
Abstract
Shortening of the healing time before loading risks impeding successful titanium implant anchorage into compromised bone. A thorough understanding at the genetic scale of the early phases of bone regeneration at the implant interface is required before the development of strategies to enhance implant osseointegration. In this study a new in vivo implant model to explore the mechanism by which titanium implant osseointegration is affected by the host bone properties is presented. An implant was conceptualized enabling standardized harvesting of peri-implant tissue for quantitative molecular analysis while preserving the mimicking of the clinical setting. The implant is partly indented to provide a well-defined healing compartment from where tissue differentiation and de novo bone formation can be investigated and partly screw-threaded to provide a good implant anchorage into the bone. The feasibility of the implant design was assessed in osteopenic bone conditions, evoked by simulated weightlessness. Wistar rats were either hindlimb unloaded by tail suspension (HU) for 9 days or acted as controls (CTL). The status of compromised bone tissue through 9-days HU was confirmed by micro-X-ray computed tomography. The implant was installed in the proximal tibial bone 7 days after the onset of HU or CTL. Two days postimplantation, the peri-implant regenerating tissue responses were recorded by measuring expression of inflammatory, angiogenic, and bone resorption parameters (hypoxia-inducible factor 1, alpha subunit; vascular endothelial growth factor A; angiopoietin 1; endothelial PAS domain protein 1; fibroblast growth factor 2; tumor necrosis factor; interleukin 11; acid phosphatase 5, tartrate resistant; tumor necrosis factor (ligand) superfamily, member 11/RANKL). We successfully demonstrated that HU-associated bone conditions evoked a significant alteration of expression of the angiogenic markers in the peri-implant regenerative tissue during initial implant osseointegration, whereas the expression levels of the inflammatory and bone resorption parameters remained unchanged. We concluded that this in vivo implant model provides a well-designed and controlled method to examine molecular responses in implant osseointegration to impaired bone conditions. This model may serve to explore the application of anabolic strategies in peri-implant osteogenesis.
Introduction
Numerous in vitro studies have been undertaken to better understand the adhesion, proliferation, and differentiation of osteoprogenitor cells in contact with titanium implants.9–12 Even though in vitro studies have the potential to partially elucidate the molecular mechanisms involved, their clinical relevance is very limited because they do not reproduce the complex biological cascade of osseointegration. 13 In vivo studies using different implant designs have described the biological events occurring during titanium implant osseointegration at the tissue level.14–18 Commonly designed (i.e., cylindrically shaped) implants were installed in direct contact with the bone, and histological and histochemical analyses focused on the adaptive response of the preexisting bone. Adversely, bone chamber models allowed ultrastructural investigation of de novo bone formation within a well-defined healing compartment,19–21 and more particularly in the peri-implant environment. 22 With regard to the molecular regulation of implant osseointegration, the sparse data available are either nonquantitatively 2 or poor representative for the clinical condition.8,23,24 Therefore, a new implant model was established in the presented study, designed for installation in direct contact with the host bone and concomitantly allowing quantitative investigation of the peri-implant tissue response at the molecular level. Moreover, to increase the clinical relevance of the new implant design, its feasibility was assessed in osteopenic bone conditions. To do so, the animal model selected was based on the NASA-designed hindlimb unloading through tail suspension model. 25 Owing to an impaired function of the musculoskeletal system in response to skeletal unloading,26–29 this experimental setup is often referred to as a model of disuse for the bone tissue. The model was upgraded to an in vivo model of implant osseointegration through implant placement in the proximal tibial bone of hindlimb unloaded animals. In this way, the impact of compromised bone conditions evoked by hindlimb unloading on the peri-implant tissue response could be investigated.
We hypothesized that the initial phases of bone regeneration at the implant surface need to be examined in detail at the genetic scale before the development of strategies to improve implant osseointegration in compromised bone. With this approach we aimed to develop an implant design, enabling standardized harvesting of peri-implant tissue and quantitative molecular analysis of the differentiating tissue. As a proof of our concept, the mRNA from the standardized explants at 2 days postimplantation was isolated for investigation by polymerase chain reaction (PCR) of inflammatory, angiogenic, and bone resorption parameters. The ultimate objective of the use of this implant model is to better understand the biological cascade of implant osseointegration in osteopenic bone tissue by comparing with the one governing in healthy bone tissue, and to further expand the model's application for favoring osseointegration.
Materials and Methods
Animals and hindlimb unloading
Adult female Wistar rats (Janvier) at 14 weeks of age were used in the experiment. The rats were housed alone and allowed to acclimatize for 7 days. A total of 20 rats were divided into two groups such that the average weight was similar between the groups. A group of 10 rats was subjected to hindlimb unloading by tail suspension (hindlimb unloading condition [HU]) for 9 days, as described by Holy and coworkers. 30 Briefly, a tape was applied to the surface of the tail to set a metal clip. The end of the clip was fixed to the overhead bar of a specifically designed Plexiglas cage (400 × 300 × 220 mm; CERMA-Biomeca). The height of the bar was adjusted to maintain an ∼30° head-down tilt with the hindlimbs elevated above the floor of the cage. Rats were allowed to move within the cage using their forelimbs, whereas their hindlimbs were kept free of weight bearing. The other group of 10 animals was housed individually under the same conditions but without tail suspension for the same duration (control condition [CTL]). All rats were kept under controlled conditions at 24°C with a ratio of 12 h light/12 h darkness cycle, fed with standard laboratory chow containing 1% calcium and 0.8% phosphorus (SAFE), and given tap water. Animals were weighed at start and daily during the study. Using a video monitoring, two tail suspended rats were observed for 24 h for evaluating animals' adaptation and function. At the end of the experiment, animals were sacrificed with an overdose of pentobarbital (Doléthal®; Vétoquinol). All experiments were conducted according to the institutional guidelines for animal welfare, and the experimental protocol has been approved by the local ethics committee for animal experiments.
Implant and surgery
A commercially pure titanium one-piece percutaneous implant was designed and fabricated (GC Corporation) (Fig. 1). The implant has a length of 8 mm, a maximum diameter of 2 mm, and a roughness value (Ra) of 1.36 ± 0.04 μm. The endosseous part facing the cortical bone is screw-threaded; the percutaneous implant part is asmachined to avoid skin irritation. The middle region of the endosseous part is featured by a threadless cavity of 2 × 0.55 mm, corresponding to a volume of 3.77 mm3 from where regenerating bony tissue can be harvested, hereafter named “tissue regeneration area” (TRA).
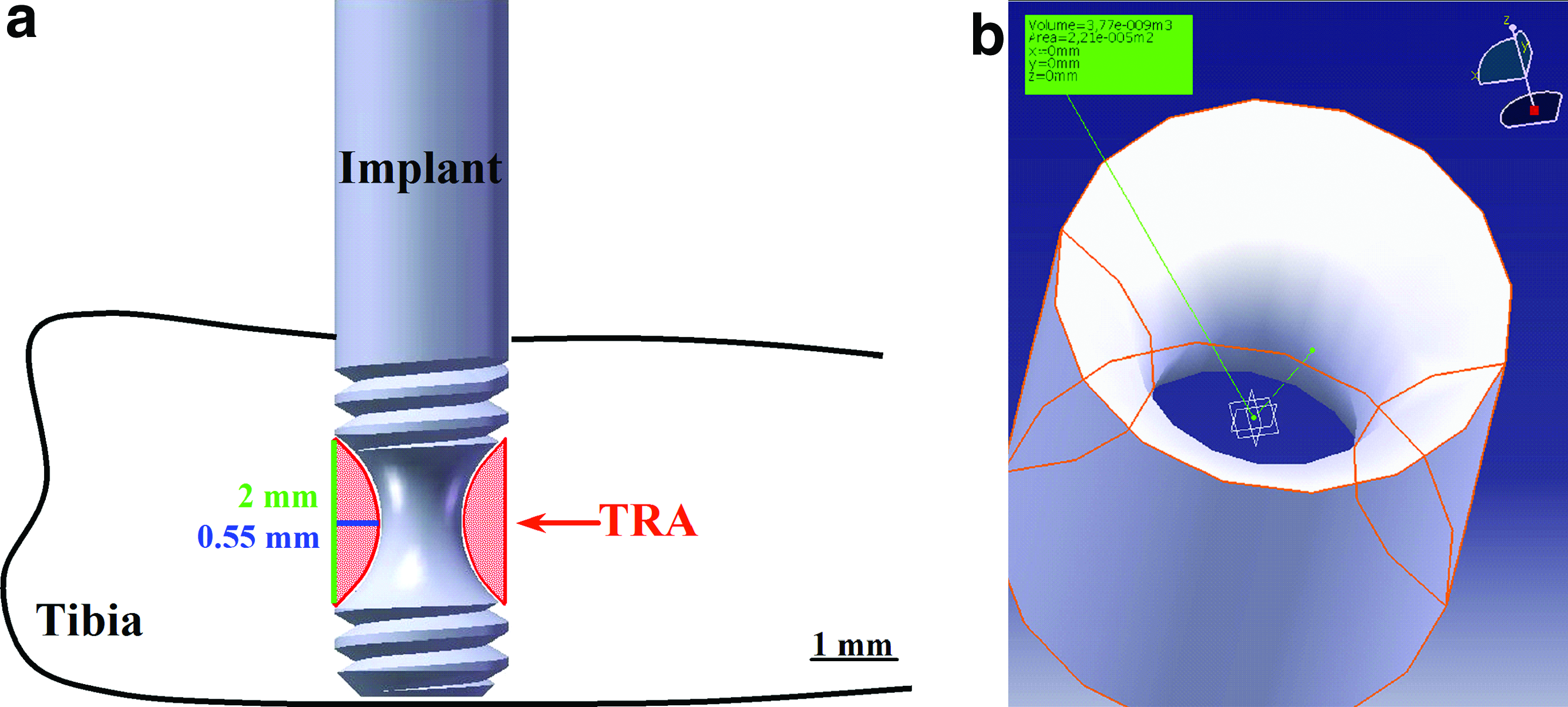
Implant design, dimensions, anatomical location, and region of interest (TRA, tissue regeneration area) (GC Corp.)
The implant was installed unilaterally in the tibia of the rats of both HU and CTL group, 7 days after the onset of skeletal unloading or of normal weightbearing, respectively. Surgery was performed under general anesthesia. The animals were anesthetized by subcutaneous injection of medetomidine (0.1 mg/kg; Domitor®; Pfizer) and ketamine (75 mg/kg; Ketamine 500®; Vibrac). A small skin incision on the medial side of the proximal metaphysis of the tibia was made to provide access to the bone. Land marking of a standardized implant positioning was performed by perforating the cortical bone with a sharp probe 5 mm distally from the proximal end of the tibia, centrally in the medio-proximal plateau of the tibia. A bi-cortical cavity with a diameter of 1.75 mm was drilled at a low rotational speed and under continuous external saline cooling. Implants were inserted by manual torque, and primary stability was ensured by bi-cortical fixation (Fig. 2). To lower the degree of micro-motion of the implant, the rat's leg was splinted with an elastic adhesive bandage (Tensoplast; BSN Medical) postoperatively. The animals were awakened thereafter by subcutaneous administration of an alpha2-antagonist (1 mg/kg; Antisedan®; Pfizer), positioned on a heating plate. Analgesics were given by intramuscular injection of meloxicam (0.3 mg/kg; Metacam®; Boehringer Ingelheim) for 2 days.
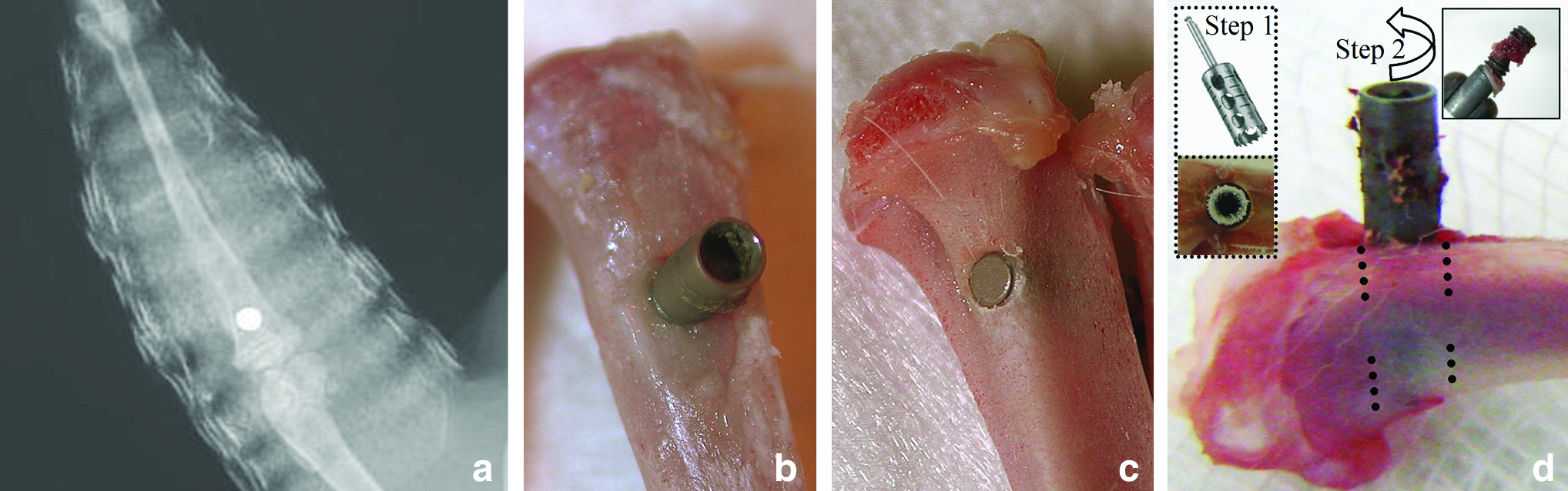
Anatomical position of the implant in the rat tibia, visualized by X-ray
Sample harvesting
After 9 days of hindlimb unloading or normal weight bearing, all animals were sacrificed. The tibiae and femora were separated from adherent muscles and connective tissues other than periosteum. Half of the tibiae without implant from HU and CTL group (n = 10) were used for micro-X-ray computed tomography (μCT) analysis of bone architectural changes in response to 9 days of unloading. These samples were preserved in 70% ethylalcohol solution. The tibiae with implant (n = 20) were used for gene expression analysis during initial (i.e., 2 days postimplantation) implant osseointegration. These entire harvested tibiae were snap-frozen in liquid nitrogen and stored in a −80°C freezer until the time of peri-implant tissue harvesting. Additionally, the bone marrow of femora from HU and CTL groups (n = 10) was harvested and the flushed cell suspensions from each group were reduced to two pools of cells for each group.
μT analysis of tibial bone architecture
For measurements of the alteration of the bone architecture in response to skeletal unloading, the proximal parts of the tibiae without implant of tail suspended and control rats were subjected to a desktop μCT, commercially available as Skyscan 1172 (Skyscan). The Skyscan 1172 machine is equipped with an 80 kV X-ray source with a camera pixel size of 9 μm. μCT images were made along the midsagittal planes in the metaphyseal region of the bones. During the scan, tibias were placed in polyethylene tubes filled with alcohol 75%. The scans resulted in reconstructed three-dimensional data sets with a voxel size of 8.45 μm. The data were subsequently quantified using CTAn automated image analysis system (Skyscan). To determine the trabecular volume of interest (VOI) in the axial direction, the growth plate was determined as reference (Fig. 3). The region of interest was set with its closest edge at 1.00 mm distally from the growth plate and with a length of 3.38 mm ( = 400 slices). The distance of 1.00 mm was chosen such that no primary spongiosa was included in the trabecular VOI in any of the samples. For each transverse slice, the VOI was established manually in an area of trabecular bone, as large as possible. The registered gray-value images were segmented using a Gaussian filter into binary images, using a low-pass filter to remove noise and a fixed threshold (26.7% of maximal gray-scale value) to extract the mineralized bone phase. Bone volume fraction (BV/TV), trabecular thickness (Tb.Th), trabecular separation (Tb.Sp), and trabecular number (Tb.N) were calculated three-dimensional as measures of trabecular bone mass and its distribution.
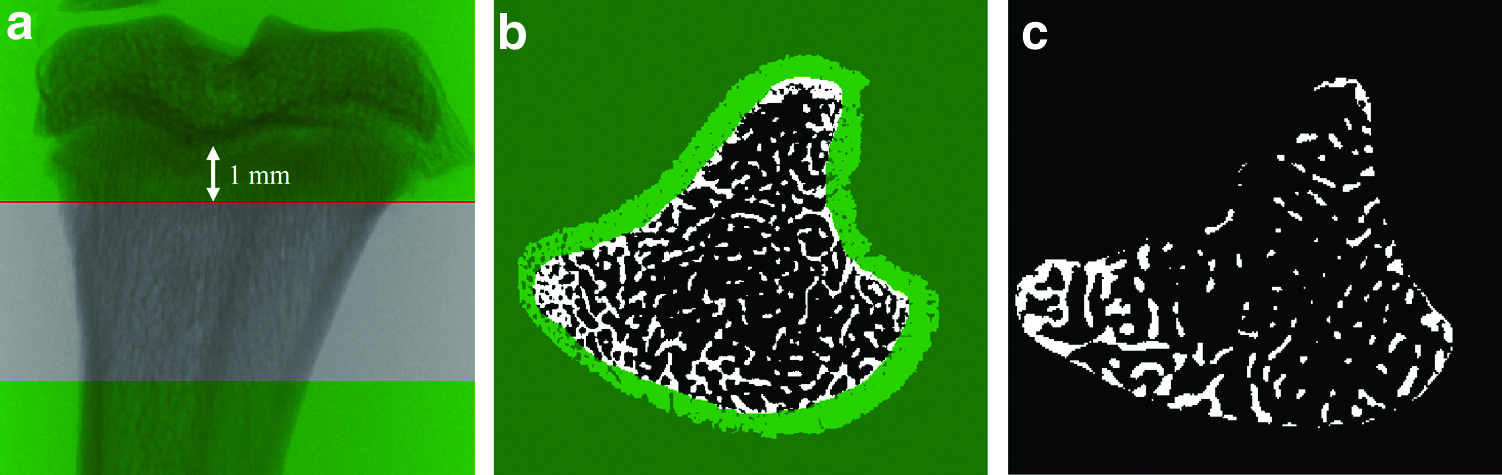
Microtomographic reconstructions of bone slices.
Molecular analyses of peri-implant tissue
The tissue in TRA of the implants was isolated in a two-step procedure (Fig. 2d). By means of a trephine burr with inner and outer diameter of 2.3 and 2.8 mm, respectively (PRAXIS), both cortices were perforated under continuous external cooling and freezing–thawing cycles in liquid nitrogen. Thereafter, the implant with tissue was removed manually and immediately immersed in 1 mL TRIzol (TRIzol® Reagent; Invitrogen). RNA from the tissue in TRA was extracted according standard protocols. 31 The RNA concentration and purity were measured using a spectrophotometer (Nanodrop 1000; Labtech). The integrity of the RNA was qualified using a microfluidics-based platform for RNA analysis (Agilent Bioanalyzer; Agilent Technologies). Random-primed cDNA was synthesized from 500 ng of total RNA using the SuperScript™ II RT Kit (Invitrogen). Equal volumes of cDNA were used to program amplifications through real-time PCR reactions using specific primers of genes encoding for hypoxia-inducible factor 1, alpha subunit (Hif-1α), vascular endothelial growth factor A (VEGF-A), angiopoietin 1 (Angpt1), endothelial PAS domain protein 1 (Epas1), fibroblast growth factor 2 (FGF-2), tumor necrosis factor (TNF), interleukin 11 (IL-11), acid phosphatase 5, tartrate resistant (Acp 5), tumor necrosis factor (ligand) superfamily, member 11/RANKL (TNFSF11), and 18S (kits TaqMan®; Applied Biosystems Inc.) in the presence of TaqMan Universal PCR Master Mix (Applied Biosystems) using an iCycler thermocycling apparatus (MyiQ™ Single-Color Real-Time PCR; Bio-Rad Laboratories). After a 10-min 95°C step for activation of DNA Polymerase, cDNA was amplified by performing 40 two-step PCR cycles: a 15-s denaturation step at 95°C, followed by a 60-s annealing and extension step at 60°C. Each sample was run in triplicate. The data were analyzed using MyiQ Software (Bio-Rad Laboratories). RNA from the harvested femoral bone marrow cell suspensions from HU and CTL groups was isolated and analyzed in identical manner.
Statistical analysis
Data were analyzed with a Fischer and Student's t-test and the nonparametric Mann–Whitney test to assess the statistical significance of comparisons between both groups. p-Values were considered significant when ≤0.05.
Results
Effect of HU on animal adaptation and growth
Through video monitoring, it was observed that the animals adapted to their new situation and that the HU apparatus allowed most of animals' functions. The rats were able to move in the cage, to rest, and to sleep. A moderate weight loss after implant surgery, but an overall increase in body weight (±14%) throughout the experiment was observed in both groups. No significant differences between the groups were seen, indicating that rat feeding activity had not been altered.
Effect of HU on μCT morphometric cancellous bone parameters
Significant differences between HU and CTL for two bone morphometric parameters were observed by μCT. The number of the trabeculae decreased and their separation increased after 9 days of skeletal unloading compared with normal weight bearing (Table 1; p-values of 0.048 and 0.039 for Tb.N and Tb.Sp, respectively). The bone volume (BV/TV) tended to be lower for HU compared with CTL rats (p = 0.051). No differences in trabecular thickness could be observed.
Values with the same sign (# or ¶) are significantly different from each other (Student's t-test, p < 0.05).
BV/TV, bone volume/tissue volume; Tb.Th, trabecular thickness; Tb.Sp, trabecular separation; Tb.N, trabecular number; HU, hindlimb unloading condition; CTL, control condition.
Molecular analysis of peri-implant healing tissue
All except one implant were bicortically installed with a good primary stability. Neither infection nor bone fracture or implant mobility could be observed at harvest. Harvesting of the tissue in the implant TRA was performed in a standardized way: the perforation of the upper and lower cortex by means of a befitting trephine burr and the implant retrieval itself were highly reproducible acts. Occasionally sampled cortical bone shells could be easily excluded from the tissue of interest. The average total RNA yield was 9.3 (±1.3) μg per implant. Spectrophotometer absorbance ratios at 260/280 ranged between 1.62 and 1.93. The RNA integrity was demonstrated by a sharp distinction of clear 18S and 28S ribosomal RNA.
Quantification of gene expression of Hif-1α, VEGF-A, Angpt1, Epas1, FGF-2, TNF, IL-11, Acp 5, and TNFSF11 was performed using the comparative threshold cycle method (ΔΔCt) with 18S as the endogenous reference. Different ways of data normalization allowed investigation of the effect of (i) implant surgery and installation and (ii) of the bone changes evoked by HU on expression of the aforementioned genes in the peri-implant tissue. The idea behind the first approach originates from the anatomy of the implantation site. The implant was installed in the proximal tibia, a site consisting of few trabeculae and a great amount of bone marrow, surrounded by compact bone. Besides the osteoblasts originating from the endosteum and from the proximal metaphyseal trabecular bone, the bone marrow tissue surrounding the implant was thought to have contributed to a large extent to the tissue regeneration in the implant cavity. Therefore, to investigate the impact of implant surgery and its installation on the expression level of the genes in the TRA, the data were normalized to the respective expression levels in the bone marrow tissue (Fig. 4a). The expression of all except Angpt1 gene markers tested in the peri-implant tissue increased after implant installation. A significant upregulation in response to implant surgery was noted for VEGF-A, Epas1, and IL-11 for both CTL and HU group (VEGF-A: 44.1- and 167.6-fold increase [p = 0.004 and p < 0.001, respectively]; Epas1: 41.0- and 33.3-fold change [p < 0.001 and p < 0.005, respectively]; and IL-11: 3.3- and 6.2-fold increase [p = 0.028 and p = 0.037, respectively] for CTL and HU, respectively). For the CTL group, a significant upregulation in response to implant surgery was observed for TNFSF11 (8.9-fold change; p = 0.003), and a significant downregulation (0.34-fold; p < 0.001) for Angpt1.
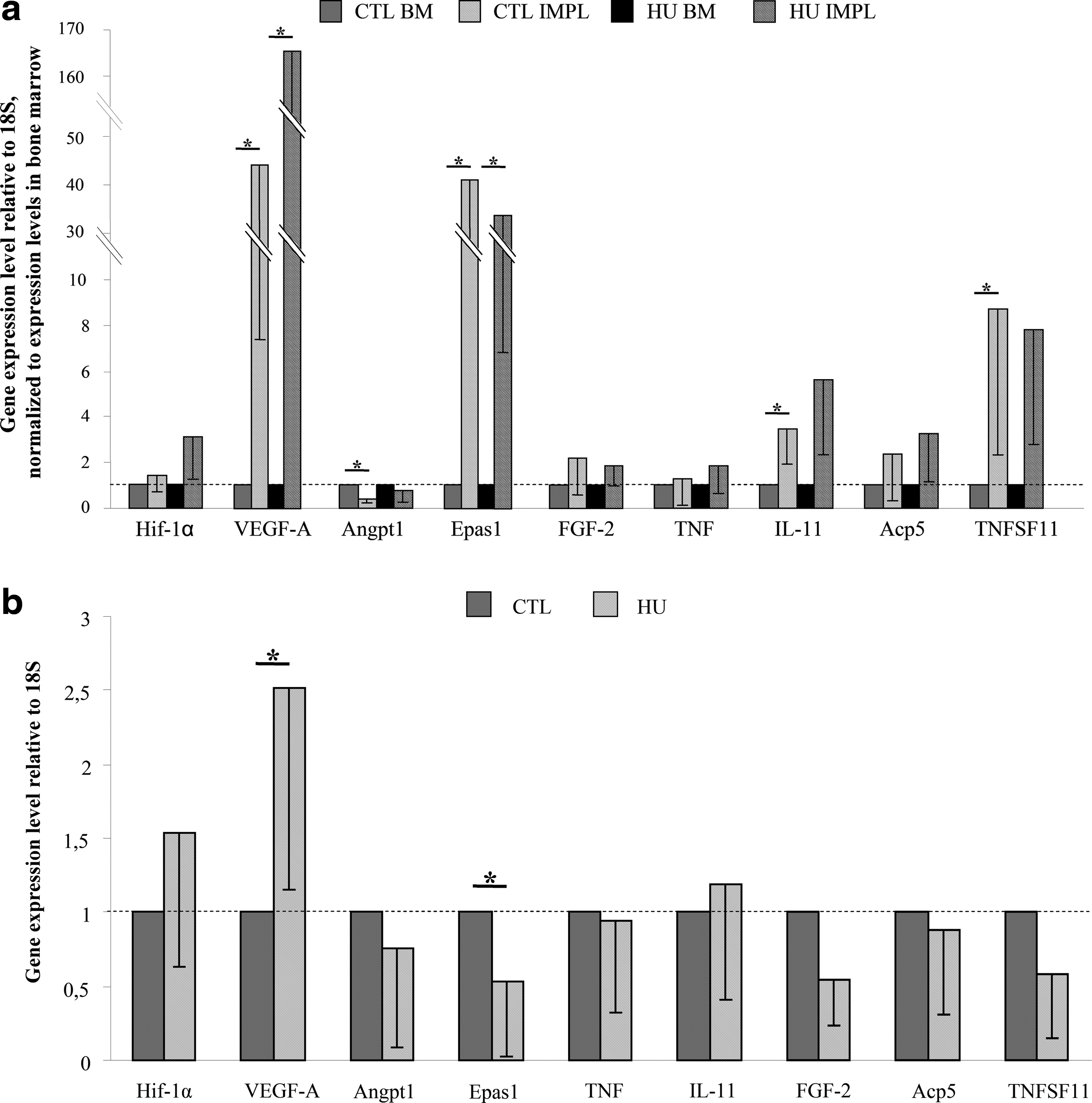
To investigate the impact of the bone changes evoked by HU on the gene expression levels, the data for HU peri-implant regenerating tissue were normalized to the respective expression levels in CTL peri-implant regenerating tissue (Fig. 4b). Impaired bone conditions significantly upregulated VEGF-A expression (p = 0.0041) and significantly downregulated (p = 0.049) Epas1 expression, with a 2.52-fold and a 0.54-fold change, respectively. No differences in expression of the markers related to inflammation and bone resorption could be observed.
Discussion
Our ultimate objective is to explore the mechanism by which titanium implant osseointegration in its initial phase is affected by the host bone properties. To this aim, we implemented a model characterized by (i) bone loss evoked by skeletal unloading and (ii) implantation of an on-purpose-designed implant with a well-defined recess from where regenerating bony tissue can be harvested.
An osteopenic bone condition for investigation of initial implant osseointegration was induced by hindlimb unloading. However, from a clinical point of view, ovariectomy-induced osteoporosis with accompanying skeletal responses similar to those in postmenopausal women 32 and with deficient implant osseointegration in the establishment stage 24 seems to be more relevant. Besides, implant survival and success optimization is highly required in irradiated and uncontrolled diabetic situations.33,34 The strategy of HU as the choice of experimental implant model was dictated by the following rationales: (i) confounding systematic, hormonal, and pharmacological factors can be excluded; (ii) the bone changes evoked by hindlimb unloading are mainly associated with a depression in bone formation,27–29,35 whereas estrogen deprivation predominantly upregulates osteoclastic activity. 36 With the aim of focusing on tissue regeneration in the implant surroundings and at the implant surface, the osteopenia model with marked impairment of the bone formation process was selected; (iii) mechanical loading plays an important role in bone homeostasis. Likewise the facts that bone loss can be counteracted and the bone mechanical properties can be improved by physical exercise,37,38 mechanical stimulation of an implant can enhance and accelerate its osseointegration.2,3 Recent experimental studies by our group using a calibrated external loading device have focused on the identification and the role of the individual mechanical parameters (nature, amplitude, frequency, duration, distribution, etc.) composing the controlled loading regime in the implant osseointegration process.39–41 Extending this setup to the HU model is particularly promising for further exploration of the role of the mechanical parameters involved in mechanical-mediated bone tissue differentiation and adaptation at the implant interface because any mechanical stimulation of the implant by physiological loading of the hindlimbs (except from muscles activity) is excluded.
Using μCT imaging, this model of disuse osteopenia was validated. Absence of mechanical loading by gravity for 9 days resulted in a decreased number and in an increased spacing of the bone trabeculae in the proximal tibia of the rat. There was a tendency toward a lower percentage of bone volume for 9-day HU compared with CTL. These results are in line with the study of David and co-workers, 26 reporting bone loss after 7 days for hindlimb unloaded rats, together with a reduction of Tb.N and an increase in Tb.Sp compared with baseline. These bone changes became significantly different with control rats on day 14. In the present study, a titanium implant was installed 7 days after the onset of HU. Apparently, implant surgery additional to HU did not alter the animal's adaptation to HU and its growth, as shown through video monitoring and body weight tracking. Also, the pattern of the bone adaptation process to microgravity conditions was unchanged in the postimplantation period, and 9-days skeletal unloading was sufficient to create a condition with adversely affected bone microarchitecture for investigation of initial implant osseointegration. Moreover, the osteopenic bone conditions evoked did not jeopardize the primary implant stability—the prerequisite for successful implant osseointegration—neither did they increase the risk for bone fractures related to the implant surgery.
The shortage of available experimental models has been a limitation in investigating quantitatively the molecular determinants that regulate titanium implant osseointegration. When conceptualizing the implant, the feasibility of analysis of the peri-implant regenerative tissue at the genetic scale together with a close mimicking of the clinical reality was aimed for. The implant is characterized by a cylindrical shape, partly screw-threaded to provide a good implant anchorage into the bone and partly indented to provide a well-defined healing compartment from where tissue differentiation and de novo bone formation can be investigated. Moreover, standardized tissue harvesting and a quantitative molecular evaluation assay of the differentiating tissue are feasible, as shown by our first results. Besides providing molecular data on titanium implant osseointegration, the system is promising for evaluation of methods to improve osseointegration such as implant surface modifications, drug responses, or controlled implant loading.
To the knowledge of the authors, this is the first in vivo report studying quantitatively the molecular players during initial titanium implant osseointegration in compromised bone. As a proof of concept, the early—that is, 2 days postimplantation—tissue response in the implant's surroundings was investigated in HU and CTL host bone. Implant installation provoked an upregulation of all tested cytokines, osteoregulating growth factors, and vascular factors (except for Angpt1) in both groups at 2 days postimplantation. This result is indicative for a physiological process of wound repair. The most elevated expression level changes were noted for the angiogenic genes VEGF-A and Epas1, confirming the neovascularization stage as the initial and primordial step in bone regeneration. 42 Investigation of the importance of the bone changes evoked by disuse on the gene expression levels demonstrated that only the angiogenic phase in peri-implant bone regeneration was involved. Expression of the genes implicated in the processes of inflammation and bone resorption during initial osseointegration of a titanium implant was shown not to be affected by the bone condition. At 2 days postsurgery, a marked upregulation of VEGF-A (p = 0.005) in the peri-implant healing tissues was observed in the HU animals. Limited O2 availability owing to a decreased blood flow in the resident vasculature in response to unloading 43 might be an explanation for the induction of VEGF-A. Hif-1α and Epas1 (synonym Hif-2α) are key markers of hypoxia and are involved in the formation of new blood vessels via the secretion of VEGF-A during wound healing.44,45 The apparent discrepancy between expression of Hif-1α (upregulated for HU; nonsignificant p = 0.058) and Hif-2α (downregulated for HU; p = 0.049) has several potential explanations. Although Hif-1α and Hif-2α are structurally closely related, their expression pattern is different 46 (HIF-1α ubiquitously expressed, whereas Hif-2α restricted to specific cell types, in particular to vascular endothelial cells 47 ). Further, some genes are activated by either Hif-1α or Hif-2α, whereas others are only activated by one or the other.48,49 Further investigation is needed to determine whether these expression alterations will be translated into an elevated proteomic secretion of angiogenic factors at the interface of an implant installed in compromised bone.
In conclusion, the present study validated a new experimental model for investigation of implant osseointegration in compromised bone conditions. A specifically designed implant presenting a circumferential recess enabling standardized harvesting of regenerating peri-implant tissue was developed. The isolated tissue was shown to be of good quality for generation of mRNAs suitable for molecular analyses. In the model, osteopenia was created in a reproducible manner by skeletal unloading. The obtained data highlight the great, though untapped potential of the model for studying of the effect of controlled mechanical loading on the process of implant osseointegration because of the exclusion of any mechanical stimulation (except from muscles activity) of the implant by physiological loading. Finally, in a first short-term study, altered expression of the angiogenic markers and unaffected expression of the inflammatory and bone resorption markers were observed.
Footnotes
Acknowledgments
This work was supported by the French Institute for Dental Research (IFRO, France) and the Research Fund of the Katholieke Universiteit Leuven (KUL, Belgium–OT/07/059). The implants were kindly provided by GC Corporation, Tokyo, Japan. The authors are especially thankful for the excellent technical support and assistance from C. André, L. Begot, X. Butigieg, and S. Renault.
Disclosure Statement
No competing financial interests exist.