
Abstract
Intervertebral disc (IVD) herniation is a leading cause of lower back pain, with symptoms ranging from tingling to disability. Discectomy, as the most common treatment, relieves pain and reduces inflammation, but the unrevealed defect in annulus fibrosus (AF) inevitably increases the risk of herniation as high as 21%. Repair and regeneration of AF are crucial to prevent herniation and recreate healthy IVD. Mechanical repair strategies, including suture, annulus closure device, and AF patch, often fall short in material-tissue integration and tissue regeneration. Recent developments in tissue engineering integrate biological science and material engineering, mainly through hybrid hydrogels and synthetic polymer scaffolds, showing promising effects on AF repair and regeneration. This review outlines various repair strategies and their limitations. It emphasizes the need for a holistic approach considering material selection, scaffold design, and incorporating cytokines or stem cells to improve AF repair outcomes. First, advancements in electrospinning, 3D printing, and porosity engineering will be discussed to enhance the integration of scaffolds with surrounding tissue to mimic a natural AF environment. Second, the benefits of adding cells or biofactors will be reviewed to strengthen cellular interactions, migration, and differentiation of stem cells. Finally, future research will be proposed to develop innovative, multifunctional scaffolds that complement personalized medicine while also considering the impact of mechanical stimulation and scaffold porosity on cell behavior and drug delivery for more efficient repair effects.
Impact Statement
The repair of the annulus fibrosus (AF) after discectomy is critical for preventing recurrent herniation. While tissue engineering (TE) scaffolds hold significant promise for AF reconstruction, there remains a paucity of comprehensive analyses addressing material selection, fabrication techniques, and diverse healing-promoting strategies. This review systematically synthesizes and evaluates the advantages and limitations of various TE approaches. Through in-depth elucidation of these emerging technologies, this study aims to advance AF repair strategies, facilitate their clinical translation, and ultimately contribute to the development of effective interventions for intervertebral disc degeneration and herniation recurrence.
Introduction
Low back pain (LBP) is a common and debilitating condition that affects millions of individuals worldwide; approximately 80% of people will experience LBP at some point in their lifetime. 1 Due to an aging population and extended working hours, the incidence of LBP and the associated medical expenditures have increased significantly, becoming a substantial socioeconomic burden.2,3 Intervertebral disc (IVD) herniation has been acknowledged as the leading cause of LBP. The IVD, composed of the highly hydrated nucleus pulposus (NP), the outer annulus fibrosus (AF), and cartilage endplates (EPs), functions to connect the upper and lower vertebrae, maintain disc height, and stabilize the spine.4,5 If AF has any injured or weakened area caused by prolonged uneven load, NP would potentially protrude outward from AF boundary and press against nerve roots, leading to painful IVD herniation.6-8 A damaged or compromised AF is recognized as a major contributor to LBP.9,10
Current clinical interventions for IVD herniation, such as discectomy, primarily focus on pain relief by removing the NP herniated portion. 11 While this approach can provide symptomatic relief, it fails to address the underlying issue of a compromised AF, which leaves patients prone to herniation and further disc degeneration.10,12B13 -16 Additionally, the avascular nature of AF and NP contributes to impaired tissue repair.17-19 The lack of vascularization could restrict oxygen, growth factors (GFs), and other nutrients and further decreases cell proliferation and function. Of note, vascularity might also regulate IVD repair directly.19,20 Due to limited healing capability, if left untreated, AF defect can result in post-surgery herniation and trigger a cascade of degenerative processes (Fig. 1), including NP dehydration, loss of disc structure, and chronic pain.11,21
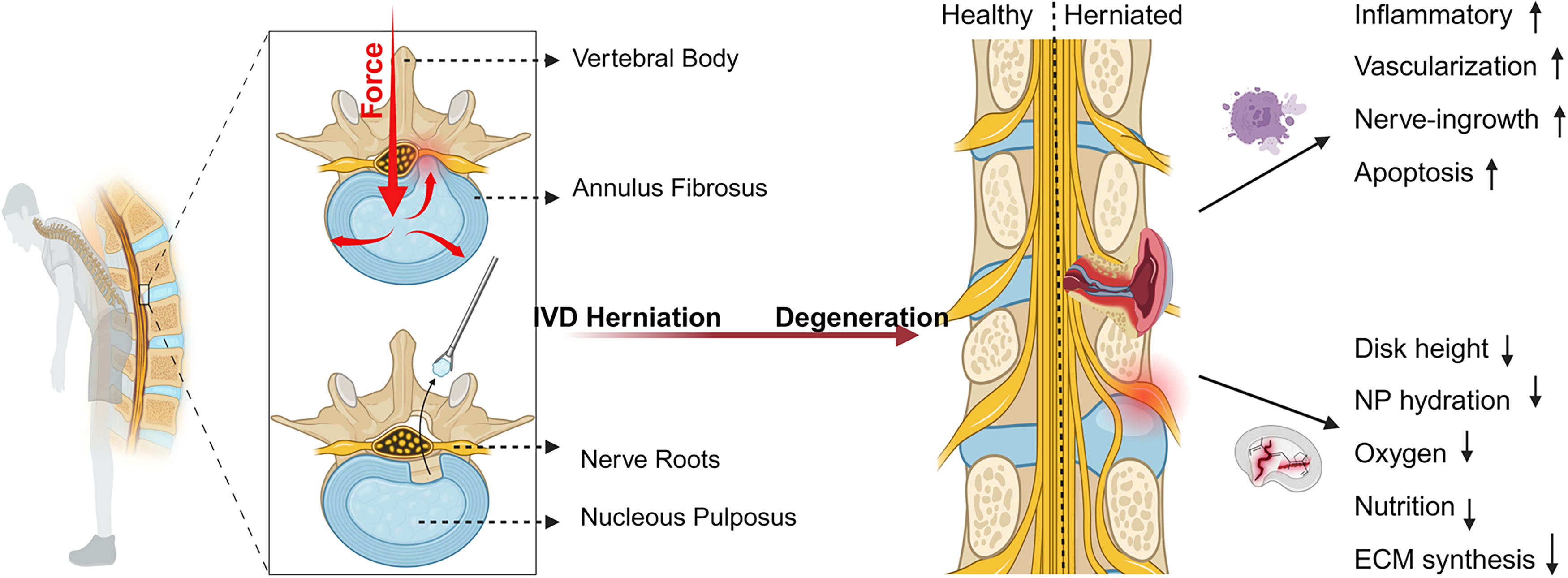
AF defect can result in post-surgery herniation and trigger a cascade of degenerative processes. AF, annulus fibrosus.
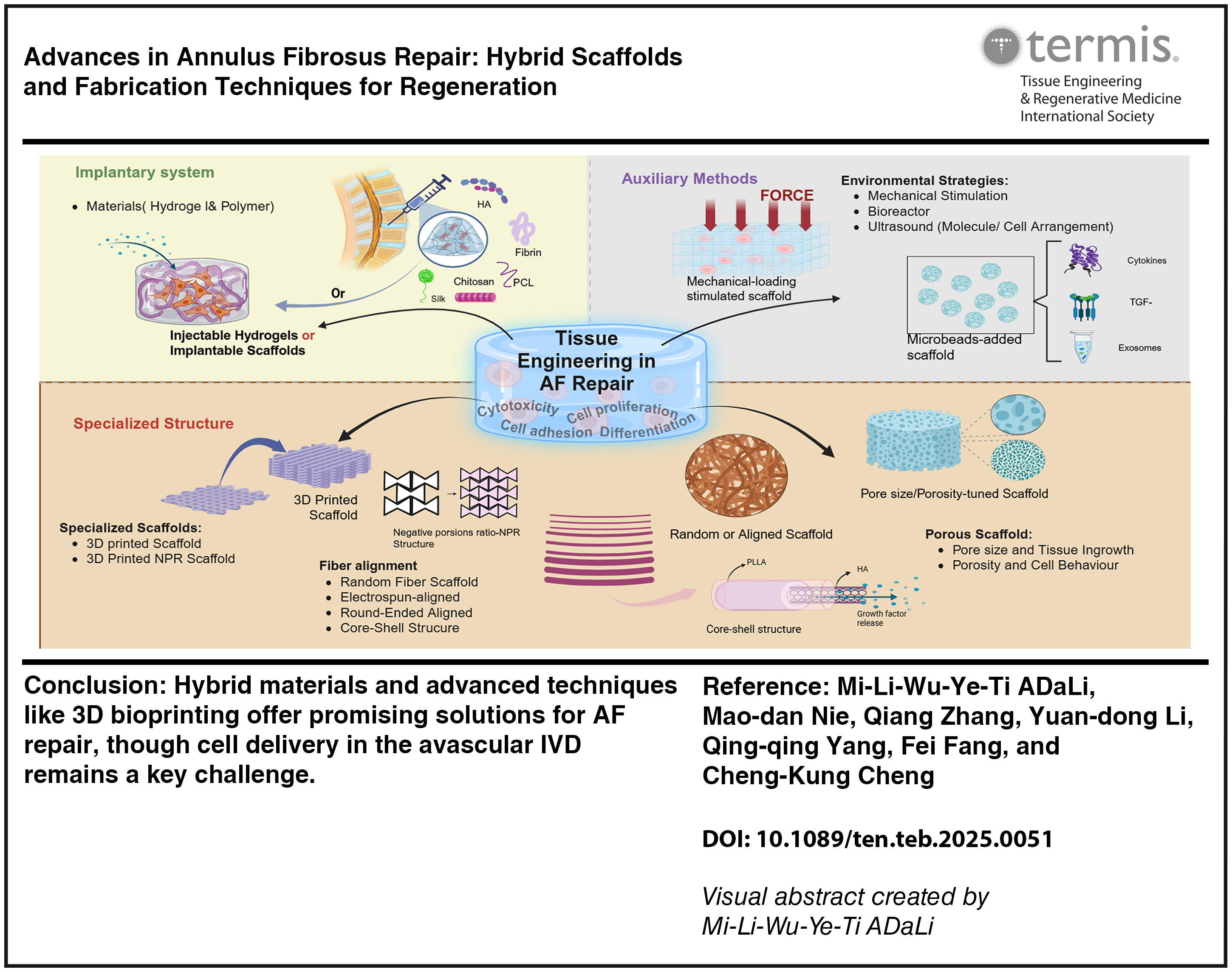
Various strategies have been explored to repair AF tissue, ranging from mechanical approaches such as suturing to biological interventions, including gene therapy, cellular therapy, and tissue engineering (TE).1,21 Among these, TE has emerged as a promising avenue, using biocompatible materials supplemented with cells or GFs to promote tissue regeneration. 17 Ideally, such TE strategies not only provide immediate structural reinforcement but also replicate the complex architecture and biomechanical properties of native AF, thereby promoting the formation of functional tissue that integrates seamlessly with surrounding structures. 22
This report systematically reviews TE strategies for AF repair, with a focus on scaffold material selection, fabrication techniques, mechanical loading, and incorporation of cells and GFs for enhancing healing. It also highlights future directions, including multifunctional scaffolds, bioprinting technologies, and personalized medicine, which would provide important guidance for advancing these technologies to translational application.
Methods
The literature review for this article was conducted using the Web of Science and PubMed to identify fully peer-reviewed research articles published between January 2012 and April 2024. The search strategy used a combination of key terms, including “annulus fibrosus,” “annulus fibrosus repair,” “electrospinning,” “3D printing,” “mechanical stimulation,” “tissue-engineered,” and “scaffold.” Studies were included if they focused on TE strategies specifically targeting AF repair using polymer-based or scaffold-sealed techniques, and only English-language articles were considered. The initial search yielded 1,157 articles. After the removal of duplicates and review articles, 461 unique studies remained. Following a thorough review of abstracts, 363 studies were excluded for not meeting the inclusion criteria, resulting in 94 full-text articles being selected for further analysis (Fig. 2).
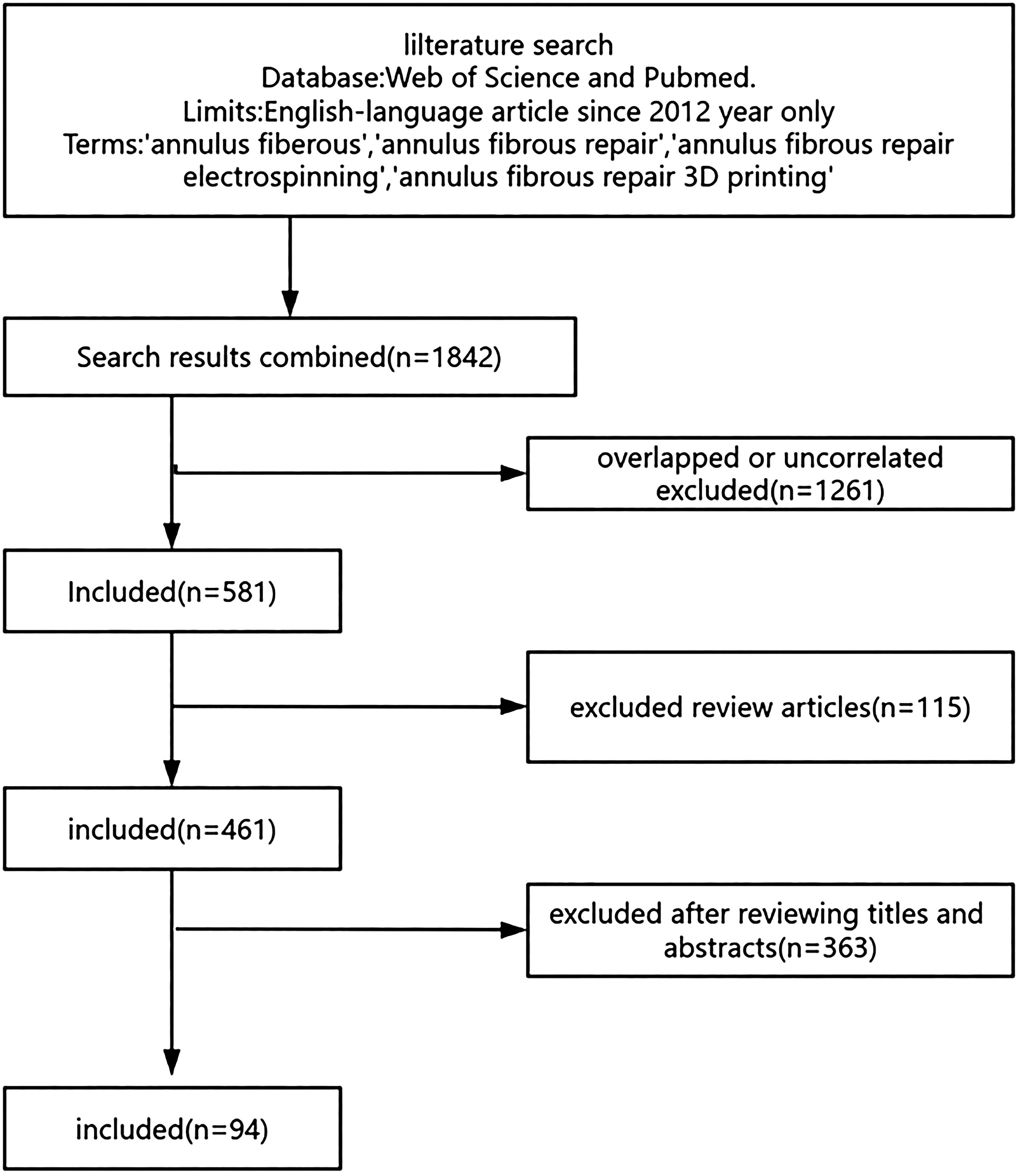
Flowchart depicting the literature search and selection process for studies investigating AF repair strategies.
The included studies were systematically categorized based on three interrelated parameters to enable structured comparison: (1) scaffold composition (distinguishing hydrogel-based from polymeric materials), (2) fabrication techniques (electrospinning, 3D bioprinting, or porosity engineering), and (3) integration of adjunctive strategies (e.g., GFs, bioactive molecules, cells, exosomes, or mechanical stimulation). Aricles were first grouped by material type, then subclassified by fabrication method, and finally stratified according to whether additional bioactive or mechanical enhancements were employed. This structured approach enabled consistent evaluation of technological and material variability while providing a systematic basis for summarizing current challenges and opportunities in AF repair scaffold development.
Discussion
Biological characteristics and challenges of AF repair
The AF is a critical component of the IVD, providing essential structural support and flexibility through its unique multilayered architecture. Composed of concentric collagen fiber lamellae arranged at alternating angles (30–45° in the inner region and 65° in the outer region), the AF features type II collagen in the inner layers and type I collagen in the outer layers.4,23-25 This complex arrangement allows AF to effectively absorb and distribute tensile, compressive, and shear forces, essential for spinal flexibility and stability.12,18,26 However, these characteristics also pose challenges for self-repair due to the low cellular turnover rate of AF cells and its avascular nature, which limits nutrient and oxygen diffusion.26B27 -29
AF injury triggers a cascade of biological responses that complicate repair. The extracellular matrix (ECM) rapidly degrades due to upregulated matrix metalloproteinases, weakening the AF structure and reducing its load-bearing capacity. 30 This is exacerbated by an inflammatory response involving cytokines (e.g., interleukin-1 and tumor necrosis factor-α) that further degrade the ECM and create a hostile microenvironment for tissue repair. 29 Subsequent fibrosis deposits disorganized ECM at the injury site, lacking the mechanical strength of native AF tissue. 31 This adverse microenvironment impedes cellular proliferation and promotes apoptosis, further limiting the AF’s healing capability. Therefore, AF injury often requires additional repair techniques to enhance repair effectiveness.
Mechanical strategies for AF repair
The complex biological and mechanical environment in and around the AF presents considerable challenges to effective repair. The complex biological and mechanical environment in and around the AF presents considerable challenges to effective repair, as diagrammed in Fig 3. However, these methods cannot completely address clinical problems. For instance, while suturing temporarily closes tissue cracks and reduces the likelihood of NP outflow, it is unsuitable for more significant defects caused by surgical procedures. This technique may also lead to secondary defects in AF surrounding patched pinholes and induce stress concentrations around the repair site. 31 Furthermore, mechanical suturing does not effectively replicate the native multilamellar architecture and mechanical characteristics of native AF and then compromises tissue biomechanical properties.32,33 Some clinical AF suturing surgeries after discectomy show that suture can effectively reduce the recurrence rate, slow the disc degeneration, and maintain the biomechanical strength of IVDs.34,35 However, it is also demonstrated in 10-year follow-up studies that even small needle punctures on AF can accelerate disc degeneration.36,37 Similarly, the annulus closure device (ACD) functions equally to sealants and is designed to fill the postsurgical gap on AF. A summarizing study on clinical results of ACD shows that the risks of reherniation and reoperation are approximately 50% lower in patients treated with discectomy and ACD compared with lumber discectomy only. 38 However, several studies demonstrated that ACD is prone to dislocation, loosening, and breakdown, potentially leading to herniation.38B39 -41 Patches with good sealing properties, low cost, and ease of fabrication show great potential in AF repair. 31 While no commercial products are certified yet, research on materials such as polycaprolactone (PCL), polyurethane (PU), and silk fibroin patches has demonstrated promising results in terms of mechanical strength and cell support for AF repair.42,43 However, patch technologies face challenges such as displacement after implantation. Additionally, AF patch fixation typically requires sutures, which complicate minimally invasive surgery. 44 More research is needed to improve the design of surgical tools and evaluate the long-term effectiveness of patch-based repairs for better clinical outcomes.
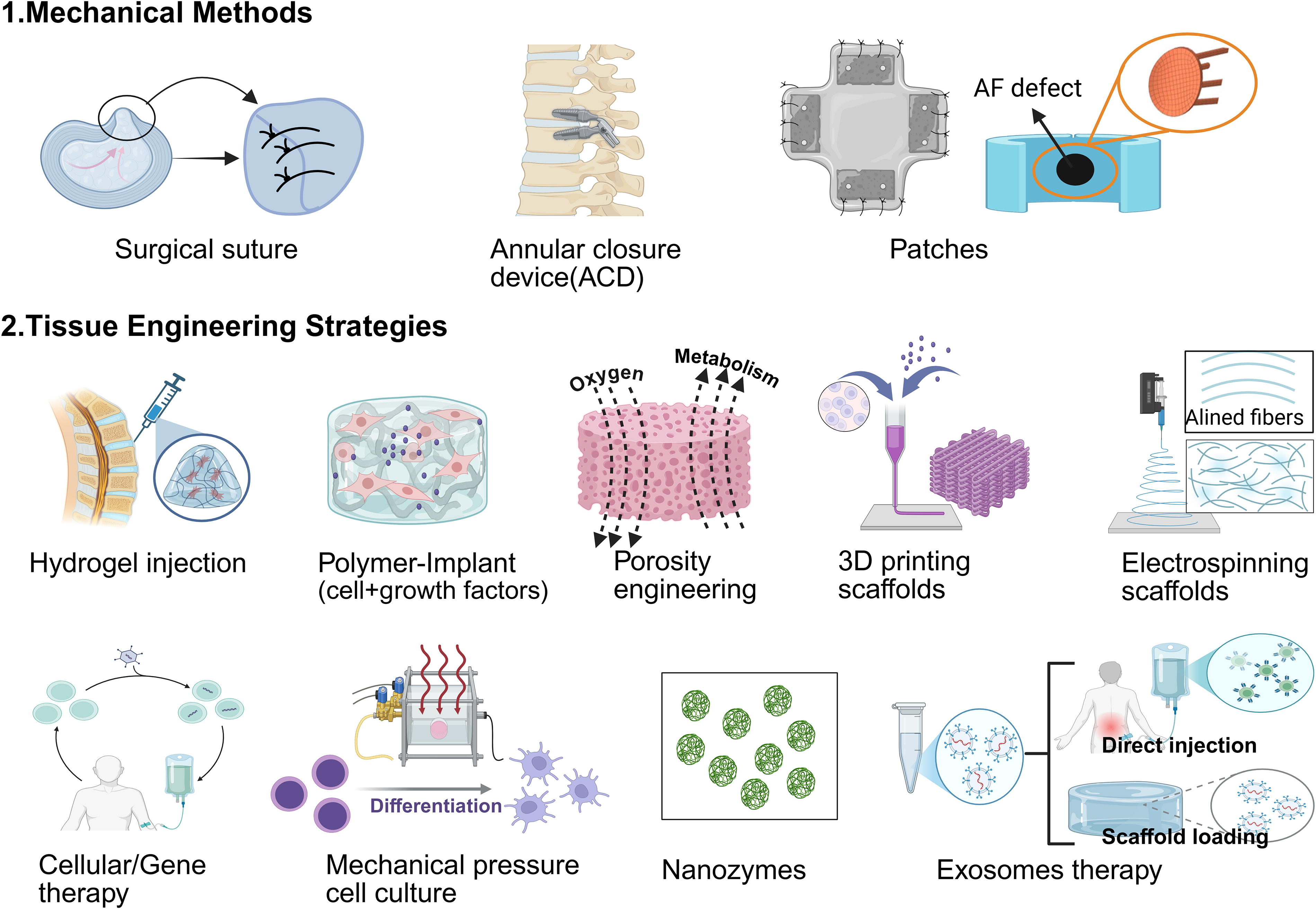
Illustrated classification of intervertebral disc repair techniques.
Therefore, existing mechanical repair techniques for AF provide short-term solutions and have obvious limitations, such as mechanical failure, incomplete tissue integration, and insufficient long-term durability. These limitations highlight the necessity for developing more advanced therapeutic strategies.
TE strategies for AF repair
TE represents a highly promising approach for AF repair, offering distinct advantages for AF repair compared with mechanical devices. Unlike mechanical devices provide immediate structural support, TE scaffolds offer mechanical strength to withstand spinal loads and promote tissue regeneration. 32 These scaffolds can be engineered to mimic the biomechanical properties of the native AF, supporting cell adhesion, proliferation, and differentiation through carefully designed materials and fabrication techniques, fostering functional tissue repair (Shown in Fig 3). This capacity to stimulate new tissue formation leads to more sustainable and biologically integrated repair, making TE a highly attractive strategy for AF repair.
Materials for scaffold preparation
The choice of material is crucial in developing tissue-engineered scaffolds for AF repair. Natural polymers, such as chitosan, hyaluronic acid (HA), collagen, silk protein, and decellularized ECM, typically display excellent cytocompatibility, biodegradability, and minimal cytotoxicity. However, their application is often limited by suboptimal mechanical properties and rapid degradation.45,46 Conversely, synthetic polymers, including PCL, polyglycolic acid (PGA), and poly(trimethylene carbonate) (PTMC), show superior mechanical strength and adjustable degradation profiles. However, it has relatively low biocompatibility, and it is not suitable for cell adhesion, proliferation, and differentiation. Optimization of these properties is critical for successful design of scaffolds for AF repair.
Hydrogel scaffolds are highly suitable for AF repair due to their flexibility, biocompatibility, and ability to replicate the hydrated, viscoelastic properties of native tissues, which are crucial for absorbing compressive loads and maintaining mobility. 47 These scaffolds can be engineered to exhibit mechanical properties similar to AF tissue by adjusting composition, crosslinking density, and water content.45,48 This tunability makes hydrogels particularly effective in balancing flexibility and stiffness, which is critical for AF repair.32,45 Additionally, hydrogels support cellular infiltration and tissue integration, contributing to better healing outcomes.
Various hydrogel formulations have been developed to address key challenges in AF repair (see Table 1). For example, fibrin, a degradable protein scaffold with over 30 years of clinical use, has shown promise49,50 but suffers from low mechanical stiffness and rapid degradation. To address these limitations, fibrin has been crosslinked with genipin to create FibGen, a hydrogel with low cytotoxicity and good adhesive properties. FibGen has been widely used as an injectable sealant for AF defects, demonstrating reduced chronic inflammation and promising biomechanical outcomes.42,51B52 -61 Other advanced hydrogels, such as PEGDA+FN-fibrin scaffolds 11 and HA-based composites (e.g., OHA-DA-PAM 48 ), have been developed to enhance integration with surrounding AF tissue and accelerate the repair process. However, their long-term efficacy and durability in vivo still require further investigation. The GelMA/HAMA composite hydrogel, incorporating transforming growth factor (TGF)-β3 and mesoporous silica nanoparticles, has been developed to mimic the biomechanical properties of the AF, possesses antioxidant and anti-inflammatory properties, and facilitates the recruitment of AF cells, enhancing ECM secretion 62 and accelerating the repair process. Bioadhesives have been explored for AF repair due to their strong adhesion and easy usage. 41 However, their temporary closure properties and lack of durability under load make them unsuitable for long-term AF repair. High-density collagen (HDC) scaffolds, with increased stiffness and hydraulic permeability, were compared with standard bioadhesives.51,63 Injectable riboflavin-crosslinked HDC gels have demonstrated the ability to “lock-in-position” with host tissue, reducing disc degeneration by securing the defect and preserving NP tissue.64-66 Although promising in rat models, further research is required to evaluate their effectiveness in larger animals or humans.
Hydrogel Scaffolds for AF Repair
AF, annulus fibrosus; GAG, glycosaminoglycan; HA, hyaluronic acid; IVD, intervertebral disc; TGF, transforming growth factor.
Synthetic polymers—including polycaprolactone (PCL), polylactic acid (PLA), poly(acrylic acid), poly(ethylene glycol) (PEG), and poly(trimethylene carbonate) (PTMC)—are extensively used in AF repair due to their advantageous mechanical properties, photopolymerization capabilities, and tunable degradation kinetics (summarized in Table 2). 67 These polymers provide essential structural support and stability under dynamic spinal loading, making them suitable for withstanding the complex mechanical demands of the IVD. Their versatility also allows for combinations with other materials to enhance AF regeneration. For example, PGA combined with HA promotes proteoglycan production, which is often reduced in degenerated IVDs. 68 PLLA nanofibrous scaffolds with an HA core 69 and PEGDA hydrogels incorporating dual-modified glycosaminoglycans (GAGs) have exhibited strong adhesion and sealing properties, reducing the risk of disc herniation 11 while promoting tissue growth and scaffold integration with surrounding AF tissue. Additionally, PEGDA combined with PLGA microsphere 70 has shown promise in improving scaffold integration with host tissues, reducing NP expulsion, and enhancing overall tissue regeneration. 71 PU membranes have been investigated as fixation patches for AF repair,42,72 stabilizing the scaffold and preventing migration. This is crucial for maintaining IVD integrity.72,73 However, ensuring long-term mechanical stability and addressing the limitations of traditional suture techniques in minimally invasive surgeries remain challenges.
Composite and Synthetic Polymer Scaffolds for AF Repair
AFSCs, AF-derived stem cells; DAFM, decellularized AF matrix; ECM, extracellular matrix; NP, nucleus pulposus; PCL, polycaprolactone; PTMC, poly(trimethylene carbonate); PU, polyurethane.
While synthetic polymers offer the necessary mechanical robustness for AF repair, they also present challenges related to biocompatibility and degradation behavior. 74 Their degradation rates must be carefully controlled to match the tissue regeneration process. Rapid degradation can compromise scaffold integrity before sufficient tissue regeneration occurs, whereas slow degradation may lead to a foreign body response or hinder tissue integration. 74 Additionally, some synthetic polymers produce acidic byproducts during degradation, which can cause localized inflammation and impair the healing process. To address these issues, various modification techniques, such as copolymerization, 75 surface functionalization, 76 and the incorporation of bioactive molecules, have been employed to enhance biocompatibility and reduce inflammatory responses. 77
Techniques for scaffold preparation
Advanced fabrication techniques, such as electrospinning and 3D printing, have been adopted to produce scaffolds with similar intricate architecture and mechanical behavior of native AF. These methods allow precise control over scaffold composition, creating multilayered, anisotropic structures that mimic AF’s mechanical properties. By replicating these properties, scaffolds effectively absorb compressive loads and maintain spinal mobility, which is critical for effective AF repair. This approach promotes functional repair and long-term integration with surrounding tissue, improving tissue regeneration and stability. Thus, advanced fabrication techniques are key to developing scaffolds that meet the mechanical and biological requirements for successful AF repair.
Electrospinning is a versatile technique widely used in fabricating scaffolds for musculoskeletal tissue repair, 78 particularly in AF repair. This method allows the creation of continuous fibers with controllable diameters, orientations, and mechanical properties to resemble native ECM architecture. 67 By adjusting the rotation speed of the collector during the electrospinning process, fiber alignment can be precisely controlled. 79 Aligned fibers have been shown to lengthen and orient AF cells compared with the random fibers, as well as enhance the differentiation of AF-derived stem cells (AFSCs) and promote the expression of AF-specific markers, such as aggrecan and collagen type-I, to further promoting the AF-cell proliferation and ECM generation compared with randomly oriented fibrous scaffolds.67,80-82 Electrospinning also allows the incorporation of natural and synthetic materials to improve scaffold biocompatibility and support AF healing. The PCL and PLLA polymers are the most commonly used materials in electrospinning. Electrospinning PCL scaffolds, for example, can mimic the native AF tissue by controlling the angular orientation of printed layers at ±30°. 83 PLLA fibers of varying diameters can induce the differentiation of AFSCs into distinct cell types corresponding to various AF zones. Electrospinning scaffolds made from materials such as poly(ether carbonate urethane)urea 84 and coaxial electrospinning scaffolds with decellularized AF matrix (DAFM) have demonstrated promise for supporting AFSC differentiation and collagen production. 85 Furthermore, combining natural polymers with synthetic materials as materials for electrospinning could enhance scaffold biocompatibility and provide additional support for AF healing, 86 such as oxygen-releasing core-shell fibers 87 and GF-loaded core-shell nanofibrous scaffolds. 88 Furthermore, electrospinning scaffolds can be engineered to include radiopaque nanoparticles, 89 which allow for in vivo imaging, aiding in surgical placement and postsurgical monitoring. 78 This integration of imaging capabilities adds an extra layer of utility to electrospinning scaffolds, ensuring better control and assessment during the healing process. However, electrospinning offers limited scaffold thickness and cell distribution.67,90
3D bioprinting has emerged as a powerful technology for TE, offering precise fabrication of patient-specific scaffolds with hierarchical architecture for AF repair and IVD regeneration. 83 For instance, re-entrant honeycomb structures have been designed to mimic AF tissue’s negative Poisson’s ratio (NPR) behavior, improving its ability to resist compressive forces and reduce NP herniation.91,92 Coating NPR scaffolds with polypyrrole has also enhanced cell adhesion and mechanical stability under spinal loading. 91 Moreover, 3D bioprinting can be combined with techniques such as electrospinning to create hybrid scaffolds. 93 For instance, the integration of electrospinning fibers with 3D-printed frameworks has led to the development of biomimetic IVD scaffolds that exhibit excellent mechanical strength and biocompatibility, with the electrospinning fibers replicating the aligned fiber structure of the AF. 93 3D bioprinting presents significant advantages in AF repair by enabling the creation of scaffolds with tailored mechanical properties, precise structural details, and enhanced biocompatibility. These capabilities make 3D bioprinting a promising platform for advancing regeneration, offering the potential for highly customized, functional, and durable tissue-engineered solutions.
Porosity engineering in scaffolds is another critical aspect of scaffold design for AF repair. Porous scaffolds enhance cell attachment and improve the repair’s mechanical stability by promoting interlocking with the surrounding tissue. 94 The pore size and porosity of scaffolds can influence cell proliferation, migration, orientation, and cellular interactions with the ECM. Smaller pores generally support fibroblast proliferation, whereas larger pores are more beneficial for bone regeneration, 95 making pore size an important consideration for optimizing AF defect and IVD regeneration. Furthermore, these factors impact the transport of oxygen and nutrients, which are essential for AF tissue repair. 96 Techniques such as solvent casting/particle leaching, gas foaming, and freeze-drying have been used to create scaffolds with controlled porosity.96B97 -99 For example, silk scaffolds created using solvent casting/particle leaching promote cell attachment and proliferation of AF cells, 99 with pores around 600 µm in size enhancing ECM accumulation and tissue formation under dynamic culture conditions. 100 Combining techniques such as electrospinning, 3D bioprinting, and freeze-drying could overcome individual limitations, creating hybrid scaffolds that improve AF repair and IVD regeneration.22,67,82,101
Auxiliary strategies for AF repair
Incorporating GFs and bioactive molecules further improves ECM production and tissue integration, which are essential for restoring mechanical properties of AF tissue. 102 These biomolecules regulate key biological processes, such as cell differentiation, promotion, and ECM synthesis, which are essential for effective tissue repair.48,56,62,71,73 GFs are particularly beneficial in AF regeneration due to their regenerative properties. For instance, TGF-β, especially TGF-β1 and TGF-β3, is widely used for AF repair as it modulates cell behavior and promotes ECM production. 103 Studies have demonstrated that TGF-β1 enhances ECM synthesis and tissue integration, whereas TGF-β3 accelerates tissue healing, exerts anti-inflammatory effects, and recruits cells to the injury site. 71 GFs can also serve as a reservoir for sustained drug release, maintaining AF tissue’s structural and functional stability over time.56,104 Incorporating anti-inflammatory agents, such as ibuprofen and TGF-β3, into electrospinning scaffolds further promotes tissue healing and regeneration in degenerated IVDs. 105 However, the short half-life of many biomolecules presents challenges in maintaining their effectiveness, necessitating the optimization of release kinetics. Additionally, including bioactive components such as oxygen-releasing agents can alleviate local hypoxia, improving cell viability and promoting tissue regeneration. 87
Cell therapy, mainly using MSCs or AF cells, has emerged as a key strategy to improve the efficacy of AF repair. MSCs, in particular, are favored for their ability to differentiate into AF-like cells, promote ECM synthesis, and contribute to tissue regeneration. 70 MSCs can help restore the structural and functional integrity of the AF, addressing the challenges posed by disc degeneration.72,106 In addition, when transplanted into the damaged area, AF cells can modulate the local environment, promote healing, and restore native tissue architecture. 64 However, the delivery and survival of these cells within the avascular environment of the IVD remain significant challenges. 107 Strategies to optimize cell survival, such as improving scaffold designs to enhance cell retention, increasing nutrient and oxygen availability, and promoting cellular differentiation, are critical to the success of these therapies.
Exosomes are a type of extracellular carriers that mediate intercellular communication. Exosomes have a variety of functions such as remaining cellular homeostasis, remodeling the ECM, and mediating cell–cell communication. TE strategies for IVD treatment and AF repair show that exosomes are small and convenient for carry various substances and have a lower immune response and higher transfection efficacy.108,109 The NP-derived and ECM-derived exosomes also have positive effects on AF cell proliferation, inhibit inflammatory cytokines expression, and promote tissue regeneration.110,111 Embed exosomes in suitable biomaterials can improve its active time, control its sustain release in AF microenvironment, and make it being a promising approach for AF repair and regeneration. 70 However, the extraction and production of exosomes still face technical difficulties for large-scale fabrication; there remains a lack of animal tests and clinical treatments.
The dysregulation of reactive oxygen species (ROS) affects the mitochondrial function in normal cells, which is a primary contributor of IVD degeneration. Nanozymes, as nanomaterials with enzyme-like activity, effectively decrease ROS levels to reverse tissue degeneration. 112 The nanozymes offer several advantages over natural enzymes, including compositional adjustability, physical stability, enhanced catalytic performance, and unique energy conversion capabilities. 113 Recently, lots of studies used varieties of nanozymes for the treatment of IVD degeneration, such as greigite nanozymes, 112 NAC-carbon dots nanozymes, 114 and Ce-Mn nanozymes, 113 and results demonstrated that nanozymes could alleviate inflammatory and IVD degeneration. 98 However, related research is still in its infancy, and further exploration is needed.
Mechanical loading plays a critical role in tissue regeneration, particularly in the development and regeneration of IVD. 115 Studies have demonstrated that dynamic mechanical loading enhances AF repair by promoting ECM synthesis and stem cell differentiation. 116 For instance, applying mechanical stress to AF defects treated with genipin-crosslinked hydrogels enhanced repair by improving stress transfer to the injured area in rats. 117 This loading also increases the production of sulfated GAGs and AF-related proteins (e.g., collagen-I and collagen-II) while activating pathways such as RhoA/ROCK1, which are critical for MSC differentiation. 118 Under strain, AF-specific genes such as Mohawk, SOX-9, and ECM markers are upregulated in human MSCs. 118
Similar findings are observed in ASCs and AF cells subjected to equiaxial strains.119,120 Additionally, tension-activated repair patches have been used in goat models to deliver anti-inflammatory factor anakinra to the AF defect, enhancing the therapeutic potential of mechanical loading strategies. 121 Despite ongoing research, the precise mechanisms of mechanical loading in AF repair remain unclear, highlighting the need for further studies to optimize these strategies for AF regeneration.
Challenges in the clinical application of AF repair scaffolds
The clinical translation of AF repair scaffolds faces several significant challenges related to material safety, fabrication reproducibility, and long-term stability. Synthetic polymer degradation may trigger inflammation. At the same time, natural materials such as collagen and HA offer better biocompatibility but suffer from inconsistent mechanical properties and uncontrolled degradation. Ensuring long-term stability without adverse immune responses is vital for clinical success. Fabrication techniques such as electrospinning and 3D printing must achieve precise control over structural parameters to replicate the complex AF architecture. However, scaling these methods for mass production while maintaining quality and meeting regulatory standards is a significant hurdle. Ideal materials, which simultaneously have structural stability properties, tuned degradability, nontoxicity, promotion of cell growth, and so on, are not yet established. Additionally, scaffolds must withstand the repetitive mechanical stresses in the IVD environment. While synthetic materials may degrade, hydrogels can struggle to maintain mechanical integrity, raising concerns about complications such as fibrosis or secondary disc herniation.
Conclusions and Perspectives
This review underscores recent advancements in AF repair. Hydrogels excel in mimicking the native AF’s mechanical characteristics but lack durability for long-term use. Synthetic polymers offer robust mechanical strength but need optimization for biocompatibility and degradation. Hybrid materials combining these properties offer a promising solution. Advanced techniques such as 3D bioprinting and electrospinning enhance scaffold design, promoting cell recruitment, and AF cell differentiation through tailored microenvironment. These methods allow for precise control of scaffold architecture, including fiber orientation and pore size, which can significantly influence tissue regeneration. Additionally, incorporating GFs and bioactive molecules further improves ECM production and tissue integration, which are essential for restoring the mechanical properties of the AF. However, delivering viable cells in the avascular IVD remains a key hurdle.
Future research should prioritize the development of multifunctional composite scaffolds that balance mechanical strength and biological responsiveness, supporting long-term tissue regeneration. Innovations will likely focus on combining hydrogels and synthetic polymers to enable dynamic adaptation and controlled release of bioactive molecules. Advanced manufacturing techniques, such as 3D printing and electrospinning, can create patient-specific scaffolds that replicate native fiber orientation and cell placement. Notably, these technologies meet clinical requirements for precision, controllability, and biocompatibility. Their ability to bridge the gap between laboratory benchmarks and clinical efficacy underscores their promise for developing better therapeutic regimens. Achieving long-term success in AF repair will also require addressing interactions between the AF, NP, and EPs, supporting coordinated regeneration. Given the clinical demand for biocompatibility and stable materials, biomedical engineering should focus on innovating new strategies or hybrid techniques. While early results are exciting and encouraging, accelerating translational pipelines through phased clinical trials will be critical to rigorously evaluate durability, safety, and efficacy. Additionally, collaboration between academic, industrial, and regulatory stakeholders will ensure that these innovations have a great impact on clinical application.
Footnotes
Acknowledgments
Mr. Colin McClean was acknowledged for his assistance with editing this article. The graphical abstract and Figure 1 are created in BioRender (Mi-Li-Wu-Ye-Ti ADaLi [2025] ![]() ).
).
Authors’ Contributions
M.-L.-W.-Y.-T.A. and M.-d.N.: Conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing. Q.Z., Y.-d.L. and Q.-q.Y.: Formal analysis and writing—review and editing. C.-K.C. and F.F.: Supervision, conceptualization, and writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the