
Abstract
Objective:
autologous chondrocyte implantation usually requires in vitro cell expansion before implantation. We compared the efficacy of cartilage regeneration by in vitro–expanded chondrocytes at high density and freshly harvested chondrocytes at low density.
Design:
surgically created osteochondral defects at weight-bearing surface of femoral condyles of domestic pigs were repaired by biphasic cylindrical porous plugs of DL-poly-lactide-co-glycolide and β-tricalcium phosphate. Plugs were seeded with autologous chondrocytes in its chondral phase, and press-fit to defects. Seeded cells were (1) in vitro–expanded chondrocytes harvested from stifle joint 3 weeks before implantation and (2) freshly harvested chondrocytes from recipient knee. Seeding densities were 70 × 106 and 7 × 106 cells/mL, respectively. Cell-free plugs served as control and defects remained untreated as null control. Outcome was examined at 6 months with International Cartilage Repair Society Scale.
Results:
the two experimental groups were repaired by hyaline cartilage with collagen type II and Safranin-O. Tissue in control group was primarily fibrocartilage. No regeneration was found in null control. Experimental groups had higher mean International Cartilage Repair Society scores than control in surface, matrix, and cell distribution, but were comparable with control in cell viability, subchondral bone, and mineralization. No significant difference existed between two experimental groups in any of the six categories. Uni-axial indentation test revealed similar creeping stress–relaxation property as native cartilage on experimental, but not control, specimen.
Conclusions:
cartilage could regenerate in both experimental models, in comparable quality. Culture of chondrocytes before implantation is not necessary.
Introduction
The procedures of ACI have evolved to the current principle that chondrocytes or other chondrogenic cells are seeded onto porous biodegradable scaffolds to constitute cartilage.6–10 Cell-seeding density on the biomaterial scaffold is considered critical to elaborate abundant matrix for quality cartilage. As high as 10–60 × 106 cells/mL is suggested necessary to constitute mechanically sound cartilage in vitro.11,12 However, the limited sparing and hypocellular nature of cartilage makes the direct harvest of so many cells difficult; therefore the number of harvested chondrocytes has to be culture expanded in vitro before implantation. This necessary step raises many problems. Chondrocytes in conventional monolayer culture lose their phenotype and dedifferentiate to fibroblast-like cells that fail to generate hyaline cartilage. 13 The facilities for the culture process, including the laboratory settings of good tissue practice, are very expensive. The cell harvest and implantation have to be accomplished in two separate surgeries.
Newer culture processes, such as the three-dimensional bioreactor system, have higher yields of chondrocytes with better preserved phenotype, 14 but other problems of ACI remain. An alternative strategy is to improve the condition of implantation to build cartilage from a smaller number of chondrocytes without culture. Recent studies indicate that chondrocytes of lower seeding density on selected biomaterial scaffold can synthesize cartilage-like matrix, 15 and that the in vivo intrarticular environment is optimal for the growth and presentation of chondrocytes. 16 We also reported good repair of porcine osteochondral defect with hyaline cartilage in 6 months, using a novel biphasic plug that was seeded with freshly harvested chondrocytes at a low seeding density of 3 × 106 cells/mL. 17
We hypothesized that the high seeding density of chondrocytes to regenerate cartilage in vitro may not be necessary in vivo. Using fewer cells, ACI could be finished in one seed-and-implant surgery. In this study we compared the outcome of cartilage repair in porcine knees with culture-expanded chondrocytes at high density, and with freshly collected chondrocytes at low density.
Materials and Methods
Biomaterials
The biphasic construct was fabricated with a modified solvent merging/particulate leaching method as previously described.17,18 Briefly, DL-poly-lactide-co-glycolide (PLGA; Purac, Gorinchem, The Netherlands) and NaCl were dissolved in acetone, and the solution was poured into a cubic mold. After solvent evaporation, the formed 0.8 mm thick PLGA–NaCl membrane was trimmed to an 8 mm diameter disk and a 25 × 5 mm sheet. The disk and sheet were assembled onto an 8 mm diameter cylindrical mold with steel-mesh bottom: the disk seated on the bottom, the sheet wrapped around inside the cylinder, and together they made a fillister. Separately, PLGA and β-tricalcium phosphate (TCP; Fluka, Buchs, Germany) of equal weight were dissolved in acetone, with NaCl added to supersaturation. After solvent evaporation, the resultant composite was grounded, and the NaCl was removed with water. The resultant PLGA–TCP composite of 250–440 μm size particles were selected and combined with NaCl particles of the same size, in 15/85 w/w. The aforementioned fillister was tightly filled with this PLGA–TCP/NaCl mixture. Solvent 1,4 dioxane was poured into the mold, let stand for 30 s, and exhausted; methanol was passed in the same way. PLGA finally precipitated and formed a matrix, which was then flushed with water to leach NaCl. Fabricated biphasic construct was sterilized with 75% alcohol, vacuum dried, and sealed until use (Fig. 1, inlay).
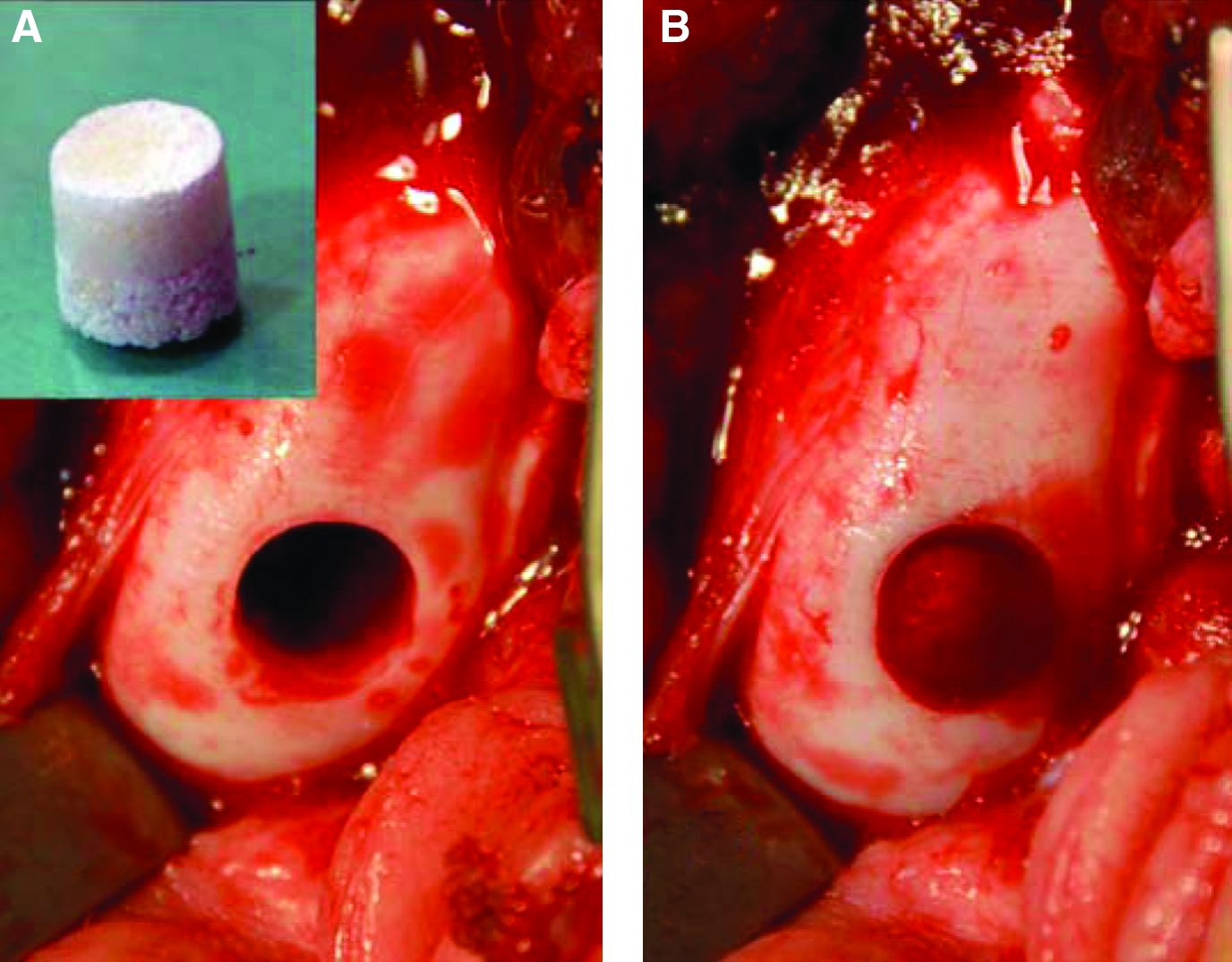
Surgical photographs showing the repair of artificially created osteochondral defect on femoral condyle by the biphasic cylindrical scaffold. (
Experimental design and surgical procedures
Animal experiment was conducted according to a protocol approved by the Institutional Animal Experiment Committee. Eleven skeletally mature (10 to 11 months old, five male and six female) domestic pigs were used. They were housed individually in a sheltered outdoor fenced space with good ventilation, and allowed forage and water ad libitum throughout the experiment. All surgeries were done in a standard operation room with routine operation-room procedures and sterile surgical techniques. The graft tissue was processed aseptically in a clean-room laboratory next to the operation room. Surgeries were done under general anesthesia, with first sedation by intramuscular injection of atropine sulfate (5 mg/kg) and Stresnil™ (Azaperonum, 4 mg/kg; Janssen, Geel, Belgium) and maintenance by mask-delivery gas anesthesia (halothane mixed with oxygen, and N2O, 1:1).
The four femoral condyles in both knees of an animal were assigned to the four groups (Table 1). For experimental group A (Exp A, n = 11), an artificially created osteochondral defect would be repaired with a construct loaded with chondrocytes harvested 3 weeks ago and culture expanded. For experimental group B (Exp B, n = 18), the defect would be repaired with a construct loaded with freshly harvested chondrocytes. For control group (n = 8), the defect would be repaired with blank, cell-free construct. For null group (n = 7), the defect would be left untreated.
The distribution of the four treatment models was designed to neutralize the laterality (the location of medial or later condyle) and cage effect (the interaction between condyles in the same joint).
A, Exp A; B, Exp B; C, Control; N, Null.
Chondrocytes' harvest for in vitro culture (Exp A)
Autogenous cartilage was harvested from the distal radius in left stifle joint 3 weeks before the implantation surgery. Approximately 35 mg of cartilage was collected from each animal and was immersed immediately in Dulbecco's modified Eagle's medium (DMEM; HyClone, Logan, UT).
In the laboratory, the cartilage was rinsed with Dulbecco's phosphate-buffered saline (DPBS; HyClone), pulverized with a tissue pulverizer (Industry Technology Research Institute, Hsinchu, Taiwan), and suspended in DMEM supplemented with 1% antibiotics (penicillin/streptomycin; Gibco, Invitrogen, Grand Island, NY). Collagenase (Collagenase C0130; Sigma, St. Louis, MO) and hyaluronidase (Hyaluronidase H3506; Sigma) were added to the final concentration of 0.4% and 0.1% w/w, respectively. The whole culture was kept at 37°C with stirring overnight for enzymatic digestion. At the end of enzymatic treatment, undigested debris was filter removed by a mesh, and the chondrocytes were washed with DPBS and centrifuge collected (300 g, 10 min). The number and viability of the isolated chondrocytes were determined with a hematocytometer and trypan blue exclusion dye test.
The chondrocytes were cultured with a three-dimensional alginate-encapsulated culture system in a bioreactor (Industry Technology Research Institute), as previously described. 14 Briefly, approximately 5 × 105 cells were contained by 7.5 mL of alginate scaffold prepared as previously described. 19 The seeded scaffolds were placed in the chamber of bioreactor with constant perfusion (8 mL/min) of circulating medium of DMEM supplemented with 10% fetal bovine serum (HyClone), 1% antibiotics, and 50 μg/mL ascorbic acid, from an exchanging reservoir through a closed aseptic piping system by the peristaltic pump (Masterflex L/S; Cole-Parmer, Vernon Hill, IL). The chamber was supplied with humidified gas of 5% CO2 and kept at 37°C.
Chondrocytes' harvest for immediate implantation (Exp B)
Both knees of the animal were operated at the same surgery through a longitudinal medial parapatellar incision and lateral dislocation of patella. An 8 mm diameter circle was marked by a punch on the center of distal weight-bearing portion of each femoral condyle. Full-thickness cartilage within one circle was peeled off for autogenous chondrocytes isolation, by procedures same as Exp A except that the enzymatic treatment lasted for only 40 min instead of overnight. After harvest, the arthrotomy was reduced and closed temporarily with sutures. The animal was kept anesthetized during the preparation of implants.
ACI surgery
The previously bioreactor-cultured chondrocyte-bearing alginate scaffold was smashed in DMEM. The hydrogel was filter removed with a mesh, and chondrocytes in filtrate were centrifuge collected. The part of 8 × 106 cells was isolated and resuspended in 0.1 mL DMEM, and loaded to the chondral phase of a construct, so that the spongy biomaterial was fully soaked. This construct served as the graft for Exp A, with seeding density in the chondral phase estimated at 70 × 106 cells/mL.
From the freshly isolated chondrocytes, the part of 0.8 × 106 cells was further isolated to prepare another construct as described above. This construct served as the graft for Exp B, with seeding density in the chondral phase estimated at 7 × 106 cells/mL.
At the time of implantation, knee joints were reopened by removing the sutures. The marked area on each condyle was further drilled to an 8 mm deep cylindrical pit. For both experimental groups, prepared constructs were manually inserted to press-fit in the defect, such that its surface appeared flush with the articular surface (Fig. 1). For control group, a cell-free construct was used instead. The arthrotomy was closed in layers after reduction of patella. The knee joints were let free for motion, and the animal resumed free activity with standing on all legs after recovery from anesthesia. For three postoperative days, antibiotics cephalexin (Glaxovet, Harefield, United Kingdom) 1000 mg/dose/day and analgesics buprenorphine–flunixin intermittently as needed were injected intramuscularly. Wound healing was ensured at 1 week.
Examination of regenerate tissue
Six months after the implantation, the animals were euthanized by overdose injection of pentobarbital, to retrieve the grafted condyles. Each grafted site was inspected grossly and bisected along the frontal plane to examine the integration of regenerate tissue with adjacent native tissue. One half of the bisected specimen was sent immediately for molecular biological test by polymerase chain reaction (PCR) and mechanical test. The other half was fixed with buffered paraformaldehyde for histochemical study.
For PCR examination, the regenerate cartilage was enzymatically dissociated to collect cells as described above. Total RNA was extracted from the retrieved cells with TRIzol reagent (Invitrogen–Life Technologies, Carlsbad, CA), and the portion of 2 μg was reverse transcribed with primer of oligo(dT)20 and reverse transcriptase. The first-strand cDNA product was subjected to PCR using oligonucleotide primer pairs (sequence shown in Table 2) for collagen type I and II, aggrecan, and GADPH as housekeeping gene. PCR protocol was an initial denaturation at 95°C for 3 min, followed by 27 cycles of polymerization at 94°C for 30 s, 55°C for 30 s, and 72°C for 45 s.
For histochemical studies, the specimen was decalcified overnight in sodium citrate–formic acid solution, embedded in paraffin, and microsectioned for routine hematoxylin–eosin (HE) staining, Safranin O staining for aggrecan, and immunohistological staining for collagen type II (Chemicon, Temecula, CA). A pathologists blind to the treatment scored the histology of specimens on the International Cartilage Repair Society (ICRS) Visual Histological Assessment Scale. 20 The matrix would be defined as hyaline cartilage exclusively when the ground substance of the matrix was homogeneous with minimal fibrous texture by HE staining, positively Safranin O stained, contained predominantly collagen type II, and the cells were round, existed individually or aligned in short columns, and sit centrally in lacunae. Cell would be considered viable by showing a clearly delineated nucleus in HE staining. 21 All specimens were evaluated on the basis of one parameter at a time. Scores of each individual parameter were analyzed statistically among groups with one-way analysis of variance test by SPSS software (SPSS, Chicago, IL), setting significance at 0.05. When significant difference existed, Fisher's Least Significant Difference was used for post hoc group pair-wise analysis.
For mechanical test, the compressive stress–relaxation behavior of the regenerate tissues and the native cartilage was defined by unconfined uni-axial indentation test22,23 with a custom-designed device. The null group specimens inconsistently contained little or no regenerate cartilaginous tissue and did not participate in this test. The test device included a stage with precise height adjust; above the stage was a stress gauge with a 2 mm diameter bold-tip probe pointing downward toward the stage. The osteochondral specimen was mounted on the stage, with the cartilage facing up. The stage was raised until the cartilage surface touched the probe tip with zero compression. The thickness of cartilaginous tissue was measured, and the stage was further raised a predetermined amount to apply a 30% strain on the center of cartilage surface against the probe tip. The reaction force was taken by the gauge and transformed to compressive stress as a function of time. The test was performed in room temperature, with the specimens adequately hydrated by intermittent irrigation with DPBS before and throughout the process. After the instantaneous peak stress, the specimens were allowed for a time-dependent stress–relaxation to equilibrium over 10 min. Four animals participated in the mechanical test.
Results
Molecular biological presentation shown by PCR
Regenerate cartilage in both experimental groups presented type II collagen and aggrecan in strong intensity and was absent of type I collagen. Contrarily, the regenerate tissues in control and null groups consisted primarily type I collagen with minimal type II collagen and aggrecan presentation (Fig. 2).
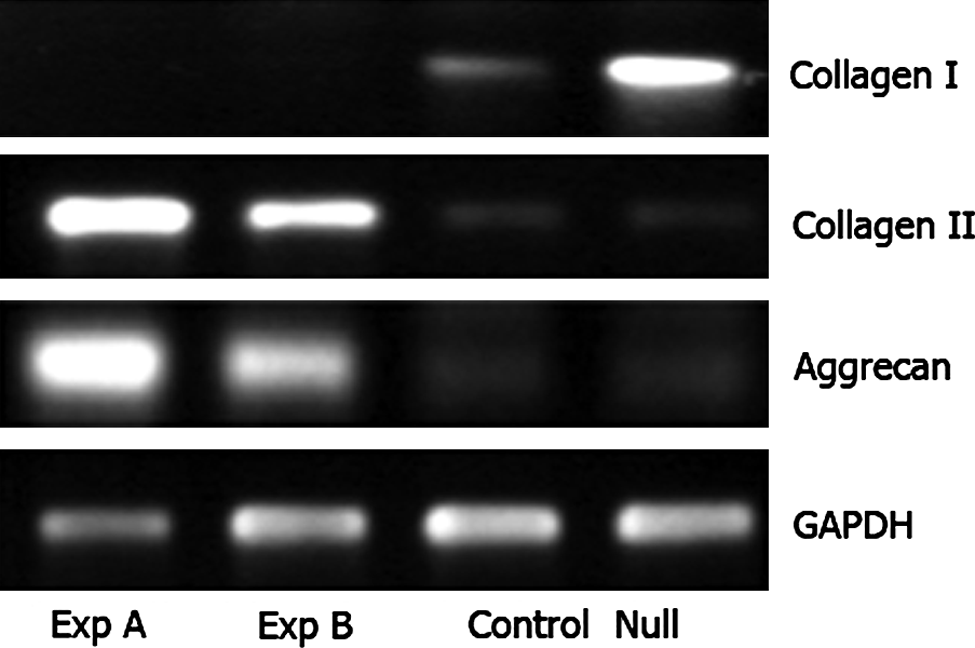
Polymerase chain reaction of total RNA of the cells retrieved from repair tissue of the four groups. Polymerase chain reaction products were analyzed by electrophoresis in 1% agarose gels containing ethidium bromide.
Macroscopic and histological (ICRS score) results
The defects of null group were incompletely filled with osseous callus with or without a thin fibrous cap and appeared as a dimple. Contrarily, the defects of the three implanted groups were consistently filled with firm bone, covered with fibrous or cartilaginous tissue, and flush with the surrounding articular surface. The covering tissue in both experimental groups consisted of elastic-firm, cartilage-like substance, whereas such tissue was found in only two defects of the control group (Fig. 3).

Gross appearance of repair outcome in the same animal, showing the osteochondral defects (arrows) of the four groups 6 months after the implant surgery. In both experimental groups, the defects were repaired with elastic-firm regenerate cartilage with smooth surface approximately flush with the articular surface. In the control group, the repair tissue was fibrous and elevated as a hump, with rough surface and poor integration with surrounding native cartilage. The defect of null group remained a dimpling and incompletely repaired with bony callus. Color images available online at
The biomaterial in the chondral phase of all implanted defects was completely resorbed and replaced with regenerate tissue, which was scored on the ICRS scale. Because the null group had scanty regenerate cartilage, this group was included only for the scoring of subchondral bone. In summary, either experimental group had significant higher scores than the control group, yet comparable to each other, in surface morphology, matrix, and cell distribution (Fig. 4). (1) Surface morphology: histological observation of surface smoothness paralleled gross finding. The regenerate cartilage of both experimental groups generally had smooth surface, although visible major fissures might exist. The surfaces in the control group were generally uneven; only one specimen had smooth surface. (2) Matrix: the nature of the ground substance in regenerate cartilage of both experimental groups showed regional variation. Generally, the matrix of these specimens was homogeneous by HE staining and contained collagen type II and aggrecan as shown by specific staining. Contrarily, the regenerative tissue in control group was consistently fibrous, with coarse dark HE-stained streaks, and deficient in collagen type II or aggrecan (Fig. 5). (3) Cell distribution: cells in the regenerate cartilage of both experimental groups were predominantly round and lacunated, but did not routinely distribute in the typical palisade pattern of native cartilage. Instead, these cells distributed evenly and appeared basically individual. Short cell columns were found, but oriented randomly rather than perpendicularly to osteochondral junction. Cell rosettes were frequently found in clusters (Fig. 6). Cells in the control group were predominantly fibroblast-like spindle cells, oriented parallel to the surface of subchondral bone, and packed tightly among intercellular fibers without lacunae. (4) Cell viability: the cells in the regenerate cartilage of both experimental groups were generally viable. The cells in the control group were also viable and were considered postoperative immigrant, because the scaffolds were implanted cell free. No significant difference was noted among the implanted groups. (5) Subchondral bone: contrarily to the chondral phase, biomaterial consistently remained in the osseous phase of all implanted defects as dark HE-stained islets scattering among the regenerate cancellous bone. The distribution of the residual biomaterial was compatible to the original shape of implant (Fig. 7). The repair bone seamlessly integrated with the native bone by interdigitation, with active cellular reaction along the junction, featuring many multinuclear cells. Callus also formed in the defects of null group. The scores had no significant difference among the four groups. (6) Mineralization: the regenerate cartilage of all implanted defects showed various extend of mineralization, as buds of subchondral bone on the tidemark, and/or isolated bone islands. No significant difference was noted among the implanted groups.
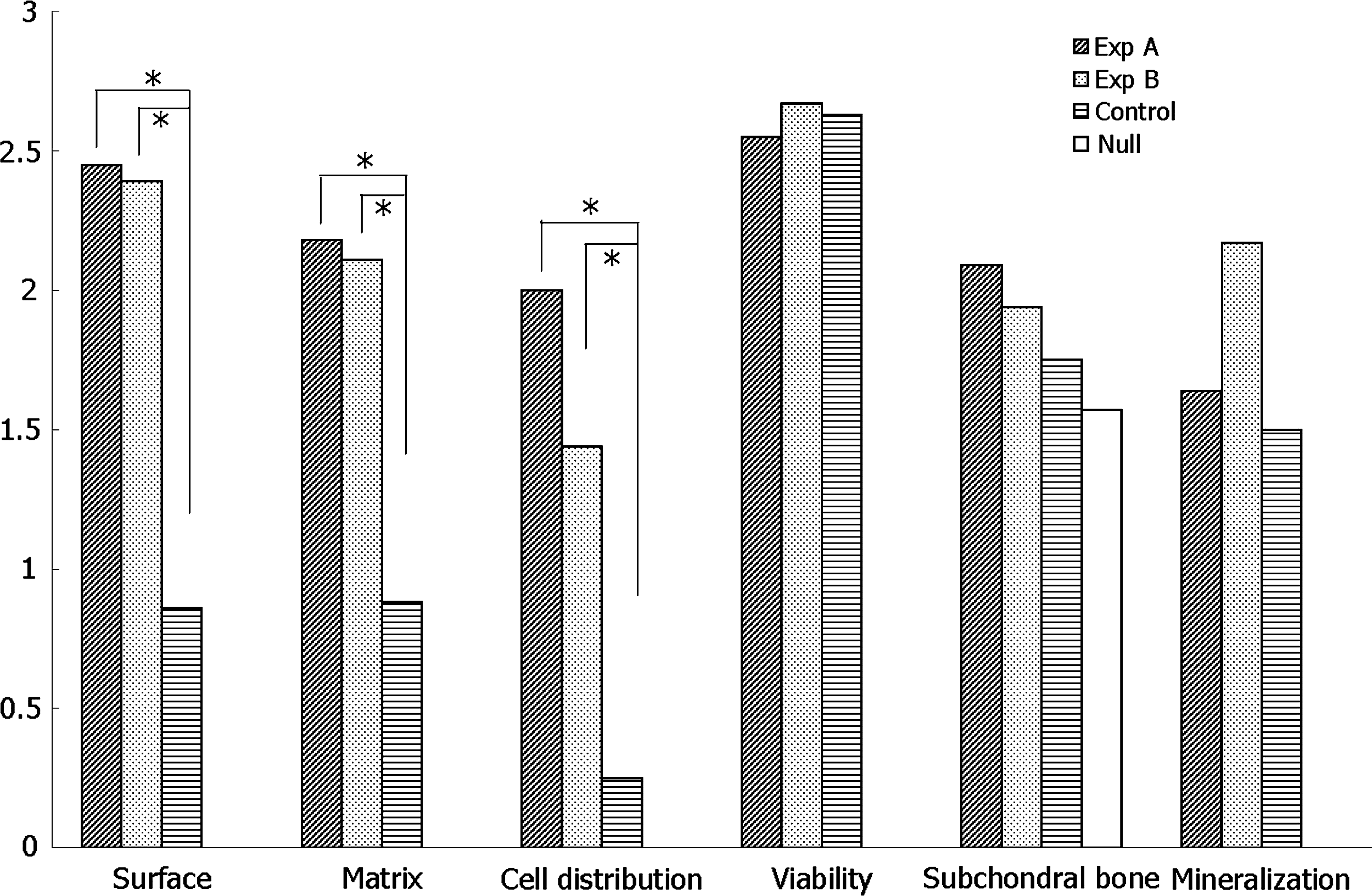
Mean scores of experimental and control groups based on International Cartilage Repair Society histological scale. Asterisks indicate statistically significant difference between groups.

Histological and immunohistochemical analysis of regenerate cartilage. Regenerate cartilage of both Exp A and Exp B groups had hyaline matrix, which consisted of homogeneous ground substance without dark HE-stained fibrous streaks and contained GAG (red Safranin O stain) and collagen type II (brown immunohistochemical stain). Regenerate tissue in the chondral phase of control group consisted of thick fibrous tissue that was dark HE stained and deficient in glycosaminoglycans (GAG) and collagen type II, as shown by the faint color in specific stains. HE, hematoxylin–eosin.

Higher magnification of a specimen from Exp B group showed even distribution of cells in the regenerate cartilage. The cells were lacunated and appeared single (arrow 1), in short ray (arrow 2), or as a rosette (arrow 3). Color images available online at

Section of repaired osteochondral defect. (
Tissue interface
In the experimental groups, the osseous and chondral tissues regenerated separately in the corresponding phases of the constructs. Cancellous bone formed under the regenerate cartilage and fused tightly with the cartilage with a clear tidemark as originally defined by the construct. The tidemark approximately aligned with the native osteochondral junction. The control group showed similar architecture, but the regenerate tissue in the chondral phase was fibrous.
In the experimental groups, the regenerate cartilage was distinguishable histologically from native cartilage in most specimens. The integration between the regenerate and native cartilage was inconsistent even in a given specimen and varied regionally from good transition with smoothly continuous surface, to separation with a gap.
Mechanical properties
At 30% strain, specimens of both experimental groups and native cartilage showed similar biphasic stress–relaxation patterns (Fig. 8). A peak stress of about 0.65 MPa was recorded rapidly in the initial 1–3 s. The stress then decayed gradually in the next 10 min, to finally equilibrate at about 0.04–0.13 MPa, with the decreasing order of native, Exp A, and Exp B cartilage. As a rule, the Exp B cartilage showed the fastest decay, as depicted by larger slope of the curve between 3 and 10 s, and equilibrated with the lowest stress.
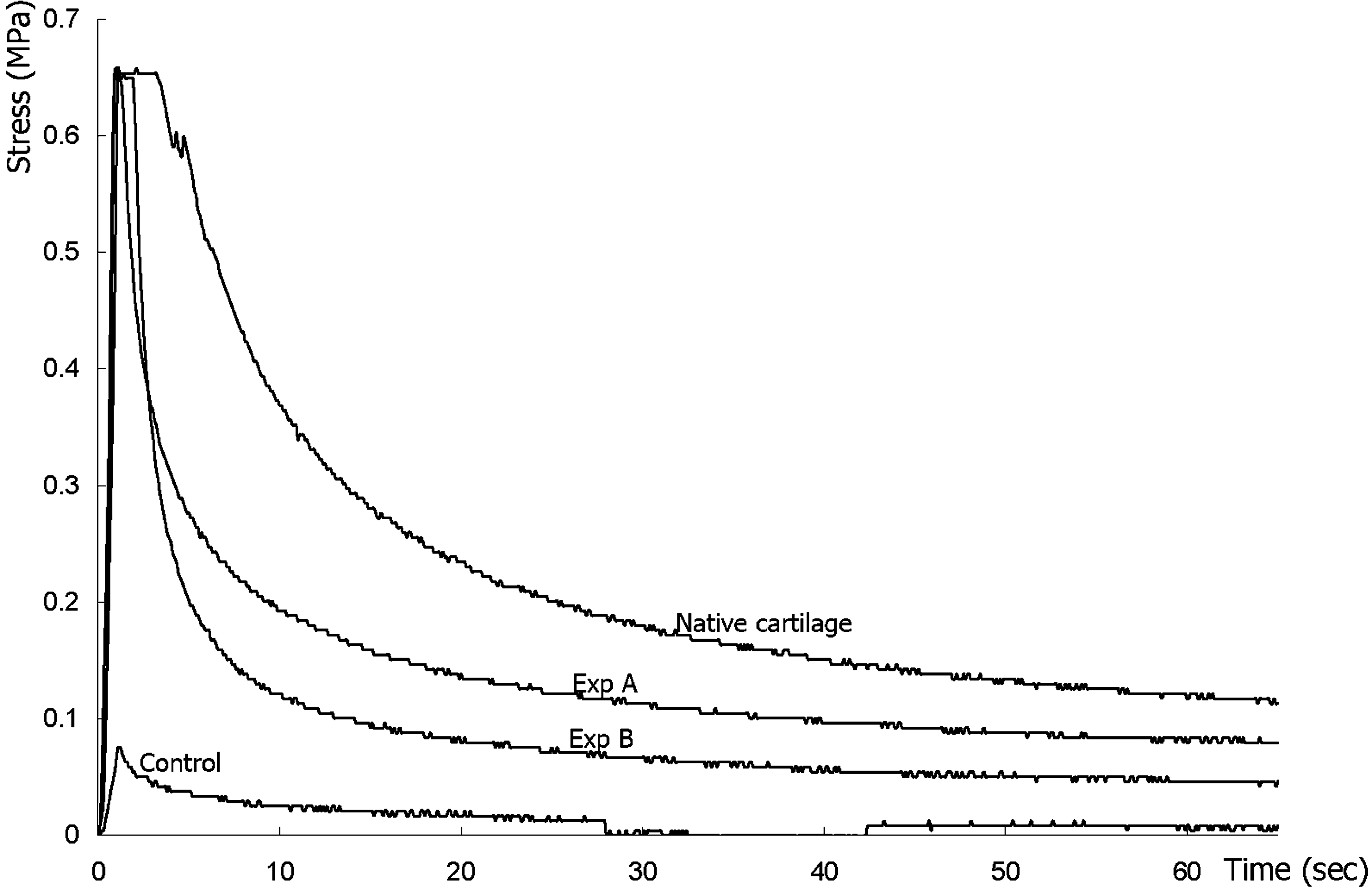
Example mechanical property of specimens by indentation test at 30% of the strain on the specimens from one animal, showing the stress–relaxation process. The stresses of the two experimental and native specimens rose to the peak within 2 s, relaxed more quickly in the next 10 s, and gradually thereafter to the equilibrium values of 0.07 MPa for native cartilage, 0.04 MPa for Exp A, and 0.02 MPa for Exp B groups. The stress of the control specimen had a slower rise, peaked at 0.07 MPa, and dropped slightly to the equilibrium value of 0.01 MPa.
The control group specimens behaved very differently under the same condition. The mean (n = 4) peak stress of 0.06 MPa was reached 2–4 s after the application of strain and only dropped insignificantly thereafter. The mean equilibrium stress was 0.02 MPa, showing a relatively smaller percentage drop in comparison with the native cartilage and experimental groups.
Discussion
ACI is a cell therapy that relies on chondrocytes to produce appropriate matrix and repair cartilage defect. 24 There is no consensus in the literature to date about the optimal seeding density for ACI. Earlier in vitro studies indicate high cell demand, but recent in vivo study suggests that lower cell density as 104 cells/mL can yield good cartilage, 25 possibly due to the naturally optimized intrarticular environment for the multiplication and presentation of chondrocytes. Excessively implanted cells may adversely affect the outcome of ACI by overgrowth of neocartilage that humps above the native articular surface. 15 The clinical relevance of engineering cartilage at low cell density is the possibility of omitting the laboratory expansion of cells, and combining cell harvest and implantation in the same surgery. This study compared the efficacy of ACI at different seeding density.
We did not consider the effects of culturing on chondrocytes in Exp A, and assumed that the cultured chondrocytes had the identical phenotype, activity, and viability as the freshly harvested chondrocytes in Exp B. Recently improved culture techniques, such as that used in this study, can better preserve the phenotype of chondrocytes than conventional monolayer culture.13,14,26 Regardless of the culture process, chondrocytes of both experimental groups in this study expressed similarly after the 6-month intrarticular growth, with the presentation of type II collagen and aggrecan.
We also considered the donor sites of autologous chondrocytes irrelevant, although some studies showed that chondrocytes from different joints and different location of the same joint behave differently.27–29 We considered the difference insignificant for the chondrocytes to build cartilage and avoided using knee joints as the donor in Exp A to reduce damage of the joints by repeated surgery.
Native chondrocytes have very limited motility30–32 and were presumed minimally possible to migrate into the implanted scaffold. Concordantly, we did not find much chondrocytes in the noncell-seeded chondral phase of the control group, where the cells were possibly migratory from bone marrow. Bone marrow–derived progenitor cells can transform to chondrogenic in vivo, but tend to generate fibrocartilage rather than hyaline. 33 The fibroblast-like cells in the chondral phase of control group might be derived from the marrow cells. The absence of chondrocyte or hyaline cartilage in the control group suggested that preseeding of chondrocytes would be necessary. In our study, the seeded chondrocytes in both experimental groups occupied the space of chondral phase, and the marrow progenitor cells either did not move into the chondral phase or transformed more like chondrocytes. Another in vitro report about a similar biphasic construct with PLGA/TCP osseous phase indicates that the seeded chondrocytes preferentially stay in the PLGA chondral phase. 34 We had the same finding.
The clinical success of mosaicplasty discloses several advantages of osteochondral repair over cartilage-only repair. The surgery is easier because the graft self-secures to the recipient site without additional fixing procedure or device. Although the in vitro constitution of an osteochondral construct requires preseeding osteogenic cells to build the osseous phase,35–37 this is unnecessary for in vivo intrarticular application. 38 The spongy construct absorbs the oozing host marrow at the recipient site, and the marrow stromal cells undergo osteogenesis when exposed to the TCP content of the construct.39–41 Our biphasic scaffolds were fabricated with predefined osteochondral junction. We did not observe the separation of the regenerate cartilage from the regenerate subchondral bone, indicating that the binding between the two phases withstood the abrasion in knee motion. This has important clinical relevance because early knee motion can promote the implanted chondrocytes to regenerate cartilage. 42 Osteochondral repair can concurrently treat the subchondral pathology that exists with cartilage defect, such as in osteochondritis dissecans and focal osteonecrosis. However, the osteogenic cells migrated into the osseous phase of scaffolds might inevitably move further into the chondral phase, as a possible origin of the mineralized islets in the regenerate cartilage in our study.
ICRS scale is the most widely used scale to evaluate regenerate cartilage. This scale was originally designed for specimen of limited amount, usually less than 2 mm diameter, from biopsy. However, we found that the nature of regenerate cartilage may show a considerable regional variation, making scoring for the entire specimen difficult. We scored the specimen by the predominant pattern that occupied the majority area. The ICRS scale scores “cell distribution” because the lack of columnar distribution of chondrocytes in the middle and lower zones of cartilage indicates abnormal maturation. 20 The unique uneven and palisade-pattern distribution of chondrocytes in native cartilage is derived from the enchondral ossification of the epiphysis during bone maturation. 43 However, most models of ACI prefer uniform seeding of cells to avoid local hypertrophy of regenerate tissue. 44 Although cartilage may remodel by mechanical stimulus of normal joint activity,45,46 the natural distribution of chondrocytes did not build in our animals.
Biomaterials remained in the osseous phase at 6 months, helped us to identify the repaired site, and proved the absence of scaffold dislodgement. Another animal study using TCP block to repair osteochondral defect also shows incomplete resorption of TCP at 30 weeks, indicating possible long-term persistence of this ceramic material. 38 However, TCP content has good osteoconductivity and can enhance the affinity of the implant with host bone.47,48 We observed good integration of the TCP-containing implant with the host bone, with cell population and callus formation in the originally cell-free construct.
Mechanical characteristics of articular cartilage are difficult to define and are influenced by many confounding factors such as the anatomical location, the models of testing, and conditions of the joint.23,49 Unconfined compression model can demonstrate the mechanical property of cartilage in physiological condition.50,51 Indentation test is an example of this model to examine the overall response of cartilage under stress. 52 We used it to analyze the relative stress responses of cartilage specimens from the same animal, instead of calculating specific mechanical parameters. Regenerate cartilage from both experimental groups and the native cartilage showed similar stress–relaxation response. The immediate peak stress was the rebounding force by the viscoelastic cartilage. The reacting force then dropped gradually with extrusion of fluid from the material, until the equilibrium reflecting the resistance from solid matrix. The faster decay of stress indicated the faster loss of the fluid content, and inferior fluid retaining ability of material, or higher permeability. In this respect, specimens of both experimental groups lost their fluid content more quickly than native cartilage, yet equilibrated at similar stress as the later, meaning a similar stiffness of their solid content and higher permeability in the regenerate cartilage. The regenerate tissue of control group depicted little stress–relaxation under compression, indicating that it was solid or contained minimal interstitial fluid.
In conclusion, our findings indicated that the biphasic cylindrical construct supports the regeneration of articular cartilage in vivo with preseeded autogenous chondrocytes in chondral phase at the density of 7 × 106 cells/mL. Higher seeding density would yield regenerate cartilage of comparable quality and would not be necessary for ACI. The construct could self-secure without additional fixation. Cancellous bone formed in the osseous phase without preseeding and integrated with the native subchondral bone. This model may be an alternative to mosaicplasty, with less donor site morbidity, that could be done in one harvest-seed-implant surgery.
Footnotes
Acknowledgments
This study was supported by a cooperative grant from the Industrial Technology Research Institute (E43230) and the National Taiwan University Hospital. We thank Mr. Kai-Jen Chen for his assistance in animal surgery.
Disclosure Statement
No competing financial interests exist.