
Abstract
Quantification of the amount of newly formed bone is an essential part of bone regeneration studies. Histomorphometry, based on histological sections of plastic-embedded specimens, is the most frequently applied technique in this assessment. Before performing image analysis, a specific region of interest (ROI) has to be determined. Based on the histological procedure, different areas within the ROI can be discriminated and assigned to relevant tissue structures. However, in literature not much attention is paid to the effect of the histological procedures on the final outcome of the histomorphometrical measurements on bone regeneration. In this study, the histomorphometrical bone formation of the intramedullary cavity of the guinea pig tibia, filled with calcium phosphate cement, was quantified in plastic-embedded and paraffin-embedded specimens and in specimens analyzed with scanning electron microscopy in the backscattering mode (SEM-BS). The data showed that the histological procedure significantly affected the measured bone amount. Therefore, it is recommended that scaffold characteristics are carefully considered in selecting a proper technique for the analysis of bone formation in bone tissue engineering studies. The results of this study identified high-resolution SEM-BS and elastic van Gieson staining of decalcified histological sections as recommendable techniques for evaluating bone formation.
Introduction
It has to be noticed that the preparation of histological sections of bone tissue including hard bone substitute materials, like CaP, is a challenge. In view of this, dedicated microtomes have been developed, such as inner-circular sawing microtomes that allow the histological processing of these plastic-embedded materials. A different approach involves decalcification of the specimens, that is, bone substitute and bone tissue, which allows paraffin embedding and use of standard microtomes equipped with a knife. Recently, we noticed that these two techniques provided different results in terms of histological appearance and amount of formed bone. Consequently, the aim of this study was to evaluate the effect of different techniques on the quantification of bone formation and to address their accuracy and reliability.
Materials and Methods
Materials preparation
CaP powders and poly(D,L-lactic-co-glycolic acid) (PLGA) were used to prepare CaP cement (CPC). CaP powder consisted of a mixture containing 85 wt% alpha-tricalcium phosphate (CAM Bioceramics BV), 10 wt% dicalcium phosphate anhydrous (JT Baker Chemical Co), and 5 wt% precipitated hydroxyapatite (Merck). CaP powder was ball milled in a sequential milling pathway according to a previously developed process. 11 Low-molecular-weight (LMW, 17 kDa) acid-terminated PLGA (Purasorb; Purac Biomaterials BV) was used to produce microparticles. Microparticles with an average size of 20 μm were obtained using a ([water-in-oil]-in-water) double-emulsion technique, as described previously. 12 To obtain this size, first and second emulsions were performed at 8000 rpm for 30 s. Injectable CPC paste was made by mixing 0.8 g of CaP powders and 0.2 g of PLGA microparticles with a 2% Na2HPO4 (Merck) solution in a liquid-to-powder ratio of 0.4. Briefly, the CaP powder and PLGA microparticles were first mixed and placed in an exit-closed syringe. Then, 0.4 mL of the 2% Na2HPO4 solution was added to the CaP powder and the piston was placed back into the syringe. The syringe was placed in a mixing apparatus (Silamat® Vivadent) and mixed for 20 s. Then, the plug was removed and the CPC paste was ready to be injected.
Surgical procedure
The animal experiment was approved by the animal ethics committee of the Radboud University Nijmegen Medical Centre (RUDEC 2009-159). A total of eight skeletally mature female guinea pigs (cavia porcellus) with an average weight of 1.0 kg were used. Surgery was performed under general injection anesthesia (0.4 mg/kg dexmedetomidine [Dexdomitor]/30 mg/kg ketamine [Nimatek; Eurovet], intramuscularly, and 4 mg/kg carpofen [Rimadyl; Cattle]). For unilateral preparation of the implantation site, longitudinal incisions were made on the medial side of the tibia above the ankle joint and below the knee to expose the bone. Two holes with a diameter of 1.8 mm were drilled in the distal and proximal part of the tibia, until reaching the medullar cavity. Low rotational speed and continuous external saline cooling was used. Once the two holes were drilled, marrow content of the medullary canal was removed by endodontic files and irrigated with saline to create an empty space. Subsequently, sterile CPC was loaded in a 2.5-mL syringe, connected to a 22G catheter (BD Venflon™ Pro, BD), and injected in the tibial intramedullary cavity from the proximal hole toward the distal one. The medullary canal was considered completely filled when the CPC paste came out from the distal hole. Excess material was cleaned, CPC paste was allowed to set, and the wounds were closed. Resorbable sutures (Monocryl 4–0; Johnson & Johnson) were used to close the muscle tissue and (Vicryl 5–0; Johnson & Johnson) to close the skin. Postoperatively, the guinea pigs received 10 mg/kg of enrofloxacine (Enrofloxoral drops; Astfarma) for 4 days to prevent infection. Buprenorfin (Temgesic; Reckit & Coleman) at 0.05 mg/kg was used subcutaneously for analgesia every 12 h for 5 days after surgery. After 8 weeks, the animals were sacrificed and the tibias were retrieved and fixed in a buffered 10% formaldehyde solution for 7 days.
Histology
After fixation, tibias were cut into two halves with a saw. Alternately, these halves were divided in two groups: the first group was composed of four proximal halves of even tibias and four distal halves of odd tibias; the second group was composed of four distal halves of even tibias and four proximal halves of odd tibias. The first group was left nondecalcified, dehydrated in a graded series, from 70% to 100%, of ethanol, and embedded in poly(methylmethacrylate) (PMMA) resin. These PMMA-embedded specimens were partly processed to thin (∼15 μm) and partly to thick (∼0.5 cm) sections using an inner circular saw microtome (SP 1600; Leica). The thin processed sections were mounted by groups of three on specimen glass slides. These sections were stained with methylene blue and basic fuchsin. This group was marked as PMMA group. Thick sections were ground with a polishing machine (MetaServ 250; Buehler) and SiC paper up to #4000 and then sputter-coated with gold–palladium (Denton Vacuum Desk III). This group was marked as the SEM group. The second group was decalcified with a specific-purpose apparatus (TDE 30; Sakura), dehydrated in a graded series of ethanol, and embedded in paraffin. These paraffin-embedded specimens were processed to thin sections (∼6 μm) using a standard microtome (RM 2165; Leica). Sections were mounted by pairs on specimen glass slides. Of each specimen, six sections were stained with the elastic van Gieson (EVG) stain and six were stained with hematoxylin and eosin (HE) stain. These sections were marked as EVG and HE group, respectively. All sections were cut perpendicular to the long axis of the tibia.
Image analysis
Images of PMMA, EVG, and HE group sections were acquired by optical light microscopy (ImagerZ1; Zeiss) with a 5× magnification. Images of SEM group sections were obtained by high-resolution SEM (LEO 1450VP; Zeiss). Images of the sections were acquired using the BS mode at 15 kV and a magnification of 40×. After image acquisition, quantitative evaluation of the region of interest (ROI), that is, the area of the medullar cavity delineated by cortical bone, was performed using an image analysis system (Leica Qwin; Leica) with custom-made programs. No special algorithms were used or created
Statistical analysis
The data were statistically analyzed using a one-way ANOVA, with a post hoc Tukey test, and a Mood's Median test (Origin Pro8; Originlab). Results were considered statistically significant at p<0.05.
Results
Figure 1 shows representative images of the obtained results using the different procedures. SEM procedure allowed, by the difference in gray level, the discrimination of the bone ingrowth into the CPC as present in the medullar cavity. In the paraffin sections, depending on the staining used, an even clearer difference between the bone, CPC, and nonmineralized tissue could be perceived. A very evident difference between these structures was obtained with EVG staining. HE staining created a nuance of pink that made the bone and nonmineralized tissue harder to discriminate. PMMA sections were found to be more difficult to evaluate compared to SEM and paraffin sections. PMMA sections did not allow an accurate discrimination for bone ingrowth into the CPC material. In the PMMA sections, the CPC seemed to be even less porous after 8 weeks of implantation compared to the EVG and HE paraffin sections.
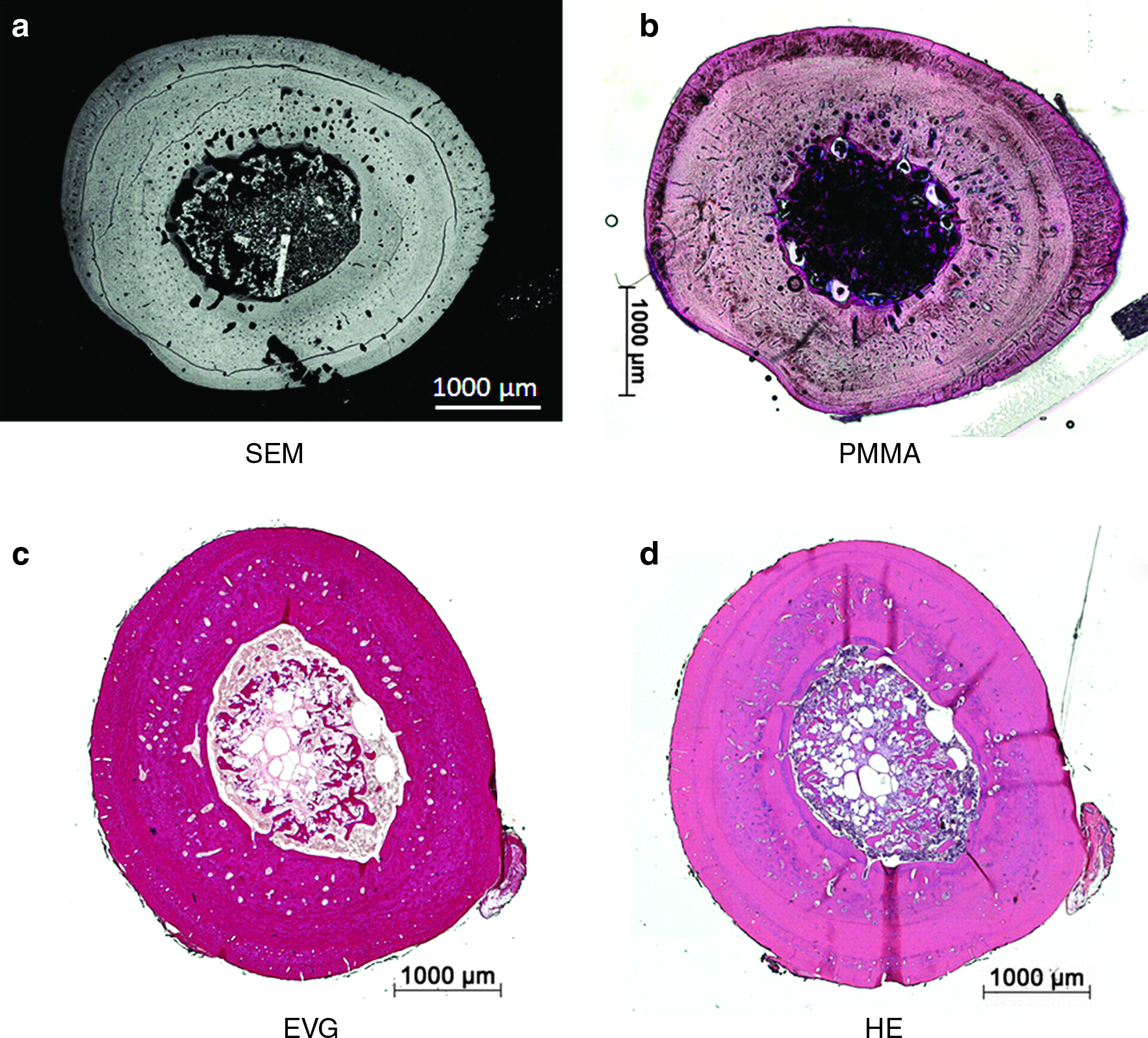
Images of cross sections of samples acquired/stained with
These subjective observations between the different procedures were confirmed by the image analysis data. Figure 2 shows the results (mean±SE) of the quantification of the bone ingrowth percentage for the different evaluation procedures. PMMA sections revealed 16.95%±3.93% of bone, while HE staining quantified 33.93%±5.16% of bone, which were significantly different (p<0.05). SEM and EVG groups showed similar values with 23.50%±4.97% and 24.03%±4.03%, respectively.

Results of the bone percentage according to the quantification technique. SEM, scanning electron microscopy; PMMA, methylene blue and basic fuchsine; EVG, elastic van Gieson; HE, hematoxylin and eosin. *Significant results (p<0.05).
Discussion
The aim of this study was to evaluate the effect of different techniques to quantitatively assess bone formation. To that end, CPC was implanted in the intramedullary cavity of the tibia of guinea pigs. After an implantation period of 8 weeks, tibia were retrieved and processed for subsequent bone formation analysis using SEM, PMMA, EVG, and HE. Each procedure used in this study has its own advantages and disadvantages. The preparation of samples for SEM analysis is relatively easy and takes less time, but special equipment and skills are needed for imaging at high resolution and further image analysis. Preparation of PMMA specimens and their sectioning is also comparatively simple and there is no need for highly specialized equipment, although some support of an experienced person is required. The disadvantage of this technique is that thicker sections are prepared compared to decalcified and paraffin-embedded specimens. On the other hand, the preparation of paraffin sections and the use of different staining procedures are time consuming and need to be performed by a well-trained specialist. The advantage of paraffin sectioning is that no material is lost during the section procedure and a larger number of sections can be obtained due to their very limited thickness. Also, the different paraffin staining procedures make possible that more information can be obtained than only the percentage of bone formation.
As confirmed by image analysis, the use of different histological stains makes the discrimination between original bone, newly formed bone, and biomaterial much easier. For paraffin-embedded sections, HE stains all nuclei blue and other cellular structures in various shades of red, pink, or orange,13,14 whereas EVG stains elastin fibers black, nuclei dark brown, and collagen pink/red.15,16 For PMMA-embedded sections, methylene blue and basic fuchsine stain nuclei purple, cytoplasm pink, and collagen/connective tissue blue.17,18 As indicated by the data, these different stains have an evident effect on the accuracy of the image analysis measurements, with EVG showing the best discriminatory properties for bone quantification. However, the use of other staining techniques, which also provide a clear and sharp discrimination between the different components of the ROI, is not discarded. It has to be emphasized that the PMMA sectioning did not permit a proper quantitative analysis of the bone ingrowth into the CPC material. The approach used for the PMMA sectioning allows evaluating consecutive histological sections, while the paraffin method allows serially sectioning of the whole sample. As a result, the sections obtained for each PMMA-embedded specimen represent a limited part of the entire sample and do not allow achieving a completely accurate comparison between samples if the analyzed parts were taken at different levels. Nevertheless, the errors have been minimized by dividing the full tibias in two halves, that is, proximal and distal tibias, which were alternatively processed for PMMA, thus to have a more complete overview of the specimen. Furthermore, the differences on the image neatness were translated in a higher or lower amount of measured bone. These differences could create false positives or mask the real in vivo effect of a bone substitute material (false negatives). The CPC included PLGA microparticles, which degrade within time and result in the creation of an internal microporosity within the CPC. This microporosity will subsequently be occupied by the ingrowing bone. This process was confirmed in the paraffin sections, but formation of porosity as well as bone ingrowth could not be observed in the nondecalcified PMMA sections. Probably, this is due to the thickness of these sections. This is a serious problem that needs further attention and can have consequences for earlier reported observations. This observation also emphasizes that the preparation and analysis of histological sections cannot be considered as an automated process. Scaffold characteristics are a very important parameter in the selection of the used histological procedure.
High-resolution SEM in the BS mode was found to be an accurate technique to assess bone formation. However, access to such special equipment is limited.10,19,20 SEM and EVG staining of decalcified paraffin sections were shown to be accurate in determining the different ROI involved in the bone formation. Both procedures are able to produce similar results when bone formation has to be quantified and they can also provide additional information. SEM will allow a better analysis of the structure of the scaffold material and growing bone, while EVG will provide additional information about the present tissues. The results emphasize also that research groups involved in bone tissue engineering have to be careful in the processing of experimental samples and their subsequent analysis, as the used procedure can have a serious effect on the study outcome. Ample knowledge of histology and histological procedures is needed when performing bone quantification and automatisms have to be avoided.
Conclusion
Bone ingrowth in a CPC was analyzed using four different techniques for quantification. The assessed bone ingrowth percentage within the tibial intramedullary cavity after the implantation of CPC depended on the procedure used. The results of the present study illustrate that the histological procedure used to quantify the bone formation can have an effect on the results and more specifically the values of bone formation. Methods that allow clear differences between the regions of interest are preferred. For the evaluation of bone formation, the use of high-resolution SEM in the BS mode or decalcified paraffin section with EVG staining is recommended.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of the TeRM Smart Mix Program of the Netherlands Ministry of Economic Affairs and the Netherlands Ministry of Education, Culture and Science. Mr. Lopez-Heredia thanks Mr. Pilet for assistance in the SEM analysis.
Disclosure Statement
Authors state that there are no commercial associations that might create a conflict of interest in connection with this article.