
Abstract
In vivo engineering of hepatic tissue based on primary hepatocytes offers new perspectives for the treatment of liver diseases. However, generation of thick, three-dimensional liver tissue has been limited by the lack of vasculature in the tissue-engineered constructs. Here, we used collagen hydrogel as a matrix to generate engineered hepatic units to reconstitute three-dimensional, vascularized hepatic tissue in vivo. Hepatocytes harvested from Sprague–Dawley rats were mixed with liquid type I collagen, concentrated Dulbecco's modified Eagle's medium (2 ×), and hepatocyte maintenance medium to create hepatocyte/collagen hydrogel constructs. The constructs were then dissociated into cylindrical hepatic units (diameter/height: 2000–4000 μm/500–1000 μm). Stacking of hepatic units under the subcutaneous space resulted in significant cell engraftment, with the formation of large fused hepatic system (more than 0.5 cm thickness) containing blood vessels. In contrast, only less cell engraftment could be achieved when hepatocytes were transplanted in a manner of whole constructs. Functional maintenance of the engineered hepatic tissue was confirmed by the expression of liver-specific mRNA and proteins. The engineered hepatic tissue has the ability to respond to the regenerative stimulus. In conclusion, large hepatic tissue containing blood vessels could be engineered in vivo by merging small hepatic units. This approach for tissue engineering is simple and represents an efficient way to engineer hepatic tissue in vivo.
Introduction
Over the past years, studies in this field have developed several approaches, including the use of biodegradable polymer scaffolds to provide a platform for hepatocyte attachment, transplantation of suspended hepatocytes with extracellular matrix components and hepatocyte sheet-layered technique, and functional hepatocyte aggregates which possessed long-term survival, have been achieved.3–7 However, one major limitation has been the lack of effective methods to overcome the limits of mass transport to create thick, vascularized hepatic tissues. An attractive experimental solution to address this problem may be to merge small engineered constructs that can be efficiently diffused and easily vascularized to form an integrated large tissue. This concept has been demonstrated to be effective in creating thick, vascularized myocardial tissue by repeating transplantations of single-cell sheets in an appropriate lag period. 8 The entrapment of cells in the hydrogels can not only provide three-dimensional growth support but also form engineered constructs with a tissue-like density which could efficiently promote cell–cell contact. 9 We therefore hypothesized that hepatic units based on hydrogels, especially on natural hydrogels that are easy to be integrated with each other as well as the recipient, 10 promise to form large, vascularized hepatic tissues when transplanted in vivo.
Here, we reported a very simple and effective tissue engineering approach based on small hepatic units to create thick, vascularized hepatic tissue using type I collagen hydrogel as a matrix for the growth and differentiation of hepatocytes. Freshly isolated hepatocytes were mixed with liquid collagen, concentrated Dulbecco's modified Eagle's medium (DMEM, 2 ×), and hepatocyte maintenance medium to generate a hepatocyte/collagen hydrogel construct. The construct was then dissociated into hepatic units. A total volume of 0.3 mL of the grafts consisting of 20–25 hepatic units was stacked under the subcutaneous space, and the engraftment of hepatocytes and tissue formation were evaluated.
Materials and Methods
Animals
Male Sprague–Dawley (SD) rats weighing 250–300 g (Laboratory Animal Centre of the Academy of Military Medical Sciences, Beijing, China) were used as donors and recipients. All animals were maintained in the Animal Center at Chinese PLA General Hospital, and all the animal experiments were approved by the Animal Care Committee of General Hospital of PLA.
Hepatocyte isolation
Hepatocytes were harvested from SD rats weighing 200–250 g by a two-step in situ collagenase perfusion technique modified from that described by Seglen. 11 In brief, SD rats received barbital sodium intraperitoneally, at a dose of 200 mg/kg rat. After laparotomy, a 21-gauge infusion needle was inserted into the portal vein and secured. The inferior vena cava beneath the liver was cut, and preperfusion started with 37°C Hank's solution without calcium but supplemented with 0.2% ethylenediamine tetraacetic acid. About 250 mL Hank's solution was flushed through the liver at a flow rate of 10 mL/min. Directly after the preperfusion, 20 mL of 37°C collagenase solution (Hank's solution with calcium containing 0.05% collagenase and 0.83 mg/mL hydroxyethyl piperazine ethanesulfonic acid) was flushed through the liver at a flow rate of 10 mL/min. Then, the liver was removed from the rat and digested at 37°C in 5% carbon dioxide for another 20 min. The liver was then placed in a dish containing DMEM and combed to release hepatocytes. The cell suspension was filtered through a steel gauze (100 mesh) to remove undigested tissue. Filtered hepatocytes were purified by three rounds of low centrifugation (500 rpm/min for 3 min). The total yield of hepatocytes was 1.7–2 × 108/rat, and the viability was more than 86% based on trypan blue exclusion.
Construction of engineered hepatic units
About 1.6 × 108 freshly isolated hepatocytes from rat were mixed with 8 mL of liquid collagen type I (2 mg/mL) prepared from SD rat tails, concentrated DMEM (2 ×), and hepatocyte maintenance medium (HepatoZYME-SFM; Gibco, Carlsbad, CA); pH was neutralized by titration with NaOH. All the above procedures were carried out on ice. The reconstitution mix was pipetted into a 1-mL syringe and incubated for 10–15 min at 37°C and 5% carbon dioxide to allow hardening of the reconstitution mix. Then, the gelled hepatocyte/collagen hydrogel construct was pushed out and dissociated into cylindrical hepatic units with a structural feature of 2000–4000 μm in diameter and 500–1000 μm in height.
In vivo implantation
Male SD rats were anesthetized by intraperitoneal injection of barbital sodium. After a mini-incision at the inguina, 20–25 hepatic units per site (a total volume of 0.3 mL) were implanted in the capsule produced by elevating the skin. Rats implanted with whole cylindrical constructs (a total volume of 0.3 mL) were used as a control group. After transplantation, the incision was closed. For the study of induction of hepatocyte proliferation, a two-thirds liver resection was further performed on rats, and 5-bromodeoxyuridine (BrdU) was administrated twice a day for 7 days. The rats were sacrificed by excess anesthesia on days 3 and 7 after implantation, and the ectal tissues of subdermal plane at the site of transplantation were harvested and subjected to histological investigation and reverse transcription–polymerase chain reaction (RT-PCR) analysis. For the rats used to examine the function of blood vessels in the engineered liver tissue, a laparotomy was performed before explantation, and the animals were administered 20 mL heparin solution (100 IU/mL) and then 20 mL India ink solution (India ink [50%, v/v, India ink; Solarbio, Beijing, China] in 5% gelatin and 4% mannitol) via the abdominal aorta.
Histology and immunohistochemistry
Specimens harvested from explanted subcutaneous tissue containing the engineered liver tissues were fixed in formalin, paraffin-embedded, and stained with hematoxylin and eosin. For immunohistochemical analyses, nonspecific sites of slides were saturated with goat serum. Slides were incubated with monoclonal rabbit anti-human albumin antibody (1:2000; Dako), monoclonal rabbit anti-rat CD31 (1:200; Boster, Wuhan, China), monoclonal mouse anti-BrdU (ready-to-use; Zhongshan, Beijing, China), monoclonal mouse anti-cytokeratin 18 (CK18, 1:200; Boster), or polyclonal rabbit anti-CD68 (ready-to-use; Boster) at 4°C overnight. The following procedure was performed according to the protocol provided in the kit of Rabbit Kit HRP-DAB System (CTS005; R&D, Minneapolis, MN) or Mouse Kit HRP-DAB System (CTS002; R&D). After rinsing, the sections were reacted for 4 min with 3,3′-diaminobenzidine (DAB) substrate and counter staining was performed with hematoxylin.
Morphometric analysis
Hepatocyte cell area in the grafts was determined from five different fields per slide (magnification, × 100), randomly selected from captured images of three hematoxylin-and-eosin slides cut from one implant (three animals at each time point or group). Proliferating hepatocytes were estimated by counting the number of positive cells obtained from 10 different immunohistochemical slides. The analysis was performed with a computer-assisted morphometric image system (Image-Pro Plus, version 6.0, Media Cybernetics, Bethesda, MD).
RT-PCR analysis
Total RNA was extracted from the rat liver, the subcutaneous tissue, or the subcutaneous tissue containing the engineered liver tissues. RT of extracted RNA was performed using random hexamer primers. The PCR with cDNA was performed with the following primers: 5′-TTG CCA AGT ACA TGT GTG AG-3′(sense) and 5′-GGT TCT TCT ACA AGA GGC TG-3′ (antisense) for albumin (a 372-bp product according to GenBank accession no. NM 134326); 5′-ACA TCC GGG GCA TCT ACA ATG-3′ (sense) and 5′-AAA GAG ATG CAG CAG GCC CAA-3′ (antisense) for glucose-6-phosphatase (G6Pase) (a 337-bp product according to GenBank accession no. NM 013098); 5′-TGC TGC TTT GGC TGT ATG T-3′ (sense) and 5′-TGA GCG TGA ACA AGA ACC A-3′ (antisense) for 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) (a 229-bp product according to GenBank accession no. NM 013134); 5′-AAT GCA TCC TGC ACC ACC AA-3′(sense) and 5′-GTA GCC ATA TTC ATT GTC ATA-3′ (antisense) for glyceraldehyde-3-phosphate dehydrogenase (a 515-bp product according to GenBank accession no. XR 031712). PCR was carried out in a programmable Omn-E Thermal Cycler (Hybaid, Teddington, United Kingdom) under the following conditions: 94°C for 5 min; and then 32 cycles, each comprising denaturation for 1 min at 94°C, annealing for 1 min at 55°C (albumin and glyceraldehyde-3-phosphate dehydrogenase) or 60°C (G6Pase and HMG-CoA reductase), and extension for 1 min at 72°C. After the PCR was completed, reaction tubes were kept for 4 min at 72°C and then at 4°C. The samples were analyzed on 2% agarose gels.
Results
Formation of fused hepatic grafts
To generate thick, engineered hepatic tissue in vivo, hepatic units that could be merged together were created using collagen hydrogel as a matrix for the growth of hepatocytes. Freshly isolated hepatocytes were mixed with liquid collagen hydrogel at a tissue-like density to generate hepatocyte/collagen hydrogel construct (Fig. 1a). On polymerization of gels, the construct was dissociated into small, cylindrical units with a structural feature of 2000–4000 μm in diameter and 500–1000 μm in height (Fig. 1b). The hepatic units stacked together and formed small interstice from each other after transplantation under the subcutaneous space (Fig. 1c). Three days after implantation, the hepatic units fused together and formed soft hepatic grafts integrated with the recipients in the implanted sites (Fig. 1d).
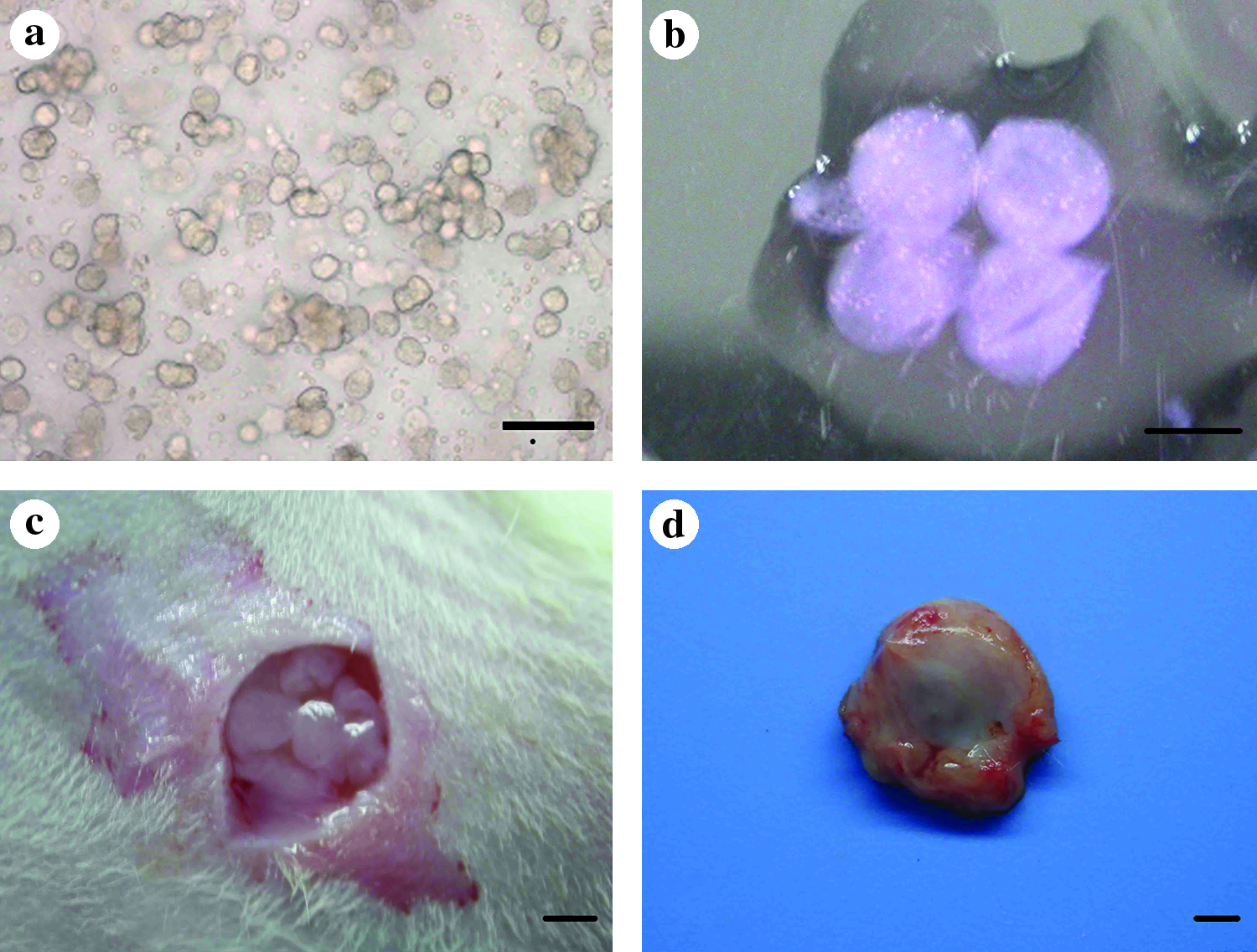
Creation and in vivo transplantation of engineered hepatic units. (
Hepatocyte engraftment
Survival and engraftment of the implanted hepatocytes under the subcutaneous space was examined by histological observation of the formed hepatic grafts. As shown in Figure 2, transplantation of hepatocytes in a manner of hepatic units promoted significantly the survival and engraftment of hepatocytes in vivo with the formation of large hepatic tissue masses (Fig. 2a–c). Quantitative analysis showed that the area of hepatocytes occupied less than 37.2% ± 5.2% of the total area in the rats implanted with whole constructs at day 3 (Fig. 2a). In contrast, significant and persistent cell survival by the formation of large hepatic tissue mass, which accounted for above 75.99% ± 4.3% at day 3 and 85.33% ± 3.2% at day 7 of the fused graft, was achieved when hepatocytes were implanted in a manner of hepatic units (Fig. 2b, c). More importantly, the large hepatic tissue masses fused together and formed larger hepatic system, and the thickness could reach 0.5 mm.
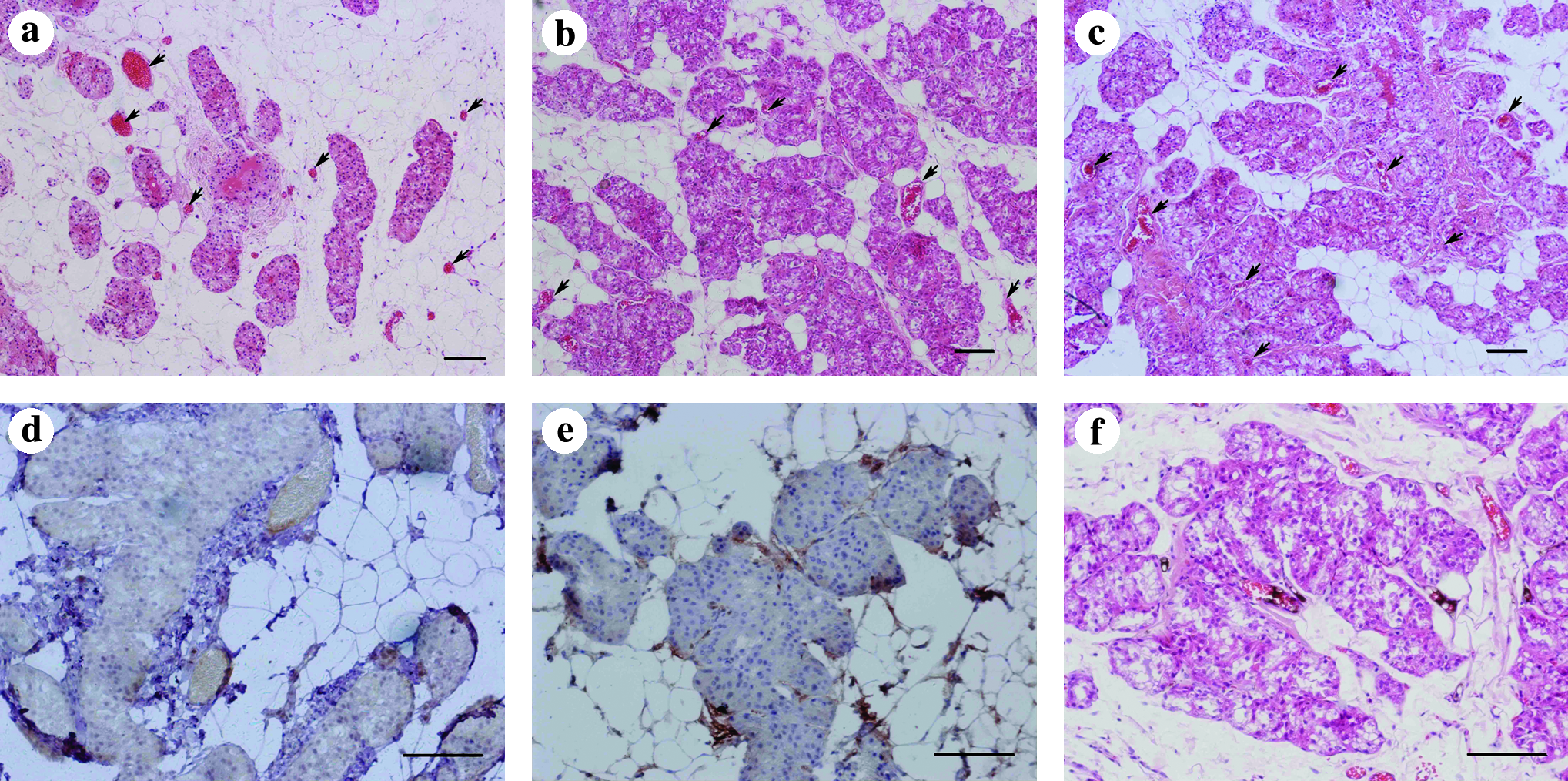
Engraftment of hepatocytes and neovascularization under the subcutaneous space. (
Neovascularization of engineered hepatic tissue
Simultaneous with the merging of the hepatic units, many newly formed blood vessels were found in the engineered hepatic system at day 3, which are mainly located at the periphery of hepatic tissue mass (Fig. 2b). The neovascularization increased with time and penetrated gradually into the inner of the hepatic tissue mass, and by day 7, many blood vessels were formed within and surrounding the hepatic tissue mass (Fig. 2c). We also confirmed that the established vascular vessels were composed of mature endothelial cells, as demonstrated by positive staining for CD31 that was expressed on mature endothelial cells (Fig. 2d, e). Functional capillaries could also be visualized by India ink labeling (Fig. 2f). These results indicated that the fused hepatic system could be rapidly and sufficiently vascularized through the infiltration of the recipient blood vessels. In addition, no positive cells for CD68 were observed in the engineered hepatic tissue (data not shown).
Characterization of the engineered hepatic tissue
The hepatocytes in the hepatic tissue mass at day 7 retained hepatocyte-specific morphology, that is, round shape, large nuclear/cytoplasm ratio, and binuclear cells, and rearranged to form gland-like structure resembling the hepatic cord of the native tissue (Fig. 3a, b). Additionally, endothelial sinusoid structure between gland-like structures could be found within the tissue which closely resembled the liver sinusoid (Fig. 3b). The detection of albumin and CK18 in the engineered tissue showed that the hepatocyte phenotype was maintained (Fig. 3c, d).
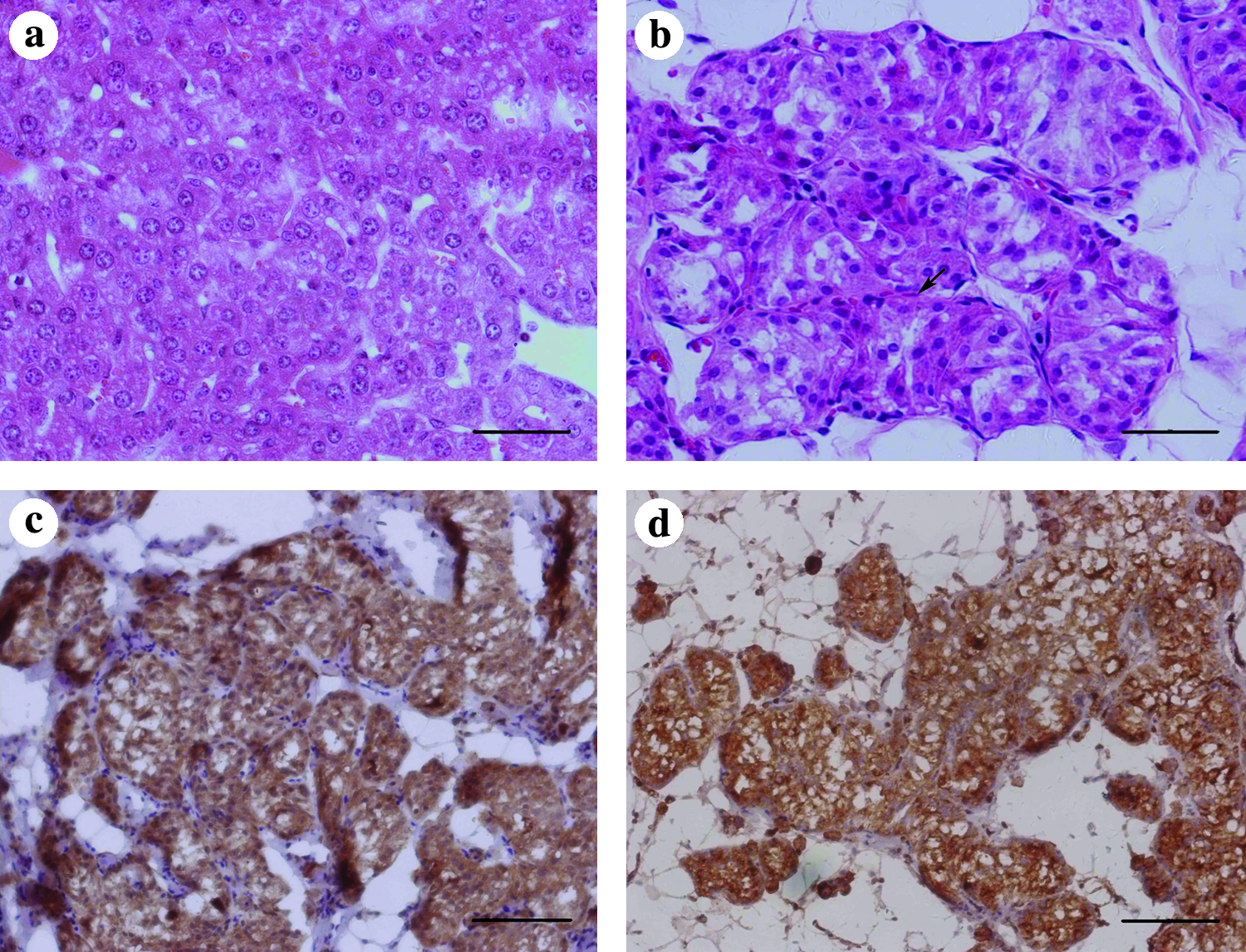
Morphological and functional characterization of the engineered hepatic tissue at day 7. (
Hepatocyte-specific mRNA expression of the engineered hepatic tissue
We then investigated whether the newly engineered hepatic tissue at day 7 had a hepatocyte-specific gene expression profile at the level of transcription. As shown in Figure 4, the expression profile of hepatocyte-specific mRNA from the engineered tissues was demonstrated by the strong expression of albumin, G6Pase, and HMG-CoA reductase (Fig. 4).
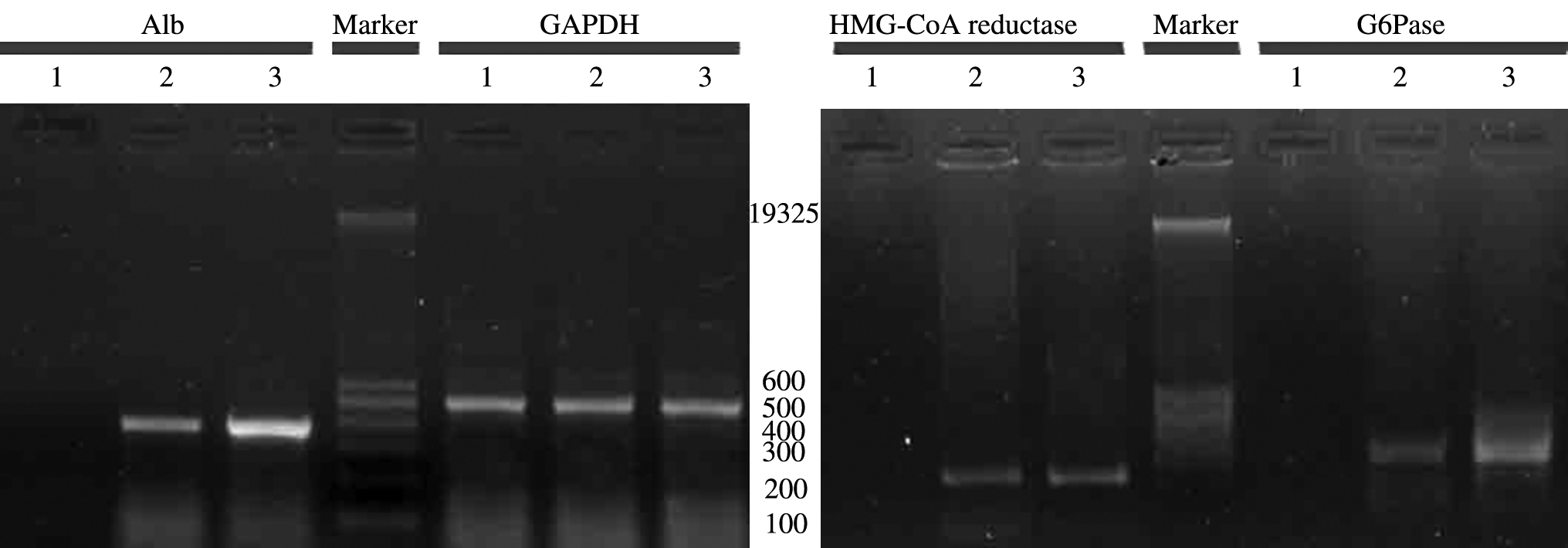
Hepatocyte-specific mRNA expression of the engineered hepatic tissues. The engineered hepatic tissue under the subcutaneous space at day 7 after transplantation expressed liver-specific gene expression (Alb, G6Pase, and HMG-CoA reductase). Lane 1: subcutaneous tissue without hepatocyte transplantation as negative control; lane 2: native rat liver as a positive control; lane 3: engineered liver tissue under subcutaneous space. Alb, albumin; G6Pase, glucose-6-phosphatase; HMG-CoA, 3-hydroxy-3-methylglutaryl coenzyme A; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Regenerative potential of the engineered hepatic tissue
To address whether the engineered hepatic tissue under the subcutaneous space has the ability to respond to a regenerative signal, we induced a regenerative stimulus by performing a two-thirds liver resection in the recipient rats and delivered BrdU for 7 days. Our results showed that 37.7% ± 2.1% of the hepatocytes were labeled with BrdU in the engineered liver tissues after the two-thirds liver resection (Fig. 5b). In contrast, in the sham-operation group, only 8.2% ± 2.5% of the cells had BrdU labeling (Fig. 5a). These data suggested that the engineered hepatic tissues had the ability to proliferate and grow in response to a regenerative event.

Immunohistological staining for 5-bromodeoxyuridine of the engineered hepatic tissues in rats that received two-thirds hepatectomy at day 7: (
Discussion
In this study, we developed an innovative tissue engineering approach, in which hepatocytes were transplanted in vivo in a manner of small hepatic units that were created from collagen hydrogel. Our results showed that efficient engraftment of implanted hepatocytes, with the formation of integrated, large hepatic tissue (more than 0.5 cm thick) containing blood vessels, have been achieved. This clearly demonstrated that the present approach could efficiently improve the diffusion of mass transport and generate thick hepatic tissue.
In vivo liver tissue engineering by implanting hepatic grafts has the potential to provide persistent functional support for a variety of liver diseases.6,7,12 However, the insufficient engraftment of hepatocytes and the subsequent limited tissue formation have been the major obstacles for producing efficient therapy. Studies have shown that higher hepatocyte survival could be achieved by implanting hepatic grafts into vascularized or prevascularized cavity, in which abundant vasculature provides sufficient nutrient supply as well as attachment of endothelial cells for the implanted hepatocytes.5–7 However, large hepatic tissue containing multilayer hepatocytes has not been reported. In fact, in vitro study showed that thicker tissue could be achieved by creating hepatic construct with an internal architecture allowing for convective flow of culture medium through the construct because hepatocytes are highly metabolic cells and require a nearby nutrient supply source for viability. 9 The implanted hepatocytes begin to metabolize at once after transplantation in vivo, whereas the process of angiogenesis and vasculogenesis from the surrounding tissue will take days to develop. 13 During this initial stage, the hepatocytes are mainly fed by passive diffusion and the inner cells of the constructs will die within several hours because of the lack of nutrient and oxygen once the thickness is beyond 100–200 μm so that the diffusion can reach. This may be the major, if not the only, reason that leads to the insufficient number of viable cells, and thus the failure of generating thick hepatic tissues. Additionally, the implanted hepatocytes experienced death when the density of hepatocytes in the grafts was too low even if they were transplanted into prevascularized cavity, indicating the importance of cell–cell contact for the engraftment of hepatocytes and formation of engineered hepatic tissues. 7 Based on the above hypotheses, we created hepatic units that could be efficiently diffused and easily vascularized by entrapping hepatocytes in the collagen hydrogel at a tissue-like density which could promote cell–cell contact. Our results clearly demonstrated that great engraftment of hepatocytes has been achieved when the hepatic units were stacked under the subcutaneous space. Moreover, rapid neovascularization of the fused hepatic system indicated that the implanted hepatocytes may maintain long survival.
Sinusoid-like structure was observed in our engineered hepatic tissues, as shown in Figure 3b. The rebuilding of liver architecture was promoted by endothelial cells. 14 Previous results as well as our study showed that the newly formed hepatic tissues contained numerous endothelial cells within the tissue. 6 However, the hepatocytes and endothelial cells in the hepatic tissue usually grew randomly to form dense cell aggregates. The formation of sinusoid-like structure indicated that our approach may be beneficial for tissue rebuilding. Another important liver-specific feature, that is, its ability to respond to a regenerative signal, was demonstrated by the BrdU incorporation experiment. In addition, liver-specific mRNA expressions, including albumin, G6Pase, and HMG-CoA reductase, similar to the results found by Yokoyamaa were also detected. 6 These results showed that our engineered tissue have the characteristics of structure and function resembling the native liver tissue. However, compared with the native liver tissue, the engineered liver tissue has many disadvantages: For example, it lacked the structure of biliary tubular and had no normal liver lobe.
The subcutaneous space is one of the most attractive sites for hepatic tissue engineering because it is readily accessible and allows for the transplantation of a large number of cells.5,6 Several researchers had successfully engineered small functional hepatic tissue under the subcutaneous space and functional substance exchange between the systemic circulation and the engineered hepatic tissues had also been demonstrated.6,7 The engineered hepatic tissue under the subcutaneous space may provide support for acute liver failure until the native livers regenerate in patients with chronic liver failure, to improve disabling hepatic encephalopathy. 12 In our study, the formation of vascularized hepatic tissue was beneficial for plasma exchange between the engineered hepatic tissue and the general circulation, and hence more efficient substance exchange may be established.
In conclusion, our results strongly demonstrated that the hepatic units based on collagen hydrogel could efficiently promote hepatocyte engraftment and thick, vascularized tissue formation in vivo. Further studies will be necessary to demonstrate its therapeutic potential for liver diseases. This approach for tissue engineering is simple and represents an efficient way to engineer hepatic tissue in vivo.
Footnotes
Acknowledgments
This work was supported by the Natural Science Foundation of China (50573091).The authors thank L. Yu for technical assistance in histological staining.
Disclosure Statement
No competing financial interests exist.