
Abstract
Kidney diseases are major global health problems, with high prevalence and mortality. However, current treatment strategies for kidney diseases fail to achieve satisfactory efficacy. Mesenchymal stem cell (MSC)-based therapy has been a promising strategy for treating kidney diseases. Preclinical studies have proven their safety and effectiveness in treating acute kidney injury (AKI) and chronic kidney disease (CKD), but the outcomes of clinical trials have shown very limited clinical efficacy. A variety of innovative approaches have been proposed to enhance the therapeutic potential of MSCs, and hydrogels are attractive candidates. Hydrogels are three-dimensional (3D) networks formed by hydrophilic polymers of natural or synthetic origin with diverse physical and chemical properties. They have been widely applied in the field of drug delivery and regenerative medicine, including MSC-based therapy. Many studies have proven that hydrogels can improve the therapeutic efficacy of MSCs for kidney diseases, but there are still challenges limiting the widespread application of this method. In this review, we introduce the application of MSCs in kidney diseases and the factors that influence therapeutic efficiency and focus on the beneficial effects of hydrogels in MSC-based therapy for AKI and CKD.
Impact statement
Hydrogels have been widely applied in the field of drug delivery and regenerative medicine, including mesenchymal stem cell (MSC)-based therapy. Many studies have proven that hydrogels can improve the therapeutic efficacy of MSCs for kidney diseases, but only a few articles summarized the application of hydrogels in MSC-based therapy for kidney diseases. In this review, we focus on the beneficial effects of hydrogels in MSC-based therapy for acute kidney injury and chronic kidney disease by introducing promising results in recent studies. We also discussed challenges in the clinical translation and widespread application of hydrogels in MSC-based therapy for kidney diseases.
Introduction
Acute kidney injury (AKI) is a clinical syndrome characterized by a rapid deterioration in kidney function and can be caused by multiple pathogenesis factors, 1 with an incidence rate of ∼15% in hospitalized patients. 2 Chronic kidney disease (CKD) is characterized by chronic and progressive destruction of kidney structure and function. The global prevalence rate of CKD is about 10%, causing 1.2 million deaths and 28 million life loss years every year. 3
Both AKI and CKD have high morbidity and mortality rates, leading to a huge burden of disease worldwide.4,5 However, current treatment strategies for AKI and CKD fail to achieve satisfactory efficacy and improve the prognosis of patients, especially for CKD.4,6 Except for kidney transplantation, other therapeutic strategies cannot improve the prognosis of patients with end-stage renal disease. 7 Renal replacement therapy and kidney transplantation also have limitations, and improved methods for better treatment have been proposed.
A clinical trial revealed that novel medium-cut-off dialyzers could reduce proinflammatory mediators, endothelial vascular endothelial growth factor production, and angiogenesis compared with current high-flux hemodialyzers. 8 Catar et al. discovered that high expression of CXC chemokine ligand 1 is associated with unfavorable tissue remodeling of peritoneal membrane during peritoneal dialysis (PD), providing a novel target to prolong PD therapy. 9
A phase I/II a clinical trial suggested that infusion of autologous natural regulatory T cells in patients after kidney transplantation can achieve stable monotherapy immunosuppression without serious adverse events. 10 These novel research findings will contribute to the improvement of dialysis treatment and kidney transplantation. Here, we focused on innovative methods in cell-based therapy for kidney diseases.
Mesenchymal stem cells (MSCs) are multipotent adult stem cells with the ability of self-renewal and multilineage differentiation. 11 The MSC acronym can stand for mesenchymal stem cell or mesenchymal stromal cell. The former is rarer and refers to a stem cell population with functionality of self-renewal and differentiation that must be proven by functional assays.12,13 They are similar in some aspects and share some similar cell surface markers.
The interchangeable use of MSCs as mesenchymal stem cells or mesenchymal stromal cells has propagated and it is hard to distinguish. 12 In this review, we defined MSCs as mesenchymal stromal/stem cells. The MSCs are considered one of the most promising strategies for treating kidney diseases, and a number of preclinical studies have proven their safety and effectiveness in treating AKI and CKD.14,15
However, when applied to patients with AKI or CKD in clinical trials, MSC-based therapy showed safety but very limited efficacy.16,17 The impaired clinical efficacy of MSCs can be attributed to low renal retention rate, poor survival rate, and other reasons. 17 To improve the clinical efficacy of MSC-based therapy for kidney diseases, scientists have proposed innovative strategies, including preconditioning and genetic modifications of MSCs, using MSC-derived exosomes and employing bioengineered hydrogels as delivery systems.18–20
Among them, hydrogel is an attractive candidate. It can provide mechanical support for cells, mimic the characteristics of extracellular matrix (ECM), and can be engineered as an injectable hydrogel.21,22 Due to these advantages, hydrogels have been widely used in regenerative medicine23,24 and are promising for kidney disease treatment.
In this review, we introduce the application of MSCs in kidney disease and factors influencing their therapeutic efficiency. Then, we focus on the beneficial effects of hydrogels in MSC-based therapy for AKI and CKD by introducing promising results in recent studies. Finally, we discuss challenges in the clinical translation and widespread application of hydrogels in MSC-based therapy.
MSCs and Kidney Diseases
Mesenchymal stem cells
The MSCs are multipotent adult stem cells that can be isolated from many tissues, including bone marrow, fat tissue, and perinatal tissue such as umbilical cord. Bone marrow, adipose tissue, and umbilical cord tissue-derived MSCs can be abbreviated as BM-MSCs, AT-MSCs and UC-MSCs, respectively. 13 BM-MSCs are predominant in the cell-based therapies but MSCs derived from other tissues including AT-MSCs and UC-MSCs have entered clinical investigation in recent years. 25
Their biological features, such as proliferation, differentiation and paracrine effects, are slightly different depending on the sources. 26 The MSCs can self-renew by dividing and differentiating into multiple cells from all three dermal lineages, including osteocytes, adipocytes, neurocytes, and hepatocytes.11,27 They can also secrete a variety of cytokines, chemokines, and extracellular vesicles to exert therapeutic effects. 28 Therefore, they have been one of the most promising candidates in tissue engineering because of their abundant secretion profile, low immunogenicity, huge therapeutic potential, and productive harvest.29,30
A considerable number of studies have investigated and proven the therapeutic potential of MSCs for various diseases, including cancer, 31 cardiovascular disease,32,33 bone and cartilage disease,34,35 inflammatory disease,36,37 neurological diseases, 38 and kidney disease.39,40
MSC-based therapy for kidney diseases
The pathophysiological mechanisms of AKI and CKD are complex, involving ischemia-reperfusion injury, inflammation, fibrosis, mitochondrial dysfunction, and oxidative stress.41,42 The exact mechanism of how MSCs provide renal protective effect is still ambiguous, but paracrine effects are considered the main mechanism.16,43
Administered MSCs can be distributed to injured tissues and secrete a variety of cytokines, chemokines, and extracellular vesicles to interact with other cells at the injured site, exerting anti-apoptosis, anti-inflammatory, anti-fibrotic, immunoregulator, antioxidant, and pro-angiogenic effects.43,44
Many animal studies have revealed the reno-protective effects of MSCs and MSC-derived extracellular vesicles (MSC-EVs) on different kinds of renal disorders. 45
MSC-based therapy for AKI
In animal models of AKI, MSCs can effectively ameliorate kidney injury and accelerate repair. The MSCs engraftment reduced the serum concentrations of creatinine and urea nitrogen, alleviated renal tubular necrosis, and promoted vascularization in ischemia/reperfusion-induced AKI (I/R-induced AKI) models.39,46 The MSC-EVs could inhibit hypoxia/reoxygenation-induced apoptosis in HK-2 cells and alleviate kidney injury induced by I/R in vivo. 47
Micro-RNAs play important roles in the protective effect of MSC-Evs by regulating the expression of target genes.47,48 In sepsis-induced acute kidney injury (SI-AKI), administration of BM-MSCs alleviated kidney injury by promoting mitophagy and inhibiting apoptosis and pyroptosis of renal tubular epithelial cells. 49 The EVs deprived from AT-MSCs could also mitigate kidney injury by enhancing autophagy and suppressing inflammation in SI-AKI rats. 50 In rhabdomyolysis-induced AKI (RM-induced AKI), BM-MSCs could ameliorate kidney injury via the activation of M2 macrophages. 51
In cisplatin-induced AKI, UC-MSCs could ameliorate early AKI and inhibit later renal interstitial fibrosis. 52 Pretreatment with UC-MSC derived EVs prevented cisplatin-induced AKI by enhanced autophagy. 53 Similar renal-protective effects can be observed in other toxicant-induced kidney injury.54,55
MSC-based therapy for CKD
The MSC therapy also showed efficacy in animal models of CKD. In rat and mouse models of diabetic nephropathy (DN), systematic administration of MSCs could slow the progression of DN, reduce proteinuria and serum creatinine, preserve residual renal function, and alleviate pathological injuries.56,57 The MSC treatment even ameliorated renal pathological changes in DN in a primate model of rhesus macaques. 58 Multiple injections of MSC-EVs improved renal function and histological outcomes of renal tissues by upregulating autophagy in the model of DN rats. 59
A meta-analysis revealed that MSCs treatment more effectively improved kidney function compared with cell products, and bone marrow is a better tissue source of MSCs for improvement of kidney function and proteinuria. 60 The role of MSCs in lupus nephritis has also been widely studied because of their immunomodulatory and anti-inflammatory properties.
In animal models of lupus nephritis, MSCs treatment improved kidney function and kidney pathological damage.61,62 In patients with lupus nephritis, MSCs treatment was safe and well tolerated. They can improve kidney function, decrease serologic markers, BILAG score, and recurrence rate. 63 They can improve kidney function, reduce tubulointerstitial fibrosis and inflammation, and increase expression of angiogenic markers in CKD mouse models.64–66
Although preclinical studies have shown the enormous therapeutic potential of MSCs in kidney diseases, the preliminary results from clinical studies cannot adequately demonstrate their reno-protective effects. Most of the clinical trials are in phase I or phase II and only a handful of these studies reached completed status and reported the results.16,67
A single-arm phase I clinical trial administered autologous MSCs isolated from bone marrow into patients with autosomal dominant polycystic kidney disease. During 12 months of follow-up, no serious adverse events were observed, but no improvement in the estimated glomerular rate was observed (p = 0.09). 68 There have been reports of adverse events with systemic intravascular infusion in some clinical trials. Thrombotic events are most common adverse events in systemic intravascular infusion of MSCs. 25
The MSCs express procoagulant tissue factor TF/CD142 on their surface, which can trigger the instant blood-mediated inflammatory reaction and clotting thrombus formation after intravascular administration. 69 This procoagulant activity depends on the tissue sources, cell-passage number, cell dose, and cell preservation methods.25,70–72
Early passage MSCs and MSCs obtained from bone marrow have a lower risk of adverse thrombotic events. 71 Compared with fresh MSCs, freeze-thawed MSCs have impaired immunomodulatory and blood regulatory properties.70,73 These evidences demonstrated that the translation of preclinical studies into clinical applications remains difficult.
Reasons for unsatisfactory clinical efficacy and improvement strategies
The beneficial effects of MSC-based therapy on kidney diseases can be constrained by a variety of factors. Low survival rate of MSCs and low MSCs distribution in kidney following systematic administration are suspected to be the main causes.74,75 It was demonstrated that only less than 1% of intravenously injected MSCs could distribute to the injured kidneys 1 h after injection and disappeared in the next few days. 76
Moreover, the microenvironment is a major contributing factor to the inefficacy of MSCs. A meta-analysis revealed that uncontrolled glycemic levels in diabetic patients impeded the therapeutic efficacy of MSCs. 77 Harmful microenvironment in injured kidneys is complex with diverse cytotoxic factors, such as inflammatory cytokines and oxidative stress, thus impairing the function of MSCs and finally minimizing their therapeutic efficacy. 78 The dosing and timing of MSCs treatment is another issue influencing the clinical outcomes.
It is believed that the therapeutic efficacy and potency of MSCs are dependent on the dosage. In animal models, a single dosing of MSCs is usually enough to exert protective effect in most diseases, while large and multiple dosages were required to induce the clinical improvement in some diseases. 79 In animal models of DN, compared with intervention on the advanced stage of nephropathy, early intervention by MSCs showed superior therapeutic efficacy. 80
Consequently, exploring suitable dosage and timing for MSCs administration is essential to guarantee the therapeutic efficacy of MSCs. The MSCs are a population of cells with high heterogeneity. They exhibit varied phenotypic, functional and secretory behavior both in vivo and in vitro, depending on tissue sources, culture conditions, and production process.12,26
As a result, it is hard to provide consistent and stable therapeutic effects in clinical trials. As discussed earlier, different culture conditions and tissue sources of MSCs can also influence the treatment outcomes.
Researchers have proposed a variety of innovative approaches to increase the therapeutic potential of MSCs, such as pretreatment of MSCs with growth factors, cytokines, and chemicals, genetic modifications of MSCs, using MSC-derived exosomes, and employing bioengineered hydrogels as delivery systems.19,81–83 These strategies can enhance the survival rate, bioactivity, and renal-protective effects of MSCs.
Considering the risk of thrombotic events with intravascular infusion of MSCs, localized biomaterial-assisted delivery should be preferred to increase safety and efficacy in treatment of kidney diseases. Here, we focus on the application of hydrogels.
Application of Hydrogels in Kidney Diseases
Hydrogels are 3D networks formed by hydrophilic polymers of natural or synthetic origin, holding diverse physical and chemical properties. The chemical or physical cross-linking of these hydrophilic polymer chains can maintain the stable structure of hydrogels when embedded in a water-rich environment.84,85 They have been applied in a wide range of fields since their discovery, and enthusiasm over this technology has been evident over the past 60 years. 23
The development of advanced cross-linking techniques and fabrication strategies has significantly enhanced the physicochemical properties and capabilities of hydrogels. 86 Advanced hydrogels such as self-healing, responsive, injectable, and interpenetrating network hydrogels have been developed and widely applied in drug delivery and tissue regeneration.86,87 In the field of regenerative medicine, hydrogels have also been extensively investigated, especially in skeletal and cardiovascular diseases.24,88
Types and advantages of hydrogels applied in MSC-based therapy
According to the source and composition of polymers, hydrogels can be classified as natural, synthetic, and hybrid types. 84 Among them, synthetic and hybrid hydrogels are most frequently utilized in MSC-based therapies for kidney diseases due to their greater mechanical strength, longer service life, higher water absorption capacity, and wide variety of resources.89,90
Hydrogels are an ideal choice for MSC-based therapies for kidney diseases because of their unique properties. First, hydrogels designed to encapsulate MSCs or MSC-EVs are safe for humans with good biocompatibility and biodegradability. 21 Animal experiments have demonstrated that well-designed hydrogels do not elicit any undesirable local or systemic side effects. 91
Second, hydrogels can serve as scaffolds that provide mechanical support, controlled bioactive molecule and cells delivery to the target tissues, and protection from harmful inflammatory microenvironment. Third, they can preserve the phenotype and properties of MSCs at the same time. 83 Some advanced hydrogels can mimic the physical and biochemical characteristics of the ECM, thus providing a moist environment for MSCs and mediating cell function processes such as proliferation, migration, and receptor–ligand binding events.21,92
Fourth, the porous structure of hydrogels also enables exchange of nutrients, waste products, and signaling molecules between cells embedded in the hydrogels and tissue outside the hydrogels. 93 In addition, injectable hydrogels can be administered in minimally invasive methods such as intravenous injection, which is simple, efficient, and convenient for multiple administrations. 94
The biophysical and biochemical properties of hydrogels are highly tunable by modifying parameters such as crosslinking density and polymer concentration or by adding bioactive molecules. Consequently, hydrogels hold versatile biomedical application possibilities and potentials. 95
Hydrogel encapsulation of MSCs and MSC-EVs for kidney diseases
Strategies to prepare complex hydrogels for MSC-based therapy
Simple hydrogels synthesized with a single component, including hyaluronic acid and chitosan, usually have good biocompatibility and degradability.96,97 However, their physicochemical properties and biological activities are often constrained and unable to meet specific application requirements. 98 With the development of biomedical materials, advanced hydrogels constituting more than one type of polymeric material have been investigated.
One of the most common strategies to prepare complex hydrogels is introducing peptides or bioactive components. C domain peptide of insulin-like growth factor-1 (IGF-1C) is a 12 amino-acid peptide identified as the active region of IGF-1 protein. Researchers linked IGF-1C into a chitosan-based hydrogel, and the results revealed that this functionalized hydrogel further increased MSCs viability and alleviated kidney injury compared with no hydrogel or chitosan hydrogel only. 83
The same beneficial effect was observed in an self-assembling peptide hydrogel made of D-amino acids. 99 RGD (Arg-Gly-Asp) peptides have strong binding affinity to integrins on the membrane surfaces of EVs and have gained attention for promoting the therapeutic efficacy of MSC-EVs. 100 Recent studies have demonstrated that RGD-modified hydrogels can facilitate the renal tubular cell endocytosis of EVs and provide superior protective effects in I/R-induced AKI.101,102 In addition, the loading of α-lipoic acid, a ROS scavenger and antioxidant agent, is effective in attenuating kidney injury in cisplatin-induced AKI. 103
Self-assembling peptide-based hydrogels (SAPHs), a kind of peptide hydrogel crosslinked by reversible physical interactions, are widely used in MSC-based therapy for kidney diseases as well. They can better mimic the architecture and properties of the ECM and usually have excellent biocompatibility and responsiveness to external stimuli.104,105
Zhou et al. designed a matrix metalloproteinase-2 (MMP2)-sensitive SAPH by inserting an MMP2-cleavable motif. Thus, the degradation of hydrogels and release of MSC-EVs could be controlled by MMP. 106 Drzeniek et al. introduced a bio-instructive collagen-hyaluronic acid hydrogel (COL-HA) for the encapsulation of MSCs.
Compared with MSCs cultured in cell culture dishes or encapsulated in standard gelatin-hyaluronic acid (Gel-HA) hydrogels, MSCs encapsulated in this COL-HA showed a significant expansion of secretory profiles. Further, they used thiol-modified glycoproteins to functionalize the COL-HA, which further enhanced the paracrine potency of MSCs. 107
These hydrogels used for the delivery of MSCs/MSC-EVs displayed satisfactory biocompatibility and biodegradability without significant local and systemic inflammatory response.
Cell experiments applying hydrogels in MSC-based therapies for AKI and CKD
The MSCs were the most common components loaded in hydrogels, while MSC-EVs are less frequently used.101,106 Endothelial progenitor cells (EPCs) and embryonic stem cells loaded hydrogels have also been studied. According to in vitro experiments, co-culturing MSCs with hydrogels could promote the proliferation and secretion of MSCs while reducing their apoptosis and oxidative stress.
In addition, an integrin receptor-binding nanofibrous peptide hydrogel developed by Najaf et al. could enhance the spreading and attachment of MSCs in vitro. 102 Zhang et al. demonstrated that RGD hydrogels can facilitate HK-2 cell endocytosis of MSC-EVs. 101 Under harmful stimulation (stimulated with hypoxia-reoxygenation or tumor necrosis factor-alpha), MSCs and MSC-EVs loaded hydrogels reduced the inflammation and apoptosis of HK-2 cells.106,108
Animal experiments applying hydrogels in MSC-based therapies for AKI and CKD
Table 1 and Figure 1 summarize the studies applying hydrogels in MSC-based therapies for AKI and CKD. These studies varied in terms of source of MSCs/MSC-EVs, route of administration, model of kidney diseases, and type of hydrogels.
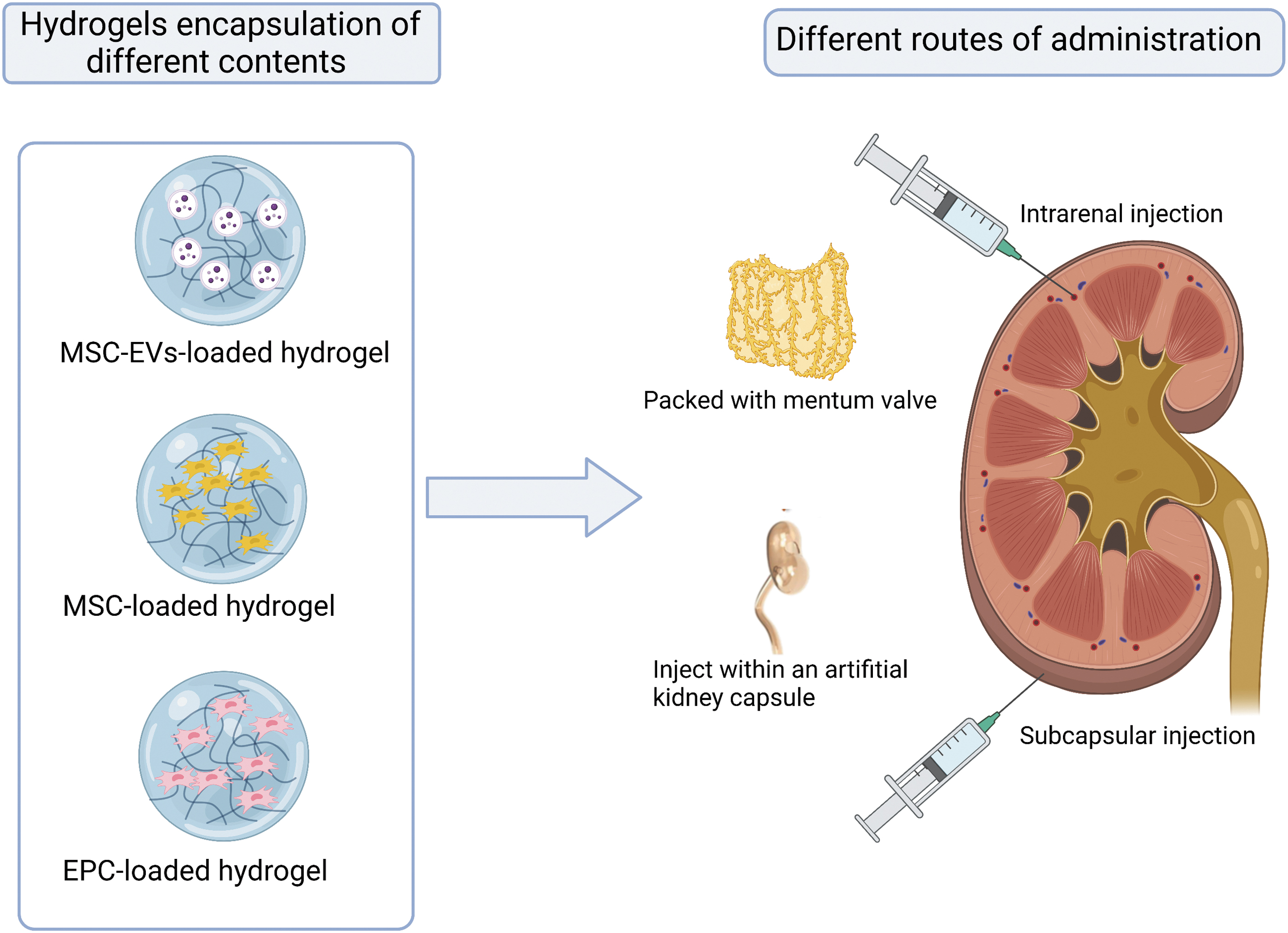
Diagrammatic summary of the application of hydrogels in kidney diseases. EPC, endothelial progenitor cell; MSC-EV, mesenchymal stem cell-derived extracellular vesicle.
Summary of Studies Applying Hydrogels in Mesenchymal Stem Cells-Based Therapies for Acute Kidney Injury and Chronic Kidney Disease
γ-PGA, Poly-γ-glutamic acid; AD-MSCs, adipose-derived mesenchymal stem cells; AKI, acute kidney injury; BM-MSCs, bone marrow-derived mesenchymal stem cells; CKD, chronic kidney disease; CS, chitosan; dECM, decellularized extracellular matrix; ECM, extracellular matrix; EPCs, endothelial progenitor cells; ESCs, embryonic stem cells; EVs, extracellular vesicles; Fmoc-FF, Fmoc-diphenylalanine; HA, hyaluronic acid; HUVECs, Human umbilical vein endothelial cells; IGF-1C, C domain of insulin-like growth factor-1; I/R-induced acute kidney injury, ischemia/reperfusion-induced acute kidney injury; MMP2, matrix metalloproteinase-2; MSCs, mesenchymal stem cells; P-MSCs, placenta-derived mesenchymal stem cells; RGD, Arg-Gly-Asp; RM-induced AKI, rhabdomyolysis-induced acute kidney injury; ROS, reactive oxygen species; Sepsis-induced AKI, sepsis-induced acute kidney injury; TGF-β, tumour growth factor β; TNF-α, tumour necrosis factor-α; SAP, self-assembling peptide; SNAP, S-nitroso-N-acetyl penicillamine; UUO, unilateral ureteral obstruction; WJ-MSCs, Wharton's jelly-mesenchymal stem cells.
Sources of MSCs included bone marrow, adipose tissue, umbilical cord tissue, and Wharton's jelly, and BM-MSCs were the most widely used type. All these studies used rats as experimental animals and the majority of MSCs were also obtained from mice. Except for mouse, human and rabbit MSCs were also employed and did not cause serious adverse events associated with immune rejection, indicating the low immunogenicity of MSCs.101,109
Most studies administered MSC-laden hydrogels by intrarenal injection and only a few studies adopted other routes. To reduce the diffusion and increase the renal retention of MSCs, Fu et al. constructed an artificial kidney capsule made of Ecoflex via 3D printing so that it could wrap the kidney and immobilize MSC-laden gelatin hydrogel. 110
Considering the significance of pedicled greater omentum valve in tissue repairing, Geng et al. utilized pedicled greater omentum valve to wrap MSC-loaded gelatin hydrogels and then packed them onto the 5/6 nephrectomized kidneys. 108 The role of hydrogels in enhancing the renal-protective effects of MSCs and MSC-EVs was investigated in a variety of experimental models of kidney injury.
The majority of studies concentrated on AKI and I/R-induced AKI was the most commonly used animal model. SI-AKI, RM-induced AKI, and cisplatin-induced AKI models were also investigated. However, studies exploring the effects of hydrogels on MSC-based therapy in CKD ware very limited. 108
All of these approaches were effective in boosting therapeutic potency of MSCs and MSC-EVs in AKI and CKD. Except for MSCs, EPCs embedded in hydrogel could alleviate renal injury, improve renal injury, and improve renal function in I/R-induced AKI and SI-AKI.111,112 Ratliff et al. even explored the renal-protective effects of stem cells by coembedding EPCs with renal MSCs in a hyaluronic acid hydrogel. However, the results indicated no improvement in therapeutic efficacy compared with EPCs alone, but enhanced the therapeutic effects of stem cells without hydrogels. 97
Compared with MSCs or MSC-EVs alone, coadministration with hydrogels could promote the survival and proliferation of MSCs and prolong MSCs retention in the kidney, thus facilitating the renal-protective effects of MSCs and MSC-EVs. However, differences existed in the extent of renal function improvement. This might be attributed to different dosages and approaches of administration, types of hydrogels, and models of kidney diseases.
Mechanisms underlying the beneficial effects of hydrogels in MSC-based therapy for kidney disease
Hydrogels alone have very limited renal-protective effects, so how can they enhance the therapeutic effect of MSCs or MSCs-EVs? Although the detailed mechanisms remain unclear, several important roles of hydrogels have been proven and acknowledged.
By labeling MSCs with fluorescence and employing an in vivo imaging system, the distribution of MSCs after transplantation can be tracked. According to results from these studies, most MSCs are trapped by the lung and liver after intravenous administration and local injection also cannot avoid the distribution of MSCs.74,113 In addition, the severe microenvironment of injured kidneys may cause significant apoptosis and poor viability of MSCs without the support of ECM because of anoikis.78,114
These obstacles have limited the therapeutic benefits and successful application of MSCs. When MSCs were transplanted with hydrogels, the number of cells trapped in the lungs and livers was markedly decreased. With the help of hydrogels, more MSCs were maintained at the injection site and preserved for longer time.96,113 This is because hydrogels can mimic stem cell niches and provide a mechanical barrier, thus increasing cell adhesion and reducing cell apoptosis caused by anoikis.114,115
In addition to hydrogels composed of a single component of ECM, entire ECM components have also been investigated and can better mimic the native stem cell niches. Zhou et al. utilized kidney ECM hydrogel to deliver MSCs into ischemic kidneys. Results showed that kidney ECM hydrogel could remarkably enhance the retention and survival rate of transplanted MSCs in kidneys and therefore improve the therapeutic effect. 113
In addition, an in vitro experiment co-culturing MSCs with ECM hydrogel revealed that ECM hydrogel could promote the secretion of growth factors and EVs from MSCs. 113 Since MSCs exert their role mainly through the secretion of multiple cytokines and EVs, this effect can obviously enhance therapeutic potential of MSCs. Co-delivering MSCs with hydrogel can also reduce oxidative stress and promote the proliferation, migration, and differentiation of MSCs.102,109
In conclusion, hydrogels showed no obvious reno-protective effects, but they can play beneficial effects on MSCs. These effects are influenced by physical and chemical properties of hydrogels such as biodegradability, stiffness, and morphology. 116 Therefore, the interactions between them are complicated and remain unclear. For better applications of hydrogels in cell-based therapy, further researches are needed to determine how hydrogels regulate the fate of MSCs.
Challenges of MSC-Laden Hydrogel Strategies for Kidney Diseases
Researchers have explored a variety of approaches to enhance the therapeutic efficacy of MSCs in kidney diseases and delivering MSCs/MSC-EVs with hydrogels is an attractive method.20,81 The beneficial effects of hydrogels on MSCs/MSC-EVs have been proven by intense research but there are still drawbacks limiting the widespread application of this method.
Most of the previous studies have concentrated on AKI and there is a lack of valuable investigations on CKD. Only a small number of studies have investigated the therapeutic efficacy of MSCs combined with hydrogels in CKD. 108 A possible reason is that more than one dosage of MSCs is required to exert renal-productive effects in the animal model of CKD, but frequent intrarenal injections are inconvenient and may cause kidney injury. Therefore, it remains unknown whether hydrogels can increase the therapeutic effectiveness of MSCs in CKD.
To achieve success in hydrogel-based therapies, the attainment of a homogenous population of MSCs is necessary. Except for positive and negative markers of MSCs, the ISCT MSC committee has proposed recommendations to further characterize MSCs, emphasizing the description of three key aspects: (1) the tissue source origin of MSCs; (2) the stemness that is supported by both in vitro and in vivo data; and (3) the functional assays to demonstrate properties of MSCs in alignment with their intended therapeutic mechanisms.
Consequently, fundamental assays for MSC-based products encompass a range of critical evaluations, including donor screening, viability assessment, purity determination, safety analysis, identity verification, and potency measurements. 12
With the rapid progress in biomedical materials, increasingly advanced and hybrid hydrogels are being applied to MSC-based therapy with more flexible properties and better efficacy than simple ones.99,102 However, the manufacturing of advanced hydrogels is complex and the cost is relatively high, which may hinder the broad application and clinical translation of more complex hydrogel-based constructs.
Although the coadministration of MSCs and hydrogels is more effective than intravenous delivery or local injection with MSCs alone, the precise mechanism is not fully elucidated. In addition, current investigations have only revealed the beneficial effects of hydrogels on MSC-based therapy for kidney diseases in animal models. There is a lack of clinical trials to determine whether hydrogels can improve the therapeutic effectiveness of MSCs in patients with AKI or CKD as well.
Conclusions
In conclusion, hydrogel remains a promising approach to improve the therapeutic potency of MSCs because of its superior properties. Many advanced hydrogels have been engineered to encapsulate MSCs/MSC-EVs for the treatment of kidney diseases and exhibit encouraging results. Future research should explore the underlying mechanism and assess the effect of MSC-laden hydrogels in CKD models to facilitate the widespread application and clinical translation of hydrogel delivery systems of MSCs and MSC-EVs in the treatment of kidney diseases.
Footnotes
Authors' Contributions
J.P. and T.H.Y. conceived and designed the work, wrote the manuscript, and were major contributors in writing the manuscript. S.S.C., N.Y.Y., and X.Y.L. assisted in the acquisition and analysis of related studies. B.H.S. and R.X.L. offered instructions, revised and edited the draft. All authors read and approved the final manuscript and the publication in Stem Cell Research and Therapy.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially sponsored by: the National Natural Science Foundation of China (Grant No.82000702), the State Key Research Programme of China (Grant No.2016YFC1103004), the 1.3.5 project for disciplines of excellence from West China Hospital of Sichuan University (Grant No. ZYJC21010), and Med+ Biomaterial Institute of West China Hospital/West China School of Medicine of Sichuan University (Grant No. ZYME20001).