
Abstract
Platelet-rich plasma (PRP) is a blood product with higher platelet concentrations than whole blood, offering controlled delivery of growth factors (GFs) for regenerative medicine. PRP plays pivotal roles in tissue restoration mechanisms, including angiogenesis, fibroblast proliferation, and extracellular matrix development, making it applicable across various regenerative medicine treatments. Despite promising results in different tissue injuries, challenges such as short half-life and rapid deactivation by proteases persist. To address these challenges, biomaterial-based delivery scaffolds, such as sponges or hydrogels, have been investigated. Current studies exhibit that PRP-loaded scaffolds fix these issues due to the sustained release of GFs. In this regard, given the widespread application of PRP in clinical studies, the use of PRP-loaded scaffolds has drawn significant consideration in tissue engineering (TE). Therefore, this review briefly introduces PRP as a rich origin of GFs, its classification, and preparation methods and discusses PRP applications in regenerative medicine. This study also emphasizes and reviews the latest research on the using scaffolds for PRP delivery in diverse fields of TE, including skin, bone, and cartilage repair.
Impact Statement
Platelet-rich plasma (PRP) is a blood product with high platelet concentrations, offering managed delivery of growth factors (GFs) for regenerative medicine. This review briefly introduces PRP as a rich source of GFs and discusses PRP-loaded scaffold applications in soft and hard tissue including skin, bone, and cartilage restoration. In the current study, the applications of PRP-loaded scaffold in soft and hard tissue regeneration (skin, bone, and cartilage) were discussed in detail.
Introduction
Tissue engineering (TE) is an impressive part of biomedical research that has emerged over the past decades, focusing on the cartilage restoration, repair, or replacement of injured or dysfunctional organs and tissues. 1 Fundamentally, scaffolds, biological products including cells, and growth factors (GFs) are the prominent components of TE-based strategies. 2 Scaffolds are three-dimensional biomaterial-based constructs created from biodegradable and biocompatible polymers. These structures resemble the extracellular matrix (ECM), offer mechanical support for cells to attach, grow, and migrate, and also can be utilized to release GFs. 3 Over the recent decades, there has been extensive research on various biomedical applications of scaffolds.4–8 Generally, in clinical studies, the designed scaffold is combined with cells or GFs and cultured in suitable conditions. Afterward, the prepared construct is implanted in vivo to conduct its desired function. 9 Recently, PRP, a hemoderivative type of biological product that is a cocktail of various GFs, cytokine, and biomolecule, has become an attractive therapeutic tool in restoring the injured tissue caused by damage or chronic illnesses. 10 The synergy of these various bio components in plasma and platelets is the PRP-based therapy central cores. 11 On the contrary, PRP has drawn remarkable attention in tissue regeneration, which is related to its safety, straightforward preparation, and low-cost processing. 12 The standard procedure for administering PRP is including patient’s whole blood extraction and centrifugation, followed by its component concentration. Finally, the activated PRP will be delivered to damaged body parts that need to be repaired. 13 Administered PRP may trigger the release of GFs that can accelerate the healing and restoration processes by starting the hemostatic cascade and stimulating revascularization. In addition, connective tissue formation may occur around the injured site.14,15 As mentioned above, PRP is an autologous biological component with no adverse side effects, making it appropriate for a variety of biomedical applications. 16 Although PRP injection into the damaged tissue is the main route of its administration, its effectiveness may be limited by drawbacks such as short lifespan and immediate inactivation in the site of action. To solve these challenges, later studies have focused on developing bioengineering approaches such as applying scaffolds for PRP delivery in a controlled manner. 17 By utilizing this delivery system, the short circulation time and half-life of PRP components are increased, which leads to their stability and durability improvement. 18 In this study, following the introduction of PRP and its applications in tissue regeneration, we had a comprehensive review of scaffold-based PRP delivery in soft and hard tissue regeneration. We have also included findings from previous research on PRP-loaded scaffold incorporation in skin, bone, and cartilage tissue restoration.
An Overview of PRP
The “PRP” term was first raised in the 1970s by hematologists to describe plasma that contains a greater number of platelets compared with peripheral blood. Initially, it was utilized to treat patients with low platelet counts, specifically in the context of blood transfusions. 19 Platelets are cytoplasmic fragments derived from megakaryocytes found in the bone marrow, with a diameter of ∼2 μm, 20 which contain over 30 bioactive proteins, including numerous coagulation factors, adhesion molecules, chemokines, cytokines, integrins, and GFs, such as VEGF, ECGF, FGF, IGF-1, EGF, PDAF, PDGF, HGF, and TGF-β.21,22 Every single GF, which was mentioned earlier, has a vital role to play in hemostasis or tissue healing (listed in Table 1). 32 Furthermore, PRP contains macrophage and monocyte mediators, as well as inflammatory mediators called interleukins (IL). 33 In a general manner, three granules (alpha, delta, and lambda) are inside the platelets. Alpha granules are the most plentiful type of platelet granules 34 and are composed of both membrane-bound and soluble proteins that are freed into the extracellular space. Earlier research indicated that over 300 soluble proteins involved in various processes, such as inflammation, blood clotting, immune response, cell adhesion, and growth, and potentially other lesser-known functions are secreted by α-granules. 35 Delta forms (dense bodies) are the second common type of platelet granules. Delta granules are mainly made up of clotting-promoting molecules, such as calcium, magnesium, and adenosine, as well as bioactive amines (serotonin and histamine). Lambda granules are composed of enzymes that have a fundamental role in degrading proteins, lipids, and carbohydrates. In addition, they are responsible for cleaning up damaged tissue and eliminating infectious agents.36–38 Via activation (e.g., with Calcium chloride (CaCl2)), one of the main steps in PRP preparation, the granules present in platelets fuse to its cell membrane (named degranulation) where it releases GFs in high concentrations. 39 A broad range of target cells, including mesenchymal stem cells (MSCs), endothelial cells, fibroblasts, osteoblasts, and epidermal cells, are exposed due to the secretion of active proteins. 40 Over the recent years, there has been a significant interest in PRP therapy in the medical field due to its favorable benefit–risk ratio and good safety profile. This interest has arisen as a result of the therapy’s promising outcomes and lack of severe adverse effects.
Growth Factors in PRP and Their Biological Functions
ECGF, endothelial cell growth factor; EGF, epidermal growth factor; HGF, hepatocyte growth factor; IGF-1, insulin-like growth factor; PDGF, platelet-derived growth factor; PRP, platelet-rich plasma; TGF-β, transforming growth factor beta; VEGF, vascular endothelial growth factor.
Platelet-Rich Plasma Classification
Platelet-rich plasma (PRP) types are including: Pure Platelet-Rich Plasma (P-PRP), or leukocyte-poor platelet-rich plasma, is the most commonly applied in dermatology; Leukocyte- and Platelet-Rich Plasma (LPRP), primarily utilized for orthopedic issues and wound healing; Pure Platelet-Rich Fibrin (P-PRF), mainly applied in oral and maxillofacial surgeries; and leukocyte and Platelet-Rich Fibrin (L-PRF), which are effective for wound healing, periodontics, and sports medicine. 41 To categorize platelet concentrates (PCs) clearly, three main parameters are required. An initial set of parameters involves the centrifuge steps and preparation kits. In addition, there is the content of the concentrate, which is the second type of parameter and the third set of parameter is related to the fibrin network that supports the platelet and leukocyte concentrate during use. These data frequently appear to be empirically defined, and cross-examination of this technical information has not been fruitful. In addition, it is not possible to determine if experiments have been carried out using P-PRP or L-PRP. Nonetheless, P-PRPs appear to be the PCs that have undergone the most extensive testing in both in vitro and in vivo studies, even though conducting a thorough review of all the available literature is not practical. 42
PRP Preparation Methods
The preparation method significantly impacts PRP composition.43,44 Healthful individuals have 150,000–350,000 platelets/µL of whole blood, whereas PCs contain 1,000,000 plates/µL of platelet preparation. Various kits are available for PRP preparation, aiming to raise platelet concentrations three- to five-fold above baseline. 45 PRP preparation can be accomplished in a numerous techniques, but differential centrifugation is a common approach. 46 As a general rule, either plasma-based (PRP) or buffy-coated (BC) approaches can be used for its preparation (Fig. 1). 47 The two processes begin with white blood cells (WBCs) but differentiate in how the different components of the blood cells are isolated and concentrated during centrifugation. 48 It is possible to isolate plasma and platelet components from WBCs using plasma-based methods. The technique involves separating whole blood into platelets and red blood cells (RBCs) by a “soft spin,” followed by a “hard spin” to obtain plasma and platelet concentrates. After the removal of most plasma, platelets are maintained in a smaller volume of the remaining plasma. 49 Using the BC approach, whole blood undergoes a “hard spin” to separate plasma, RBCs, and buffy coats. It takes 1–2 h for the separated BC to rest, subsequently a “soft spin” is performed on the BC to produce PC. It takes less time to separate components using plasma than BC since a compulsory downtime of 1–2 h is required for the latter. It is important to note, however, that the BC method of component separation has some upsides over other methods, such as lower contamination with WBCs, and higher yield of plasma and platelets. The PRP approach of platelet preparation involves subjecting PRP to a “hard spin” that leads to the creation of aggregates that cause platelets to activate. On the contrary, a “hard spin” of the BC method causes platelets to be cushioned between RBCs instead. As a result, PRP generates less activated platelets than PRP.50,51 Basically, several factors can affect the yield of PRP, including how is blood drawn, time and temperature of centrifugation, and utilization of anticoagulants. 46
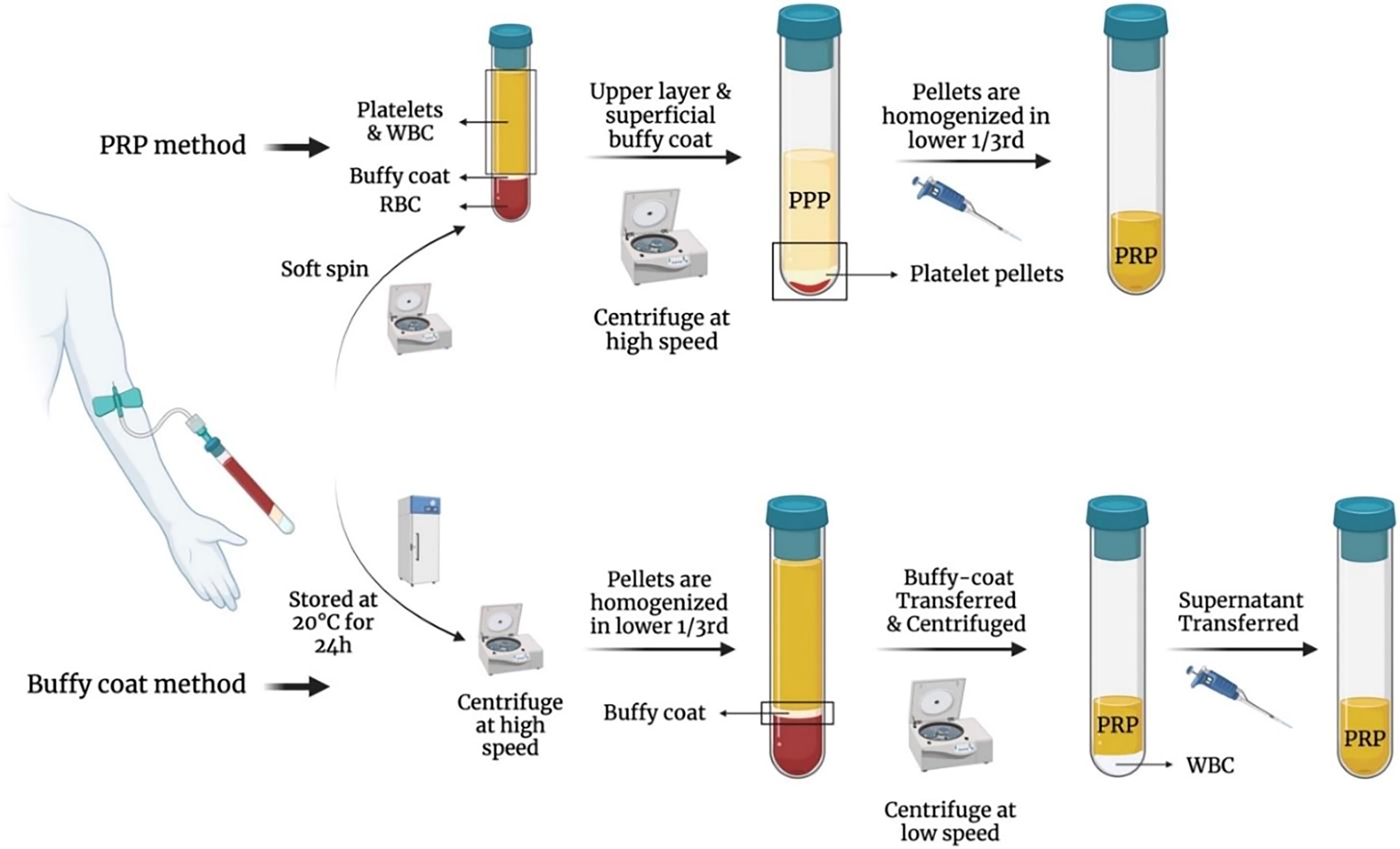
The steps of two common PRP preparation method. PRP, platelet-rich plasma.
PRP Applications in Regenerative Medicine
In the 1990s, regenerative medicine emerged as a new area of medicine dedicated to repairing damaged cells, tissues, and organs to restore their functionality.52–54 Although traditional medicine tends to focus primarily on replacing damaged tissues, this field aims to stimulate self-renewal in the injured site. 55 As mentioned before, emerging regenerative therapy approaches aim to harness and utilize the body’s own stem cells and autologous GFs. These GFs, which are polypeptide molecules, interact with receptors on target cells to convey signals related to cell movement, growth, specialization, longevity, and secretory functions. 55 Although TE uses natural GFs, there are certain clinical limitations, and GF-enriched bioformulations are difficult to create with precise, cost-effective methods; the use of these materials in biomedical applications is therefore hindered by this limitation. 56 It has been recognized that PRP-based GF delivery is an effective strategy to restart the tissue-repair cascade to restore soft and hard tissues damaged by trauma. 57 Using PRP has some advantages, for instance, obtaining the PRP from a patient’s blood is simple. A technique using autologous PRP was first presented by Ferrari et al. in 1987 for cardiac surgery. 58 In addition, PRP is considered safe and natural due to the fact that it uses your own cells without any further modifications. This also makes sure that the preparations do not trigger an immune response. 59 Second, by controlling the processing technique and activation protocol, it is feasible to regulate the dose of GFs released on activation. The use of PRP in oral and maxillofacial surgery has so far been shown to enhance the healing of both hard and soft tissues, and it is gaining popularity and attention among orthopedic and sports medicine practitioners for treating many different kinds of problems, such as bone, cartilage, ligaments, and tendons.60,61 Many clinical trials have evaluated PRP’s effectiveness in treating musculoskeletal injuries, including tendinopathies, osteoarthritis, and fractures. The findings suggest that PRP effectively alleviates pain and enhances functionality for individuals experiencing these conditions. 62 Also, PRP is used in the dermatology sector for procedures, such as facial rejuvenation, hair loss, scar revision, and wound healing. 63 As a result of its ability to induce type I collagen synthesis, human dermal fibroblast proliferation, and improve the texture of the skin, PRP is becoming increasingly popular for facial rejuvenation. Dermatologists use PRP to improve the treatment of chronic wounds that pose a serious health concern. Several millions of people around the world suffer from chronic wounds, which can result in infections and amputations if left untreated. Consequently, PRP has been utilized to enhance the healing of chronic wounds, such as diabetic foot ulcers and venous leg ulcers.10,64 It is crucial to highlight that there are still numerous challenges to tackle regarding the application of PRP in regenerative medicine, particularly concerning the efficient delivery of platelet-derived GFs to specific injury sites, which will be discussed further.
Delivery Systems for PRP-Derived GFs
In most cases, PRP therapy is administered using autologous blood drawn and centrifuged to separate the platelet concentrate from the blood. Once PRP has been activated (typically by CaCl2 and thrombin), it is injected, applied topically, or combined with surgical procedures at the defect/injury site. 65 However, there is concern that PRP’s clinical efficacy may be negatively affected by its inefficient and inconsistent delivery of GFs. Due to the quick release of GFs from PRP, their activity may severely diminish within a short period of time. 66 A GF delivery system used to regenerate or engineer tissues must take several considerations into account. Furthermore, it is crucial to choose a method of factor delivery that will target the desired cell population and minimize the propagation of signals to nontarget tissues and cells. Second, biological activity within the system must be maintained for a relatively long period of time. Third, the release profile of the GF needs to be careful in terms of time and location depending on the tissue injury or disease they are intended to treat. 67 Therefore, PRP can enhance healing and regeneration and increase bioavailability by combining it with a controlled-release carrier. 68 To meet the requirement for continuous GF release, scientists have utilized scaffolds as delivery mechanisms for PRP, which will be elaborated on below.
Scaffold-based delivery system
Regeneration of tissues is most commonly accomplished with the direct delivery of GFs at the site of action through a carrier vehicle (scaffold). In addition to maintaining the integrity of a damaged site, scaffolds can prevent PRP from migrating and allow sustained GF release. 69 The scaffolding environment may also enhance GFs’ bioactivity by facilitating their interaction, leading to different effects than those produced by free-form GFs. 70 Furthermore, bioactivation can be achieved by incorporating PRP and its derivatives into designed scaffolds. Consequently, it has been possible to design scaffolds with a proper multiscale hierarchical structure over the past decade, as well as delivery systems with the ability to deliver active proteins according to almost any complex pattern in the past decade. 71 An optimal scaffold for TE should function as a framework for three-dimensional tissue development by facilitating tissue infiltration, blood vessel formation, and the transport of nutrients via its interconnected porous structure. In addition, it would promote the differentiation, growth, and preservation of phenotype in the surrounding tissues by engaging with host tissues without creating scar tissue. 68 This has resulted in scaffold-based delivery systems that come in a variety of configurations, such as hydrogels and sponges, and that use different types of synthetic and natural biomaterials. 68 The use of nanoparticle delivery systems has also been reported in studies to deliver GFs spatiotemporally. 72 PRP is delivered locally to the regeneration sites with tissue-engineered scaffolds, covered sutures, or can dissolve in fibrin-like encapsulations in biomaterial-based systems. 73 Numerous biomaterials have been tested for the controlled delivery of GFs, and a huge number of experiments are being conducted to find the best method. 74 As a result, PRP delivered by scaffolds made of biomaterials has quickly gained popularity. 75 To improve the control of GF release profiles from scaffolds, several techniques have been developed. Many of these strategies focus on embedding GFs within biodegradable polymer networks, allowing for their gradual release into the wound as the scaffold decays. In the future, this process could be enhanced to maintain a therapeutic dose for a longer period compared with the existing fast-releasing scaffolds. PRP-derived GFs can be released in a kinetically controlled manner using hydrogels, sponges, and nanofibers. They are ideal for sustained release and improved bioavailability of GFs at the site of injury because of tailorable scaffold degradation, which impacts the release of included factors.76,77 As a result, the scaffold material can significantly impact factors such as degradation rate, which, in turn, can lead to variations in PRP component release profiles. In conclusion, it is important to note that the most frequently used biomaterials in clinical applications alongside PRP are natural options such as alginate, collagen, chitosan, and hyaluronic acid, as well as synthetic materials, such as poly(lactic-co-glycolic) acid, poly(caprolactone), and polyethylene glycol.78,79
PRP-Loaded Scaffold in Tissue Regeneration
Wound healing
Physical, mechanical, chemical, and pathogenic damages to tissues and organs of the body are protected by the skin. 80 The body responds to skin injuries by launching a number of subtle and complex mechanisms that enable it to rebuild its integrity and restore its normal operations. 81 Developing TE skin substitutes has been possible because of current advances in TE and regenerative medicine.82,83 So, multiple forms of scaffolds (particulate, printed, porous, and fibrous) have been developed for the treatment of skin wounds, and such scaffolds have been broadly employed as skin replacements.84–87 In spite of this, wound healing is a complex process that relies on a variety of materials to be effective. Biological base materials can recreate the ECM to fix skin damage, for instance, because vascularization is vital for wound healing. It is, however, impossible to induce enough blood vessels with a single substrate. 88 For this purpose, GF-releasing systems have been used to activate biological scaffolds with GFs before vascular growth. 17 The processes of wound healing can be improved through the use of GFs and cytokines. Specific roles of GFs in wound healing are mentioned in Figure 2. Innovations based on GFs are promising for optimal wound healing because they regulate cellular behavior during wound healing processes (hemostasis, inflammation, proliferation, and remodeling). 72 It is possible to rejuvenate the skin safely and effectively with PRP because it provides cytokines, GFs, and other biologically active substances associated with tissue regeneration and restoration. 89 Wound healing can be aided by GFs in PRP, such as EGF, PDGF, TGF-β, and VEGF.90,91 In addition, PRP can suppress inflammation by inhibiting cytokine release. This could improve tissue healing and regeneration, stimulate the growth of new capillaries in chronic wounds, and speed up the process of epithelization. PRP also contains a few leukocytes, which synthesize ILs as part of a nonspecific immune response, bolstering the host’s defense system at the wound site via signaling proteins that attract macrophages. Several gram-positive and gram-negative bacteria have been shown to be susceptible to PRP antimicrobial activity in previous studies. 92 Increasing matrix metalloproteinase (MMP) expression allows PRP to remodel the ECM and improve cellular proliferation and differentiation in the skin by degrading damaged ECM components. As a result of the increased secretion of hyaluronic acid, PRP makes the skin more elastic and turgid through hydration. 93 Although PRP poses a number of advantages, there are also potential drawbacks, such as a high risk of contamination during administration via injection, a low viability, and portability concerns. The GFs in PRP should ideally be released within 10 min. However, the majority are typically secreted over an hour. As a result, these GFs can become diluted and break down quickly once they enter the bloodstream after injection. 94 These obstacles limit the efficiency and effectiveness of platelet-based therapies. Therefore, recently, tissue-engineered constructs combined with biomaterials have been examined to develop synthetic and nonsynthetic platelet mimics to dominate these restrictions.90,95 This integrated system, which includes platelets and biomaterials, can be delivered through multiple methods, such as topical application, intracavitary injection, or intravascular delivery to directly engage with the site of bleeding and injured tissue. These systems gradually release various GFs obtained from PRP to facilitate wound healing in a regulated way. 96 A number of research have been conducted to verify the clinical benefits of PRP-based therapies, and the majority showed that wound size could be reduced significantly without side effects. Accordingly, in the study by Amaral et al., 97 collagen-glycosaminoglycan PRP-loaded scaffolds were used to evaluate the potential for wound healing within the skin. Research indicated that the composite scaffold emitted GFs that aid in wound healing (FGF, TGF-β) and promote vascularization (VEGF, PDGF) for a duration of up to 14 days following its implantation. Likewise, vascularization assays demonstrated increased wound healing potential by enhancing angiogenic and vascularization potential. Another study by Liu et al. 82 examined the wound healing effect of a cocoon scaffold loaded with PRP or platelet-poor plasma. It was found that both composite materials could facilitate wound healing in vivo, but the cocoon composites combined with PRP exhibited the most effective results and were most effective. Consistent with this, Xu et al. 88 applied granule-lyophilized platelet-rich fibrin (PRF) within a polyvinyl alcohol hydrogel to treat wounds in animals. Their immunohistochemical and histological analysis revealed that the scaffold improved collagen deposition, granulation tissue formation, and the development of new blood vessels. In addition, in vivo studies indicated that these scaffolds could serve as an optimal dressing for acute full-thickness skin wounds. Table 2 provides a summary of related research on PRP-loaded scaffolds in the context of skin wound healing.
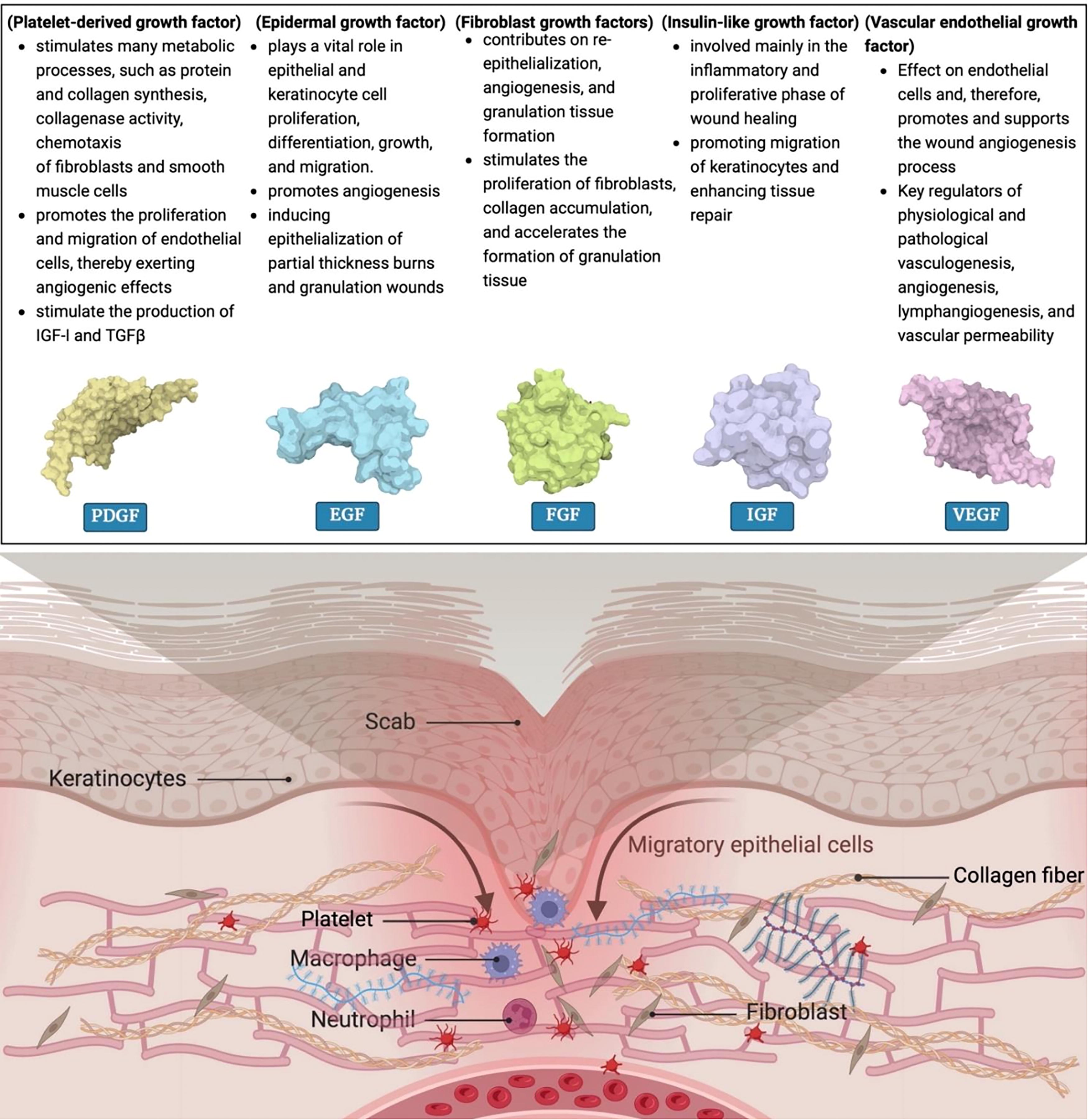
Functions of various GFs and their effect in wound healing. GF, growth factors.
PRP-Loaded Scaffolds in Skin Wound Healing Applications-Related Studies
GF, growth factor; PPP, platelet-poor plasma; PRF, platelet-rich fibrin; PVA, polyvinyl alcohol.
Bone regeneration
Interestingly, human bone has an inherent capacity for regeneration. Despite this, spontaneous healing is not possible for defects larger than a critical size. A bone’s healing process usually involves four stages that overlap each other: inflammation and vascularization, soft callus formation, hard callus formation, and bone remodeling. As such, the development and utilizing clinical translation of impressive bone regeneration modalities is helpful.114–116 In most cases of bone deformities, bone grafting is the most prevalent procedure. The definition of a bone graft is a material implanted into the body to encourage bone regeneration. 117 There are three major categories of bone grafts: autografts (a tissue or bone that comes from the patient), allografts (a tissue or bone from a human cadaver), and xenografts (a tissue or bone taken from an animal). 118 Other options include biomaterials derived from synthetics and biology, tissue-engineered materials, and combinations of these materials. 119 In the clinical setting, it is still quite common to utilize autografts and allografts for addressing substantial bone defects. However, these methods come with certain drawbacks. For example, although harvesting donor tissue for autografts, there is a risk of causing secondary injury, and with allografts, there exists the potential for pathogen transmission and immune rejection. 120 Recently, using novel biotechnology strategies and bone TE (BTE) might become an effective tool for the healing of bone defects as they are expected to overcome these shortcomings.118,121–124 Among the critical elements of BTE, scaffolds serve the purpose of being both a temporary substrate and a carrier of biochemical factors. In addition to providing anchorage sites, the scaffolds provide both appropriate physical stimulation (e.g., mechanical properties) and biochemical stimulation (such as cytokines and chemokines), thereby supporting cell growth and maintaining cell function.120,125 Hence, scaffolds as grafts in bone grafting are effective in eliminating problems caused by traditional treatment. Furthermore, it is more effective in treating various diseases that damage bones. 126 A good bone regeneration scaffold should possess several essential characteristics: (1) There are four main components to biocompatibility: osteoconductivity, bioactivity, and osteoinductivity: Boosting angiogenesis and supporting normal cellular activity without toxicity; (2) biodegradability or bioresorbability: It is generally preferable to create controlled spaces for new tissue to grow into and eventually replace mature bone tissue; (3) mechanical integrity: For the bone tissue to match that of the host; and (4) interconnected pore architecture: To improve nutrient transportation and waste disposal and to direct the growth of new tissues. Because a biomaterial-based scaffold alone does not possess the intrinsic osteogenic capacity, biomimetic and functional scaffold designs have been developed and combined with GFs or osteoinductive agents to overcome these limitations. 127 It is thought that GFs control the differentiation, proliferation, and synthetic functions of bone cells, influencing the healing of fractures and the process of bone remodeling. 128 Certain GFs play a role in both the creation and healing of bone (Fig. 3). Some of these factors encourage processes that specifically lead to bone formation, such as enhancing osteoinduction, whereas others, such as VEGF and PDGF, facilitate angiogenesis and the development of new blood vessels from preexisting ones.76,114 There are also osteoinductive GFs such as IGFs and TGFs-ß that have demonstrated great potential for regulating cell behavior in bone healing and osteogenesis, such as recruitment, migration, proliferation, adhesion, and differentiation.129,130 Regarding this, PRP-based therapy by delivery of GFs is a promising approach to facilitate new bone formation and can be utilized as an alternative bone graft substitute. In addition, the plasma component of PRP contains proteins, such as fibrinogen, albumin, and several immunoglobulins, which play a remarkable role in bone regeneration.131,132 Furthermore, some released cytokines by PRP also affect fracture repair such as IL-1, IL-6, and tumor necrosis factor-alpha (TNF-α). 133 Based on conducted studies, IL-1 and TNF-α both play a crucial role in recruiting osteoblasts to the fracture site.134,135 In addition, IL-6 has been shown to influence callus remodeling and mineralization that significantly improves later stages of bone healing. 136 To maximize the regenerative potential of PRP-derived factors, delivery vehicles capable of releasing them over an extended period are needed because bone regeneration is a lengthy process (adequate strength can be restored within 3–6 months). 114 To date, PRP’s use and delivery for bone regeneration have not been optimized, even though some efficacy has been demonstrated in vitro and in vivo scenarios. To overcome this limitation, several in vivo and clinical studies have evaluated the effects of PRP in combination with scaffolds as an alternative bone graft substitute. For example, Jiang et al. 137 investigated the effects of 3D-printed PRP-gelatin methacryloyl (GelMA) hydrogel scaffold on osteochondral regeneration in a rabbit model. Their findings showed that the prepared composite could accelerate osteochondral repair via immune regulation by M2 polarization and could be a potential selection for osteochondral tissue remodeling. Also, PRP-GelMA hydrogels coordinated and enhanced some overlapping osteochondral repair events, such as osteochondral differentiation, dynamic immune regulation, and chemotaxis of MSCs. In another recent study, Gan et al. 138 used a lyophilized platelet-rich fibrin (LPRFe) exudate-loaded carboxymethyl chitosan/GelMA hydrogel scaffold. In vitro tests indicated that the LPRFe-loaded hydrogel improves the adhesion, growth, movement, and bone-forming differentiation of rat bone MSCs. In addition, animal studies revealed that the hydrogel exhibited excellent biocompatibility and biodegradability, and the incorporation of LPRFe into the hydrogel can notably speed up the bone healing process, making it a potentially effective treatment for bone defects. As part of a study by Lee et al., 139 hydroxyapatite/collagen/PRP ceramic scaffolds were used for bone tissue regeneration. This research investigated the PRP release rate over an extended cultivation period (up to 35 days). The findings revealed that the sustained release of PRP had beneficial impacts on preosteoblast cells, enhancing both their proliferation and differentiation processes. Some other PRP-loaded scaffolds that have assayed in bone regeneration have been mentioned in Table 3.
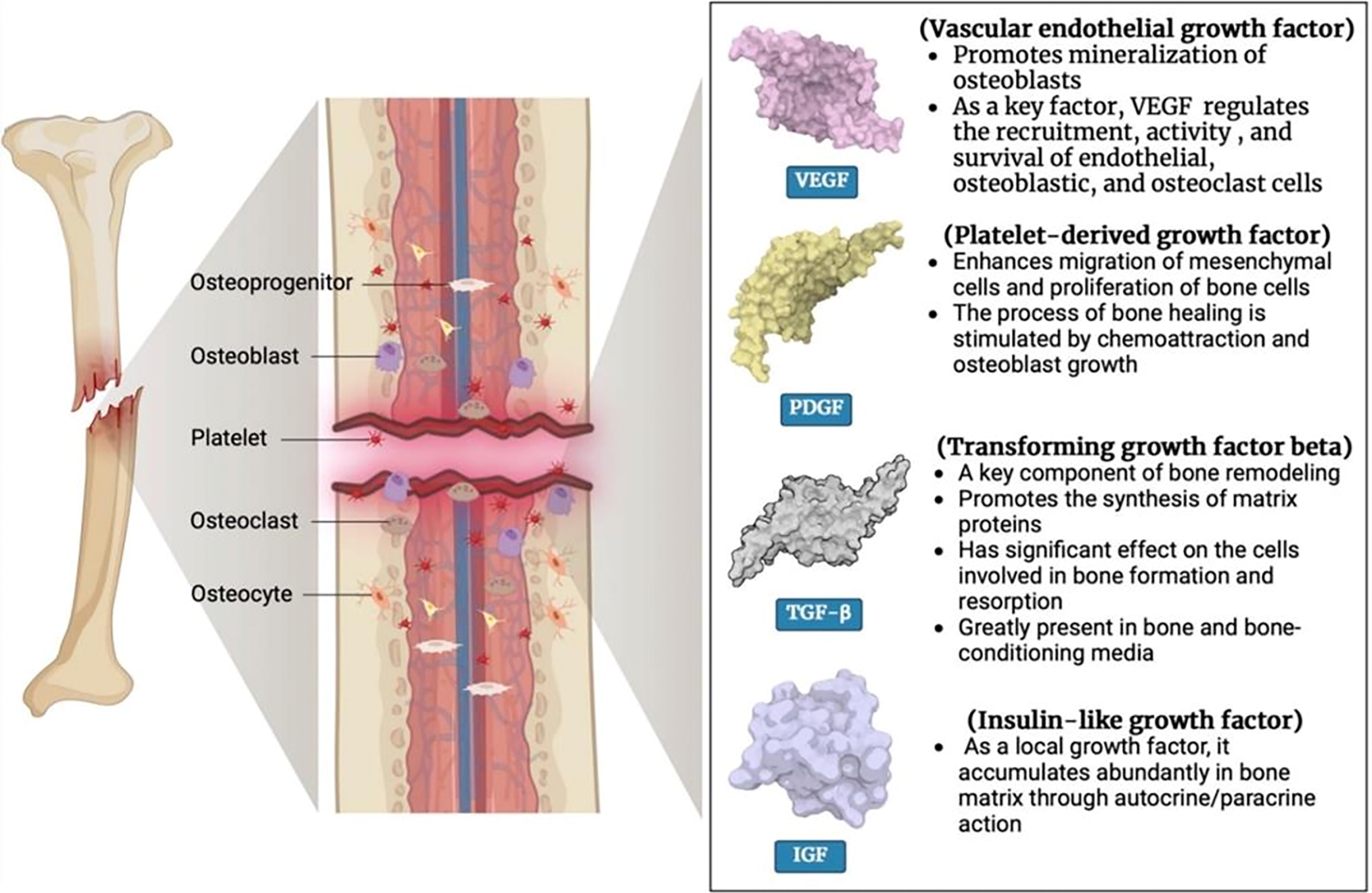
Roles of PRP components in bone regeneration.
Summary of Research That Used PRP-Loaded Scaffold in Bone Regeneration
Cartilage repair
Cartilage defects resulting from various causes such as illness or injury remain a significant challenge for surgeons due to the cartilage tissue’s limited ability to heal. 166 When the cartilage of the joint is damaged, the joint’s structure and function will be affected. A failure to treat it in time will result in joint pain and movement issues. In large defects, cartilage’s self-repair capacity is limited due to its low vascularity and restricted number of chondrocytes with weakened proliferation and migration. 167 Within the past decade, several techniques for treating cartilage defects have been developed. The use of cell-based therapies (autologous chondrocytes, matrix-induced autologous chondrocytes, bone marrow stem cells, adipose stem cells, microfracture, and cytokines) to repair cartilage can facilitate this process. Despite these efforts, it has not been possible to regenerate hyaline cartilage with similar morphology in these cases. 168 In recent years, TE has emerged as a promising approach for addressing cartilage defects.169,170 In the 1990s, advances in scaffold materials aligned with the progress made in GFs for cartilage TE. Scaffolds show promise as a feasible surgical solution for cartilage repair. As a result, the development of methods that combine scaffolds and GFs is still a burgeoning field of study at the moment. In general, in the field of cartilage regeneration, some GFs, such as IGF-I, bFGF, HGF, PDGF, and the TGF-β superfamily, are among the GFs whose research has recently received the most attention. In Figure 4, the commonly related GFs involved in cartilage repair and their function are illustrated. 171 Currently in research related to repairing cartilage, PRP is gaining recognition as a biological method for supplying elevated levels of GFs and cytokines to the location of injury. Furthermore, the fibrinogen present in platelet-rich plasma has the potential to become active and create a fibrin matrix fills in cartilage lesions and meets the necessary conditions for natural wound healing. PRP has been widely utilized in orthopedic injury-related diseases due to its ability to decrease inflammation, enhance angiogenesis, and stimulate the growth and specialization of cartilage cells, ultimately aiding in the healing process of bone and cartilage injuries. 170 Also, it has been found that cartilage healing via PRP therapy may reduce IL-1β-induced inhibition of type II collagen and aggrecan, as well as increase their protein levels. 172 In addition, studies have shown that PRP could decrease the raised level of nitric oxide, which induces chondrocyte apoptosis, increases the production of MMPs, and suppresses collagen synthesis, causing cartilage degradation.173–175 Furthermore, it may also restore self-renewal capacity and alter quiescence in aging cartilage by inducing chondrocyte autophagy, which could reinstate the regenerative process of cartilage. 176 PRP also includes various plasma proteins, which play essential roles in the repair process of connective tissues. 177 Although PRP has achieved success in treating articular cartilage injury, there is still debate surrounding its mechanism of action, effectiveness in clinical treatment, and preparation method due to its complicated composition. 178 So far in various studies, both forms of uninjectable (solid scaffolds) and injectable constructs containing PRP have been used, and their cartilage repair potency was investigated. 167 The scaffold utilized for cartilage TE must be made from materials that are both biocompatible and biodegradable, capable of offering sufficient mechanical stability throughout the regeneration process, and able to support articulate contact. Polymers and decellularized ECM are the top choices for scaffold preparation in cartilage TE. 179 The influence of platelet-derived GFs on chondrogenesis has been studied through both in vitro and in vivo models to understand their role in cartilage development. In a study, Lee et al. 180 evaluated the regenerative abilities of PRP when combined with a composite scaffold made of chondrocytes/hydrogel [gelatin-poly (ethylene glycol)-tyramine] in treating articular cartilage defects in a rabbit model. Their findings showed that using a PRP-containing hydrogel scaffold can improve the development and preservation of hyaline cartilage characteristics in articular cartilage defects when implanted. In addition, the results indicated that the continuous release of GFs from PRP in hydrogels improves the regeneration of hyaline chondrocytes and the formation of perichondrium-like normal joint cartilage by upregulation of CB1 and CB2. In a research conducted by Maria Sancho-Tello et al., 181 the advantages of using activated PRP along with a stabilized porous chitosan scaffold for cartilage regeneration were assessed. The activated PRP-loaded scaffold showed a significant increase in cell count compared with the stabilized porous chitosan scaffolds. Chondrocytes grown on the stable porous chitosan exhibited higher levels of type I collagen, whereas type II collagen was not observed. In contrast, cells cultured on activated PRP-loaded porous chitosan scaffolds showed high levels of type II collagen and low levels of type I collagen. To sum up, activated PRP boosts cell clustering and promotes the development of cartilage cells grown on stable porous chitosan scaffolds. Some other related studies are listed in Table 4.
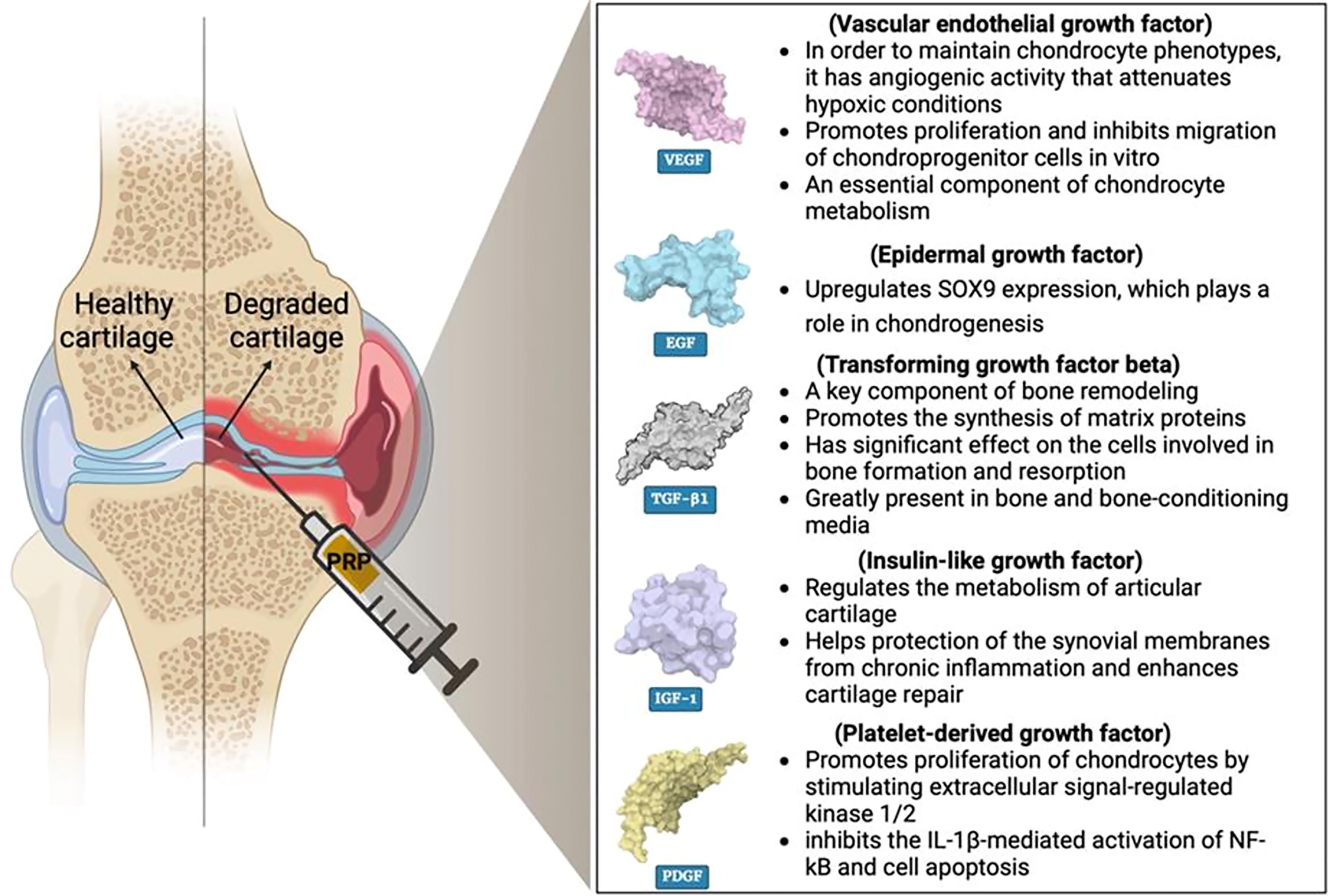
PRP-related GFs and their mechanism in cartilage repair.
Example of PRP-Loaded Scaffold Application in Cartilage Repair
ECM, extracellular matrix.
Future Prospect of PRP Therapy
Although considerable basic science research combined the effect of PRP and TE, wide variability in the preparation of platelets and lack of standard reporting makes it difficult to elucidate the efficacy of PRP in regenerative medicine; therefore, validated platelet preparation methodologies are essential for future clinical trials. Advances in the development of biomaterials have opened new avenues for the delivery of platelets. It should be considered that long-term storage and simple incorporation of PRP in TE scaffolds could significantly help clinical applications as on-site preparation of scaffolds adds cost and complexity. Although the prospects remain promising, robust and long-term clinical trials for using PRP in TE are essential to help translate these results to clinical practice.
Conclusions
Despite the promising potential of GFs in tissue regeneration, their utilization in clinical settings has been restricted due to their short biological half-life, fast degradation, high cost, and severe side effects under physiological conditions. Platelets store GFs and are essential for many important bodily functions, such as healing damaged tissue. Therefore, an alternative method for delivering concentrated GFs to the site of healing is through the utilization of PRP. The PRP is composed of plasma that has higher than normal levels of platelets, making it a promising option for regenerative medicine treatments for a range of conditions, such as musculoskeletal injuries and chronic wounds. PRP can be combined with a carrier to improve its effectiveness in healing and regenerating tissues, as well as enhancing the availability of GFs by utilizing a controlled release approach. The perfect release mechanism should enable the release of multiple factors and, most importantly, should be able to synchronize the timing of releasing factors derived from PRP with those needed for tissue regeneration. In terms of this issue, transport mechanisms utilizing biological and synthetic polymer scaffolds have proven effective in numerous medical uses. In this review, the application of PRP-loaded scaffold in soft and hard tissue regeneration, including skin, bone, and cartilage, was discussed in detail.
Footnotes
Authors’ Contribution
Conceptualization: N.K-N., R.K.O., and A.S.; Writing—original draft: N.K-N., B.T., and B.A.; Writing—review & editing: T.M., R.K O., and A.S.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.