
Abstract
Autologous fat grafting is a common procedure in plastic, reconstructive, and aesthetic surgery. However, it is frequently associated with an unpredictable resorption rate of the graft depending on the engraftment kinetics. This, in turn, is determined by the interaction of the grafted adipose tissue with the tissue at the recipient site. Accordingly, preconditioning strategies have been developed following the principle of exposing these tissues in the pretransplantation phase to stimuli inducing endogenous protective and regenerative cellular adaptations, such as the upregulation of stress-response genes or the release of cytokines and growth factors. As summarized in the present review, these stimuli include hypoxia, dietary restriction, local mechanical stress, heat, and exposure to fractional carbon dioxide laser. Preclinical studies show that they promote cell viability, adipogenesis, and angiogenesis, while reducing inflammation, fibrosis, and cyst formation, resulting in a higher survival rate and quality of fat grafts in different experimental settings. Hence, preconditioning represents a promising approach to improve the outcome of fat grafting in future clinical practice. For this purpose, it is necessary to establish standardized preconditioning protocols for specific clinical applications that are efficient, safe, and easy to implement into routine procedures.
Impact Statement
The present review provides an overview of preconditioning strategies in fat grafting. In preclinical studies, these strategies have already been shown to improve the survival of transplanted adipose tissue by activating tissue-protective mechanisms. Hence, these strategies may markedly contribute to improve the future clinical success rates of common surgical interventions in plastic and reconstructive surgery.
Introduction
First introduced in 1893 by the German surgeon Gustav Adolf Neuber, 1 autologous fat grafting is a common technique in plastic and reconstructive surgery for a broad spectrum of therapeutic approaches (Fig. 1). These include the treatment of scars, wounds, and congenital deformities as well as postsurgical organ reconstruction and contour improvement, for instance, in the breast.2–6 Furthermore, autologous fat grafting is widely used for regenerative and antiaging purposes,7–10 as adipose tissue is considered an ideal soft tissue filler with a high regenerative capacity. 11 Moreover, it can easily be harvested in large quantities by means of minimally invasive procedures. In addition, it is nonallergic and nontoxic and, thus, exhibits an ideal biocompatibility in contrast to many artificial biomaterial implants.11,12 Finally, fat is a rich source of growth factors, adipose-derived stem cells (ASCs), and microvessels that contribute to its strong regenerative capacity.13,14

Clinical examples of autologous fat grafting.
However, fat grafting is also associated with certain problems, such as the unpredictable resorption rate, fibrosis, and microcalcification of the grafted tissue.15–18 Their incidence is dependent on the engraftment kinetics of fat tissue, which is crucially determined by the close interaction of the graft with the surrounding tissue at the recipient site. In fact, during the initial phase of engraftment, transplanted adipose tissue lacks its own blood supply and, thus, is nourished only by passive oxygen and nutrient diffusion.19,20 Accordingly, adipocytes located in the central zone of the graft are at risk of ischemia-induced cell death. Of interest, these adipocytes can be partly replaced by ASCs that are more resistant to hypoxia. 21 This results in three distinct zones within the graft, that is (1) the peripheral survival zone, where both adipocytes and ASCs survive, (2) the intermediate regenerative zone, where ASCs replace dead adipocytes, and (3) the central necrotic zone, which is characterized by fibrosis due to the death of both adipocytes and ASCs (Fig. 2). 22 The ratio between the necrotic and surviving or regenerating zones of the graft determines the final volume retention rate.

Immunohistochemical analysis of adipocyte viability in grafted adipose tissue in a mouse model according to Eto et al. 22 Three samples seen in each row were obtained from three different mice at different time points. The area filled with viable adipocytes (strongly positive for perilipin) is colored in red, the area filled with dying adipocytes (weakly positive) is shown in yellow and the area of dead adipocytes or connective tissue (negative area) is shown in black. The red area was dramatically reduced on day 1 and most of the yellow area had disappeared by day 5. Scale bars: 1 mm. Reprinted from Eto et al. 22 with permission from Wolters Kluwer Health, Inc.
Under ideal circumstances, the maximum depth of the regenerative zone is 1.6 mm. 23 Hence, larger grafts will invariably suffer from central necrosis since oxygen diffusion is limited by the reduced interface between the graft and the host tissue as well as the maximum diffusion distance of oxygen. 4 Furthermore, the pressure resulting from the transplantation of large amounts of adipose tissue in a closed compartment increases the risk of ischemia. 20 This is even more important in case of hostile recipient sites that are characterized by poorly vascularized, fibrotic host tissue due to previous trauma or radiotherapy. In this scenario, the grafted tissue is subject to severe ischemic conditions, resulting in higher resorption rates and eventually less volume retention.24,25
To overcome these problems, several promising strategies have been developed in recent years to enhance the survival rate of fat grafts. These include the enrichment of the grafted tissue and/or the recipient tissue with growth factors, stem cells, microvascular fragments, or active gels, which directly induce biological effects in these target tissues, as previously reviewed in detail. 26 Alternatively, the tissues may be exposed to different stimuli before transplantation to trigger endogenous responses, which finally also result in beneficial biological outcomes in the posttransplantation phase, referred to as preconditioning. The present review provides an overview of such preconditioning strategies (Fig. 3, Table 1), which have been evaluated in different experimental settings to improve the outcome of future clinical fat grafting.

Preconditioning strategies for fat grafting. These include the preconditioning of the transplanted adipose tissue by dietary restriction. Moreover, the host tissue at the recipient site can be pretreated by means of EVE, IEP, or microtraumatization, as well as heat and fractional CO2 laser. In addition, both the grafted tissue and the recipient site can be exposed to hypoxia, which is induced by temporary tissue ischemia following vessel occlusion or pharmacologically by DFO. DFO, deferoxamine; EVE, external volumetric expansion; IEP, internal expansion; CO2, carbon dioxide.
Overview of Preconditioning Strategies for Fat Grafting. Where Available, Fat Graft Origin, Recipient Species, Maximum Follow-Up, and Effects on the Graft and/or the Recipient Site Are Listed
↑ = Increased; ↓ = Reduced; ↔ = Unchanged.
CO2, carbon dioxide; DFO, deferoxamine; EVE, external volumetric expansion; IEP, internal expansion; VEGF, vascular endothelial growth factor.
The Principle of Preconditioning
Preconditioning is defined as a strategy to enhance the resistance of tissues to subsequent stressors. For this purpose, tissues are exposed to different stimuli to induce protective cellular adaptations, such as the upregulation of stress-response genes and the release of cytokines.42,43 Notably, preconditioning does not primarily involve the addition of external components, such as growth factors or stem cells, to the treated tissues, but focuses on triggering an endogenous response within the tissues themselves.
Preconditioning has been widely tested for several clinical applications, highlighting its versatility as a therapeutic approach. Particularly hypoxic preconditioning is highly effective in preventing tissue and organ damage. For instance, short-term exposure to hypoxia before cardiovascular surgical procedures, such as percutaneous coronary intervention and coronary artery bypass grafting, has been shown to markedly reduce the risk for myocardial infarction with the consequent improvement of the overall outcomes.44–46 Interestingly, this preconditioning phenomenon is not restricted to the heart, but has also been observed in numerous other organs, including the kidneys, lungs, liver, intestine, pancreas, stomach, ovaries, and skin. 47 In plastic surgery, preconditioning has been known for 50 years as the “delay phenomenon.” 48 This means the stepwise elevation of a flap over a time-period of approximately 14 days to induce hypoxia in the tissues, stimulating arterio- and angiogenesis and subsequently increasing the flap’s resistance to critical perfusion while ultimately transferring the flap. Furthermore, several additional nonhypoxic preconditioning modalities deserve to be highlighted. These include preconditioning by means of dietary restriction, heat, local mechanical stress, and exposure to fractional carbon dioxide (CO2) laser, which are also capable of inducing an endogenous protective response.49–52
Preconditioning of Fat Grafts
Hypoxic preconditioning
Hypoxic preconditioning has been shown to protect different tissues from ischemic injury.53–58 Of note, hypoxia upregulates the expression of the transcription factor hypoxia-inducible factor (HIF)-1α. Under normoxic conditions, HIF-1α is subject to ubiquitination and proteasomal degradation by proline hydroxylase-2 (PHD-2) and von Hippel–Lindau ubiquitin ligase complexes. Furthermore, factor inhibiting HIF-1 hydroxylates HIF-1, which prevents its interaction with the coactivators p300 and CREB binding protein and, thus, inhibits its transcriptional activity. Under hypoxic conditions, these mechanisms are suppressed, resulting in the stabilization and activation of HIF-1α. 59
An important function of HIF-1α is the stimulation of angiogenesis by inducing the transcription of genes encoding for several proteins, such as the vascular endothelial growth factor (VEGF), matrix metalloproteinase-2, cathepsin D, and keratin.59–62 Moreover, HIF-1α contributes to the shift from aerobic to anaerobic metabolism, which ensures cell survival in oxygen-depleted conditions. This is due to the fact that HIF-1α induces the expression of glycolytic enzymes and glucose transporters, such as aldolase A and pyruvate kinase M, while decreasing mitochondrial oxygen consumption by activating pyruvate dehydrogenase kinase I and inhibiting the citric acid cycle. 59 Cell survival is further promoted by HIF-1α-mediated transcription of Max-interacting protein 1 (MXI1), a repressor of the transcription factor C-MYC. C-MYC, in turn, inhibits glycolysis and increases mitochondrial respiration. 63
In the context of autologous fat grafting, Zhong et al. 27 hypothesized that the exposure of adipose tissue to temporary controlled hypoxia improves its viability and longevity after transplantation. To test their hypothesis, a U-shaped adipose flap was raised in the inguinal region of rabbits and sutured back into place to delay the flap for hypoxic preconditioning according to the approach originally described by Reinisch et al. 48 Twelve hours after the delay operation, a significantly higher VEGF expression was detected in the flap when compared with matched nonpreconditioned fat tissue. Three weeks later, the preconditioned and control fat tissue was grafted into dorsal pockets for histological analyses throughout an observation period of 12 months. These analyses revealed an improved vascularization and survival of the preconditioned fat grafts when compared with controls. 27 Comparable beneficial results were achieved by Gassman et al. 28 by repeatedly applying a tourniquet to induce three cycles of 5-min ischemia and 5-min reperfusion on the proximal hind limbs of transgenic mice expressing green fluorescent protein and luciferase. Thereafter, subcutaneous adipose tissue was harvested from the proximal hind limb, grafted into dorsal skinfolds of wild-type mice for 28 days and analyzed by means of bioluminescence and histology. In comparison with nontreated control fat grafts, the ischemically preconditioned fat grafts showed a better survival and contained less interstitial fibrotic tissue.
Ischemic preconditioning can not only be achieved mechanically through the transient occlusion of the perfusing arterial vessel of a target tissue, but also pharmacologically by the less invasive administration of deferoxamine (DFO). This iron-chelating compound is clinically used for the treatment of acute iron intoxication, chronic iron overload, and hemochromatosis. 64 On the contrary, it can also act as a hypoxia-mimetic agent. Indeed, DFO has been shown to stabilize HIF-1α through chelating iron that is required as a cofactor for the activation of PHD-2.32,33,65–67 Accordingly, several studies successfully performed ischemic preconditioning of random flaps or entire organs, such as the liver before hepatectomy, by means of local injection or intravenous administration of DFO.67–69 Furthermore, DFO has been used to precondition bone tissue, which has been shown to enhance its vascularity before radiotherapy or during distraction osteogenesis.70–74 Finally, topical administration of DFO on the skin represents a promising approach for the improvement of wound healing, particularly under pathological conditions, such as diabetes.75,76
Lin et al. 29 mixed isolated human adipose tissue with different concentrations of DFO or vehicle as control. Subsequently, the tissue was grafted into nude mice for 1 and 3 months. By this, they could show that DFO-treated grafts exhibited a significantly higher weight/volume retention rate when compared with controls. This was associated with an improved adipocyte integrity and vascularization, while cyst formation was markedly reduced within the DFO-treated tissue. 29
Taken together, these findings indicate that hypoxic preconditioning is a highly promising approach to improve the success rates of fat grafting. However, hypoxia may largely vary within the treated tissue depending on the applied method and it is not clear so far, which time periods and levels of hypoxia are most effective for the preconditioning of fat grafts to increase their survival rate. Therefore, further preclinical studies are needed to establish safe and efficient preconditioning protocols under highly standardized conditions, which then should be evaluated in clinical trials.
Dietary restriction
Dietary restriction is an attractive option for perioperative treatment, which has shown tissue-protective effects against hypoxic stress in several organs, such as the heart, kidneys, and brain.43,49,77–79 In general, caloric restriction (reduced overall caloric intake), periodic fasting (lasting 2 to 7 days repeated once per month or less), and intermittent fasting (lasting 12 to 48 h repeated every 1 to 7 days) can be distinguished as typical forms of dietary restriction. 80 Initially investigated in the context of healthy aging and longevity using long-term protocols, even short-term dietary interventions have been shown to induce beneficial effects, such as resistance to acute stress, making it an attractive approach in the clinical setting. 81
Dietary restriction enhances not only the resistance to stress resulting from nutrient deprivation but also induces a cross-resistance against oxidative stimuli. 82 During dietary restriction, the inhibition of insulin-like growth factor-1 and the upregulation of antiapoptotic pathways have been described, resulting in a shift from a proliferation-oriented to a survival-oriented cellular state.83–85 This adaptation also renders cells more resistant to ischemic insults. 86 In addition, dietary restriction stimulates the expression of HIF-1α, induces angiogenesis via the upregulation of VEGF expression, and mitigates oxidative stress and inflammation by suppressing reactive oxygen species (ROS) production in mitochondria.87–90 Simultaneously, it upregulates the expression of stress-response genes, such as heme oxygenase-1, as well as antioxidant enzymes such as superoxide dismutase-2 and glutathione peroxidase-1, further suppressing ROS formation. 43
Recently, Cha et al. 30 evaluated whether dietary restriction could also be beneficial for the preconditioning of adipose tissue intended for transplantation. For this purpose, white adipose tissue was harvested from donor mice, which either had free access to food or starved for 24 h, and grafted into the subcutaneous tissue overlying the skull of recipient mice. Subsequently, the survival of the grafts was analyzed throughout an observation period of 8 weeks. Of interest, it was found that fasting reduced the size of adipocytes by inducing lipolysis. This was associated with the upregulation of lipolysis- and angiogenesis-related genes. Accordingly, fat grafts originating from starved mice exhibited significantly higher numbers of viable adipocytes and microvessels as well as lower numbers of macrophages. This resulted in larger final volumes and heavier weights of the fat grafts when compared with controls. 30
These preliminary results provide clear evidence that a short duration of 24-h fasting may already be sufficient to improve the engraftment process and eventually the long-term outcome of fat grafting. If this finding also holds true in patients, dietary restriction may be a highly attractive preconditioning strategy. In fact, in contrast to other preconditioning methods it does not require additional devices, drugs, or surgical interventions. Hence, this approach is simple, safe, and cost-effective. Moreover, a 24-h fasting period may easily be implemented into clinical routine procedures without markedly affecting the standard treatment protocol of patients undergoing fat transplantation. In addition, dietary restriction is a systemic approach. Therefore, it may not only improve the biological properties of the fat graft but also of the host tissue at the recipient site, which, in turn, may further increase its efficacy.
Preconditioning of the Recipient Site
Hypoxic preconditioning
Similar to the hypoxic preconditioning of fat grafts, the host tissue at the recipient site may be also stimulated by subjecting it to defined periods of ischemia and reperfusion or by the administration of hypoxia-mimicking drugs.
Gassman et al. 31 transplanted subcutaneous adipose tissue from transgenic mice expressing green fluorescent protein and luciferase into wild-type mice to analyze the survival of the grafts by means of bioluminescence and histology throughout an observation period of 28 days. Of interest, they included experimental groups in their study, in which only donor or recipient animals or both were exposed to intermittent temporary hind limb tourniquet application for hypoxic preconditioning before fat harvest and transfer, respectively. Accordingly, they could demonstrate that the survival and tissue integrity of the grafted adipose tissue were mostly improved when hypoxic preconditioning was applied in both donor and recipient mice.
Kim et al. 33 injected DFO into rat scalps for a period of 5 days, followed by the transplantation of inguinal adipose tissue. The DFO-treated rat scalps exhibited an increased VEGF expression and microvessel formation when compared with nontreated controls. These positive effects on the recipient site also improved the survival rate of the fat grafts, as indicated by a higher adipocyte viability and microvessel density. 33 Flacco et al. 32 achieved similar results after DFO injection into irradiated scalp skin of immunocompromised mice before human fat grafting. By means of laser Doppler and immunofluorescent analyses, they were able to demonstrate a significantly increased perfusion and vascularization of the recipient site after this pretreatment. Accordingly, the fat grafts also exhibited a markedly improved retention rate at 8 weeks posttransplantation. 32 The latter findings support the view that preconditioning may be particularly recommended in cases of a poorly vascularized recipient site. However, when using DFO for this purpose, it should be considered that repeated injections of this pharmacological compound to the recipient site before fat grafting may be inconvenient and, thus, not tolerated well by patients. This problem may be overcome by using transdermal drug delivery systems for DFO. 91 Hence, it would be of great interest to evaluate the efficacy and safety of these systems in future studies focusing on fat grafting.
Mechanical preconditioning
Preconditioning of the recipient site can also be achieved by mechanical stimulation with external volumetric expansion (EVE), a technique that was first described by Khouri et al. in 2000 for breast enlargement. 92 The same group demonstrated in 2009 that EVE is not only capable of enlarging breast tissue but also improving the survival rate of transplanted fat in the context of breast augmentation. 51
The principle behind EVE is the local application of mechanical forces induced by negative pressure of variable intensity and duration on the target tissue through specific devices. 93 These forces induce a state of transient hypoxia,20,94,95 which stimulates the expression of angiogenic growth factors, including VEGF, epidermal growth factor, and transforming growth factor (TGF)-β20,94,96 leading to cell proliferation and vascular remodeling.94,97 In addition, they have been shown to promote adipogenesis.98,99 The microtraumatic volumetric expansion using EVE further leads to an improved compartment elasticity and compliance of the recipient tissue. This reduces the pressure resulting from grafting tissue into a closed compartment and allows the injection of bigger fat volumes as well. Hence, it markedly decreases the risk of pressure-induced ischemia within the first weeks after transplantation, particularly in the case of large grafts. 20
Several animal studies on negative pressure wound therapy demonstrated that angiogenesis is effectively stimulated by applying a continuous negative pressure of −125 mmHg for one week.100–102 In line with these findings, Lee et al. 34 conducted an in vivo study applying the same protocol in rabbit ears. Of interest, this intervention resulted in a higher survival rate and improved vascularization of the grafted adipose tissue. 34 In contrast, Giatsidis et al.36,103 suggested that the ideal negative pressure to induce angiogenesis at the recipient site should only be −25 mmHg. Moreover, they found that cyclic intermittent negative pressure application, including 6 cycles of 30 min interrupted by a 1-h break for 5 days, triggers a more effective response when compared with the application of continuous negative pressure. Similarly, the protocol proposed by Lujan-Hernandez et al. 20 involved the daily application of a negative pressure of −25 mmHg for 6 h during 5 consecutive days, while Ye et al. 35 used a negative pressure of −23 mmHg for 10 h per day during a treatment period of 4 weeks before fat grafting. These studies demonstrate the efficacy of locally applied negative pressure to precondition the recipient site. However, to date there is no clear consensus about the extent and duration of negative pressure to provide ideal conditions at the recipient site for subsequent fat grafting. This is particularly interesting, since this approach of tissue preconditioning is already widely used in daily clinical practice of aesthetic and reconstructive breast surgery.104–109
Another mechanical preconditioning strategy, which is very similar to EVE, is internal expansion (IEP). In this case, a silastic tissue expander is implanted at the recipient site to improve the elasticity of the tissue and to provoke transient hypoxia-induced angiogenesis. 110 This type of preconditioning is already in clinical use in the field of fat transplantation and can be particularly beneficial for patients with contracted soft tissues following radiotherapy.111–113
He et al. 37 recently conducted a preclinical study to analyze the mechanisms underlying the effects of IEP on the recipient site. For this purpose, they expanded the left inguinal tissue of 16 rats for 7 days by implanting cylindrical soft-tissue expanders and used the untreated right inguinal tissue as a control. After implant removal, adipose tissue from donor rats was transplanted into the left and right inguinal region. The expanded recipient site exhibited an upregulation of proangiogenic genes, including HIF-1α and VEGF, and a higher number of recruited circulating stem cells from the blood stream when compared with controls. This led to a higher retention rate, increased vascularization, less fibrosis, and fewer oil cysts in the fat transplanted to the expanded recipient site at 10 weeks after transplantation. 37
The recipient site for fat grafts can also be mechanically preconditioned through microtraumatization of the tissue. The basic principle of this method involves the creation of skin microwounds with needles to trigger the wound healing process and increase tissue vascularization. In fact, transdermal penetration promotes the endogenous production of collagen and growth factors, such as fibroblast growth factor, VEGF, platelet-derived growth factor, TGF-β, and TGF-α. 114 Of note, skin microtraumatization is widely applied in plastic surgery and aesthetic medicine for various indications, including the treatment of scars, striae, and hair loss disorders.115–117 Moreover, it has been shown to enhance skin rejuvenation and facilitate drug delivery.118–121
So far, two preclinical studies evaluated the effects of microtraumatization on the outcome of fat grafting in rats. Samdal et al. 38 preconditioned subcutaneous tissue over the right pectoral muscle through abrasion with 20 strokes of an 18-gauge needle. One week later, adipose tissue from the inguinal region was autologously transplanted into the pretreated area, whereas nontreated rats served as controls. Of interest, microtraumatization of the recipient site resulted in higher survival rates of the fat grafts. 38 Sezgin et al. 39 used a microneedling device, as introduced by Fernandes, 122 to create microchannels at the dorsum of rats to stimulate the wound healing response. After one week, their inguinal fat pads were harvested and autologously transplanted into the pretreated area. Compared with control grafts in nontreated animals, these grafts exhibited a significantly higher survival rate at 15 weeks posttransplantation. Additional histological analyses revealed an increased capillary density and adipocyte integrity, while tissue inflammation and fibrosis were markedly reduced. 39
Taken together, these results indicate that mechanical preconditioning of the recipient site promotes the engraftment and survival of transplanted adipose tissue in different experimental and clinical settings. For this purpose, preconditioning is usually performed several days before the transplantation of adipose tissue to allow the induced regenerative processes at the recipient site, such as angiogenesis, to take effect and provide an ideal environment for subsequent fat grafting. In addition to the necessary time, this approach requires specific devices. On the contrary, mechanical preconditioning bears the major advantage that it not only increases the survival rates of fat grafts but also improves the soft tissue quality at the recipient site. This may be particularly beneficial for patients suffering from tissue contractions or scars.
Heat preconditioning
Heat preconditioning by means of short-term tissue exposure to supraphysiological temperatures (> 40°C) has been previously described in experimental flap surgery123–125 and in breast surgery 126 with excellent results. This approach promotes the development of new blood vessels by the upregulation of VEGF. 127 In addition, stress by local heat induces the expression of heat shock proteins (HSPs), particularly HSP-32, which are the main endogenous source of carbon monoxide (CO). 128 HSP-32 acts as a potent vasodilator, which contributes to a better cell viability by enhancing tissue perfusion. 129
Kim et al. 40 recently investigated the effects of heat preconditioning in the context of fat grafting. They first performed experiments in mice to determine the ideal temperature for inducing a beneficial tissue response without causing burns and subsequent scars. For this purpose, they applied varying degrees of local heat on the dorsal skin of the animals using a digitally controlled thermal block. Based on these experiments, they subsequently exposed the dorsal skin of mice to room temperature as control or to a temperature of 44°C or 48°C for 20 s. This was followed by the transplantation of human adipose tissue, which was harvested after 7, 14, and 49 days for morphological, histological, and genetic analyses. These analyses showed that the grafts at the recipient sites exposed to a temperature of 44°C exhibited the highest survival rate, microvessel density, and adipocyte integrity, as well as the lowest levels of inflammation and fibrosis. 40
This first preclinical study indicates that local heat preconditioning is a promising strategy to improve the outcome of fat grafting. Moreover, it is cost-effective and can be easily applied within a relatively short time period. Nevertheless, further studies are required to confirm the findings of Kim et al. 40 and to establish safe and efficient heat preconditioning protocols for clinical application in patients. Alternatively to the approach of Kim et al., 40 it may be also interesting to study the direct effects of heat preconditioning on isolated fat grafts. If successful, this may bear the major advantage that potential risks, such as burn wounds at the recipient site, could be avoided completely.
Laser preconditioning
Another physical preconditioning method is the application of fractional CO2 laser. This technique is already widely used for the treatment of dermatological pathologies, such as cutaneous warts, nail disease, and acne scars.130,131 Moreover, in urogynecology, it serves for the therapy of incontinence, prolapse, the genitourinary syndrome of menopause and postmenopausal vulvovaginal atrophy.132–134 Exposure of tissue to CO2 laser has been shown to exert various biological reactions, including the upregulation of cytokines and growth factors, the stimulation of angiogenesis, and the replacement of collagen.135–138
Kim et al. 41 applied CO2 laser treatment as a preconditioning step in fat grafting. For this purpose, the dorsum of rats was pretreated with fractional CO2 laser one week before the transplantation of inguinal fat pads, while in controls, fat was transplanted without pretreatment of the recipient site. Subsequent analyses over 28 days revealed a better integrity of adipocytes, reduced inflammation, fibrosis, and vacuolization together with a higher expression of VEGF as well as an increased microvessel density and survival rate of the grafts at the pretreated recipient site when compared with controls. 41
Fractional CO2 laser treatment may be particularly suitable for the preconditioning of body areas with thin skin, such as the face, where it additionally can exert rejuvenation effects. 139 In contrast, it may not be recommended in areas with thicker skin, such as the extremities, where the laser may not be effective, because it cannot penetrate to the recipient tissue.
Conclusion
Preconditioning is an effective strategy to improve the outcome of biological processes, such as the engraftment of transplanted adipose tissue. In fact, it activates tissue-protective mechanisms and stimulates the body’s adaptation to critical conditions by upregulating stress-response genes with the consequent release of anti-inflammatory cytokines and angiogenic growth factors. Hence, there is no need for any prolonged pharmacological therapy, which always bears the risk of side effects.
The herein summarized preclinical studies clearly indicate that the survival of fat grafts can be enhanced by preconditioning the adipose tissue before transplantation, the host tissue at the recipient site, or a combination of both. For this purpose, different stimuli have proven to induce a beneficial biological tissue response (Fig. 4), including hypoxia, dietary restriction, local mechanical stress, heat, and exposure to fractional CO2 laser. However, they may largely vary in their efficacy and applicability depending on the treatment protocol, the type of grafted adipose tissue, as well as the soft tissue conditions at the recipient site. Moreover, the discussed forms of preconditioning differ in terms of patient burden, technical effort, and duration (Table 2). For a successful transfer into clinical practice, an ideal preconditioning strategy should be easily applicable, safe, efficient, cost-effective, and implementable into clinical routine procedures. From this point of view, dietary restriction and local heat preconditioning may be highly attractive. Nonetheless, other preconditioning approaches also bear their specific advantages. For instance, preconditioning via local mechanical stress is not only effective in increasing the survival rate of fat grafts but also for improving the soft tissue quality at the recipient site, which may be particularly beneficial for patients suffering from scars or local tissue contractions. Finally, it should be considered that there are also other preconditioning approaches, which have not yet been tested in fat grafting. Hypothermic preconditioning has been shown to reduce inflammatory cytokine production and attenuate oxidative damage of liver tissue.140,141 In addition, it is well known that different types of physical exercise can protect myocardial tissue against ischemia–reperfusion injury. 142 Hence, it may be highly interesting to clarify in future studies whether these approaches also improve the outcome of fat grafting.
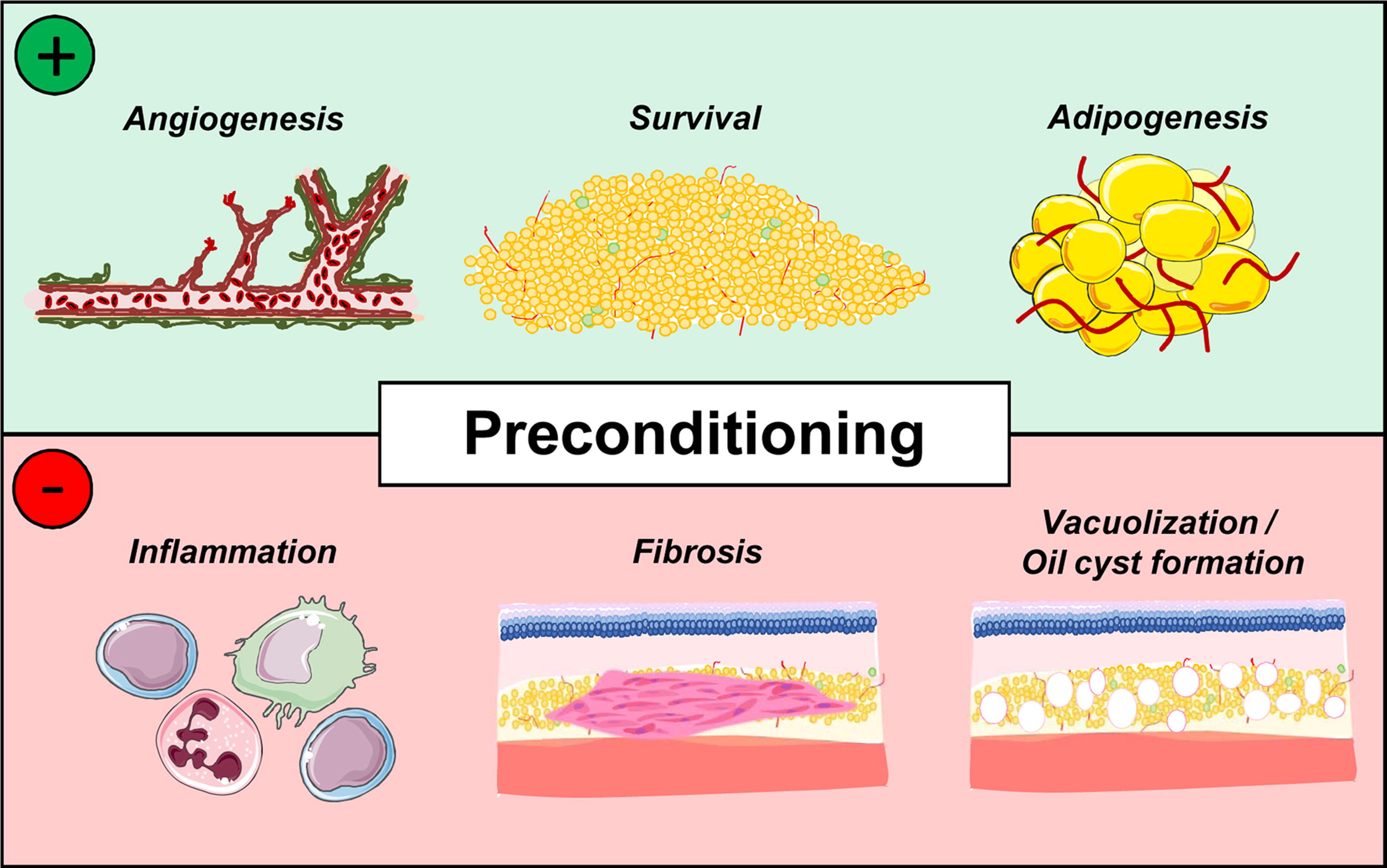
Beneficial biological effects of preconditioning on fat grafts and/or the recipient site. These include the induction of angiogenesis and adipogenesis as well as improved tissue survival. On the contrary, preconditioning inhibits inflammation and prevents fibrosis, vacuolization, and oil cyst formation within the grafted adipose tissue.
Main Characteristics of Preconditioning Strategies for Fat Grafting
+ = low; ++ = medium; +++ = high.
Taken together, different preconditioning strategies indicated for specific conditions and clinical scenarios may likely be available in the future. To implement the preconditioning of fat grafts and their host tissue into daily clinical practice, it is therefore important to establish standardized protocols for both the donor and the recipient site.
Footnotes
Acknowledgment
Authors’ Contributions
F.B., E.L., and M.W.L. conceptualized the review and wrote the original article draft. All authors edited the article and approved the final version.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Statement
There was no specific funding of this review.