
Abstract
The temporomandibular joint (TMJ) comprises the mandibular condyle, the articular surface of the temporal bone, and the articular disc. The articular cartilage in the TMJ is classified as fibrocartilage, which has distinct zones: the fibrous, proliferative, mature, and hypertrophic zones. TMJ osteoarthritis (TMJOA) is a prevalent condition affecting the TMJ, with its pathogenesis involving multiple factors such as trauma, occlusal instability, joint overload, and others. Current treatment options encompass noninvasive, minimally invasive, and surgical interventions. However, no definitive cure has been found. Tissue engineering offers a novel approach to treating TMJOA by promoting cartilage repair and regeneration by constructing artificial cartilage grafts made from a combination of cells, bioactive factors (BFs), and biodegradable scaffolds. Among the scaffolds commonly used in research are hydrogels, nanoparticles, and three-dimensional-printed structures, with mesenchymal stem cells serving as the primary cell source. Additionally, exosomes and gene therapy have shown promise in TMJOA treatment. Despite significant progress, optimizing the integration of seed cells, BFs, and scaffold materials remains a critical focus for future research. This article provides an in-depth review of the latest advancements in TMJ condylar cartilage tissue engineering.
Impact Statement
This review comprehensively overviews tissue engineering advancements for temporomandibular joint condylar cartilage regeneration. It highlights key progress in scaffolds, cell-based therapies, bioactive factors, and gene therapies. The review offers valuable insights for future research and potential clinical applications, contributing significantly to developing novel therapeutic strategies for temporomandibular joint osteoarthritis.
Overview of Temporomandibular Joint Osteoarthritis
The temporomandibular joint (TMJ) is a synovial joint composed of the mandibular condyle, the articular surfaces of the temporal bone, and the articular disc. The articular cartilage of the TMJ is made up of fibrocartilage, which covers the surface of the mandibular condyle. It can be categorized into four distinct zones: the fibrous, proliferative, mature, and hypertrophic zones. 1 The fibrous zone consists of flattened fibroblasts and type I collagen. The proliferative zone contains mesenchymal stem cells (MSCs), which are precursors to chondrocytes. The mature and hypertrophic ones are characterized by loosely organized type II collagen and mature chondrocytes. Proteoglycans are mainly located in the mature and hypertrophic zones, with relatively low levels in the fibrous ones. The collagen fiber network and proteoglycans work together to enable the mandibular condyle to perform its load-bearing functions2,3 (Fig. 1).
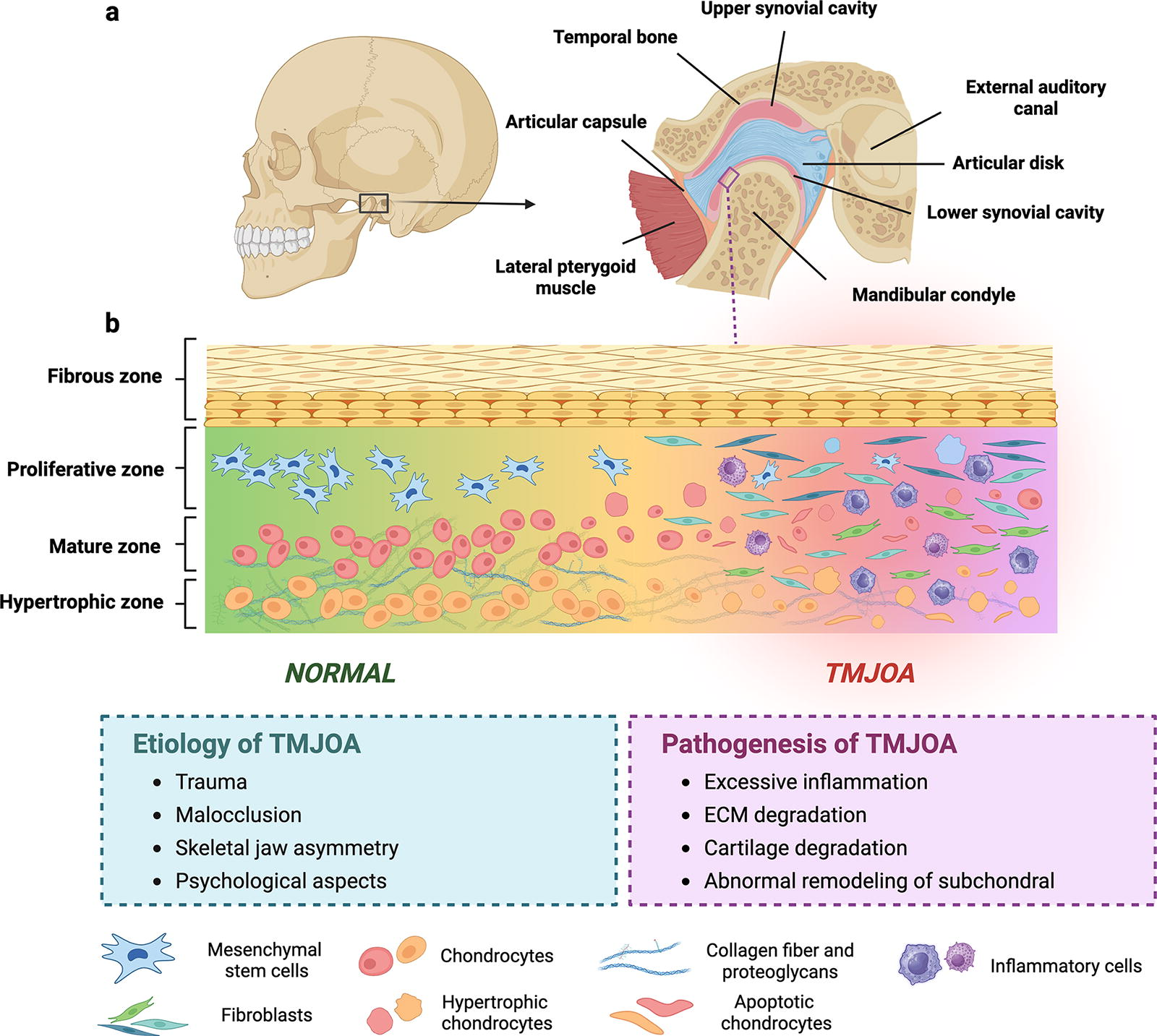
Osteoarthritis (OA) is a prevalent degenerative and inflammatory disorder affecting the TMJ, with a global prevalence of 8–16%.4,5 It is associated with various factors, including trauma, unstable occlusion, excessive joint loading, systemic diseases, aging, and hormonal changes. These factors can individually or synergistically trigger TMJ degeneration, resulting in symptoms such as facial pain, restricted mouth opening, joint clicking, and crepitus, which impair normal functions such as swallowing and communication.
TMJ osteoarthritis (TMJOA) primarily involves chondrocyte-mediated degeneration of the articular fibrocartilage, decreasing in extracellular matrix (ECM) components such as collagen and proteoglycans. This disrupts the joint’s biomechanical properties and hinders its capacity for self-repair due to a limited blood supply and metabolic activity within the cartilage. If left untreated, cartilage damage can progress to severe OA6-8 (Fig. 1). Treatment options for TMJOA are noninvasive (e.g., occlusal splints, nonsteroidal anti-inflammatory drugs [NSAIDs], orthodontic devices, and physical therapy), minimally invasive (e.g., arthrocentesis, arthroscopy, and intra-articular injection), and surgical interventions (e.g., arthroplasty, reconstruction, and TMJ replacement).9B10 -15 Noninvasive methods are typically employed for mild cases, while surgical options may be considered for severe structural damage and intractable pain. However, no definitive cure currently exists, and ongoing research aims to identify effective therapies to slow or reverse the progression of TMJOA.
The Modeling of TMJOA
The modeling of TMJOA is essential for investigating the pathophysiological mechanisms underlying the condition and evaluating the effectiveness of novel therapeutic approaches. Although various animal models have been developed, no universally accepted gold standard model exists. These models can be broadly categorized into several types: spontaneous, chemically induced, surgical, mechanically stimulated, and gene-edited models. Each methodology offers unique insights into the disease process and therapeutic potentials, thus contributing significantly to our understanding of TMJOA.4,16B17 -20 Kitami et al. have established a natural TMJOA model using aged mice to simulate the high prevalence of the disease in the elderly population. 21 Chemically induced methods, such as those using complete Freund’s adjuvant, monosodium iodoacetate (MIA), vascular endothelial growth factor (VEGF), or collagenase, have been widely adopted in rats to construct TMJOA models due to their predictability and reproducibility. However, these methods typically replicate only specific symptoms of TMJOA.22B23 -25 Mechanical stimulation paradigms, such as unilateral anterior crossbite, have been shown to induce TMJOA lesions through mechanical stress. Notably, following lesion induction, the removal of the metal tubes allows for research in the natural recovery process of TMJOA.26,27 Another widely utilized method is anterior disc displacement surgery, which is performed by drilling a hole anterior to the zygomatic arch junction and securing the anterior band of the articular disc. 28 Several researchers employ a unilateral anterior large overjet dental appliance to induce Class II malocclusion and TMJOA-like features. 16 Despite these advancements, chemically induced methods remain the most widely favored for establishing TMJOA models.29,30 Gene-edited models, such as those involving short stature homeobox 2, transforming growth factor-beta 1 (TGF-β1), or beta-catenin (β-catenin) overexpression, or the inhibition/knockout of discoidin domain receptor 1 (DDR1), fermitin family homolog 2 (Kindlin-2), adrenoceptor beta 2 (Adrb2), brain and muscle ARNT-like protein 1 (Bmal1), and fibroblast growth factor receptor 3 (FGFR3), vitamin D receptor, can also precipitate TMJOA31B32 -37 (Fig. 2). Collectively, these models provide indispensable tools for elucidating the pathogenesis of TMJOA and evaluating novel therapeutic interventions.
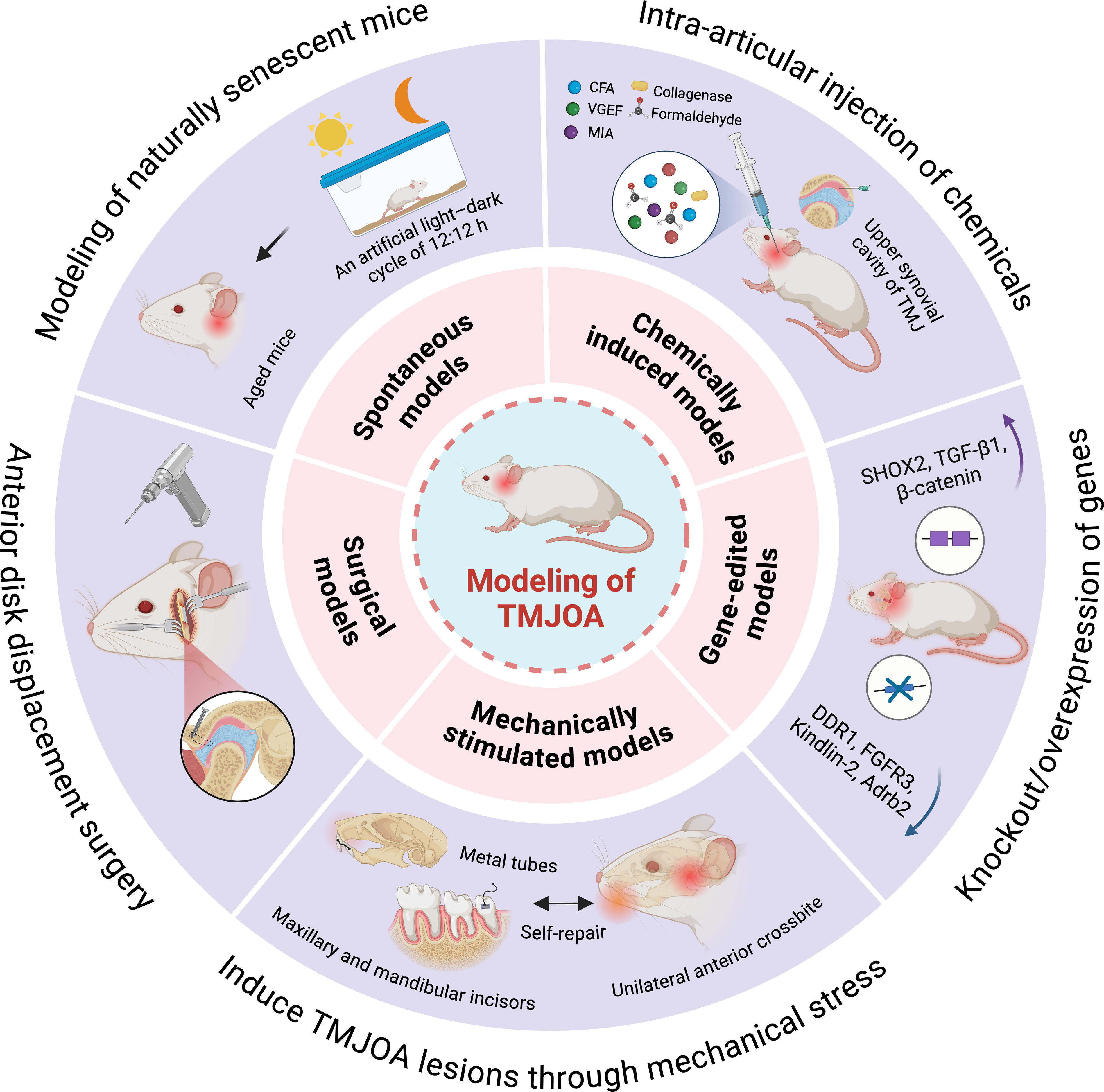
Temporomandibular joint osteoarthritis model.
Cartilage Tissue Engineering Therapy
Cartilage tissue engineering has garnered increasing attention with advances in biomaterials and regenerative medicine. The core of this approach is to select specific cells as seed cells, which are combined with bioactive factors (BFs) and then planted on biodegradable scaffolds. Meanwhile, drugs and gene therapy have also made significant progress in this field38,39 (Fig. 3). This process constructs artificial cartilage grafts that can be implanted into cartilage defect sites, thereby facilitating the repair and regeneration of cartilage tissue.
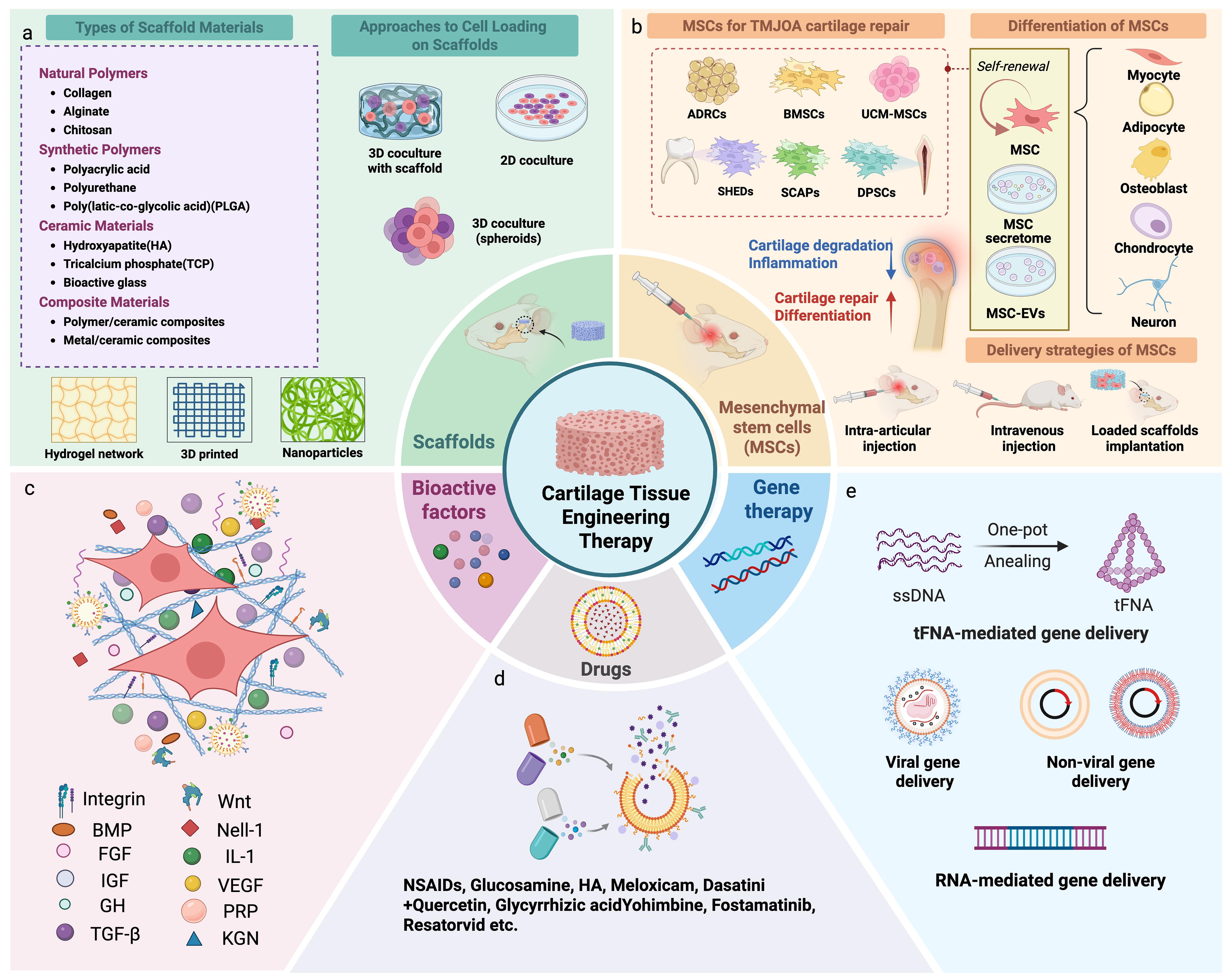
The key factors in tissue engineering for the repair of TMJ cartilage therapy.
Scaffolds for tissue engineering
In recent years, substantial progress has been witnessed in TMJ cartilage regeneration, driven by innovations in nanomaterials, advanced hydrogels, and three-dimensional (3D) printing techniques. Current scaffolding materials used in cartilage tissue engineering mainly fall into natural and synthetic categories. Natural materials, such as collagen, hyaluronic acid, and chitosan, are biocompatible and biodegradable. They can mimic the natural microenvironment of cartilage cells, promoting cell adhesion, proliferation, and differentiation. 40 For example, collagen scaffolds, resembling the ECM of cartilage cells, can effectively support cell growth and induce cartilage matrix synthesis. On the contrary, synthetic materials, including polylactic acid, polyglycolic acid, and their copolymers, offer adjustable mechanical properties and degradation rates based on molecular weight and copolymer ratios.41,42 This flexibility can be tailored to meet the requirements of different cartilage repair sites. For instance, polylactic-coglycolic acid scaffolds provide stable growth conditions for cartilage cells and gradually degrade as new cartilage tissue forms. Composite materials, such as those combining nanoparticles with polymers, are also gaining attention for their enhanced mechanical and biological performance.43,44 The selection and design of these scaffolding materials should consider the physiological characteristics of cartilage tissue, the mechanical demands of the repair site, and the biological behavior of cells to ensure optimal outcomes in cartilage regeneration.
Hydrogels
Hydrogels have emerged as promising biomaterials for TMJ cartilage repair. Hydrogels provide a versatile microenvironment that supports complex cell-matrix and cell–cell interactions, enabling precise spatiotemporal regulation. Cells can either be cultured on the hydrogel surface for 2D expansion or encapsulated within the matrix for 3D growth. To enhance the attachment, proliferation, differentiation, and secretion of MSCs, hydrogels are often functionalized with integrin-binding peptides, degradable sequences, nanoparticles, chemokines, or growth factors. 45 In clinical practice, intra-articular injection of high-molecular hyaluronic acid (HA) is commonly used to improve joint function and alleviate pain in TMJOA, positively affecting articular cartilage regeneration.46B47 -49 Additionally, various composite hydrogel materials have been developed for TMJ cartilage regeneration, including cell-mediated bilayer hydrogel-biphasic calcium phosphate (BCP) scaffold, TGI/HA hydrogel, Gel-MA-MSC microspheres, Hst1/Gel-MA hydrogel, HA-based microparticles, and RDGel50B51 -54 (Table 1, Fig. 4). These hydrogels possess good biocompatibility and injectability, and they can promote cartilage repair through multiple mechanisms such as immunomodulation, anti-inflammation, antioxidation, and cell protection. However, despite the promising repair effects demonstrated in experiments, their clinical application still faces challenges. First, hydrogels’ biodegradability and long-term stability require further validation to ensure their safety and effectiveness in the body. Second, the mechanical properties and drug release characteristics need to be optimized according to specific clinical needs for optimal therapeutic effect. In addition, improvements in the preparation process and cost-effectiveness are necessary to enhance their feasibility in clinical applications. Future research directions include developing new types of hydrogel materials, exploring their application effects in different TMJ diseases, and further investigation into their mechanisms of action. A multimodal treatment approach, combining gene therapy, cell therapy, and drug therapy, is expected to enhance the efficacy of hydrogels in TMJ cartilage regeneration. The integration of new technologies, such as microfluidic technology, organ-on-a-chip, and decellularized hydrogels, has further enhanced hydrogels’ performance and application potential. Microfluidic technology can precisely regulate the cellular microenvironment, organ-on-a-chip can simulate physiological and pathological processes, and decellularized hydrogels provide natural BFs.55,56 By combining these technologies, it is possible to achieve precise nutrient supply, cell behavior regulation, and tissue regeneration, along with advantages such as injectability, good biocompatibility, and ease of operation, and it is expected to improve the efficacy of TMJ cartilage repair significantly. Moreover, conducting clinical trials will be crucial to validate the practical application of these hydrogel materials and provide more effective solutions for treating TMJ diseases.
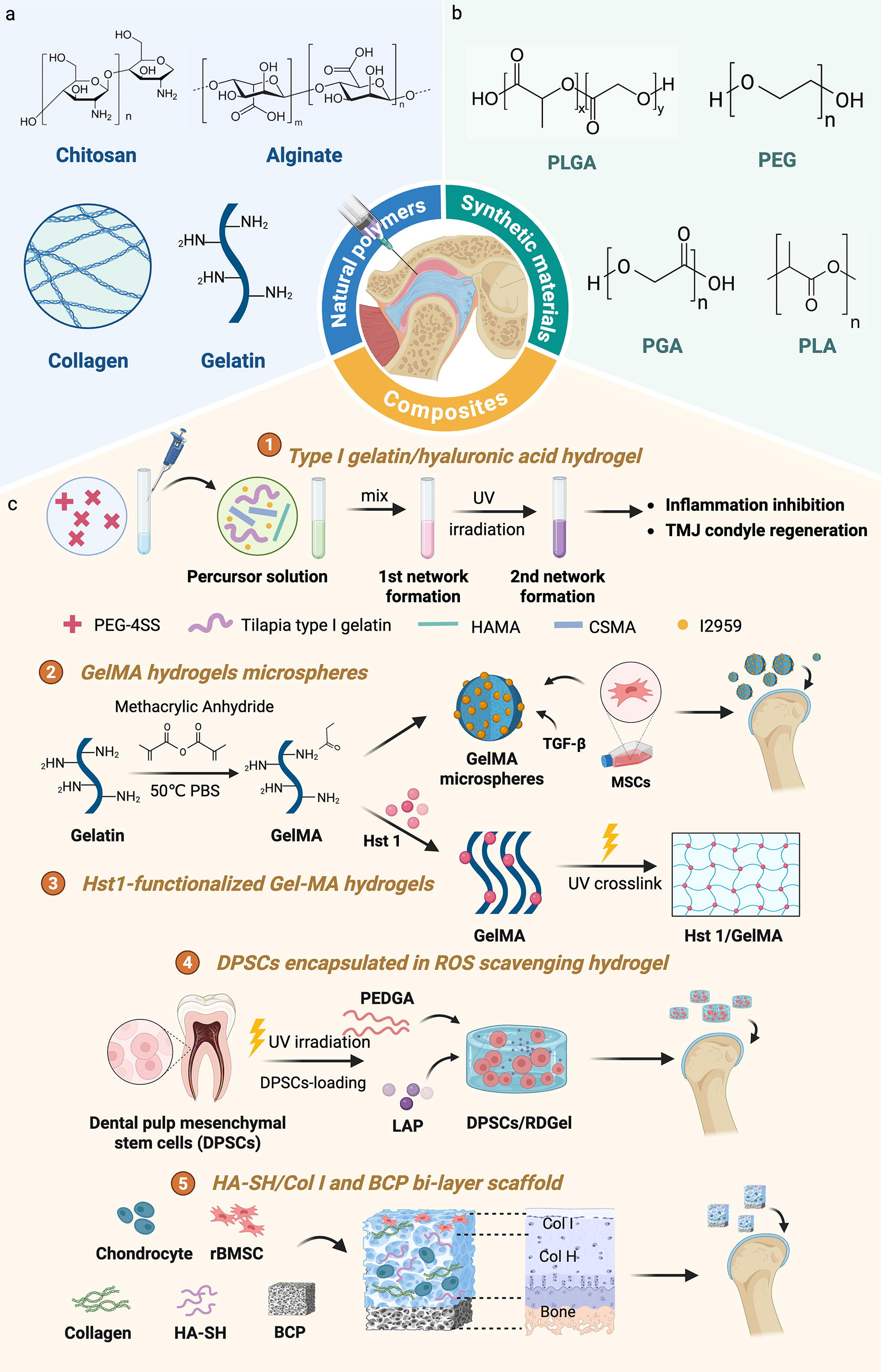
Schematic representation of various hydrogels used in TMJOA treatment.
Reported Composite Hydrogel Scaffolds
Nanomaterials
Recently, nanomaterials have demonstrated significant potential in TMJ cartilage regeneration due to their unique physicochemical properties and excellent biocompatibility.41,57 This review summarizes the application of nanomaterials in TMJ cartilage regeneration, including cerium oxide nanoparticles, Pt@PCN222-Mn cascade nanozymes, poly(p-coumaric acid) nanoparticles, γ-Fe2O3@TA@ALN magnetic nanoparticles, and self-assembled nanospheres58B59 -62 (Table 2, Fig. 5). These materials promote cartilage regeneration through various mechanisms, such as antioxidant, anti-inflammatory, and antiapoptotic effects, providing lubrication and reducing wear. However, they also face several challenges that need to be addressed, including uncertainties regarding long-term stability, in vivo metabolism, and potential immune responses. Additionally, the biosafety of nanomaterials, the potential toxicity of their degradation products, and the feasibility of clinical applications require further investigation. Future research directions should focus on the following aspects. For starters, the development of nanomaterials with longer-lasting effects reduces the frequency of repeated injections. On top of that, in-depth studies on the in vivo metabolic processes of nanomaterials to ensure their long-term safety. Besides, the exploration of combining nanomaterials with other therapeutic strategies (such as gene therapy and cell therapy) promotes cartilage regeneration. Through these efforts, nanomaterials are expected to become a highly effective therapeutic approach for TMJ cartilage regeneration.
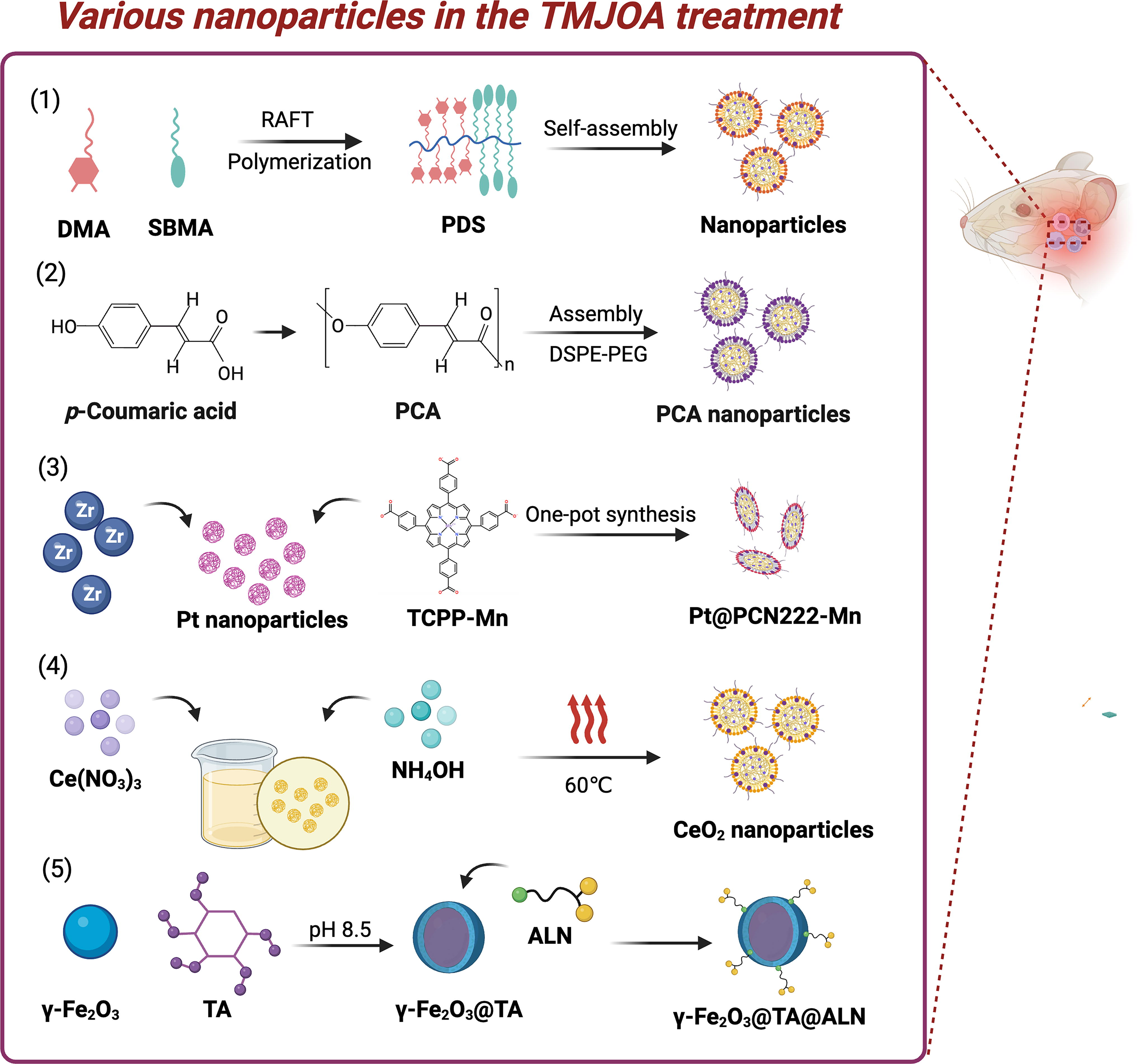
Schematic of various nanoparticles in the TMJOA treatment. (1) Schematic diagram of self-assembled drug-free nanospheres with drug-active function for treating TMJ osteoarthritis. This figure is adapted and is freely accessible from reference 58 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (2) Schematic diagram of PCA NPs contributes to the mitigation of TMJOA progression. This figure is adapted and is freely accessible from reference, 60 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (3) Schematic illustration of Pt@PCN222-Mn remodels the inflammatory microenvironment in TMJOA. This figure is adapted and is freely accessible from reference 61 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (4) CeO2 NPs could effectively remove ROS in chondrocytes to protect TMJ cartilage. This figure is adapted and is freely accessible from reference, 62 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (5) Schematic diagram of the γ-Fe2O3@TA@ALN on TMJ cartilage. This figure is adapted and is freely accessible from reference, 59 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). PCA NPs, poly(p-coumaric acid) nanoparticles.
Reported Nanomaterial Scaffolds
3D printing techniques
3D printing technology holds great potential for TMJ cartilage repair.63,64 TMJ cartilage damage often results in pain and functional impairment, and traditional treatments have limitations to varying degrees. 3D printing allows for the precise fabrication of personalized and biocompatible scaffolds, making it possible for cartilage regeneration. For example, Schek et al. have utilized image-based design and solid free-form techniques to create biphasic composite scaffolds, which successfully promoted the simultaneous generation of bone and cartilage in mice. 63 Helgeland et al. have explored dual-crosslinked 3D-printed gelatin scaffolds, which have demonstrated excellent biocompatibility and mechanical properties and can promote the chondrogenic differentiation of MSCs, providing a novel material option for TMJ cartilage regeneration 65 (Fig. 6). These studies indicate that 3D printing technology, combined with biomaterials and cell therapy, could become an effective means for TMJ cartilage repair. Nevertheless, challenges remain, such as the long-term stability of scaffolds, optimization of cell sources, and BFs. Further research is essential to fully realize its clinical application.
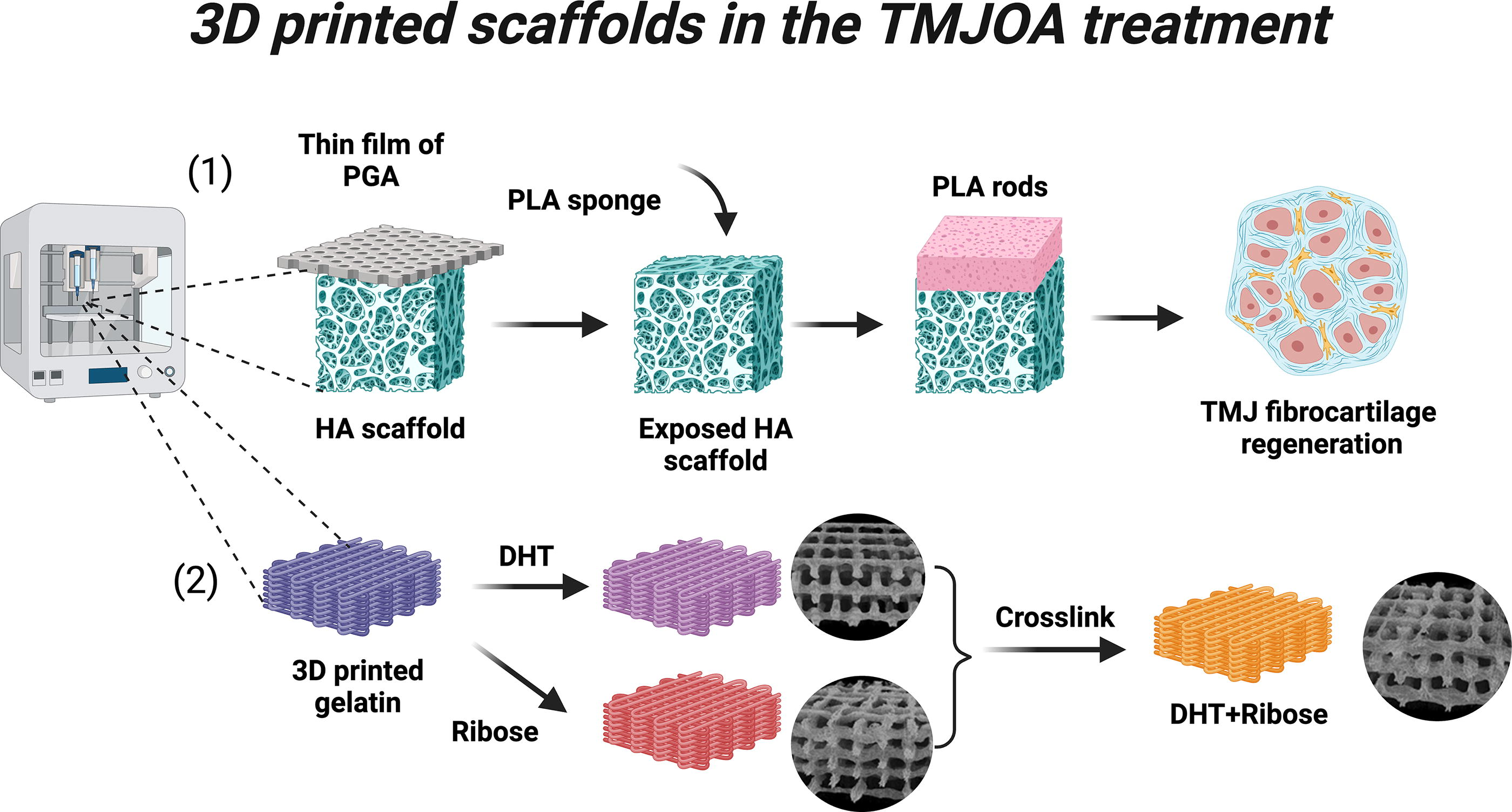
Schematic of various 3D-printing scaffolds in the TMJOA treatment. (1) 3D-printed scaffolds for the regeneration of mandibular condylar fibrocartilage. This figure is adapted and is freely accessible from reference, 63 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (2) 3D-printed gelatin scaffolds, dually crosslinked with ribose and Dehydrothermal (DHT) methods, promote the chondrogenic differentiation of BMSCs. This figure is adapted and is freely accessible from reference, 65 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). 3D, three-dimensional.
Cell seeding in tissue engineering
MSCs are central to cartilage tissue engineering owing to their self-renewal and multipotent differentiation capacities, making them a promising therapeutic strategy for articular cartilage repair.66,67 In preclinical TMJOA studies, MSCs have shown considerable potential to promote cartilage repair, delay degradation, enhance both chondrogenic and osteogenic differentiation, and improve subchondral bone volume and structure.68,69 Commonly used MSCs for cartilage repair include human umbilical cord matrix-derived MSCs, bone marrow stem cells (BMSCs), human adipose-derived regenerative cells, and dental pulp stem cells (DPSCs). For instance, BMSCs have effectively restored condylar cartilage defects in mice, 70 while adipose-derived stromal cells (ADSCs) have shown robust repair capabilities in rabbits, even under hypoxic conditions. 71 Dental-derived stem cells, such as DPSCs and stem cells from human exfoliated deciduous teeth (SHED), are highly accessible and possess significant differentiation potential. 53 Recent studies have shown that DPSCs can inhibit the expression of MMP3 and MMP13 through the STAT1 pathway to treat TMJOA.72,73 The conditioned medium derived from SHED (SHED-CM) has been shown to promote the polarization of M2 macrophages, which secrete inhibitors of the Wnt signaling pathway. This action helps transform chondrocytes from a catabolic (degradative) state to an anabolic (synthetic) state, thereby significantly improving cartilage injury in the TMJ of mice. 74 Additionally, SHED-CM treatment has been demonstrated to enhance the regeneration and repair of mechanically induced TMJOA in mice. 75 Additionally, betaine enhances the chondrogenic differentiation of stem cells from the apical papilla and promotes cartilage repair in TMJOA. 76 Current stem cell delivery methods for OA treatment include local injection, scaffold transplantation, and systemic administration. 77 Local injection directly introduces stem cells into the joint cavity. Scaffold transplantation uses biodegradable supports to facilitate cartilage repair. Systemic administration, such as intravenous injection, delivers stem cells throughout the body but requires careful management to avoid off-target distribution. Each method has its strengths and should be chosen based on the specific clinical scenario. Biomaterial scaffolds designed to deliver stem cells can enhance cell viability and signal release. 78 However, most studies are limited to preclinical settings, and further validation in humans is needed. Key factors such as optimal MSC dose, cell type, implantation method, immunological rejection, treatment durability, and scaffold-stem cell interactions require in-depth investigation to refine MSC-based therapies for TMJOA.
Exosomes delivered via tissue engineering scaffolds
MSC-derived exosomes (MSC-Exos) are nanoscale vesicles secreted by MSCs through paracrine pathways. Their lipid membrane structure plays a crucial role in intercellular communication. MSC-Exos can interact with various cell types through receptor–ligand interactions on the extracellular membrane, thereby modulating cellular behavior and maintaining microenvironmental homeostasis. Enriched with proteins and enzymes, MSC-Exos can regulate ECM homeostasis.79,80 In TMJOA models, MSC-Exos have demonstrated anti-inflammatory effects, enhanced cell proliferation and matrix synthesis, reduced apoptosis and degradation, and promoted joint repair and regeneration.81,82 For instance, extracellular vesicles (EVs) derived from BMSCs can induce TMJOA cartilage reconstruction via the autotaxin-YAP signaling axis, offering a minimally invasive treatment option. 83 Meanwhile, EVs from ADSCs, carrying miR-27b-3p, can regulate macrophage activity by targeting CSF-1, promoting condylar cartilage regeneration under inflammatory conditions. 84 In a mouse TMJOA model induced by MIA, BMSC-derived microvesicles (BM-MSCs-MVs) can outperform platelet-rich plasma (PRP) in therapeutic efficacy, although PRP still improves condylar structure compared to untreated controls. 85 Additionally, exosomes from urine stem cells (USC-Exos) have been explored for their ability to inhibit or reverse TMJOA progression. 86 The integration of exosomes into biomaterial scaffolds, such as Exo-Gel, has emerged as a promising cell-free strategy for TMJ tissue regeneration, highlighting the need for suitable scaffolds to support exosome delivery and function.87B88 -90 However, research on the role of chondrocyte- or macrophage-derived exosomes in TMJOA remains limited91-93 (Fig. 7). Current evidence for MSC-Exos’ molecular mechanisms and clinical efficacy in TMJOA is primarily from small animal models (e.g., rats and mice), with few studies in rabbits. Further large-animal testing is needed for clinical translation. Further testing in larger animals is needed to advance toward clinical application. Additionally, challenges remain in efficiently and consistently producing exosomes at scale, which poses a significant hurdle for their clinical use. Addressing these issues requires interdisciplinary collaboration to refine MSC-Exo-based therapies and ultimately benefit patients.

The mode of action of extracellular vesicles in promoting TMJ cartilage regeneration. (1) Inflammation-stimulated adipose-derived mesenchymal stem cell (ADSC)-derived small extracellular vesicles (sEVs) that highly express miR-27b-3p may regulate macrophages by targeting macrophage colony-stimulating factor-1 (CSF-1), thereby promoting TMJ cartilage regeneration. This figure is adapted from reference, 84 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (2) Human embryonic stem cell-derived sEVs enhance s-GAG synthesis and suppress IL-1β-induced nitric oxide and MMP13 production, with these effects being partially abrogated by inhibitors of adenosine receptor activation, AKT, ERK, and AMPK phosphorylation. This figure is adapted from reference, 81 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (3) Bone marrow mesenchymal stem cell (BMSC)-derived sEVs induce cartilage reconstruction of TMJOA via the autotaxin-Yes-associated protein (YAP) signaling axis. This figure is adapted from reference, 83 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (4) Abnormal biomechanical load can alleviate abnormal calcification of TMJOA degenerative cartilage by affecting exosome composition and secretion of TMJ condyle chondrocytes, promoting cartilage matrix calcification, and inhibiting exosome formation. This figure is adapted from reference, 91 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0). (5) Human urine-derived stem cell exosomes (USC-EXOs) protect chondrocytes by inhibiting apoptosis, reducing inflammation, and promoting proliferation, enhancing cartilage integrity and smoothness in damaged condyles. This figure is adapted from reference, 86 licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0).
BFs loaded in tissue engineering constructs
BFs, including growth factors, mineral ions, and intracellular signaling molecules, are crucial for articular cartilage regeneration. They can be integrated into tissue engineering scaffolds to enhance performance, promote cell growth and differentiation, and support ECM production and homeostasis. Common BFs used for cartilage regeneration include PRP, wingless-type mouse mammary tumor virus (MMTV) integration site family proteins (Wnts), bone morphogenetic proteins, fibroblast growth factors, insulin-like growth factors, TGF-β, tumor necrosis factor-alpha, neural ectoderm-linked gene 1, sex-determining region Y-box family transcription factors (SOX family), interleukin-1 (IL-1), and VEGFs. PRP, in particular, is a rich source of BFs.94B95 -97 Animal studies show that intra-articular injection of PRP promotes fibrocartilage repair and improves subchondral bone microstructure. PRP can also be incorporated into bioinks for 3D-printed scaffolds, promoting MSC differentiation and ECM deposition. Recent research highlights that combining PRP with HA significantly improves therapeutic efficacy, restoring fibrocartilage and normalizing subchondral bone morphology. 47 Clinical trials involving PRP/HA combinations have demonstrated condylar cartilage regeneration, reduced disc displacement, pain alleviation, and improved mouth opening. In another study, PRP-loaded gelatin methacryloyl has been utilized to create an injectable in situ hydrogel for treating significant bone defects. 98 Notably, the Wnt pathway is pivotal in TMJOA. 33 Its aberrant activation induces chondrocyte instability, inflammation, matrix degradation, and bone alterations, driving cartilage degeneration and joint dysfunction. Recent studies show that SHED-conditioned medium, by inducing M2 macrophages to secrete secreted frizzled-related protein 1, inhibits the Wnt pathway, promotes chondrocyte proliferation and matrix formation, and significantly alleviates TMJOA symptoms. 75 Another study indicates that a hydrogel therapy (StemJEL), which restores the Wnt inhibitory niche by combining HA and sclerostin, effectively relieves TMJOA symptoms, improves chondrocyte identity, and demonstrates significant therapeutic effects in multiple animal models.74,99 Kartogenin (KGN) promotes chondrocyte proliferation, increases cell density in the superficial and proliferative zones of the TMJ condylar cartilage, enhances fibrocartilage stem cell proliferation and differentiation, and upregulates chondrogenesis-related factors.100,101 Growth hormone, which targets chondroprogenitor cells, can improve OA scores in rat TMJ without significantly affecting condylar growth. 102 Arthrocentesis combined with a concentrated growth factor injection can improve unilateral TMJOA symptoms in the short term. 103 Daidzein injection reduces oxidative damage and early OA in rabbit TMJ models. 104 Also, lipoxin A4 (LXA4) shows anti-inflammatory properties and improves chondrocyte injury in rat models. 105 Although these novel bioactive molecules promise TMJOA repair, their efficacy and safety require further investigation. Intra-articular scaffold delivery systems, such as liposomes, hydrogels, nanoparticles, and microparticles, have been widely used for sustained drug release. These systems are expected to enhance the therapeutic outcomes of novel bioactive molecules in the future.
Tissue engineering-based drug delivery systems
Tissue engineering scaffolds are currently a focal point in the development of drug delivery systems, owing to their exceptional biocompatibility, biodegradability, nonimmunogenicity, and their versatile, responsive, and tunable properties. In the treatment of TMJOA, NSAIDs are the most commonly used medications. These include celecoxib, diclofenac sodium, acetaminophen, and aspirin. Nevertheless, the use of NSAIDs is often limited due to their notable side effects, which primarily stem from their inhibition of cyclooxygenase-1 (COX-1)-dependent prostaglandin synthesis. In addition to NSAIDs, corticosteroids, glucosamine, and HA have also been employed in managing TMJOA.106,107 Recent advancements include liposomes encapsulating meloxicam to enhance TMJ lubrication and protect cartilage, 108 as well as the use of dasatinib and quercetin to mitigate age-related TMJ cartilage degeneration by targeting senescent cells. 109 The pathogenesis of TMJOA involves factors such as MIA-induced chondrocyte glycolysis disruption, leading to OA-like changes in condylar cartilage. Glycyrrhizic acid, with its anti-inflammatory and antioxidant properties, has shown potential in alleviating MIA-induced TMJOA in rat models. 110 Other promising agents include Bafilomycin A1 (Baf A1), which inhibits osteoclast formation and reduces Netrin-1 secretion to mitigate TMJOA degeneration and pain. 111 Fostamatinib, which preserves cartilage homeostasis via MAPK/NF-κB and AKT/mTOR pathways, 112 as well as yohimbine, which inhibits NF-κB signaling to reduce inflammation. Also, abaloparatide can promote mandibular condylar growth and cartilage repair in adolescent rats.113,114 Other emerging drugs, such as plumbagin, resatorvid, and etanercept, target ferroptosis, TLR4 signaling, and hypoxia-induced pathways, respectively, to reduce inflammation and cartilage damage and improve the cartilage repair microenvironment.115,116 Despite these advances, many novel therapeutic agents are still in the early research stages, lacking rigorous experimental designs and sufficient follow-up periods, leading to inconsistent and uncertain outcomes. Therefore, tissue engineering scaffolds are being explored for precise drug delivery platforms, with intelligent scaffolds capable of responding to environmental stimuli to dynamically adjust drug release patterns and meet diverse therapeutic needs.
Tissue engineering-based gene therapy
Gene therapy, which uses nucleic acids to modulate gene expression, is rapidly advancing disease management and shows significant potential for treating TMJOA. 117 Preclinical and clinical studies have successfully applied gene therapy via intra-articular or intraperitoneal injection of viral vectors, such as adenoviruses or lentiviruses. For example, adenovirus-mediated delivery of lysyl oxidase-like 2 (LOXL2) upregulates the aggrecan gene, exerting chondroprotective effects. 118 Additionally, studies have shown that abnormal mechanical loading activates the mTOR complex 1 (MTORC1) signaling pathway, leading to cartilage degeneration, suggesting that inhibiting MTORC1 could be a novel therapeutic strategy. 119 Other promising approaches include targeting glucose-6-phosphate dehydrogenase to modulate inflammation, using mRNA-based therapies encoding IL-1Ra to reduce joint inflammation, and leveraging noncoding RNAs like circular RNAs and long noncoding RNAs to mitigate cartilage degradation and synovial inflammation.120-122 Tetrahedral framework nucleic acids carrying siRNA-NF-κB have also been used to reduce inflammation and promote TMJOA regeneration. 123 Furthermore, polyamidoamine conjugates have shown potential in mitigating TMJOA inflammation by enhancing the clearance of cell-free DNA. 124 While gene therapy integration in tissue engineering for TMJOA remains underexplored, future studies combining viral vectors with nanotechnology could pave the way for overcoming cartilage regeneration challenges.
The Challenges of Clinical Research
Despite the growing interest in tissue engineering for TMJ cartilage, clinical applications remain limited and lack standardization. To date, therapeutic strategies for TMJOA have predominantly focused on symptomatic management, primarily targeting inflammation reduction, pain alleviation, and restoration of limited mouth opening, rather than actively promoting regeneration of damaged cartilage or subchondral bone. Recent advancements have introduced a novel self-assembling tissue-engineered cartilage, with preclinical studies demonstrating partial efficacy in facilitating TMJ cartilage repair. 125 HA injection therapy can effectively relieve pain and enhance mandibular function in elderly patients suffering from TMJOA. 126 The combination of HA and PRP has shown potential in reducing inflammation, relieving pain, and promoting cartilage regeneration in vitro, in vivo, and in clinical trials.126,127 However, the latest study has conducted a systematic review of randomized controlled trials involving patients with TMJOA and finds that cell-derived orthobiologics, including PRP and other cell-derived products, demonstrate superior efficacy in pain relief and improvement of maximum mouth opening compared to HA. Interestingly, PRP alone shows no significant advantage over other treatments in these trials. 128 Furthermore, a randomized clinical trial reveals that autologous tissue-like stromal vascular fraction injections, combined with joint puncture, outperform arthrocentesis alone in reducing pain and improving mouth opening in patients with TMJOA. 129 However, these studies collectively exhibit several limitations. Sample sizes are generally small, and some studies are marred by participant dropout or the absence of a randomized controlled design, which undermines the reliability and generalizability of the findings. In terms of evaluating therapeutic effects, most studies concentrate on short-term improvements in clinical symptoms, neglecting direct assessments of cartilage repair and regeneration, as well as comprehensive considerations of long-term impacts on patient function and quality of life. Furthermore, treatment parameters such as dosage, duration, and concentration have yet to be standardized. Personalized treatment plans tailored to patients with varying types and severities of TMJOA also require further exploration. To address these issues, efforts should focus on three main aspects. First off, research design quality should be enhanced by increasing sample sizes, improving randomized controlled trials, and reducing participant dropout rates. Second, treatment effects should be comprehensively evaluated by combining short- and long-term indicators, directly assessing cartilage repair and regeneration, and taking into account patients’ overall quality of life. Third, treatment parameters should be standardized by establishing consistent protocols and exploring personalized treatment plans. Specific measures, such as multidisciplinary collaboration, clinical trial validation, and dynamic adjustment of treatment plans, can be employed to improve the reliability, comprehensiveness, and effectiveness of the research.
Conclusion
Overall, the optimal treatment strategy for TMJOA should not merely focus on repairing cartilage defects but also aim to restore the structure and function of the TMJ comprehensively. Despite the progress made, several challenges remain. Although various methods have been proposed to induce cartilage regeneration, identifying the optimal combination of seed cells, BFs, and scaffold materials remains a critical focus in TMJ fibrocartilage tissue engineering. This area warrants further investigation in future studies to optimize therapeutic outcomes. In particular, recent research has highlighted the potential of stem cell-based approaches and the use of advanced biomaterials with enhanced biocompatibility and mechanical properties. These developments are expected to advance the field and improve patient outcomes in treating TMJOA.
Footnotes
Authors’ Contributions
J.M. and Y.F.: Contributed equally to this work. They were involved in the conception and design of the review, as well as the drafting and revision of the article. X.N. and Q.Y.: Participated in the literature search, data collection, and analysis. They also contributed to the writing and editing of specific sections. J.L.: Provided critical guidance and supervision throughout the research process. She contributed to the final revision and approval of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the Natural Science Foundation of Zhejiang Province (LMS25H140004).