
Abstract
Autologous fat grafting has been widely adopted in cosmetic and reconstructive procedures recently. With the emerging of negative-pressure-assisted liposuction system, the harvesting process of fat grafting is more standardized, controllable, and efficient. Each component in the system could influence the biomechanical environment of lipoaspirate. Several reviews have studied the impact of negative pressure on fat regeneration. As the initial part of the harvesting system, cannulas possess their unique mechanical parameters and their influence on lipoaspirate biomechanical characters, biological behaviors, and regeneration patterns remains unclear. Basic in vivo and in vitro studies have been performed to determine the possible mechanisms. Instant in vivo studies focus on adipocytes, stromal vascular fraction cells, fat particles, and growth factors, while in vivo grafting experiments analyze the graft retention rate and histology. Understanding the different regeneration patterns of lipoaspirate and the mechanisms behind may facilitate the choice of harvesting cannulas in clinical practice.
Impact Statement
The retention rate and regeneration pattern of autologous fat grafting vary widely. As a mechanically sensitive tissue, fat experiences various kinds of forces and shows different biomechanical characters, which could also affect the graft result. However, a comprehensive overview of biomechanics in fat grafting is absent. In this review, we focus on negative-pressure-assisted harvesting step (especially cannulas) and summarize the available in vivo and in vitro studies. This review innovatively employs biomechanical knowledge to link clinical instruments, laboratory experiments, and animal studies together, providing alternative strategies for plastic surgeons to choose harvesting cannulas during fat grafting.
Introduction
Autologous fat grafting has become a widely adopted technique in cosmetic and reconstructive procedures over recent decades, including breast augmentation, breast reconstruction, and facial contouring. 1 The history of fat grafting could be divided into three distinct periods: the open-air period, the nonpurified or traumatic period, and the purified or atraumatic period (Coleman technique). 2 At the beginning, adipose tissue was obtained by surgical excision. With the introduction of negative-pressure-assisted harvesting methods, fat grafting offers unique advantages, such as a minimally invasive approach, and higher procedural efficacy and became polular. 3 Then Coleman published a standardized, controllable, and efficient protocol, which further improved the popularity of negative-pressure-assisted fat grafting. 4 Plastic surgeons now select harvesting methods based on clinical demands, such as the body mass index of the patient, the condition of the recipient site, the volume of the fat required to transfer, and the procedural efficiency. 5 However, the specific impact of the components of liposuction systems on fat regeneration remains unclear.
Fat, composed of adipocytes and stromal vascular fraction cells (SVFs), is sensitive to mechanical forces, which can alter the biological behavior of lipid droplets within mature adipocytes. 6 During the harvesting process (Fig. 1), fat is subjected to mechanical forces such as negative pressure and shear stress. 7 These stimuli affect different tissue components diversely, resulting in variations in the characteristics and regeneration patterns of the lipoaspirate. 8 While several reviews have examined the impact of negative pressure from suction pumps or syringes on fat regeneration, the biomechanical parameters of lipoaspirate and the biomechanical environment in the whole suction system (specifically cannulas) have recently garnered attention from plastic surgeons.
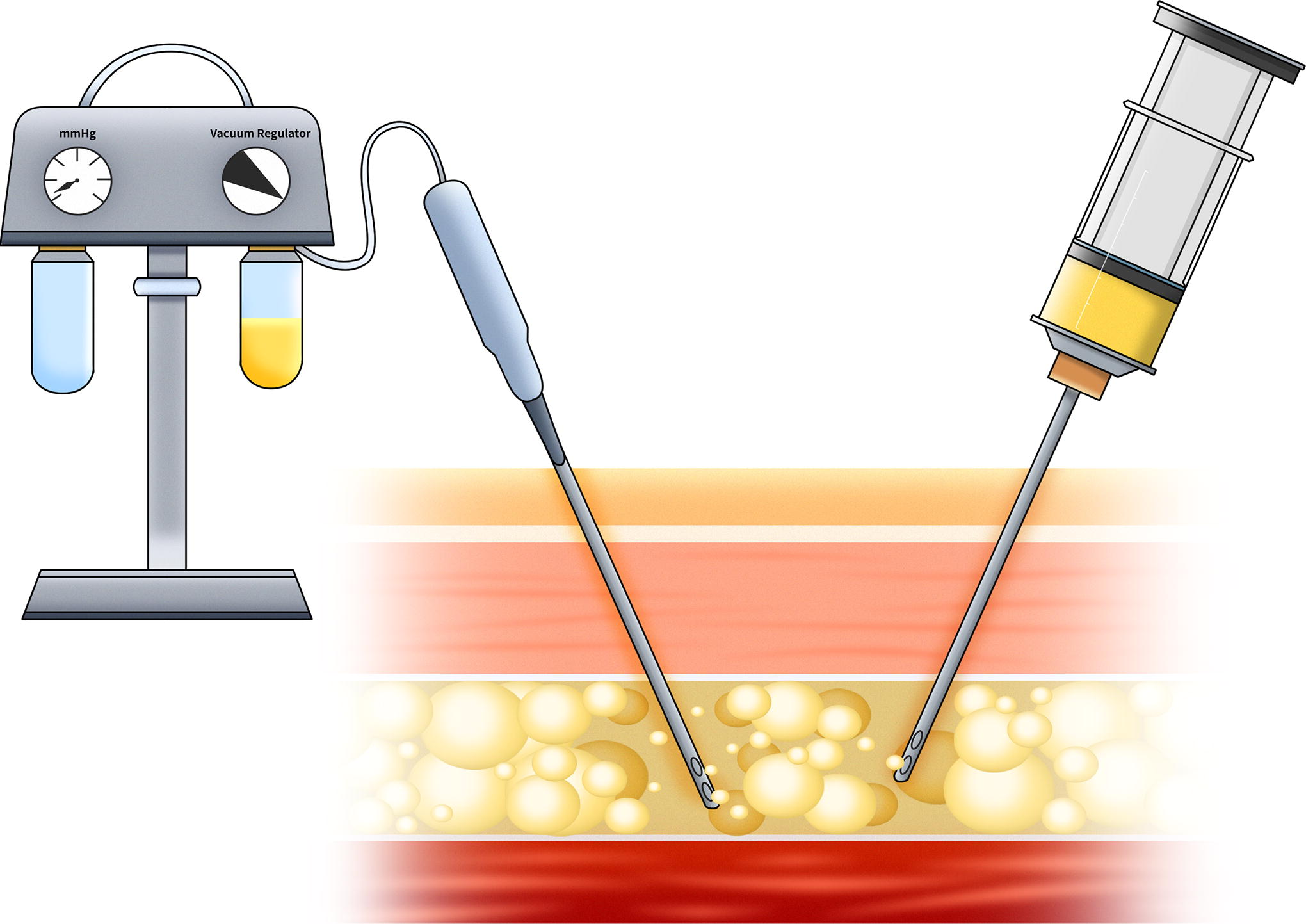
Graphic illustration of negative-pressure-assisted liposuction in clinical practice. Negative-pressure-assisted liposuction system is composed of harvesting cannulas, connecting tubes, and syringes (right) or suction pumps (left) which could generate negative pressure.
This review aims to summarize the biomechanical characteristics of lipoaspirate and the biomechanics within negative-pressure-assisted suction systems, including factors like negative pressure, frictional loss, and dynamic loss. It will particularly focus on the design of cannulas and their biomechanical influence on the biological behavior and regeneration patterns of lipoaspirate.
Biomechanical Characters of Lipoaspirate
Lipoaspirate, being an incompressible fluid, exhibits rheological properties such as storage modulus and viscosity. A higher storage modulus indicates a greater ability of the fluid to resist force, while higher viscosity means the fluid is more resistant to spreading. One study measured the elastic modulus of Coleman fat at 69.94 ± 15.61 Pa. 9 Other studies have assessed the viscosity of Coleman fat, finding it ranges from 15.37 to 140 cSt.9–11 Tong et al. also studied the viscosity of four samples harvested by suction pump and observed a mean viscosity of 5.4 cP. 12 The considerable variations in these results can be attributed to differences in viscosity measurement methods, with syringe-based methods yielding higher values than sensor-based devices (Fig. 2, above).
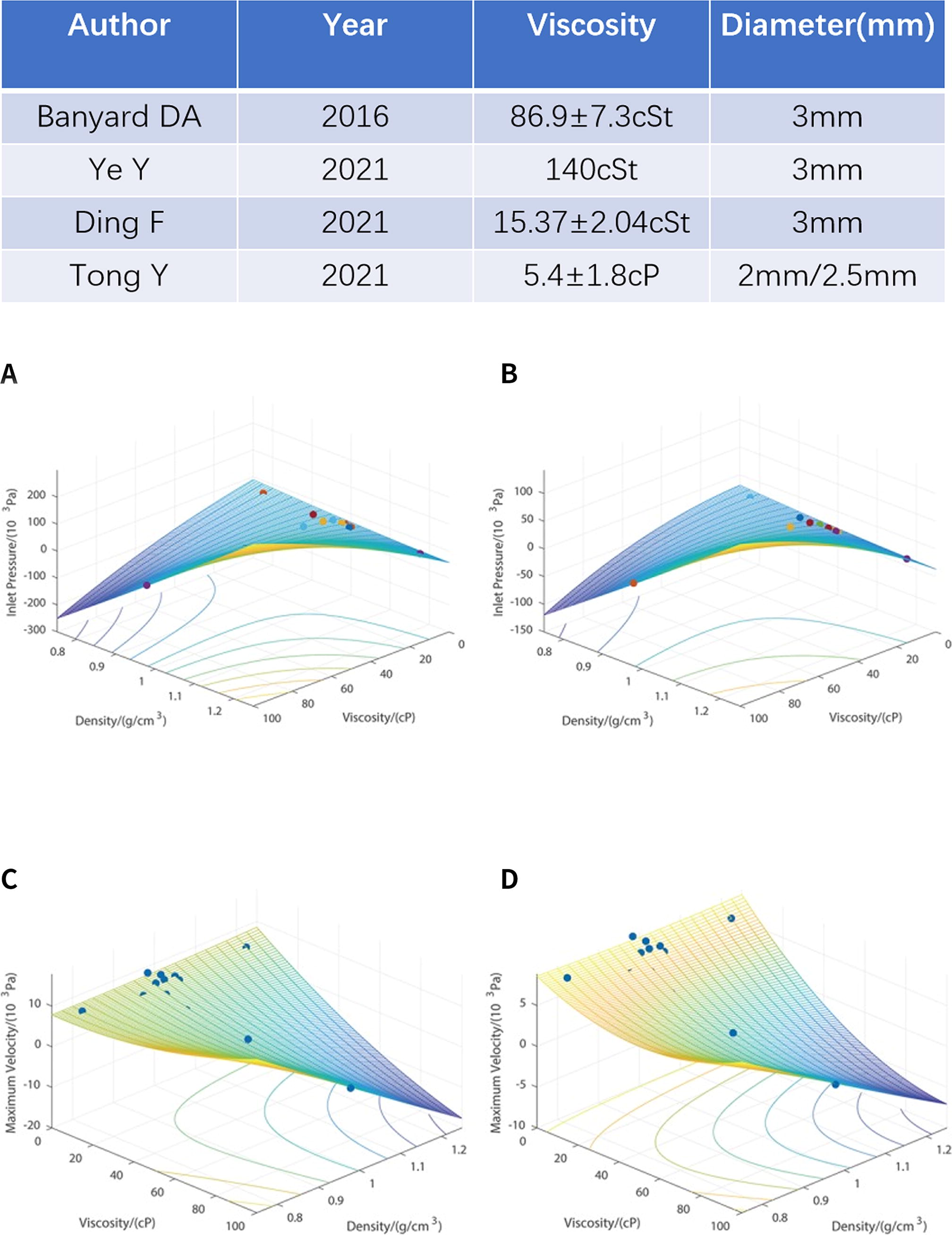
Viscosity of lipoaspirate of the existing studies and its relationship with inlet pressure and maximum velocity according to Tong et al.
12
Details of the experiments studying lipoaspirate viscosity are summarized in a table (above). The relation among the inlet pressure, viscosity, and density of liposuction cannula with a diameter of 2.5 mm
Newton categorized fluids based on whether their viscosity is independent of the shear rate. A Newtonian fluid is characterized by viscous stresses that are linearly correlated to the local strain rate. 13 Newtonian fluids are the simplest mathematical models of fluids that incorporate viscosity. Using this concept, Tong et al. developed a Newtonian fluid mathematical model to simulate the behavior of lipoaspirate during harvesting. They found that lipoaspirate harvested with a 2.5 mm cannula behaved as a Newtonian fluid. However, in the 2 mm cannula group, the relationship between inlet pressure and viscosity reversed when viscosity decreased further, indicating non-Newtonian behavior (Fig. 2, middle). 12 This information could be used to predict the flow state of lipoaspirate in cannulas. When Newtonian fluids flow through a cannula, increased shear stress near the walls causes a decrease in velocity. This leads to a faster fluid flow at the center of the pipe, and a slower fluid flow at the walls. In contrast, the velocity profiles are asymmetrical, changing, and unpredictable for non-Newtonian fluids because the shear stress affects not only the viscosity. 14
Biomechanics in Negative-Pressure-Assisted Suction System
Negative-pressure-assisted liposuction was initially developed to harvest fat through small incisions, reducing both procedure time and associated risks. 15 Whether powered by suction pumps or syringes, the effectiveness of this system relies on the pressure differential, enabling the aspirate to flow from the higher pressure within the body to the lower pressure in the collection container. 16 As a viscous fluid, lipoaspirate experiences friction loss while passing through the cannula, which is influenced by the generalized Reynolds number. Furthermore, dynamic loss occurs when the direction of the lipoaspirate is altered by any component of the suction system 17 (Fig. 3).
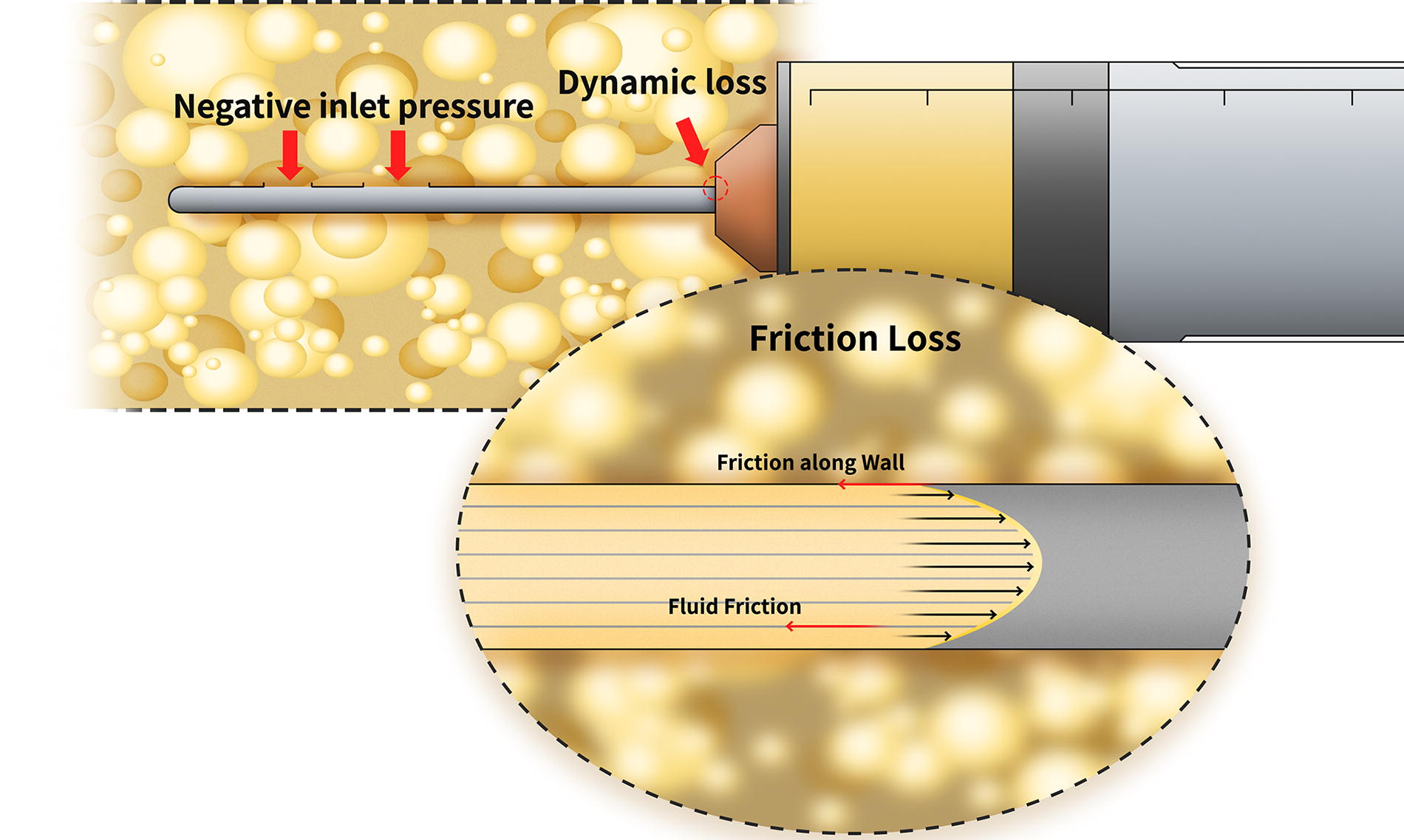
Schematic illustration of the flow state and biomechanics of lipoaspirate in suction cannulas. Lipoaspirate suffers from negative inlet pressure around the aperture at the head of the cannulas and from fluid friction and wall friction inside the cannulas. Dynamic loss occurs when the flow directions of the lipoaspirate change.
Negative pressure
Negative pressure refers to the difference between ambient atmospheric pressure and the internal pressure generated either by suction pumps or syringes. Most studies referenced in this article use syringes ranging from 10 to 65 mL to create a vacuum, with maximum negative pressures ranging from −0.81 atm (−615.6 mmHg) to −0.96 atm (−729.6 mmHg). In general, larger syringes could generate higher negative pressure. However, the maximum achievable negative pressures of syringes do not increase proportionally with volume; the pressure/volume curve slope drops significantly within 10 mL. 7 Some surgeons also use suction pumps to harvest fat, with parameters ranging from −250 to −700 mmHg. 18 Although syringes are more accessible and widely used, suction pumps can generate a more consistent negative pressure, and the large containers to collect lipoaspirate make the mega-volume grafting more efficient. Reviews have shown mixed results regarding the impact of suction pressure: half of the experiments indicated better outcomes with low negative pressure, while the other half reported no significant differences. Interestingly, no studies have shown better results using high negative pressure.19–21
Friction loss
In a negative-pressure-assisted suction system, there are two types of cannulas: harvesting cannulas and grafting cannulas. Most of the harvesting cannulas are cylindrical duct of uniform diameter, made of hard mental, and share common characters such as smooth-surfaced, straight, and parallel. 4 The design and selection of cannulas vary significantly, featuring different internal diameters, lengths, and aperture sizes and numbers. 22 Each of these parameters can affect the flow state of lipoaspirate in harvesting cannulas.
The lipoaspirate in the cannula presents inertial forces against viscous forces, which is called fluid friction (a unitless measure of pressure drop per unit length of pipe), and is dependent on the Reynolds number. 23 For lipoaspirate flowing in the cannula, the Reynolds number is generally defined as ReD = ρνD/μ = ρQD/μA (ρ is the density of the fluid, ν is the mean velocity of the fluid, D is the internal diameter of the cannula, μ is the dynamic viscosity, Q is the volumetric flow rate, and A is the cross-sectional area). 24 Usually, laminar flow occurs when ReD <2300 25 and turbulent flow occurs when ReD >2900.26,27 Tong et al. tested the viscosity and density of the lipoaspirate harvested with 2.5 and 2 mm cannulas and simulated the velocity profiles within the cannulas. We used their data to calculate the ReD of lipoaspirate and found it much lower than 2300, indicating a laminar flow in cannula. Their simulation of velocity distributions showed that lipoaspirate flows slowly and asymmetrical at the inlet of the cannulas and become laminar when stable, which is also in line with our calculation and hypothesis. 12 In fluid dynamics, the Darcy–Weisbach equation is an empirical equation that relates the pressure loss, due to friction along a given length of pipe, to the average velocity of the fluid flow for an incompressible fluid. In a cylindrical pipe of uniform diameter, flowing full, the friction loss can be characterized as f (△p/L)= fDρν2/2D (L is the length of pipe and fD is the Darcy friction factor). 28 For laminar lipoaspirate in cannulas (fD = 64/Re), then the fluid friction could be calculated by Hagen–Poiseuille equation16—flam(△p/L) = 32μLν/D2 = 128μQ/πD4. Even though the materials of cannulas are steel or other smooth-surfaced metals, lipoaspirate still endures friction along wall of the cannulas. However, since the lipoaspirate adheres to the wall (no-slip condition) and the laminar layers cover the roughness of the wall, this has no additional influence on the pressure loss.29,30 As we discussed above, the friction loss is dependent on the flow rate, so we continue to study this in suction cannulas.
Harvesting cannulas are characterized by three parameters: length, diameter, and aperture size, each of which can affect the speed of lipoaspirate. Scholars concerning the flow rate of lipoaspirate in cannulas all agree that (1) an increase in length results in a decrease in flow rate and (2) an increase in diameter leads to an increase in flow rate.4,17,31 Because the harvesting cannulas are usually designed multiholed at the head, the impact of aperture size should be discussed both in single port area and total port area. Fodor et al. customized a set of suction cannulas with different fabrications and found that: First, if the area of a single aperture exceeded the cross-sectional area of the cannula’s lumen, there was no additional benefit of total port area/lumen area in terms of flow rate. Second, if the area of a single aperture was less than about half the area of the lumen, the flow rate significantly decreased with the drop of total port area/lumen area. This phenomenon was only observed when port number reduced from two to one, which could be explained by the nature of negative-pressure-assisted liposuction. Suction cannulas work by avulsion of adipose tissue. When there is only one small side port in the head of the suction cannulas, the avulsed fat particles and fibrous adipose tissue would easily clog around the inlet port, resulting in a reduction in flow rate. Third, when the total port area exceeded about 1.5 times the cross-sectional area of the lumen of the cannula, there was no additional benefit with regard to speed as total port area/lumen area increased. Specifically, when invented in comparable total port area/lumen area ratio and internal diameter, the flow rate of a multismall port design was faster than the two-large port design by an average of 24%. 31
Previous studies showed that as the cannula diameter increases, both the lipoaspirate viscosity 12 and the flow rate 31 increase. Then the friction loss (quantified by flam) of the lipoaspirate in cannulas is even harder to predict. To address this, Fodor et al. 31 introduced an empirically derived concept of Resistance = L/D1.5. This simple but elegant formula could be used to roughly estimate the friction loss and flow rate of the cannulas, guiding the selection of harvesting cannulas in clinical application.
Dynamic loss
Dynamic loss arises from disturbances in the lipoaspirate flow caused by components that alter its direction, such as the cannula inlet, sudden changes in the internal passage area, and the discharge of lipoaspirate into the pump. 31 Existing data indicate that the greater and more abrupt the changes in flow speed, the higher the dynamic loss. However, due to the significant variations in liposuction systems and their components, calculating dynamic loss is challenging. 17 Although computerized simulations have been employed to predict lipoaspirate motion, the precise calculation of dynamic loss in liposuction systems remains an area that requires further research.
Biomechanical Parameters of Harvesting Cannulas and Their Influence on Lipoaspirate
Adipose tissue is supported by a structured extracellular matrix (ECM) that includes mature adipocytes encased in fibrous septa, a reinforced basement membrane, 1 and highly heterogeneous SVFs located within the ECM and around the capillary network. 32 The nature of negative-pressure-assisted liposuction is avulsion of fat particles from the surrounding tissue. Two evaluators of the flow in cannulas may affect the microstructure of lipoaspirate: the inlet negative pressure around the aperture and the maximum velocity of the flow. A higher inlet negative pressure would tear the adipocytes harder and may cause severer damage to the capillary, releasing more SVFs and tissue fragments. Meanwhile, a higher maximum velocity can cause sharper pounding between the adipocyte. The existing one study showed that both inlet negative pressure and maximum velocity were higher in smaller cannulas. 12 The studies reviewed here primarily focus on the biomechanical impact of cannulas on components of lipoaspirate. See Table 1 for the list of articles used in this review with in vitro characteristics.
Details of the In Vitro Studies Investigating Influence of Harvesting Cannulas on Lipoaspirate
Adipocytes
Each adipocyte is ∼80 μm in diameter and contains a large lipid vacuole, which is susceptible to rupture by mechanical force. 33 When adipocytes rupture, they exhibit morphological changes such as membrane wrinkling, pore opening with oily material leakage, a reduction in cellular diameter, and partial to total collapse of the cellular membrane. 34 Rubino et al. compared 2 and 3 mm cannulas using scanning electron microscope (SEM) and found no significant differences in adipocyte diameter between the two groups. The authors attributed this to SEM’s limitation of providing only a two-dimensional view, which is insufficient to capture the collapse of the outer membrane and volume decrease of mature adipocytes. 34 Several other studies also examined the morphology of lipoaspirate using hematoxylin and eosin (H&E) staining.18,35,36 These studies consistently found significant cell damage in the group harvested with a 1 mm cannula, while no significant differences of adipocyte diameter were observed among the groups harvested with 2–4 mm cannulas. The 5 mm group showed nearly no cell loss.
In addition to morphology, the number of viable adipocytes was also studied. Most studies utilized collagenase digestion and trypan blue vital staining, finding that lipoaspirate harvested with a 6 mm cannula contained more viable adipocytes compared to smaller cannulas. However, the results for 2 and 4 mm cannulas were inconsistent. Ozsoy et al. reported that lipoaspirate harvested with 4 mm cannulas had 216% more viable adipocytes than that harvested with 2 mm cannulas. 37 In contrast, Erdim et al. found that although the mean number of viable adipocytes was higher in the 4 mm group, there was no statistically significant difference in adipocyte viability between 2 and 4 mm cannulas. 38 Additionally, Mecott et al. used customized cannulas and discovered that aperture size did not influence the viability of adipocytes in the aspirate. 39
We could preclude from the data that significant adipocytes rupture happens when cannula diameter is below 2 mm, and nearly no cell loss occurs in groups with cannula diameter above 4 mm. As for the diameter range from 2 to 4 mm, the adipocyte morphology and number of viable adipocytes remain a controversy. One explanation could be that lipoaspirate harvested with larger cannulas experiences less cellular disruption from mechanical manipulation. However, the diameter of most popular used cannulas happens to range from 2 to 4 mm, resulting in a various designs and different combinations of aperture size and cannula diameter and length. Due to the existence of confounding variables, it is hard to draw a conclusion from these clinical experiments.
SVFs
Becker et al. defined SVFs as fractions that could pass through a strainer with 0.5-mm openings and found that the volume of SVFs was higher in the 5 mm group when compared with the 1 mm group. 40 Other studies reviewed here all processed SVFs using the standardized protocol previously described.41,42 The number of viable cells was determined by excluding those with stained nuclei, indicating nonviable cells. 43 Both Alharbi et al. and Trivisonno et al. compared SVFs from aspirate harvested with 2 and 3 mm cannulas, noting that the total number of SVFs and adhesion rate were significantly higher in the 2 mm group, although cell viability was similar between the two groups.
Researchers proposed two main reasons for the higher number of SVFs in the 2 mm group. First, the higher surface-to-volume ratio of harvested pieces in the 2 mm group indicated that each cell experienced more stress, making SVFs more easily dislodged from the ECM. 42 Second, SVFs typically reside around vascular structure, 44 and smaller cannulas might facilitate the harvest of more superficial layers of adipose tissue, which are more vascularized and contain more SVFs. 43 Additionally, the higher adhesion rate of SVFs in the 2 mm group may be due to a higher concentration of growth factors, enhancing the adhesion response of stromal cells. Due to their spindled shape, stromal cells are less likely to be damaged by mechanical force, which helps maintain their viability across different groups. 45 Interestingly, SVFs in the lipoaspirate harvested by smaller cannulas exhibit higher adipogenic 46 and angiogenic 43 potential although the reasons for this remain to be further investigated.
Fat particles
Adipose tissue harvested using suction cannulas typically appears as “fat particles,” 47 which comprise 98–100% intact adipocytes, small blood vessels, and fibrous tissue at the core, with 10%–15% cell disruption at the periphery. 18 The size of these fat particles depends on the parameters of the harvesting cannulas, including diameter, aperture size, and design. Even when using the same cannula, the particle size can vary significantly, with the largest particles corresponding to the diameter of the cannula.48,49 Generally, fat particles collected with smaller cannulas are much smaller in diameter compared with those harvested with larger cannulas.43,49 Pak et al. examined the size of fat particles and found that in groups using smaller cannulas, the average size of stromal fragments (including fibrous tissue and collagen fibers) was less than 1 mm. In contrast, in groups using larger cannulas, 37.5% of the fragments averaged 1–1.5 mm, and in 25% of cases, the fragments exceeded 1.5 mm. 36 Yang et al. compared four most popular commercially available cannulas and found fat particle diameter ranging from 1.9 ± 0.59 to 3.03 ± 0.78 mm. 49 Collectively, the size of fat particles harvested by different cannulas in this review ranges from 1 to 3 mm. Our own experiment also observed that fat harvested by cannulas with different combinations of diameter and aperture (3 mm (7 × 1.5 mm), 4 mm (9 × 2 mm), and 5 mm (10 × 2.5 mm)) exhibited fat particle size ranging from 1.23 to 1.59 mm (data not shown). We were surprised to find that it may be the aperture size rather than the diameter of cannula that determines the size of fat particles. Moreover, as fat particles could squeeze into the apertures, the inlet negative pressure around the ports may be another crucial factor.
Growth factors
The secretory abilities of adipose tissue, particularly the paracrine effects of SVFs, have been extensively studied. 49 Paracrine signals include vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), insulin-like growth factor (IGF), platelet-derived growth factor (PDGF)-BB, and various inflammatory cytokines. 50 When mechanical force is applied to adipose tissue, SVFs are released from the surrounding ECM and secrete growth factors. Alharbi et al. conducted a comparative study on the growth factors released by adipose tissue harvested using 2 and 3 mm cannulas on the contralateral area of the abdomen. 42 This study is currently the only one addressing the influence of cannula design on growth factor secretion. They found that the concentrations of IGF-1 and VEGF were significantly higher in the 3 mm group than in the 2 mm group, while no significant differences were observed in the concentrations of bFGF and PDGF-BB.
As we discussed previously, the smaller cannulas could generate higher inlet pressure and maximum flow velocity, resulting in harder avulsion of fat particles from surrounding tissue, releasing more soluble growth factors from the ECM. In clinical practice, the native aspirate sample is often centrifuged, discarding the upper oil layer and lower aqueous layer to collect purified fat. This process makes soluble factors like IGF-1 and VEGF move to the aqueous layer. Then lower testable concentrations of the sample were observed in the 2 mm group. Since bFGF and PDGF-BB are more intracellular, their concentrations remain unaffected by the processing steps and are similar between groups. 42 Additionally, Yang et al. cultured fat particles and observed that VEGF concentrations were significantly higher in the 5–7 mm group compared with the 2–4 mm group at days 4 and 6. This suggests that larger particles experience increased hypoxia, leading to the secretion of more revascularization-related growth factors compared with smaller particles. 49
Biomechanical Influence of Harvesting Cannulas on Fat Regeneration
Retention rate and histology of the grafts
Most studies reviewed here observed a consistent trend: retention rates increased with cannula diameters, specifically within the 2–5 mm range.12,51 However, evaluating the regeneration pattern requires more than just retention rate; histological changes in the grafts are also important. De Arruda et al. conducted an autologous fat grafting experiment in a porcine model, comparing graft integration between 3 and 5 mm groups at day 28. Using H&E staining to identify intact adipocytes, fat necrosis, fibrosis, inflammation, and oil cysts, along with immunohistochemical staining for perilipin-A, TNF-α, and CD31-positive cells to represent adipocytes, tissue necrosis, and neoangiogenesis, respectively, they found no significant differences between the groups. 52 In early stages (6 weeks), Kirkham et al.’s histological analysis showed more intact adipocytes, fewer inflammatory cells, and less fibrosis in the 5 mm group compared with the 3 mm group. 51 Tong et al. extended the observation period to 6 months, noting the presence of central necrosis and small oil cysts in the periphery of grafted fat in the 2.5 mm group, while no oil cysts were observed in fat harvested with a 2 mm cannula. 12 See Table 2 for the list of articles used in this review with in vivo characteristics.
Details of the In Vivo Studies Investigating Influence of Harvesting Cannulas on Fat Regeneration
Summarizing these findings (Fig. 4, right):
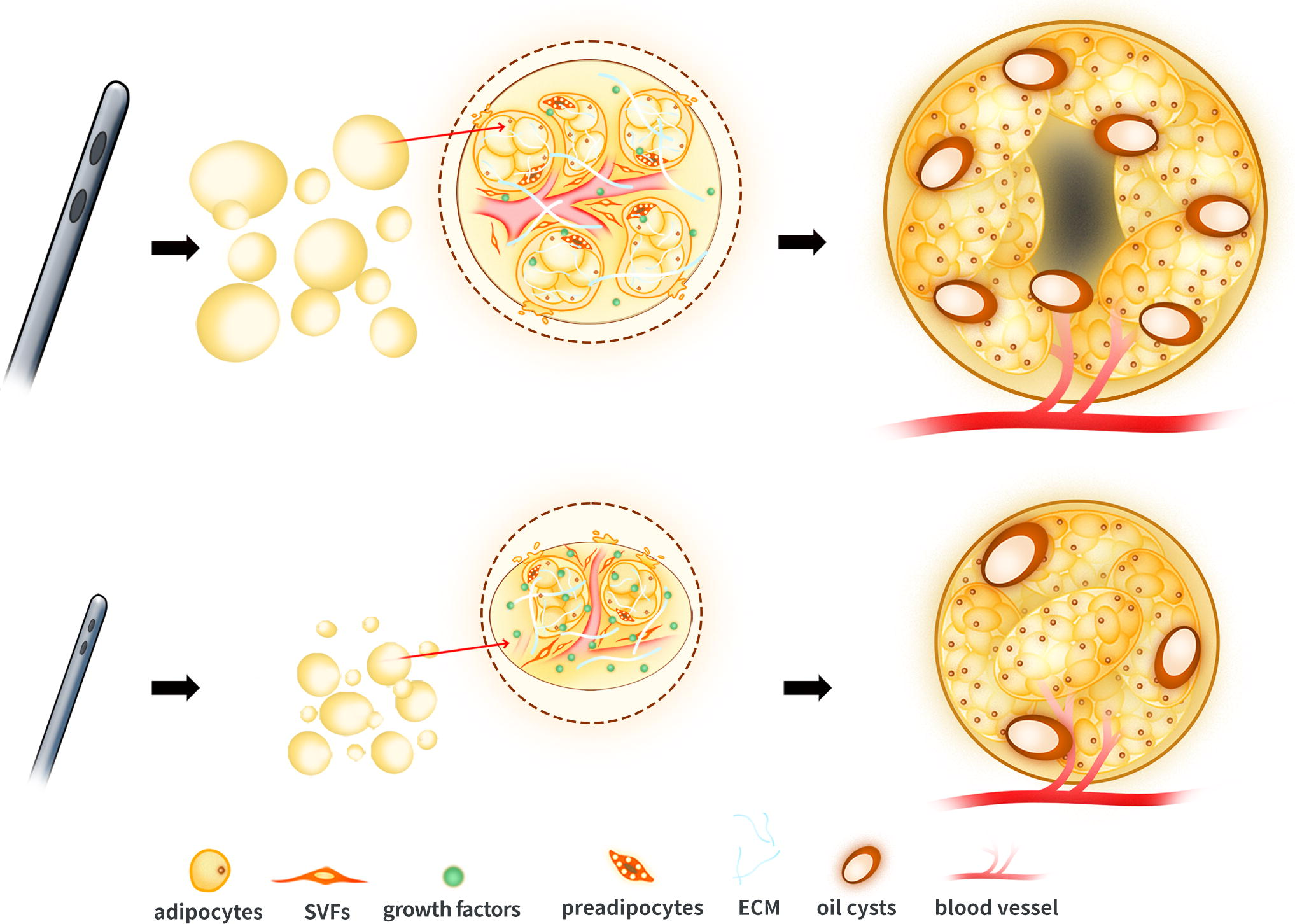
Schematic illustration proposed influence of harvesting cannulas on lipoaspirate microstructure and fat regeneration. Cannulas with larger diameter and aperture generate larger fat particles (left row), with more intact “fat lobule” structures, fewer released growth factors and vascular fraction cells (SVFs) in each particle (middle row). Long-term observations show that grafts from larger cannula groups tend to develop central necrosis and more oil cysts, yet obtain larger volume retention (right row).
1. Larger cannulas generally result in better fat regeneration when assessed by retention rate.
2. Grafts from larger cannula groups tend to develop central necrosis and more oil cysts in the long term, yet show more intact adipocytes, fewer inflammatory cells and less fibrosis in the early stages.
Our previous animal studies align with these conclusions. By mincing the inguinal fat pads of mice into particles with 1-mm interval diameters and allografting them, we found similar results. 47 Overall, retention rate alone is insufficient to evaluate the regeneration patterns of grafted fat. The contradictory histological findings at early and late stages indicate that fat grafts with different particle sizes exhibit distinct regeneration patterns.
Regeneration patterns for grafts with different particle sizes
Unlike en bloc fat grafting, free fat grafts exposed to injury and mechanical forces during harvesting exhibit unique regeneration patterns. Currently, three primary theories describe this process: graft survival theory, host cell replacement theory, and the three-zone theory.53–55
The graft survival theory, first proposed by Peer et al., 56 suggests that intact adipocytes initially survive through nutrient diffusion from plasma 57 until neo-vessels grow from the recipient site. 58 Conversely, the host cell replacement theory has gained traction, supported by multiple studies.59,60 For instance, Dong et al. conducted a long-term cross-grafting experiment with fragmental fat and found that graft angiogenesis predominantly involved host cells in a “vessel branching” mode, and adipogenesis mainly occurred in adipose precursor cells derived from the host. The landmark “three-zone theory” by Eto et al. described three distinct zones from the periphery to the core of a grafted fat pad in mice at 2 weeks: the surviving area (where adipocytes survived), the regenerating area (where adipocytes died but ASCs survived and replaced dead adipocytes), and the necrotic area (where both adipocytes and ASCs died). 61 This study was the first to report that some mature adipocytes might die and be replaced by ASCs although it did not identify the source of these ASCs. Hong et al. refined this theory using cell-assisted free fat grafting in two different transgenic reporter mice. 62 Their findings included the following: first, donor ASCs contributed to angiogenesis directly by differentiating into endothelial cells and indirectly by secreting growth factors to promote vascular ingrowth from the recipient; second, surviving donor ASCs could differentiate into mature adipocytes, integrating well with both donor and recipient adipocytes. This evidence supports a combined concept of graft survival and host replacement theory. 54
Neovascularization, whether from the donor or the host, is crucial in fat graft regeneration. 63 In clinical practice, the graft-to-recipient interface and interstitial fluid pressure limits64,65 are vital for nutrient diffusion from plasma and revascularization from surrounding tissue posttransplantation. 66 However, the roles of donor and host cells in the revascularization of fragmental fat grafts remain debated. Dong et al. asserted that graft angiogenesis was primarily driven by host cells via a “vessel branching” mode. 59 In contrast, Hong et al. concluded that donor ASCs directly participated in angiogenesis by differentiating into endothelial cells and integrating with the host vascular structure. 62 To clarify the angiogenesis pattern and revascularization stages in fragmental fat grafting, Fu et al. conducted an innovative animal experiment. They mixed GFP-positive SVFs with minced inguinal adipose tissue from C57BL/6J mice and co-implanted them into nude mice. 67 They observed CD31+ cells forming small clusters by day 14 and mature vascular structures by day 28. Donor ASCs were initially detected next to these vascular structures on day 28 and eventually fully incorporated into them. Additionally, donor ASCs were found among the new blood vessels. Data in the previous part of this review indicates that fat harvested by smaller cannulas appears in smaller particles, with severe capillary damage inside. Therefore, host cells mainly contribute through a classic “vessel branching” mode in smaller ones, whereas larger cannulas often generate larger particles, with more intact native vasculature. Then integration of host and donor vasculature is more common in larger ones.
Regarding adipogenesis, the conventional “three-zone theory” primarily explains phenomena observed in en bloc inguinal fat pad grafting. Subsequent experiments on adipogenic mechanisms in fragmental fat grafting have not reached a clear consensus. Dong et al. observed that almost all mature adipocytes and SVFs died within the first week postgrafting, with only a few surviving in the outer layer. As host blood vessels grew into the graft, a significant number of recipient-derived CD34+ cells infiltrated and gradually replaced the tissue through differentiation from week 4 onward. 59 Conversely, Li et al. proposed that mature adipocytes initially endure an avascular environment postgrafting, leading some adipocytes to lose lipid droplets and shrink in response to hypoxia and ischemia. Adipocytes that did not dedifferentiate died quickly.57,68,69 This aligns with observations by Fu et al., who noted that GPF−/perilipin+ small adipocytes (<50 μm in diameter) appeared on day 14 after grafting, indicating donor-derived dedifferentiated adipocytes. 67 From these studies and the literatures contained in this review, it can be inferred that fat particles harvested by smaller cannulas experience more adipocyte rupture, while contain more SVFs and release growth factors instantly. All these contribute to their possible adipogenic pattern may present as host replacement theory proposed by Dong et al. While larger particles in larger cannula groups possess more intact adipocytes and could exhibit an adipocyte survival and dedifferentiation pattern as suggested by Li et al.
Why do the angiogenic and adipogenic patterns differ between small and large particles? Reviewing the literature, we propose the “fat lobule” hypothesis: a minimal structure necessary for adipocyte survival and is 0.1–0.2 mm in diameter.70–72 The protective mechanism likely involves the robust ECM structure. Fat lobules have two main fibrillar matrix compartments: the stroma and the fibrous septa. The septa, composed of COL1, COL3, and elastin, are dense networks surrounding the lobule units, while the stroma, consisting of laminin, COL4, and perlecan, 44 are sparsely located fibers within the lobules between adipocytes. Each fat lobule is also supplied by a separate arteriole, ensuring a minimal size to maintain adipose function. 73 Although the presence of venules in fat lobules is unclear, this specialized blood supply could influence fat regeneration. A study concerning skin–fat composite grafts already found that preservation of the interlobular septa and vessels resulted in better survival. 74 For free fat grafts, as mentioned above, smaller particles endure severer adipocyte rupture and capillary damage at the periphery, indicating more thoroughly disruption of the “fat lobule” structure. This could also explain the higher concentrations of SVFs and released growth factors in smaller groups (Fig. 4, above, center). By comparison, larger groups show more intact adipocytes and native vasculature, implying better preservation of “fat lobule” structure (Fig. 4, below, center). Even the inventor of the nowadays most popular fat grafting technique—Coleman—himself proposed this hypothesis in his own article nearly 30 years ago. 71 As the laboratory techniques develop, maybe it is time for us to uncover the mystery behind this. Plastic surgeons’ experiences also support this hypothesis.8,66,75,76 However, no clinical studies in this review included both in vitro immediate analysis of aspirate and in vivo graft experiments; so the “fat lobule” hypothesis lacks sufficient evidence and requires further research.
Strategy to Choose Harvesting Cannulas During Fat Grafting
Scholars have contributed various perspectives on surgical decision-making in autologous fat grafting.5,77 Here, we offer our recommendations for selecting harvesting cannulas during fat grafting procedures. First, efficacy is a crucial factor in clinical practice. Larger cannulas with smaller holes can significantly increase the amount of lipoaspirate harvested within the same time frame. 31 Second, for achieving long-term volume increase, larger cannulas are advisable, provided that patients can tolerate the formation of oil cysts.
Footnotes
Acknowledgment
The authors would like to thank Mr. Baicheng Luo for his assistance with graphic illustration of the article.
Authors’ Contributions
Z.Q.: Conceptualization, methodology, investigation, formal analysis, and writing—original draft. G.C.: Data curation, formal analysis, and writing—original draft. N.W. and J.L.: Data curation and investigation. M.Y. and J.W.: Supervision. B.G.: Validation. Z.Z.: Supervision and writing—review and editing. Z.Z.: Conceptualization, funding acquisition, supervision, and writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (82202479, 82102355).