
Abstract
Subcutaneous tissue was proposed as an optimal transplant site for islets in treatment for type I diabetes mellitus. However, vascular networks in subcutaneous tissue are too poor in their natural state to allow survive and function of the transplanted graft. This study examined whether subcutaneous implantation of adipose tissue–derived stromal cells (ADSCs) combined with minced adipose tissue could form vascular-rich beds suitable to support islet transplantation. ADSCs were isolated from male C57BL/6J mouse inguinal subcutaneous adipose tissue. ADSCs and minced adipose tissue were implanted syngeneically in subcutaneous tissue of the back of recipient mice. Four weeks later, vascularization in the implanted subcutaneous tissue was evaluated, and islets were transplanted onto the vascularized pockets. Mice that received ADSCs mixed with minced adipose tissue showed a richly vascularized pocket of tissue with significantly higher capillary density than in mice implanted with either ADSCs or minced adipose tissue only. All recipient mice of the combination ADSCs and minced adipose tissue group showed correction in blood glucose level within a week after islet transplantation and maintained normoglycemia for over 8 weeks. These mice became hyperglycemic again after removal of the subcutaneous grafts. This novel method will expand the indications for islet transplant therapy and potential clinical application of cell-based therapy.
Introduction
Subcutaneous tissue has many advantages as a transplant site for islets. The area is accessible with minimal invasiveness under local anesthesia, it provides massive transplantable capacity, and the tissue is removable if severe adverse events eventuate due to the transplanted grafts. However, vascular networks in subcutaneous tissue are too poor to maintain insulin-producing function. 9 Some studies described functional grafted islets with insulin-producing function in subcutaneous tissue pretreated with angiogenic factors and synthetic vascularizing devices to form vascular-rich beds.10–13 Unfortunately, these combined devices are difficult to apply clinically because the synthetic materials would need to remain in the body for a long term.
Adipose tissue–derived stromal cells (ADSCs) are multipotent progenitor cells capable of differentiating into endothelial cells.14,15 In animal experiments, ADSCs induced postnatal neovascularization resulting in collateral formation, and improved the reperfusion of blood flow in femoral artery-ligated ischemic limb.16,17 Further, ADSCs were used successfully to support and augment soft tissues after lipotransfer by vascularizing the transferred adipose tissue. 18 These reports indicated that transplantation of a mixture of ADSCs and minced adipose tissue could potentially form vascular-rich beds in subcutaneous tissue. This study further examines whether such a mixture could be implanted subcutaneously to vascularize pockets of tissue and support grafted islets for long-term function.
Materials and Methods
Animals
The study was conducted in C57BL/6J male mice (CLEA Japan, Inc., Tokyo, Japan) anesthetized with an intraperitoneal injection of 2.5% tribromoethanol. All transplant experiments were performed syngeneically. The Osaka University Graduate School of Medicine Standing Committee on Animals approved all experimental protocols.
Isolation of mouse ADSCs
ADSCs were isolated from the inguinal subcutaneous adipose tissue of 8-week-old C57BL/6J male mice, as reported previously. 19 The cells were cultured in Stem Cell Medium (Nacalai Tesque, Kyoto, Japan) containing 10 ng/mL epidermal growth factor (EGF; PeproTech EC, London, UK), 1 nM dexamethasone, 100 μM ascorbic acid (both from Sigma–Aldrich Japan, Tokyo, Japan), and 5% fetal bovine serum (FBS; Invitrogen, Carlsbad, CA). The ADSCs were used for experiments after 3–5 passages.
Flow cytometric analysis
The ADSCs were characterized by flow cytometry using fluorescein isothiocyanate (FITC)–conjugated mouse monoclonal antibodies to mouse Ly-6A/E (Sca-I), CD31, CD44, CD45, CD117 (all from BD Pharmingen, Franklin Lakes, NJ), and CD34 (Santa Cruz Biotechnology, Santa Cruz, CA). Isotype-identical antibodies served as controls. Analyses were performed using a FACSCalibur flow cytometer and CellQuest Pro software (BD Biosciences, Franklin Lakes, NJ).
Subcutaneous vascularization with ADSC and adipose tissue
Eight-week-old C57BL/6J male mice were used as recipients. Recipient mice were divided into four groups, and implanted as follows to create a rich vascular network in the subcutaneous tissue: group I (n = 6), ADSCs (5 × 105 cells) mixed with minced inguinal adipose tissue (150 μL); group II (n = 5), ADSCs (5 × 105 cells) only; group III (n = 6), minced inguinal adipose tissue (150 μL) only; and group IV (n = 6), nothing implanted. To facilitate the islet transplant technique, a spacer made of nonbiodegradable and non-cell-adherent material (polyester, 10 × 12 mm) was subcutaneously implanted with each of the grafts. Specifically, a small incision was made at the back of recipient mice, and the subcutaneous tissue was split gently. A spacer was inserted in the split space in the subcutaneous tissue. Then, the graft of groups I and III mentioned above was implanted around a spacer. In group II, ADSCs with 300 μL phosphate buffered saline were injected into the subcutaneous tissue contacted with a spacer. In group IV, nothing is implanted except a spacer in the subcutaneous tissue. Finally, the incision was closed with 5-0 absorbable suture. Four weeks later, vascularization in the subcutaneous tissue was examined after removal of the spacer. Twelve-week-old C57BL/6J male mice that were not pretreated with ADSCs, adipose tissue, and a spacer were evaluated additionally as control mice (n = 5).
Isolation of mouse islets
Islets were isolated from 10-week-old C57BL/6J male mice as reported previously. 20 Briefly, type XI collagenase solution (0.5 mg/mL; Sigma-Aldrich Japan) was injected into the common bile duct of mice and digested for 25 min at 37°C. The digested fragments were collected and washed with Hanks' balanced salt solution (HBSS). Islets were purified through a discontinuous Ficoll gradient (Nacalai Tesque), and the islet-rich layer was collected for transplantation.
Subcutaneous islet transplantation
Separate recipient mice of above four groups were set up for subcutaneous islet transplantation. Islet transplantation was performed 4 weeks after each pretreatments for vascularization. Recipient mice were made diabetic by a single peritoneal injection of streptozotocin (250 mg/kg body weight; Sigma-Aldrich Japan) at 7 days before islet transplantation. The diabetic mice were defined as having nonfasting blood glucose levels >350 mg/dL. Islets were transplanted into the subcutaneous tissue pockets of each group after removal of the spacer. All groups received 600 islets (group I, n = 7; group II, n = 7; group III, n = 5; group IV, n = 5). Blood glucose levels were measured once a week by tail snipping, using a portable glucose meter (Nipro Care Fast Meter; Nipro, Tokyo, Japan). After 8 weeks, the graft-bearing subcutaneous tissues from the recipient mice were evaluated by histological examination.
Intraperitoneal glucose tolerance test
After overnight fasting, mice were injected intraperitoneally with glucose at 2 g/kg body weight. Blood glucose levels were measured at 0, 15, 30, 60, 90, and 120 min after glucose injection. Glucose tolerance was tested in recipient mice of group I (n = 5) at 3 weeks after islet transplantation and in nondiabetic mice (n = 5).
Histological and immunohistochemical examination
Graft-bearing subcutaneous tissues were removed and processed for sectioning (4 μm thickness) and staining with hematoxylin and eosin. To evaluate vascularization and the function of the grafted islets, the graft specimens were also immunostained using an anti–von Willebrand factor (vWF) polyclonal antibody (1:1000; Chemicon-Millipore Corporation, Billerica, MA) or anti-insulin polyclonal antibody (1:500; Santa Cruz Biotechnology), respectively. Vessels were identified by positive staining for von Willebrand factor and by morphology. Vessel number was evaluated by randomly counting the vessels in 10 different subcutaneous areas.
Statistical analysis
The pathologist who conducted the blood vessel counting was blinded to the method used in surgical preparation of the animal. Values are expressed as mean ± SD. Statistical comparisons among groups were performed with ANOVA for multiple comparisons. A p-value <0.05 was considered statistically significant.
Results
Characterization of ADSCs
The isolated ADSCs obtained from mouse inguinal adipose tissue were spindle-shaped in morphology (Fig. 1A). Flow cytometric analysis showed these cells to be positive for Ly-6A/E (Sca-I) and CD44 as surface markers of mesenchymal stem cells, but negative for CD31, CD34, CD45, and CD117 as hematopoietic and endothelial lineage markers (Fig. 1B). These results indicated that the ADSCs used in this study were mesenchymal stem cells.

Characteristics of isolated adipose tissue–derived stromal cells (ADSCs). (
Pocket creation for subcutaneous transplantation
The ADSCs and minced adipose tissue were implanted together or alone in the subcutaneous tissue of the back in each group of mice, as detailed in the Materials and Methods section. In addition, a polyester spacer (Fig. 2A) was subcutaneously implanted with all grafts to facilitate the islet transplant technique. Four weeks later, the spacer was removed, leaving a subcutaneous tissue pocket into which islets could be easily transplanted (Fig. 2B). Figure 2C shows the inner surface of the pockets. In group I mice (ADSCs mixed with minced adipose tissue implanted), a reddish and richly vascularized pocket was formed in the subcutaneous tissue. However, vascularization was poor in the tissue pockets of mice in groups II (ADSCs implanted only), III (minced adipose tissues implanted only), and IV (nothing implanted as control).
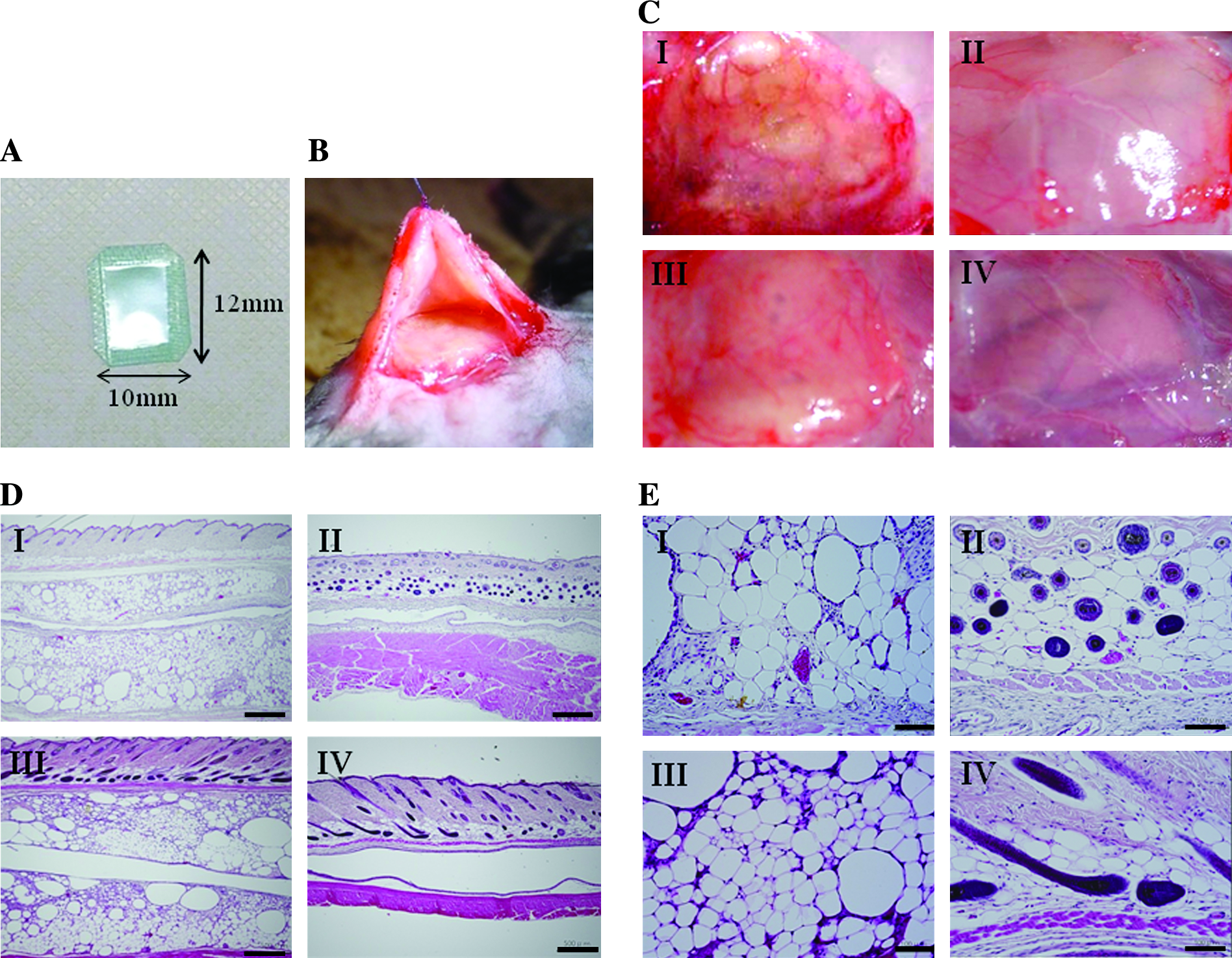
Pocket creation for subcutaneous transplantation of islets. (
The subcutaneous space of recipient mice preimplanted with ADSCs and/or adipose tissue was examined histologically (Fig. 2D, E). Group I recipient mice showed a grafted adipose tissue layer in the subcutaneous space (Fig. 2D). The removed spacer had clearly passed through the center of the grafted adipose tissue. Tissue sections from group I mice also showed an abundant vessel structure filled with red blood cells, while this was not seen in mice from the other three groups (Fig. 2E). Recipient mice from group III had a similar grafted adipose tissue layer to group I mice, but the vascular formation was poor. Mice from group II showed some vessel-like structures around a capsule in the subcutaneous tissues, and a few vessels were observed histologically in group IV mice.
Evaluation of vascular beds in the transplantation pocket
To evaluate vascular bed formation in the pocket, sections of subcutaneous tissues from mice of groups I–IV were stained for von Willebrand factor (Fig. 3A) to visualize such vessels. Vascularization was evaluated by the vessel number per square millimeter of subcutaneous tissue harvested at 4 weeks after implantation (Fig. 3B). The number of detectable vessels in group I mice was significantly higher than in those from all other groups (group I, 57 ± 12/mm2; group II, 29 ± 7/mm2; group III, 21 ± 4/mm2; group IV, 16 ± 4/mm2; nonpretreated control mice, 12 ± 3/mm2). The density of these vessels was higher in groups II and III than that in nonpretreated control mice, although not to the extent of group I. There was no significant difference in vessel number between group IV mice (spacer only inserted) and nontreatment control mice, indicating that the spacer had no effect on vascularization. These results indicate that implantation of a mixture of ADSCs and minced adipose tissue is the most promising for vascular bed formation before islet transplantation.

Evaluation of vascular networks in the subcutaneous pockets. (
Islet transplantation into the vascular-modified subcutaneous pockets
To examine whether the subcutaneous tissue pockets could support functional islet transplantation, nonfasting blood glucose levels of recipient mice after transplantation were determined serially (Fig. 4A). All recipient mice of group I (implanted mixture of ADSCs and minced adipose tissue; n = 7) showed a rapid decrease in blood glucose level to normoglycemia (<200 mg/dL) within 1 week after islet transplantation, and the normoglycemia was maintained for over 8 weeks. These mice became hyperglycemia again after removal of the subcutaneous graft. The nonfasting blood levels decreased slightly after islet transplantation in group II mice (n = 7), but not to normoglycemic levels. No recipient mice of group III (n = 5) or group IV (n = 5) showed a decrease in nonfasting blood glucose levels during the 8-week posttransplantation period.

Vascular network–formed subcutaneous pockets are suitable sites for islet transplantation. (
Intraperitoneal glucose tolerance tests were performed for recipient mice of group I at 3 weeks after islet transplantation (Fig. 4B). All mice in this group showed a good response to the glucose load with an immediate return to normoglycemia, as observed in nondiabetic mice.
Many viable islets were detected in the grafted adipose tissue of group I mice at 8 weeks after islet transplantation (Fig. 4C). Immunohistochemical examination revealed that the engrafted islets could also produce insulin in vivo over the longer term (Fig. 4C, right panel), indicating that the grafted islets received sufficient oxygen and nourishment via the neovascularization for adequate function in the subcutaneous tissue.
Discussion
Subcutaneous tissue was proposed as an optimal site for therapeutic islet transplantation based on easy access for implantation and removal of the graft with minimal invasiveness. However, unmodified subcutaneous tissue lacks the blood flow needed to support the transplanted islet in a functional state, leading to graft ischemia and necrosis. It is thus necessary to establish dense vascular networks to sufficiently nourish the transplanted grafts and maintain long-term function. We have established a technique to prepare vascular beds in subcutaneous tissue suitable for a transplant site by preimplanting a combination of ADSCs and minced adipose tissue.
Previous studies subcutaneously implanted artificial devices containing basic fibroblast growth factor (bFGF) or matrigel, with a pored stainless steel diffusion chamber serving as the vascularizing device.10–13 The grafted islets in these cases showed functional insulin production at the subcutaneous tissue sites.10–13 However, long-term placement of artificial material in the body may cause overgrowth of fibroblasts and calcification surrounding the device due to chronic inflammation, leading to a diminished supply of oxygen and nutrition to the transplanted graft. 21 Our method avoids these problems by using the patient's own tissues, thus making it more attractive for clinical application.
A previous study demonstrated vascularization followed by reperfusion of blood flow to ischemic sites when ADSCs were implanted in ischemic model animals. 22 The vascularization effects of ADSCs probably depend on the following two mechanisms. First, ADSCs secrete angiogenic growth factors such as hepatocyte growth factor and vascular endothelial growth factor (VEGF).22,23 Second, ADSCs can themselves differentiate into endothelial cells to make new vessels.14,15 Further, ADSCs augment the secretion of angiogenic growth factors such as VEGF under hypoxic conditions. 23
In the present study, dense vascular networks were induced in the subcutaneously grafted adipose tissue in recipient mice implanted with a mixture of ADSCs and minced adipose tissues. In addition, the density of capillary vessels in the subcutaneous tissue was significantly higher in these mice than in the other experimentally implanted or nonimplanted mice. We propose the following mechanisms for the improved vascularization with a mixture of stem cells and adipose tissue over either of the components implanted alone. First, mixing ADSCs with the adipose tissue stimulates an artificial hypoxic state, setting off a signaling cascade from the adipose tissue to the ADSCs to respond to the ischemia by vascularization. In addition, the adipose tissue forms an ideal scaffold for the ADSCs to engraft and function in subcutaneous tissue.
The vascular beds in subcutaneous tissue prepared by our method supplied sufficient blood flow to the engrafted mouse islets for successful long-term engraftment and function. The results of intraperitoneal glucose tolerance tests indicated that the grafted islets functioned similar to normal islets in nondiabetic mice, and that all recipient mice became hyperglycemic again after removal of the graft-bearing subcutaneous tissues. These data confirmed that the transplanted islets were functional and able to correct the blood glucose levels of the diabetic recipient mice. Our study therefore showed for the first time that the rich vascular beds needed for transplantation were successfully induced in normal subcutaneous tissue by ADSCs.
In another similar article, Chen et al. reported that the intraabdominal epididymal fat pad had high blood flow and was a useful site for islet transplantation as well as the liver via portal vein in a mouse model. 24 However, their technique is a invasive procedure for the recipient, because a laparotomy under general anesthesia is necessary. At the same report, they said that the epididymal fat may not be a practical site for clinical islet transplantation. Although the subcutaneous tissue has insufficient blood flow, the clinical application of subcutaneous islet transplantation is possible enough by adding pretreatment. Considering the relationship of the skin surface area and implanted islet volume, we think that approximately 400,000 human islets are able to be transplanted in an area of 10 cm2.
Regenerative medicine for diabetes is an emerging area for potential clinical application, and administration of these transdifferentiated insulin-producing cells looks promising as a novel therapy.25,26 For realization of stem cell–derived cellular therapy, the transdifferentiated cells should not elicit adverse events such as carcinogenesis or infection. One big advantage of our method is that if such complications occur after administration, the grafts could be removed relatively easily in comparison to conventional islet transplantation procedures.
In conclusion, we successfully established rich vascular networks in subcutaneous tissue using the recipient's own bioresources, that is, ADSCs and subcutaneously derived adipose tissue. Islets implanted into these vascularized sites engrafted successfully and functioned well in the subcutaneous tissue over a long term. Our study promises the potential of islet transplant therapy and a future platform for cell-based treatment of diabetes involving regenerated insulin-producing cells.
Footnotes
Acknowledgments
This study was supported in part by a Grant-in-Aid to Yoshiki Sawa from New Energy and Industrial Technology Development Organization (NEDO), Japan, and in part by a Grant-in-Aid to Akifumi Matsuyama from Kobe Translational Research Cluster, the Knowledge Cluster Initiative, Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan.
Disclosure Statement
No competing financial interests exist.