scavenger. 51 It could regulate excessive inflammatory responses and prevent the oxidative stress induced by ROS. 51 In the acute inflammatory phase (1 week), NAC-pretreated TDM/DDM exhibited less accumulation of osteoclasts and inflammatory cells, resulting in slighter resorption of TDM/DDM. 12 By alleviating ROS, NAC could also alleviate the suppression of H2O2-induced cell differentiation. A better regeneration outcome was then reached, where significant cementum-like tissue, dense collagen fibers and blood vessels were observed at the TDM/DDM periphery. 12 rh-BMP 2 was used for the treatment of bone defect associated with extraction sockets in sinus and alveolar ridge augmentations with absorbable collagen sponges (ACS). 52 The inflammation induced by rhBMP 2 was reduced compared with those treated without this molecule. 53 After implantation of the combination of rhBMP 2 and TDM/DDM, faster bone/tissue regeneration was observed. 13
In a case series using rhBMP 2/TDM/DDM for socket preservation, immune responses of the host were displayed as collagenolytic resorption of the TDM/DDM, infiltration of adipocytes, and multinucleated giant cells. tBHQ, an antioxidant mentioned before, could also suppress TDM/DDM-induced osteoclastogenesis through upregulating HO-1, downregulating HMGB1, and downregulating osteoclast-related genes such as RAGE, Cath-K, RANK, and NF-κB p65. 14 Combination of other molecules, such as PLGA/gelatin, CMC, and BFP-1 with TDM/DDM all fulfilled biocompatibilities well, while detailed host responses remain to be further discussed. 54
Drawing on approaches of treating skin collagen, atelopeptidization has been performed on TDM/DDM. Using pepsin, acid protease enzymes and lyophilization technologies, collagen of TDM/DDM could be modified, then generating nonimmunogenic atelocollagen. 55 Compared with nontreated groups of 1-, 7-, and 13-day demineralization, atelopeptidized TDM/DDM all showed less aggregation of macrophages, lymphocytes, and neutrophil. 9 Furthermore, atelopeptidization enhanced differentiation of DPSC, but for 13-day demineralization, gene expression decreased in DPSC loaded on atelopeptidized TDM/DDM. 9 This suggests that different aspects of the fabricating protocols may act simultaneously on the same properties of the TDM/DDM, in this case, collagen structure of the 13-day demineralized may have reduced surface area for cell attachment, and the combination of 1-day demineralization and atelopeptidization had the best regeneration effect for dentin/pulp tissue. 9
Outlook for the future
As a unique masticatory organ, tooth is essential for overall health. Regenerative strategies are promised to repair irreversible damages, and TDM/DDM-oriented technique has reached favorable regeneration outcome for both bone/tissue and tooth/tissue. Non-negligible inflammatory and immune responses are first reviewed in this article.
Both autogenous and allogeneic TDM/DDM showed good biocompatibility in original and clinical studies, while a few cases reported the observation of inflammatory cells around tissue samples. Considering the limited volume of autogenous and allogeneic TDM/DDM for human during clinical practice, we also focused on summarizing the host immune responses of xenogeneic TDM/DDM. Despite the satisfied regenerative outcome, multiple immune responses were revealed. Immune cells, including eosinocytes, macrophages, lymphocytes, and mutinucleated giant cell are involved, HMGB1/HO-1 pathway and antimicrobial peptides, including neuropeptide substance P, neurokinin A, calcitonin gene-related peptide, and adrenomedullin also participate. M1/M2 system and Th1-type CTL response are the predominance during xenogeneic TDM/DDM-guided dental regeneration. M1 macrophage of proinflammatory secreted IL-12, IL-6, TNF-α, VEGF, IFN-γ, and MCP-1; M2 macrophage of anti-inflammatory secreted IL-10, VEGF, PDGF, TIMP-1, MMP-1, MMP-2, MMP-9, TIMP-3, Arg-1, and ANT-1.
M2 macrophage could both inhibit differentiation from common thymocyte to CTL and promote PPAR-γ/NF-κB pathway.
As for the processing methods, not only traditional fabricating protocols, but also combination of molecule, and novel technologies such as atelopeptidization were related to host response/modulation of TDM/DDM implantation and regeneration effects. Smaller particle size, lower density, appropriate degree of demineralization, autoclaving for sterilization, cryopreservation or lyophilization for preservation, combination of molecules, and atelopeptidization could all reduce immunogenicity of TDM/DDM, then reduce host response and reach better regeneration effect.
Further studies could be performed with reference to the prospective as follows:
Deeper investigation of all kinds of TDM/DDM-related immune responses should be valued, especially xenogeneic TDM/DDM. Vacancy in roles of B cells, and its interaction with other immune cell clusters might be filled. Integrated fabrication approaches should be introduced to reduce host responses of TDM/DDM. For instance, Meng et al. developed a practical sandwich structure with one kind of seed cell and three kinds of graft materials (Vitamin C, TDM and Matrigel).
56
Vitamin C could induce DPSC cell sheet, and Matrigel could promote proliferation of DPSCs. A s a result, generation of periodontium, dentin, and pulp-like tissues were obtained. The multiapplication of several approaches may foster host response reduction and bone/dental regeneration. To fully understand the immune pattern after TDM/DDM-oriented implantation, single-cell RNA sequencing (scRNA-seq) might provide assistance. scRNA-seq analysis could be used for unbiased discovery of unidentified cell types, cell states, and biologically meaningful cellular heterogeneity. Together with the advances in genomic, chromatin, methylation, and proteomic assays, the integrated strategies may allow us for full understanding of TDM/DDM-related host responses.
Footnotes
Authors' Contributions
T.W. and Y.G. conceived and designed research; T.W. prepared figures; T.W. drafted the article; T.W. and Y.G. edited and revised the article; T.W. and Y.G. approved the final version of the article.
Disclosure Statement
No conflicts of interest are declared by the authors.
Funding Information
This work was supported by the National Natural Science Foundation of China (No. 32171308).