
Abstract
Dental pulp, covered with dental hard tissue, is a promising source of mesenchymal stem cells and osteoprogenitor cells for regenerative medicine. Our previous studies showed that 73% of dental pulp cells isolated from magnetically cryopreserved teeth where their viability, morphology, and expression of stem cell surface markers were similar to the cells isolated from fresh teeth, suggesting that magnetic cryopreservation is an applicable method for intact tooth as well as dental pulp tissue banking. However, the cryoprotectant, concentration, contact surface, and equilibration time for magnetic cryopreservation of dental pulp require optimization. In addition, the integrity and viability of post-thawed dental pulp with and without dental hard tissue covering after magnetic cryopreservation were investigated. Lower concentration of the cryoprotectant (5% dimethyl sulfoxide [DMSO]) and shorter preequilibration time are required for magnetic cryopreservation compared with the conventional cryopreservation method. The structure of at least 33% of post-thawed pulp with dental hard tissue from the open end remained intact where >80% of cells were viable. The addition of the cryoprotectant additive trehalose did not replace or improve DMSO's efficacy for magnetic cryopreservation of dental pulp or intact tooth. Tooth banking for transplantation provides an alternative treatment to replace missing teeth. The optimized cryoprotectant conditions for dental pulp tissue during magnetic cryopreservation should lead to more satisfactory outcomes in clinical applications such as autotransplantation and the isolation and expansion of dental pulp stem cells for tissue repair.
Introduction
Dental pulp is a long and slender tissue embedded in dental hard tissue with one opening end interacting with the jaw's internal environment (blood and sensory nerve). The limited permeability of the pulp cavity to the cryoprotective agent makes it difficult to preserve the pulp tissue. 6 Hence, protocols for enzymatic digestion of dental pulp to obtain DPSCs followed by cryopreservation have been reported and the differentiation activity of DPSCs after thawing is promising.7–9 However, the isolation of DPSCs caused damages to the integrity of dental hard and soft tissues, which limit their clinical applications.
Dimethyl sulfoxide (DMSO) has been a common cryoprotectant for cell banking due to its ability to induce cell fusion, and its permeability may balance the osmosis across the cell membranes. 10 The cell banking protocol for tooth preservation was applied by immersing intact tooth in 10% DMSO for 1 h; certain amounts of viable cells were obtained from entire post-thaw pulp. 11 However, the cooling effect and penetration of cryoprotectant through different types of tissue are different 12 ; the cryopreservation condition for intact tooth as well as isolated dental pulp needs to be optimized.
Physical effects such as slow or rapid freezing, 13 pressure, 14 or microwave15,16 to avoid ice damage for maintaining the integrity of tissue during cryopreservation have been reported. However, the required high energy and uneven heat conduction maybe concerned. A programmed freezing with magnetic field protocol for tooth banking has been generated and the implantation outcome using the thawed teeth is acceptable; in addition, similar proliferative ability of post-thawed periodontal ligament cells compared with the fresh ones was also demonstrated. 17 Our recent studies using the same magnetic freezing protocol for tooth banking indicated that dental pulp cells isolated from the post-thawed tooth retained 73% viability. 18 It suggests that magnetic cryopreservation is an alternative and effective method for preserving intact tooth containing dental hard and soft pulp tissues. This study aims to identify the optimal cryopreservation medium of magnetic cryopreservation for tooth banking. Wistar rat teeth were used for the experiments. We examined the effects of (1) cryoprotectant contact surface area, (2) cryoprotectant preequilibration time, and (3) the concentration of DMSO with or without trehalose additive for magnetic cryopreservation on post-thawed pulp tissue explant activity. The chemical and physical effects of cryoprotectant and magnetic field for tooth banking are discussed. The optimized protocol for magnetic cryopreservation of dental pulp may facilitate and improve post-thawed tooth's clinical applications for transplantation, tissue repair, and regeneration.
Materials and Methods
Rat tooth and pulp extraction
Intact teeth and the extracted pulp tissues were obtained from 8-week-old male Wistar rats. Rats were sacrificed by cervical dislocation and the teeth were immediately excised. Mandibles and maxillae were carefully reflected with a scalpel on one side to expose the entire tooth, which was then gently elevated intact, thereby avoiding any fracture of the dental tissues. 19 The apical-bud extending from hard tissue was removed with a sharp scissor. The incisor pulp chamber is inherited with one open end, hence an intact tooth group contains pulp with hard tissue covering and one end is opened. For pulp-exposed groups, after extraction, incisors were split and the entire pulp was removed using a delicate tissue forceps. The Taipei Medical University Animal Care Ethics Committee approved this study (LAC-99-0008).
Cryopreservation of intact teeth or pulp tissues
Intact teeth or pulp samples were incubated separately in one of the following solutions, 5% DMSO, 10% DMSO, 5% DMSO+0.3 M trehalose, or 10% DMSO+0.3 M trehalose, in a 2 mL cryogenic vial (Corning) and equilibrated for 15, 30, or 60 min. The tissues were then frozen using a magnetic cryopreservation method in a programmable freezer (ABI), in the presence of a 0.01 mT magnetic field. The samples were kept at 4°C until placed in this freezer at −5°C. The temperature was then continuously lowered by −0.5°C/min until it reached to −32°C. The samples were immediately transferred to a −150°C freezer (MDF-11561; Sanyo) for long-term storage. Intact teeth or dental pulp tissues were cryopreserved in an isopropanol-jacketed freezing container (Mr. Frosty; Nalgene) in a −80°C freezer overnight and subsequently stored in a −150°C freezer (MDF-11561; Sanyo), which represented the nonmagnetic cryopreservation group. After storage for a week, the teeth or pulp tissues were rapidly thawed in a 37°C water bath. Cryoprotectant was gradually removed and the tissues were rinsed with phosphate buffer saline (PBS) for the following assays.
Explant viability assay
After washing with PBS, each thawed pulp was divided into three 1.5 mm2 segments: coronal, middle, and root (Fig. 1E). Duplicate samples of all segments were placed separately in the center of wells in a six-well culture plate and cultured with 0.65 mL Dulbecco's modified Eagle's medium supplemented with 1% penicillin–streptomycin and 10% fetal bovine serum in a 37°C and 5% CO2 incubator for 8 days. Fibroblast outgrowth was observed with an inverted microscope (Optima BI-503) at 40× magnification. The image was recorded and we calculated the mean of three longest cell outgrowth distances, which represent the viability of each tissue segment. The explant viability assay data are reported based on the average of three independent experiments (n=3).
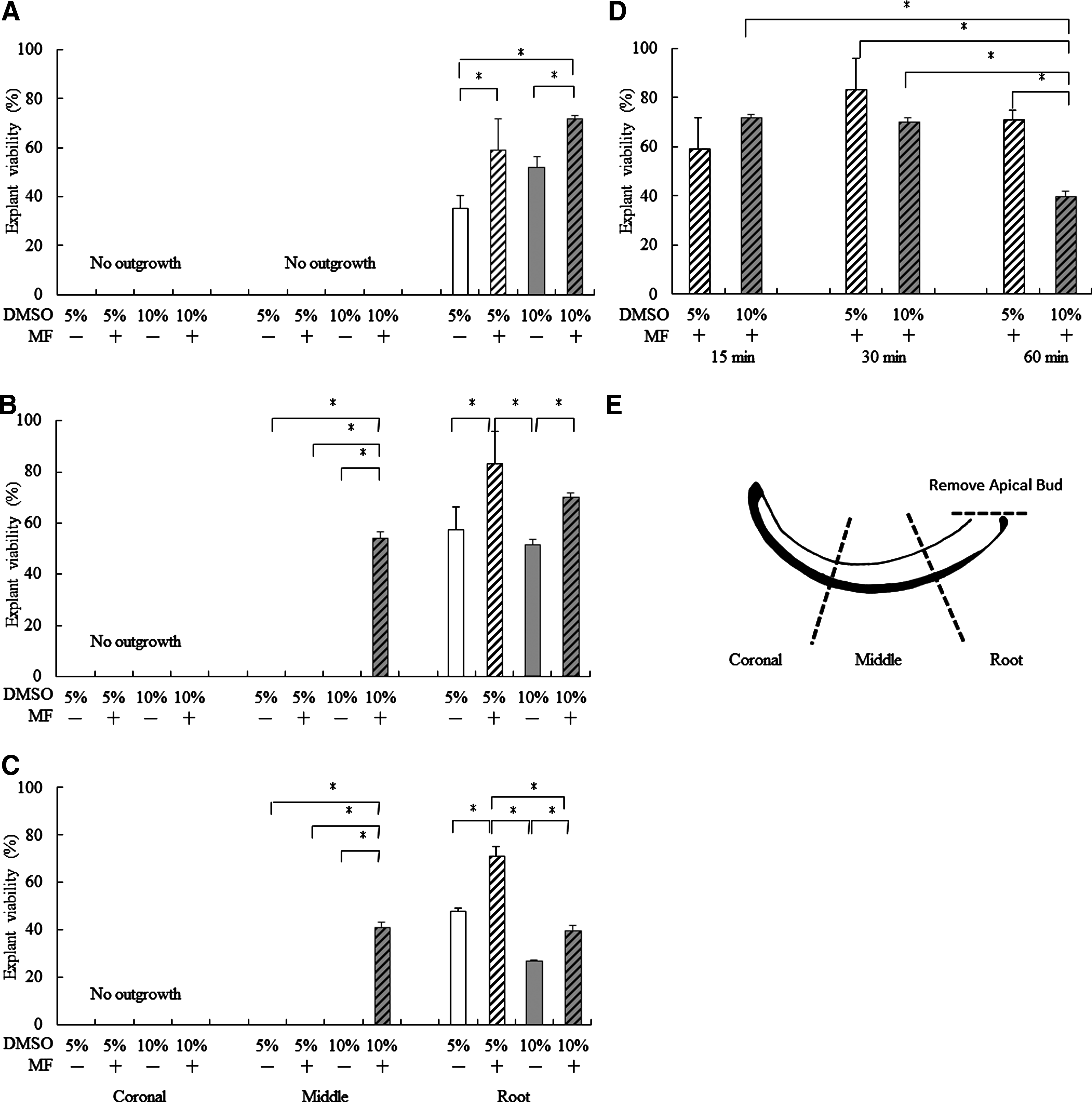
Post-thaw viability of intact rat incisor subjected to magnetic and nonmagnetic cryopreservation. Rat incisors were preequilibrated with the cryoprotectant containing the indicated percentage of DMSO for
Adhesion and morphology of the cells isolated from post-thawed dental pulp tissue
Intact teeth or pulp samples were respectively incubated in 5% DMSO for 30 min. The tissues were then frozen following the magnetic cryopreservation method or the nonmagnetic cryopreservation method as described previously. After thawing, the dental hard tissue was removed and the soft dental pulp was cut into three equal parts: coronal, middle, and root. Each piece (∼1.5 mm3) was then digested with collagenase and trypsin following by plating in a 24-well plate. After 48 h, the unattached cells were washed off and the adhered viable cells were observed and counted by phase-contrast microscopy. The cell adhesion assay data are reported based on three independent experiments (n=3).
Histological analysis
Thawed pulps and teeth were fixed in 4% neutral-buffered paraformaldehyde for 48 h. After fixation, intact teeth were further demineralized in 10% ethylenediaminetetraacetic acid for 4 weeks. 20 X-ray imaging was used to determine when demineralization was ceased. Teeth or pulps were then processed and embedded in paraffin wax for histological examination. The slices 2 μm from the mid-sagittal line of each tooth or pulp were stained with hematoxylin and eosin. Morphological differences between coronal and root sections were observed with an inverted microscope (Optima BI-503). Histological analysis data are based on the most representative slides from two independent experiments (n=2).
Statistical analysis
Post-thaw explant measurements were compared with those of fresh controls and expressed as percentage of explant viability (%). One-way analysis of variance (ANOVA) and a Scheffé post hoc test were used to compare all possible combination of factors. Two-way ANOVA and a Scheffé post hoc test were used for the analysis containing two nominal variables. A p-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS version 13.0 (SPSS, Inc.).
Results
Viability of frozen-thawed pulp tissue from magnetically cryopreserved intact teeth
To determine the optimal concentration of the cryoprotectant, contact surface, and incubation time for dental pulp subjected to magnetic cryopreservation, the isolated pulp tissue and intact teeth were preequilibrated with 5% or 10% DMSO for 15, 30, and 60 min followed by magnetic or nonmagnetic cryopreservation. The explant viability assay of pulp tissue from coronal, middle, and root sections of thawed intact teeth was performed (Fig. 1E). No explant outgrowth was observed in the coronal portion of the post-thawed teeth either in 5% or 10% DMSO for magnetic or nonmagnetic cryopreservation. The magnetically cryopreserved middle portion of intact teeth preincubated with 10% DMSO for 30 or 60 min contained 40%–60% explant viability, which is significant compared with the middle portion in the same cryoprotectant that was subjected to conventional, nonmagnetic cryopreservation (Fig. 1B, C). The root portion of post-thawed pulp from magnetically cryopreserved intact teeth exhibited the best explant viability. The viability of post-thawed root portion preincubated with either 5% or 10% DMSO for 15, 30, or 60 min was significantly higher by magnetic freezing (p<0.05) (Fig. 1A–C). Statistical analysis indicates that the post-thaw viability of incisor root preincubated with 5% DMSO for 30 min followed by magnetic cryopreservation was the best (Fig. 1D) (p<0.05).
Viability of frozen-thawed pulp tissue by magnetic cryopreservation
Dental hard tissue may interfere with the cryoprotectant penetration resulting in poor viability of the post-thawed pulp. Therefore, pulp was extracted and equilibrated with different cryoprotectant followed by cryopreservation in the presence or absence of a magnetic field. The viability of coronal, middle, and root sections of post-thawed pulp was examined. Explant outgrowth was observed in all coronal and middle portions of pulp except the coronal segment incubated with 5% DMSO for 15 min followed by freezing without the magnetic field (Fig. 2A). No matter which part of the pulp was thawed, the explant viability of the pulp preequilibrated with 5% or 10% DMSO for 15 or 30 min or with 5% DMSO for 60 min followed by magnetic cryopreservation was significantly higher than the pulp preincubated under the same conditions but not magnetically cryopreserved (Fig. 2A–C). Furthermore, explant viability was reduced when the pulps were preequilibrated with 10% DMSO for 60 min, suggesting that incubation with higher DMSO (>5%) concentrations for longer than 30 min was toxic (Fig. 2D). Adherence and cell morphology of the cells from post-thawed dental pulp tissues were also investigated. The flat and fibroblastic-like cells with spindles were more from magnetically cryopreserved pulp compared with the cells from nonmagnetically cryopreserved pulp (Fig. 3A). The viable and adhered cell number was more from the coronal and middle parts of pulp extracted from magnetically cryopreserved teeth whereas the viable and adhered cell number of root from isolated dental pulp with or without magnetic cryopreservation has no significant difference (Fig. 3B).

Post-thaw viability of dental pulp subjected to magnetic and nonmagnetic cryopreservation. The pulp was extracted from rat incisor and equilibrated with the cryoprotectant containing the indicated percentage of DMSO for

Adhesion and morphology of the cells isolated from post-thawed dental pulp. Intact teeth or isolated dental pulp tissues were respectively preequilibrated with 5% DMSO for 30 min. The tissues were then frozen following the magnetic cryopreservation method (+MF) or the nonmagnetic cryopreservation method (−MF) as described in the “Materials and Methods” section.
Trehalose as cryoprotectant additive for cryopreserving the intact teeth
Trehalose has been used as a cryoprotectant additive, 21 which can prevent over-dehydration and cell membrane fusion. 22 We also investigated whether trehalose in combination with DMSO can improve the post-thaw viability of magnetically cryopreserved dental pulp. Therefore, trehalose (0.3 M) was included in 5% DMSO or 10% DMSO; however, the viability is decreased (Fig. 4A–C).

Post-thaw viability of intact rat incisor preequilibrated with the cryoprotectant containing the indicated DMSO (D) percentage with 0.3 M trehalose (T) for
Histological analysis of post-thaw incisor and pulp
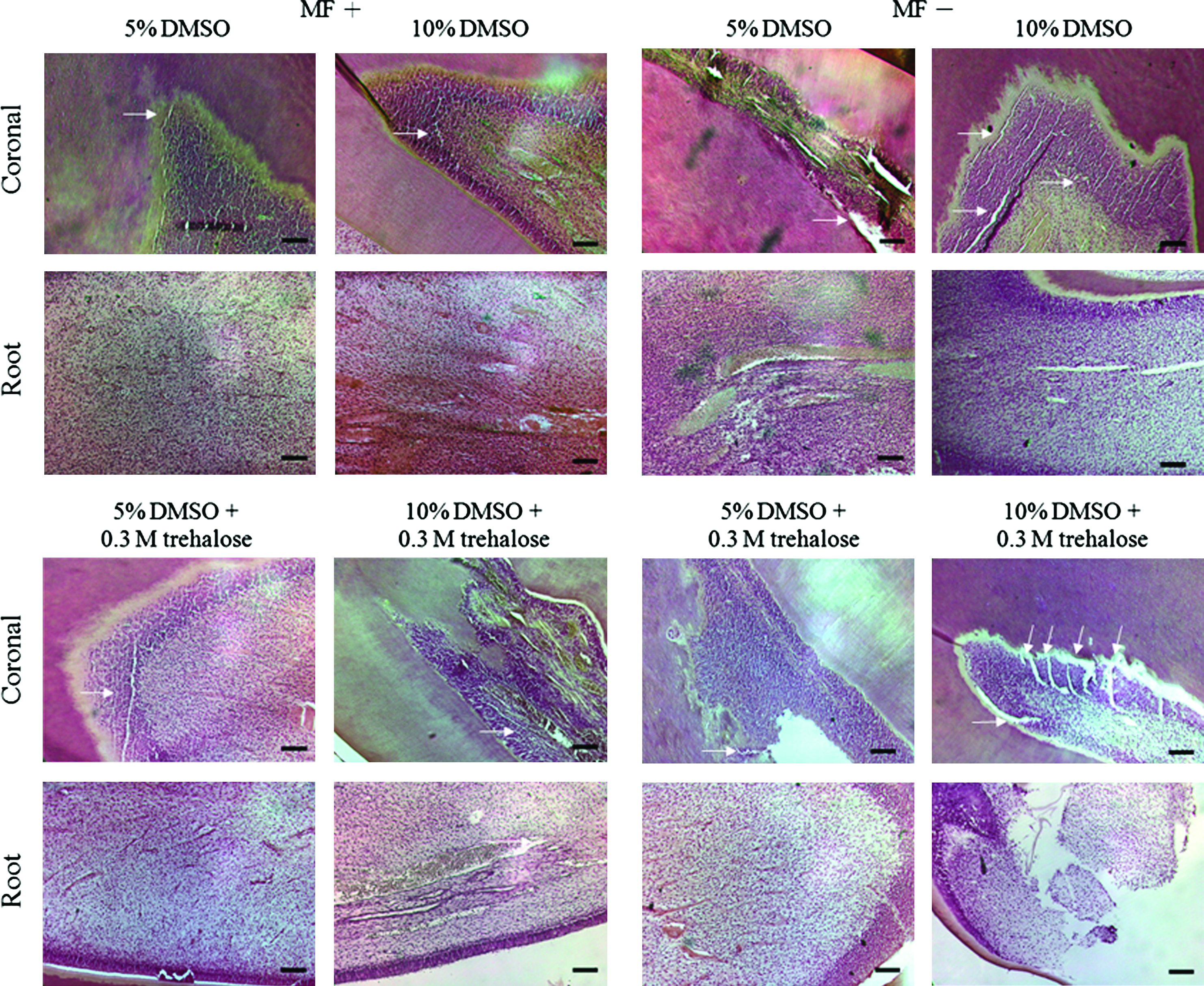
Histological analysis was carried out to observe morphologic changes of the post-thawed teeth and pulp tissues. In agreement with the outcomes of explant viability assay, the integrity and structure of the naked pulp, which has the most contact area with the cryoprotectant, was retained compared with the pulp covered with dental hard tissue that contained cracks (Figs. 5–7). In addition, there were fewer cracks in both intact incisors and naked pulp by magnetic cryopreservation compared with the tissues by nonmagnetic cryopreservation (Figs. 5–7). More cracks in the coronal portion were observed compared with the root of pulp extracted from the post-thawed tooth (Fig. 5). This suggests that sufficient preequilibration time and the penetration of cryoprotectant is important to prevent pulp tissue from cracking. Furthermore, cracks were evident in the cryopreserved intact teeth and the naked pulp preincubated with the trehalose-containing DMSO-based cryoprotectant (Figs. 6 and 7).

Histological observations of the post-thawed coronal and root portions of magnetically frozen (MF+) or nonmagnetically frozen (MF−) intact teeth and pulp. Samples were all preequilibrated with 5% DMSO for 15 min followed by cryopreservation. After quick thawing, the tissue was sectioned and fixed by H&E staining. The white arrows indicate the tissue cracks. Cracks are more evident in the coronal portion of nonmagnetically frozen intact teeth than magnetically frozen tissues (Routine H&E staining, scale bar: 100 μm). H&E, hematoxylin and eosin. Color images available online at
Histological observations of post-thawed coronal and root portions of magnetically frozen (MF+) or nonmagnetically frozen (MF−) intact teeth, which were preequilibrated with the indicated cryoprotectant for 60 min. The white arrows indicate spacing within tissue structure. Cracks are more evident in both coronal portions of nonmagnetically frozen intact teeth and the tissues preincubated with a trehalose-containing DMSO-based cryoprotectant (H&E staining, scale bar: 100 μm). Color images available online at
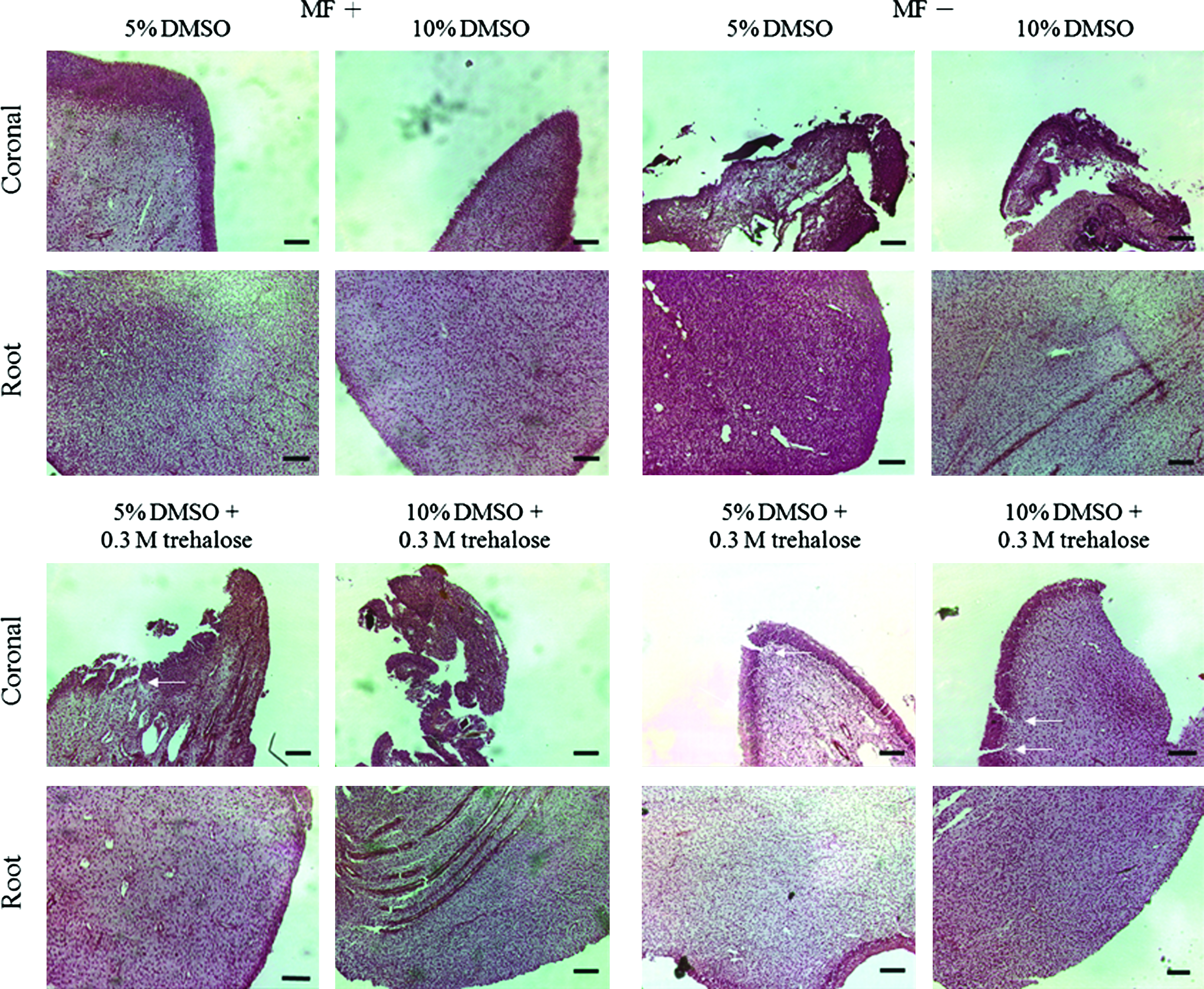
Histological observations of coronal and root portions of magnetically frozen (MF+) or nonmagnetically frozen (MF−) pulps, which were preequilibrated with the indicated cryoprotectant for 60 min. The white arrows indicate spacing within tissue structures. Cracks are more evident in tissues preincubated with a trehalose-containing DMSO-based cryoprotectant (Routine H&E staining, scale bar: 100 μm). Color images available online at
Discussion
Tooth formation starts from the dental bud, followed by the crown, and ends with the root. The long and slender dental pulp is covered by dense, hard tissue with an opening end at the dental root tip, which is responsible for blood circulation. The current study showed that preequilibration of intact tooth with 10% DMSO for 30 min, or 5% DMSO for 30 or 60 min could preserve the post-thawed root explant viability up to 70% whereas coronal and middle parts of the dental tissue had no activity. On the other hand, removal of dental hard tissue could preserve entire dental pulp tissue with 60% of explant viability (Figs. 1 and 2). It indicates that dental hard tissue hampers the cryoprotectant penetration into dental pulp. It is agreed that tissues can only be preserved during freezing when contact with cryoprotectant. In adult rat incisor, the root end is opened, which is similar to the structure of human immature teeth and the mature third molar where the root can contact with a cryoprotectant. A study by Temmerman et al. reported younger human tooth (the third molar) with more viable pulp after cryopreservation; an immature tooth with a minimum dimension of 9.42 mm2 enables the cryoprotective agent to penetrate sufficiently from apex to crown. 23 In addition, while the cryoprotectant penetrates through the outer tissue layer, the concentration of the cryoprotectant in inner tissue could remain lower. 24 To adequately equilibrate the inner tissue layer with the cryoprotectant, high concentrations of cryoprotectant or longer preequilibration time for organ or tissue cryopreservation maybe applied.25,26 However, prolonged equilibration with cryoprotectant such as DMSO is deleterious due to chemical toxicity. 12 Our studies showed that the explant viability of the root preequilibrated with 10% DMSO for 60 min was significantly lower than 5% DMSO for the same equilibration time. Compared with DMSO, trehalose is a less-toxic natural cryoprotectant. 22 Trehalose is a larger molecule and can bind to more water molecules. 27 The usage of 0.3 M trehalose and 10% DMSO for pancreatic islets at temperatures ranging from 5°C to 9°C increased membrane permeation and cryopreservation. 21 Other studies suggested that trehalose can prevent cells from over-dehydration. 28 Therefore, trehalose may benefit cryopreservation of cells or soft tissues such as pulp tissue. However, the current study using trehalose as an additive to DMSO-based cryoprotectant did not improve the preservation of intact incisors with or without magnetic cryopreservation (Fig. 4). Histological observations revealed the loss of structural integrity while the incisor was preequilibrated with cryoprotectant-containing trehalose (Figs. 6 and 7). Extended exposure to trehalose may increase the risk of osmotic stress resulting in poor viability.29,30 Although the protective mechanism of trehalose for tooth preservation remains unclear, the preservation medium containing 0.3 M trehalose with 5% or 10% DMSO of hypertonic condition did not improve intact tooth preservation by magnetic cryopreservation.
Magnetic field applied during cryopreservation may improve the penetration of cryoprotectant. The intact tooth preincubated with 10% DMSO for at least 30 min followed by magnetic freezing can preserve about two-thirds of the dental pulp (root and middle parts) from post-thawed tooth with explant viability (Fig. 1). Optimal use of cryoprotectant should also include effective equilibration times to avoid toxicity.31,32 Therefore, it is important to balance equilibration time against the harmful effect of overexposure to cryoprotectant before cryopreservation and during its removal after thaw. 33 Permeation of tissue with appropriate cryoprotectant to avoid the lethal effect of ice crystal formation and the build-up of extracellular salts are critical for tissue or organ cryopreservation. 12
Explant viability assay can be utilized in vitro to study tissue or organ responses to toxins, growth factors, or hormones, as well as to assess tissue health, growth, differentiation, and post-thawed viability. 34 The explant viability assay adopted in this study differs from Takashima's study that includes addition of enzymatic dissociation agents such as dispase or trypsin to enhance the liberating cells from tissue clumps. 35 Cells can be observed to grow out of tissue clumps in 3–4 days, reaching confluence after 9–12 days. 23 The protocol we used is simpler and does not involve proteases. 36 This assay requires cells not only to be viable but also to have adequate migration and proliferative activity. In our studies, cells indeed took longer time on average 8 days to grow out from thawed dental pulp. More spindle-shaped and flat cells were found in trypsin-liberating cells from magnetically freezing dental pulp compared with the cells from nonmagnetically freezing pulp that were round and less proliferative (Fig. 3).
Vitrification, which can be achieved by rapid cooling method, 37 may avoid ice crystal formation to preserve tissue integrity. 38 Compared with the rapid freezing method, cooling at −80°C in an isopropanol bath (∼−1.0°C/min) and cooling under magnetic cryopreservation at −0.5°C/min was considered as a slow cooling method. 39 Although it is unclear whether vitrification occurs during magnetic cryopreservation, application of a magnetic field has been proven to reduce water molecule aggregation during freezing. 40 While water molecules aggregate to form crystals, a weak electric current is generated, 41 which can disrupt the cell membrane's lipid bilayer, thus results in cell damage during freezing. 42
Preservation of intact tooth has broad clinical applications not only for DPSC isolation but also for tooth autotransplantation. Kaku et al. 17 have shown that magnetically frozen intact tooth in 10% DMSO can preserve greater viability of human periodontal ligament (PDL) cells surrounding the root and the activity of PDL cells correlates to the successful rate of autotransplantation. 6 In addition, periodontal ligament stem cells can be isolated from cryopreserved PDL. 43 Therefore, magnetic cryopreservation providing the better preservation for dental root, in terms of greater cell viability and intact histological structure, is an appropriate approach for long-term preservation of tooth for clinical applications. The structure of Wistar rat incisor pulp tissue we used in this study is also a mature, slender, cone-shaped soft tissue, which is covered by dense hard tissue with one end opened at the root. The root of the post-thawed pulp was the most viable part. Removing hard tissue, which increases the cryoprotectant's contact area with pulp, indeed improves the post-thaw viability of the crown segment. It should be noticed that although removing hard tissue allows the full exposure of the coronal portion to the cryoprotectant, the root and coronal segment viability still differs. Several in vivo and in vitro studies have indicated that the cell types and the extracellular matrix (ECM) molecule expression and distribution are different between dentin and pulp segments.44–46 The different ECM compositions may affect cryoprotectant penetration efficiency resulting in differential responses of the embedded cells to the cryoprotectant. Apicoectomy, a surgical technique to remove dental hard tissue and enlarge the pulp orifice, maybe performed to increase the pulp's cryoprotectant contact surface. 47 Cryopreserved immature teeth with unclosed root ends and mature intact teeth with apicoectomy procedure have a similar revascularization success rate after transplantation. 47
Conclusion
Reversible cryogenic storage of cells or tissue for future tissue repair or replacement becomes an important issue as the long life span of human society develops. This study demonstrates that magnetic cryopreservation is an effective method for intact tooth and dental pulp tissue banking. The required lower concentration of the cryoprotectant and the shorter preequilibration time should improve the successful rate of implantation and allow more convenient and higher biological activity recovery of the extraction and expansion of DPSCs from post-thawed tooth and pulp tissue.
Footnotes
Acknowledgments
This work was supported by the Center for Teeth Bank and Dental Stem Cell, Taipei Medical University, Taiwan, and a grant from Li Jian Biotechnology Corporation Limited (98TMU-IIC-035). The authors also like to thank Dr. Wei-Lin Liu for the technical supports in cell culture.
Disclosure Statement
No competing financial interests exist.