
Abstract
Closure of diabetic dermal chronic wounds remains a clinical challenge. Implant-assisted healing is emerging as a potential class of therapy for dermal wound closure; this advancement has not been paralleled by the development in complementary diagnostic techniques to objectively monitor the wound-healing process in conjunction with assessing/monitoring of implant efficacy. Biopsies provide the most objective morphological assessments of wound healing; however, they not only perpetuate the wound presence but also increase the risk of infection. A noninvasive and high-resolution imaging technique is highly desirable to provide objective longitudinal diagnosis of implant-assisted wound healing. We investigated the feasibility of deploying optical coherence tomography (OCT) for noninvasive monitoring of the healing of full-thickness excisional dermal wounds implanted with a novel in situ gelable hydrogel composed of N-carboxyethyl chitosan, oxidized dextran, and hyaluronan, in both normal and db/db mice. The results showed that OCT was able to differentiate the morphological differences (e.g., thickness of dermis) between normal and diabetic mice as validated by their corresponding histological evaluations (p < 0.05). OCT could detect essential morphological changes during wound healing, including re-epithelization, inflammatory response, and granulation tissue formation as well as impaired wound repair in diabetic mice. Importantly, by tracking specific morphological changes in hydrogel-assisted wound healing (e.g., implants' degradation and resorption, cell-mediated hydrogel degradation, and accelerated re-epithelization), OCT could also be deployed to monitor and evaluate the transformation of implanted biomaterials, thus holding the promise for noninvasive and objective monitoring of wound healing longitudinally and for objective efficacy assessment of implantable therapeutics in tissue engineering.
Introduction
New optical approaches have recently been applied to enhance in vivo wound imaging, which include digital elliptical measurement to reduce interobserver variation of wound size, 4 spectral imaging in the visible and near-infrared for monitoring of cutaneous edema, 5 orthogonal polarization spectral imaging of the microcirculation of human burn wound, 6 laser Doppler imaging for burn depth assessment, 7 and photoacoustic monitoring of burn. 8 In addition to multiphoton microscopy (e.g., 2-photon fluorescence and second-harmonic generation) that has shown great promise to differentiate cell types and collagen microstructural organization, 9 optical coherence tomography (OCT), including Doppler OCT 10 and polarization-sensitive OCT, 11 may eventually provide noninvasive diagnosis of skin morphology and function at greater depths. OCT is a backscattering-based cross-sectional imaging technique that enables noninvasive optical biopsy for various biological tissues, including skin, at resolutions close to histopathology and over a large field of view (FOV).12,13 Besides, OCT is instantaneous and simple to operate, and requires virtually no sample preparation, thus offering great potential for performing diagnosis over conventional medical imaging techniques such as ultrasound, magnetic resonance imaging, and X-ray computed tomography. Studies performed on human and animal dermal tissues have demonstrated the utility of OCT in delineating cutaneous morphological details (e.g., epidermis, dermis, sweat ducts, and subcutaneous adipose tissue). 14 Our recent study showed the feasibility of OCT in tracking the wound-healing process and tissue regeneration in wound beds implanted with clinically deployed collagen matrices. 15 Nonetheless, these commercially available implants are relatively rigid and lack adhesiveness to attach to wound beds. A conformable in situ gelable hydrogel system readily adhering to tissue and wound bed is clearly advantageous. Although in situ gelable hydrogels have been explored as a class of bioagents to accelerate wound healing, virtually all of them require the utilization of either small molecule crosslinkers or photoinitiators for ultraviolet-induced crosslinking reactions, and these reagents are potentially cytotoxic. We have recently developed a crosslinker-free, noncytotoxic, and bioresorbable N-carboxyethyl chitosan and oxidized dextran composition that is capable of rapid in situ formation of tissue adherent hydrogels, 16 and we performed animal studies to demonstrate its efficacy for wound repair using conventional biopsied histology.17,18 In this investigation, we sought to further validate the utility and identify potential limitations of OCT in monitoring the healing of diabetic dermal wound implanted with an enhanced in situ gelable hydrogel formulation comprised of N-carboxyethyl chitosan, oxidized dextran, and hyaluronan. Accordingly, we performed comparative implant-assisted wound-healing studies on a diabetic mouse model along with its normal/nondiabetic counterparts, and compared these results with nonassisted spontaneous wound healing.
Materials and Methods
Animal model
Male mice (5 weeks old, ∼25 g each) of normal (C57BL/Ks; Jackson Lab, Bar Harbor, ME) and diabetic (B6.Cg-m +/+Leprdb/J, db/db) phenotypes were anesthetized with isoflurane (5% for induction and 2.5% for maintenance). The hair on the dorsal surface of the animals was removed, and full-thickness excisional dermal wounds (∼10 mm in diameter) were surgically created. An in situ gelable hydrogel (∼0.1 mL) composed of partially oxidized dextran (oDext, 1.75% w/v in phosphate-buffered saline [PBS]) and N-carboxyethyl chitosan (CEC, 1.75% w/v in PBS),16,18,19 enhanced by adding 0.5% of hyaluronan (in PBS) (denoted as DCH hydrogel), was deposited in each wound bed. It was previously demonstrated 19 that a comparable hydrogel formulation (i.e., without hyaluronan) was capable of enhancing wound healing in similar animal models. Both normal and db/db mice were divided into two groups, receiving either the hydrogel or PBS as controls, after performing the procedure, each wound bed was sealed by a transparent Tegaderm™ overlay followed by the application of a Band-Aid (fabric, width 1″; J&J, New Brunswick, NJ) to secure the wound site. Sequential two-dimensional (2D) OCT scans across each wound bed were performed in vivo on six animals (three normal and three db/db mice) on day 3 postsurgery; thereafter, the scanned areas were pin-point marked, and digital surface images were captured. The entire wound beds, including the intact dermis adjoining the wounds, were excised, fixed in 10% formalin, embedded in paraffin, and sectioned under the guidance of the pin-point marks, and surface images to ensure histological sectioning to be performed were in proximity to the previously captured OCT scans. The specimens prepared were hematoxylin and eosin (H&E) stained for histological evaluations and correlated with the corresponding 2D OCT images. Likewise, the same procedures were performed on days 5, 7, 10, and 14, respectively, followed by tissue specimen collection.
OCT imaging
A handheld spectral-domain OCT system, used to perform all the imaging studies presented herewith, was illustrated in Figure 1 in which a fiberoptic Michelson interferometer was illuminated with a ∼12 mW pigtailed broadband light source. The central wavelength was at 1310 nm, and the spectral bandwidth was ∼90 nm, yielding a coherence length of Lc = 8.5 μm that determined the axial resolution of OCT. A 3 × 2 fiber coupler split the 1310 nm light equally into reference and sample arms for OCT imaging and concurrently introduced a green laser light (530 nm) for visual guidance. While the reference arm was connected to a stationary mirror to match the optical path lengths, the sample arm was connected to a bench-top stereoscope in which light exiting the fiber was collimated to ϕ5 mm, scanned laterally by a servo mirror, and focused by an f = 40 mm achromatic lens onto the mouse skin surface under examination. The light returning from the sample and the reference arms was recombined in the detection arm and connected to a spectral radar in which it was collimated by a fiberoptic achromat (f = 55 mm), diffracted by a holographic grating (d = 1200 mm−1), and then focused onto a 1D InGaAs array (1024-pixel, pixel size: 25 μm), which detected the spectrograph (over ∼110 nm) at a spectral resolution of Δλ ≈0.11 nm. Each spectrograph was digitized by a two-channel 12-bit A/D at 5 MHz, and processed (e.g., fast Fourier transform (FFT)) by a computer to convert to a depth-resolved backscattering profile (A-scan) of the tissue; sequential transverse scans of the sample beam were synchronized after acquisition of each spectrograph so that a 2D spectral-domain OCT image could be reconstructed and displayed at ∼8 fps, covering a FOV of 6 × 2.9 mm2 in the lateral and axial directions. The measured axial and lateral resolutions were 8.9 and 12 μm, respectively, and the system dynamic range was ∼111 dB. As the wound bed (∼ϕ10 mm) was wider than the FOV of an OCT image (6 mm), multiple scans were performed and later digitally fused to collectively cover the wound bed and the adjunct transitional area with intact normal skin. As OCT measured the pathlength-resolved backscattering in skin or wound bed, the refractive indices of 1.34 for implants and of 1.40 for cutaneous tissue 20 were assumed to transform the measured original images to the depth-resolved 2D OCT images.
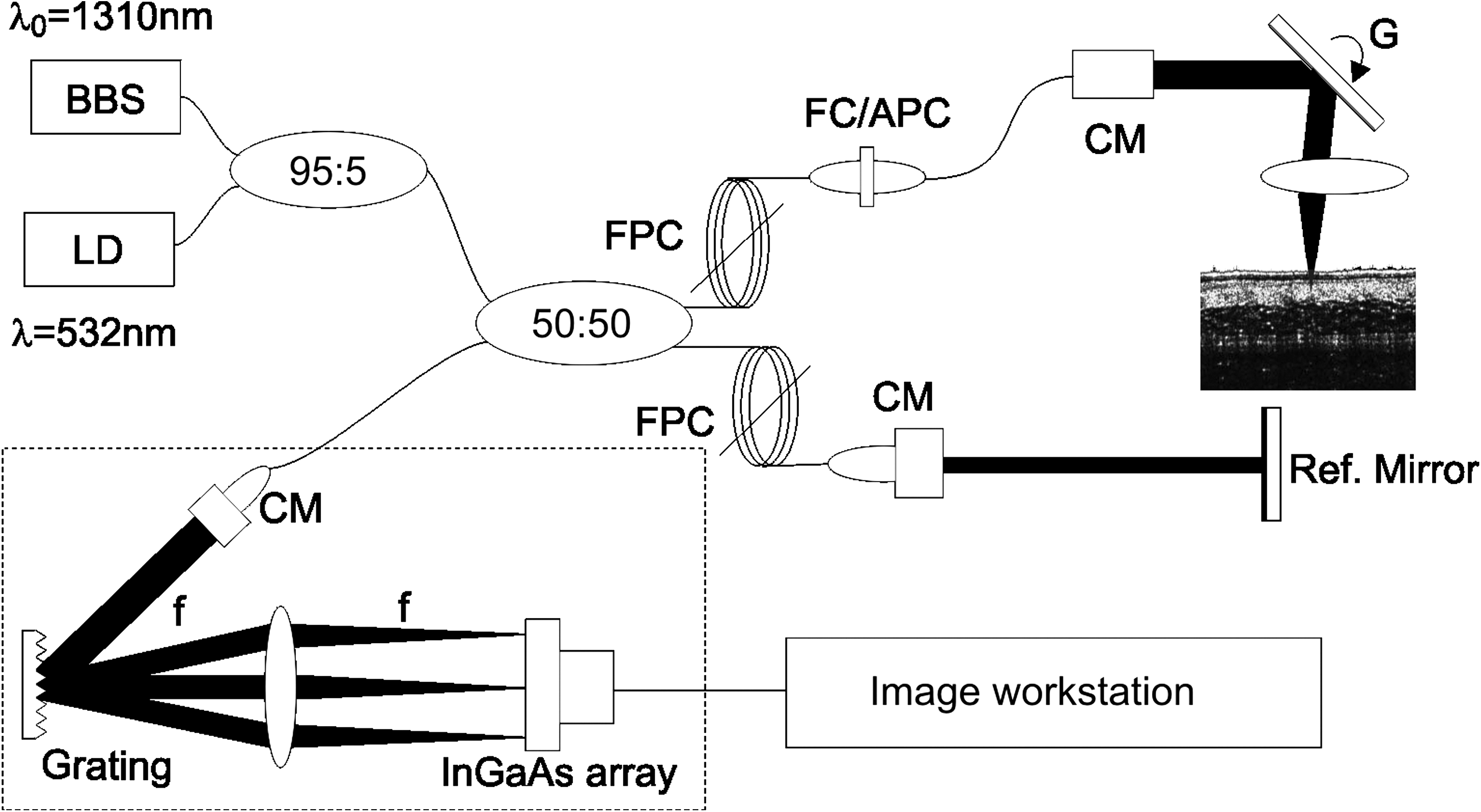
Schematic diagram of the spectral radar–based spectral-domain optical coherence tomography (OCT) system. BBS, broadband source (λ0 = 1310 nm, ΔλFWHM = 90 nm, p = 12 mW); LD, aiming laser diode (λ = 532 nm); CM, fiberoptic collimator; FPC, fiber polarization controller; G, servo mirror; FC/APC, angled fiber connector. System provides an field of view of 6 × 2.2 mm2 per scan with spatial resolutions of 8.9 μm axially and 12 μm laterally.
Histological analysis
The H&E-stained histological slides of the dissected wound beds were photographed under a Nikon, Melville, NY, E800 light microscope (4 × Obj) and digitally assembled to compare with the corresponding cross-sectional OCT images to validate the specific morphological transformation during dermal wound repair. In addition, higher magnification images (20 × Obj) were also captured to further examine the details in the regions of interest.
Results
A total of 30 mice (15 normal and 15 db/db mice) were evaluated at five time points (days 3, 5, 7, 10, and 14) postimplantation. All OCT images were presented in pseudo color to enhance observation, where the bright-to-dark look-up table reflected the magnitudes of backscattering (high to low) from different components of the intact cutaneous tissue and the wound bed. OCT identification of morphological components (e.g., epidermis, dermis, adipose tissue, and granulation) was based primarily on their backscattering characteristics.
Monitoring of unintervened wound beds (control group)
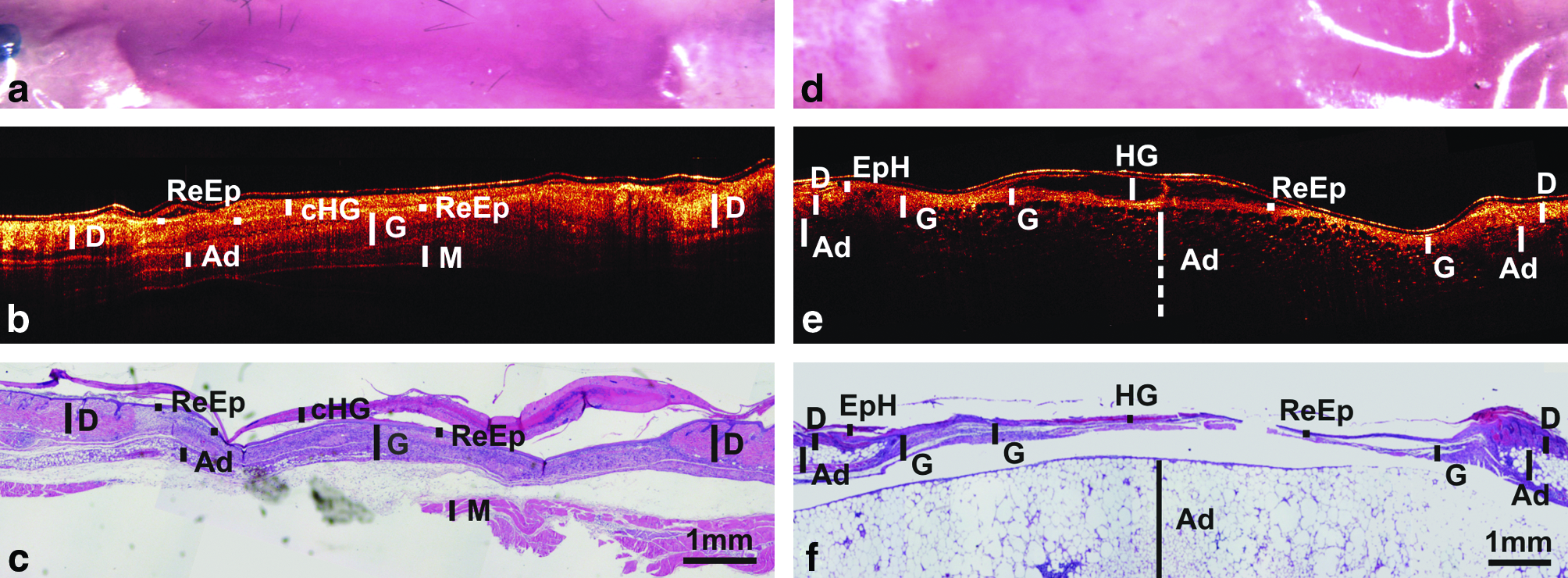
Figure 2 shows the results on day 7 postimplant for both normal (Fig. 2a–c) and db/db (Fig. 2d–f) mice. An initial overall comparison revealed strong correlations between OCT and histological images. Evidently, OCT delineated important dermal structures in accordance with their distinct backscattering patterns. For instance, in normal mice, OCT was able to differentiate the high-scattering thinner epidermis (E) from the thicker dermis (D); in addition, hair follicles appeared as dark and mostly vertical streaks strewn along the dermis of the normal skin. In the wound bed where the high-scattering layers (e.g., E and D) of skin were removed, the effective imaging depth of OCT was greatly enhanced, and it was able to reveal the deeper muscle layer (M). Compared to their normal counterparts, interesting morphological differences of the wound beds of db/db mice were delineated in the OCT images. For instance, due to the considerably thinner dermis in db/db mice, OCT was able to detect the loose and pore-like adipocytes (Ad) underlying the dermis, and this observation was confirmed by histological analyses. Likewise, OCT could be utilized to quantify the thickness of the dermis in both normal and diabetic mice (dnr and ddb); the OCT measurements, dnr = 525 ± 58 μm and ddb = 263 ± 25 μm, closely matched those derived from histological evaluations (i.e., dnr = 505 ± 26 μm and ddb =264 ± 17 μm). For db/db wounds, surface image was unable to provide definitive measures of the wound sizes (8–13 mm), but the OCT measurement (9.6 mm) strongly correlated with the histology (9.7 mm). A thorough comparison with histology revealed that OCT was able to differentiate early stage morphological transformations during wound healing. As indicated in Figure 2b and e, OCT was able to identify the critical structural changes typically manifested, including re-epithelization (ReEp) as a high-scattering thin layer, early stage epidermal hyperplasia (EpH) as lower-scattering thicker epidermis, and infection or inflammatory response (Infl) and connective tissue (C, mostly collagens) as high-scattering components leading to decreased imaging depth. A significant change during this stage manifesting wound healing was granulation tissue (G) formation. Evidently, the granulation tissues of normal animals showed higher scattering in the OCT images as compared to their db/db counterparts, which was corroborated by histological examination attributable to the abundance of collagen in granulation tissue. In addition, a comparison between histology and OCT with the general gross-structural guidance of the surface image revealed that the latter provided important complementary structural information for deducing the morphophysiological transformation of the wound beds during their healing, even though surface images, per se, typically do not provide any meaningful depth information. For instance, the inflammatory response, an integral initial component of wound repair, appeared as white, while granulation tissues were epitomized by a characteristic pinkish color due to blood vessel formation. The measured percentage of granulation tissue coverage over the wound bed was ∼43%, which was slightly greater than that of histology (∼38%), but this difference could likely be attributable to the artifacts of histological processing, for example, some structures fell off in Figure 2f.
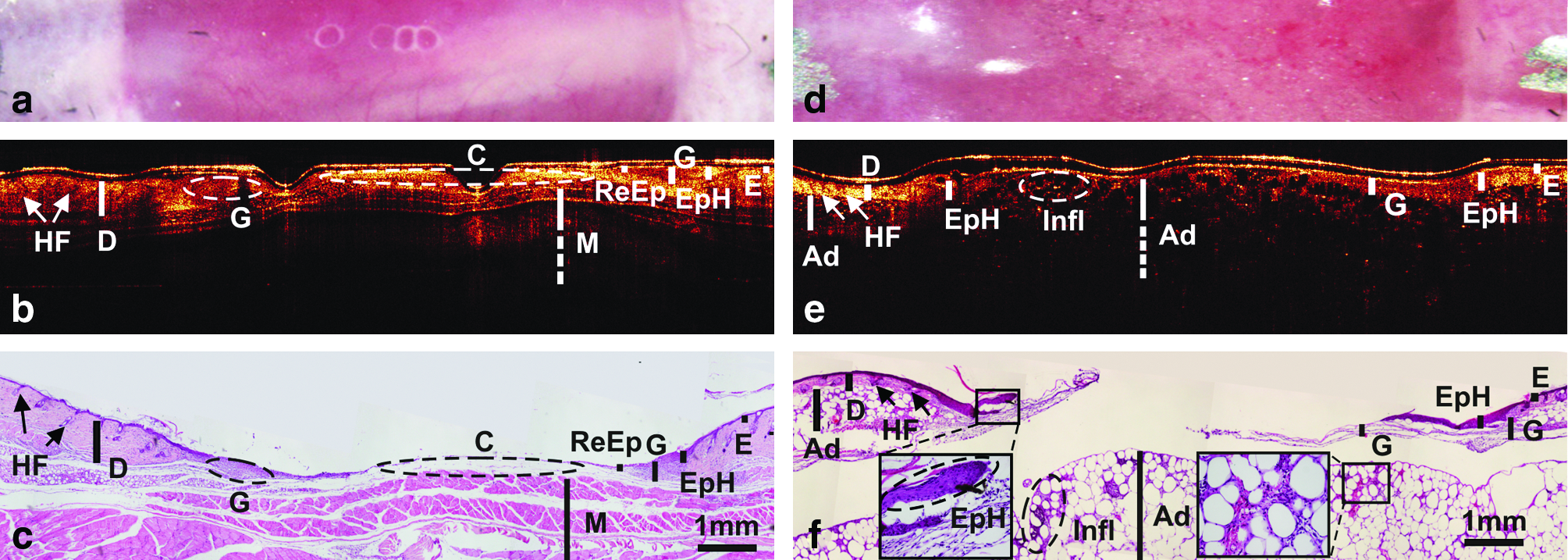
Surface, cross-sectional OCT images, and histological sections of unintervened wound beds at day 7 for normal (
Figure 3 shows two typical wound beds at a late stage of healing (day 14 postsurgery). Apparently, the wound beds of both normal (Fig. 3a–c) and db/db (Fig. 3d–f) mice were healed as evidenced by wound bed contraction. Moreover, the newly formed tissue inside the healed wound bed (Fig. 3e) had begun remodeling (e.g., G) where collagen, deposited as an integral component of granulation tissue, was being transformed and realigned along tension lines. Conversely, the OCT images of the wound beds of normal mice (e.g., Fig. 3b) showed the presence of a uniformly low-scattering area (extracellular matrix [ECM]) with a distinctive boundary adjoining the dermal tissues (D), suggesting a more advanced stage of wound bed remodeling and thus healing; this observation was corroborated by the parallel histological analyses. In comparison, the residual wound bed of the db/db mice (e.g., Fig. 3e) appeared more heterogeneous with several embedded blisters, and its boundary was less clearly defined, suggesting an impaired or delayed wound recovery. These results revealed that compared to conventional surface visual inspection, OCT was able to provide high-resolution cross-sectional images with significant depth information to differentiate various morphological features of the wound beds and their resorption with both precise quantitative and qualitative details between normal and db/db animals. As the stages of wound healing are defined by their characteristic continual morphological transformation on the dermal architectural features, the results presented here validated the utility of OCT in monitoring the wound-healing process, including unequivocal differentiation and tracking of the transformations of morphologically distinct wound beds in both normal and db/db mice. In both cases, OCT and histology revealed 100% wound closure, whereas surface images were not specific about wound sizes (e.g., 3–7 mm for db/db, ∼4 mm for control). In the db/db mouse, the OCT-measured thickness of the granulation tissue (∼430 μm) matched that of histology (∼430 μm); in the normal mouse, the ECM thickness by OCT (∼650 μm) was also close to that of histology (∼620 μm).
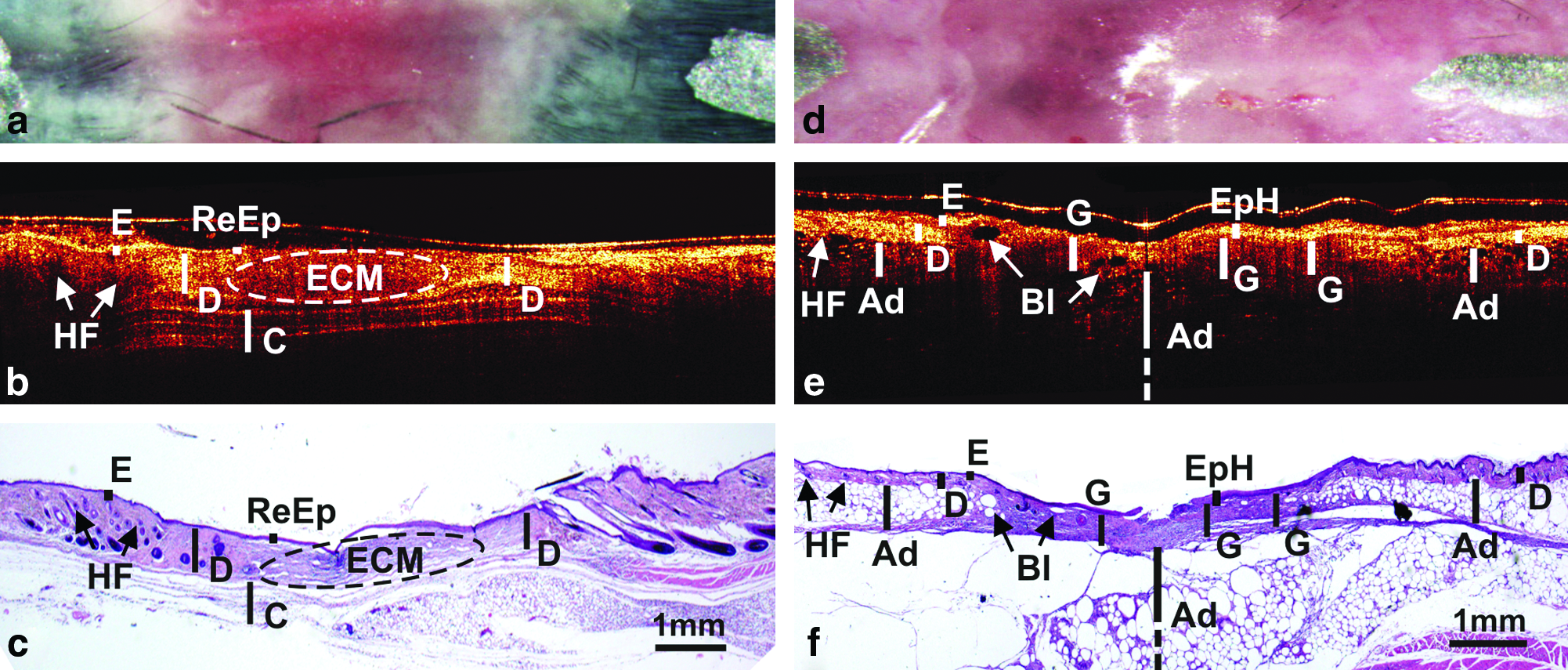
Surface, cross-sectional OCT images, and histological sections of unintervened wound beds at day 14 for normal (
Monitoring of hydrogel implant–assisted wound healing
To further evaluate the utility of OCT in noninvasive monitoring of the efficacy of biomaterial implant–assisted wound healing, we performed longitudinal OCT imaging on the morphophysiological transformations of wound beds implanted with DCH hydrogels and validated the results with their corresponding histological evaluations at different time points postsurgery (days 3, 5, 7, 10, and 14).
Figure 4 depicts the typical wound beds of both normal (Fig. 4a–c) and db/db (Fig. 4d–f) animals 3 days after implantation. Consistent with the results of the control group presented above, OCT was able to exploit the differential backscattering features of various components of the dermal tissues to distinguish their morphological compositions. The structures identified by OCT include fibrous exudates (F), epidermis (E), dermis (D), hair follicle (HF), muscle (M), and adipose tissue (Ad). Further, the DCH hydrogel (HG), discernible as an optically homogeneous and translucent bulk material residing inside the wound bed, was clearly visible. Figure 4a–c depicts the presence of a DCH hydrogel residing in the wound bed of a normal mouse, and it was largely comparable to that of implanted in the wound bed of a db/db mouse as shown in Figure 4d–f, despite the expected discrepancy in their sizes and shapes. The DCH hydrogel was optically transparent and did not interfere with OCT propagation; thus, the structural features of the tissues underneath the hydrogel and those developed over it were clearly visible. Importantly, as indicated in the images, OCT detected the aggregation of inflammatory cells (Infl), appeared as relatively high-scattering clusters, in both normal and db/db animals. As expected, this inflammatory response appeared to be considerably more intense in normal animals as compared to their db/db counterparts, which could implicate a delayed inflammatory response of the latter. OCT was able to discern re-epithelization as a low-scattering thin layer, occurring on top of the inflammatory stratum in the wound bed of the db/db mice. Moreover, as OCT was able to detect the decreasing ReEp thickness it migrated toward the center of the wound bed, and the result revealed that initiation of re-epithelization emerged at the tissue (e.g., epithelial hyperplasia) adjoining the DCH hydrogel implant and progressing toward the interior, suggesting that the DCH hydrogel was at least amenable if not conducive to epithelial growth. OCT was able to identify 52% ReEp coverage of the wound bed in db/db mouse, which was higher than that of histology (41%); however, some parts of the tissue specimen appeared to have detached (as indicated by the abrupt transition) during histological processing. The total wound bed measured by surface imaging (8.4 mm) and OCT (8.2 mm) matched well with histology (8.1 mm).
Surface, cross-sectional OCT images, and histological sections of hydrogel implant–assisted wound beds at day 3 for normal (
Figure 5 depicts the typical wound beds on day 5 postsurgery. The surface images (Fig. 5a, d) of both wound beds appeared to be almost uniform and not yielding meaningful diagnostic information. OCT was able to reveal considerable details of the morphophysiologcal transformation occurred in the wound beds of both normal (Fig. 5b) and db/db (Fig. 5e) animals as compared to those on day 3 (i.e., Fig. 4). The DCH hydrogels in the wound beds of both normal (Fig. 5b) and db/db (Fig. 5e) mice appeared to have degraded noticeably. The residual hydrogel (e.g., cell-infiltrated hydrogel implant [cHG]) implanted in normal mice showed higher scattering than those (e.g., HG) implanted into db/db mice; histological examination at higher magnifications revealed the presence of cells residing inside the DCH hydrogel, contributing to the increased scattering. There was also detectable increase of backscattering inside the partially degraded hydrogel implanted into the wound beds in db/db mice, which could be indicative of cell infiltration (presumably inflammatory cells) into the hydrogel, leading to its partial degradation along the tissue–hydrogel interface. Moreover, the wound bed of the normal mouse (Fig. 5b) had evidently been fully re-epithelialized, and this was manifested as a higher scattering stratum. As delineated by OCT, the relatively thick and high-scattering stratum situated directly underneath the ReEp layer covering the entire wound bed was the granulation tissue (G). Conversely, both the ReEp layer and G strata of the db/db mice (Fig. 5e) were thinner than those observed in the normal controls (Fig. 5b) and only partially covered the wound bed. Collectively, the results derived from OCT were corroborated by the corresponding histological assessments. For instance, the measured thicknesses of G strata were ∼270 μm for db/db and ∼452 μm for control, which matched well with those of histology (i.e., ∼287 and ∼490 μm). It is noteworthy that granulation tissue formation is an integral element of wound healing involving inflammatory cell infiltration, ECM formation, and revascularization; these dynamic processes could likely alter the optical properties of individual components of the wound bed; thus, monitoring the evolution of the optical properties (i.e., scattering patterns) could be employed as a surrogate indicator to track the morphophysiological transformation of wound beds during the healing process. Histology is not only destructive to the specimens but also prone to inevitable distortion during specimen processing; these issues are epitomized by artifacts, including gaps, and detachment of hydrogel fragments appeared on the histological specimens. In contrast, OCT is capable of nondestructive delineation of the structures of a wound bed longitudinally and is completely free from distortion. This underscores the advantages of real-time noninvasive OCT imaging in providing reliable and unequivocal diagnosis.
Surface, cross-sectional OCT images, and histological sections of hydrogel implant–assisted wound beds at day 5 for normal (
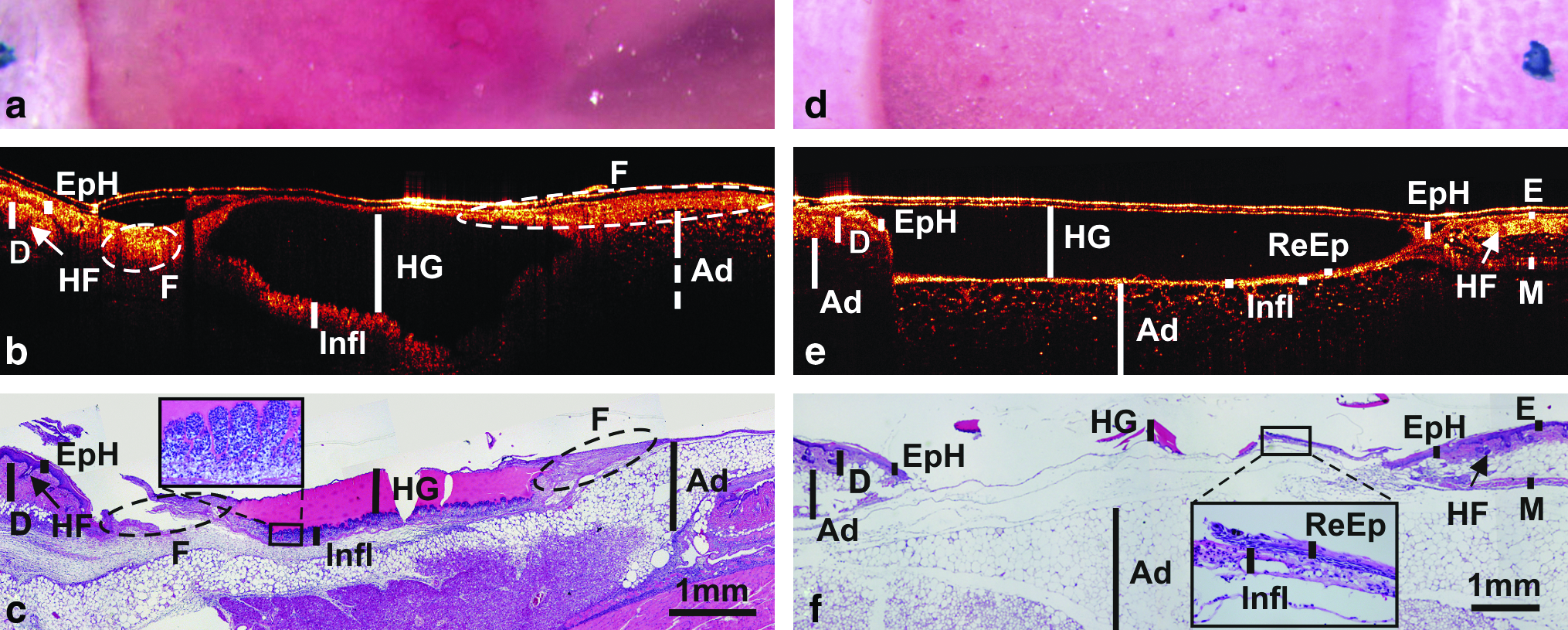
Figure 6 depicts the wound beds of normal (Fig. 6a–c) and db/db (Fig. 6d–f) mice 7 days postsurgery. The wound beds of both animals had begun contraction, implying the progress of the healing process. Comparisons between OCT images and their corresponding histological sections demonstrated the unique utility of OCT to unequivocally track the presence of the hydrogel in the wound bed and additionally to discern the morphophysiological transformation of the healing wound covered by the hydrogel implant. Specifically, OCT both detected and differentiated the presence of the degrading DCH hydrogel implant (e.g., cHG) and wound enclosure or contraction in normal animal (Fig. 6b). However, the high scattering in cHG compromised the imaging depth of OCT to identify the underlying structures such as the granulation tissue (G). On contrary, a considerable portion of the implanted hydrogel, with a thickness of up to ∼1.5 mm, remained in the wound bed of the db/db mouse (Fig. 6e). This could be due to initial deposition of excess hydrogel precursor during the surgical procedure. Clear indications of granulation tissue (G) and connective tissue (C) formations and ReEp were observed in the wound beds of the db/db mice; these were confirmed by the histological image (Fig. 6f). OCT (Fig. 6e) measured 100% Infl and 31% ReEp coverage of the wound bed, but artifacts (tissue falling off ) prevented histology (Fig. 6f) to provide accurate validations. Additionally, the presence of some exceedingly high-scattering areas in the OCT images, extending from the edge of the wound bed to areas beyond Tegaderm coverage due to dehydrated DCH (DH) or regrown hair (H), clearly attenuated the penetration depth, thereby compromising the capability of OCT in resolving the morphological details of these areas. Histological analyses of these highly scattering regions (e.g., DH) revealed the presence of partially dehydrated hydrogels that considerably increased its optical density and thus random scattering.

Surface, cross-sectional OCT images, and histological sections of hydrogel implant–assisted wound beds at day 7 for normal (
Figure 7 depicts the wound beds 10 days postsurgery. Apparently, the wound bed of the normal mouse (Fig. 7b) had completely healed and was undergoing remodeling; this was exemplified by the presence of lower-scattering loose connective tissue (ECM) and the emerging dermis (D) on both sides due to wound contraction, whereas the surface imaging for wound size identification was nonspecific (e.g., ∼5.5 mm for db/db and ∼6 mm for control). For the db/db animal (Fig. 7e), the OCT image showed that the DCH hydrogel implanted had mostly degraded and been replaced by rigorous granulation tissue (G), ReEp with signs of wound contraction occurring, indicative of a progressing healing process toward completion. The measured thickness of G strata by OCT (∼560 μm) for db/db mouse matched well with that of histology (i.e., ∼556 μm). A portion of the implanted hydrogel, apparently oozed out of the wound bed during the original application and covered by the edge of the Tegaderm dressing, was dehydrated forming a layer of highly scattering debris (DH), thereby reducing the effective penetration depth of OCT to image the underneath structures.

Surface, cross-sectional OCT images, and histological sections of hydrogel implant-assisted wound beds at day 10 for normal (
Discussion
DM is frequently associated with impaired wound healing such as DFU, which can substantially affect the life quality of diabetic patients. A reliable and accurate diagnostic method for monitoring the morphophysiological changes within the wound bed is critical for devising new treatment for chronic wounds. Current diagnosis is mostly based on en face visual inspection, which lacks depth information, and the assessment is known to be ambiguous and subjective. While other imaging techniques, such as ultrasound, computed tomography, and magnetic resonance imaging, can produce 2D or three-dimensional (3D) cross-sectional images, the level of resolution is not sufficient to detect detailed morphological changes. Therefore, a high-resolution subsurface imaging technique capable of producing tomographic information is highly desirable. Interestingly, several new optical imaging techniques have been applied to enhance noninvasive skin imaging and wound (e.g., burn) assessment. For instance, a simple spectral imaging technique was able to detect subsurface cutaneous edema 5 and even the microcirculation of the human burn wound 6 by employing additional orthogonal polarization optics to reduce surface reflection. More advanced approaches such as laser Doppler and photoacoustic techniques7,8 showed great promise of enhanced monitoring of burn wounds, for example, burn depth and local hemodynamics in the healing process. Confocal and multiphoton microscopy may provide more specific imaging identifications of important wound-healing features such as distinct differentiation of early ReEp and the resportion of granular tissue, ECM to dermal strata based on their collagen types, contents, and microstructural organizations. Complementary to these promising optical imaging techniques, OCT is an enabling noninvasive optical imaging approach that can provide 3D cross-sectional images at sub 10-μm resolution and 1–2 mm imaging depth without focal tracking, which is highly suitable for in vivo noncontact cutaneous wound monitoring. As for intact skin, the useful imaging depth was limited to ∼0.5 mm because of the high scattering of both the epidermis and dermis. The results of our previous study revealed that when the epidermis and dermis were both removed, the imaging depth increased drastically to 1.5–2 mm. The intermediate imaging depth and noninvasive and instantaneous longitudinal imaging capability render OCT a potentially very useful imaging tool in many clinical applications.
Here we further investigated the utilities and identified the limitations of OCT by conducting two parallel and sequential studies on comparing hydrogel implant–assisted and nonassisted wound healing in diabetic and normal animals, respectively. All OCT images of both diabetic and normal animal correlated well with their corresponding histological counterparts. The readily resolvable morphologies include epidermis, dermis, hair follicle, and adipose tissue. Because of its high resolution, OCT was able to quantify the thickness of the dermis as well as differentiate individual adipocytes in diabetic animals. Presence of excessive and large adipocytes and thinner dermis are two of the most characteristic attributes of the dermal tissue of diabetic mice; OCT was clearly able to discern these two distinctive features. More importantly, OCT was able to resolve the essential morphological changes during wound healing, such as ReEp, inflammatory response, granulation tissue formation, wound bed contraction, and remodeling, in both diabetic and normal animals. In addition, OCT could detect blisters and other structural imperfections by differentiating the backscattering intensity and heterogeneity of the regenerated tissues (e.g., Figs. 3 and 4), and confirm the impaired or delayed wound healing in diabetic mice. All these results suggest that OCT can potentially be deployed clinically as an in vivo diagnostic tool to facilitate wound care. Our next study will examine the utility of OCT in monitoring assisted wound repair in porcine models (close human homolog) to tack ReEp, 21 granulation tissue formation, wound bed contraction, and remodeling.
Tissue regeneration techniques, including biomaterial scaffold implants aimed to accelerate wound healing, are still emerging as treatments for chronic wounds. The results of our first study conducted on the wound beds of normal mice implanted with collagen matrices 20 showed that OCT could be deployed to evaluate and monitor implant-assisted wound healing by tracking the resorption of the collagen implant as well as its interaction with the wound bed. Moreover, in a parallel study by conventional biopsied histology assessment, we showed the efficacy of an in situ gelable hydrogel (formulated from oxidized dextran and N-carboxylethyl chitosan) in accelerating wound healing in normal mouse models. 19 Based on these findings, in this investigation, we expanded the scope to show the feasibility of deploying OCT to monitor the wound healing of diabetic mouse models implanted with an improved hydrogel formulation (composed of oxidized dextran, N-carboxylethyl chitosan, and hyaluronan, i.e., DCH hydrogel); thus, the overall objective is incremental of the previous two investigations. The primary interests were to validate the in vivo efficacy of our novel in situ gelable DCH hydrogel in enhancing wound healing in both diabetic and normal mice, in conjunction with validating OCT's capability for monitoring DCH hydrogel-assisted wound healing. Other than the capacity of discriminating wound beds of diabetic and normal subjects, OCT could clearly differentiate the structural details of wound beds from the implanted hydrogels and monitoring the latter's biodegradation. OCT retained high spatial resolution with extended imaging depth to penetrate the relatively thick implants, thereby enabled monitoring of the morphological transformations occurring underneath the hydrogel. For instance, OCT was able to discern inflammatory cell aggregation within the wound bed and epidermal hyperplasia on the adjacent intact skin in both diabetic and normal animals (Fig. 3). Importantly, the development of granulation tissue, a crucial component for gauging the extent of wound repair, could be clearly tracked on normal as well as diabetic subjects. Histology remains the clinical standard for unequivocal diagnosis; however, it is compromised by some inevitable drawbacks. First, histological artifacts such as folding and facture frequently found in processed specimens could obscure objective assessments. This is exemplified by the abundance of adipocytes in the dermal tissues of db/db mice causing the fragility of histological sections, thereby frequent specimen fractures. Second, our experience has shown that due to the differential shrinkage of the implants and tissues during the initial steps of histological processing, the former could easily fracture and detach from the tissues, which adversely affected the objective evaluation of wound healing. It could also be inferred that this is commonly encountered in comparable materials designed for implantation. More importantly, conventional biopsy is highly invasive and inevitably inflicts further damages to the wound bed, thus compromising wound closure. As a noncontact and noninvasive imaging approach, OCT circumvents these complications. A highly clinically relevant finding in Figure 6 was that accumulation of a large numbers of inflammatory cells was readily identified by OCT due to the enhanced scattering of these cells, and this observation was in fact confirmed by histology. Inflammatory cells (e.g., macrophages) are smaller in size (i.e., with smaller cytoplasmic volume) and thus tend to be of higher backscattering according to our previous study characterizing OCT contrast. Our future study will include quantitative analysis of backscattering increase pertaining to cell migration and accumulation in translucent hydrogel as a precursor for early wound repair as well as detection of infection (i.e., excessive accumulation inflammatory cells).
As a backscattering based optical imaging technique, both the contrast and resolution of OCT image could be compromised by nonspecific identifications caused by backscattering changes of tissue and wound bed as well as light attenuation including those induced by surface roughness. For instance, both ReEp and granulation tissue are highly scattering, it could interfere with OCT's capability to fully differentiate them during wound healing when they are being developed adjacent to each other and morphing simultaneously. Nevertheless, this intricate shortcoming could largely be compensated by correlating several known and well-characterized general pathophysiologic parameters, including the thickness of the epidermal tissues being regenerated (i.e., ReEp), the scattering properties of granulation tissues being formed, depths/locations of characteristic tissues, and the differential architectures of adjacent tissues. The distinct dimensions and proximities of these parameters could be utilized to assist the interpretation of OCT images. Recent technological advances in OCT, for example, polarization-sensitive OCT, 11 have enabled more specific complementary diagnosis potentially very useful for enhancing the assessment of wound repair. For instance, recent technological advances in Doppler OCT have dramatically enhanced the sensitivity and resolution to image minute subsurface blood flows in 2D and even 3D,22–24 thus rendering it a promising technique to detect neo-vascularization, which is a crucial physiological parameter for wound repair. Polarization-sensitive OCT can provide better identification of collagen or other fibrous tissue components. 20 Future coupling of these complementary but related optical techniques could result in diminishing the current shortcomings of the OCT technique being utilized to perform this study; the combined system will essentially obviate the need to employ the anatomical proximities of individual components of dermal structures in assisting resolution of the tissues being regenerated. More importantly, the emerging ultrahigh-resolution OCT (uOCT) 25 offers the potential to further enhance tissue differentiation at a resolution down to cellular level to enable more accurate and objective diagnosis and evaluation. Figure 8 shows our current capability of 3D uOCT for subcellular imaging of living mouse skin in which EpD, D, hair follicles, glands, and dermal of cells (the dark spots were likely the nuclei of cells) were readily resolved and correlated well with their corresponding H&E histology (40 ×, 0.65NA (numerical aperture)).
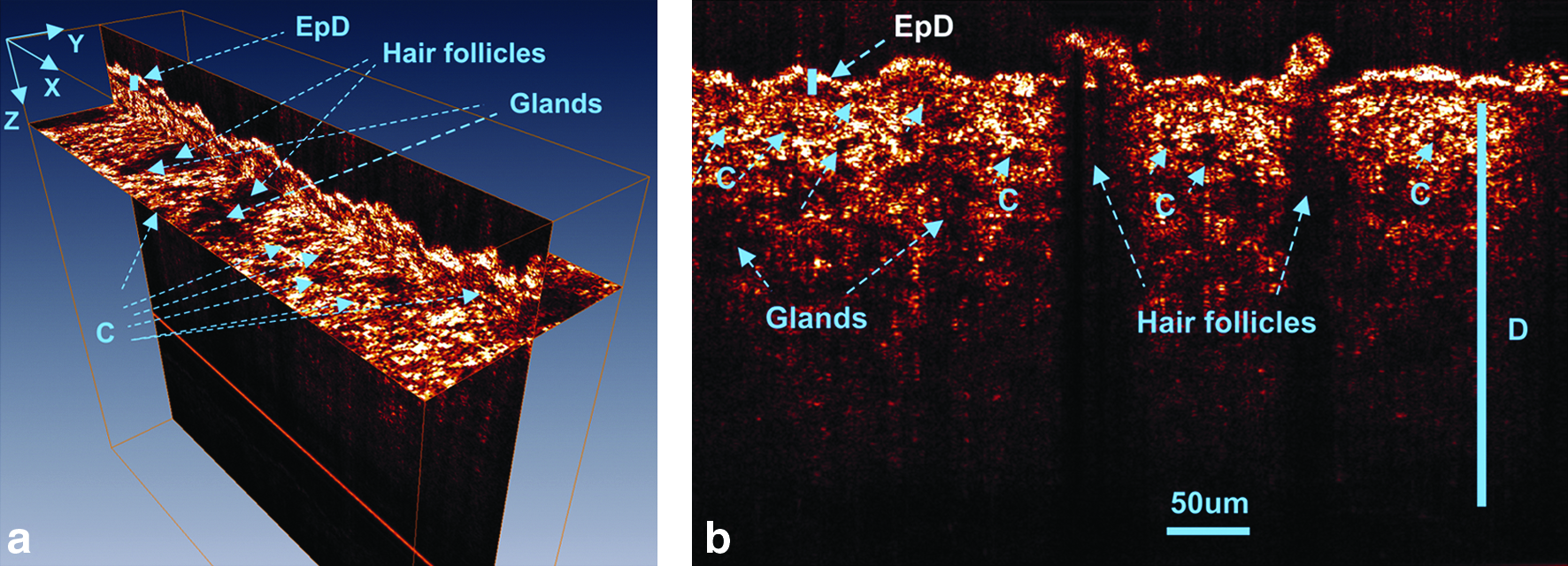
Ultrahigh-resolution OCT images of mouse skin in vivo. (
Conclusions
In summary, OCT, as an enabling noninvasive instantaneous imaging technique, has the unique capability to image subsurface morphological changes during the dermal wound-healing process at ∼10 μm resolution and up to 2 mm imaging depth in both normal and diabetic mice. Further, OCT can detect essential morphological changes during wound healing, such as ReEp, granulation tissue formation, and inflammatory response in addition to resolving morphological structures such as epidermis, dermis, hair follicle, and adipose tissue. For instance, OCT can differentiate the dermal tissue components of diabetic mice from normal mice based on their structural features (e.g., thinner dermis and characteristics of adipocytes). OCT also detects impaired wound healing in diabetic mice. More importantly, by imaging specific morphological changes in the hydrogel-assisted wound healing, such as implants degradation and resorption, cell-mediated material degradation, and accelerated re-epithelization, OCT could also be deployed to both monitor and evaluate the transformation of implanted biomaterials. It should be noted that the rapid advances in implantable biomaterial to enhance wound repair have not been paralleled by a comparable development in a complementary technique for monitoring of implant efficacy. OCT promises the potential to be deployed in tandem with implantable therapeutics for objective efficacy assessment. Moreover, recent technological advances in polarization OCT, Doppler OCT, and uOCT may further enhance the contrast and resolution of OCT to provide more specific diagnosis, thereby allowing for optical biopsy to noninvasively assess wound repair instantaneously and longitudinally.
Footnotes
Acknowledgment
This work was supported by NIH Grants R01-DK068401 (W.C. and Y.P.) and 2R01-DK059265 (Y.P.). Please address inquiries regarding DCH hydrogel implant and wound model to W. Chen and inquiries regarding in vivo OCT imaging and assessments to Y. Pan, respectively.
Disclosure Statement
No competing financial interests exist.