
Abstract
Having genetically related offspring remains an unattainable dream for couples with reproductive failure. Mesenchymal stem cells (MSCs) are multipotent stromal cells derived from various human tissues and organs. As critical paracrine effectors of MSCs, extracellular vesicles (EVs) can carry and deliver bioactive content, thereby participating in intercellular communication and determining cell fate. Mesenchymal stem cell-derived extracellular vesicles (MSC-EVs) have shown promising therapeutic effects, including repairing injured endometria, restoration of ovarian functions, and improving sperm quantity, morphology, and motility, owing to their regenerative potential, abundant sources, high proliferation rates, low immunogenicity, and lack of ethical issues. However, limited knowledge on purification and isolation of MSC-EVs, therapeutic effects, and unpredictable safety have caused challenges in overcoming female and male infertility. To overcome them, future studies should focus on modification/engineering of MSC-EVs with therapeutic biomolecules and combining attractive biomaterials and MSC-EVs. This review highlights the latest studies on MSC-EVs therapies in infertility and the major challenges that must be overcome before clinical translation.
Impact statement
Mesenchymal stem cell-derived extracellular vesicles (MSC-EVs) represent a novel and promising therapeutic approach in infertility, owing to their regenerative potential, abundant sources, high proliferation rates, low immunogenicity, and lack of ethical issues. Promising therapeutic effects include repairing injured endometria, restoring ovarian functions, and improving sperm quantity, morphology, and motility. However, research on MSC-EVs therapies (MSC-EV-Ts) in infertility still needs improvement in many aspects, including establishing standard disease models, optimizing administration routes, and using tissue engineering to enhance retention and efficacy. This review highlights the latest studies on the potential mechanisms and preclinical effects of MSC-EV-Ts, and provides suggestions for future studies.
Introduction
Infertility, a condition currently affecting 15% of couples worldwide, is the inability to achieve pregnancy with regular unprotected sexual contact for >1 year. 1 Ovulatory dysfunction, endometriosis, tubal disease, and male infertility are among the most common causes of infertility in couples. These issues can be resolved with conventional treatments such as ovulation-inducing drugs or assisted reproductive technologies (ART). 2 However, numerous couples cannot conceive even after ART, especially those with endometrial injury, ovarian failure, or nonobstructive azoospermia (NOA). Therefore, there is an urgent need to understand the underlying mechanisms and develop effective and timely therapeutics for such disorders.
Mesenchymal stem cells (MSCs) are now garnering significant attention as a promising alternative approach in the field of regenerative medicine,3–5 owing to their abundance, low immunogenicity, and simplicity of isolation and manipulation in vitro. The therapeutic effects of MSCs rely on their paracrine activity. As major paracrine effectors of MSCs, extracellular vesicles (EVs) carry multiple biological information (proteins, nucleic acids, and lipids) and deliver the contents of the vesicles to target cells, thereby mediating the intercellular communication system. 6
Interestingly, mesenchymal stem cells-derived extracellular vesicles (MSC-EVs) can reportedly promote comparable therapeutic activities as MSCs, effectively promoting tissue regeneration capacity. 7 Moreover, MSC-EVs therapies (MSC-EV-Ts) can reduce MSC engraftment risks, allow the crossing of biological barriers and improving safety. The emergence of novel biomaterials and recent modification/engineering of MSC-EVs further enhances confidence in MSC-EV therapy.
Studies have been conducted to evaluate their implications in models of organ infertility, focusing on endometrial-, ovarian-, and testicle-related infertility. Research on MSC-EVs therapies in infertility still needs to improve in many aspects, including establishing standard disease models, optimizing administration routes, and using tissue engineering to enhance the retention and efficacy of MSC-EVs.
In this study, we summarize the characteristics, molecular properties, and biological functions of MSC-EVs. Next, we systematically review the existing research describing MSC-EVs in fertility biology and infertility disorders and discuss their limitations and potential priorities in therapeutic regimens. Finally, we suggest some improvements for MSC-EVs treatment in infertility to enable clinical application.
Overview of MSC-EVs
Origin, characterization, and roles of MSCs
MSCs are multipotent stromal cells obtained from various human tissues and organs. MSCs were first identified in the bone marrow 8 and subsequently in various tissues, such as the umbilical cord, menstrual blood, and adipose tissue. 9 In 2006, MSCs were officially defined by the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy as (a) plastic-adherent cells when maintained in standard culture conditions, (b) expressing CD105, CD73, CD90, without expressing CD45 CD34, CD14 or CD11b, CD79α or CD19, and HLA-DR surface molecules, and (c) having the capacity to differentiate into osteoblasts, adipocytes, and chondroblasts in vitro. 10
MSCs obtained from different tissues vary in isolation success rate, phenotype, morphology, proliferation potential, and multidifferentiation capacity; however, they display many common characteristics attributed to their bone marrow counterparts.11,12
MSCs are notable for their self-renewability and multilineage differential potential. 13 For the past decade, our understanding of the mechanisms underlying MSC-based tissue regeneration has significantly evolved. Despite the initial model of MSCs homing into injury sites and differentiating into multiple cell types, there is a consensus that another mechanism underlying the therapeutic functions of MSCs exists, of which paracrine signaling is considered a critical player. 14 Therefore, several experts recommend renaming MSCs as medicinal signaling cells to reflect this fact more accurately. 15
In addition, MSCs release a broad range of biologically active factors, including cytokines, chemokines, growth factors, and vesicular secretions, termed EVs, which are decision-makers of local cellular fate. 16 Consequently, acellular therapies that harness MSC secretions to promote tissue repair are becoming increasingly popular in regenerative medicine.
Molecular properties and biological functions of MSC-EVs
EVs are membrane-enclosed nanosized particles released from all living cells with potent autocrine and paracrine biological activities. 17 EVs are classified into three categories based on their size and release route: exosomes (Exos, ∼30–150 nm), microvesicles (MVs, ∼100–800 nm), and apoptotic bodies (ABs, ∼200–5000 nm). 18 Exos are vesicles resulting from the inward invagination of the endosomal membrane and the fusion of multivesicular bodies with the plasma membrane.
MVs are formed by direct outward budding from the plasma membranes of healthy cells, and ABs are formed by outward blebbing of the plasma membrane during apoptosis. 19 It is obvious that there are overlaps between the classic EVs subgroups, thus isolated EVs can be very heterogeneous. Further understanding of the diversity of EVs (vesicle size, density, RNA, protein, DNA cargo, and morphology) will be required for future classifications.
EVs are abundantly present in various human body fluids, 20 and their properties depend on the originator cells and may be influenced by physiological stress or pathological conditions, 21 suggesting potential as biomarkers for diagnosis or prediction. EVs facilitate intercellular communication by contacting or internalizing contents (proteins, nucleic acids, and lipids) and by fusion with or endocytosis into recipient cells. 22
The cargo-transferring ability of EVs can be exploited to deliver therapeutic molecules. Notably, there has been a growing interest in modified/engineered MSC-EVs to deliver many therapeutics, including miRNA, RNAi, CRISPR/Cas9, membrane proteins, and cytoplasmic proteins to target tissues, including the reproductive system. 23
Therefore, MSC-EVs are highly attractive for harnessing the clinical benefits of MSC therapy through cell-free strategies.
Key steps in therapeutic applications of MSC-EVs
The transition from preclinical to clinical applications involves the acquisition, culture, and identification of MSC-EVs in vitro, followed by infusion of the MSC secretome through intravenous or transcutaneous delivery to achieve the desired therapeutic effects, directly or indirectly (Fig. 1).
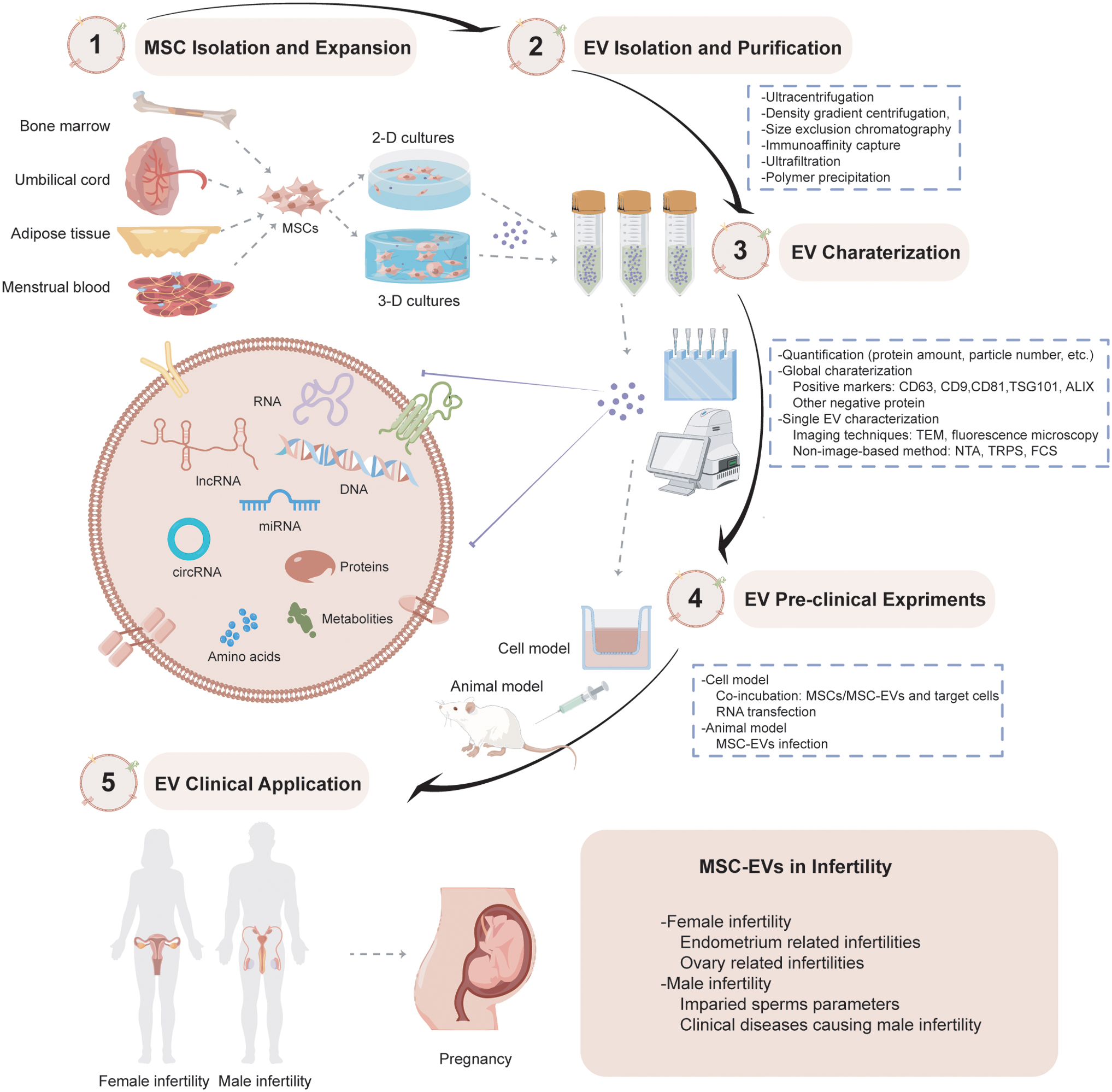
MSC-EVs' key steps in the process of therapeutic applications, including their origins, biogenesis, purification, characterization technologies, and preclinical experiments. EV, extracellular vesicles; FCS, fluorescence correlation spectroscopy; IUA, intrauterine adhesion; MSC, mesenchymal stem cells; MSC-EVs, mesenchymal stem cells-derived extracellular vesicles; NTA, nanoparticle tracking analysis; PCOS, polycystic ovarian syndrome; POI, premature ovarian insufficiency; TEM, transmission electron microscopy; TRPS, tunable resistance pulse sensing. Color images are available online.
The availability, characteristics, and regenerative potential of MSCs isolated from different tissues vary significantly. Bone marrow MSC-EVs are the most commonly used EVs in clinical trials. MSC-EVs from adipose tissue can be obtained by liposuction and easily expanded and enriched in vitro. Compared with MSCs obtained from adipose tissue or bone marrow, umbilical cord MSCs offer low immunogenicity, higher proliferative capacity, and activated secretion of chemokines, pro-inflammatory proteins, and growth factors. 24 Therefore, it is important to choose the proper cell source and isolation and manipulation techniques according to the specific requirements of the research or clinical application.
MSC-EVs express transmembrane, glycosylphosphatidylinositol-anchored, and cytosolic protein markers, including CD29, CD73, CD44, and CD105, which can be detected using western blotting or enzyme-linked immunosorbent assay. 25 Therefore, specific markers should be identified before further experimentation and application. Moreover, transmission electron microscopy and nanoparticle tracking analysis are commonly used to characterize EVs at the single-particle level. 26
The future of MSC-EVs depends on large-scale culture and effective isolation methods. Culturing vesicles using existing methods results in low yields and are unscalable; therefore, novel approaches have been adopted to increase EV production by maximizing the surface area of cultures, such as microcarrier-based three-dimensional cultures, resulting in a 20-fold higher yield. 27 In addition, cell culture supernatants can be used to isolate MSC-EVs; for this approach, several technical factors (such as cellular confluence, oxygen concentration, cytokines, and serum content of the medium) should be standardized to ensure reproducibility across batches. 28
Furthermore, different isolation methods have been established for MSC-EVs based on their physical and chemical characteristics, including ultracentrifugation, density gradient centrifugation, immunoaffinity capture, size exclusion chromatography (SEC), ultrafiltration, and polymer precipitation. 29 Several studies have demonstrated that ultrafiltration and SEC give a high yield of EVs and preserve their biophysical and functional properties. 30 Nevertheless, low-cost methods for obtaining high-purity, high-integrity, and high-yield MSC-EVs are lacking.
Moreover, it is critical to consider the biodistribution, targeting mechanisms, and safety profiles of MSC-EVs. Recently, clinical trials conducted on MSC infusion have shown its role in tissue regeneration, immunomodulation, and treatment of graft-versus-host diseases, cardiovascular diseases, and liver cirrhosis. 31 However, EV therapy in clinical practice is still relatively new, and future research will likely see a huge increase in the number of MSC-EVs replacing MSCs.
Female Infertility and MSC-EVs
Female infertility can be caused by various disorders, such as intrauterine adhesion (IUA), premature ovarian insufficiency (POI), endometritis, thin endometrium, and polycystic ovarian syndrome (PCOS). MSC-EV therapy has been shown to repair injured endometria and restore the ovarian reserve. In this section, we summarize the evidence for the effectiveness of MSC-EV therapy for infertility in women (Table 1 and Fig. 2).
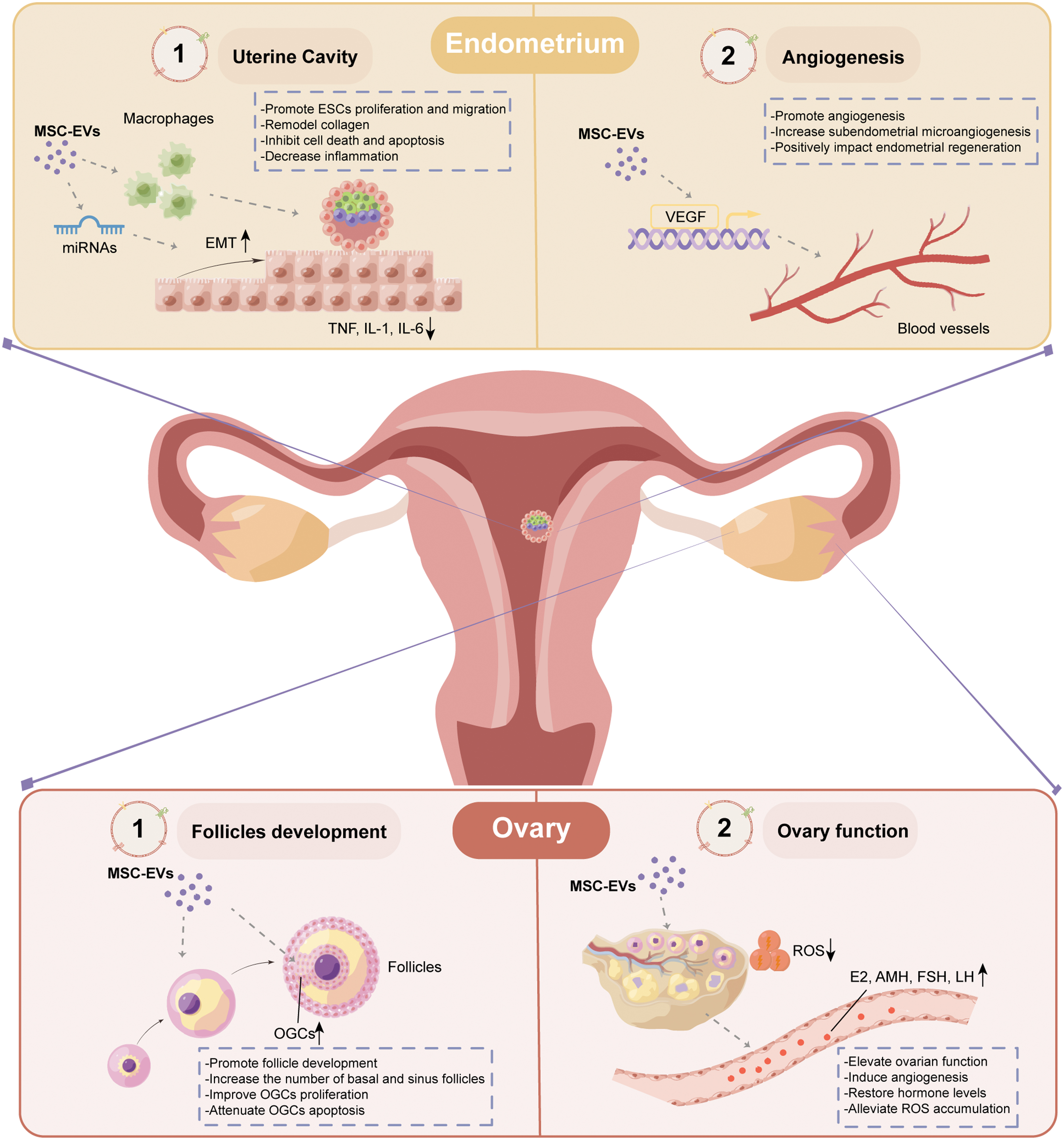
Physiological functions of MSC-EVs in female infertilities. AMH, anti-Mullerian hormone; E2, estradiol; EMT, epithelial–mesenchymal transition; ESCs, endometrial epithelial cells; FSH, follicle-stimulating hormone; LH, luteinizing hormone; OGCs, ovarian granulosa cells; ROS, reactive oxygen species. Color images are available online.
Effects of Mesenchymal Stem Cells-Derived Extracellular Vesicles in Female Infertility
AB, apoptotic body; AFSC, amniotic fluid stem cells; AMH, anti-Mullerian hormone; AMSC, adipose-derived mesenchymal stem cell; AS, Asherman's syndrome; BMSCs, bone mesenchymal stem cells; BUS, busulfan; CCs, cumulus cells; CTF1, cardiotrophin-1; CTX, cyclophosphamide; DHEA, dehydroepiandrosterone; E2, estradiol; EMT, epithelial–mesenchymal transition; EPCs, endothelial progenitor cells; EVs, extracellular vesicles; Exos, exosomes; FSH, follicle-stimulating hormone; IL, interleukin; iPSC, induced pluripotent stem cell; IUA, intrauterine adhesion; LH, luteinizing hormone; LIF, leukemia inhibitory factor; LPS, lipopolysaccharide; LTZ, letrozole; MenSCs, menstrual blood-derived stem cells; MSC-EVs, mesenchymal stem cells-derived extracellular vesicles; OGCs, ovarian granulosa cells; PCOS, polycystic ovarian syndrome; PARP, poly(ADP-ribose) polymerase; POI, premature ovarian insufficiency; ROS, reactive oxygen species; TGFβ1, transforming growth factor β1; UCMSC, umbilical cord mesenchymal stem cell; UMSC, uterus derived mesenchymal stem cells; VCD, 4-vinylcyclohexene diepoxide.
Intrauterine adhesion
IUA (also called Asherman's syndrome or endometrial fibrosis) is an endometrial repair disorder after uterine injury, which may lead to complications, such as recurrent abortion and secondary infertility. Hypoxia, inflammation, and decreased revascularization are commonly seen. 32 IUA is mostly treated by hysteroscopic adhesiolysis (HA), a minimally invasive procedure that cuts and removes scar tissue and maintains a physiological structure from the uterus. However, surgery may not be feasible or successful in every case, especially severe ones. The IUA recurrence rate after HA is as high as 76%. 33 Besides, complete restoration of the functional endometrium in patients is still a problem.
In vitro studies have shown that MSC-EV treatment could promote ESC proliferation and migration, possibly reversing ESC fibrosis and repairing IUA.34–36 In in vivo experiments, Zhang et al. 37 demonstrated that the transplantation of menstrual blood-derived stem cells (MenSCs)-sEVs promoted the regeneration of endometrial glands and blood vessels in IUA rats, safely and effectively improving fertility.
In addition, Zhao et al. 38 revealed that adipose-derived mesenchymal stem cell (AMSC)-Exos could improve endometrial receptiveness by promoting collagen remodeling, endometrial regeneration, and expressions of integrin-9, leukemia inhibitory factor, and vascular endothelial growth factor (VEGF). 38 Moreover, Yao et al. 39 found that bone mesenchymal stem cell (BMSC)-Exos significantly increased the number of endometrial glands with increasing treatment time in IUA rabbits.
Recently, a study highlighted the different efficacy of MSC-EVs subpopulations in IUA treatment. They isolated two subgroups of EVs (EV20K and EV110K) by two centrifugation speeds (20,000 and 110,000 g), and found that EV20K is more cost-effective and feasible for preventing IUA, 40 emphasizing that effective EVs subpopulations are needed for obtaining optimal therapeutic outcomes.
MSC-EVs exert biological functions through various components, including miRNAs. Li et al. 34 found that umbilical cord mesenchymal stem cell (UCMSC)-Exos ameliorate transforming growth factor β1-induced endometrial fibrosis through the miR-145-5p/ZEB2 axis. In addition, exosomal miR-223-3p delivered by BMSCs could ameliorate lipopolysaccharide (LPS)-induced acute uterine injury by interacting with endothelial progenitor cells. 41 Furthermore, AMSC-Exos may alleviate endometrial fibrosis through lncRNA-MIAT, regulated by miR-150-5p. 42
miR-29a and miR-340 are also involved in effectively attenuating endometrial fibrosis and preventing IUA.35,36 These studies suggest a link between IUA and Exo-miRNAs, although the exact mechanisms need to be elucidated to achieve optimized RNA cargo for IUA therapy. Further understanding of EV-miRNAs will likely lead to the development of next-generation targeted therapies in tissue engineering and regenerative medicine using modified/engineered EVs.
EVs were recently found to be better retained and released in uterine when combined with biomaterials. Xin et al. 43 designed a construct of exosome-laden scaffold (CS/Exos) in a rat endometrium-damage model, and found that the transplantation of CS/Exos potently induced endometrium regeneration, collagen remodeling, and fertility restoration. They later discovered that the injection of an AB-laden hyaluronic acid hydrogel (HAH) promoted endometrial regeneration and fertility restoration in murine acute endometrial damage-induced IUA models. 44
Overall, MSC-EVs may serve as a clinically feasible and novel therapy for treating IUA by remodeling collagen, increasing proliferation and vascularization, reversing endometrial fibrosis, exerting immunomodulatory effects, and enhancing endometrial receptivity. However, the following issues should be considered in future IUA studies.
Establishing an ideal animal model is the basis for studying IUA. Chemical injury (such as ethanol injection), mechanical injury, and infective methods (LPS) are typically used to establish IUA models 45 ; not all can fully simulate clinical IUA. Induction of IUA with chemical reagents has good consistency and reproducibility, but is contrary to clinical practice.
Dilation, curettage, and thermal injury are similar to iatrogenic endometrial injury; however, endometria tend to regenerate and repair rapidly in experiment animals, making establishing a long-term model difficult. 46 Thus, we recommend combining mechanical damage with an infective method to induce long-term IUA, since inflammation and infection are major causes of IUA. Besides, biological indicators, including collagen remodel, angiogenesis, gland regeneration, endometrial receptivity, and fertility, should be measured.
Research has identified specific therapeutic miRNAs enriched in EVs. These are small, light, easily transfected, remain stable when encapsulated in EVs, and remain functionally intact in recipient cells. 47 Thus, IUA therapies may benefit from enriching/loading these miRNAs in EVs.
A major problem affecting the clinical application of MSC-EV-Ts is that EVs have a short half-life and are easily cleared by host cells. Fortunately, the combination of biomaterials with MSC-EVs has increased retention and engraftment of MSC-EVs. HAH and CS are commonly used biomaterials in IUA treatment. CS, a natural biomaterial matrix, can provide a three-dimensional scaffold for cell proliferation, differentiation, and infiltration. 48 However, CS cannot adapt to the irregular shape of the uterine cavity. Thus, HAH injection is more convenient than CS implantation. 44 Therefore, manipulating tissue engineering biomaterials for IUA is likely to be of benefit in the future.
Premature ovarian insufficiency
POI is defined as a loss of ovarian function before the age of premature ovarian insufficiency 40. Its etiology can be genetic, chromosomal, and/or autoimmune. 49 Moreover, the increasing number of POI cases is also related to iatrogenic POI (undergoing ovarian surgery, radiotherapy, or chemotherapy). POI is characterized by reduced follicles and hormone secretion, leading to infertility. Even though up to 25% of POI patients can ovulate, only 5–10% conceive and deliver. 50 Currently, there is no effective treatment strategies to increase ovarian activity in POI patients except oocyte donation.
Oocyte development and maturation are supported and regulated by granulosa cells (GCs), which are essential components of ovarian follicles. In various studies in POI mice, MSC-EVs were able to target and be internalized into GCs, thereby recovering the disturbed estrous cycle, levels of estradiol (E2), anti-Mullerian hormone, follicle-stimulating hormone (FSH), body weight, and the number of ovarian follicles.51–55 Moreover, UCMSC-MV transplantation may recover ovarian function by inducing angiogenesis through the miR-21-5p/PI3K/AKT signaling pathway. 56
In addition, Huang et al. 55 showed that AMSC-Exos improve POI ovarian function through the SMAD signaling pathway. Other studies have also found that UCMSC-EVs protect GCs from alkylating agent-induced apoptosis and inflammation, 57 alleviate reactive oxygen species (ROS) accumulation, 58 and induce cisplatin-induced cell stress and apoptosis in vitro. 59 Notably, a study using POI mouse models compared the therapeutic effects of intravenously injected MSCs and MSC-Exos, demonstrating that both restored the estrous cycle and serum hormone levels. 60 Moreover, MSC-EVs can improve fertility without affecting the cognitive performance of POI mouse offspring. 61
However, the aforementioned studies have some limitations, such as incomplete establishment standards and observational indicators of animal models. The widely used POI animal models are classified as chemotherapy drug-induced POI, autoimmune POI, mental stress POI, and galactose (GAL) POI according to the POI etiologies. Chemotherapy drug-induced POI, such as cyclophosphamide (CTX), busulfan (BUS) and cisplatin, is the most common POI animal model because of its simple operation and short cycle, which can well simulate the postchemotherapy state of cancer patients.
However, the POI induction effect of these chemotherapy drugs varies widely depending on the treatment period and concentration, which are overlooked in most studies. A study demonstrated that CTX (120 mg/kg)/BUS (12 mg/kg) should be treated for at least >2 weeks and cisplatin (2 mg/kg) for at least >10 days to establish the most effective POI mouse model. 62 Compared with chemotherapy drug-induced POI, GAL-induced POI (200 mg/kg per day; 42 days) can better simulate the physiological aging characteristics of clinical POI patients, and can also be used for future research. 63
Autoimmune and mental stress POI models are rarely used in MSC-EV-Ts studies, thus the effect of MSC-EVs on other types of POI is still unclear. The evaluation of POI animal models should focus on fertility, histological assessment of the ovarian reserve, hormones (anti-Mullerian hormone [AMH], FSH, luteinizing hormone [LH], E2, etc.), and biomarker evaluation of GCs (Ki67, Bcl-2, Bax, caspase-3/-9, etc.).
In addition, biomaterials, including alginate, HAH, and CS, have decreased loss of stem cell transplantation in POI therapy. 64 Shin et al. used a scaffold to increase the retention of human embryonic stem cell-derived mesenchymal progenitor cells in ovary, which could effectively restore ovarian functions and female fecundity in cisplatin-induced POI. 65 The combination of biomaterials and EVs in the treatment of POI may be a less-explored but potential direction for future research.
Thin endometrium
Adequate endometrial growth is crucial for successful implantation and invasion. A thin endometrium is characterized by <6 mm thickness, 66 high-impedance blood flow of the radial arteries, poor epithelial growth, decreased VEGF secretion, and poor vascular development. 67 Clinical pregnancy and live birth rates decline as endometrial thickness decreases in both fresh and frozen embryo transfer cycles. 68 Several treatments have been used to ameliorate refractory endometrium, including hormonal manipulation by estrogen and gonadotropin-releasing hormone (GnRH) agonists, vitamin E or pentoxifylline, vasoactive measures, intrauterine infusion of growth factors, and regenerative medicine; however, the treatment of thin endometrium remains a challenge. 69
Zhang et al. 70 established a novel rat model using ethanol foam and found that human umbilical cord mesenchymal stem cell (hUMSC)-Exos treatment increased the thickness of the endometrium, number of glands, and sub-endometrial microangiogenesis, possibly improving endometrial receptivity and pregnancy rate.
Recently, genetic modification has become a major EV therapeutic strategy. Cardiotrophin-1 (CTF1) is a cytokine in the interleukin-6 family and has been identified as an important promoter of successful embryo implantation. 71 Later, Zhu et al. 72 generated CTF1-overexpressing BMSC-derived exosomes and found CTF1-modified BMSC-Exos in a hydrogel suspension could more effectively enhance angiogenesis, promote endometrial and myometrial regeneration, and improve endometrial receptivity in rat models. Genetically engineering MSC-EVs to overexpress specific molecules is a likely focus of future research.
Endometriosis
Endometriosis refers to endometrial growth outside the uterine cavity, 73 adversely affecting the functions of the ovaries, tubal structures, and uterus, resulting in infertility. 74 Its pathophysiology involves adhesion-invasion-implantation. 75
Hirakawa et al. 76 reported that the infusion of adipose tissue derived stem cells (ASCs) inhibited pro-inflammatory and pro-fibrotic cytokines and suppressed endometriosis-like lesions. Wang et al. 77 found that 120 μg/mL UCMSC-Evs inhibited the proliferation, invasion, and released contents (SF-1, ERβ, and aromatase) of ectopic stromal cells, possibly alleviating endometriosis.
However, no consensus has been reached on the positive effects of MSC-based therapies for endometriosis. A recent study highlighted that MenSCs modulated biological processes involved in angiogenesis, proliferation, cell migration, and inflammatory responses, which may favor endometriosis. 78 Another study discovered that human UCMSCs-Exos enhanced the migratory ability of endometrial glandular epithelial cells by promoting epithelial–mesenchymal transition. Hence, endometriosis may be caused by the high mobilization of MenSCs or other sources of MSCs.
Based on these controversies, the therapeutic effect of MSC-EVs on endometriosis is doubtful and requires further exploration. In addition, compared with existing drug treatments, such as GnRH agonists, progestins, and danazol, 79 MSC-EV does not have an absolute advantage in endometriosis treatment.
Polycystic ovarian syndrome
PCOS accounts for 90% of anovulatory subfertility and is characterized by hyperandrogenism, ovulatory dysfunction, polycystic ovarian morphology, and metabolic abnormalities. 80 Several evidence-based mechanisms have been proposed to explain the pathogenicity of PCOS, identifying chronic low-grade inflammation, oxidative stress, immune system overstimulation, and GC or cumulus cell (CC) dysfunction as key contributors.81,82 Current treatments for PCOS merely address symptoms, and oral contraceptive pills, the most common treatment, do not treat infertility. Therefore, new and effective treatment strategies are urgently required.
Several in vivo studies have focused on the effects of MSC-EVs in PCOS treatment. Park et al. reported that the intravenous injection of UCMSC-EV regulates androgen production in vitro in H295R cells (a human-ovarian-theca-like cell line), reverse insulin resistance, and improve infertility in letrozole (LTZ)-induced PCOS mouse model. 83 Recently they discovered that intravenous injection of MSC-EVs was more effective for serum glucose regulation, and an intraovarian injection was more effective for ovary restoration in LTZ-induced PCOS model. 84
Cao et al. 85 reported that the tail-vein injection of AMSC-Exos restored glucose homeostasis in dehydroepiandrosterone (DHEA)-induced PCOS rats by transferring miR-21-5p/Btg2 to the liver. Moreover, in vitro, AMSC-derived exosomal miR-323-3p promoted cell proliferation and inhibited apoptosis in CCs by targeting PDCD4 in PCOS. 86 In addition, Zhao et al. 87 demonstrated that UCMSC-Exos showed an anti-inflammatory effect on GCs in PCOS by inhibiting the NF-κB signaling pathway.
PCOS treatment focuses on antagonizing androgen, improving metabolic status, and restoring ovulatory fertility. Methods for inducing PCOS in animal models and the route of administration of MSC-EVs need to be further established. It is recommended to investigate androgen resistance in PCOS using a DHEA-induced PCOS model and intravenous injections. The LTZ-induced PCOS model and intraovarian injection provide a more appropriate method for examining the effect of MSC-EVs on ovarian function in PCOS. Future research should also focus on improving the ability of MSC-EVs to target the ovary.
Male Infertility and MSC-EVs
Male infertility is a rising health problem affecting ∼8–12% of couples globally. 88 It has multiple etiologies, including innate and genetic diseases, testicular torsion, erectile dysfunction (ED), varicocele, infection, testicular trauma, immunological disorders, systemic diseases, and altered lifestyle. 89 Notably, MSC-EVs, as functional cell secretions, can induce spermatogenesis and capacitation, and improve sperm glucose metabolism and adhesion.89–91
Chen et al. 92 showed that exosomes derived from cells could cross the blood–brain barrier under stroke-like conditions in vitro, indicating that the lipid surface structure makes EVs a potential drug carrier for delivering drugs into the blood–testis barrier. We summarize the evidence on the effectiveness of MSC-EV therapy for infertility in males in Table 2 and Figure 3.

MSC-EVs take part in male infertility therapy by promoting testicular and erectile function. CCSMCs, corpus cavernosum smooth muscle cells; ICP, intracavernosal pressure; MAP, mean arterial pressure; nNOS, neuronal nitric oxide synthase; OS, oxidative stress; VEGF, vascular endothelial growth factor. Color images are available online.
Effects of Mesenchymal Stem Cell-Derived Extracellular Vesicles in Different Clinical Diseases Causing Male Infertility
ADSC, adipose-derived stem cells; ICP, intracavernosal pressure; MAP, mean arterial pressure; nNOS, neuronal nitric oxide synthase; NO, nitric oxide; OFSCs, orbital fat-derived mesenchymal stem cells; SCF, stem cell factor; VEGF, vascular endothelial growth factor.
Nonobstructive azoospermia
Manifesting as the complete absence of sperm in the ejaculate, NOA causes infertility in 10% of cases, accounts for >70% of azoospermia cases, and is mainly caused by congenital factors resulting in spermatogenic failure.93,94
Sertoli cells (SCs) are the only somatic cells in the spermatogenic epithelium of epididymis, which mainly provide structural support and nutrients for spermatogenic cells to regulate spermatogenesis. Proteomic analysis of exosomes from the epididymis identified a number of proteins involved in sperm motility, acrosome reaction, prevention of premature sperm capacitation, and male infertility. 95
The key proteins and miRNAs involved in spermatogenesis-related signaling pathways in exosomes secreted by SCs can be used as diagnostic and regenerative targets for male infertility. 96 However, there are difficulties in mass production of SCs, and coupled with the problem of low exosome yield, the clinical application of SCs-derived exosome therapy is still difficult to attain. Thus, modified MSC-EVs with effective proteins and miRNAs detected in SCs-EVs may be more effective for NOA treatment.
Studies based on MSC-EVs treating NOA are still limited, although MSCs derived from various tissues (adipose tissue, bone marrow, amniotic membrane, lung, umbilical cord, and Wharton's jelly) of different species (humans, mice, rats, dogs, goats, and sheep) have shown the capability of differentiating into male germ cells in vitro, 94 demonstrating that restoring NOA with MSC transplantation is possible. Some researchers believe that MSC provides an improved somatic microenvironment (niche) with essential growth factors/cytokines for embryonic-like stem cells (a type of tissue-resident stem cell) through pancrine support and is vital in endogenous tissue-resident stem/progenitor cell proliferation/differentiation.97–99
Studies have shown that BMSC can improve the fertility of BUS-induced azoospermic mice, possibly due to the altered expression of some spermatogenesis-related miRNAs carried by exosomes, which reduce apoptosis of spermatogenic cells and enhance intercellular adhesion.100,101 Moreover, Guo et al. 102 discovered that BMSC-Exos ameliorated CTX-induced spermatogenic dysfunction by downregulating the AKT and p38MAPK/ERK signal pathways in vitro and in vivo. Adipose-derived stem cell (ADSC)-Exos has demonstrated promoting spermatogenic cell proliferation and migration through inhibiting their apoptosis by activating PI3K/AKT and MAPK/ERK1/2 pathways. 103
To sum up, although these studies have found MSC-EVs capable of treating NOA, more research is needed to clarify the cargoes carried by MSC-EVs that reverse spermatogenic failure. Given that specific miRNAs and proteins in SCs-EVs are effective factors, engineered MSC-EVs packaging these cargos seems to be a novel therapeutic choice for NOA.
Testicular torsion
Testicular torsion, also called spermatic cord torsion, is caused by a sudden force or violent shock, resulting in testicular and spermatic cords twisting to a certain extent.
When microvascular blood flow changes, pro-inflammatory cytokines are released, and large amounts of ROS are produced, causing surgical detorsion-induced ischemia-reperfusion injury. 104 Excessive ROS can damage sperm function by reducing motility, causing DNA fragmentation, morphological defects, and apoptosis, leading to male infertility and unsuccessful pregnancy outcomes.105–107
Evidence that MSC-EVs reduce ROS is already seen in various cell types.108–112 Local injection of human orbital fat-derived mesenchymal stem cell (OFSC)-stem cell factor (SCF) has been found to protect testicular torsion-induced germ cell injury with a reduction of ROS, which is likely caused by paracrine support. 90 In addition, ADSC-EVs can reduce ROS and promote spermatogenesis in a rat model, indicating its potential in treating testicular torsion. 103
Besides alleviating ROS-induced sperm damage, injection of human OFSC-SCF can activate the Akt/GSK3 axis and promote glycolysis in sperm, thereby increasing ATP content and reversing sperm glycolytic imbalances, contributing to the regulation of sperm motility in a testicular torsion–detorsion rat model. 90 Moreover, ADSC-Exos has been found to inhibit inflammation and promote spermatogenesis in a rat model, indicating its potential in treating testicular torsion. 103 Finally, human orbital fat-derived MSC-SCF reportedly promote testosterone secretion in rats, showing a positive effect on testicular torsion-induced germ cell injury; however, the underlying mechanism is still unclear. 113
Overall, evidence has indicated MSC-EVs to reverse oxidative stress, reduce inflammation, improve metabolism and endocrinology (increase ATP content and testosterone secretion), and promote spermatogenesis; however, it is still unclear which components of exosomes play these roles, bringing great difficulties in clinical applications. Testicular-torsion-induced-impairment of sperm parameters has confounding mechanisms. Thus, the most specific molecules should be screened for different etiologies and packaged into engineered MSC-EVs to achieve the most efficient clinical outcomes.
Erectile dysfunction
Erection requires the cooperation of the cavernous body, blood, and nerves (penile dorsal nerve and major pelvic ganglion)—the interruption of any of these aspects can cause ED. 114 ED is characterized by fibrosis, decreased corpus cavernosum smooth muscle cell (CCSMCs) content, increased collagen amount, and decreased intracavernosal pressure (ICP) to mean arterial pressure (MAP), decreasing blood flow to the penile tissue. 115
Intracavernosal injection of MSC-EVs has shown positive effects in different ED rat models.116–118 In cavernous nerve injury rat models, Ouyang et al. 116 discovered that BMSC-Exos inhibited CCSMC apoptosis and promoted neuronal nitric oxide (NO) synthase in the corpus cavernosum. In addition, Li et al. 117 found that injection of ADSC-Exos and BMSC-Exos increased the smooth muscle-to-collagen and ICP-to-MAP ratios.
Furthermore, in bilateral internal iliac artery ligation-induced ED rat models, BMSC-Exos promoted cavernous sinus endothelial formation, NO synthases, smooth muscle-to-collagen ratio, and reduced ROS in the corpus cavernosum, probably by carrying VEGF and activating the NO/cGMP signaling pathway.
Recently, diabetes mellitus-induced ED has attracted increasing attention. In vivo studies, Zhu et al. 119 discovered that rat ADSC-Exos, containing proangiogenic and antifibrotic microRNAs, restored erectile function by promoting endothelial cell proliferation and decreasing fibrosis of the corpus cavernosum, and Huo et al. 120 found that rat BMSC-Exos suppressed PDCD4 expression and inhibited CCSMCs apoptosis.
In conclusion, ED is also a multicausal disorder, requiring multifactorial combination therapy including improved blood circulation, nerve recovery, spermatogenic disorders, and oxidative damage. Studies focused on the treatment of diabetes mellitus-induced and nerve injury related ED with MSC-EVs have shown positive effects in rodents. Notably, ED induced by different models has different etiologies and mechanisms, and more attention should be paid to the study of corresponding injury when studying the function of MSC-EVs.
Intracavernous penile injections are currently the main mode of drug delivery for ED treatment, but there are drawbacks such as increased invasiveness (injection), skill requirements, postinjection pain, and possible penile deformation after long-term injection. Thus, new modes of drug delivery (e.g., urethral injection) are needed to be further investigated for application in clinical studies.
Conclusions and Future Research Directions
This review highlights MSC-EVs as an attractive and promising opportunity to restore female and male fertility using novel cell-free therapies, especially in IUA, POI, PCOS, NOA, and ED. To date, reported results on the use of MSC-EV-Ts for infertility are optimistic, particularly regarding the role of MSC-EVs in repairing the injured endometrium, restoring ovarian function, and improving sperm quantity, morphology, and motility.
For the past decades, with the development of novel bioengineering and tissue technologies, bioengineered MSC-EVs combined with the use of therapeutic biomolecules and attractive biomaterials have opened up new avenues for advances in the treatment of infertility.
However, there is a need for improvement in preclinical studies of MSC-EV-Ts in infertility, particularly with regard to aspects such as developing standard disease models, optimizing delivery routes, and enhancing the efficacy of tissue engineering. Several challenges for the clinical application of MSC-EVs also need to be addressed, such as the lack of standardized protocols for purification and identification, convenient and affordable storage, delivery, shipping, and safety issues. In this regard, we would like to emphasize the following points:
A homogenous population of MSCs should be developed. BMSC-EVs and UCMSC-EVs are most commonly used in female infertility therapies. UCMSCs offer several biological advantages, such as low immunogenicity and higher proliferative capacity, thus we recommend UCMSC as the first choice of EV cell source for female infertility. ADSC-EVs and BMSC-EVs are the mostly used MSC-EVs in male infertility therapies due to accessibility. EVs with testicular or epididymal origin, especially those derived from SCs or Leydig cells, may be more effective novel alternatives for future research; however, mass production is still currently problematic. To date, most studies on the therapeutic activity of MSC-EVs for infertility are on collective effects of MSC-EVs. EVs consist of several different subpopulations in terms of morphology, density, and cargo. In future studies, careful isolation of specific subpopulations of EVs will be critical to obtain optimal therapeutic outcomes. Standardized disease animal models and accurate efficacy observational indicators are key to the reliability of research. Detailed opinions on specific animal models and observational indicators are given in the text. The dose, duration, and route of administration of MSC-EVs need to be detailed in future studies for better reliability and reproducibility. The route of administration should be chosen carefully. For endometrial-related infertility, intrauterine injection can be used to directly act on the endometrium. However, for ovarian-related infertility, intraovarian injection is better than intraperitoneal injection. Intravenous injections are most effective for androgen resistance and glucose homeostasis in PCOS. They are also more acceptable in testis-related infertility in animal models since testis is a hypervascular tissue. Intracavernous penile injections are mostly used in ED related infertility due to its potent effect and rapid onset of action; however, there is more invasiveness, skill requirements, postinjection pain, and possible penile deformation after long-term application. A central focus of future research should be MSC-EV cargo mechanisms and modification/engineering of EVs with therapeutic biomolecules. Current studies have identified various small, easily transfected, and stable therapeutic miRNAs enriched in MSC-EVs that are strong candidates for MSC-EV-Ts. Another focus should be developing safe methods to improve local MSC-EVs retention at sites of interest and create cell-free therapies. Notably, the combination of novel biomaterials and MSC-EVs has improved retention and provided successful sustained release of EVs, representing great hope for future MSC-EV-Ts, although safety and off-target effects still require research.
These issues need to be examined in future studies. Overall, it is anticipated that with improvement of tissue engineering technology, MSC-EV-Ts will lead to significant developments in the clinical treatment of infertility.
Footnotes
Acknowledgments
We would like to thank Figdraw (www.figdraw.com) for drawing support, and Home for Researchers (www.home-for-researchers.com) and Editage (![]() ) for language editing.
) for language editing.
Authors' Contributions
Conceptualization (lead), writing—review and editing (equal), and visualization (equal) by Y.-X.L. Writing—review and editing (equal) and visualization (equal) by S.-Q.W. Writing—review and editing (equal) by S.L. Supervision (lead) by P.-S.Z. All authors revised and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.