
Abstract
Vascular surgery is facing a critical demand for novel vascular grafts that are biocompatible and thromboresistant. This urgency is particularly applicable to bypass operations involving small caliber vessels. In the realm of tissue engineering, the development of fully vascularized organs is promising as a solution to organ shortage for transplantation. To achieve this, it is essential to (re)construct a biocompatible and nonthrombogenic vascular network within these organs. In this systematic review, we identify, classify, and discuss basic principles and methods used to perform in vitro/ex vivo dynamic thrombogenicity testing of perfusable tissue-engineered organs and tissues. We conducted a preregistered systematic review of studies published in the last 23 years according to PRISMA-P Guidelines. This comprised a systematic data extraction, in-depth analysis, and risk of bias assessment of 116 included studies. We identified shaking (n = 28), flow loop (n = 17), ex vivo (arteriovenous shunt, n = 33), and dynamic in vitro models (n = 38) as the main approaches for thrombogenicity assessment. This comprehensive review reveals a prevalent lack of standardization and provides a valuable guide in the design of standardized experimental setups.
Impact Statement
The thrombogenicity of synthetic or biological engineered organs and tissues is the primary obstacle to their integration into clinical applications and should be properly examined. This review outlines the technical aspects associated with each method commonly implemented for dynamic thrombogenicity testing. Readers can learn about the experimental setup implemented in the main four methods, including shaking, flow loop, ex vivo dynamic perfusion, and arteriovenous shunts. Each table depicts detailed information on relevant parameters for each method. We are confident that this review will contribute to increasing standardization in the field and aid researchers in the process of conception and experiment design.
Introduction
Peripheral artery disease (PAD) is a global concern of the 21st century and is associated with a high morbidity and mortality. In cases of a vascular occlusion exceeding 70%, the restoration of blood flow through interventional endovascular therapy or bypass surgery is required. Autologous veins, the current gold standard, are not available in 30% of the cases. 1 It is imperative to develop novel vascular prostheses that exhibit lower inherent thrombogenicity than current synthetic ones. This is not only crucial in the field of vascular surgery but also in the broader domain of tissue engineering (TE) for whole organ development. TE of whole vascularized organs involving techniques such as de- and recellularization, as well as 3D printing, has emerged as an important attempt to address the long waiting list for suitable organs for transplantation.2–4 These three-dimensional structures, encompassing a well-preserved acellular vascular tree, hold immense potential for repurposing into autologous, personalized organs, vessels, or tissues.5–8 In addition to recellularizing with organotypical cells to generate bioengineered lungs and livers,9–11 a decellularized small animal (e.g., rat) liver or lung can be repurposed into a functional endocrine neo-pancreas by seeding the parenchymal compartment with islets of Langerhans.12,13
An inherent limitation of all these tissue-engineered constructs is the absence of the natural endothelium that lines the vascular tree and prevents thrombus formation by establishing a highly nonthrombogenic microenvironment. 14 A particular concern arises due to the thrombogenic nature of the basement membrane exposed upon the removal of the endothelial cells through decellularization. 14 Failure to rebuild a perfusable, thromboresistant vascular network would negatively affect the viability and function of engineered organs and tissues.6,15 Therefore, thorough examination of the graft surface through in vitro/ex vivo thrombogenicity testing is crucial to address this issue. As there are various methods to construct the graft surface, please refer to the separate studies for its specific qualities (natural vs. hybrid vs. synthetic material; smooth vs. rough; fiber structure vs. a continuous porous or nonporous material), because these are all crucial components that can determine the success of cell adhesion, surface functionalization, and intrinsic thrombogenicity. 16
The primary aim of this systematic review is to analyze, categorize, and compare studies conducted in the last 20 years that focus on performing in vitro/ex vivo thrombogenicity testing of perfusable tissue-engineered or 3D printed vessels, organs, and tissues. Initially, we distinguish between static and dynamic thrombogenicity testing and subsequently investigate the methods used for dynamic in vitro/ex vivo testing. These methods are classified into four groups as follows: shaking, dynamic in vitro perfusion systems, flow loop models, and ex vivo perfusion models (arteriovenous shunts, AV shunts). Finally, we conduct a comprehensive analysis and comparison of these groups, considering experimental parameters such as flow rate, use of whole blood/blood components, perfusion duration, as well as selected readout parameters and their corresponding results.
Methods
Protocol registration
Our study followed the steps recommended in the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist. 17 The protocol for this study was published on the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42022306465 in March 2022.
Search strategy
The systematic research for this study was performed on PubMed®. The Boolean Search was carried out using the following search term:
((decell*[tw] OR recell*[tw] OR “tissue engineered organ*”[tw] OR “tissue engineering” [MeSH] OR “bioartificial organs” [MeSH] OR “blood vessel prosthesis” [MeSH] OR “vascular graft”[tw]) AND (thrombogenicity[tw] OR hemocompatibility[tw] OR thromboresistance[tw] OR “thrombogenicity testing*”[tw] OR “platelet activation”[tw] OR “platelet adhesion” [tw] OR “platelet attachment” [tw] OR “blood coagulation tests” [MeSH] OR “whole blood perfusion” [tw])) NOT (Review [Publication Type]).
A restriction filter was applied to include only studies published after 2000. An initial PubMed® search was performed on the 13th of January, 2022, and a final PubMed® search was carried out on the 4th of March, 2023, to include all recently published studies. In addition, a manual search was performed by screening reference lists of relevant publications. The entire search strategy and selection process is provided in Figure 1. No further restrictions were applied inside the final publication date range from 2000 to 2023.

Process of selection of studies included in the systematic review. From 711 detected studies, only 116 studies fulfilled our inclusion criteria. In total, 278 of the identified studies were excluded because they reported static in vitro (n = 166) and in vivo (n = 112) thrombogenicity testing.
Selection criteria
The criteria for including studies in our systematic review were as follows:
The publication of the study is available in full text. The published article is available in English. To ensure that our systematic review reflects the current state of the art in thrombogenicity testing of anastomosable tissue-engineered constructs, we included studies that were published after the year 2000. Only original articles are included. The study makes methods for thrombogenicity testing of implantable, anastomosable tissue-engineered constructs subject of discussion.
The exclusion criteria were as follows:
The article is a review, meta-analysis, lecture speech, abstract only, or clinical trial. The article refers to any topic other than thrombogenicity testing of perfusable, implantable tissue-engineered constructs. The approach for thrombogenicity testing is not intended for tissue-engineered implantable organs or constructs. The approach for thrombogenicity testing involves static or in vivo experimentation. The approach involves TE of heart valves.
The screening process of the studies involved three independent reviewers (L.H., Y.Z., and E.K.) who screened the titles and abstracts. During this stage, studies that did not perform thrombogenicity testing and studies that focused solely on static or in vivo thrombogenicity testing were excluded. The full texts of the remaining articles were then thoroughly examined and divided into the four method groups. Any uncertainties were resolved through discussions with the other reviewers and the supervisor (K.H.), leading to a final decision.
Data extraction
Data extraction from the included articles was performed by three independent reviewers (L.H., Y.Z., and E.K.) and recorded in a specifically designed table. In case of discrepancies the reviewers engaged in discussions to reach a consensus. If a consensus could not be reached, the supervisor (K.H.) was consulted to facilitate resolution and ensure agreement among the reviewers.
Risk of bias assessment
Despite conducting thorough research, we were unable to identify a specific tool for assessing the risk of bias that was tailored to our study’s requirements. Therefore, we adapted an evaluation approach based on a previous study. 18 We considered parameters commonly employed in multiple tools frequently used for assessing the risk of bias, including the Cochrane Collaboration, Joana Briggs Institute Clinical Appraisal for experimental studies, QUADAS Tool, Timmer’s Analysis Tool, and OHAT Tool. 19
The parameters used for quality assessment were categorized into four groups. First, we assessed whether the study clearly presented the rationale for the conducted research. Second, we evaluated the quality of sample preparation, which in our case refers to the tissue-engineered organ/tissue and the assessment of hemocompatibility. Third, the quality of experimental procedures used to evaluate thrombogenicity testing was assessed. Finally, we examined whether the study reported the results in a complete and comprehensive manner. The scoring system for assessing the risk of bias in the included studies was as follows: If a specific parameter was clearly reported, the article received a score of 0 for that parameter. If a parameter was reported but was inadequate or unclear, the article received a score of 1. If it was not possible to find the information, the article received a score of 2. Based on these scores, articles were categorized as having a low risk of bias (scores 0–6), medium risk of bias (scores 7–13), or high risk of bias (scores 14–20). Two reviewers (E.K. and L.H.) independently evaluated the risk of bias for all the studies. The scores assigned by each reviewer were then compared, and in case of discrepancies, they were discussed to reach a final decision. If a consensus could not be reached, a third reviewer (K.H.) was consulted to provide input and help to make a final determination.
Results
Our initial PubMed® search yielded 711 studies related to thrombogenicity testing of tissue-engineered constructs published in the last 20 years. A total of 322 studies that were not relevant and 279 studies that implemented only static (n = 167) or in vivo (n = 112) testing were excluded from our final analysis. A total of 110 studies met the inclusion criteria for our systematic review. In addition, a manual search discovered 6 relevant studies, bringing the total number of included studies to 116 (Fig. 1).
We identified the following four primary systems commonly utilized for in vitro/ex vivo dynamic thrombogenicity testing: 1. Shaking: agitated and incubation models, 2. Dynamic in vitro perfusion systems, 3. Flow loop models, and 4. Ex vivo perfusion models (AV shunts). In the final analysis, we summarized the key aspects of each model, including the main concept and experimental setup, and the relevant readout parameters. As depicted in Figure 2, 14 studies that reported using more than one of the four methods performed shaking experiments complemented by flow loop, dynamic in vitro or ex vivo experiment. The rest (n = 102) of our included studies focused solely on one method. For context, in vivo experiments, which were performed as an additional method in several of the included studies but are not subject of this review, are also represented in Figure 2.
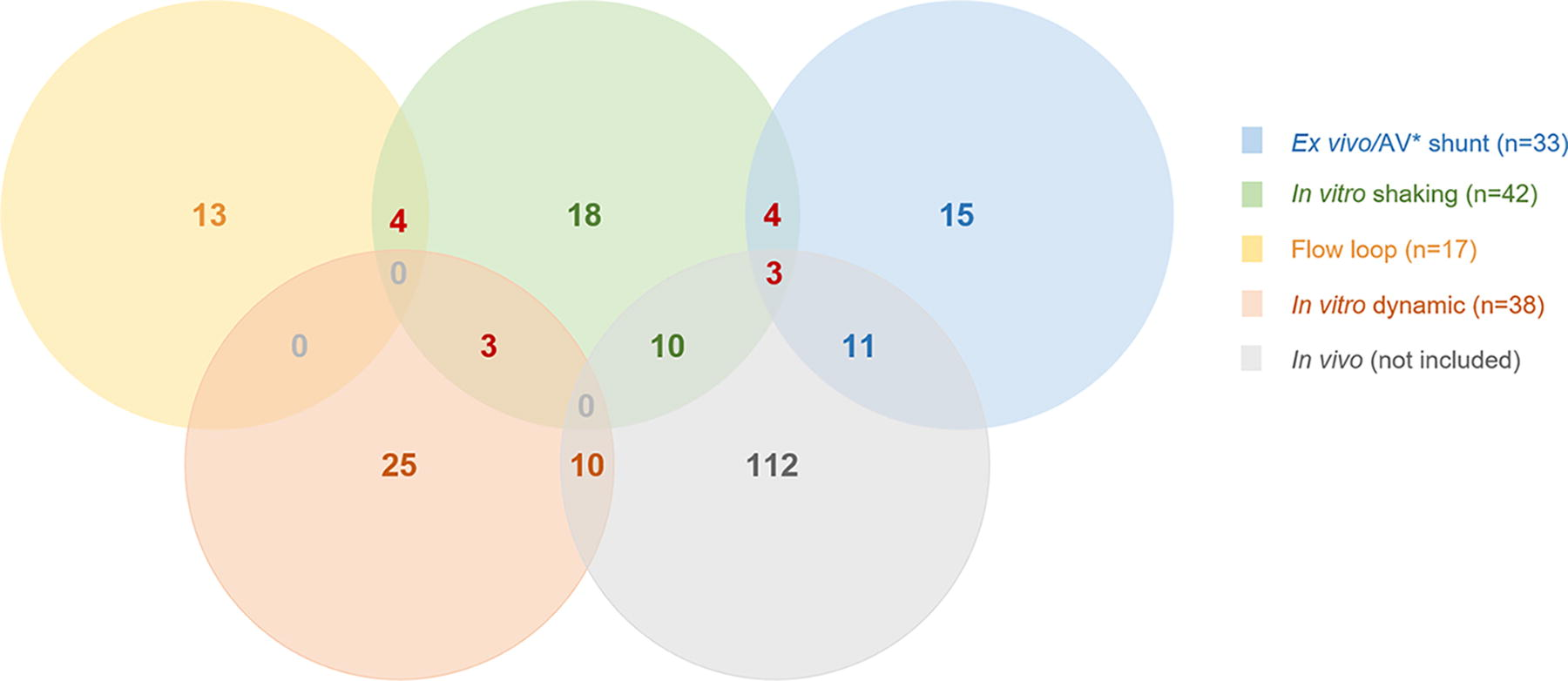
Distribution of methods selected to perform thrombogenicity testing. In total, 116 studies performed dynamic in vitro thrombogenicity testing. Of these, 28 performed shaking, 17 studies implemented flow loops, 38 dynamic in vitro testing, and 32 studies implemented ex vivo AV shunts. Of these, four studies performed both shaking and flow loop, three performed shaking and in vitro dynamic perfusion, and four studies performed shaking followed by AV shunt. Importantly, many studies performed in vivo evaluation of the tissue-engineered construct as supplementary to in vitro shaking (n = 10) and AV shunt (n = 11). Three studies implemented shaking, AV shunt, and in vivo evaluation for thrombogenicity testing.
Figure 3 is a graphical depiction of the four identified methods and the most commonly used experimental models within each. It is worth noting that all studies included in our analysis are referenced in their respective tables, so they will not be individually cited when mentioned in the following sections (Tables 1–4).

Graphical representation of the experimental setups most commonly implemented for thrombogenicity testing R2.1. and their advantages and disadvantages, including a sequential progression from syringe perfusion systems, to flow loop systems and complex dynamic perfusion systems, inTY -55 TYcluding whole organ perfusion models, to AV Shunt Models as the last phase prior to in vivo evaluation.
Studies Performing in Vitro Thrombogenicity Testing Using Shaking
The majority of studies included in our systematic review demonstrated low risk of bias (Supplementary Tables S1, S2, S3, and S4, Supplementary Data S1). The most common areas of potential bias were related to the description of sample size and the evaluation of identical procedures within different groups. In addition, studies that performed shaking and dynamic testing exhibited some risks of bias in terms of “Full description of procedure” and “Ability for replication.”
Shaking: agitated and incubation models
Agitated or shaking incubation models are considered a simple semistatic method for conducting thrombogenicity testing. Among the evaluated studies, a total of 42 publications reported the use of an agitated incubation model for thrombogenicity testing (Table 1). Eighteen of these reported shaking experiments either in isolation or in combination with static methods, whereas the remaining studies used shaking as a supplementary technique (Fig. 3).
Experimental setup
While shaking models are relatively simple in design, there are several important variables to consider in the experimental setup. These variables include the following:
Surface area to blood volume ratio: Most experimental setups (n = 19) utilize standard tissue culture well plates (12–96 wells) with flat sample sheets, discs, or coated films placed at the bottom of the wells. The wells are then filled with a specific volume of blood or blood-like fluid. Movement mode and speed: Common modes of agitation include shaking or rocking (n = 30). The speed of agitation can vary, with commonly used parameters ranging from 50 to 200 rounds/min (rpm) on horizontally or orbitally moving shaker plates (n = 10). Temperature: Incubation temperature is a critical parameter to mimic physiological conditions. The majority of studies (36 of 42 studies) indicated an incubation temperature of 37°C. Only 2 studies reported setups at room temperature. Incubation period: The duration of shaking experiments directly affects platelet aggregation and clotting processes. Most experiments were conducted for 30 min (n = 10), 60 min (n = 22), or 120 min (n = 11). It is important to note that short shaking experiments are typically performed in combination with longer incubation durations (≥30 min, n = 4) to allow sufficient time for clotting processes. In contrast, incubations longer than 120 min were not reported.
Importantly, some studies lacked a detailed description of the experimental setup, providing limited information such as “gentle shaking” without specifying the direction or speed of shaking. In addition, a few studies utilized closed incubation chambers or tubes that can be fully filled with blood and rotated overhead (1–6.6 rpm) to minimize air contact and cell sedimentation (n = 4).
Implication, efficacy, and limitations
Shaking models are frequently used for evaluating the thrombogenic potential of flat material sheets or coated surfaces. While the majority of experiments are conducted with human blood (n = 25), rabbit blood is also used (n = 8). Platelet suspension (n = 32) is the preferred method over whole blood perfusion (n = 14). Scanning electron microscopy (SEM) is used to assess platelet adhesion, the readout parameter of choice for characterizing thrombogenicity in 34 out of 42 evaluated studies. While introduction of agitation and blood movement into the experimental design allows for a more accurate replication of physiological thrombus formation and prevents the sedimentation of blood cells, these models typically lack directed flow and defined shear stress rates. The latter constitutes the main limitation of shaking models.
Dynamic in vitro perfusion systems
To minimize the blood volume required many dynamic in vitro perfusion setups are designed as closed systems (n = 17). The blood is recycled and circulated through the circuit, including the test section, multiple times. In general, a custom-made circuit is used. Hollow circuit tubing, often constructed from flexible poly- or elastomer materials, is used to connect the test section with other components of the circuit. Pumps (n = 14) and reservoirs (n = 8) were commonly used components in the circuits. To maintain physiological conditions, the system was typically kept at 37°C using a water bath or an incubator chamber (n = 12). In recirculating systems, flow was predominantly generated using roller pumps, which allowed researchers to simulate flow conditions, system pressure, and shear rates based on the intended clinical application of the material being tested. Perfusion rates ranged from 6 to 200 mL/min, and shear rates of up to 1000/s were reported. Perfusion durations varied, ranging from 15 min to 2 days. While the majority (n = 12) reported durations of ≤120 min, three studies reported longer durations of 3 to 6 h, and only one study reported a perfusion time of 2 days 90 (Table 2).
Studies Performing in Vitro Thrombogenicity Testing Using Dynamic Perfusion
In vitro single pass perfusions are characterized by simple and short flow paths (n = 6). A common approach involves tightly attaching the test graft or perfusion chamber to a syringe pump. The flow is generated either from the syringe itself (n = 3), where the previously filled syringe is emptied through the test section into a collecting vessel, or toward the syringe (n = 3), where blood is drawn from a reservoir through the test section into the syringe. The shear rates can be adjusted by controlling the expulsion speed or suction force of the syringe pump. Reported durations for single pass perfusions did not exceed 5 min, with two publications not specifying the exact time.
Perfusion of tissue-engineered whole organs (8 studies) presents a unique scenario for thrombogenicity testing. A common approach involves single-pass perfusions using diluted whole blood (reported in 5 studies). In addition, alternative perfusion strategies have been reported, including heavily heparinized blood (10 IU/mL, n = 1), citrated strained blood (n = 1), and platelet-rich plasma (n = 1). The blood is infused through a cannulated vessel at a very low speed (<10 mL/min, n = 3) either with a peristaltic pump or manually using a syringe. During the blood infusion, the pressure in the vascular system can serve as an indicator of resistance due to thrombus formation. Subsequently, the blood exits the organ’s vascular tree through the venous system and can be collected for further analysis. Suitable readout parameters to indicate thrombogenic processes include blood clearance, arterial or venous resistance, as well as micro and macroscopic assessment, for platelet adhesion and clot formation. Thrombogenicity testing of whole organs is typically conducted preimplantation using blood of the corresponding animal model used (n = 6) (Table 2).
Implication, efficacy, and limitations
Dynamic thrombogenicity testing is the standard procedure for perfusable tissue-engineered constructs. The hemodynamic variables highly depend on the specific experimental setup and chamber geometries, so they must be tailored accordingly. The perfusion rates ranged from 6 to 200 mL/min, and the shear rates reached up to 1000/s. The majority of studies utilized human blood (n = 16) or porcine blood (n = 5), either as anticoagulated whole blood (n = 14) or as Platelet rich plasma (n = 8). Assessment of platelet adhesion and activation on the exposed biomaterial surface was a common element in postexperimental analysis in most studies, typically performed using techniques such as Scanning electron microscopy, fluorescence microscopy, or immunohistochemical staining. Flow cytometric analysis and enzyme assays of the perfusate are also frequently used to determine platelet activation. However, there are significant limitations to this method. First, inconsistencies in reporting of flow and shear rates across studies and on variations in terms of blood preparation, anticoagulation methods, and platelet concentrations make it difficult to compare the results. Second, there is a wide range of readout parameters used, and it is rare to find two studies using exactly the same endpoints. Therefore, lack of standardization is a significant issue.
Flow loop models
Seventeen publications reported the use of flow loop models (Table 3). The loop configuration facilitates the generation of flow resembling the conditions observed at vessel curvatures and bifurcations. Notably, thrombi formed in flow loops exhibit morphological and biochemical characteristics similar to those formed in vivo. 136 The Chandler loop, invented by A.B. Chandler as an in vitro model for thrombus formation, was first described in a landmark study published in 1958. Since then, the original design has been modified in various ways, leading to inconsistent usage of the term “Chandler loop” and the distinction from a modified Chandler loop in studies published over the past 22 years. Due to the lack of standardized loop designs and terminology, this systematic review groups similar flow loop designs together for simplicity (Table 3).
Studies Performing in Vitro Thrombogenicity Testing Using Flow Loops
Experimental setups
Flow loops generally comprise a hollow tubing circuit, with the tube ends firmly connected, creating a self-contained circulatory system. Commonly, silicone or polyvinyl chloride (PVC) tubing is used. The length and diameter of the circuit tubing can be adjusted and, in most cases, fall within the range of 40 cm (n = 8) to 50 cm (n = 7) in length, with an inner diameter of 5 ± 1.5 mm. To minimize cell activation and thrombus formation, a firm end-to-end tubing connection causing minimal turbulence is favorable. This is typically achieved by fitting an external cuff with an inner diameter precisely matching the outer diameter of the loop tubing (n = 8). Alternatively, Luer locks and metal connectors may be used (n = 3). The circuit tubing itself can be composed of the tested biomaterial or it may incorporate an inserted test section (n = 2 and n = 15, respectively). Stents allow convenient insertion through their own release mechanism, and tubular grafts can be anastomosed to the circuit tubing with connectors. If the shape of the material being tested does not permit the mentioned methods, small samples can be placed tightly inside the tubing. For extra stability, the Chandler Loop System® suggests securing difficult material probes with an external fixation cuff. After assembly, the loop is filled with blood and placed in a 37°C water bath (n = 16). Only one study reported incubation at ambient temperature. 51 Three distinct mechanisms have been reported for generating flow in loop setups: rotation (n = 12), utilization of a roller pump (n = 3), or implementation of a unidirectional valve (n = 2).
Implication, efficacy, and limitations
These models are implemented exclusively for perfusable tissue-engineered structures. They offer a standardized approach and allow for the simulation of physiological flow conditions by incorporating various hemodynamic variables. The most commonly reported perfusion time was 60 min (n = 10). Perfusion durations exceeding 60 min were exclusively reported in rotating loop setups (n = 6). Fifteen studies utilized human whole blood for their experiments. One study employed human PRP, whereas another used rabbit whole blood. The anticoagulant concentration was chosen based on the specific experimental conditions. In rotating loops, it was found that low anticoagulant concentrations of 0.5 IU heparin per mL of human blood (n = 4 studies), or even no anticoagulation at all in rabbit blood (n = 1), were sufficient for a 60-min perfusion. However, for longer perfusion durations, heparin concentrations at or above 1 IU/mL (n = 6) were utilized. The main endpoint was platelet adhesion (n = 13), which was determined by examining the biomaterial surface or indirectly by assessing the platelet count in the perfusate. Platelet activation (n = 12) and coagulation activation (n = 8) are also commonly evaluated endpoints. In some cases, formed thrombi were assessed for weight and morphology (n = 3) as an alternative measure.
Ex vivo perfusion models
Ex vivo perfusions occupy a unique position between in vitro and in vivo methods, offering one of the best approaches to simulate physiological conditions for thrombogenicity testing of perfusable constructs. Continuous and direct perfusion with freshly supplied blood from a living organism bypasses the need for blood collection, processing, and storage, which can potentially activate blood components prior to the start of the experiment. The experimental setups vary considerably across studies, with notable differences observed in the choice of animal model, circuit assembly, and method of flow generation. Notably, only two studies reported performing an ex vivo perfusion in a human model.
Experimental setups
The majority of ex vivo perfusion setups are based on AV shunts, whereby a short circuit within the arteriovenous system is established to perfuse an interposed test section (n = 31 studies, Table 4). In this setup, one end of the circuit tubing is connected to an artery, whereas the other end is connected to a vein, creating a shunt between the two systems. Blood flows from the artery through the tubing and is subsequently returned to a vein of the animal’s cardiovascular system, allowing for recirculation. In animal models, AV shunt catheters are typically connected unilaterally or bilaterally to the femoral artery and vein (n = 17), or to the carotid artery and jugular vein (n = 8), with less common placement in abdominal vessels (n = 4).
AV shunts are primarily utilized for thrombogenicity testing of tubular vascular grafts, with a lesser extent for the application of stents (n = 26 and n = 4, respectively). In certain cases, a shunt with multiple parallel flow paths allows for simultaneous perfusion of two or more grafts (n = 2). If the level of platelet deposition on the material is insufficient, a thrombogenic source such as a collagen coated graft can be interposed upstream of the test section in order to accentuate differences in thrombogenic behavior (n = 1).
Studies Performing Ex Vivo Thrombogenicity Testing Using Ex Vivo Dynamic Models
Two publications introduced an ex vivo perfusion method that deviates from the traditional shunt connection approach, where blood is not returned to the cardiovascular system after perfusion. Instead, this method involves connecting one end of the test section to a vein, rather than an artery, and attaching the other end to a syringe. By gently aspirating the syringe, blood flows from the vascular system over the test surface into the syringe. In a goat model using a parallel plate perfusion chamber with four channels, perfusion was performed for 30 s at a rate of 12.5 mL/min from the jugular vein. 134 Similarly, in a human model perfusing a single tubular vascular graft, perfusion was conducted for 6 min at a rate of 20 mL/min from the antecubital vein. 135
Implication, efficacy, and limitations
The experimental setups vary considerably across studies. There are notable differences observed in the choice of animal model, circuit assembly, and method of flow generation. Only two studies reported performing an ex vivo perfusion in a human model.
Discussion
The lack of standardization in methods used for in vitro/ex vivo assessment of thrombogenicity is immense. In this systematic review, we provide a comprehensive overview of the experimental setups, the types of blood or blood-like fluids used, and the readout parameters utilized. To the best of our knowledge, this is the first study to systematically depict such an overview in this field.
Although agitated shaking and incubation models are among the simplest methods for in vitro testing, drawbacks such as the presence of a relatively large blood–air surface can lead to premature protein and platelet aggregation.137,138 Moreover, the flow paths are nonuniform and chaotic, lacking the ability to create directed flow and defined shear rates, which are essential in physiological thrombus formation. Our findings demonstrate that shaking can be effectively utilized for thrombogenicity testing of planar material films and coatings. However, it remains insufficient for comprehensive characterization of a biomaterial’s thrombogenic potential. Ideally, it should be complemented with other dynamic testing methods such as flow-loop studies for better simulation of physiological conditions, prior to in vivo evaluation.
In contrast, in vitro dynamic perfusion systems are also far from perfect and display issues such as hemolysis and platelet and leukocyte activation due to micromechanical (shear) stress during circulation. 51 This shear stress is a crucial factor in premature cell activation and thrombus formation, interfering with the results of thrombogenicity testing.
Single-pass perfusions and pumpless systems, such as AV shunts, offer advantages by avoiding pump-induced blood damage and providing consistent experimental conditions throughout the perfusion. However, the requirement for high blood volumes to achieve physiological shear rates limits the suitability of single-pass experiments for extended perfusion experiments, particularly when using scarce human blood resources. In addition, invasive procedures like surgical shunt placement raise ethical concerns, making large scale testing, especially in human models, challenging.
Moreover, in the absence of a test section, the flow system itself can induce platelet and leukocyte activation. To assess cell activation and determine appropriate perfusion times and experimental settings, flow cytometric examination of the perfusate after various circulation times and conditions can be used. 72 Computational fluid dynamics (CFD) is a widely utilized method for describing and analyzing fluid flow using numerical solution models. 139 CFD simulations enable the prediction of flow dynamics in tubular grafts and the cardiovascular system by calculating velocity, pressure, temperature, and density of the moving fluid. Interestingly, our search identified only two studies that implemented CFD to test thrombogenicity in perfusable and implantable tissue-engineered constructs.51,75 Indeed, dynamic perfusion designs have highly diverse setups, varying from simple to highly complex designs. Controlling and coordinating the numerous interrelated variables are challenging, particularly as the system complexity increases. Tables 2, 3, and 4 demonstrate that many studies involving flow loops, AV shunts, and dynamic testing only reported flow rates while failing to provide crucial information on shear stresses. This lack of data and flow monitoring significantly hinders the interpretability and reproducibility of measurements, while compromising the validity of reported findings—especially for future in vivo applications. Dynamic perfusion studies are indispensable, and flow loops are the better standardized version. Following static thrombogenicity testing or shaking for further construct characterization, implementation of this step should be associated with an exact description of the duration of perfusion and applied shear stress to allow replication.
Finally, it is crucial to consider species-specific rheologic characteristics and respective variations in coagulation mechanisms when selecting an animal model for thrombogenicity testing. In addition, it is essential to account for inherent physiological differences between animal models and humans when interpreting results for future clinical translation. Indeed, to cope with biological variability and achieve reliable and significant data, much higher numbers of experiments with (nonpooled) human blood samples are required than experiments in cell culture or pooled blood experiments. In addition to physiological similarity, the selection of an appropriate animal model should take into account various other criteria, including ease of handling, cost, availability, and ethical considerations. For further information and guidance on choosing suitable animal models for specific experimental designs, dedicated publications addressing this topic can be referenced.140,141 These publications provide valuable insights and recommendations to aid in the selection process.
Our review clearly depicts the lack of standardization but fails to select or divide one approach as the solution to the problem that could or should be implemented as the method of choice for thrombogenicity testing. Although identifying one main approach was our aim at the beginning, we were unprepared for the great variety that we would encounter in all steps involved in thrombogenicity testing, including experimental setups, duration of exposure to blood, implementation of blood or blood-like fluids, and selected endpoints and assessment methods. It is evident that flow loops and AV shunts represent the well-established and standardized methods for dynamic in vitro/ex vivo thrombogenicity testing. However, the majority of studies continue to rely on static in vitro and in vivo assessments for thrombogenicity evaluation. Prior to in vivo evaluation, conducting in vitro/ex vivo thrombogenicity testing is crucial to identify and eliminate constructs that may fail after implantation, thereby preventing unnecessary animal testing and facilitating more targeted modifications to improve construct performance. 142 While static thrombogenicity testing is commonly implemented in hemocompatibility studies, it fails to replicate in vivo physiological processes due to the absence of blood flow.142,143 In line with existing literature, most studies in our search (n = 167) used this method by incubating fresh blood or PRP with the construct surface at 37°C, mimicking physiological conditions. 142 However, static thrombogenicity testing suffers from several limitations that can compromise the validity of the results, such as nonspecific platelet activation resulting from the large blood–air interface and extensive cell sedimentation. A major drawback identified in our systematic review is the infrequent follow-up of static testing with dynamic or in vivo assessment. In addition, our search revealed 112 studies that solely relied on implantation as the chosen method for evaluating hemocompatibility. Although in vivo thrombogenicity testing serves as the currently undisputed gold standard, it is associated with high risk of failure and difficulties in identifying and addressing mechanistic problems that require further development.
Based on the data, we propose that a simple way to standardize thrombogenicity testing is to include a sequential progression from in vitro static thrombogenicity testing to in vitro and ex vivo dynamic testing, culminating in in vivo evaluation as the final and most comprehensive method. As depicted in Figure 2, some studies have already organized their experiments based on this logic. For further standardization, we suggest implementation of human blood for testing. Although this would avoid conflicting results when performing animal-based in vitro and human-based in vivo experimentation, higher numbers of experiments for both in vitro and in vivo setups are required due to high donor variability.
Besides perfecting and standardizing the current methods used for thrombogenicity testing, we propose that attempts should also be made at discovering novel ones that ideally address downsides of existing setups. For example, branched flow models could be implemented for cylindrical tissue-engineered scaffolds that can occlude due to thrombosis, in order to imitate physiological collateralization. 144 Moreover, a study showing a flow-enhanced vascularization in a kidney organoid used fluorescent beads to show perfusability of the novel vascular tree. 145 Although thromboresistance was not tested here, a similar setup could be used to assess platelet adhesion in single pass thrombogenicity studies.
Limitations and Conclusion
Our initial intention was to incorporate perfusable 3D printed constructs and tissues into the analysis. Regrettably, none of the identified studies met our inclusion criteria, which required both perfusability and thrombogenicity testing, as these constructs were predominantly subcutaneously implanted rather than being suitable for perfusion-based assessments. Thus, this study can serve as an incentive to initiate and establish thrombogenicity assessment of perfusable 3D printed constructs.
In conclusion, our comprehensive systematic analysis has highlighted not only a lack of standardization between studies but also the insufficient detail provided on in vitro/ex vivo experimental setups widely implemented for thrombogenicity assessment. Among the various methods evaluated, flow loops and ex vivo AV shunts emerged as the most standardized approaches. The key promise which these methods can deliver is high consistency and physiologically relevant experimental conditions. However, we firmly believe that our findings can serve as a valuable guide during the experimental design process and contribute significantly to the ongoing efforts toward standardization of thrombogenicity assessment.
Footnotes
Acknowledgments
Luna Haderer is BIH-Medical Doctoral Research scholarship holder funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. Dr. Eriselda Keshi and Dr. Karl Hillebrandt is a participant in the BIH-Charité Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health. The author acknowledges the support of the Cluster of Excellence »Matters of Activity. Image Space Material« funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany’s Excellence Strategy—EXC 2025—390648296.
Authors’ Contributions
L.H. and Y.Z. had a crucial role in performing the literature research, classification of the articles, performing the risk of bias analysis, and writing the article. P.T. helped during all parts of the project, helped in writing the article, and proofread the article. A.D. had an important role in developing the methodology and proofread the article. B.G. helped in performing the final analysis and proofread the article. F.K. helped with conceptualization of the tables and proofread the article. A.R.S. extensively discussed results and proofread the final version of the article. M.W. supervised the ideation and design of the systematic review and proofread the article. J.P. discussed the results and proofread the article. I.M.S. developed the project idea, discussed the results, proofread the article, and is the guarantor of this study. K.H.H. and E.K. were involved during all parts of the project, discussed the results, and proofread the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was required to support this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.