
Abstract
Angiogenic and inflammatory responses to biodegradable scaffolds were previously studied using the dorsal skinfold chamber for testing different scaffold materials. In this model, the angiogenic response originates from the soft tissue of the skin. Herein, we introduce a new model that allows the study of developing microcirculation of bone defects for testing tissue-engineered constructs. A bone defect was prepared in the femur of Balb/c mice by inserting a pin for intramedullary fixation, and a custom-made observation window fixed over the defect allowed constant observation. This study included three different groups: empty defect (control), defect filled with porous poly(
Introduction
Therefore, angiogenesis can be defined as a vital prerequisite for bone repair since the activity of osteoblasts and osteoclasts depends on sufficient ingrowth of vessels. The dorsal skinfold chamber represents a well-established model for angiogenic and inflammatory responses to different biodegradable scaffolds in vivo, and this method has been a successful advancement in the study of microcirculatory properties of various tissues in conjunction with the application of intravital fluorescence microscopy. Using the dorsal skin fold chamber in mice, different three-dimensional (3D) scaffold materials showed adequate biocompatibility and promoted vascular ingrowth comparable to that triggered by bone transplants.9–12 The growth of microvessels in this model originated from the surrounding soft tissue. However, to test the suitability of bone substitutes for grafting bone defects, the analysis of osseointegration and thus vascularization in an osseous environment is an indispensable requirement. Recently, different bone chamber models have been described. The cranial window for intravital microscopy was first described by Forbes in 1928 with the intention of observing pial vessels. 20 Different applications for this cranial window have subsequently been described. In addition to observing the angiogenesis of malignant tumors, 21 Sinikovic et al. described a model that is suitable for assessing the vascularization of 3D osseous substitutes in the desmal bone. 22 Different pathways of osteogenesis and fracture repair have been described for chondral and desmal bone.23,24 Hansen-Algenstaedt et al. described a “femur-window” in c57-black mice for intravital observation of chondral bone. 25 To observe the vasculature of cancellous bone, the corticalis was ground down by 50 μm on an area of 5×1 mm with a scalpel to establish a plane area, and bone defect healing was observed over 12 days. This technique preserved the mechanical properties of the bone, but it was not possible to integrate any tissue-engineered construct into the defect. According to the critical size defect described by Schmitz and co-workers, Garcia et al. developed a reliable nonunion model for mice. A 1.8-mm gap resulted in 100% nonunions after 10 weeks.24,26 This model relied on the radiological and histomorphological analysis of end-point samples; therefore, in vivo data describing the continuous growth of microvessels in the defect were not generated.
The aim of the present study was to develop a bone chamber suitable for the in vivo analysis of different biodegradable scaffold materials by utilizing long-term intravital fluorescence microscopy. This model should be able to integrate different scaffolds in between the defect. Combining the observation window and the nonunion model, this modification allowed the repetitive observation of the angiogenic and inflammatory responses of different materials for bone regeneration in chondral bone.
Materials and Methods
Observation window
The observation window was produced by the research workshop of Hannover Medical School, Hannover, Germany. It was shaped out of 1 piece of high-tensile sterilizable steel. The main part of the observation window was a steel cylinder with an inner diameter of 4 mm and an outer diameter of 5 mm containing a circular steel plate (Fig. 1A–D) at the top (observation side) and base ends (femoral side). After femoral fixation, the soft tissue could be adjusted around the steel cylinder flanked by top and base end plates. Femoral fixation was performed by sutures through the holes and around the femur to preserve periostal blood supply.
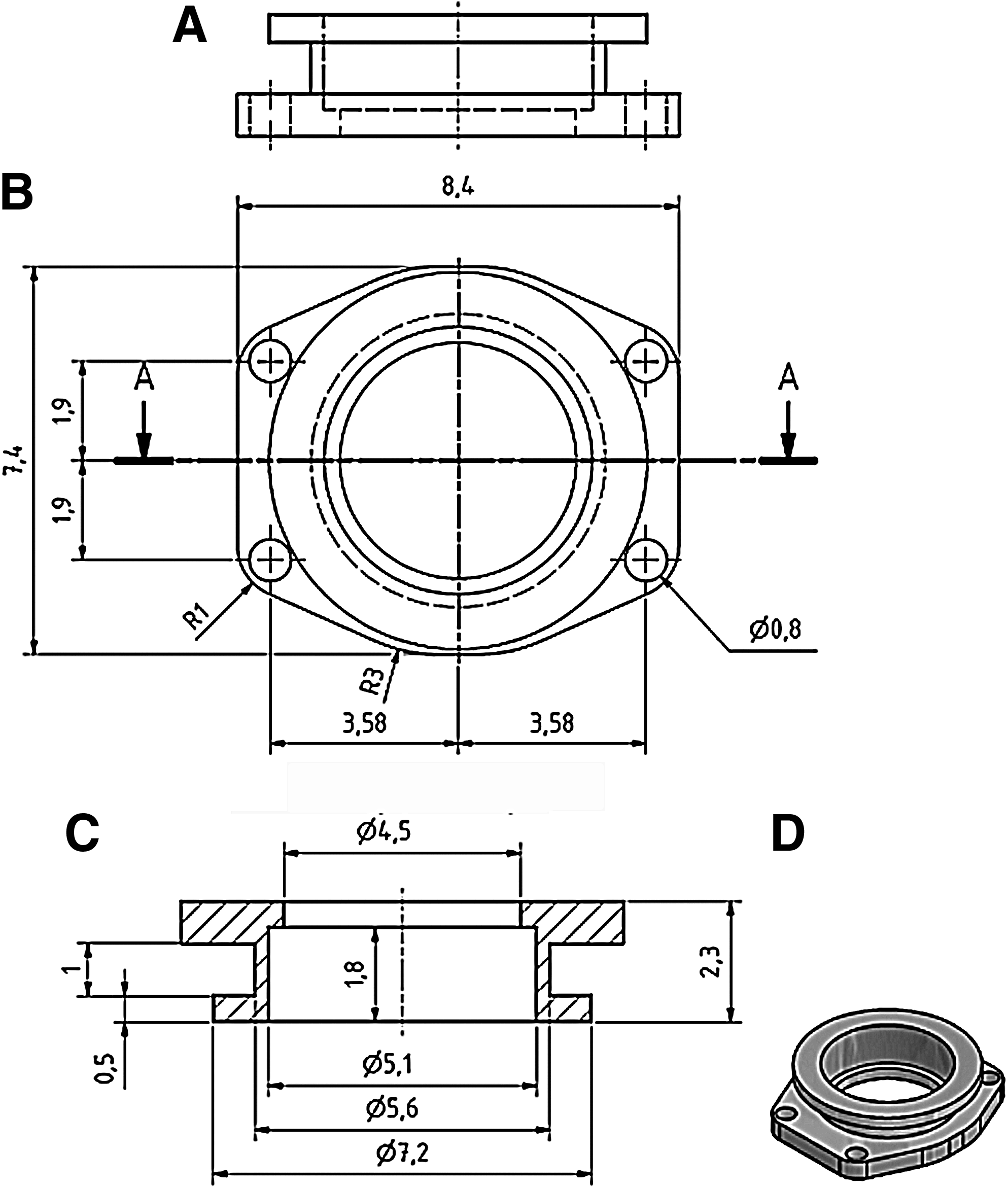
Technical drawing of observation window design: lateral view
Animals
The experiments were conducted in accordance with the German legislation on protection of animals and the NIH Guidelines for the Care and Use of Laboratory Animals (NIH Publication #85–23 Rev. 1985) and were approved by the local governmental animal care committee. The study involved 12–16-week-old female Balb/c mice with a body weight of 22–25 g. The animals were housed 1 per cage at a room temperature of 22°C–24°C and a relative humidity of 60%–65% with a 12-h day–night cycle. Mice had free access to tap water and standard pellet food (Altromin, Lage, Germany) throughout the experiment.
Surgical procedure
The skin of the posterior leg was shaved and depilated after anesthesia by intraperitoneal injections of 0.1 mL saline solution per 10 g bodyweight (bw) containing 90 mg/kg bw ketamine hydrochloride (Ketavet®; Parke Davis, Freiburg, Germany) and 25 mg/kg bw dihydroxylidinothiazine hydrochloride (Rompun®; Bayer, Leverkusen, Germany). The surgical procedures were performed under aseptic conditions while preserving body temperature by using a heating plate (ThermoLux; Witte + Sutor, Murrhardt, Germany). The instruments and observation window were sterilized and the skin was disinfected with Octenisept© solution (Schülke & Mayr, Norderstedt, Germany). Thereafter, the animal was placed onto a sterile drape. The surgical procedures were performed using a stereo microscope (MZ6; Leica Mikrosysteme, Wetzlar, Germany). A 14-mm skin incision was made approaching the femur from lateral. The femur was carefully exposed by blunt dissection between the flexor and extensor muscles to ensure muscle functionality after window preparation. After exposition and medial luxation of the patella, a small hole was drilled into the intercondylar region of the distal femur, and a steel pin was inserted for intramedullary fixation. After shortening the pin, a defect was prepared in the middle of the femoral bone approaching the previously inserted pin. The longitudinal distance of the defect was 2 mm. Scaffolds were inserted into the defect or the defect was left empty. The observation window was fixed by suture (2–0 vicryl; Ethicon, Norderstedt, Germany) to the femur. Subsequently, the skin was draped around the window and sutured with 4–0 vicryl (Ethicon) (Fig. 2A–D). The mice were left under observation beneath a heating lamp until they were completely awake.

Window preparation.
Scaffold fabrication and implantation
PLGA scaffold fabrication has been described in detail elsewhere. 27 The scaffolds were manufactured using a 3D Bioplotter™ operated by PRIMCAM software (Primus Data, Einsiedeln, Switzerland). PLGA granules (Resomer 824; Boehringer, Ingelheim, Germany) with an 80:20 ratio of lactide:glycolide were melted in the heatable dispenser of the 3D Bioplotter, which was then moved in all three dimensions (x/y velocity: 300 mm/min, z velocity: 200 mm/min; internal diameter of the application needle: 0.25 mm, pressure: 5 bar). Scaffolds of 2×2×1 mm were produced. A strand thickness of 250 μm was chosen and a height of 500 μm was used for each layer. The direction of each new layer was changed by 90°. This procedure created a 4-layer mesh with a distance of 250 μm between layers.
The accuracy of scaffold fabrication was micromorphometrically verified using light microscopy (DM4000B; Leica Mikrosysteme, Wetzlar, Germany) and image analysis software (analySIS; Soft Imaging System, Muenster, Germany).
Beta-tricalcium-phosphate (β-TCP) scaffolds were prepared from commercially available β-TCP blocks (chronOs®; Synthes, Solothurn, Switzerland). β-TCP provides a porosity of 60%–80% and a macro-pore size ranging from 100 to 500 μm wherein 95% of the macro-pores are interconnecting. The blocks were cut into pieces of 2×2×1 mm, corresponding to the size of the PLGA scaffolds by using a microdrill (W&H Dentalwerk GmbH, Buermoos, Austria) equipped with diamond-coated cut-off wheels and rotating burrs (Komet Dental; Gebr. Brasseler GmbH & Co. KG, Lemgo, Germany). The graft materials used were endotoxin-free, as specified by the appropriate manufacturers.
Intravital fluorescence microscopy
For in vivo microscopy, the mice were anesthetized as described above and immobilized in a custom-made stereotactic frame. After intravenous retrobulbar injection of 0.1 mL of 5% fluorescein-isothiocyanate-labeled dextran (FITC-dextran, MW 150,000; Sigma, Deisenhofen, Germany) for contrast enhancement of blood plasma and 0.1 mL of 0.1% rhodamine 6G (Sigma) for direct observation of leukocytes, intravital fluorescence microscopy was performed using a modified Zeiss Axiotech microscope equipped with a 100-W mercury lamp and an illuminator with blue, green, and ultraviolet filter blocks (Zeiss, Jena, Germany) for epi-illumination. The microscopic images were recorded by a charge-coupled device video camera (FK-6990, COHU; Prospective Measurements, San Diego, CA) and were transferred to a DVD recorder (LQ-MS 800; Panasonic, Hamburg, Germany) for off-line evaluation. Long-distance lenses (10×and 20×magnifications) were used for displaying the images on a 14-inch video screen (Panasonic, DVD video recorder LQ-MD 800E; Matsushita Electronic Industrial Co Ltd., Osaka, Japan).9–12
Video analysis
Quantitative off-line analysis of the recorded data was performed using the computer-assisted image analysis system CapImage (Zeintl, Heidelberg, Germany). Leukocyte–endothelial cell interaction, microhemodynamics, and macromolecular leakage were assessed at a magnification of 400×in four different microvascular regions of interest (ROIs) in the border zone of the scaffolds and the corticalis. In control animals, four comparable ROIs were analyzed in defects that were not grafted with any material. In each ROI, 1–3 venules (inner diameter,×20–40 mm) were selected for measurements. Leukocytes were stained in vivo with 0.1% rhodamine 6G and classified according to their interaction with the vascular endothelium as adherent, rolling, or free-flowing cells as described.9–12 Adherent leukocytes were defined in each vessel segment as cells that did not move or detach from the endothelial lining within a specified observation period of 20 s, and are given as the number of cells per square millimeter of endothelial surface calculated from the diameter and length of the vessel segment studied, assuming a cylindrical vessel geometry. Rolling leukocytes were defined as cells moving with a velocity <40% of the centerline velocity, and are given as number of cells per minute passing a reference point within the microvessel.
Macromolecular leakage was assessed as a parameter of microvascular permeability after an intravenous injection of the macromolecular fluorescent dye FITC-labeled dextran (MW, 150,000) by determining densitometrically gray levels in the tissue directly adjacent to the venular vessel wall (E1), and in the marginal cell-free plasma layer within the vessel (E2). Extravasation (E) was calculated as E=E1/E2. Angiogenesis was analyzed at a magnification of 400×in four different microvascular ROIs in the previously described border zone.
Experimental protocol
For intravital fluorescence microscopy, 24 Balb/c mice were equipped with an observation window. The scaffolds consisting of PLGA (n=8) or β-TCP (n=8) were implanted into the bone defect taking care to avoid contamination, mechanical irritation, and damage of the chamber. In addition, 8 control animals without any material implantation into the femoral defect were prepared. The macroscopic appearance of the observation window preparations and the implanted scaffolds were documented daily. Intravital fluorescence microscopic analysis of leukocyte–endothelial cell interaction, microhemodynamics, macromolecular leakage, and angiogenesis was performed 6, 10, 14, 18, and 22 days after surgery.
Histology
Histological examinations were performed at the end of the in vivo experiments. For light microscopy, specimens were fixed immediately in 3% buffered formalin, dehydrated, and embedded into methylmethacrylate. Sections (thickness, 30–70 μm) of the embedded specimens were prepared using a diamond-edged blade in a rotating saw (Leitz, Hamburg, Germany) perpendicular through the center of each implant and adjacent areas covering approximately two-third of the material. Surface staining (methylene blue and alizarin red) was employed according to standard procedures to evaluate the histological specimens for vascularity and structure of the newly formed bone. The estimation of the newly formed bone was performed semi-quantitatively by 2 examiners (percentage of gap bridging: 0, no new bone; 1, <25%; 2, <50%; 3, <75%; and 4, >75%).
Statistical analysis
Results are expressed as means±standard error of the mean. Differences between groups were assessed by one-way analysis of variance (ANOVA) and differences within each group were analyzed by one-way repeated measures ANOVA. Student-Newman-Keuls or Dunn's post-hoc tests were used to isolate specific differences. Results with p<0.05 were considered significant.
Results
After waking from anesthesia, animals recovered from surgery within 12–24 h showed species-specific behavior, and no signs of severe pain or stress were observed. All animals were able to bear at least partial weight on their treated legs after the surgical procedure. In controls (no material implanted into the femoral defect), only a hematoma and no angiogenesis was detected throughout the observation period (data not shown).
Inflammatory response
The implantation of PLGA scaffolds caused temporary leukocytic inflammatory response in the postcapillary venules (Fig. 3A) as demonstrated by an increased number of rolling leukocytes at days 6, 10, and 14. Leukocyte counts then returned to the level measured directly after scaffold implantation. In contrast, animals with β-TCP scaffolds showed a significantly higher number of rolling leukocytes at days 10, 14, 18, and 22 compared to PLGA scaffolds. Leukocyte counts decreased from day 18 but did not reach baseline values (Fig. 3A).

Numbers of rolling leukocytes (cells/min)
Leukocytes adherent to the endothelium of the postcapillary venules moderately increased in the immediate vicinity of the scaffolds from day 6 to day 10 after implantation (Fig. 3B). The inflammatory leukocytic response was accompanied by increased macromolecular leakage from the postcapillary venules (Fig. 3C). The elevated permeability did not normalize but rather increased during the entire 22-day observation period in both scaffold types.
A comparison of β-TCP and PLGA scaffolds showed a more pronounced recruitment of adherent leukocytes to β-TCP scaffolds, similar to the characteristics observed for leukocyte rolling (significant at days 10 and 14, Fig. 4A, B and Fig. 5E, F [p<0.05]). However, leukocyte adherence decreased to double baseline levels in both PLGA and β-TCP scaffolds on day 22.

Intravital fluorescence microscopy of β-TCP
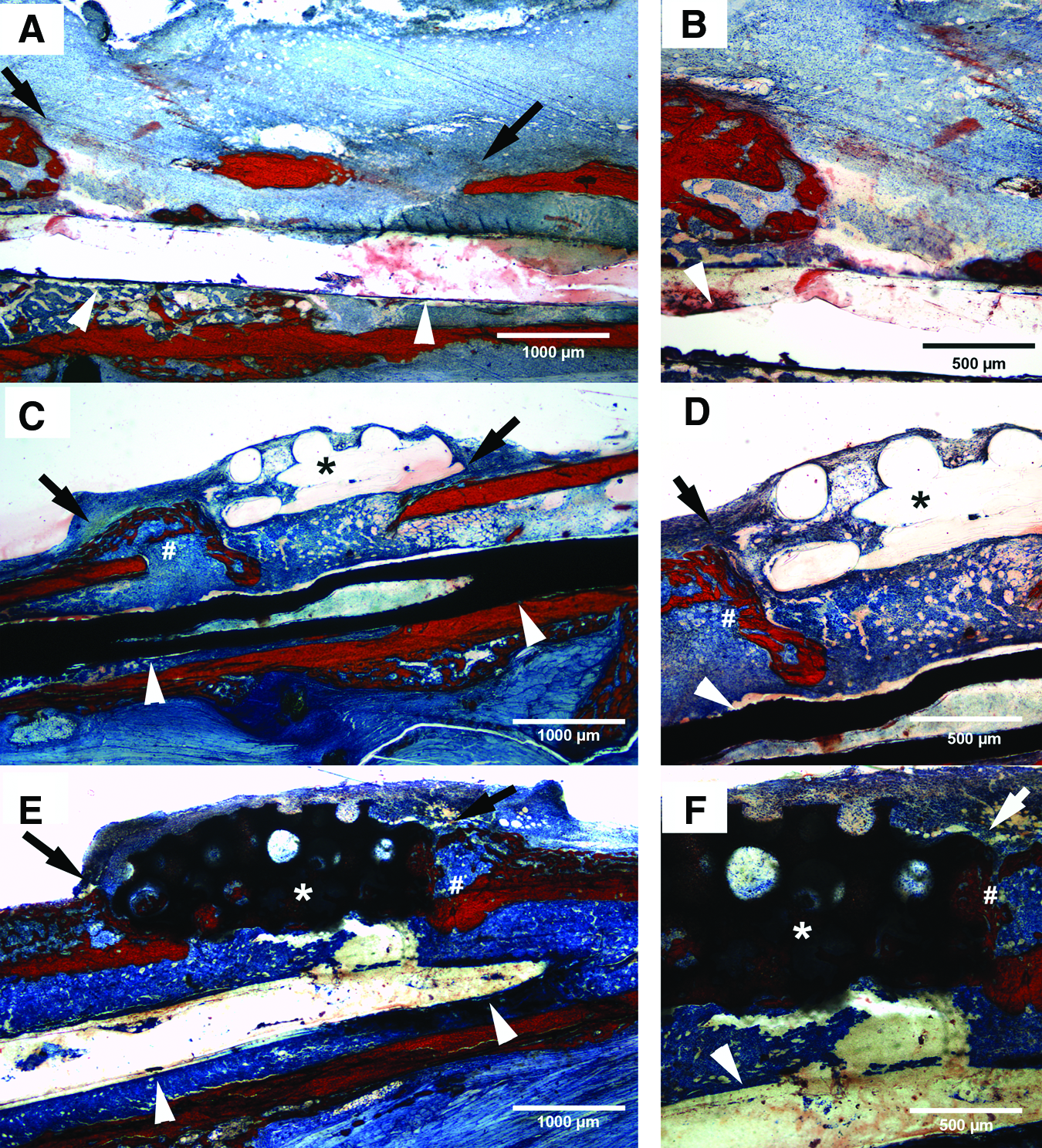
Alizarin/methylene blue-stained cross sections of empty defects
Angiogenesis and neovascularization
The control group showed no signs of angiogenesis at any time point, neither in the center of the observation window nor in the immediate vicinity of the frame (data not shown). In both scaffold types, the first signs of angiogenesis were detectable at day 6 after implantation and consisted of capillary dilation and formation of capillary buds and sprouts. These sprouts were interconnected and formed new red blood cell-perfused microvascular networks within 22 days (Fig. 4A–F). The quantitative analysis of angiogenesis demonstrated a significantly increased density of the microvascular network that grew into β-TCP scaffolds compared to PLGA scaffolds throughout the observation period (Fig. 6).
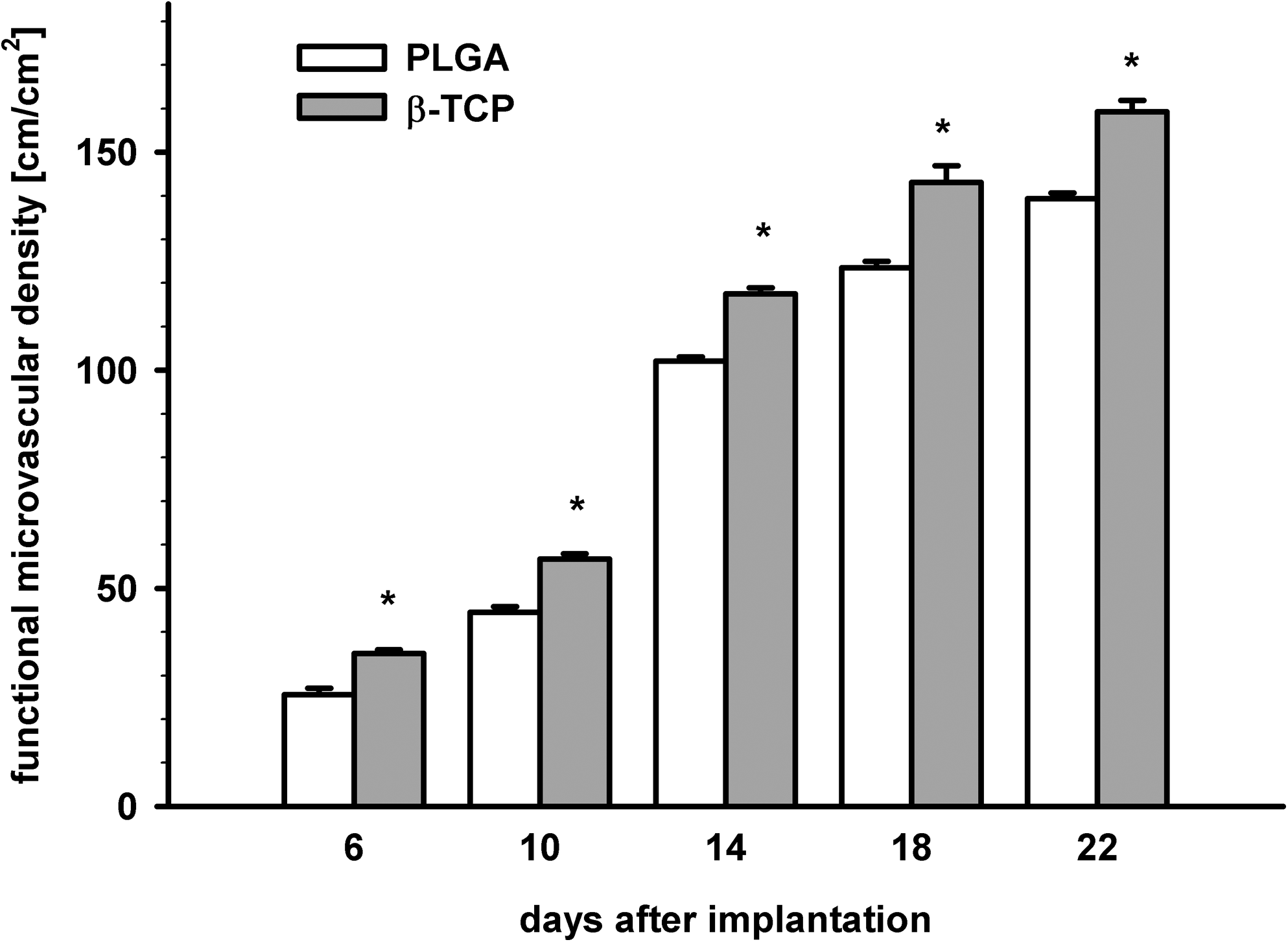
Functional microvascular density of newly formed microvessels expressed in cm/cm2 in PLGA (white bars) and β-TCP scaffolds (gray bars) on days 6, 10, 14, 18, and 22 after implantation into femur defects in Balb/c mice. No angiogenesis was detectable in controls; therefore, this group was not included in the figure. Values represent means±SEM. *p<0.05 versus PLGA scaffolds.
Histological examination
Histological examination on day 22 after scaffold implantation confirmed our intravital microscopic findings. All scaffolds exhibited a vascular host tissue response with the formation of a densely vascularized granulation tissue despite distinct infiltration of inflammatory cells and some giant cells. This host tissue response is evidence of adequate engraftment of the scaffolds in host tissue. The controls showed no signs of vascularization.
Despite that no angiogenesis was detected in the controls, first signs of new bone formation were visible (Fig. 5A, B). In addition, bone growth was detected at the border zone between the femur and PLGA scaffolds (Fig. 5C, D) growing toward the scaffold without intergrading it. Groups containing β-TCP scaffolds were characterized by a sustained formation of new bone tissue and distinct ingrowths of bone into the scaffold pores (Fig. 5E, F). The semi-quantitative estimation presented a significantly stronger bone ingrowth induced by β-TCP-scaffolds compared to that induced by PLGA-scaffolds (Fig. 7).

Semi-quantitative estimation of newly formed bone (0, no bone; 1, <25%; 2, <50%; 3, <75%; and 4, >75% defect bridging). Values represent means±SEM. #p<0.05 versus controls; *p<0.05 versus controls and PLGA scaffolds.
Discussion
Different models for intravital microscopy have been established. The dorsal skinfold chamber is the most common model for assessing the angiogenic and inflammatory responses to the implanted material or tissue based on the surrounding soft tissue. 28 In this model, all recorded parameters are based on the soft tissue response of the dorsal skin. However, estimating the suitability of bone substitutes also requires the analysis of integration and vascularization in an osseous environment.
Therefore, aim of the present study was the development of a bone chamber for long-term intravital microscopy comparing different biodegradable scaffold materials. We introduced a novel approach to intravital microscopy of tissue-engineered constructs by combining the observation window described by Hansen-Algenstaedt et al. 25 and the nonunion model described by Garcia and Co-workers.26,29 The design of the observation chamber made the bone defect accessible and the implantation of different materials suitable for bone regeneration possible. This newly developed model allowed the direct observation of angiogenesis and inflammation in chondral bone defects as a response to the implanted material.
The 3D scaffolds composed of either PLGA or β-TCP induced a strong angiogenic reaction of the surrounding bone tissue. In marked contrast to this observation, no angiogenesis was detected in empty defects. However, this can be attributed to the lack of a guiding structure and, thus, meets the definition of a critical size defect. 24
Recently, our group showed a direct comparison of β-TCP and PLGA scaffolds in terms of inflammation and vscularization. 30 The technique of intravital fluorescence microscopy allows a comparison of results obtained with the skinfold chamber and the here presented new model, since identical parameters were recorded. Both scaffold materials showed the induction of vascular growth. In both models the angiogenic and inflammatory effect induced by β-TCP and PLGA was comparable, but the onset of angiogenesis was delayed until the sixth day after implantation, which might have resulted from the occurrence of hematomas during defect preparation. Implantation of β-TCP caused a strong increase in activated leukocytes at day 14 compared to that observed with PLGA scaffolds. Ghanaati et al. demonstrated that variations in the physical properties of β-TCP can influence the extent of the inflammatory reaction. 31
Both scaffold materials induced the formation of new bone material that grew into the defect area. This inducing effect was more pronounced for β-TCP, where the pores of the scaffold material were partially filled with the newly grown bone, than for PLGA, where new bone formation did not occur in the scaffold pores. This observation is comparable to other recent results such as the prospective study using an ovarian critical size defect model conducted by Haberstroh et al. The direct comparison between PLGA and β-TCP showed that β-TCP induced formation of more new bone and showed more ingrowth into the scaffold area compared to that with PLGA. 32
In contrast to our newly developed model, which made an observation period of 3 weeks possible, the results from Haberstroh et al. were obtained after 14 weeks. Although first signs of bone growth were detected histologically at the end of the observation period in our experimental setting the intention was the observation of changes in the microvasculature after implantation of scaffold materials. Different methods have been established to observe and quantify the vascularization and mineralization of scaffold materials suitable for bone reconstruction. Microscopic and histological methods allow the analysis of vascular growth and inflammatory parameters, but in contrast to intravital microscopy, fixation of tissue is required and therefore repetitive observations over a period of the same animal are impossible.33,34 The same holds true for angiography, which also requires fixation and allows only end point studies. 35 Further, the resolution of angiography is limited by the size of the tracer used, and therefore small vessels could not be detected. 36 In terms of spatial resolution and the possibility of analyzing the same experimental animal repetitively microcomputed-tomography is comparable to intravital microscopy, 37 but it does not allow the measurement of inflammatory parameters, which are essential for evaluation of biocompatibility of the scaffold material.
For the experimental analysis of vascularization of scaffold materials and in the field of tissue engineering, there is not just one ideal method that allows quantification of all necessary parameters. The ideal method depends on the type of experiment and the aim of the study. Our here presented new bone chamber for intravital observation of scaffold materials for bone reconstruction by fluorescence microscopy is especially suitable for the analysis of early events after implantation. The observation window design allows quantitative analysis of the morphological and functional properties of microcirculation in terms of vascular density, leukocyte-endothelial interactions, and microvascular permeability at a high spatial resolution. Therefore, it is an ideal tool for quantification of the onset of vascular growth and the inflammatory answer of the recipient tissue. The combination of intravital-microscopy with the nonunion model enables the evaluation of the physiological and pathological processes of bone and bone remodeling.
Footnotes
Acknowledgment
This study was granted by the Hannover Medical School, HiLF Nr. 79592005, Hannover, Germany.
Disclosure Statement
No competing financial interests exist.