
Abstract
The repair of nasal septal cartilage is a key challenge in cosmetic and functional surgery of the nose, as it determines its shape and its respiratory function. Supporting the dorsum of the nose is essential for both the prevention of nasal obstruction and the restoration of the nose structure. Most surgical procedures to repair or modify the nasal septum focus on restoring the external aspect of the nose by placing a graft under the skin, without considering respiratory concerns. Tissue engineering offers a more satisfactory approach, in which both the structural and biological roles of the nose are restored. To achieve this goal, nasal cartilage engineering research has led to the development of scaffolds capable of accommodating cartilaginous extracellular matrix-producing cells, possessing mechanical properties close to those of the nasal septum, and retaining their structure after implantation in vivo. The combination of a non-resorbable core structure with suitable mechanical properties and a biocompatible hydrogel loaded with autologous chondrocytes or mesenchymal stem cells is a promising strategy. However, the stability and immunotolerance of these implants are crucial parameters to be monitored over the long term after in vivo implantation, to definitively assess the success of nasal cartilage tissue engineering. Here, we review the tissue engineering methods to repair nasal cartilage, focusing on the type and mechanical characteristics of the biomaterials; cell and implantation strategy; and the outcome with regard to cartilage repair.
Impact statement
Nasal septal cartilage is key to the cosmetic and function of the nose. To repair important damage to the nasal septum, current surgical techniques are complex and limited by graft source availability. Conversely, tissue engineering is a promising strategy to reproduce the dimensions and mechanical properties of the nose without causing donor site morbidity. This approach, however, remains overlooked for the reconstruction of the nasal septum compared with other cartilaginous tissues. This review describes the specific challenges associated with nasal cartilage repair and the pioneering studies leading to advances in the growing field of nose tissue engineering.
Introduction
The nasal septum is the cornerstone of the nasal framework, with morphological and respiratory functions. It is composed of cartilage, an avascular tissue with poor regenerative abilities. Consequently, the repair of traumatic, post-operative, or constitutional lesions of the nasal septum represents a major medical challenge. For instance, the deviation of the nasal septum is thought to affect close to 90% of the general population. 1
The nose is also exposed to multiple traumas, infections, and skin or mucosal tumours 2 that affect nasal morphology and respiratory function. In addition, rhinoplasty, which involves altering the shape or size of the nose, is one of the most commonly performed surgical procedures, 3 despite significant side effects (notably due to possible airway obstruction, which requires additional intervention 4 ) and a high rate of patient dissatisfaction.
Following an accident or serious illness, patients hope to regain the best possible quality of life, which encompasses a state of physical, mental, and social well-being. 3 Indeed, as the nose is an important aesthetic marker, its deformities have a negative impact on the patient's psychological health, 4 in addition to causing nasal airway obstruction. Reconstruction of the nose framework is thus essential. This commonly relies on grafting autologous tissue, in most cases rib cartilage, to replace the nasal septum, but this procedure is strongly limited by donor graft availability and may cause donor site morbidity. 5
If the nasal envelope is also damaged, skin and mucosal flaps are also needed, ideally from the forehead. Free skin flaps can alternatively be taken from the forearm in situations where facial skin is not available.6,7 These are sometimes prepared with insertion of a framework under the skin before displacement, and are called composite flaps. 8
Nowadays, surgery is increasingly assisted by tissue engineering to avoid shortcomings such as harvesting a large amount of material from the patient.9–12 Like articular cartilage, the nasal cartilages are hyaline. Thus, although nasal cartilage engineering is a relatively recent area of research, it is likely to progress rapidly, as it will benefit from efforts devoted to articular cartilage engineering. In this context, the traditional paradigm of tissue engineering of combining biomaterials with cells and stimulating factors applies to nasal cartilage engineering as well.
Thus, nasal cartilage engineering involves fabricating biocompatible cellular scaffolds with suitable biological and mechanical properties to restore the aspect and function of the nose, without eliciting immune or inflammatory response that may result in implant rejection. These biomaterials, assembled from biomolecules (such as collagen or alginate) or synthetic polymers (principally polycaprolactone), host chondrocytes or mesenchymal stem cells (MSCs), which are induced to undergo chondrogenesis under the influence of selected growth factors.
Although non-resorbable materials (made for instance from MedPor or GoreTex) are routinely used to fabricate acellular nasal grafts, the progressive degradation and replacement of biomaterials by neo-synthesized extracellular matrix (ECM) significantly improve their integration within native tissues.13,14 Mechanical properties may evolve over time, as the new ECM progressively replaces the biomaterial. At the same time, the neo-synthetized tissue must maintain its structural integrity and shape, to continuously provide support for the respiratory function of the nose.15–17
A growing number of studies are investigating the stiffness, elasticity, and degradability of the biomaterial and of the engineered tissue, to compare them with native septal cartilage.17–24 Assessing the long-term evolution of such devices, however, remains a challenge. Preclinical trials are also hampered by the absence of an animal model with an external nose protruding from a flat face, which is a human specificity. 25 This review aims at presenting the advances, short-comings, and promising approaches in biomaterial design for nasal septum tissue engineering.
Anatomy of the Nose
Structure and function of nasal cartilage
Structure of the nose
To support its structure and regulate airflow, the nose is composed of the following tissues, each possessing interactive functions: (1) The skin, the outer layer, provides a protection against external elements. (2) Fatty and fibromuscular layers separate the skin from the cartilage and mucosa below, and contribute to nose flexibility, shape, and stability. (3) A mucosa rich in blood vessels nourishes nasal cartilage by imbibition. Its outermost subsection is exposed to airflow and acts as a protective barrier, whereas its innermost part, known as the perichondrium, is adjacent to cartilage. (4)
The nasal bone forms the upper part of the nose, contributes to its overall structure and stability, and provides anchorage points for the nasal septum. (5) Finally, nasal cartilages (Fig. 1), which include: the upper lateral cartilage located below the nasal bone, forming soft lateral sidewalls; the lower lateral cartilage (also called alar cartilage) that determines the shape of the tip of the nose and the opening of the nostrils; and the nasal septum, located in a central position. The septum rests on the maxilla in front, joins the bony nose at the top, and links with the bony septum at the back. It divides the nose into two nasal cavities and it is structurally the most important cartilage component of the nose, supporting the upper and lower cartilages, as well as the overlying nasal skin.
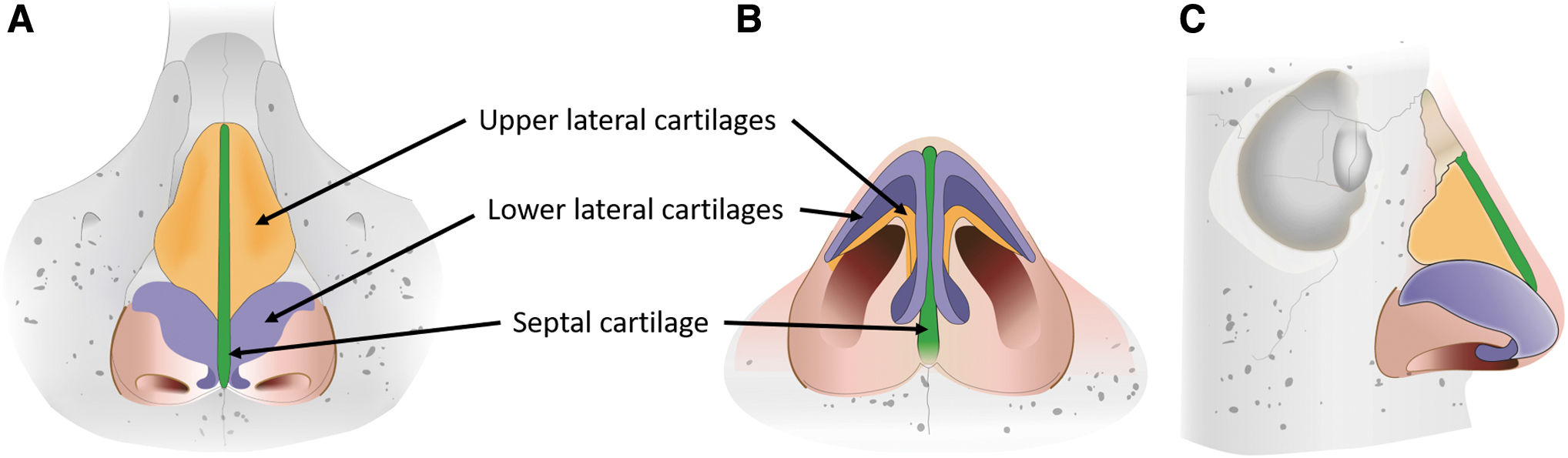
Anatomy of human nasal cartilage. Views with skin removed to show upper (yellow) and lower (purple) lateral cartilages and septal cartilage (green).
Composition
Septal cartilage is a hyaline cartilage containing chondrocytes embedded in an ECM rich in glycosaminoglycans (GAGs) and collagen, with type II collagen being the most abundant. In its superficial zone, chondrocytes have an elongated morphology and are aligned parallel to the surface. There, collagen is also organized in thick sheets of fibres that orientate perpendicularly to the surface. 26 In contrast, chondrocytes in the central zone are more rounded and collagen lacks a definite arrangement (this is also the case in alar cartilage).
The GAG/collagen ratio also varies according to location within the septum, with a higher abundance of GAGs in the central zone and of collagen in the superficial zone. 26 In addition, unlike other hyaline cartilages, the superficial zone of nasal septal cartilage contains nasoseptal progenitor cells (NSPs). This cell type shares surface markers and proliferation potential with MSCs, suggesting an intermediate state of differentiation between MSCs and chondrocytes.27,28
Function
The shape of the nose conditions nasal breathing in humans. Nasal permeability is essential to filter, warms and humidifies the air, and regulates breathing by secreting mediators to the lungs and brain. 29 The respiratory flow is conditioned by the intrathoracic depression and the shape of the nose. This shape is linked to the static caliber of the nasal cavities (affected by possible deviation of the nasal septum, or the thickness of the nasal mucosa 30 ), as well as the capacity of the nose to resist dynamic inspiratory collapse. 31
If the cartilaginous structure of the nose is not resistant enough, the airflow in the nasal cavity creates a transmural pressure differential that may lead to the collapse of the nasal nostrils by Venturi effect 32 and valve-related obstruction. 33 As a consequence, the cartilage tissues of the nose have a crucial morphological and mechanical role. The nasal septum, in particular, maintains sufficient tension to prevent collapse during inspiratory flow.
Pathologies of nasal cartilage
Due to the avascular nature of the cartilage, injuries to the nasal septum do not have the ability to heal, and are at best filled with fibrous tissue. During development, septal cartilage is one of the drivers for the shaping of the face. Its growth is hampered by the nasal bone possessing a different embryonic origin and developing in the opposite way. 34 Excess growth of nasal septum may exceed the capacity of the overlying skin, resulting in a deformation inside the nose with narrower zones that are responsible for a decrease in respiratory flow. Besides deformation due to extreme growth, the weakening or destruction of nasal septum is most often caused by trauma, prone to occur due to the protruding nature of the nasal pyramid.
Although trauma is often tolerated to some degree due to the elastic properties of cartilage, it can cause dislocation of the septum from the nasal bone and, in more severe cases, fracture. Following a fracture, nasal cartilage resistance is permanently altered and constraints exercised by the overlying skin will lead to additional deformation. 35 Nasal cartilage loss may also result from cartilage infection (chondritis), or from excessive cartilage resection following rhinoplasty, an extremely frequent procedure that can lead to the iatrogenic loss of nose support. 36 This deficiency can lead to a reduction of the size of the nasal cavities and subsequent static obstruction or collapse of the nasal cavities during inspiration, called the nasal valve phenomenon.
Following trauma, a hematoma appearing between the cartilage and the perichondrium can lead to prolongated ischemia and eventually to necrosis of the cartilage while the mucosa is still present. 37 The nasal mucosa is also subjected to autoimmune (such as Wegener's or Churg-Strauss disease) and inflammatory (such as vasculitis) diseases. These lead to capillary damage and mucosal destruction, resulting in necrosis of the underlying cartilage, collapse of the nasal pyramid and nasal airway obstruction.
Destruction of the nasal mucosa also occurs in cases of amputation of the nose following, for instance, excision of a tumor, or advanced burns. In such cases, the repair of the nasal septum is particularly challenging, as the mucosa (and potentially the overlying skin) must be replaced with vascularized tissue that is able to supply nutrients to the nasal cartilage. 6 This procedure is demanding and technically very complex, with issues related to the availability of vascularized tissues. As an alternative, patients can use a removable prosthesis that is fixed to the skin on a daily basis with glue, magnets or anchor bolts, either as a permanent solution or while waiting for surgery. 38
Current Surgical Techniques
Cartilage grafts
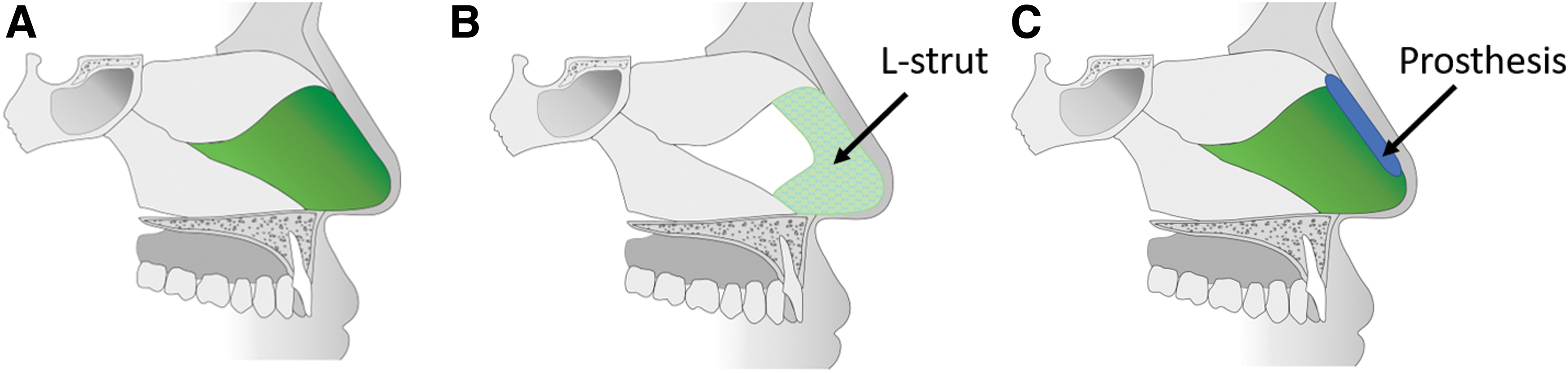
Posteroinferior deformities of the nasal septum are the most common constitutional problems. The usual approach to nasal septoplasty is to remove the deformed areas without reconstruction, while preserving the anterior and superior part of the septal cartilage forming a square resting on the maxillary bone and joining the bony nose (Fig. 2A). This L-shaped square is usually sufficient to preserve the shape of the nasal pyramid and its respiratory function (Fig. 2B). However, if the anterior and superior zones of the septal cartilage are affected by deformities or are destroyed, an L-shaped cartilaginous structure (called L-strut) is reconstructed.
The L-strut is completed with a dorsal graft at the top to enable interlocking with the bony nose, and spreader grafts on each side connecting the neo-septum to the upper lateral cartilage on each edge of the nose (Fig. 3). 39 Whenever possible, grafts are sutured to the remaining native cartilage and surgical attachment to the bony nose is not required. This autologous grafting approach is highly preferred, as the grafts elicit little immunogenic responses and are very well accepted in an anatomical position.
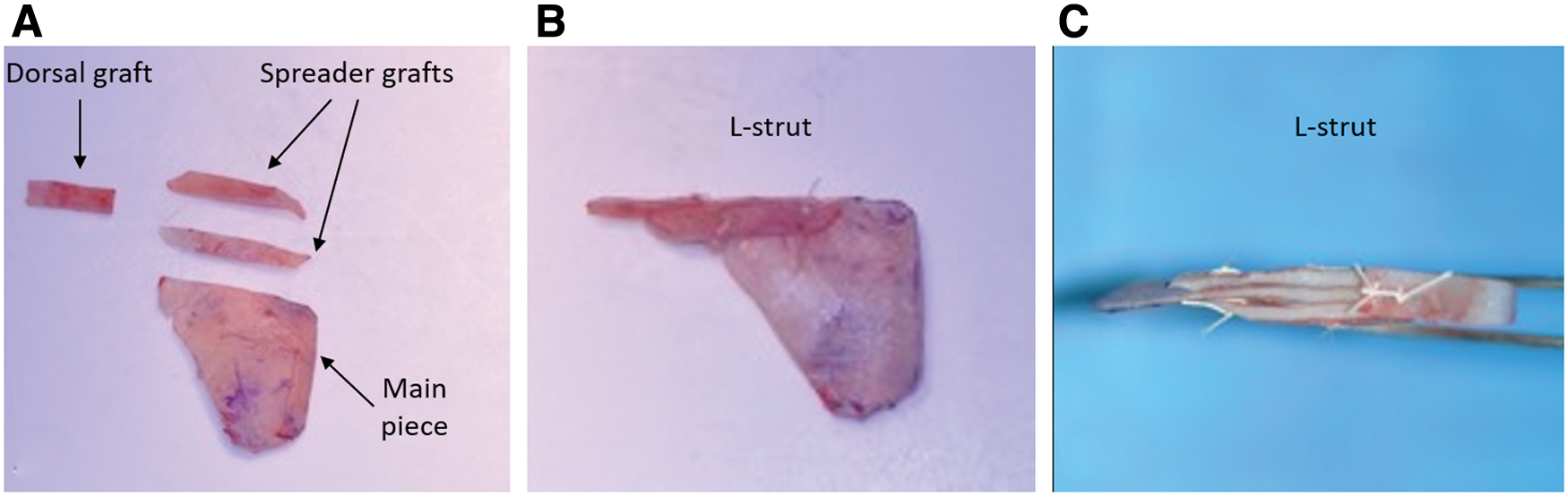
Reconstruction of the nasal septum using the extracorporeal L-strut septoplasty technique.
Autografts made from the posterior fragments of the septum are ideal, due to the adequate stiffness, thickness, and straight morphology of septal cartilage. If there is not enough septum left to constitute an L-strut, autografts may be made from ear or rib cartilage instead. Autologous cartilage L-strut grafts are commonly performed on patients undergoing subtotal or total framework reconstruction of nasal defects, including for autoimmune, malignant, traumatic, and iatrogenic etiologies.40–42 Clinical trials resulted in good aesthetic results as well as a clear improvement in nasal breathing.
In addition, numerous clinical trials have been carried out using autologous cartilage in aesthetic augmentative rhinoplasty procedures.43–46 However, the deformation and resorption of the autologous grafts remained a major drawback, with costal cartilage frameworks undergoing deformation in almost 60% of cases. 42
However, the quality of the ear or rib cartilage is not identical to that of the septal cartilage and the available quantity is limited. Ear cartilage is not abundant enough and too thin to reconstruct the entire cartilaginous septum; its removal implies a skin scar, which is often not apparent but is likely to evolve into a hypertrophic or even keloid aspect; and there is a risk of pain and collateral deformation of the auricle. 47
Moreover, the composition of ear cartilage is different from that of septal cartilage, with a higher elastin content associated with lower tissue stiffness. 48 Conversely, costal cartilage is relatively abundant compared with the dimensions of the nasal septum. Because of its availability and stiffness, it can alone replace the entire septum and provide the spreader grafts. Nevertheless, the thoracic scar is visible, and the harvesting site is very painful postoperatively. Complications such as pneumothorax, diaphragmatic hernia, or secondary deformation of the chest wall are also possible. 49 This cartilage is also stiffer than the nasal septum, and may undergo unexpected deformation following surgery. 50
The harvesting of cartilage grafts therefore entails morbidity at the donor site. Allografts represent an alternative to circumvent this issue, but are limited by donor availability and represent a higher risk of immune response. While the immunogenicity of cartilaginous allografts can be reduced by irradiation to remove resident cells,51–56 their use in nasal cartilage septoplasty remains understudied. Dorsal augmentations of the septum have also been performed with equine, porcine, and caprine cartilage xenografts.57–59
Although these grafts provide good aesthetic results for augmentative rhinoplasty, they possess a high risk of immune reaction and rejection, as well as disease transmission.
Synthetic grafts
Synthetic materials such as Gore-Tex (made from expanded PTFE), MedPor (made from porous polyethylene), or silicone-based implants are commonly employed in septoplasty due to their availability in different sizes and shapes, their simple surgical use, and their low cost. However, the ectotopic implantation of such non-resorbable materials under the skin of the nose leads to high complication rates. These materials are considered biocompatible and non-toxic, but often lead to superinfection and rejection (in 21% of cases with MedPor 60 ).
Moreover, their excessive stiffness may result in extrusion and perforation of the skin. 16 The behavior of the skin above the implant is evaluated clinically, but no mechanical analyses has been performed, as these implants had no structural purpose. To date, the potential of these implants for functional purposes remains unknown.
As an example of a straightforward implantation of synthetic grafts in the nose, silicone prostheses have been used for nasal dorsum augmentation in surgeries aiming to “westernize” the nasal pyramid, a strong demand in Asia where noses are generally characterized by a low projection of the dorsum. 61 These prostheses are positioned under the skin of the nose, above the nasal osteo-cartilaginous skeleton, in a non-anatomical position (Fig. 2C). These non-degradable implants were not subjected to mechanical studies, as their design was not aimed at any functional role. Unfortunately, infection and spontaneous extrusion are favored by the thinness of the integument covering these prostheses on the cutaneous or mucous side, and the frequency of trauma and micro-trauma to the nasal pyramid (due to nose blowing, scratching, dressing, practicing sports). 62
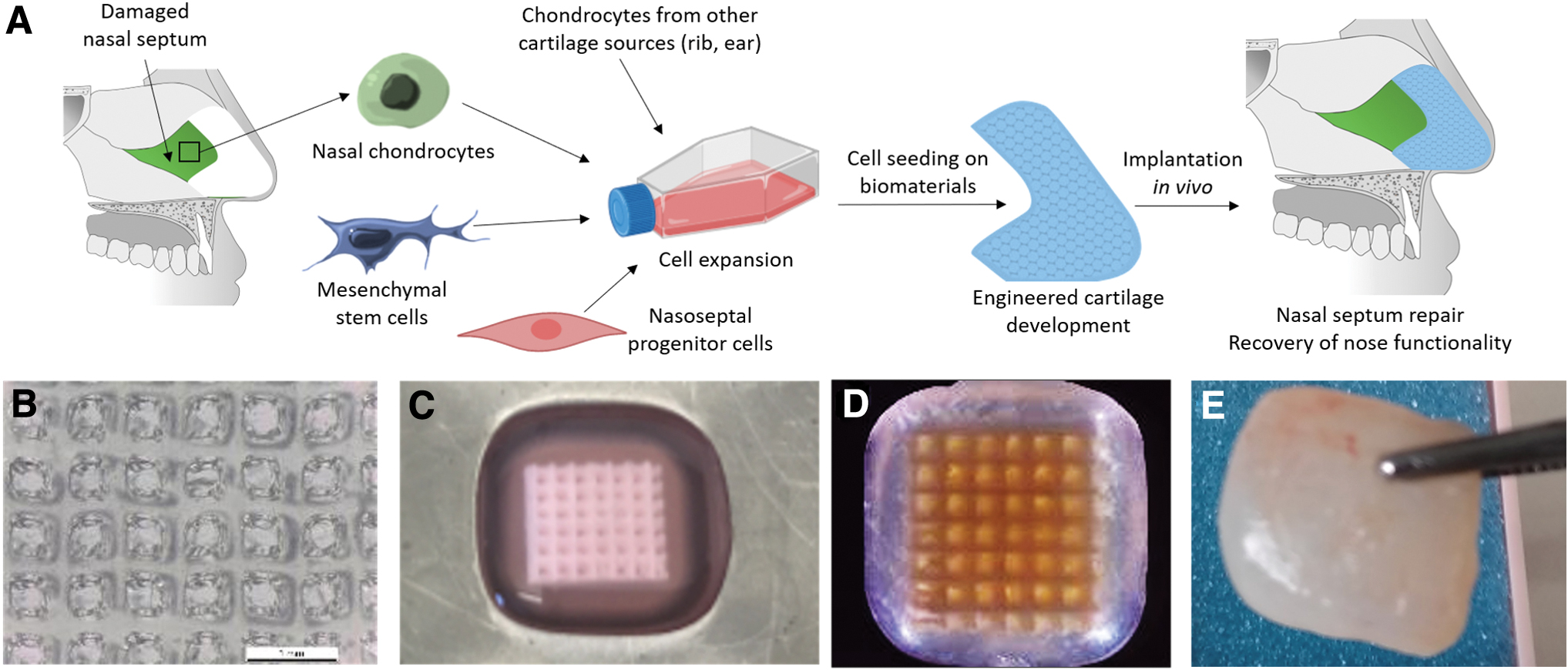
In addition, a superinfected synthetic material cannot be cleared of germs and must be removed. Instead, biomaterials providing a suitable environment for cell activity and for the secretion of the ECM, to eventually constitute a cartilage tissue, represent a more promising class of medical devices (Fig. 4A).
Challenges in nasal cartilage engineering
Tissue engineering aims at developing biomaterials that mimic the function of a healthy biological tissue. Hyaline cartilages are characterized by a very low cell density and a dense ECM,27,63 giving the tissue its unique histological and mechanical characteristics. The particularity of the septal cartilage resides in its greater rigidity and lower elasticity than that of alar or auricle cartilages, 48 providing shape stability and preventing fracture in the event of minor trauma. However, the elastic behavior of the septal cartilage is non-linear, which results in the possible fracture if the stress is too high. 64
Moreover, since this tissue is not vascularized, the cartilage has no regenerative capability and the septum does not regain its overall mechanical characteristics following fracture. Thus, a major challenge in septal cartilage engineering is to develop an artificial tissue that mimics the unique elastic characteristics of human septal cartilage, so as to give shape and support to the lateral cartilages, while being well supported by the skin. 65
Such engineered tissues must also resist contraction due wound healing and repeated long-term respiratory nasal valve deformation. As a consequence, evaluating the compressive or tensile modulus of biomaterials is a crucial step to predict their successful use in nasal cartilage engineering. In a biomimicry approach, this notably involves the production of a cartilaginous ECM with a high content in type II collagen and GAG by live cells seeded in biomaterials.
An additional obstacle is the protrusion and very thin overlying skin that are specific to the human nose, and not found in any animal model for preclinical studies. Thus, while implanting the prosthesis subcutaneously in animals (e.g., flat on the back of nude mice) enables testing of a certain resistance to skin tension, it does not reproduce the actual positioning of the nasal septum anatomically perpendicular to the skin. As a result, animal experimentation allows researchers to study the stability of the engineered nasal cartilage, but without replicating its true morphological or respiratory function.
Combining Cells and Biomaterial Scaffolds for Nasal Cartilage Engineering
Cells
Chondrocytes, the cellular components of cartilage, are the most intuitive cellular candidates for septum engineering. Human chondrocytes can be obtained by extraction from surgical septal residues, expanded in vitro, and re-differentiated into chondrocytes using culture media containing bone morphogenic protein 2. 66 If the residual septum is not available in sufficient quantity, other cartilage tissues could serve as a source of chondrocytes.
However, the proliferative and chondrogenic capacity of chondrocytes varies according to their origin: auricular, nasal, and costal chondrocytes could be easily amplified, but auricular and nasal chondrocytes generate better quality cartilage pellets than costal chondrocytes, as evidenced by higher production of type II collagen and proteoglycans. 67 Moreover, nasal chondrocytes have a higher proliferative and chondrogenic capacity than articular chondrocytes, 68 which has prompted clinical trials using autologous nasal chondrocytes for the treatment of focal traumatic lesions of articular cartilage. 69
These data suggest that it will be more difficult to reconstruct good-quality nasal cartilage using non-nasal chondrocytes. Clinical trials using chondrocytes extracted from nasal septum for nasal reconstruction are underway, with very satisfactory initial results for functional alar lobule restoration. 70
Alternatively, MSCs can be preferred for their proliferative nature and versatility, and their potential to undergo chondrogenesis 71 in the presence of transforming growth factor-beta 3 (TGF-β3). 72 MSCs from adipose tissue,73–75 Wharton's jelly, 76 or bone marrow77–79 have already been successfully differentiated into ECM-producing chondrocytes. As the stabilization of the chondrocyte phenotype as well as the production of ECM by chondrocytes is favored by a three-dimensional environment, 80 cell matrices in the form of hydrogels are usually preferred to obtain a cartilage-like tissue.
Finally, NSPs are extremely promising cell candidates for cartilage tissue engineering. They have the potential to differentiate into a chondrogenic and osteogenic (but not adipogenic) lineage 27 and they possess a proliferation potential similar or greater than MSCs.18,81 However, the use of NSPs is highly limited by tissue availability, in particular for cases where the nasal septum has been heavily damaged or requires total replacement.
Materials for nose cartilage engineering
In the literature, the most frequently reported building block for producing biomaterials for nasal cartilage engineering is polycaprolactone (PCL)17,19,28,75,82–88 (Tables 1–3), followed by natural biomolecules such as alginate,23,79,89–91 collagen,24,70,92,93 fibrin,21,84 elastin, 95 hyaluronic acid,24,95 or gelatin.21,24,77,84,94,95 As an example, alginate can be employed on its own as beads to encapsulate growth factors 89 or chondrocytes,23,90,91 leading to enhanced type II collagen and GAG production. Importantly, PCL,17,19,28,75,82–86 as well as poly(glycolic acid), poly-L-lactic, 22 type I collagen,92,93 or hyaluronic acid, 24 are compatible with 3D-printing, an advantage for reproducing the specific shape of patients' nasal cartilage, as part of personalized medicine approaches.
Mechanical Properties of Scaffolds Developed for Nasal Cartilage Engineering
ECM, extracellular matrix. PCL, polycaprolactone.
Neocartilage Extracellular Matrix Production in Cellularized Biomaterials for Nasal Cartilage Engineering
GAG, glycosaminoglycan.
Host Response of Biomaterials Developed for Nasal Cartilage Engineering Implanted In Vivo
PLGA, poly(lactic-co-glycolic acid); TGF, transforming growth factor; MSC, mesenchymal stem cell.
As a synthetic alternative to PCL, polymers such as poly(lactic-co-glycolic acid) (PLGA), 78 poly(glycolic acid), 22 or poly(vinyl alcohol) 90 have shown promising results, with the GAG accumulation in constructs implanted subcutaneously in nude mice. Further, in a comparative study involving six different scaffold types, polydioxanone, poly-3-hydroxybutyrate-co-3-hydroxyvalerate, and PCL materials best supported cartilage ECM and GAG deposition. 74
Improving biomaterials for nasal cartilage engineering
Ideally, the hydrogels used for tissue repair should progressively degrade as they are replaced by the ECM secreted by seeded cells. The time required for this substitution to occur, however, is difficult to master, and a few degradable hydrogels possess sufficient rigidity to withstand the mechanical stresses sustained by the native nasal septum. To solve this problem, a solid scaffold whose biomechanical properties mimic those of the native septum can be combined with a hydrogel (Fig. 4B–D).17,21,75,76,88 The role of this solid scaffold is threefold:
Ensure the structural integrity of the chondrocyte-containing hydrogel in areas exposed to mechanical loads. This notably involves preventing the hydrogel from collapsing under the stress imposed by the overlying nasal skin. Strong attachment of the hydrogel to the scaffold can be enhanced by maximizing contact between the gel and the scaffold, for example by creating pores and increasing the hydrophilicity of its surface. Determine the shape and volume of the tissue to be reconstructed. 3D printing technology is particularly well suited, thanks to an automated manufacturing process that can generate scaffolds with precise geometries and internal architectures (such as pore size) that plays a critical role in tissue formation in vitro and in vivo.96,97 This technology also allows scaffolds to be customized to suit patient- and clinical-specific needs. Provide mechanical properties to the hydrogel-scaffold construct that mimic those of the native septum. These properties can be adjusted by selecting the type, concentration, and cross-linking method of the scaffold components.
As an example of combining robust scaffolds with softer but more biocompatible hydrogels, PCL combined with alginate formed 3D-printed biomaterials that stimulate ECM production by chondrocytes and are stable for 4 weeks after ectopic implantation in mice. 85 PCL has also been combined with agarose, 87 fibrin, 84 and gelatin 19 to enhance cellular interactions, thus promoting cartilage tissue formation. In addition, the incorporation of a decellularized matrix has proven to be a powerful tool for improving the adhesion, proliferation, and viability of cells seeded onto scaffolds of PCL, 88 chitosan and agarose, 76 or fibrin cross-linked with genepin. 21
However, even with a decellularized matrix, colonization of seeded cells throughout the scaffold structure remains a major challenge. 73 To circumvent this problem, 3D bioprinting has been performed with bioinks encapsulated with live cells. Type I collagen or nanofibrillated cellulose/alginate were tested as a scaffolding material in combination with nasal chondrocytes or MSCs, but in vivo studies have been limited to subcutaneous implantation in nude mice.79,98,99
Biocompatibility of Reconstructed Nasal Cartilage
Mechanical properties
The mechanical properties of the nasal cartilage are highly dependent on its ECM composition, notably the collagen to GAG ratio. 100 Ideally, engineered nasal cartilage constructs will aim at mimicking the biomechanical properties of the native septum as close as possible (Table 1). Decellularized nasal cartilage may serve as a cellular scaffold, provided that the stability and rigidity of the ECM are preserved 20 or restored by chondrocyte culture over 6 weeks. 18 In synthetic biomaterials, 3D-printing procedures have been employed to modulate Young's modulus, for instance in PCL-based biomaterials. 87
A 3D-printing approach was also used to fabricate customized poly-L-lactic acid porous implants to reconstruct nasal septum perforations, designed with a topography that could accommodate nanoparticles for drug delivery applications. 22 Further, the compressive or tensile modulus of engineered nasal septa was evaluated both in vitro in the presence of chondrocytes from the human nose17,28,88,89,91,93 or sheep condyle, 19 or human MSCs 73 ; and in vivo with human,22,23,70,90,92,94 rabbit articular, 84 or goat ear 24 chondrocytes.
Overall, following ECM deposition by cells seeded in PCL-based biomaterials, the measured biomechanical properties were akin to that of native nasal cartilage.17,86 However, the mechanical evaluation of collagen/hyaluronic constructs over 8 weeks after in vivo implantation in mice showed insufficient resorption time and stiffness, 24 although the deposition of cartilage ECM was promoted. With other biomolecules, cross-linking has been successfully used to modulate the stiffness and stability of fibrin 21 and gelatin76,77 hydrogels, but these remain considerably lower than those of native cartilage.
Therefore, efforts to produce biomaterials that better mimic the mechanical properties of the nasal septum are still needed in the field, to ensure that the engineered cartilage is compatible with the respiratory function of the nose on the long term.
Degradability
Non-resorbable implants such as Medpor (porous polyethylene), Gore-Tex, or silicon that are often used in purely aesthetic procedures (for instance, to increase the profile line of the dorsum) are positioned ectopically under the overlying skin of the nose. These materials are considered biocompatible and non-toxic; however, their rate of rejection and superinfection in the nose is significant. 60
Aesthetic results and complications were retrospectively evaluated after augmentation rhinoplasty, 16 and showed that rejection rate and adverse evolution of the capsule around the implant are high, particularly with Medpor.60,62 Further, mechanical analyses of these implants with no functional or biological aim remain overlooked to this day.
In parallel, efforts have been made to produce rhinoplasty implants with improved tolerability, using degradable materials. For instance, PCL has successfully been used as a scaffold to accommodate and provide a mid-term structural basis for hydrogels. In a first study, it was expected that PCL scaffolds filled with alginate gels or decellularized cartilage ECM loaded with human adipose-derived stem cells would change shape in vivo over time as the PCL degraded. 75
However, in most reported cases, PCL scaffolds retained their structural integrity, 85 including after 12 weeks of implantation 75 (although the formation of neo-cartilage was not significant in this case). Although it is very difficult to perform in vivo studies that cover this time frame, studying the evolution of PCL biomaterials on the long run is an essential step before initiating human translation procedures. To circumvent the problems of premature degradation of biomaterials, PCL scaffolds were mixed with graphene, a non-resorbable material, to provide a long-term biocompatible porous and elastic material with antibacterial properties. 17
The production of a cartilage ECM by cells seeded onto medical devices is key to their acceptance by the host following implantation, and thus to their biocompatibility (Table 2). However, the production and remodeling of neo-synthesized ECM is likely to modify their mechanical properties over time. For example, the mechanical strength of type I collagen hydrogels was increased two-fold after a 5-week subcutaneous implantation in mice, possibly due to the production of ECM by seeded chondrocytes. 92
Similarly, alginate 23 or poly(glycolic acid) and poly-L-lactic 22 scaffolds containing chondrocytes and implanted subcutaneously in mice exhibited biomechanical properties that evolved toward those of native cartilage. The stiffness of alginate beads could also be improved by stimulating chondrocytes with growth factors. 89
Further, the combination of 3D printed alginate with cellulose, as well as chondrocytes co-cultured with bone marrow MSCs, showed improved maximum compression test (probably due to the neo-synthesis of the ECM, as the lifetime of natural polymers is expected to be short) over 60 days in vivo. 79 Finally, in the decellularized matrix as well, the stiffness of the artificial cartilage increased over 6 weeks to approach the stiffness of native nasal cartilage. 18
In vivo response
To further investigate the potential of these biomaterials to repair damaged nasal cartilage, orthotopic implantations were performed (Table 3), first along the nasal septum in New Zealand White rabbits.77,83,84,94 After 12 weeks, the PCL implants retained their shape and did not result in adverse distribution or inflammatory response.83,84 However, new cartilage ECM was not detected in significant amounts, with the presence of vascularization instead. 84
In comparison, biomolecule-based biomaterials, made from elastin/gelatin/hyaluronic acid composites 94 or photocrosslinked gelatin encapsulated with TGF-β1, 77 showed improved septum repair. Orthotopic implantation has also been performed on the nasal tip of rats. In this case, the PLGA/alginate/acellular gelatin composite scaffold was loaded with TGF-β3 to promote cellular homing of stem/progenitor cells from neighboring tissues, triggering cartilage tissue formation in the implanted scaffold. 101
In addition, orthotopic implantation has been studied in minipigs, where PCL constructs were grafted to the nasal periosteum, showing good tolerance and cartilage repair over 6 months. 82 We believe that orthotopic positioning of an entire artificial septum would help tissue engineers assess the ability of an implant to maintain nasal airway respiratory flow, but no animal model recapitulates the projected positioning of the human nose.
As an alternative, mechanical investigations could be conducted on cadavers. So far, in humans, implantation of synthetic nasal cartilage has been performed for restoration of the alar lobule after excision of skin cancer. 70 In this first human trial, autologous chondrocytes were cultured on collagen membranes in vitro and then implanted as a support under the skin, with satisfactory morphological and functional results, without adverse effects. Overall, these results indicate that medical devices developed for nasal cartilage engineering elicit an appropriate host response, thus meeting key criteria for biocompatibility.
Biocompatibility requirements for clinical application
Regulatory bodies, such as the Food and Drug Administration (FDA) in the USA and the European Medicines Agency (EMA), require specific tests to be carried out in accordance with a series of standards developed by the International Organization for Standardization (ISO) to guarantee biocompatibility. Specifically, ISO 10993 tests are generally required to assess the safety of the implant material and its interaction with the human body. Tests typically relevant to nasal cartilage implants include:
Cytotoxicity tests (ISO 10993–5) to assess the potential of the implant material or its extract to cause damage to cells. This is a pivotal prerequisite to the development of implants, and is routinely verified in tissue engineering studies for nasal cartilage repair both in vitro17–20,28,73,74,76,87–89,91,93 and in vivo.22–24,70,75,77–79,84,85,90,92,94
Implantation test (ISO 10993-6) to assess the tissue response to the implant material when implanted in the body. In a tissue engineering approach, this involves the progressive replacement of the biomaterial with neo-synthesized ECM. This aspect is notably central to the nasal cartilage repair studies reported in Table 2.
Sensitization test or reactivity test (ISO 10993-10) to assess the potential of the implant material or its extracts to cause allergic reactions, irritation, or inflammation. The lack of inflammation has been checked in vivo for implants made from PLGA, 78 poly(glycolic acid) and poly-L-lactic, 22 Poly(vinyl alcohol) and alginate, 90 hyaluronic acid and collagen, 24 elastin and gelatin, 94 fibrin 84 and PCL.82,83
Subacute and subchronic toxicity tests (ISO 10993-11) to assess the potential toxic effects of the implant material or its extract over a long period of exposure. The evolution of tissue engineering constructs in humans has so far been monitored up to 12 months and showed no adverse effects. 70
Future Research and Perspectives
Research on nasal cartilage engineering has suggested the possibility of generating a neo-synthesized ECM produced by cells seeded in biomaterials that replicate the characteristics of the native nasal septum. Such engineered cartilages constitute promising tools for the future development of medical devices that will assist surgeons in recapitulating the structural and respiratory function of the nose. Long-term mechanical measurements will help validate further the potential of candidate biomaterials for septum engineering.
Future research in nose regenerative medicine may also include the analysis of macrophagic response following implantation, to assess the inflammatory effects of biomaterial degradation by-products. In addition, the use of non- or minimally-invasive sensors would be of great interest for monitoring the quality of nasal cartilage reconstruction in vivo.
Biosensors that are being used in microfluidic tissue engineering platforms could be employed to monitor cartilage-specific macromolecule secretion, inflammatory or immune markers, and chondrocyte behavior in situ. Finally, the integration of the biomaterial into the native nasal mucosa will be crucial to provide the engineered cartilage with nutrients and establish the clinical applicability of the biomaterials envisioned for nasal septum reconstruction.
Footnotes
Acknowledgment
The author thanks Monique Billaud from the Innovation Conception et Accompagnement pour la Pédagogie (ICAP) of the University of Lyon 1 for providing the illustrations presented in this review.
Authorship Confirmation Statement
All authors confirm that the manuscript has been read, reviewed, and approved by all named authors, and that there are no other persons who satisfied the criteria for authorship but are not listed. The authors further confirm that the order of authors listed in the manuscript has been approved by all.
Authors' Contribution
D.V.-C.: conceptualization, funding acquisition, writing (original draft), and writing (review and editing); F.M.-G.: conceptualization, funding acquisition, project administration, writing (original draft), and writing (review and editing); E.P.-G.: funding acquisition, project administration; E.-J.C.: conceptualization; C.A.M.: funding acquisition; J.-D.M.: conceptualization, project administration, writing (original draft), and writing (review and editing).
Disclosure Statement
All authors confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
Funding Information
E.P.-G. and C.M. were supported by the “Fondation des Gueules Cassées” (2021); D.V.-C. was supported by the “Hospices Civils de Lyon” (2022); and F.M.-G. and J.-D.M. were supported by the Prematuration Program of the CNRS (2022).