
Abstract
This article describes the development of a new surgical approach to periodontal treatment. Twenty patients who suffered from bone defects without existing bony walls due to adult periodontitis were treated in three different groups using methods of bone tissue engineering. At that time no surgical technique existed that could be applied to those patients to generate new bone. The periodontal surgeries were performed between 2004 and 2008. All patients received follow-up examinations at 6, 12, and 24 months after surgical procedure. Measured parameters were compared to baseline. The surgical approach and the augmentation material have been improved based on the results of the previous group. This strategy was applied because of the ethical fact that a medical treatment of patients has to be carried out with the knowledge and experience of previous settings. All groups received recombinant human bone morphogenetic protein 2 and platelet-rich plasma. The above-mentioned procedure had been approved in other indications in the field of oral and maxillofacial surgery. The first group underwent conventional muco-periosteal flap technique and obtained an augmentation with absorbable collagen sponge (ACS). The second and third groups were treated using endoscopically assisted microsurgery due to wound healing disturbances that appeared in the first group. The augmentation was carried out with demineralized bone matrix (DBM) instead of ACS (group 2) or tricalciumphosphate as a further development instead of DBM (group 3). The radiological control 12 months (group 1), 18 months (group 2), and 2 years (group 3) after surgery proved the following results—first group: 1.7 mm (average) vertical bone development (VBD); second group: 2.5 mm (average) VBD; third group: 3.2 mm (average) VBD. These results of single patient treatment open new ways into periodontal surgery. They have to be confirmed by prospective case series and multicenter studies.
Introduction and Scientific Background
Conventionally, the initial therapy includes professional dental cleaning and educating the patient in proper oral hygiene, scaling, root planning, and killing of bacteria. In cases of bone defects with loss of soft tissue with the resultant reduction of attached gingiva (gingiva in close contact to the dental roots) different surgical techniques were described. All of them aimed at recreating the initial healthy situation as optimally as possible. It must be mentioned that the below listed techniques need at least two or three bony walls to produce new bone.
The standard techniques in periodontal surgery are as follows:
1. Guided tissue regeneration (GTR) with the use of different types of membranes which cover the bone defect and protect it from insertion of soft tissue in combination with wound healing1,2
2. Implantation of hard and soft tissue:
The common surgical approach of the above appears to be a conventional muco-periosteal flap technique. The papillae are cut and the flaps are prepared both at the buccal and oral sides. Because of the narrow situation at the end of the papillae the reunification of these parts of the soft tissue appears to be the major difficulty. Wound healing disturbances occur in a high amount of surgical treatments in this position.2,11
Some authors report on adding platelet-rich plasma (PRP) to the augmentation material to enhance the bone development and healing of the soft tissue.12–14
The use of PRP therapy in surgery was introduced in the late 1990s. There is still controversial discussion regarding the use of PRP and whether or not it favors bone regeneration.15,16
However, all authors agree that platelets are the main regulators of the inflammatory phase and play an essential role in the proliferation and differentiation phase. 17
Today there seems to be a consensus on the following facts and influence concerning PRP:
1. Importance of controlled release systems of growth and differentiation factors using biomaterials in combination with PRP 18
3. Inhibition of osteoclast activation 21
4. The enhancement of bone density adding PRP to a suboptimal doses of recombinant human bone morphogenetic protein 2 (rhBMP-2) 22
5. The activation of PRP using calcium chloride or/and thromboplastin solution 23
6. Positive effect of PRP in bone regeneration in animal trials and clinical studies in humans24–27
The history of bone regeneration using BMPs instead of bone transplantation dates back to the 1960s. In 1965, Urist wrote about bone growth by induction. 28 A variety of different techniques have been developed in bone tissue engineering during the last 20 years. Meanwhile, many international articles have been published on this innovative treatment.
Zheng et al. 29 reported at an early stage that rhBMP-2 induces endochondral ossification. It supports
1. Proliferation and differentiation of mesenchymal cells into chondroblasts and osteoblasts
2. Production and maturation of cartilage and bone matrix
3. Differentiation of circulating osteoclast precursor cells into osteoclasts
Raida et al. 30 proved that rhBMP-2 promotes vascularization.
In the field of oral and maxillofacial surgery, different authors have reported about newly regenerated bone in animal models and clinical studies in humans using growth factors,31–36 such as rhBMP-2 (INFUSE®; InductOs®; Wyeth Medicine). The other material commonly used is bovine collagen (absorbable collagen sponge [ACS]). INFUSE/InductOs is provided as rhBMP-2 powder and a separate collagen sponge (ACS). Thus, INFUSE/InductOs enables a complete splitting of both parts. We have demonstrated the advantages of using rhBMP-2 in combination with other carrier materials and scaffolds instead of ACS.37–39
Although most of the authors present favorable results using BMPs the disadvantages have to be mentioned. For example,
1. High cost
2. BMPs induce the development of osteoblasts and osteoclasts, which means a contrary development to the main target is also initiated
This negative effect can partly be counteracted by combining the BMPs with PRP. Cenni et al. 21 proved the inhibition of osteoclast activation using PRP.
The release of transforming growth factor-β from PRP seems to be most important for inhibiting osteoclast development. We presented this in a literature overview and compared it with our own experiences in 2011. 39
The delivery of BMPs in the past was predominantly carried out using collagens, for example, the bovine collagen ACS. Thus, this is xenogenic material that causes immunological reactions in 18% of patients. 40 Moreover, ACS is not able to provide suitable structural support for the agglomeration of osteoblasts to reconstruct larger bony defects. 37
Demineralized bone matrix (DBM), a form of allograft, has been applied in bone surgery worldwide. It possesses the properties of osteoinductivity 41 and osteoconductivity. 42 A large body of data obtained from extensive preclinical studies has supported the effectiveness of DBM or DFDBA in human clinical settings. Nevertheless, it is important to mention that DBM products differ concerning their biological properties due to the host environment, the methods of allograft preparation, particle size and shape, and donor selection criteria. DBM functions best in a healthy tissue bed but should be expected to have little impact in an anoxic or avascular tissue bed. 43 Allogenic material such as DBM opens the potential for disease transmission.
Due to the well-known disadvantages of ACS, DBM was used in combination with BMPs. While Lin et al. 44 and Zhao et al. 45 reported on a limited BMP-2 binding ability of DBM, which could be increased using heparin or cyclic thioimidate, Tsiridis et al. 46 proved an optimized osteoinduction using DBM combined with rhBMP-7 compared with DBM alone. These results are supported by Clokie and Sándor 47 in their review of 10 clinical cases with major mandibular defects. They implanted DBM soaked with rhBMP-7 and were successful in growing new bone.
However, no bone development could be achieved in periodontal surgery using DBM.48,49
TCP is an established anorganic augmentation material in bone surgery throughout the world. It is applied in combination with cells, signaling molecules, and autogenous bone.50,51 An important aim implementing modern bone regeneration is the reduction of risks compared with bone transplantation. Therefore, materials that include risks of infection and allergenic reactions should be avoided as far as possible. In the consequence of this, synthetic materials like TCP as matrices have to be preferred to products of allogenic or xenogenic origin.
Materials and Methods
Between 2004 and 2008, 20 patients with 45 periodontal bone defects without existing bony walls were surgically treated. Each of the patients was regarded as a single case, which could not be cured using common care. All patients received comprehensive information concerning rhBMP-2, including off-label use and the fact that the suggested therapy was a new approach in periodontal treatment.
The ethical authorities were aware of this medical treatment. Different to a clinical study this treatment of single cases needed no approval and review, because this is not a structured clinical study. In fact it is the development of a new periodontal therapy.
The presented article has to be regarded as a review on the treatment of 20 patients aged between 43 and 78 years at the time of surgical treatment, an average age of 57 years. Surgical treatment was carried out on 9 women and 11 men; pregnant women and smokers were excluded. All teeth that needed bone development due to a loss of bone >2 mm in vertical dimension were included (molars, premolars, and incisors) in the treatment. Regarding this article only data from those teeth that presented bony defects without existing bony walls by proof of radiograph and optical presentation during surgery were considered. Thus, the preoperative status of defects are comparable.
The surgical approach and the augmentation material have been improved based on the results of the previous group. This strategy was applied because of the ethical fact that a medical treatment of patients has to be carried out with the knowledge and experience of previous settings.
The first group of patients was treated in 2004. In these cases we used the surgical technique well known at that time—the muco-periosteal flap technique. Cuts were made according to the marginal gingiva and through the papillae. The muco-periosteal flaps were separated from the hard tissue. Granulation tissue was removed from the bone defects. Afterward rhBMP-2 (INFUSE; InductOs; Wyeth Medicine) on ACS was implanted and prepared PRP was added. The muco-periosteal flaps were readapted and fixed with interdental stitches. Eight patients belonged to this group, three female and five male, with 18 periodontal defects without bony walls.
The second group was treated in 2005. Due to wound healing disturbances caused by the swelling of ACS in the first group, we developed a new surgical approach—the bridge flap technique to prevent the papillae and avoid dehiscences. This surgical approach had to be carried out endoscopically assisted. Vertical incisions were made and, afterward, the mucoperiostal bridge flap was elevated from the alveolar ridge. After the insertion of the endoscope, the soft tissue was removed using microsurgical instruments. As augmentation material we used DBM (Grafton®; Netherlands Bonebank Foundation) instead of ACS and added rhBMP-2 and prepared PRP. Another reason for replacing ASC with DBM was new information concerning the insufficient structural support provided by ACS. 37 The augmentation was performed endoscopically. This group consisted of five patients, one female and four male, with 11 periodontal defects without bony walls.
The third group of patients was cured between 2006 and 2008. The surgical approach was the same as in the second group with an endoscopically assisted surgical treatment. Instead of DBM we used TCP (Vitoss®; Stryker) as augmentation material in combination with rhBMP-2 and PRP. This change was implemented because of the development of bone tissue engineering in other parts of oral and maxillofacial surgery. The main reasons were the risk of disease transmission caused by DBM and a better structural support provided by TCP. 39 Seven patients belonged to this group, five female and two male, with 16 periodontal defects without bony walls.
Preoperative preparation
The preoperative screening contained x-ray, using analog orthogonal dental radiographs, measurement of pocket depth (PD) at six points per tooth using pocket explorer (mesio-buccal, buccal, disto-buccal, mesio-palatal, palatal, and disto-palatal) and determination of periodontal bacteria using polymerase chain reaction (micro-IDent®; Hain LifeScience). Analyzed bacteria were Haemophilus actinomycetemcomitans, Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythia, Treponema denticola, Peptostreptococcus micros, Fusobacter nucleatum/periodonticum, Campylobacter rectus, Eubacterium nodatum, and Eikenella corrodens Capnocytophaga spec. Samples were taken using sterile paper-tips. All patients received professional dental cleaning, root planning, and education in hygiene. Depending on the results of bacteria assignment, antibiotic therapy was given to them (e.g., Metronidazol, Clindamycin, or a combination of both).
Surgical procedure
All surgical treatments were carried out under analgosedation with local anesthesia and perioperative antibiotic therapy (Amoxicillin 3×1000 mg/day over 1 week or Cephalosporine 400 mg/day over 1 week). As part of the perioperative process conducted by an anesthetist, 20–80 mL of venous blood was drawn and centrifugated in two steps (first centrifugation 10 min/2400 rpm—separation of plasma with platelets—second centrifugation 15 min 3600 rpm—separating of the PRP). The analysis of platelet concentration in the PRP compared to venous blood presented results between 3.6 and 9.1-fold, an average of 6.9-fold. Except for the first group, where the traditional muco-periosteal flap was carried out (Fig. 1) the second and third groups received a surgical treatment with transversal cuts through the soft tissue. After this, the complete soft tissue, including the periosteum, was separated from the bone using the bridge flap technique developed in our institute. The augmentation material containing rhBMP-2 (INFUSE; InductOs; Wyeth Medicine) (between 0.6 and 2.0 mg in total [1.5 mg/mL])) was implanted.
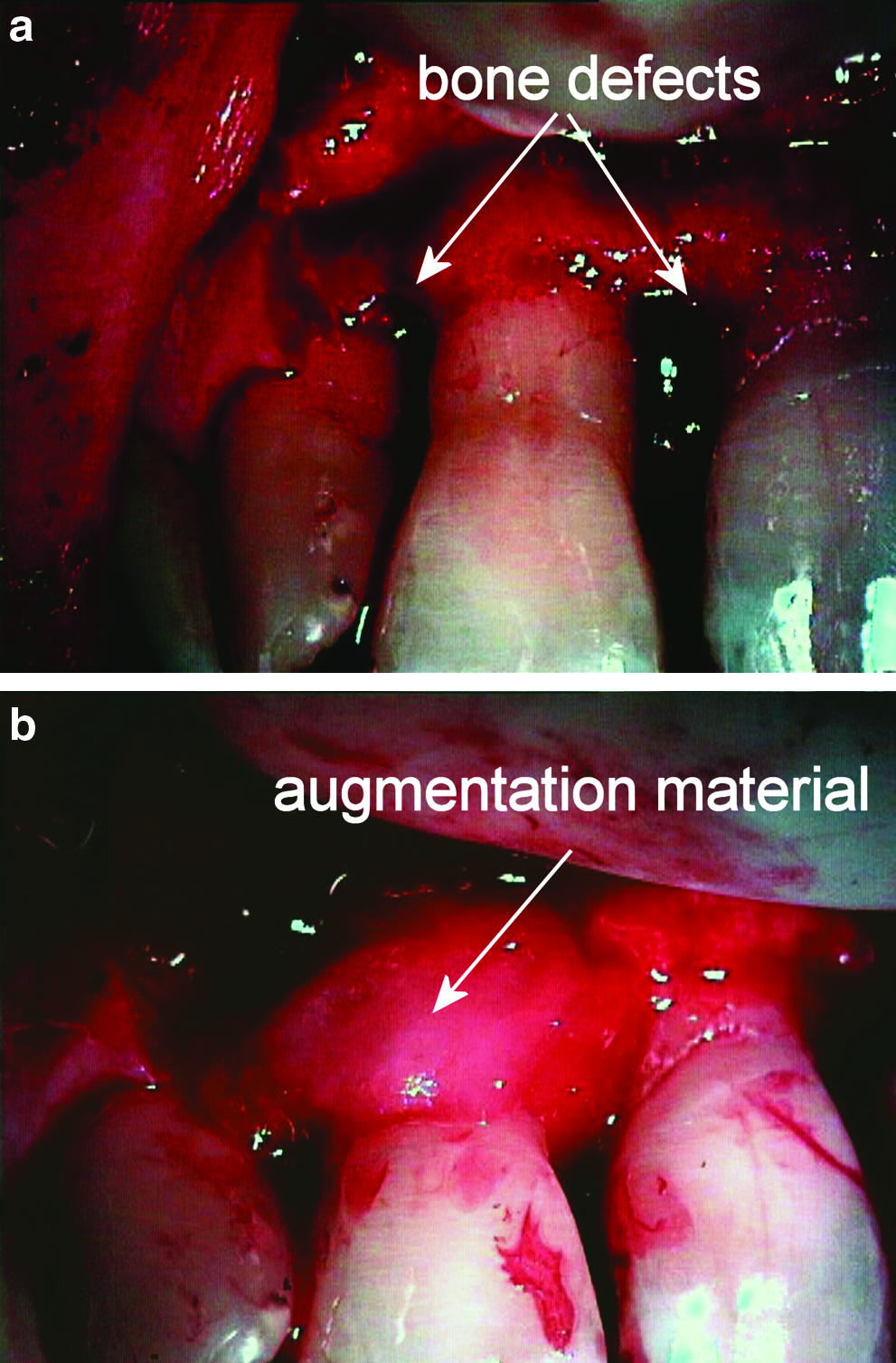
Periodontal surgery, conventional flap technique.
Results
Stitches were removed between 6 and 10 days after the surgical treatment. A wound healing disturbance occurred on one periodontal defect from one patient of the first group. In this defect 1 mm of bone was reabsorbed. On one periodontal defect from one patient of the second group with a wound healing defect no bone development could be achieved.
All patients underwent hygiene control with measurement of PD, plaque, and calculus removal in intervals of 2–3 months during the control period.
For our analysis, we present interdental PDs (deepest point of interdental pocket) measured 6 months, 12 months, and 2 years after the surgical treatment and compared to baseline: group 1: PD reduction (average) from 5.4 mm (baseline) to 2.4 mm after 2 years; group 2: from 5.4 mm to 2.6 mm; group 3: from 4.9 mm to 2.6 mm. The average results of all groups are illustrated in Figure 2. There seem to be no differences in pocket reduction concerning all three groups of patients. The slight increase of PD in group 3 between measurement at the point of 6 months and 2 years can be explained by different levels of oral hygiene at the time of control.
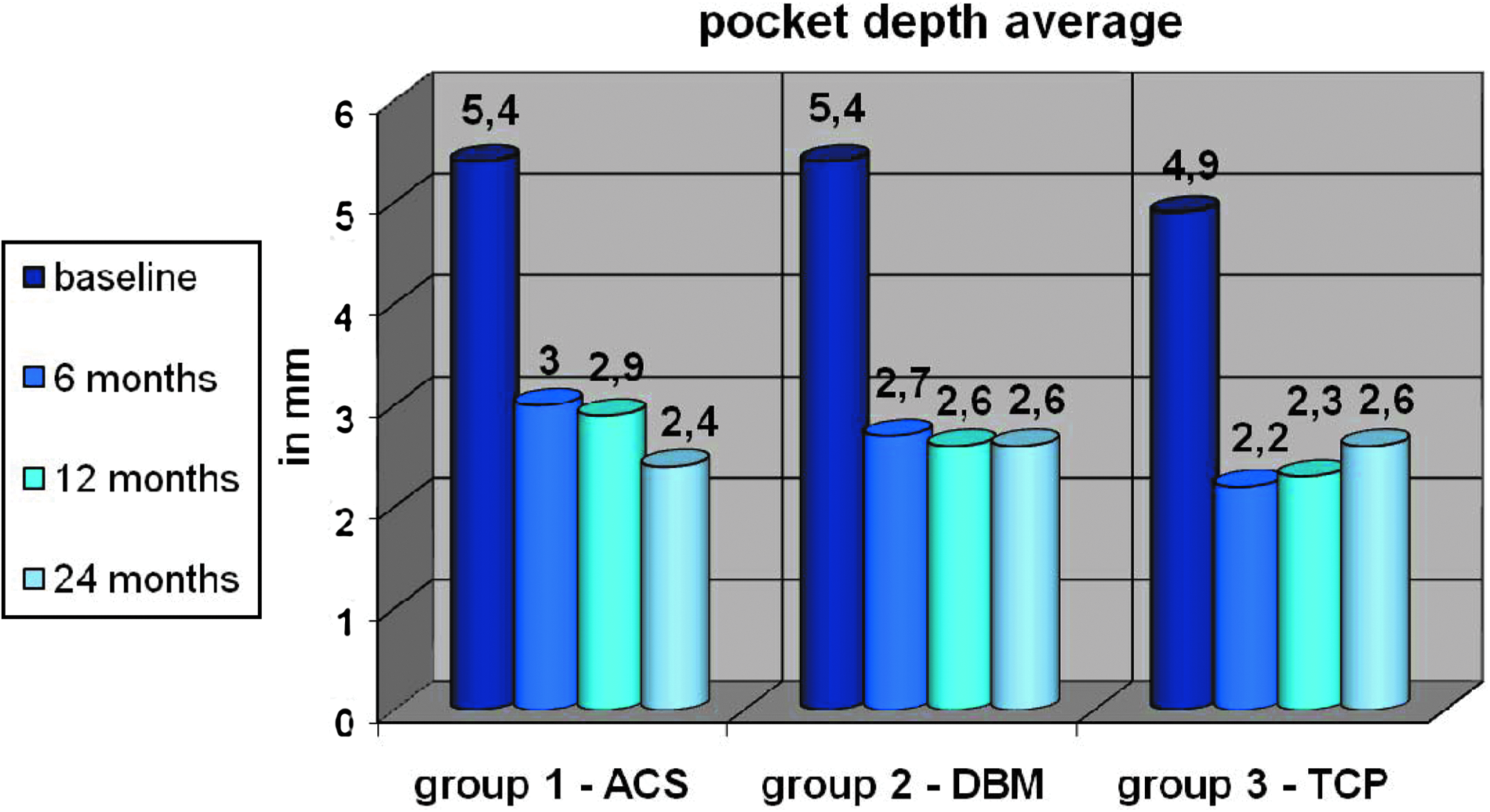
Pocket depth average, 6 months, 12 months and 2 years compared with baseline. Numbers indicate pocket depth average in mm. Color images available online at
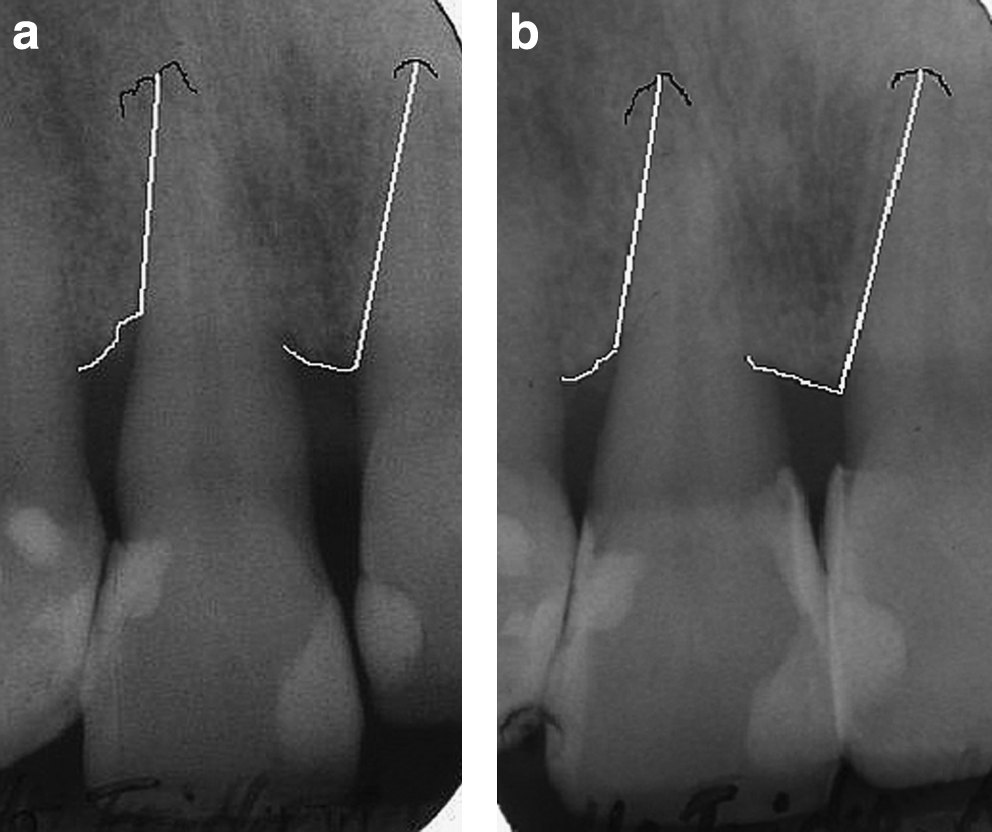
Bone level (the distance from the deepest point of the bone defect to the root tips) was measured radiographically at baseline and 12–24 months after treatment. Radiographs were taken orthogonal and using, in addition, orthopantomography (correction factor 1.27) concerning anterior teeth in maxilla due to projection problems according to the arch of anterior maxilla. Analysis was carried out analogously using diagnostic magnifying glasses. In this article we present radiographs of one patient from each group representing the different technologies and results.
The dental radiographs (Fig. 3) explain the bone situation of a patient belonging to the first group before and 1 year after treatment. A slight difference of bone level is visible.
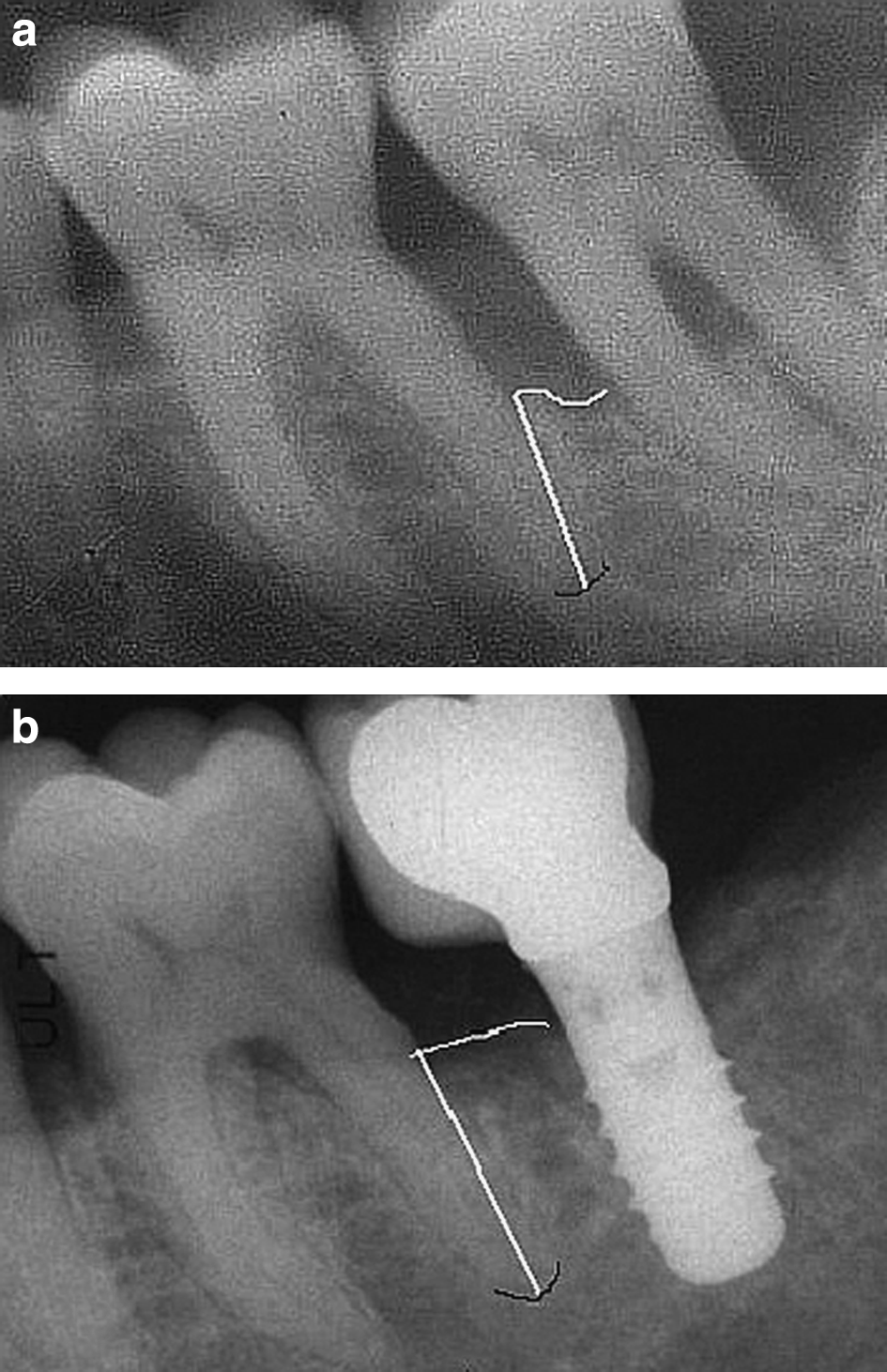
By using the dental radiographs from a part of the mandible, we indicate the newly grown bone in a patient from the second group (Fig. 4).

VBD in the molar region of the left side in the mandible of a patient belonging to group 3 is demonstrated using dental radiographs (Fig. 5).
ACS and DBM are translucent materials under aspects of radiology. Thus, newly visible hard tissue can be regarded as bone. TCP is radio-opaque. In combination with BMPs, TCP is biodegraded in <1 year. This was proved in implant treatment after bone development by means of tissue engineering (TE)-techniques using bone samples.39,52
VBD was achieved in group 1 (−1 to 3 mm; average: 1.7 mm); group 2 (0 to 4 mm; average: 2.5 mm); and group 3 (1 to 7 mm; average: 3.2 mm) (Fig. 6).
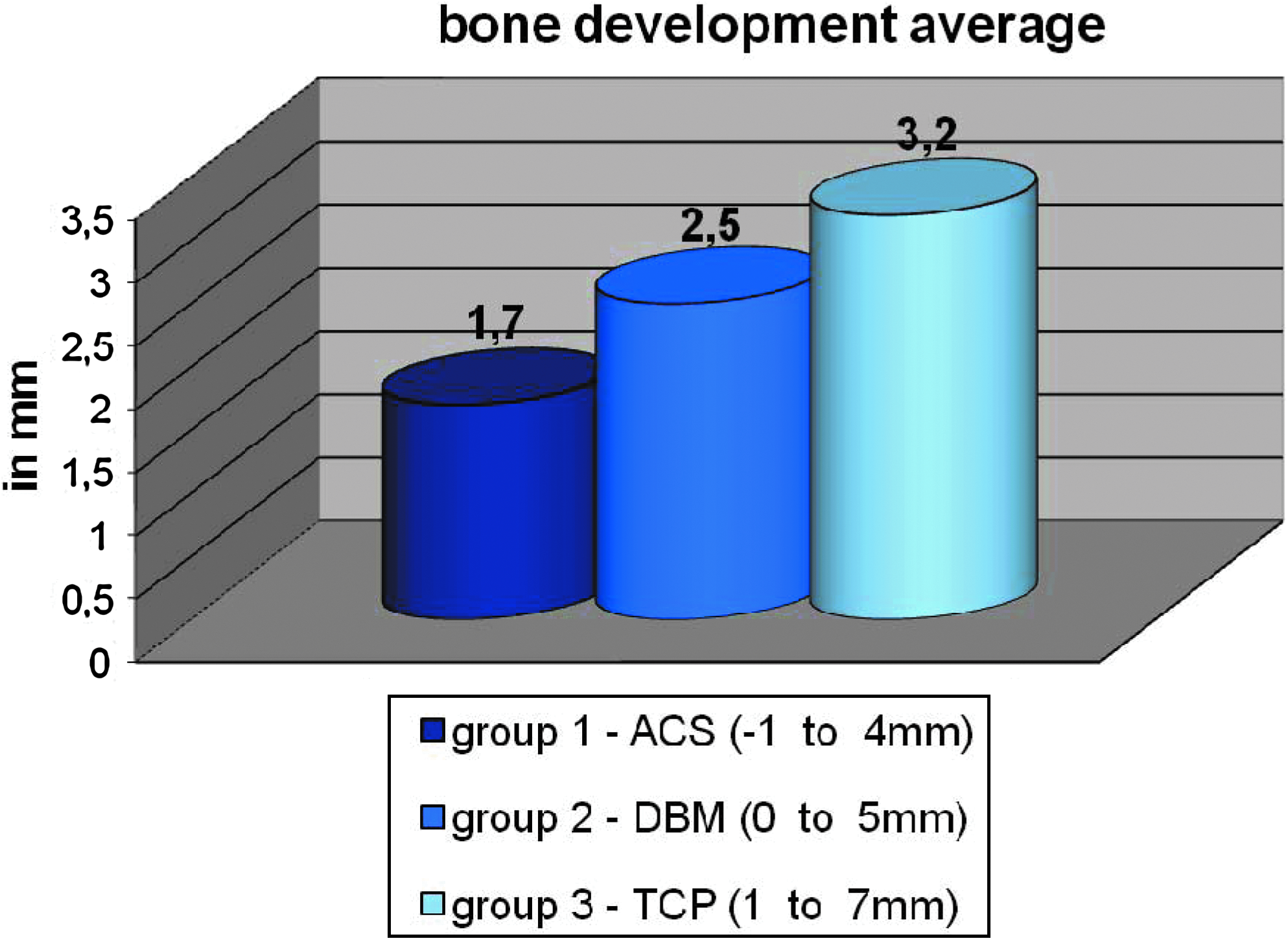
Vertical bone development average, result after 2 years compared with baseline. Numbers indicate vertical bone development average in mm. Color images available online at
Statistical analysis
Although this article does not present results from a clinical study, we tried to verify whether the amounts of newly grown bone demonstrate a significant difference. Statistical analysis was performed in addition to clinical observation.
We used t-test for statistical evaluation (significance level α=0.05). No significance could be determined comparing VBD results of
Group 2 with group 1 | t |=1.685<2.120=t (1-α/2, f)=t (0.975, 16) and
Group 3 with group 2 | t |=0.801<2.074=t (1-α/2, f)=t (0.975, 22).
The comparison of group 3 with group 1 | t |=2.607>2.258=t (1-α/2, f)=t (0.975, 20) proved statistical significance. This can be attributed to the endoscopically assisted surgery as well as to the combination of augmentation material.
Therefore, we conclude that the combination of rhBMP-2 and PRP in addition to TCP and the endoscopically assisted surgery leads to the best results.
Since the development of soft tissue was not our main target, no special soft tissue measurement was performed. However, in addition to the newly grown bone, a considerable development of soft tissue could be achieved in several cases. Figure 7 explains the development of soft tissue in the case presented from the first group. Figure 8 details the same development concerning the patient from group two.
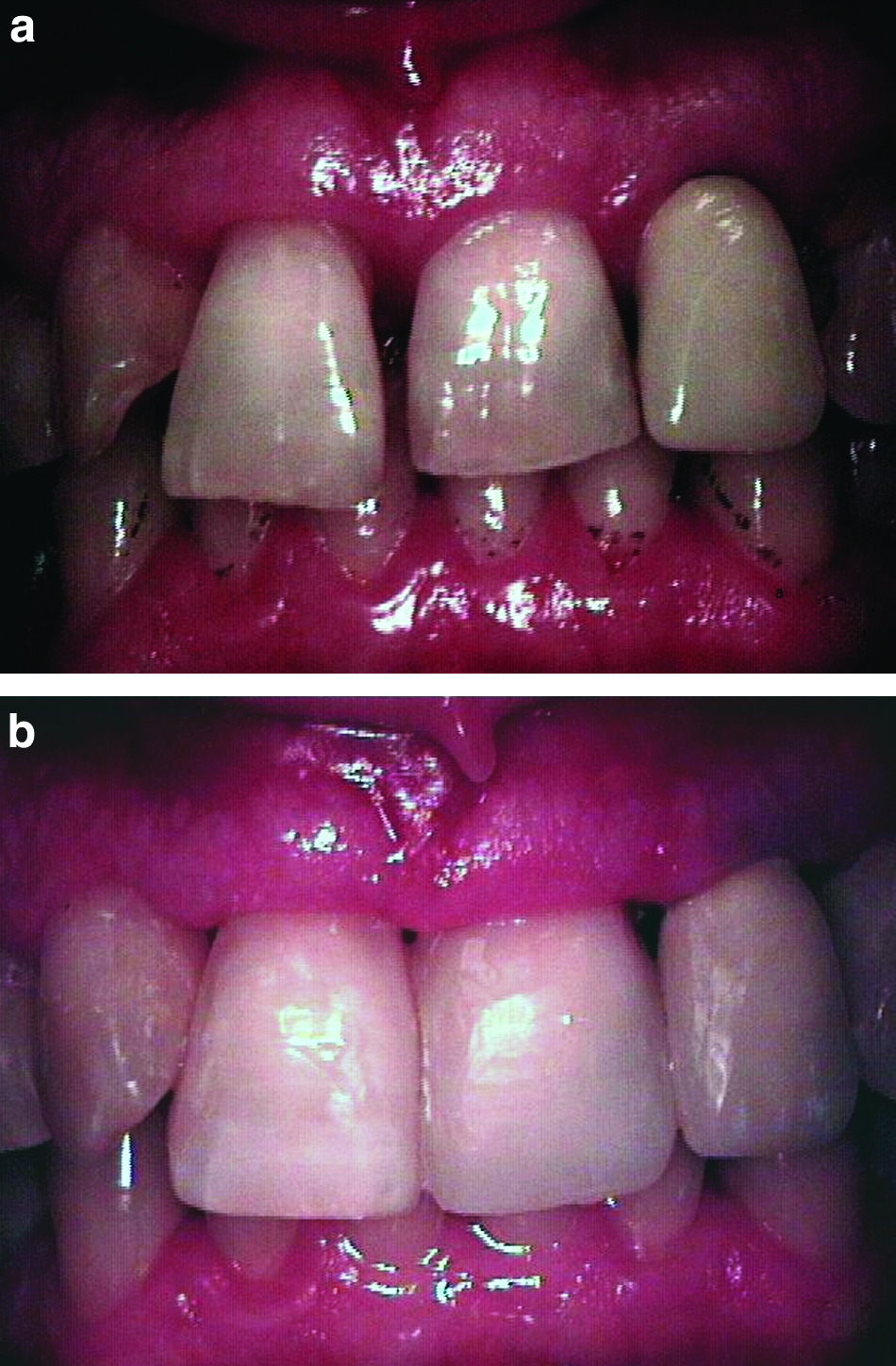

Clinical situation (belongs to patient from Fig. 4).
Discussion
Many authors report on good results using different types of augmentation in periodontal bone defects. Their articles are all based on defects with existing bony walls (two or three walls). They all compare PD at the end of control period with baseline. Some of them also indicate bone development.
Guided tissue regeneration
Polimeni et al. 53 and Nygaard-Østby et al. 2 reported problems using poly (DL-lactide) (PLA) membranes. Of the PLA barriers, 89% became exposed within 3 weeks after surgery, 2 and did not resorb within a 12-month healing interval. 53 Nygaard-Østby et al. 2 proved 1.2 mm bone fill at GTR side and also when only autologous bone was transplanted into the defects. They concluded that using a bioresorbable PLA membrane does not provide additional value to reconstructive surgery including autogenous bone grafting in intra-bony periodontal defects. Our own experiences using resorbable membranes during the 1990s point in the same direction as Polimeni et al. 53 and Nygaard-Østby et al. 2 reported. In addition, most of the membranes—also called barriers—protect the defects from the periosteum, which is necessary for angiogenesis. Due to this, wound healing disturbances often occur 11 and reduce the positive effect of augmentation.
Implantation of hard and soft tissue and EMPs
Nygaard-Østby et al. 2 and Orsini et al. 3 treated intra-bony periodontal defects using autogenous bone grafts. While Nygaard-Østby et al. 2 reported on 1.2-mm new bone, Orsini et al. 3 presented no information on bone development.
Markou et al. 4 and Aspriello et al. 54 used DFDBA alone or in combination with PRP 4 or enamel matrix derivative 54 for treatment of human periodontal intra-bony defects. Okuda et al., 6 Santana et al., 55 and Heinz et al. 7 applied hydroxyapatite to intra-bony defects. Okuda et al. 6 added PRP and human cultured periosteum sheets. The bone development on the surface of existing bony walls can be achieved up to the top of the bone defect using DBM, which is comparable to DFDBA in combination with PRP. 56 Hydroxyapatite possesses osteoconductive potential, which enables it to heal bone defects with surrounding walls. 57
Several authors reported on the advantages of using EMPs in addition to different periodontal surgical techniques.58–60 They all proved better results concerning PD after treatment compared to baseline. No information pertaining to bone development could be found in their articles. Only Sculean et al. 10 presented data on newly grown bone using EMPs combined with a biphasic calcium phosphate. They stated that the amount of newly formed bone was limited and varied from 0.0 to 0.7 mm. The treated initial situation in parts was comparable to the patients of our review, as the authors accounted on 1 and 2-wall intra-bony defects. A 1-wall defect is described as a defect with bone contact only at one side of a tooth. Due to this, bone development has to be achieved predominantly in the vertical dimension.
The above-mentioned publications point out the current state of the art in surgical periodontal treatment including the limits concerning bone regeneration.
Our scientific work is based on this accepted background and includes options offered by bone tissue engineering. The first group of patients received the muco-periosteal flap as the surgical approach and rhBMP-2 combined with ACS, which is part of the medical equipment used instead of other conventional augmentation material. Parallel to other indications, we realized that ACS is not able to provide suitable structural support.37,38,52
In addition, the swelling of the soft tissue particularly in the papillae region forced us to develop a totally new surgical approach. We designed the endoscopically assisted periodontal surgery. This technique avoids wound healing disturbances and invasion of bacteria. 61
As an alternative to ACS we utilized DBM containing allogenic collagens to release the BMP-2 and provide better structure compared to ACS. This combination was carried out in the second group of patients.
Because DBM is an allogenic material, it contains risks of transferring diseases. 39 Because of this information, we looked for a synthetic material with a better structure than collagen.
Corresponding to the application of DBM in other indications we replaced it by TCP. 52
The third group of patients presented the best results. No wound healing disturbances occurred. We are convinced that the implementation of microsurgical approaches using endoscopically assisted surgery, paved the way to periodontal bone development in onlay technique.
As far as we know, this is the first presentation of a group of patients who received periodontal surgery treatment by means of TE techniques endoscopically assisted using PRP, rhBMP-2 and various scaffolds.
With this new TE technique we were able to recreate new bone in periodontal defects of patients in a manner that did not exist before. Clinical studies are needed to prove the technique and our results. The creation of a synthetic scaffold, which is not radio-opaque (e.g., polycaprolactone) and available in a suitable size and shape for periodontal surgery, will ensure bone development without taking bone samples in the future.
From our point of view the following criteria have to be fulfilled before starting the surgical treatment mentioned above:
An optimal preparation including
1. Analysis of bacteria and antibiosis
2. Clarification of internistic background
3. No untreated diabetes, HbA1c ≤5.9%
4. No smoking
Footnotes
Acknowledgments
These reviewed cases were performed with the knowledge of the ethical authorities. Unlike clinical studies, in the run-up to these single cases in off-label use, no written application or final acceptance is required. The authors wish to thank Ms. Helberg and Mr. Jochen Eichholtz for their technical support and Ms. Conny Helbling for her linguistic review as a native speaker.
Disclosure Statement
No competing financial interests exist.