
Abstract
Rotator cuff tear (RCT) is the most common cause of disability in the upper extremity. It results in 4.5 million physician visits in the United States every year and is the most common etiology of shoulder conditions evaluated by orthopedic surgeons. Over 460,000 RCT repair surgeries are performed in the United States annually. Rotator cuff (RC) retear and failure to heal remain significant postoperative complications. Literature suggests that the retear rates can range from 29.5% to as high as 94%. Weakened and irregular enthesis regeneration is a crucial factor in postsurgical failure. Although commercially available RC repair grafts have been introduced to augment RC enthesis repair, they have been associated with mixed clinical outcomes. These grafts lack appropriate biological cues such as stem cells and signaling molecules at the bone–tendon interface. In addition, they do little to prevent fibrovascular scar tissue formation, which causes the RC to be susceptible to retear. Advances in tissue engineering have demonstrated that mesenchymal stem cells (MSCs) and growth factors (GFs) enhance RC enthesis regeneration in animal models. These models show that delivering MSCs and GFs to the site of RCT enhances native enthesis repair and leads to greater mechanical strength. In addition, these models demonstrate that MSCs and GFs may be delivered through a variety of methods including direct injection, saturation of repair materials, and loaded microspheres. Grafts that incorporate MSCs and GFs enhance anti-inflammation, osteogenesis, angiogenesis, and chondrogenesis in the RC repair process. It is crucial that the techniques that have shown success in animal models are incorporated into the clinical setting. A gap currently exists between the promising biological factors that have been investigated in animal models and the RC repair grafts that can be used in the clinical setting. Future RC repair grafts must allow for stable implantation and fixation, be compatible with current arthroscopic techniques, and have the capability to deliver MSCs and/or GFs.
Impact statement
This review makes the case that a gap exists between the promising tissue engineering modalities for rotator cuff (RC) repair that have been tested in animal models and the current commercially available RC grafts that are used in the clinical setting. It identifies both the current techniques being used to enhance RC repair and the needed advancements required for these techniques to have clinical application. Future RC grafts must incorporate biological factors such as mesenchymal stem cells and growth factors while also being compatible with arthroscopic surgical procedures to improve RC healing in the clinical setting.
Introduction
Rotator cuff tear (RCT) is the most common cause of disability in the upper extremity. 1 It results in 4.5 million physician visits in the United States every year and is the most common etiology of shoulder conditions evaluated by orthopedic surgeons.2,3 In the primary care setting, shoulder pain is the third most common musculoskeletal presentation, with RCT treatment serving as a significant economic burden on the U.S. health care system.4,5 Over 460,000 rotator cuff (RC) repair surgeries are performed in the United States annually. 6 Successful RC repair results in an average improvement of 0.62 quality-adjusted life years (QALYs) and lifetime societal savings of $3.44 billion. 7
The RC is composed of four muscles and their tendons: supraspinatus, infraspinatus, teres minor, and subscapularis. 8 The RC stabilizes the glenohumeral joint and allows for abduction, internal rotation, and external rotation of the humerus. 9 The tendons of supraspinatus, infraspinatus, and teres minor insert onto the greater tuberosity of the humerus, whereas the tendon of subscapularis inserts onto the lesser tuberosity of the humerus.8,10 These insertions are referred to as entheses and are characterized by four zones spanning from muscle to osseous attachment: tendon, nonmineralized cartilage, mineralized cartilage, and bone (Fig. 1).11–13 Collagen is an important component of enthesis extracellular matrix. During the skeletal maturation process RC entheses comprises collagen types I, III, VI, IX, and XI. 14 Eventually, mature RC entheses predominantly expresses collagen types I, II, and X. 15

Four zones of the RC enthesis. Created with BioRender.com. RC, rotator cuff.
Because RC entheses transfer mechanical stress from muscle to bone, they are vulnerable to injury. 16 Although the transition between these zones is crucial for function and attachment, the development and degeneration of RC entheses are not well understood. 17 Scarring of RC entheses after surgical repair can lead to inadequate healing and increase the risk of future retear. 16
Surgical repair of RCT is recommended in young, healthy patients with acute tears, as well as in older patients with chronic degenerative tears, which have failed a trial of nonoperative treatment. 18 Recent and ongoing study continues to investigate the most effective treatment for the different types and sizes of RCTs.1,19 Factors taken into consideration when deciding treatment include the following: size of the tear, muscle atrophy and retraction, symptomatology, age and functional demand of the patient, and any medical comorbitities. 20 Current literature suggests operative treatment has limitations in providing successful enthesis regeneration. 21 Regardless of surgical technique, RC retear remains a significant postoperative complication. 22 A challenge of RC repair is the inability to regenerate enthesis to its native, organized manner. 17 Weakened and irregular enthesis regeneration is a crucial factor in postsurgical failure, 23 with retear rates ranging from 29% to as high as 94%.24,25
Like articular cartilage, the RC entheses are relatively hypovascular tissues. Intact and asymptomatic RC demonstrates decreased vascularity with age. 26 Because vascularity is crucial to healing, this relative hypovascularity further diminishes the regenerative capacity of the RC postsurgical fixation and increases the risk of retear.
Suture migration and scar tissue formation postsurgery are important factors in RC weakening and retear. The greatest risk of RC retear occurs within the first 3 months of surgical repair with RC retears typically occurring between 12 and 26 months postsurgery. 27 During this time the RC is not fully healed to the tuberosity and mobility restriction is prescribed to reduce the risk of retear. After this 3-month period strengthening of the RC muscles can begin.
Commercially available RC repair grafts have been introduced to augment RC repair. However, they have been associated with poor clinical outcomes.28,29 These grafts lack appropriate biological cues such as signaling molecules or stem cells at the bone–tendon interface. They do little to prevent fibrovascular scar tissue, which causes the RC to be susceptible to retear. Biological treatments and tissue engineering provide promising solutions for improving regenerative and functional outcomes for RCT patients. Mesenchymal stem cells (MSCs) and growth factors (GFs) have been shown to enhance enthesis regeneration in animal models; however, their compatibility with clinical use has not been demonstrated.
To achieve improved clinical outcomes in RC repair, the arthroscopic compatibility of commercially available RC repair grafts and the regenerative benefits of MSCs and GFs should be integrated. Future RC repair grafts should allow for stable implantation and fixation of the graft with current arthroscopic techniques and have the capability to deliver MSCs and/or GFs. There remains a need to integrate all these factors into a safe and surgically compatible technology that would prove effective in the clinical setting. This review identifies the tissue engineering techniques being used to effectively enhance RC repair, while also identifying the remaining challenges that must be addressed for applicability in the clinical setting.
Fixation and Stability at the Site of RCT
Effective RC repair grafts must be able to achieve mechanical stability by suture and/or suture anchor. Biomechanically the RC is critical for two functions. First, RC muscles generate forces on the humerus to internally rotate, externally rotate, and abduct the upper limb. Second, RC muscles stabilize the glenohumeral joint by applying compressive force of the humerus on the glenoid. 30 RC repair grafts must provide mechanical stability in the setting of RCT by anchoring the repaired tissue using suture fixation while withstanding mechanical forces generated by the RC muscles during healing (Fig. 2).

Dermal matrix allograft used in RC repair. Arthroscopic picture taken from the lateral portal demonstrating the surgical environment in which the tissue-engineered RC graft must be delivered.
Current suture anchor technique has proven effective in providing initial mechanical stability to the RC. Current tendon–bone grafts are used by either augmenting surgical repair, or by bridging the gap between tendon and bone. 31 These grafts are sutured to the RC tendon and the humerus (greater or lesser tuberosity). 32 These grafts commonly feature a porous acellular matrix composed of collagen and/or cadaveric dermal tissue.
The use of acellular human dermal grafts to reinforce RC repair has been shown to increase the mechanical strength and healing rates of surgically repaired RCs. 33 Commercially available RC repair grafts are used in conjunction with suture anchors to attach into both the tendon and bone. 34 Acellular allografts provide structural stability for the weakened RC tissue and a matrix into which host cells may proliferate. However, the strength of these grafts remains an area of ongoing research with one study finding a failure rate of 84% at 6 months postoperation.35,36
Commercially available grafts comprising collagen are commonly used in arthroscopic RC repair (ARCR). Collagen implants have been shown to integrate into host anatomy and enhance RC healing in long-term studies of surgical RC repair. Bokor et al. demonstrated that collagen RC grafts effectively integrated with host tendon and provided improved outcomes at 24 months postoperation. 37
RC xenografts utilize collagen from bovine or porcine sources. These grafts are acellular and rely on host cells incorporating themselves into the construct during RC healing. The success of these collagen-based xenografts has been mixed. 38 Common complications resulting from porcine-derived collagen grafts include postoperative inflammation and immunogenic reaction. Because of this, many of these grafts are not recommended or require additional research to verify their efficacy. 38 Limited data support the use of bovine-derived collagen grafts, which have demonstrated enhanced RC healing with adequate biocompatibility. 39
In animal models, larger species such as sheep and goats shed light on the biomechanical properties of experimental bioengineered grafts. Credille et al. demonstrated that biphasic interposition allografts may have clinical application by using an ovine model. 34 These larger species provide an RC anatomy that is more similar in size to humans compared with smaller animal models and therefore can undergo strenuous biomechanical property testing.
Integrating Local MSCs
Effective RC repair grafts must not only provide mechanical stability to the site of damage but must also enhance the natural healing process and enthesis regeneration. Tissue engineering allows for the delivery of stimulatory cells and molecules to the site of injury. This is carried out by seeding cultured cells (often harvested from the patient) on biologic or synthetic scaffolds, which are transplanted to the site of damage. 40 In the case of RCT, research shows that tissue engineering can play a critical role in the regeneration of natural enthesis. This has the potential to reduce rates of postoperative retear.
MSCs are heterogeneous stem cells that can differentiate into multiple cell types including muscle, tendon, and bone (Fig. 3). They play an important role in sensing tissue damage and modulating the subsequent immune response to tendon and bone injury. 16 Recent literature suggests that MSCs offer multiple benefits to the environment surrounding enthesis injury including anti-inflammation, osteogenesis, angiogenesis, and chondrogenesis. 16
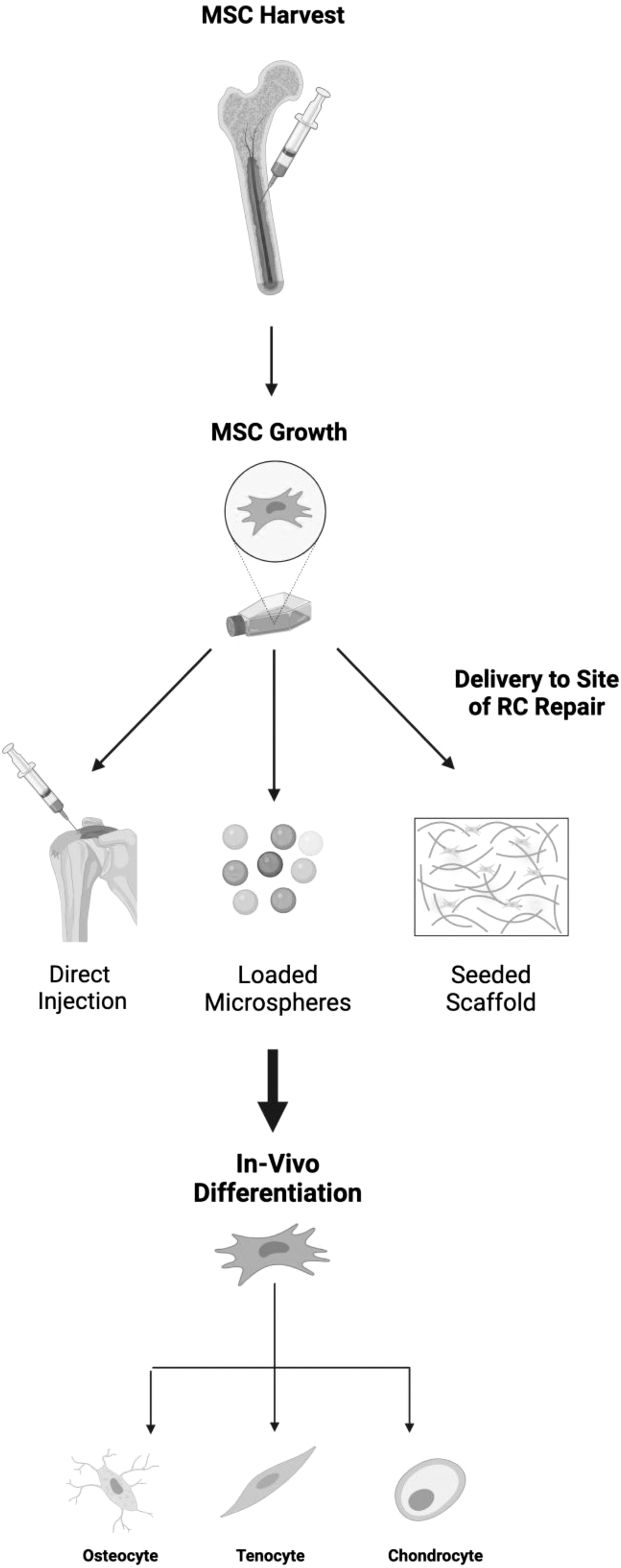
Overview of MSC delivery to the site of RCT. MSCs can be harvested from multiple anatomic sites including bone marrow. They are then cultivated in vitro, before being delivered to the site of RCT through methods including direct injection, via microspheres or exosomes, or by saturation and/or seeding of implant material. Once implanted MSCs enhance the recovery process by differentiating into cell types found in native RC enthesis. Created with BioRender.com. MSC, mesenchymal stem cell; RCT, rotator cuff tear.
Animal models have demonstrated that MSCs have application in RC enthesis regeneration. 41 MSCs can be harvested from synovium, periosteum, and adipose tissue. 42 Bone marrow aspirate has been used to enhance enthesis healing, demonstrating that stem cells may be effective in reforming the gradient from bone to uncalcified tendon that is required for RC function and attachment. 43 In the setting of RC repair, MSC tenogenic differentiation is essential for the formation of repaired tendon.
MSCs used in RC repair may be arthroscopically harvested from the subacromial bursa and humeral head bone marrow. The subacromial bursa and proximal humerus are located in close proximity to the RC making them ideal sites from which to harvest MSCs. Literature suggests that the subacromial bursa yields a higher number of MSCs and that these MSCs have a high proliferation potential. 44 Morikawa et al. demonstrated that MSCs arthroscopically harvested from the subacromial bursa showed potent regenerative properties in vitro. 45 Pancholi and Gregory demonstrated that MSCs derived from subacromial bursectomy have increased differentiation and gene expression capabilities compared with MSCs harvested from other sites. 44
Bone marrow–derived stem cells (BMSCs) have also shown proliferative potential in the setting of RCT. Research by Dai et al. illustrated that BMSCs exhibited superior tenogenic differentiation capacity compared with MSCs derived from synovium or adipose tissue. 46 In this experiment 4 × 106 MSCs were injected using a mouse model and the proliferative potential was measured at 3 and 6 weeks postinjection. Thangarajah et al. similarly showed that the use of MSCs increased tendon healing with enhanced weight bearing at 12 weeks in an ovine model. 47
Research by Novakova et al. demonstrated that interposed RC tendon grafts treated with BMSCs displayed increased enthesis regeneration at 6 months in an ovine model. 48 The long-term tenogenic differentiation of MSCs delivered to the RCT environment is an important consideration for proper enthesis healing.
Research by Smietana et al. observed that tissue-engineered tendon constructs derived from MSCs were effective at regenerating native enthesis in both acute and chronic injury of the supraspinatus tendon in a rat model. 23 This trial used scaffold-less three-dimensional tissues cultured in a growth medium with MSCs at a density of 21 × 103 cells/cm2. Analysis of RC repair was performed 8 weeks postimplantation of the MSC construct. These tissue-engineered constructs demonstrated natural architecture and greater fibrocartilage formation compared with suture-repaired tendon. 23 Fibrocartilage is an important factor in the mechanical strength and force transmission of enthesis. 23 The researchers posited that the compliance of the tissue-engineered construct allowed for mechanical cues and subsequent biological factors to aid in enthesis regeneration compared with suture-repaired tendon that relies on rigid fixation of tendon to bone. 23
Research by Chen et al. investigated the possibility of seeding bioengineered scaffolds in vivo using a rat model. Arguing that in vitro seeding adds time and limits the efficacy of transplanted cells, they proposed that RC enthesis can be best repaired by first implanting a fibrocartilage graft at the tear site and then injecting MSCs in vivo. 49 Their decellularized fibrocartilage graft included stromal cell–derived factor 1 alpha (SDF-1α), which allowed for the chemotaxis and tethering of collagen fibers postimplantation. 49 After implanting the fibrocartilage graft 106 synovium-derived CXCR4+ MSCs were injected into the shoulder joint 4 days postoperatively. In vivo functional evaluation was carried out at 4 and 8 weeks postsurgery. These cells were recruited by the SDF-1α–populated graft. 49 This approach led to a decrease in MSC disruption owing to shoulder inflammation and effective regeneration of RC enthesis. 49 Potential advantages of this approach include an increase in efficiency by avoiding the in vitro scaffold seeding process.
Research by Roßbach et al. found that in vitro seeding of an RC graft with autologous tenocytes resulted in improved RC healing in an ovine model. 50 Using an interlaid type 1 collagen-based scaffold cultivated in a medium containing 10 million autologous tenocytes, they observed greater histological and mechanical outcomes at 12 weeks postsurgery. 50
Local GFs
In addition to MSCs, local GFs have been shown to enhance the regenerative potential of RC repair grafts. GFs affect enthesis regeneration throughout the repair process. Multiple GFs have been implicated in tendon healing including: transforming growth factor (TGF)-β, platelet-derived growth factor (PDGF)-BB, insulin-like growth factor-1 (IGF-1), bone marrow–derived platelet-rich fibrin (BM-PRF), vascular endothelial growth factor (VEGF), SDF-1α, fibroblast growth factor-2 (FGF-2), bone morphogenic protein (BMP)-7, and BMP-12 (Table 1). 51
Growth Factor Implicated in Rotator Cuff Enthesis Regeneration
Inlay, between tendon and bone; onlay, on top of tendon.
BM-PRF, bone marrow–derived platelet-rich fibrin; BMP, bone morphogenic protein; FGF-2, fibroblast growth factor-2; IGF-1, insulin-like growth factor-1; PDGF, platelet-derived growth factor; RC, rotator cuff; SDF-1α, stromal cell–derived factor 1 alpha; TGF, transforming growth factor; VEGF, vascular endothelial growth factor.
TGF-β has been shown to stimulate tenocyte differentiation and promote collagen production at the site of RCT.11,52 IGF-1 and PDGF-BB both stimulate fibroblast production with IGF-1 providing an anti-inflammatory effect and PDGF-BB increasing the mechanical properties of damaged connective tissue. 53 BM-PRF has been shown to improve RC healing by enhancing bone–tendon continuity and maturation. 54 VEGF promotes angiogenesis and regulates blood flow and inflammation at the site of RCT. 55 Although vascularization is an important aspect of enthesis regeneration, additional research is needed to determine what role VEGF will play in the fairly hypovascular environment of the healing RC. 51
SDF-1α induces chemotaxis of regenerative cells to the site of RCT. 56 Basic FGF has been shown to enhance the mechanical strength of healing RC by increasing formation of RC tissue. 57 BMP-7 has demonstrated the ability to aid in RC enthesis matrix regeneration. 58 FGF-2 has been shown to induce growth of muscle, tendon, and bone at the site of RCT. 59 However, recent study using FGF-soaked collagen implants in an animal model found no therapeutic effect. 60
Extracellular vesicles (EVs) or exosomes have demonstrated promise in augmenting the healing environment of the RC. They are stem cell–derived, membrane-bound extracellular structures that include nucleic acids and signaling factors that regulate surrounding cells via autocrine and paracrine signaling. 61 Multiple studies using animal models have shown that adipose-derived stem cells and MSC-derived exosomes can be used to enhance RC tendon healing by increasing angiogenesis, strengthening the bone–tendon interface, and increasing tenogenesis gene expression.62,63 MSC-derived and tendon stem cell–derived EVs have been shown to reduce the inflammatory response post-RCT by modulating macrophages.64,65 These findings suggest that EVs have the potential to enhance RC healing via multiple mechanisms. Using an ovine model, von Stade et al. demonstrated that tenocyte-derived EVs preferentially signaled macrophages to induce greater tendon healing compared with MSC-derived EVs. 66
Genetic components such as SRY-box9 (SOX9) and Scleraxis (Scx) play an important role in the stem cell–driven repair of RC enthesis (Table 2). 43 Specifically, cells expressing these transcription factors appear to be abundant in younger, well-healing animal models. 67 Indian Hedgehog (Ihh) signaling is crucial to the mineralization and generation of enthesis. Ihh stimulates parathyroid hormone–related peptide and regenerates the enthesis mineralization gradient. 68 Although many genetic components play a role in skeletal and connective tissue development, SOX9, Scx, and Ihh provide immediate potential for RC repair grafts given the therapeutic effects they have demonstrated in existing animal model-based research.
Genetic Factors Implicated in Rotator Cuff Enthesis Regeneration
Ihh, Indian Hedgehog; Scx, Scleraxis; SOX9, SRY-box9.
Adequate delivery of GFs to the anatomical site of enthesis damage remains a challenge. 21 Common experimental techniques used in animal models include delivering GFs via injection, hydrogels, saturated sutures, and GF-loaded scaffolds. 21 Incorporating these GFs into RC repair grafts has been shown to result in a more sustained release compared with injection of GFs. 69 Research by Bai et al. provided evidence that bioprinting tissue constructs with layer-specific GFs can improve RC enthesis regeneration. Specifically, their bioprinted model used human umbilical cord MSCs with GF-loaded microspheres to induce graded, in situ tenogenic, chondrogenic, and osteogenic cell differentiation. 70 Their bioprinted scaffold demonstrated in vivo enthesis regeneration with structural and compositional similarity to native RC enthesis. 70 Histological and mechanical study of their bioprinted enthesis confirmed that this technique shows promise for regenerating enthesis in the human RC. By layering GFs, they were able to successfully generate the bone-to-tendon gradient that is vital for enthesis function.
Similar research by Chen et al. further investigated using layered GFs on a bioengineered scaffold to recreate the natural RC enthesis gradient. Unlike previous studies that have seeded scaffolds with MSCs, this research used urine-derived stem cells, which can be harvested autologously, noninvasively, and at low cost. 71 This technique produced a graded graft that featured cells of osteogenic, chondrogenic, and tenogenic lineages. Its morphology and tensile strength were highly similar to natural RC enthesis. Although GFs have been shown to enhance the healing process of RCT in animal models, their incorporation into clinical practice is not yet widespread.
Compatibility with Surgical Techniques
Previous sections have highlighted innovative biological factors with the potential to enhance RC enthesis regeneration. These factors, however, will only increase RC repair in the clinical setting if they can be effectively integrated into current surgical technique. ARCR is more commonly performed than open RC repair. 72 Rates of ARCR are estimated to be 74–80%.34,73 Although current studies demonstrating the effectiveness of incorporating MSCs and GFs into RC grafts in animal models are promising, there exists a gap in applying these techniques to arthroscopic surgical procedures.
Two factors pose a challenge to effectively deliver MSCs and GFs to the RCT environment during ARCR. First, ARCR utilizes small arthroscopic ports (<1 cm in diameter) through which all surgical implants must be passed. 74 Second, ARCR uses consistent fluid irrigation of the shoulder joint, which creates positive fluid pressure in the RCT environment during the procedure. This fluid has the potential to flush away MSCs and GFs that are not adequately integrated into the RC repair graft.
Current commercial RC repair grafts are compatible with arthroscopic surgical technique and provide mechanical stability to the damaged RC (Table 3). Many of these grafts include a porous or fibrinous design that allows for incorporation of native tissues and biological factors. Most grafts, however, do not include exogenous MSCs or GFs that have been shown to improve RC enthesis regeneration in animal models. Early clinical trials that have incorporated factors such as plasma rich in GFs have not exhibited clinical success. 75
Examples of Commercially Available Rotator Cuff Implants
GFs, growth factors; MSCs, mesenchymal stem cells.
Discussion
The interaction between MSCs and GFs and the RC environment are responsible for improved postoperative tendon healing and enthesis regeneration. The importance of integrating biological factors into RC repair is especially important owing to the fact that the RC footprint at the proximal humerus naturally has relatively few endogenous MSCs. 76 Exogenous MSCs delivered to this site must also be directed toward a tenogenic lineage and away from the fibrosis pathway to minimize the risk of postsurgical retear.
Existing literature reveals that limitations remain between the tissue-engineered solutions to RC repair that have shown promise in animal models and the surgical environment of the clinical setting. 77 To optimize the role of tissue engineering in RC repair clinically focused considerations must be incorporated into future study.
Animal models feature open repair of the RC without substantial irrigation. This favorable environment does not allow for the effectiveness of these biological factors in the clinical setting to be fully evaluated. Arthroscopic procedure and fluid irrigation should be incorporated into future models to determine the success of MSC- and GF-delivery techniques.
To provide better outcomes for RCT patients, future RC repair grafts must allow for stable implantation and fixation of the graft with current arthroscopic techniques as well as have the capability to deliver endogenous MSCs and/or GFs (Fig. 4). The increased size of the human RC anatomy must also be taken into consideration when studying the mechanical stability of a tissue-engineered graft. Although large animal models such as sheep and goats are less frequently used than small animal models such as rats and rabbits in RC repair studies, they provide more comparable anatomic size and biomechanical properties with the human anatomy. 78 Bolam et al. demonstrated that a combined GF hydrogel containing IGF-1, TGF-β1, and parathyroid hormone enhanced the mechanical strength of healing RC enthesis in a small animal model (rats), but did not demonstrate enhanced mechanical strength in a large animal model (sheep). 79
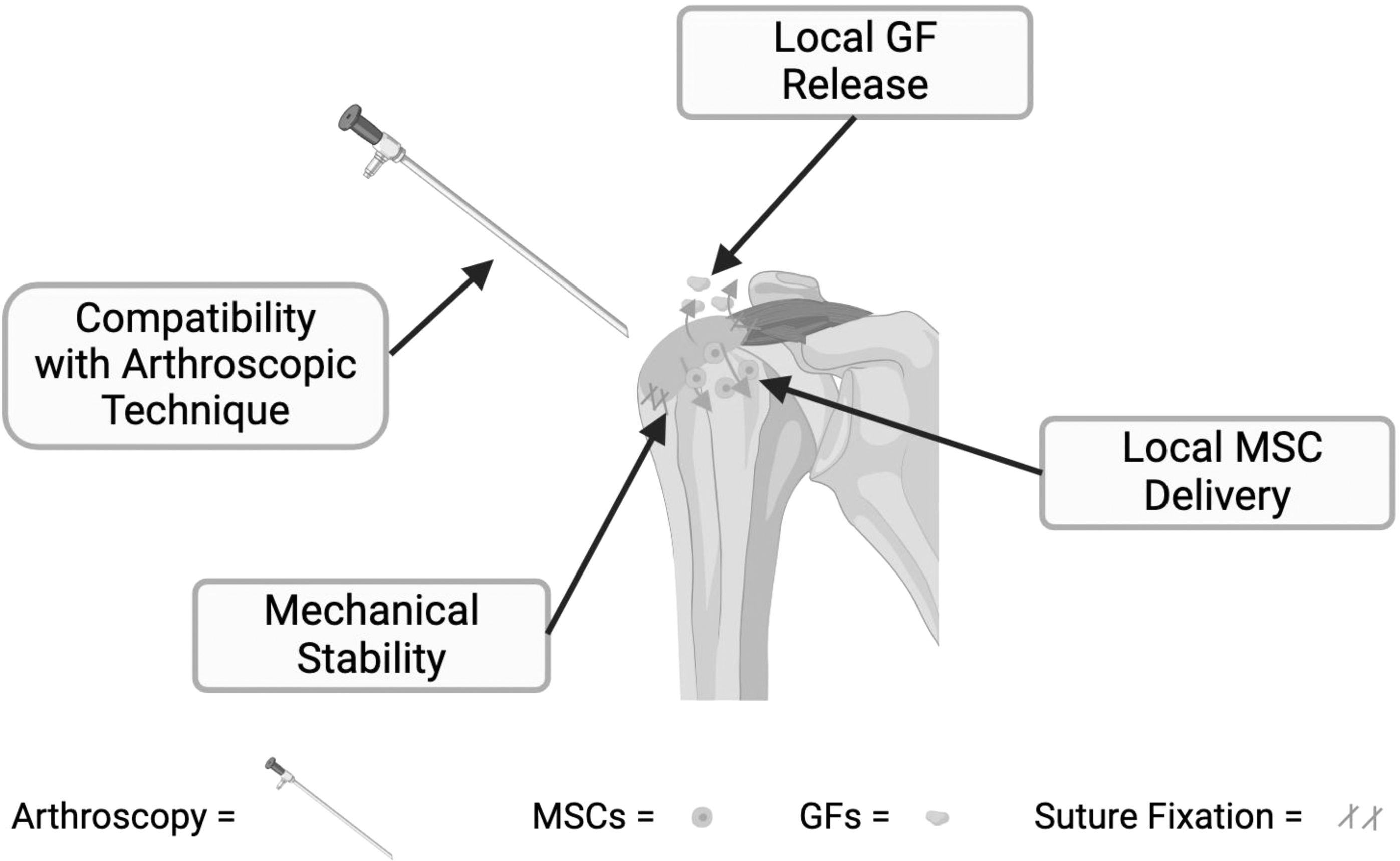
Four factors of effective future RC repair graft. Future grafts must incorporate: (1) mechanical stability via suture fixation; (2) MSC recruitment or delivery into the RC environment; (3) GF release; (4) compatibility with arthroscopic technique that includes a port diameter <1 cm and continuous, pressurized irrigation. Created with BioRender.com. GF, growth factor.
Similarly, Dickerson et al. showed that cancellous bone-derived scaffolds that resulted in organized RC tissue healing in an ovine model, however did not result in enhanced biomechanical strength. 80 These findings shed light on the applicability of these tissue-engineered solutions in clinical practice. Future studies should consider the scale of animal model being used and incorporate large animal models when possible. This can provide a more representative model in which to test biomechanical strength.
Limitations also include differences in the anatomy and biomechanics of animal RC and human RC. Although species such as rats, mice, and sheep are commonly used as animal models to investigate promising healing modalities, there exist differences between animal and human anatomy and biomechanics. One challenge is the natural regenerative capacity that the rat RC possesses which features a lack of supraspinatus fat accumulation and lower RC retear rates compared with human RC. 81 In addition, the biomechanical stresses on the RC of quadrupedal species differ compared with bipedal humans.
Future studies that integrate arthroscopic delivery of the tissue-engineered construct, continuous fluid irrigation of the RC environment, and a larger animal model to optimize biomechanical testing will only enhance our understanding of RC repair and regeneration. This would demonstrate which delivery methods of MSCs and GFs are compatible with the surgical setting and which graft constructs are strong enough to provide mechanical stability. By validating that a tissue-engineered technique can withstand these conditions, a strong connection would be made between success in an experimental animal model and the clinical setting.
Conclusion
RCT treatment remains challenging given the inconsistency of RC healing. Biological treatments and tissue engineering have demonstrated promise in enhancing the regeneration of RC enthesis. A gap exists between the promising biological and tissue-engineering modalities that are effective in animal models and successful in the clinical setting. Currently available commercial grafts are compatible with arthroscopic surgical techniques; however, they lack biological augmentation from MSCs and GFs. This may contribute to the fact that they have shown mixed outcomes in the clinical setting. Future RC repair grafts must combine MSCs and GFs with arthroscopically compatible technology to optimize RC healing potential in the clinical setting.
Footnotes
Authors' Contributions
M.S.D.: Writing—original draft and editing, investigation, formal analysis; S.K.: writing—review and editing; J.L.: writing—review and editing; C.K.: writing—review and editing; C.C.: writing—review and editing; E.C.: writing—review and editing; M.S.: writing—review and editing; G.A.: writing—review and editing, resources; Y.P.Y.: conceptualization, investigation, resources, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded through the financial support of National Institute of Arthritis and Musculoskeletal and Skin Disease (NIAMS) grants U01AR069395 (Y.P.Y.), R01AR072613 (Y.P.Y.), R01AR074458 (Y.P.Y.), Department of Defense (DoD) grants W81XWH-20-1-0343 (Y.P.Y.), and W81XWH-21-PR211291 (Y.P.Y.).