
Abstract
This study was performed to assess the bone healing supporting characteristics of porous calcium phosphate (Ca-P) cement when implanted in a rabbit segmental defect model as well as to determine the reliability of torque testing as a method to verify bone healing. The middiaphyseal radius was chosen as the area to create bilaterally increasing defect sizes (5, 10, and 15 mm), which were either filled with porous Ca-P cement or left open as a control. After 12 weeks of implantation, torque test measurements as well as histological and radiographic evaluation were performed. In two of the open 15 mm control defects, bone bridging was visible at the radiographic and histological evaluation. Bone was observed to be present in all porous Ca-P cement implants (5, 10, and 15 mm defects) after 12 weeks. No significant differences in torque measurements were observed between the 5 and 10 mm filled and open control defects using a t-test. In addition, the mechanical strength of all operated specimens was similar compared with nonoperated bone samples. The torsion data for the 15 mm open defect appeared to be lower compared with the filled 15 mm defect, but no significant difference could be proven. Within the limitation of the study design, porous Ca-P cement implants demonstrated osteoconductive properties and confirmed to be a suitable scaffold material in a weight-bearing situation. Further, the used torque testing method was found to be unreliable for testing the mechanical properties of the healed bone defect.
Introduction
Calcium phosphate (Ca-P) cement is a synthetic bone grafting material. An important advantage of this material is that it is injectable, can be maintained locally, and is easy to shape, which makes it very effective for the restoration of large bone defects with an irregular or abnormal shape. After setting, the material can provide mechanical support and can serve as a substratum upon which the cells attach, proliferate, and undergo differentiation because of its high similarity and compatibility with natural bone.1–4 The Ca-P cement can be provided with an additional porosity. It is anticipated that such porosity will further increase the osteoconductivity and enhance the degradation of the material.5,6 Also, the material can be used as a delivery system for the supplementary release of growth factors to further boost bone formation. 7
Standard techniques to assess the bone forming capacity of a bone graft substitute are X-ray, microcomputed tomography, and histological analysis. Besides, mechanical testing is applied to determine the strength of the regenerated bone defect. A review of the literature shows that mechanical tests, such as torsional,8–15 three points bending, 16 and tensile strength 17 measurements, are used to evaluate the force of the healed bone. All these mechanical methods are associated with advantages and disadvantages. For example, for long segmental defect models, torsional testing is considered to be appropriate, but such a torque test can be performed in different ways.18–20 Some studies assess the total ulna–radius complex during torque testing, whereas others separate the radius or ulna to examine the characteristics of the single bone alone. It can be questioned whether such a separation is feasible without damaging the regenerated tissue.
In view of the aforementioned, the aim of this study was to determine the bone regenerative capacity of porous Ca-P cement when applied in segmental defects created in the radius of rabbits. In addition, we intended to determine the reliability of torque testing as a method to verify bone healing, with the complete ulna–radius complex maintained during the torque assay. 18 We hypothesized that the porous Ca-P cement would enhance bone healing independent of the created defect size.
The porous Ca-P cement was used in a preset form to avoid experimental variation due to differences in implant shape or total amount of implant material. The middiaphyseal radius was chosen as the area to create the defects. Three different defect sizes were created, that is, 5, 10, and 15 mm. It was decided to create no defects larger than 15 mm to avoid problems with the installation of the porous Ca-P implants because of the curvature of the radius. It is claimed that this segmental defect model does not need any kind of internal or external fixation because the left intact ulna provides sufficient stability.18,21–24
Materials and Methods
Preparation of porous Ca-P cement
In total, 30 porous Ca-P cement implants were created by a CO2 induction technique. 25 The implants were tubular shaped with a diameter of 4.2 mm and length of 5, 10, and 15 mm, respectively. Specifically designed Teflon molds were used to prepare the implants. The implants were made out of Calcibon® (Biomet Merck, Darmstadt, Germany). This cement consists of a mixture of 62.5 wt% α-tricalcium phosphate, 26.8 wt% anhydrous dicalcium phosphate, 8.9 wt% calcium carbonate, and 1.8 wt% hydroxyapatite. The ideal liquid/powder ratio for clinical applications of the cement has been shown to be 0.35 mL/g. 26 To create porosity, NaHCO3 was added to the cement powder. All components (0.5 G of standard powder plus 0.05 g of NaHCO3) were placed into a syringe (Sherwood medical monoject, [St Louis, MO] 2 mL) with aqueous Na2HPO4 (2%). The syringe was closed with an injection plunger and fixed in a mixing apparatus (Silamat®; Vivadent, Schaan, Liechtenstein). After a mixing time of 15 s, the plunger was removed and NaH2PO4 (8%) aqueous solution was added. Thereafter, the syringe was shaken again for 2 s. Finally, the mixed cement was injected immediately into the respective Teflon molds to ensure the standardized shape of the implants. Subsequently, the samples were placed in an oven at 50°C for 1 h.
After cooling, the implants were sandpapered to ensure a standardized size. Subsequently, the specimen was sterilized by autoclaving for 15 min at 121°C.
Surgical procedure
A total of 30 adult female New Zealand white rabbits (2.5–3.5 kg, 6 months of age) were used. National guidelines for the care and use of laboratory animals were respected. The rabbits were divided into three groups: 5, 10, and 15 mm defect groups (porous Ca-P implant and open defect).
Surgery was performed under general inhalation anesthesia. The anesthesia was induced by an intravenous injection of Hypnorm® (0.315 mg/mL fentanyl citrate and 10 mg/mL fluanisone) (Abbeyvet Export, Leeds, United Kingdom) and atropine and was maintained by a mixture of nitrous oxide, isoflurane, and oxygen through a constant volume ventilator. To reduce the perioperative infection risk, antibiotic prophylaxis (Baytril®, 2.5%; KPV Pharma, Kiel, Germany) was given. Preoperatively, all rabbits received Finadyne® (Schering-Plough, Segre, France) 0.02 mg/kg twice a day during 2 days for pain treatment. An extra 40 mL fluid was administered before surgery to prevent dehydration.
After induction of anesthesia, the animals were immobilized in a prone position. In each animal the front legs were shaved and disinfected with povodine–iodine. A 4.5 cm longitudinal skin incision was made at the dorsal part along the radius. After dissecting the muscles, the radius was exposed. The periosteum was partially pushed off and a 5, 10, or 15 mm segmental defect was created in the middiaphyseal part of the radius using a diamond-bladed dental drill with continuous saline cooling.
In all groups, bilateral segmental radial defects of the same size were made in both radii.
The porous Ca-P cement implants were pressed into place, according to a randomization scheme, in the left or right limb and the other limb served as the control group (Fig. 1). After finishing this procedure, the muscle layers and the skin were closed in separate layers with a Vicryl 4.0 suture.

Implantation of the scaffold in the radius.
The rabbits were euthanized at 12 weeks postoperatively for histological and radiological evaluation and for mechanical testing and histological evaluation. Of each experimental group, six of the ulna–radius complexes were harvested for torque testing. The remaining ulna–radius complexes were used directly for histological evaluation. Further, the mechanical specimens were also prepared after application of the torsional load for additional histological analysis.
Radiographic analysis
A mediolateral X-ray of the ulna–radius complex was made immediately after surgery (day 0) and at 2 weeks and 12 weeks postoperatively. The radiographs were made with a Siemens Mobilett (Munich, Germany) X-ray machine. The obtained X-ray images were only used for a subjective description of the bone healing characteristics such as callus formation, quality of union, and bone remodeling in the three different experimental groups.
Mechanical testing (torque test)
After harvesting, the ulna–radius complexes of 18 rabbits (six of each experimental group) were dissected free of all soft tissue. The ulna and the radius were connected to each other because of fibrosis and new bone formation. A dental plaster was used to fix the specimen for mechanical testing (Fig. 2A, B). Therefore, both ends of the forearm were placed in square-shaped molds, which were filled with dental plaster. After setting, these square models fitted precisely in the torque apparatus (Instron, Norwood, MA). Before mechanical testing, two transcortical cuts were made as distal as possible at the lateral ends of the ulna using an oscillating saw. This was done to eliminate the mechanical contribution of the ulna and to isolate the radius during torque testing. Separation of the radius from the ulna was not an option because of ulnar hypertrophy, scar tissue formation, and fibrous fusion. 27 The experimental groups were also compared with 12 nonoperated complete bone samples retrieved from rabbits of the same age.
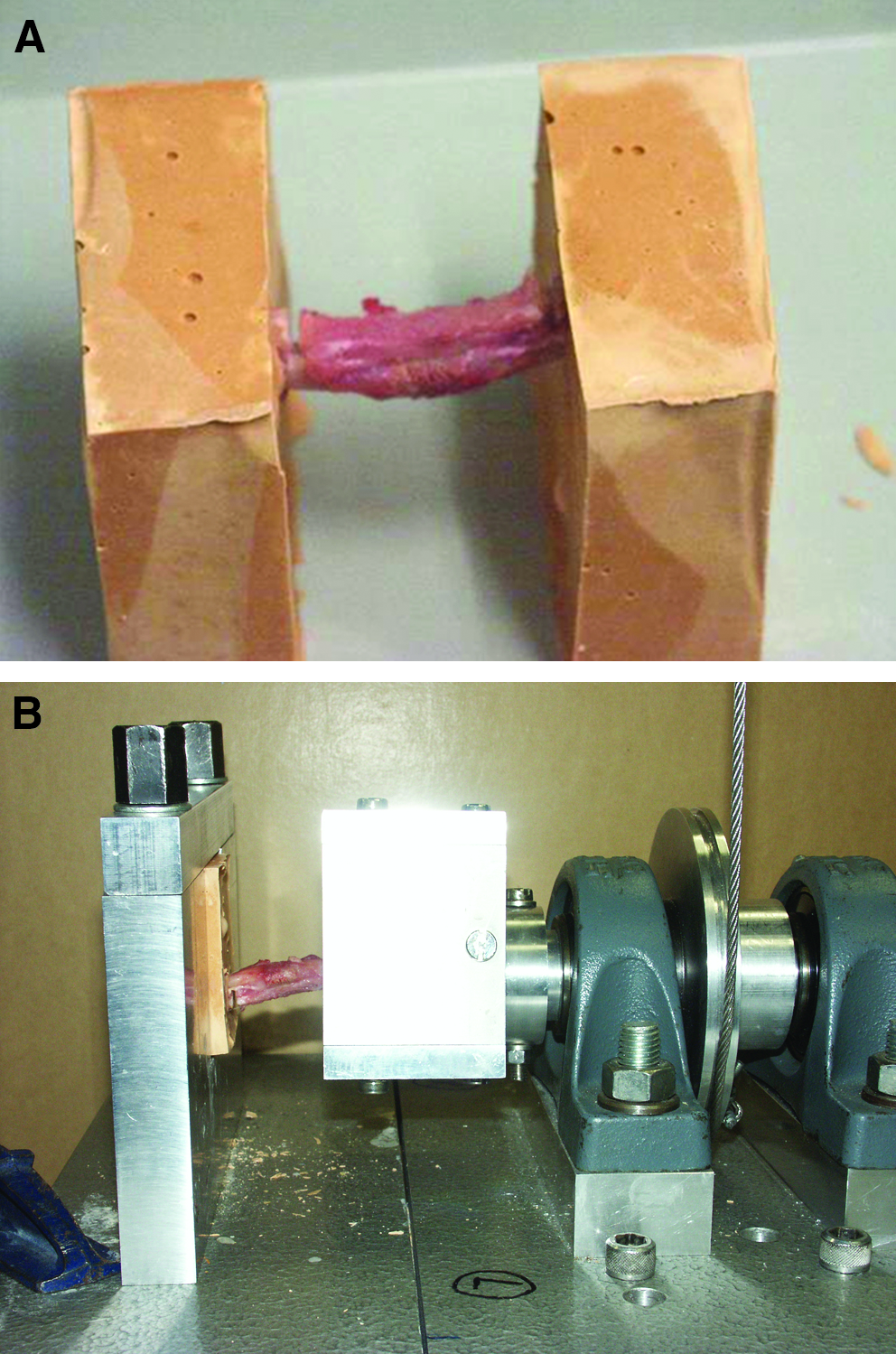
Torque test measurement. (
An Instron® apparatus was used to measure the maximum stress, which could be submitted to the ulna–radius complex (values of ultimate torque/torque at failure) with or without porous Ca-P cement. The torque speed was 5 mm/min. The angular displacement at torque failure could also be extracted from the data. With these measurements, the energy absorbed and the stiffness of the specimens were calculated:
Torque = Force × real distance (N · mm)
Energy = Force × real distance × degree ([N · mm] × degree)
Stiffness = Torque/degree ([N · mm]/degree)
Histological evaluation
All the samples for histological examination (also all the torqued ones) were fixated in 4% phosphate-buffered formalin solution, dehydrated in a graded series of ethanol, and embedded in methyl methacrylate. After polymerization, thin longitudinal sections (10 μm) were prepared (at least three per implant) with a sawing microtome technique. These sections were stained with methylene blue/basic fuchsin and examined with a light microscope for concise histological description (Leica BV, Rijswijk, The Netherlands).
Statistical analysis
All data are reported as means and standard deviations. Measurements from the mechanical testing were statistically evaluated using a paired t-test (GraphPad®, Instat 3.05 Software, San Diego, CA). Differences were considered statistically significant at p-values less than 0.05.
Results
In this study, two of the animals died directly after the surgical procedure (one animal of the 5 mm defect group and one of the 15 mm defect group). The remaining (n = 28) survived the 12 weeks and were able to walk within 3 h after surgery. The rabbits remained in good health, did not lose weight, and did not show any direct wound complication. The total ulna–radius complex could be taken out for further investigation.
Radiographic analysis
The radiographs taken directly after surgery confirmed that all implants were installed correctly. At 2 weeks the X-rays showed a minimal amount of bone healing in all three groups.
After 12 weeks implantation time, the radiographs showed bone bridging over the total length of the defects of all three porous Ca-P cement groups (5, 10, and 15 mm defects) (Fig. 3B). The porous Ca-P cement implants also remained in place according to X-ray examination and were clearly visible in the radius of the rabbit. One of the 15 mm implants showed a fracture line through the implant.

Radiographic analysis of the 15 mm implant after 2 and 12 weeks of implantation: (
In the control group (no implants), all 5 mm defects were closed. In group II (10 mm), 1 out of 10 control defects was still open. In the third group (15 mm), seven out of nine defects appeared to be still open (Fig. 3A2). Results are presented in Table 1. The two 15 mm control defects that were closed showed a thin bone bridge at the ulnar side of the radius.
Ca-P, calcium phosphate.
Mechanical testing (torque test)
Of each experimental group, six ulna–radius complexes were used. In addition, the same test was carried out with an intact bone group as retrieved from rabbits of the same age (n = 12).
During the torque tests, two animals of the 10 mm group and one of each 15 mm group were excluded of this paired test, because of technical failure during the torque test in one of the ulna–radius complexes (fracture of the dental plaster when used for the fixation of the ulna–radius complex or unstable fixation of the ulna–radius complexes in this dental plaster). The ultimate forces and distances were measured and the calculated torque, theta, stiffness, and energy were calculated (Table 2).
Torque, stiffness, and energy were calculated as follows: torque = force × real distance (N · mm); stiffness = torque/degree ([N · mm]/degree); energy = force × real distance × degree ([N · mm] × degree).
SD, standard deviation.
Statistical analysis of the torque measurements using the paired t-test showed that the 5 and 10 mm defects with or without porous Ca-P implants achieved similar values at 12 weeks of implantation (p-value in the 5 mm group [n = 6] was 0.13 [95% confidence interval of difference: −69.3 and 399.2] and p-value in the 10 mm [n = 4] group was 0.71 [95% confidence interval of difference: −472.5 and 365.5]) There was also no statistically significant difference with the retrieved nonoperated bone samples. Further comparison suggested that the torsion data for the 15 mm open defect were lower compared with the filled 15 mm defect as well as the nonoperated specimens (15 mm group [n = 5]: p = 0.11 [95% confidence interval of difference: −499.2 and 73.3]).
Histology
Group I (5 mm)
After 12 weeks, residues of the Ca-P were visible, but not in all the samples. One of the implants showed an old hematoma, without signs of infection. Ingrowth of blood vessels was observed throughout the porosity of the porous Ca-P implants. At the implant–ulna border, new bone formation had occurred, which resulted in fusion between the porous Ca-P implant and the ulnar bone. Also at the original defect border, the newly formed bone was in contact with the porous Ca-P surface. Only occasionally, intervening fibrous tissue was present between the radius defect border and the implant surface. Bone formation had penetrated through all scaffolds, but the amount of bone varied. In the newly formed bone, osteoblasts and osteocytes could be detected.
All empty control defects showed regeneration of the radius and were completely closed with new bone tissue. In addition, fusion of ulnar and new radial bone was seen in almost all samples.
Group II (10 mm)
In 9 out of 10 specimens, bone formation was present in the porous Ca-P implant as characterized by the presence of osteoblasts and osteocytes (Fig. 4A2). However, the amount of bone varied between the various specimens. Bone formation was associated with the ingrowth of blood vessels. An intervening soft tissue layer was present at radial defect border of three samples and no bone ingrowth from this side was observed. Some bone tissue and fibrocartilagenous tissue was interposed between the porous Ca-P implant and ulna. Further examination revealed also that two of the scaffolds showed some displacement out of the defect.
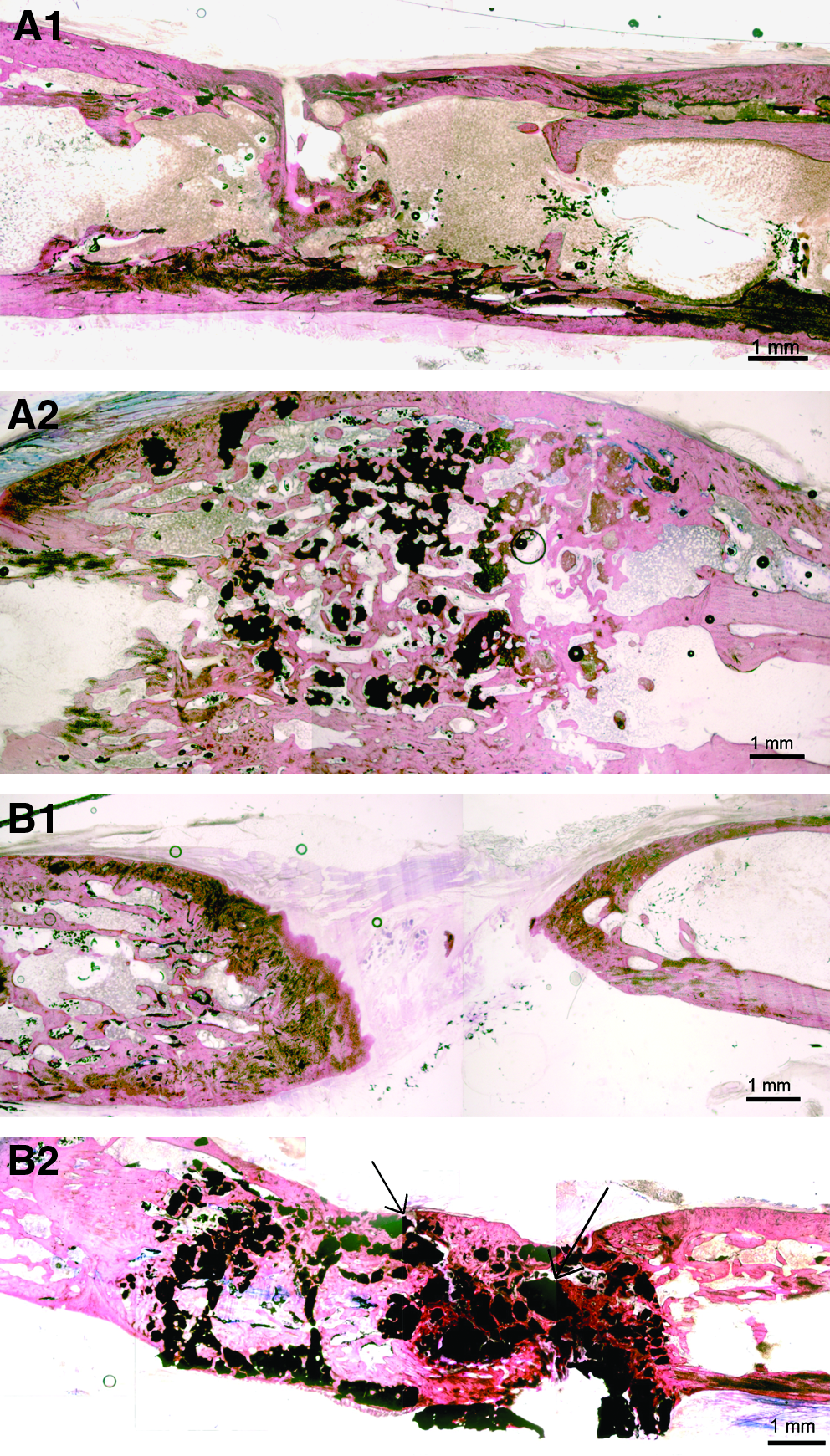
Histology results after 12 weeks implantation time: (
Bone regeneration in the open control defects was similar to the group I defects, but in two of the open control defects there was no bone bridging. The rest of the nonfilled defects (n = 7) were completely closed histologically (Fig. 4A1).
Group III (15 mm)
The porous Ca-P cement implants were still in place after 12 weeks of implantation and all specimens showed bone formation throughout the Ca-P implant porosity (Fig. 4B2). Again, blood vessel ingrowth was observed in these implants. Fibrocartilagenous and limited bone tissue had formed in the area between the porous Ca-P implant and ulna. Further, an intervening soft tissue layer at the implant radial defect border was present in two samples. Although bone was still present in the implant porosity of these implants, ingrowth did not occur from the edges. Two of the implants were found to be displaced and two of them showed fracture lines, without dislocation.
The sections of the empty control defects showed that seven of these defects were still open after 12 weeks. Only in two out of nine, bone bridging was visible histologically, but the formation at the ulnar surface was limited.
Discussion
This study aimed to assess the bone healing supporting characteristics of porous Ca-P cement when implanted in a rabbit segmental defect model as well as to determine the reliability of torque testing as a method to verify bone healing. Bone formation into the cement porosity was seen in all three defect sizes in which implants were inserted. In view of this, the results provide evidence that porous Ca-P cement shows osteoconductive properties. A similar observation was done in a previous study dealing with the regeneration of large-sized cranial defects in rabbits.6,28 In addition, the torque data revealed that the used test approach, that is, without separation of the ulna–radius complex, was not valid to discriminate between Ca-P-filled defects and nonoperated radii.
The torque or torsional test is described as a method to measure the strength of bone and is preferred to evaluate the mechanical properties of bone associated with fracture healing. Therefore, torsional testing is a frequently used technique to evaluate bone healing in long bone segmental defect models, because bone fails in torsion at the weakest point along the shaft.
It has to be emphasized that there are different approaches to perform a torque test. In some studies, separation of the radius or ulna is performed.29,30–33 For example, Cook et al. created 15 mm defects in the ulna of a rabbit, isolated the ulna carefully from the radius, and placed the distal ends in an aluminum sleeve. 30 As the ulna has a curved shape, the ulna had to be mounted eccentrically to keep the axis of the ulnar rotation coaxial with the testing device. 30 The measured average torsional strength and energy absorption of the healed ulna defect was comparable to the intact ulna after 12 weeks' implantation time. Beck et al. created 15 mm segmental defects in the rabbit radius and augmented the defects with a combination of bone marrow and transforming growth factor β1. 29 They isolated the radii using bone rongeurs when the ulna was fused to the operated radius, and thereafter mechanical testing was carried out. 29 They also removed 1 cm of the distal and proximal radius before fixing them into the mechanical testing apparatus. However, it has to be noticed that when the distal bone fragments are removed, the torque results can be influenced because the angle of rotation changes more when the length of the radius is shorter. Also, Mori et al. isolated the radius carefully from the ulna of a rabbit and cut it into a 5-cm-long sample. 32 Subsequently, both ends were fixed in a square mold. 32 In this 24-week study, no statistically significant differences were found between ulnae regenerated by rhBMP-2/PLGA capsules and the intact contralateral bones.
The difficulties that occur when the radius and ulna are separated before mechanical testing are especially evident in the study of Sheller et al., who created noncritical-sized defects in the radii and noncritical-sized defects in the ulnae of New Zealand white rabbits. 31 All ulnae and radii were separated before torsional testing was done. Finally, they observed that 6 out of 16 control bones could not be tested as they either were fractured because of the separation process or had no bridging. When 37.5% of the control samples are lost, as was the case in Sheller's experiment, it might be difficult to draw any conclusion. In addition, bone formation outside the defect site and bone not spanning the defect might be difficult to distinguish during the separation process, which can as well influence the final measurements. In agreement with the aforementioned, it will be clear in this experiment that the separation of the bones would have influenced the test results because histological examination of the samples revealed some bone and also fibrocartilagenous tissue located in the area between the radius and ulna. Also, bone overgrowth (i.e., osseoconduction over the implant surface) is difficult to discern macroscopically. This gives the additional risk of removing too much of the newly formed bone, which results in an unreliable measurement.
Similar to the technique used by Wheeler et al., 18 we potted the ulna–radius complex in dental plaster and made transcortical incisions as close as possible near the embedding of the ulna in the plaster. This was done to eliminate the mechanical contribution of the ulna. Nevertheless, it has to be questioned whether this discontinuous ulna segment has still no effect on the fracture torque or stiffness of the radius, as the 15 mm control defects showed still on average a torque value of 305 N · mm (compared with the 566 N · mm of intact bone specimens) (Fig. 5). This value is rather high, especially when taking into account that the radiographs showed that seven out of the nine 15 mm control defects were open after 12 weeks of implantation. Light microscopy revealed that bone and cartilagenous tissue formation had occurred in the area between the radius and ulna, which undoubtedly has an effect on the measurements. This effect can even become enhanced by additional experimental flaws as related to the used torque approach, such as variability of the transcortical incisions, fracture of the dental plaster, and instability of the fixation.

The ulna–radius complex after creation of the transcortical incisions. The discontinuous ulna segment can affect the torque because of fusion in the area between radius and ulna.
Because of these unavoidable complications of the torsional test, other methods have been suggested to measure the strength of newly formed bone in a segmental defect. An alternative approach is the use of a compression test, but separation of the ulna and radius is required in this method as a load is applied vertically to the specimen along the longitudinal axis of the ulna or radius. Of importance is that, in this test, the angle of the radius and the fixation of the bone in the instrument can influence the measurements. Besides compression, a bending test can be done, but the disadvantages of this method are that (1) there are no equal loads to all sections of the bone and (2) the test is relatively insensitive to specimen length and orientation.15,34,35
Besides the applied mechanical test method, there are a lot of other additional variables that can influence the outcome of mechanical assays. For example, anatomical differences, which cause angular variation between the radius and ulna, can influence the measurements, as well as the inherent strength of a radius will vary from rabbit to rabbit. Also, the mechanical properties of the scaffold material are important, for example, the use of a mechanically strong material will result in less displacement or impression compared with weaker scaffold materials. All these limitations were present in this study and could not be excluded, which can explain the high standard deviation in the measurements as well as the lack of observing any significant effect.
To assess the suitability of porous Ca-P cement as a bone substituting material, this experiment aimed to create various defect sizes in the radius of New Zealand white rabbits. The radiology results showed that two of the 15 mm control defects showed signs of spontaneous closure, which was confirmed by histological analysis. As a consequence, the created 15 mm defect cannot be considered as critical sized. This corroborates with the available literature, as the reported size of a critical defect varies between 15 and 20 mm.18,22,29,36–40 The size of a critical defect is known to depend on the breed and age of the experimental animal model used as well as the location of the defect. Also, the experience and skills of the surgeon and the surgical technique, such as the saline used for cooling, the way of treating the periosteum (whether it is taken away or lifted), and removal or maintenance of the interosseus membrane, are of main importance. For example, Sheller et al. reported that a segmental defect could elicit bone formation from the periosteum of the nearby radius when an ulna defect is created. 31
Considering the histological evaluation, a limitation in the study design was that we were not able to quantify the amount of bone formation and cement degradation. The torqued specimens showed fracturing of the porous Ca-P implants, which prevented the performance of reliable histomorphometrical measurements, and the number of nontorqued specimens was too limited to allow appropriate statistical analysis. In addition, no clear sign of cement degradation was observed in the histological sections, which corroborates with our previous study dealing with rabbit cranial defects. 38 An explanation for this lack of degradation can be the animal model used, as significant degradation of Ca-P cement has been reported in studies with different animal species.25,41
Conclusions
Within the limitation of the study design, porous Ca-P cement implants demonstrated osteoconductive properties and confirmed to be a suitable scaffold material in a weight-bearing situation. Further, the torque testing method used was found to be unreliable for testing the mechanical properties of the healed bone defect.
Footnotes
Acknowledgments
This study was supported by the NWO-AGIKO Foundation. The authors thank E. Bronkhorst for his statistical support and Vincent Cuypers for his histological advice.
Disclosure Statement
No competing financial interests exist.