
Abstract
Arterial stenosis caused by atherosclerosis often requires stent implantation to increase the patency of target artery. However, such external devices often lead to in-stent restenosis due to inadequate re-endothelialization and subsequent inflammatory responses. Therefore, re-endothelialization strategies after stent implantation have been developed to enhance endothelial cell recruitment or to capture circulating endothelial progenitor cells. Notably, recent research indicates that coating stent surfaces with biogenic materials enhances the long-term safety of implantation, markedly diminishing the risk of in-stent restenosis. In this review, we begin by describing the pathophysiology of coronary artery disease and in-stent restenosis. Then, we review the characteristics and materials of existing stents used in clinical practice. Lastly, we explore biogenic materials aimed at accelerating re-endothelialization, including extracellular matrix, cells, and extracellular vesicles. This review helps overcome the limitations of current stents for cardiovascular disease and outlines the next phase of research and development.
Impact Statement
Due to the potential risk of restenosis in all types of vascular stents, re-endothelialization strategies should be considered in stent development. This review discusses the use of biogenic materials, including extracellular matrix, cells, and extracellular vesicles, on stent surfaces to induce endothelial cell recruitment and suppress inflammatory responses, thereby preventing neointimal hyperplasia. Compared with other strategies, biogenic materials offer greater stability and safety with fewer side effects, addressing current unmet needs. Consequently, this review offers a novel perspective on the development of a new generation of stents.
Introduction
Coronary artery disease (CAD) is one of the major cardiovascular diseases arising from atherosclerosis and remains the leading cause of death worldwide. 1 Aggressive management of risk factors such as hypertension, diabetes, smoking, and hyperlipidemia, and the best medical treatment are essential for the treatment of CAD.2,3 However, many patients with obstructive CAD require appropriate revascularization to treat CAD, and coronary artery bypass grafting (CABG) and percutaneous coronary intervention are representative modalities of revascularization in CAD.4,5 While PCI offers shorter procedural time, avoids the need for anesthesia, and promotes faster recovery compared with CABG, stents have been reported to cause restenosis of the blood vessel. For example, bare-metal stent (BMS) frequently leads to restenosis due to vascular injury during implantation along with inflammatory responses. 6 Thus, a more biocompatible and a thinner drug-eluting stent (DES) was developed, as various drugs introduced to the DES inhibit restenosis caused by neointimal hyperplasia, but DES still has a problem of late thrombosis or late stenosis occurring at one year postsurgery. 7 Recently, bioresorbable stents (BRSs) have been developed, nonetheless, the high cytotoxicity of the drug interferes with re-endothelialization, the most decisive aspect of stent implantation. 8
Re-endothelialization at the site of stent implantation is a major factor in the occurrence of restenosis.9,10 One of the strategies to enhance re-endothelialization involves stents coated with antibodies capturing endothelial progenitor cells (EPCs).11–13 However, during the adsorption process of antibody coating, steric resistance at the antigen binding site can lead to over 90% denaturation. 14 For example, anti-CD34 antibody showed significant clinical results upon its initial application, but was reported to have higher side effects compared with BMS at 6 months postoperation.15,16 In addition, the efficiency of antibody-EPC binding may depend on the circulating concentration of specific EPCs,17,18 and the captured EPCs may not all differentiate into endothelial cells (ECs), but rather differentiate into vascular smooth muscle cells (SMCs). 19 Another strategy is immobilization of angiogenic chemokines to recruit neighboring ECs. 20 However, vascular endothelial growth factor (VEGF) has been challenged by its short in vivo half-life and low stability,21,22 and stromal cell-derived factor-1α recruits not only ECs but also other hematopoietic cells and SMC progenitor cells, potentially leading to restenosis. 23 Recently, ongoing research has focused on overcoming these limitations by using synthetic peptides for re-endothelialization.24,25
Biogenic materials, including extracellular matrix (ECM) components, cells, and extracellular vesicles (EVs), have emerged as novel materials for surface modification to promote in-stent re-endothelialization. ECM is composed of polysaccharides and proteins, which provide the microenvironment for cells, supporting structural integrity of the tissue and cell growth. 26 In addition, the biochemical signals in the ECM play a crucial role in regulating cellular functions, profoundly influencing cell growth, migration, and differentiation. 27 These signals are instrumental in promoting re-endothelialization after stent implantation by interacting with host ECs.28,29 Grafting angiogenic cells such as ECs or mesenchymal stem cells (MSCs) or EVs secreted from those cells onto the stent surface can also promote in-stent re-endothelialization, but the fast bloodstream may induce their unwanted detachment.30–32 Therefore, several studies are in progress to stabilize coating of cells or EVs directly on the stent surface. In this study, we first present an overview of CAD pathogenesis and restenosis following stent implantation. In addition, we review the currently used stents, then discuss various stent coating methods based on biogenic materials, including ECM, cells, and EVs that effectively induce re-endothelialization to prevent long-term restenosis.
Pathophysiology of CAD
CAD is a disease that results from the hardening and narrowing of coronary arteries, leading to an inadequate supply of blood to the heart. 33 Atherosclerosis is a chronic condition characterized by the accumulation of lipids and fibrous materials on the inner walls of blood vessels (Fig. 1). The inflammatory response has a significant role in the development of atherosclerosis, which begins with the endothelial dysfunction of ECs and oxidation of low-density lipoprotein (LDL) in the subendothelial space. The initiation of vascular dysfunction induces expression of vascular cell adhesion molecules and intercellular adhesion molecules on the endothelium to recruit immune cells.34,35 The monocytes move into the subendothelial space and transform into macrophages under the influence of cytokines. Oxidized LDLs are taken up into macrophages, forming foam cells, generating a fatty streak in the subendothelial space. 34 Subsequently, SMCs migrate from the medial layer to the intima, positioning themselves above the fatty streak. SMCs secrete ECM molecules that deposit collagen and elastin fibers, forming a fibrous layer that covers the fatty streak. Moreover, foam cells undergo necrosis within the fatty streak layer, contributing to lipid accumulation in the extracellular space. The accumulation results in the formation of a lipid-rich necrotic core with severe inflammatory responses. The emerging plaque gradually obstructs blood flow, disrupting the exchange of nutrients between vascular cells and causing the vessel wall to deteriorate. The vasculature undergoes calcification in advanced stages, which contributes to the development of atherosclerosis. 34
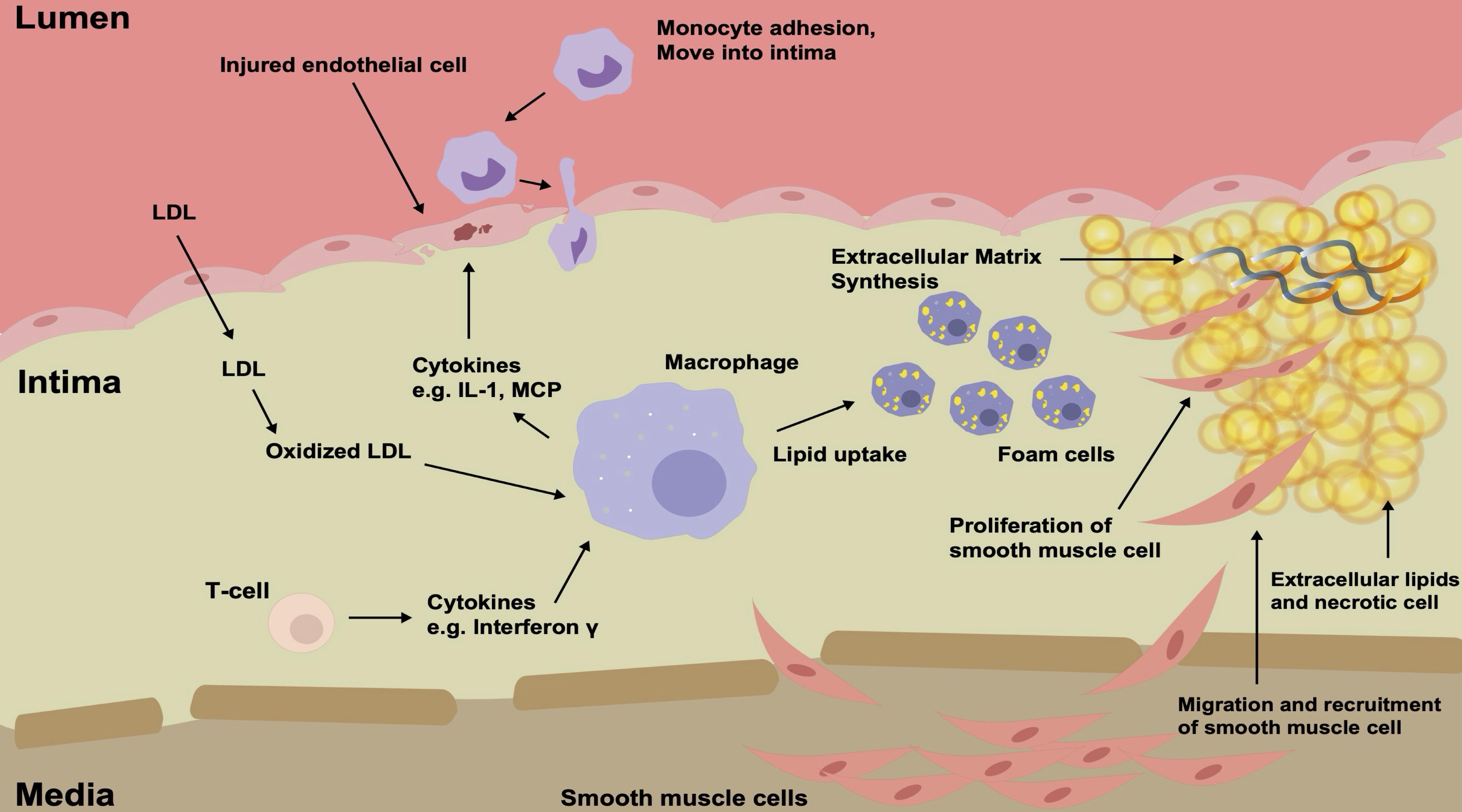
Pathophysiology of atherosclerosis. Atherosclerosis is a complex pathogenic cascade involving endothelial dysfunction, immune response, and lipid composites, leading SMC migration and vascular calcification.
Pathophysiology of In-Stent Restenosis
Restenosis is clinically defined as the occurrence of stenosis greater than 50% in diameter at the site of stent implantation. Restenosis is categorized into an early phase (days to weeks) and a late phase (weeks to months), each involving the action of growth factors and cytokines (Fig. 2). 36 In the early phase, plaque relocation, thrombus reorganization, and acute inflammation occur with minimal elastic recoil due to stent rigidity. EC damage occurring during stent implantation leads to thrombus formation and deposition of fibrin and platelets at the site of injury. 37 Subsequently, there is an increase in leukocyte migration to the implantation site, penetrating the vessel wall. 38 Moreover, leukocytes are recruited by cytokines and chemoattractants secreted by platelets, monocytes, and SMCs. Several weeks following stent implantation, the process transitions to the late phase, characterized by phenotypic modification of SMCs, inducing faster migration and proliferation. Simultaneously, ECM constitution in the intimal tissue alters, as newly formed ECM emerges as the predominant component, consisting primarily of proteoglycan and collagen. After the stent implantation, ECM synthesis predominates for several months before SMC proliferation takes over.39,40

Pathophysiology of in-stent restenosis. The injured EC induced by stent implantation triggers an inflammatory response. The restenosis is initiated by the attachment of platelets and immune cells onto the endothelium, secreting inflammatory cytokines. Subsequently, the SMCs in the medial layer are activated by the inflammatory microenvironment, starting to migrate toward the endothelial layer and proliferate. During the process, the contractile phenotype SMCs transition to synthetic phenotype SMCs and synthesize ECM components and exacerbate restenosis. EC, endothelial cell; ECM, extracellular matrix; SMC, smooth muscle cell.
Current Stent Type in Use
Bare-metal stents
Coronary angiography and balloon angioplasty were introduced in the late 1970s. Arterial recoil and restenosis frequently occur due to the absence of stent implantation in balloon angioplasty. To address this problem, the first BMS was introduced in 1986.41,42 The early stainless steel BMS had thick struts and outcomes that promoted SMC proliferation. SMC proliferation led to in-stent restenosis, highlighting the need for thin and biocompatible stents.43,44 As a result, metals such as cobalt and chromium began to be used in the manufacturing of BMS.45,46 These materials improved on the shortcomings of BMS, but were still not sufficient to prevent high rates of in-stent restenosis.47,48 Thus, various coating methods were applied to reduce attachment of platelets and fibrinogen. Specifically, titanium-based and magnesium-based coatings have been used to mitigate thrombus formation and enhance biocompatibility. Despite attempts to increase biocompatibility and reduce adverse effects, complete prevention of restenosis and thrombosis remains unachieved.
Drug-eluting stents
Polymers are commonly used in the treatment of cardiovascular diseases, particularly in DES and stent platforms. The first-generation DESs, such as Cypher and Taxus, used synthetic polymers such as poly(ethylene-covinyl acetate) (PEVA) and poly(n-butyl methacrylate) (PBMA). 49 However, these synthetic polymers delay vascular healing during stent implantation and can trigger hypersensitivity reactions.50,51 To address these issues, Xience utilized highly biocompatible polymers such as poly(vinylidene fluoride co-hexafluoropropylene) (PVDF-HFP) and PBMA. Despite the use of polymers with high biocompatibility, the occurrence of local inflammatory responses could not be prevented, emphasizing the importance of bioresorbable polymers. Bioresorbable polymers such as poly-L-lactic acid (PLLA) offer excellent biocompatibility and provide advantages in terms of re-endothelialization.52,53 However, polymeric BRSs typically have lower mechanical strength than metal stents, necessitating the use of thicker struts to enhance their strength. 54 Furthermore, several studies have demonstrated a higher risk of in-stent thrombosis in polymeric BRS compared with DES.55,56 Thus, achieving higher mechanical properties and advanced surface modifications are required for clinical translation.
First-generation DES
The development of DES addressed the major issue of in-stent restenosis in BMS.57,58 The primary aim of DES was to inhibit neointimal hyperplasia and prevent in-stent restenosis through drug delivery. DES consists of a platform, polymer, and drug. The first-generation DES utilized a stainless-steel platform coated with a drug-eluting polymer. Sirolimus-eluting stent Cypher and paclitaxel-eluting stent Taxus are examples of first-generation DES. 59
Cypher, introduced in 2003, is based on a stainless steel platform coated with PEVA and PBMA to deliver sirolimus. 60 The stent has a thickness of 140 μm and is designed to release 80% of the drug within 30 days of implantation. Sirolimus binds sequentially to FKBP12 binding protein and mTOR in the body, inhibiting the progression of vascular SMCs from the G1 to the S phase.61,62 Taxus was approved for patient use in 2004. 63 It features a stainless-steel platform and is coated with a poly(styrene-block-isobutylene-block-styrene) polymer to release paclitaxel. The thickness of the coating is 132 μm. The drug was released with a higher concentration for the first 48 h, followed by a lower rate of release for the following two weeks. Paclitaxel released from the Taxus stabilizes microtubules within cells inhibiting the proliferation of vascular SMCs. Follow-up studies after DES implantation have shown a significant reduction in restenosis and decrement of need for revascularization for both Cypher and Taxus.64–71
Second-generation DES
The first-generation DES had limitations such as stent thrombosis and delayed re-endothelialization.72,73 There was a significantly higher incidence of very late-stent thrombosis occurring after one year with DES compared with BMS.73–75 This was attributed to delayed re-endothelialization at the implantation site or hypersensitive reactions induced by antiproliferative drugs and polymers.50,51 Consequently, the second-generation DESs were developed, which are designed to promote vascular regeneration to reduce adverse effects. These stents replace stainless steel with cobalt-chromium or platinum-chromium, allowing for thinner designs.45,46,59 Furthermore, biocompatible polymers such as polycarbonate and polylactic acid (PLA) have been used in conjunction with antiproliferative drugs such as zotarolimus and everolimus. 50
The zotarolimus-eluting stent Endeavor, which is based on cobalt-chromium and has a relatively thin thickness of 91 μm, uses a phosphorylcholine-based polymer to release zotarolimus.76,77 Within 15 days after implantation, 95% of the drug was released. 78 Zotarolimus inhibits mTOR in a similar way to rapamycin, preventing the proliferation of vascular SMCs. It has shown significantly lower inflammatory responses compared with the first-generation DES and has demonstrated highly effective inhibition of in-stent restenosis. Everolimus-eluting stent Xience is made of cobalt-chromium and has a thickness of 81 μm. It released everolimus from a polymer based on PVDF-HFP and PBMA and 80% of the drug was released within 30 days postimplantation. Everolimus inhibits the proliferation of vascular SMCs through a mechanism similar to sirolimus. 59
Third-generation DES
Research is currently underway to reduce vascular inflammation response caused by polymers. This includes coating stent surfaces with bioresorbable polymers or developing fully BRSs. After 6 to 9 months postimplantation, the bioresorbable polymer layer is absorbed, resulting in a stent that resembles a BMS. The biolimus-eluting stent BioMatrix, which is based on 316L stainless steel, is coated with a PLLA layer. Biolimus is an analogue of sirolimus that exhibits anti-inflammatory properties. However, it is more lipophilic than sirolimus, resulting in higher cellular uptake. 79 The stent’s polymer is designed to release the drug in two stages. It initially releases a high concentration of the drug, followed by complete absorption of the remaining drug and polymer into the body within 6 to 9 months. Following the development of stents with bioresorbable polymers, research has been conducted on BRSs that completely degrade within the blood vessel after the treatment period. 80 The main polymers currently used for BRSs are PLLA and poly-D,L-lactide, and this significantly reduces the incidence of in-stent thrombosis.
Biogenic Materials for Re-Endothelialization
ECM coating
Collagen
Collagen is a major component of the ECM and contributes to the strength, elasticity, and tensile strength of cells. Furthermore, collagen controls cell attachment through biochemical signaling.81–83 Collagen provides a three-dimensional environment that allows cells to grow and acquire the appropriate morphology. 84 Coating stent with type III collagen (Col III) has been engineered to eliminate functions associated with platelet adhesion while preserving EC attachment capability. 85 In this study, PLA stents were immersed in a 2 mg/mL dopamine solution and a 20 mg/mL polyethyleneimine solution for 2 h each (Fig. 3). 85 Subsequently, they were immersed multiple times in a solution of Col III to deposit Col III onto the surface. 85 The results showed that the Col III-coated stents facilitated re-endothelialization and demonstrated a reduction in neointimal hyperplasia through the inhibition of SMC proliferation. 85
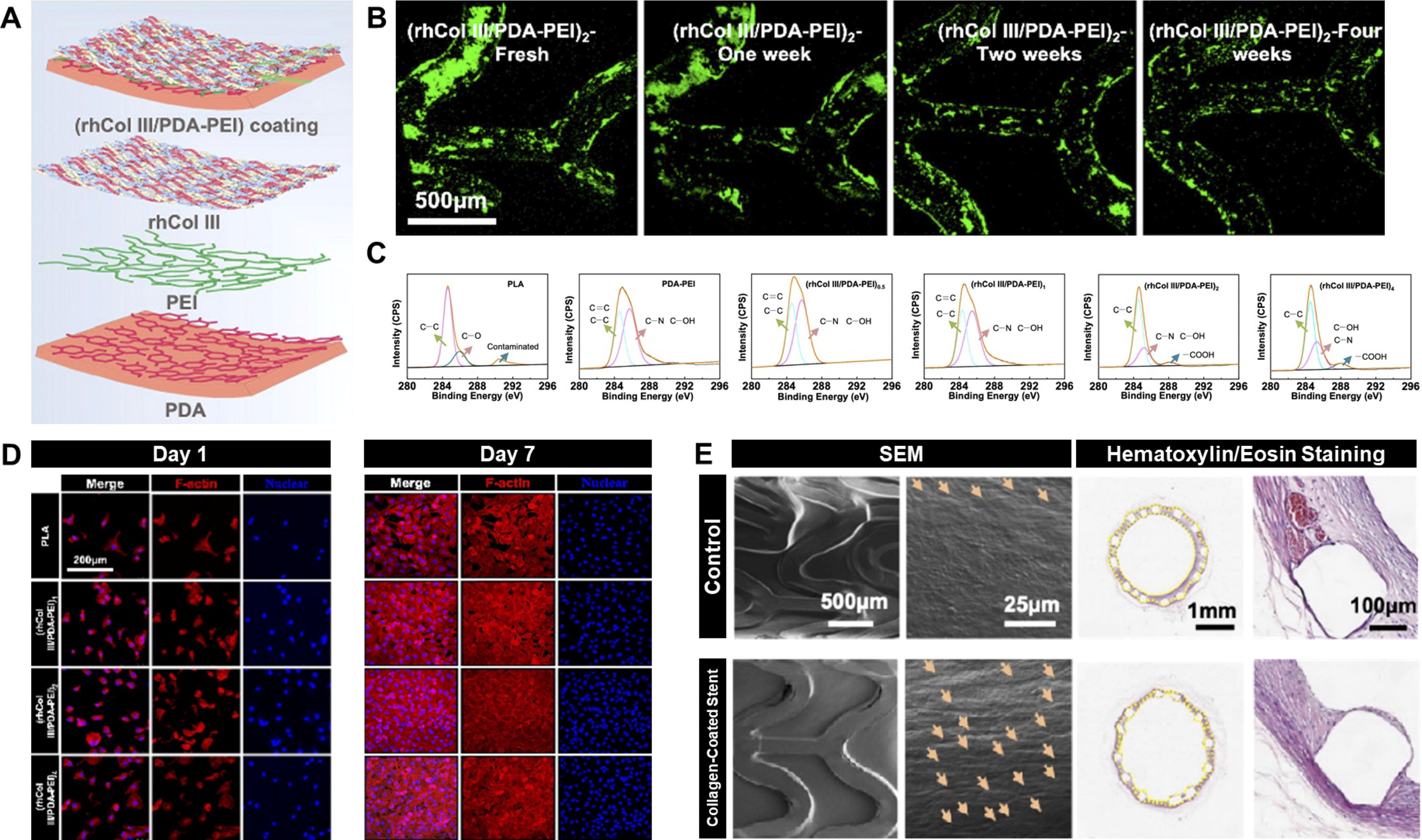
Type III collagen-coated stent for re-endothelialization.
Another study aimed to inhibit neointimal hyperplasia by using type IV collagen (Col IV) and hyaluronic acid (HA). 86 In the experiment, Col IV was diluted in HA solution and titanium was immersed in the Col IV-HA solution and incubated at 37°C for 12 h. 86 The results showed that the coating of Col IV-HA enhances the attachment of Col IV to the surface and induced the contractile SMC phenotype by Col IV. 86 SMC exhibits a contractile phenotype under normal conditions, but transition to a synthetic phenotype immediately after the atherosclerosis. While most DESs use cytotoxic drugs to remove excessively proliferated SMCs, they failed to modify the SMC phenotype and might have damaged the vascular ECs. Thus, the utilization of Col IV to promote the SMC contractile phenotype and HA to support it induced significant changes in the SMC phenotype. 86
Laminin
Laminin is a major component of the basement membrane and self-assembles into sheet-like structures.87,88 It serves as a cross-linker due to its ability to cross-link with other ECM components. Laminin plays a vital role in cell adhesion, cell differentiation, and stabilizing phenotype.82,83,89 In EC, laminin expression plays a crucial role in maintaining the vascular stability and ensuring proper cell morphology. 90 The basement membrane below the endothelium is composed of laminin, Col IV, fibronectin (FN), and others.91–93 Compared with ECs, of Col IV, SMCs have a higher abundance indicating that Col IV can enhance the expression of contractile SMCs. 94 Moreover, due to the higher presence of laminin in ECs, laminin can promote the proliferation of ECs. 94 To investigate EC proliferation and inhibit platelet attachment, a titanium surface was coated with laminin and Col IV. 94 In the experiment, the HA pattern coating was used to mimic shear stress in blood flow, while demonstrating the endothelialization effect of laminin. 94 The study also showed significant results in regulating SMC contractile phenotype and inflammatory response. 94
In another study, heparin/poly-L-lysine (PLL) nanoparticles loaded with laminin were coated onto titanium to reduce thrombus formation and platelet adhesion. 95 To synthesize nanoparticles, a mixture of heparin solution and 50 μg/mL laminin solution was incubated at 37°C for 3 h. 95 Next, the solution was dropwise added with 0.5 mg/mL PLL solution under ultrasonic conditions, followed by centrifugation at 15000 rpm. 95 The separated sediment was resuspended in phosphate buffer saline (PBS). 95 To immobilize the nanoparticles, dopamine-coated titanium was immersed in the nanoparticle suspension and incubated at 37°C for 12 h. 95 The nanoparticle coating method used in this experiment exhibited a significant inhibitory effect on platelet adhesion and thrombus formation. 95 In addition, it showed significant results in the proliferation of EPCs and ECs. 95
Fibronectin
FN is a glycoprotein composed of two polypeptide chains. It binds to cells and can promote binding to other substances, allowing ECs to engage in complex interactions with their surrounding environment. FN, fibrinogen, and tropoelastin were coated onto the surface of stents to study the proliferation and migration of SMCs. 96 The study results showed that the coating not only prevented SMC proliferation but also reduced inflammation and thrombus formation. 96 Another experiment was conducted to compare the attachment of vascular ECs to surfaces coated with FN and PLL. 31 Both substances were found to promote cell growth and adhesion compared with the control group. 31 Nitinol stents were coated with solutions containing different concentrations of FN and PLL. 31 The control group consisted of uncoated stents, while the experimental groups included stents coated with PLL alone and stents coated with FN/PLL. 31 Human umbilical vein endothelial cells (HUVECs) were then seeded onto the stents. 31 A shear stress of 24 dyne/cm2 was applied for 24 h. 31 No significant cell detachment was observed on stents coated with PLL and FN compared with the control group. 31 In contrast, significant cell detachment was observed in the control group after 12 h, and most of the cells were lost after 24 h. 31 FN was predicted to enhance cell attachment by interacting with integrin receptors on the cell membrane. 31
Hyaluronic acid
HA is a glycosaminoglycan composed of disaccharides linked by β-glycosidic bonds. 97 As one of the major components of the ECM, HA plays a crucial role in regulating cell behavior, including immune responses, and has been shown to prevent neointimal hyperplasia by inhibiting the abnormal proliferation of SMCs.97,98 In addition, HA has demonstrated anticoagulant and anti-inflammatory properties, facilitating the recovery of damaged ECs.98–100 Numerous studies have utilized HA for stent surface modification, as it can be used solely to provide better surface properties, or as a drug delivery platform, or utilized as a cell culture platform based on its capacity for micropatterning through lithography, which is further discussed in section 5.1.5.100–105
For example, HA was coated on 316L stainless steel to improve biocompatibility and re-endothelialization ability. 101 In this study, dopamine was used to conjugate stainless steel with HA, by immersing 316L stainless steel in a 2 mg/mL dopamine solution for 24 h, followed by an HA solution for 12 h. 101 The HA/dopamine-coated group demonstrated significantly reduced platelet adhesion and activation, and enhanced HUVEC proliferation and migration. 101 In a similar study, surface modification with sulfonated HA was performed on Mg-Zn-Y-Nd alloy (ZE21B), as sulfonated HA has shown higher stability against hyaluronidase and improved therapeutic efficacy for atherosclerosis.102,106 In this study, ZE21B alloy was immersed in hydrofluoric acid solution for 48 h to obtain MgF2 layer. 102 Subsequently, sulfonated HA was deposited onto the MgF2 layer via a self-assembly method, followed by a PLLA coating to prevent sudden release of HA. 102 The sulfonated HA-coated group exhibited accelerated EC proliferation, anti-inflammatory response, and regulation of SMCs to a contractile phenotype. 102 Such biogenic material-coated BRSs may reduce the risk of immune rejection and shorten the recovery period, and also show reduced cytotoxicity against degradants due to immunoregulatory functions.54,107 As an example of drug delivery platform, one study has utilized HA on stent surface modification for NO delivery. 103 In the healthy vascular microenvironment, NO is secreted by ECs and is known to inhibit thrombosis and abnormal SMC proliferation. 108 To mimic these EC functions, PLA was conjugated with thiol-functionalized HA, in the presence of a copper ion (Cu) catalyst, which degrades NO donors in the body such as S-nitrosothiols to produce NO, thereby enabling the continuous release of NO. 103 The HA/Cu-coated group exhibited significantly reduced platelet adhesion and activation, and enhanced HUVEC proliferation and migration. 103
Decellularized ECM
The limitations of a single ECM coating rely on its inadequate ability to mimic the complex microenvironment of native tissue. 27 To address this limitation, decellularized ECM (dECM) has emerged as a potential biogenic material, which contains the structural and physicochemical properties of naturally secreted ECM derived from in vitro cultured cells or in vivo tissue. 27 Thus, arterial cell-derived dECM coated on a stent could minimize the loss of 109 healthy vascular characteristics while improving EC function. For example, EC-derived dECM (EC-dECM) coated on a 316L stainless steel-based stent significantly enhanced EC proliferation and hemocompatibility. 109 The structure and composition of the ECM were regulated by unidirectional alignment of the ECs, which mimics the microenvironment under shear stress from healthy blood flow. 109 For EC alignment, the surface was modified with HA micropatterns, using the soft lithography method on PDA-modified 316L surface, before EC seeding. 109 On the HA micropattern-modified surface, 5 × 104 cells/mL, HUVECs, were seeded and decellularized after 72 h. 109 This process was repeated three times to create a triple-layer EC-dECM surface. 109 The EC-dECM coating resulted in significantly enhanced HUVEC proliferation, reduced platelet adhesion, and a nonactivated macrophage phenotype. In addition, the EC-dECM-coated group showed reduced macrophage adhesion and TNF-α release, which are associated with the prevention of macrophage aggregation and inflammation in poststent implantation. 109
Another study has developed a layer-by-layer dECM derived from SMC and EC (SMC/EC-dECM), which was utilized with a similar HA micropatterning technique. 104 In addition to the therapeutic role of EC-dECM as mentioned above, SMC-dECM is known to have a different ECM composition from that of EC-dECM, providing mechanical and biochemical support and enhancing the proliferation of ECs and NO release.104,110 HA micropatterns were introduced on the titanium surface for/EC-unidirectional cell alignment, and then, SMCs were seeded at a density of 5 × 104 cells/mL and decellularized after 72 h. 104 HUVECs were then seeded onto the SMC-derived dECM at a density of 5 × 104 cells/mL, and the structure was decellularized again after 72 h. 104 Another study similarly applied the SMC/EC-dECM onto the surface of ZE21B alloy. 105 In this study, HA micropatterns were coated on an empty tissue culture plate, followed by sequential culturing and decellularization of SMCs and HUVECs to obtain the SMC-dECM. 105 The SMC/EC-dECM was dispersed in normal saline by ultrasonication and conjugated to the ZE21B alloy surface using the EDC/NHS coupling method. 105 In both studies, the SMC/EC-dECM demonstrated reduced platelet adhesion and activation, and increased EC proliferation rates and NO release in the EC/SMC-dECM-coated groups compared with the control group.104,105 Although various dECM have been widely used for tissue regeneration, low reproducibility of therapeutic effect due to batch-to-batch heterogeneity depending on the biochemical composition has been repeatedly reported as a major challenge. In addition, standardization, cost reduction, and productivity increase should be achieved for clinical translation.
Cell-based coating
As mentioned earlier, stent restenosis can be prevented by rapid re-endothelialization.111–113 However, spontaneous EC recruitment to the implantation site is challenging. Several studies have shown that transplanting EC or MSC into the vascular injury site inhibits restenosis.114–118 Therefore, stents coated with cells present a promising approach to enhance endothelial recovery and restenosis occurring after transplantation. In this study, we explore strategies for promoting stent re-endothelialization through EC and MSC coating.
Endothelial cell
EC is the lining of arteries, veins, and capillaries, involved in the contraction and relaxation of blood vessels, as well as the movement of fluids and blood cells.119–121 Furthermore, it helps maintaining normal vascular function by inhibiting abnormal SMC proliferation. The low spontaneous attachment of ECs to the stents is due to the high flow rate and limited quantity of cells in the blood flow. A homogeneous EC layer may reduce platelet and leukocyte adhesion after stent implantation, thereby reducing the risk of thrombosis and restenosis. Therefore, transplanting ECs onto the surface of the stent to promote rapid re-endothelialization might be promising. A study was conducted to promote re-endothelialization of stents by coating ECs onto the surface of the stent. 30 ECs extracted from veins were coated onto stainless-steel-based heparin-coated stents. 30 As a control, ECs were also coated onto PLA-coated stents using the same method. 30 Shear stress tests were conducted on the stents within the bloodstream using a blood flow mimicking device. 30 A shear stress of 100 dyne/cm2 was applied to the stents and measurements were taken at 0-, 12-, 24-, and 48-h intervals. 30 No significant cell detachment was observed in the heparin-coated stent. 30 In contrast, significant cell detachment was observed over time in the PLA-coated stents used as controls. 30 In addition, a smoother cell layer was observed on the heparin-coated stent when compared with a PLA-coated stent. 30 The result is likely attributable to the stent coating method and underlines the importance of developing substances that are more effective in promoting cell attachment. Moreover, relevant research has confirmed that gene transfection-mediated expression of VEGF in ECs promotes re-endothelialization and suppresses neointimal hyperplasia.122,123
Mesenchymal stem cell
MSCs are cells with multipotent properties that can be easily isolated from sources such as the umbilical cord, bone marrow, and adipose tissue.124–127
Cytokines and growth factors secreted by MSCs can increase cell survival and induce cell differentiation. To improve re-endothelialization, MSCs were applied to the surface of the stent (Fig. 4).
128
The use of MSCs offers advantages in terms of cell recovery and anti-inflammatory properties.
128
The researchers seeded MSCs onto stents coated with gluten and polylysine, while stainless-steel stents were used as controls.
128
The MSCs were seeded onto the stent at a density of 1
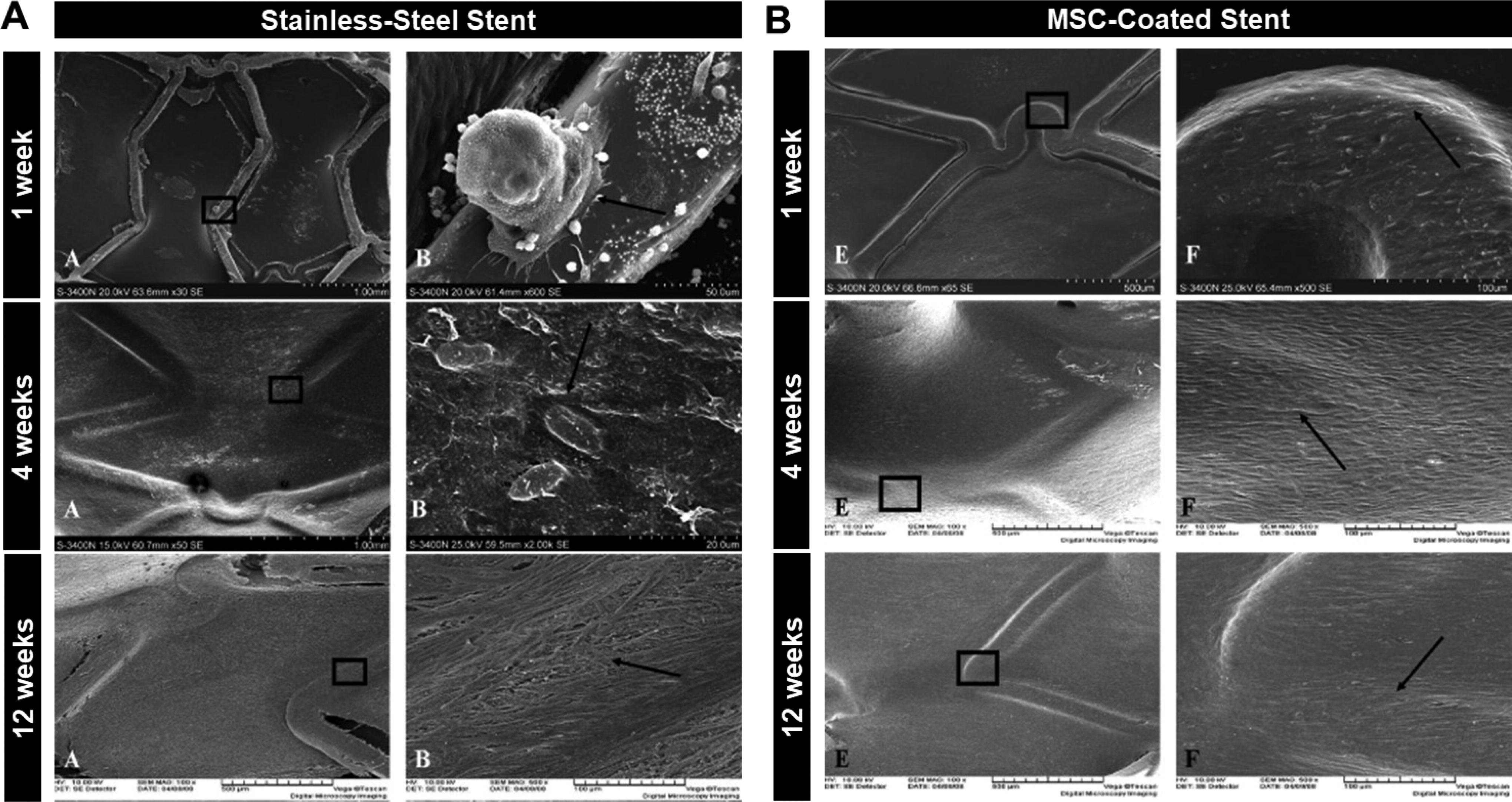
MSC-coated stent for re-endothelialization. Re-endothelialization and thrombus formation were evaluated by SEM imaging of the retrieved posttransplanted stents.
In a related study, MSCs engineered to secrete VEGF and hepatocyte growth factor (HGF) using a genome editing system were coated on a cobalt-chromium stent.
129
The stent was coated with a 1 mg/mL dopamine solution dissolved in 10 mM Tris-buffer and washed three times with ultrasonication before being dried.
129
After dopamine coating, the stent was incubated overnight in 50 μg/mL FN solution followed by seeding with 1
EV coating
Cell-derived EV coating
Exosomes are a type of EVs that range in size from 40 to 200 nm, composed of a lipid bilayer, containing nucleic acids and proteins inside.130–137 They play a significant role in cellular interactions and material exchange in physiological processes. In the field of regenerative medicine, exosomes are widely studied due to their nanosized structure having less risk of capillary stenosis, lower immunogenicity, and the ability of storage in a ready-to-use form as a nonliving biomaterial, compared with the parent cells.138–142 Particularly, MSCs secrete numerous exosomes based on their paracrine activity. The MSC-derived exosome (MSC-Exo)-coated stent was engineered to release exosomes in environments where reactive oxygen species (ROS) are generated. 143 Oxidative stress occurring in atherosclerosis induces neointimal hyperplasia, SMC proliferation, and ECM deposition.144,145 MSC-Exos share similar properties with MSCs, including anti-inflammatory effects and promotion of EC proliferation. Exosomes were attached to the stent surface using ROS linkers that can be cleaved in conditions of local ROS production. 143 Approximately 20% of exosomes were released from the stent over 48 h under normal vascular conditions. 143 However, in environments that produce ROS, 40–60% of exosomes were released from the stent over the same time. 143 The released MSC-Exos promoted EC proliferation while inhibiting SMC proliferation. 143 In addition, there has been a study utilizing MSC-Exo to promote vascular healing of stents; however, data related to re-endothelialization could not be confirmed. 146 In addition to MSC-Exo, research has been conducted to promote re-endothelialization using HUVEC-derived exosomes (HUVEC-Exo). 147 A 9-mm-diameter nitinol disk was immersed in a 5 mg/mL dopamine solution and incubated at 200 rpm for 24 h. 147 Subsequently, it was coated with heparin and chitosan solutions sequentially to form layers. 147 In this experiment, exosomes combined with endothelial affinity peptide (Cys-Arg-Glu-Asp-Val, REDV) were utilized. 147 The exosomes, REDV, and nitinol surface were immobilized through click reaction. 147 The evaluation of EC proliferation showed that the experimental group, HUVEC-Exo-REDV-coated nitinol disk, had higher EC viability compared with the control nitinol disk. 147 In addition, inhibition of SMC proliferation was observed in the HUVEC-Exo-REDV-coated stent. 147
Serum-derived exosome coating
A study was conducted to promote re-endothelialization following stent implantation by coating the surface of stainless steel with blood-derived exosomes. 148 Exosomes are secreted by cells and function as carriers of proteins, lipids, nucleic acids, and other substances. They are involved in cell physiology by influencing cell migration, differentiation, and immune responses. PDA/exosome coating increased EC attachment to the stent surface and contributed to improved EC function. 148 An 8-mm-diameter stainless steel disc was immersed in a 2 mg/mL dopamine solution followed by a 25 μg/mL concentration of exosome solution and incubated at 37°C for 16 h. 148 Following this, immobilized exosomes were removed by washing with PBS. 148 Exosome-coated stainless steel disk inhibited the adhesion of M1 macrophages involved in inflammation and the proliferation of SMCs, while an anti-inflammatory effect was observed along with the expression of M2 macrophage phenotype and contractile SMCs. 148 Similar experiments involved coating the surface of a ZE21B alloy with PDA, followed by immobilizing exosomes onto the surface (Fig. 5). 107 Released exosomes increase EC proliferation and decrease inflammation and ROS levels of macrophage. 107 Furthermore, another study has also corroborated the promotion of HUVEC proliferation and the inhibition of SMC phenotype modification through the application of a neurointerventional nitinol-based stent coated with serum-derived exosomes. 149 Exosome coating strategies onto the stent surface are currently undergoing extensive research as one of the promising candidates for replacing DES, due to their therapeutic efficacy inherited from the parent cells and minimized side effect from abnormal cell fate as not being a living biomaterial, compared with cell therapy.
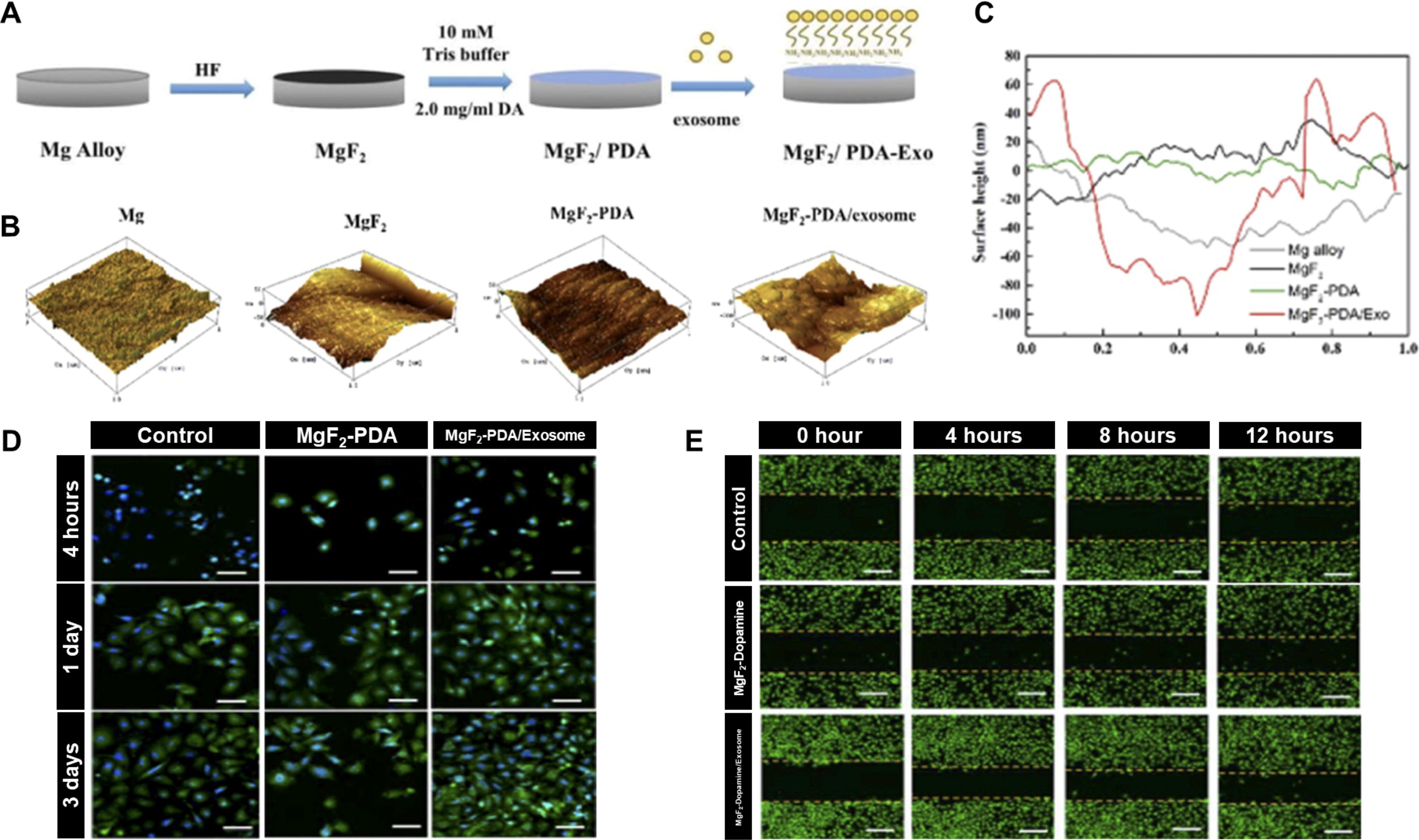
Serum-derived EV-coated stent for re-endothelialization.
Conclusion
The surface coating of stent has been extensively researched over time to minimize the postimplantation side effects. Antibodies or aptamers to capture circulating EPCs have been recently studied widely, but their low therapeutic effect and side effect such as the unexpected fate of EPCs have been repeatedly reported. In recent times, ECM and cell-based coatings have presented a novel breakthrough for challenges unaddressed by biocompatible polymers and antistenotic drugs. Consequently, they have emerged as promising materials to enhance the long-term safety of stents. ECM components such as collagen, laminin, and FN have provided an environment in which ECs can efficiently attach to stents, especially in cases where re-endothelialization is difficult due to rapid blood flow. In addition, cell- or EV-coated stents are considered to have great potential as significantly reduced the time required for re-endothelialization and prevented the attachment of platelets and leukocytes. Particularly, EVs containing the therapeutic effects identical to those found in their parent cells have been proposed as a promising alternative by overcoming the limitations of cell therapy. However, the stability of cell- and EV-based coatings under arterial blood pressure needs to be studied more thoroughly, due to the risk of biogenic aggregates detaching from stents, which could potentially occlude blood vessels, along with host immune responses. Since the application of biogenic materials in stent engineering is in its early stages of development, extensive preclinical and clinical studies are essential to thoroughly evaluate their safety, efficacy, and long-term stability to ensure that they can reliably improve patient outcomes without introducing new risks.
Footnotes
Authors’ Contributions
Conceptualization: J.-K.Y. and S.-H.H. Writing—original draft: M.-K.K. and S.-H.H. Writing—review and editing: S.-H.H. and J.-K.Y.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was financially supported by (i) the