
Abstract
Objective:
The aim of tissue engineering is, for instance, to create a new valve or organ that is similar to the native one. This new construct may have the capability of growth, repair, and remodeling. One instance where tissue engineering offers an enormous advantage is in the treatment of Tetralogy of Fallot. After repair of this defect, pulmonary valve regurgitation with late ventricular dysfunction is not uncommonly observed.
Methods:
In this study, we compared the use of endothelial cells (ECs) and smooth muscle cells (SMCs) derived from the carotid artery (group 1/n=5) with CD133+-cells derived from the bone-marrow (group 2/n=5) of juvenile sheep. Western blot analysis and histology were done before and after percutaneous pulmonary valved stent implantation. After seeding of the pulmonary valved stent with one of the cell groups, the construct was placed in a dynamic bioreactor for 16 days. After incubation, the valved stent was seeded again for 3 days. Finally, the valved stent was implanted percutaneously under angiographic control.
Results:
In group 1, α-actin and calponin were found in the EC and SMC population by using Western blot analysis. In contrast, CD31 was found in EC, but not in the SMC population. Cells from group 2 demonstrated a pure population. CD133+-cells were detected in the CD133+-cell population and no CD133+-cells were found in the negative fraction. Three months after implantation, the transvalvular gradient was significantly higher in group 1 compared to group 2. CD31-staining demonstrated a confluent monolayer in both groups. Immunohistochemistry revealed strong expression of α-smooth-muscle-actin and an in-growth into the leaflets of both groups (p=ns). CD3-, CD20-, CD45-, and CD68-staining confirmed no signs of inflammation in group 2, whereas in group 1 small amounts of inflammation were detected in all analyzed animals. Von Kossa staining revealed mild to moderate calcifications in the annular region of group 1. In contrast, less calcification was detected in group 2.
Conclusion:
Autologous CD133+-cells derived from bone marrow had a better outcome with regard to calcification, inflammation, and transvalvular gradient compared to autologous cells derived from the carotid artery. Therefore, CD133+-cells are more advantageous for tissue engineering of heart valves.
Introduction
The endothelial progenitor cells (CD133+-cells) can be isolated from different cell sources: cord blood, amniotic fluid, bone marrow, or peripheral blood.3–6 CD133+-cells are advantageous because they can differentiate into endothelial cells (ECs) 7 and these ECs have a good prevention against infection. 8 ECs play an important role in tissue responses. Butcher et al. analyzed ECs of aortic and aortic valvular origin. 9 These cells demonstrated different responses to the flow. Aortic valve ECs were aligned perpendicular to the flow, whereas the aortic ECs were aligned parallel to the flow. These different results showed that the vascular ECs have different responses to mechanical forces compared with the valvular cells. This is an important finding for the use of cells for cardiovascular tissue engineering.
In contrast to ECs, it is unknown whether smooth muscle cells (SMCs) can differentiate out of these CD133+-cells. Nevertheless, SMCs are needed for preparing a typical heart valve because they were found in the ventricularis of a native leaflet. 10 These cells are highly specialized and their principal function is contraction, regulation of blood pressure, and distribution of blood flow. 11 The role of SMCs is not yet clearly defined in tissue-engineered heart valves (TEHV).
However, folded biological heart valves were endovascularly implanted into the pulmonary valve in an animal model 12 and later on clinically 13 at the beginning of this century. The bovine jugular vein valved stent, 13 for instance, is a good alternative to the Synergraft® valve, 14 which becomes clinically degenerated and calcified very quickly. 14 However, the transcatheter delivered Melody® valve is a bovine jugular vein segment sutured into a platinum iridium stent and has also the potential to calcify.
In comparison, the Contegra® conduit is a bovine jugular vein graft and the Matrix P Plus® conduit, which is a combination of a porcine heart valve and an equine pericardial patch is completely decellularized before implantation and induces a supravalvular stenosis.15,16 Furthermore, the Matrix P Plus® shows also inflammation, infiltration, and a severely fibrogenic pseudointimal reaction. 16 These commercially available valve prostheses are used for treating children with right ventricular outflow tract (RVOT) dysfunction with the support of the heart–lung machine. At this time, optimal TEHV are available neither for children nor for adults.
Our group already demonstrated the feasibility of implanting a completely percutaneous autologous tissue-engineered pulmonary valve into an ovine model using a self-expanding nitinol stent.17–19
The aim of this study was to compare ovine ECs and SMCs derived from the carotid artery as already described with ovine CD133+-cell-derived cells from the bone marrow in terms of their suitability for TEHV. The reason for doing this is to have a reliable cell source for tissue engineering an optimal heart valve.
In case a patient needs an autologous heart valve, usually stem cells from amniotic fluid, cord blood, or peripheral blood are not available. For these patients, CD133+-cells from bone marrow will be most useful for tissue engineering.
Unfortunately, blood contains only 0.01%–0.1% of CD133+-cells, but bone marrow contains 1% 20 and it is consequently easier to isolate them from the bone marrow.
Materials and Methods
In this study, 10 pulmonary heart valves were implanted in sheep (weight between 32–45 kg, age between 6 and 9 months) and analyzed 3 months after implantation. Animals received human care in accordance with the Principles of Laboratory Animal Care and the Guide for the Care and Use of Laboratory Animals (National Institutes of Health, Publication 85–23, revised 1985). An ethics committee on animal research at the Kiel University approved the protocol.
Valve and submucosa harvest
Porcine hearts and small ovine intestines were obtained under clean conditions from a local slaughterhouse. Pulmonary valves were excised and freed of adherent fat and most of the myocardium, leaving only a thin ridge of subvalvular muscle tissue and the pulmonary artery. Two porcine pulmonary valves were dissected to match the size of the stent and the valve for each stented valve. The valve diameter was determined with a Hegar sizer before sinus removal and muscular trimming. 21 Segments of the ovine small intestine were cleaned by thoroughly washing with phosphate-buffered saline (PBS) (PAA Laboratories Inc.), followed by incubation in a povidone–iodine solution (Mundipharma) for 15 min. Decontaminated segments were repeatedly washed with PBS, and the mucosa and any connective tissue were removed mechanically. The remaining small intestinal submucosa was transferred into PBS containing an antibiotic solution and stored at 4°C for 48 h as described elsewhere. 21
Cell harvest
Two groups of cells were separated. For one group (group 1), a 5 cm-long segment of the recipient ovine carotid artery was removed under sterile conditions. ECs were obtained using 0.2% Collagenase A (Roche Diagnostics GmbH) and cultured in a 24-well plate (Nunc GmbH) in a cell culture medium [M199-medium (Biochrom)], 1% Penicillin–Streptomycin, 10% fetal calf serum, and recombinant human fibroblast (Fibroblast growth factor [FGF]; Peprotech).
The carotid artery segments were cut into 1-mm2 pieces, then divided into two wells of a 6-well plate and cultured in the cell culture medium (M199-Medium). Both cell populations were incubated at 37°C and 5% CO2 and serially passaged with accutase (PAA Laboratories GmbH). 21
In the second group (group 2), 5 mL of bone marrow of juvenile sheep was diluted with PBS and layered onto Ficoll for isolation of mononuclear cells (MNCs). 1×107 MNCs were washed twice with PBS and 1×105 CD133+-cells were isolated by using anti-CD133+ (Miltenyi) and the EasySep® Biotin Positive Selection Kit (Stemcell Technologies). These cells were cultured in a 96-well plate with the cell culture medium [M199-medium (Biochrom)], 1% Penicillin–Streptomycin, 10% fetal calf serum, and recombinant human fibroblast (FGF; Peprotech).
Decellularization and reseeding procedure
The complete valved stent (a self-expanding nitinol stent with the small intestinal submucosa and integrated valve scaffold) was washed for 30 min at room temperature in the povidone–iodine solution and sterile PBS, followed by another overnight incubation at 4°C in an antibiotic solution. After decontamination, the valves were placed in a solution of 0.05% trypsin and 0.02% EDTA (Biochrom AG) at 37°C and 5% CO2 for 12 h during continuous three-dimensional shaking. After removal of the trypsin-EDTA, the constructs were washed with PBS for another 24 h to remove residual cell debris.19,21 The decellularized matrices were immediately processed for subsequent cell seeding.
After cell expansion to a total quantity of ∼1×107 cells, SMCs or CD133+-cells were trypsinized, resuspended in the culture medium, and seeded onto the decellularized pulmonary valves in a sequential seeding process that involved 3 days of static seeding on the inner and outer surface. Subsequently, the valves were placed in a pulsatile flow system (bioreactor) and exposed to defined physical signals with a fixed frequency (1 Hz) and pressure conditions (3 L/min and 60/40 mm Hg) over a time period of 16 days. A final coating with a mix of ECs and SMCs (1×107 cells) or CD133+-cells for 3 days under static conditions, which allows the cells to form sediment on the valve wall and the leaflets, completed the reseeding. The entire culture period was conducted in a standard incubator at 37°C and 5% CO2. A PS supplement (5 mL) was added every 4 days. Viability of all cell types has been tested before and after reseeding.19,21
Western blot analysis
Cells of both groups were lysed with a complete lysis puffer (Roche) and processed for protein measurement. A protein concentration of 15 μg for each cell lysate was used. The protein was separated by sodium dodecyl sulfate–polyacrylamid gel electrophoresis and later electrotransferred to a nitrocellulose membrane. Nonspecific antibody binding sites were blocked by incubation with a blocking buffer (1× TBS/0.5% Tween 20 with 5% nonfat dry milk) for 1 h at room temperature. After this incubation, the membranes were incubated with primary antibodies (α-actin, Beckmann Coulter; Calponin, Abcam; CD31, Abbiotec; CD133, Miltenyi) at 4°C overnight. Cell lysates were made from both analyzed groups followed by Western blot analysis. Anti-CD31, specific to ECs as well as α-actin, a special antibody against SMCs, was used to detect these cell populations. The CD133+-cell antibody is specific to CD133+-cells.
After washing with TBS/T, membranes were incubated with secondary antibodies (goat anti-mouse, swine anti-goat; Santa Cruz technologies), then diluted in 2.5% nonfat dry milk for 1 h at room temperature. Proteins were detected by incubating the membrane with ECL Plus (GE Healthcare Europe). Protein expression was analyzed in an LAS-3000 Imager from Fuji (Raytest).
Implantation procedure
The size of the native valve was measured directly before implantation using angiography. For implantation, the construct was folded carefully and inserted into a modified commercially available delivery system. 17 Through a 22-French sheath, it was positioned into the right femoral vein. The 20-French delivery system was inserted and the autologous tissue-engineered valved stent was successfully positioned on top of the native pulmonary valve under fluoroscopic control as previously described. 17 The sheep received Ketanest (2%) and Propofol (2%) for sedation, then Cefuroxime (100 mL), Heparin (5000 IU), and Protamin (5000 IU) during implantation and Rimadyl (1 mL) at the end of the study. The antibiotic Baytril (10%) was given on the following 5 days for prevention of endocarditis. Three months after implantation, animals underwent re-angiography with subsequent stent explantation followed by postmortem investigation and processing of the leaflets for histology and immunohistochemistry as described elsewhere. 19
Echocardiography
Transthoracic echocardiography (TTE) was performed after implantation, after 6 weeks and after 3 months with the Ultrasound System Five (Vingmed Sound) using a multiplane 2.5-MHz transducer probe. The echocardiographic probe was applied at the right hemithorax between the fifth and sixth intercostal space. Echocardiographic evaluation of the tissue-engineered valve status was performed using the M-mode, two-dimensional, color-flow, pulsatile, and continuous wave Doppler. TTE was used for standard longitudinal and cross-sectional views and was recorded, stored, and analyzed offline by an experienced investigator. Maximum velocities across the pulmonary valve were determined by a continuous wave Doppler imaging transducer. Semiquantitive assessment from grade 0 to 4 of pulmonary regurgitation (0 absence, 1+ trivial, 2+ mild, 3+ moderate, 4+ severe) was based on the length and width of the regurgitant jet and the distance that it reaches into the RVOT on the parasternal short-axis view. The transvalvular pressure gradient was determined using the Bernoulli equation.
Angiography
An angiography unit (Optimus M 200; Philips Medizin Systeme) was used for fluoroscopic investigation of the position and function of the tissue-engineered valves. Semiquantitive assessment from grade 0 to 4 of pulmonary regurgitation was performed as described in the echocardiography section. Angiography of the valved stent was performed 5 min and 12 weeks after implantation.
Hemodynamic measurement
Arterial pressure, right ventricular pressure (systolic, diastolic, and mean), and pulmonary artery pressure (systolic, diastolic, and mean; use of a microtip Millar Catheter, Millar Instruments, Inc.) were recorded using Haemodyn-Software (Hugo Sachs Electronics). The software calculates the maximum of the first derivative of the ventricular pressures (dp/dtmax) as an indicator of the contractility and its minimum (dp/dtmin) as an indicator of the relaxation behavior. Times of pressure measurements were baseline, 5 min after implantation, and at 3-month follow-up.
Postmortem investigation
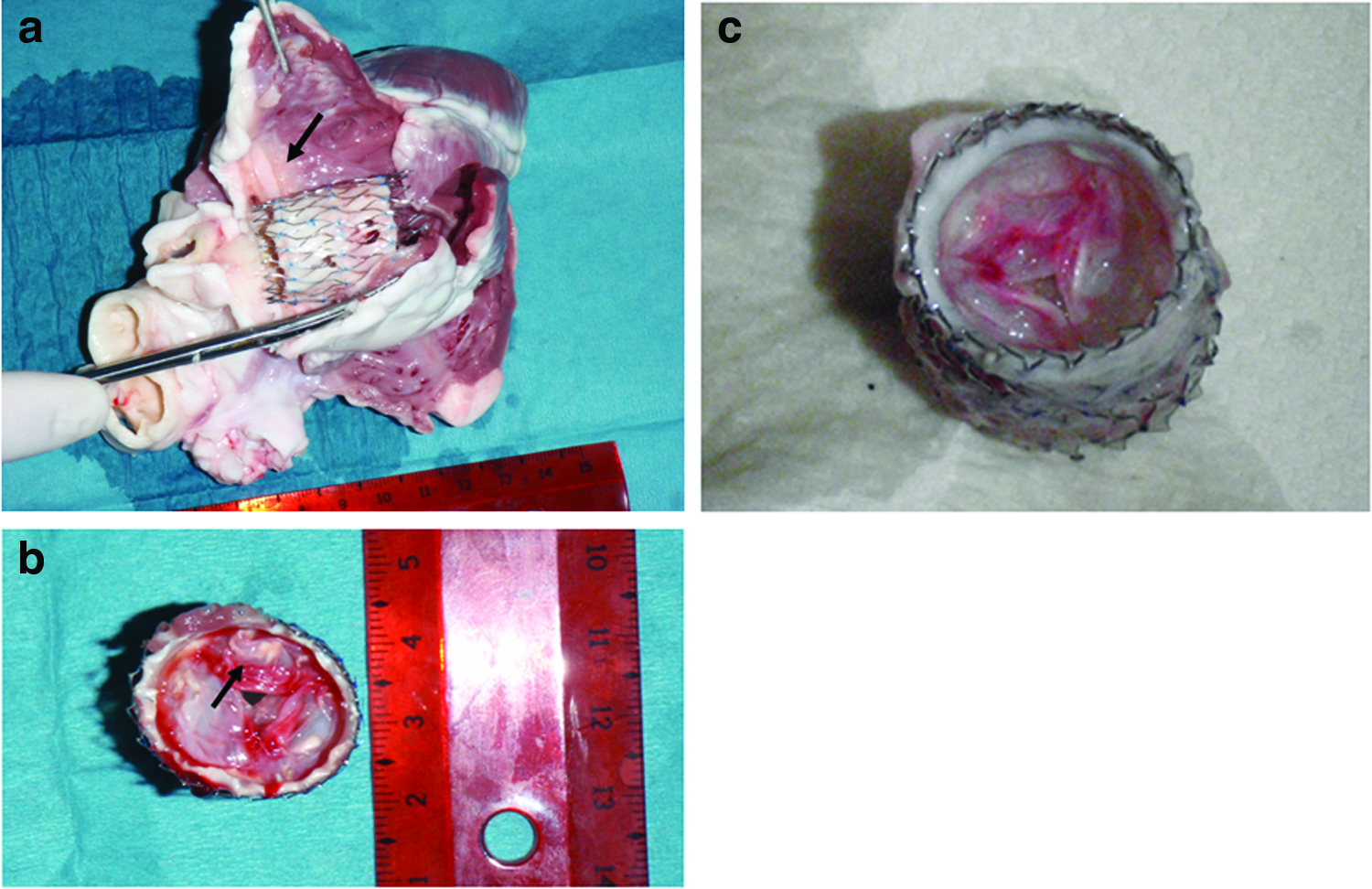
The explanted tissue-engineered pulmonary valved stent was analyzed by postmortem investigation. The morphology of the leaflets and calcification were analyzed. The calcification was graded as follows: 0=no detection of calcification; grade 1=microcalcification was observed in the form of small spots; grade 2=mild localized calcification; grade 3=moderate calcification; and grade=4 severe calcification. 22 Sub-, supra-, and valvular areas were dissected (Fig. 1). The position of the stent was determined and, finally, the damage or fracture of the stent was analyzed.

Anatomical view of the analyzed postmortem sections after complete dissection of right ventricle and A. pulmonalis specimens were taken from sub-, supra-, and valvular areas.
Histology and immunohistochemistry
The valved stent was fixed in 4% formalin. Each leaflet was separated and carefully removed from the stent. One leaflet was processed for histology. Specimens were fixed for 72 h at 20°C in 4% paraformaldehyde in a 0.1 mol/L cacodylate buffer, pH 7.4. They were washed in tap water for 2 h, dehydrated in graded alcohol, and finally embedded in paraffin (Merck). Sections (1-2μm) of each tissue sample were deparaffinized and rehydrated. For general morphology, serial sections were stained with the hematoxylin–eosin stain (cellular components and nuclei) and movat-pentachrome. For identification of ECs on the tissue surface, the CD31 antibody was conducted and to identify myofibroblasts (MF) α-actin-related antigen staining. To quantitively assess inflammation, anti-CD3 specific for T-cells (DCS), anti-CD20 for B-cells (Biologo), anti-CD45 for leucocytes (AbdSerotec), and the CD68 antibody for macrophages (Biologo) was used. Signs of inflammation were graded in grade 0 (no inflammation), grade 1 (micro- >10 positive cells), grade 2 (mild- >20 positive cells), grade 3 (moderate- >40 positive cells), and grade 4 (strong inflammation >60 positive cells) if it was possible. 23
Von Kossa staining was applied for identification of microcalcification. Sub- and supravalvular areas, the annular region and the edge of the leaflets were analyzed. The calcification was graded as follows: 0=no detection of calcification; grade 1=microcalcification was observed in the form of small spots; grade 2=mild localized calcification (big spots); grade 3=moderate calcification (small and big spots); and grade 4=severe calcification (big black areas). 22
Sections were analyzed and documented using brightfield light microscopy (Axiovert; Zeiss) as described elsewhere. 19
Statistical analysis
Values are presented as mean±standard deviation. Data were analyzed based on the paired Student's t-test to compare related data for normally distributed data; non-normally distributed data were analyzed by the SPSS 10.1 software (SPSS, Inc.). The p-values less than 0.05 were considered statistically significant.
Results
The results are also given in Figs. 1–9 and Tables 1–3.

Western blot analysis of endothelial cells (ECs) and smooth muscle cells (SMCs) derived from the carotid artery with
Postmortem investigation of the explanted heart
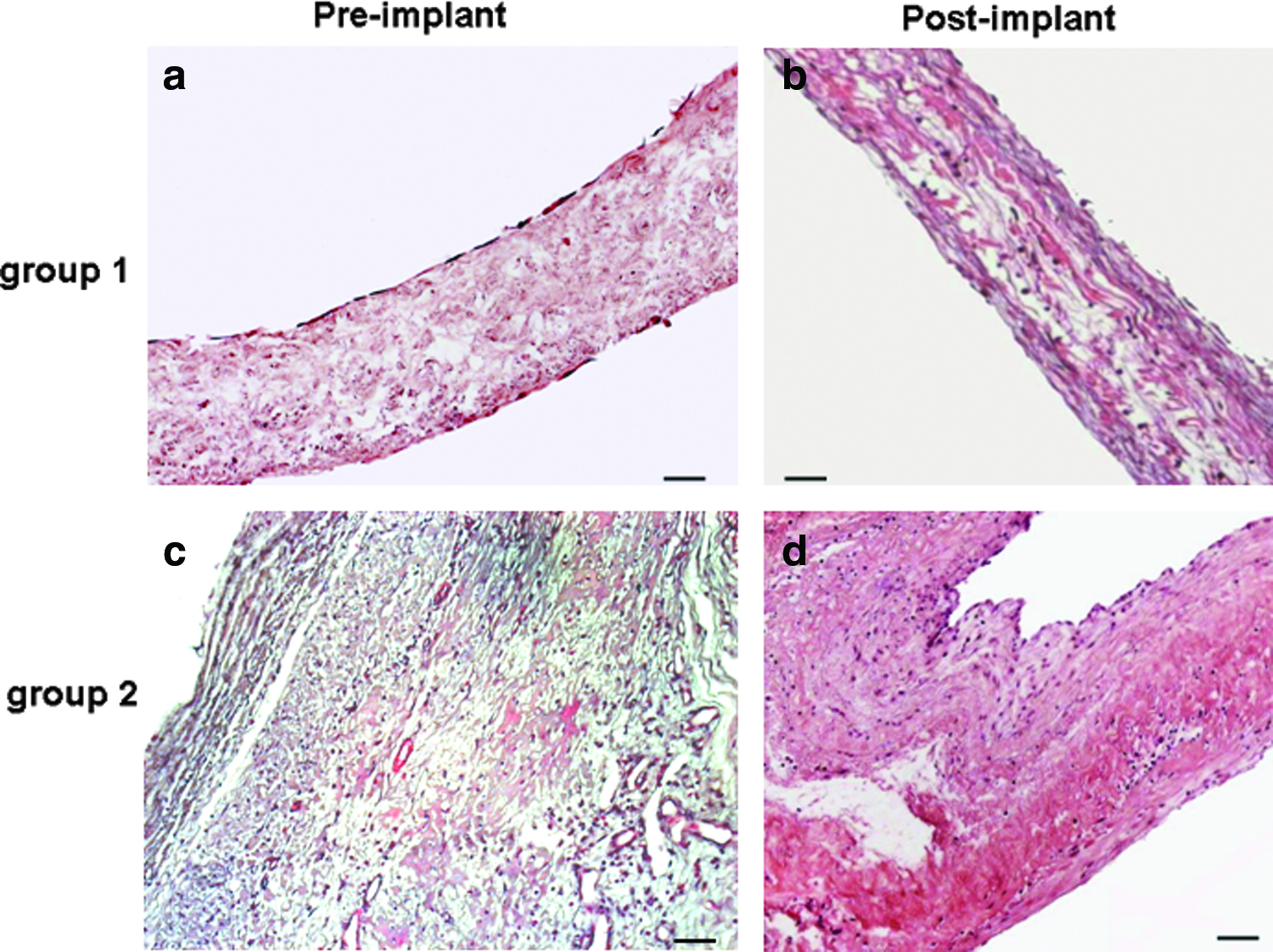
Hematoxylin and eosin (HE) staining. General histological HE staining of the leaflets:
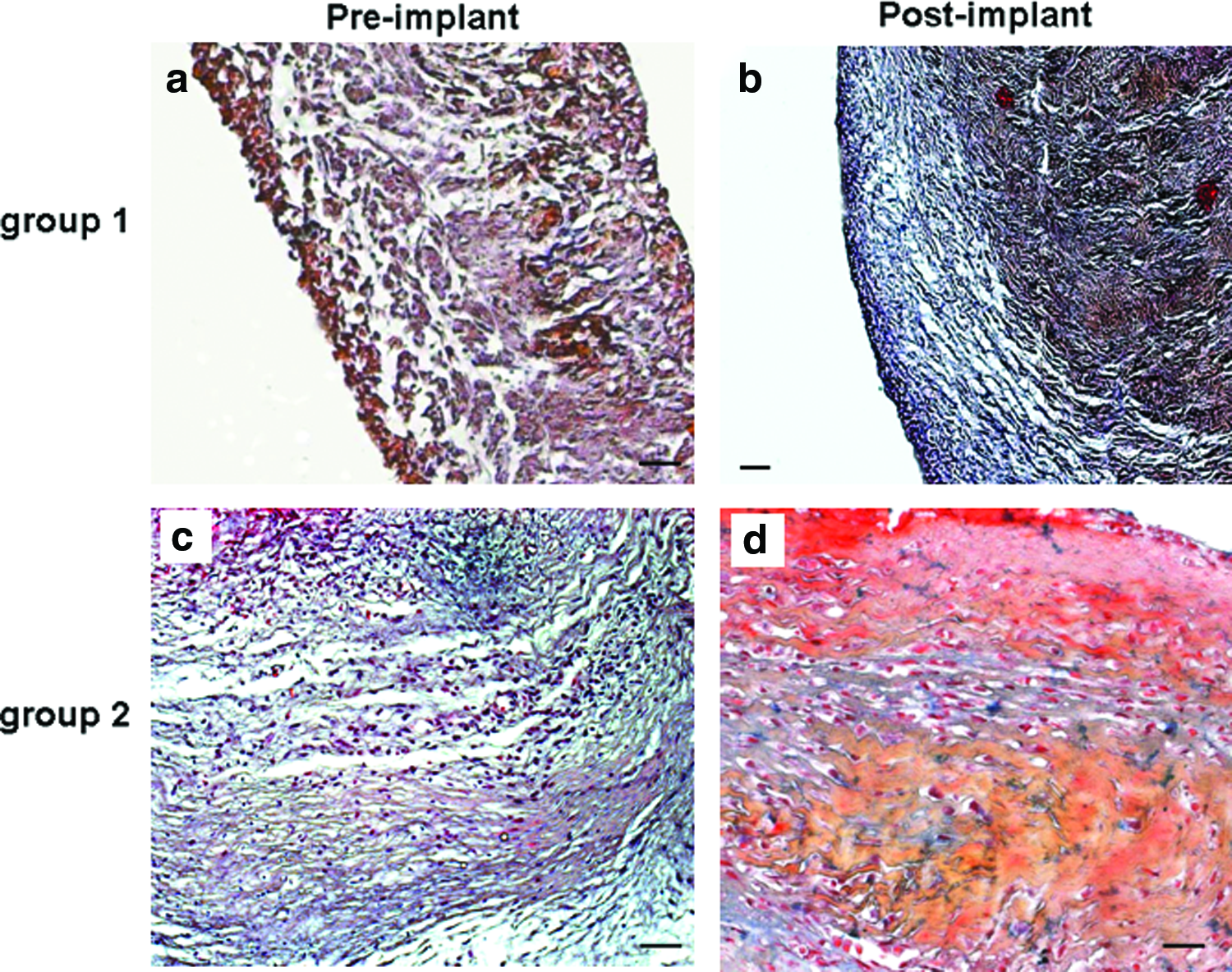
Movat-Pentachrome staining of the leaflet

Endothelial staining.
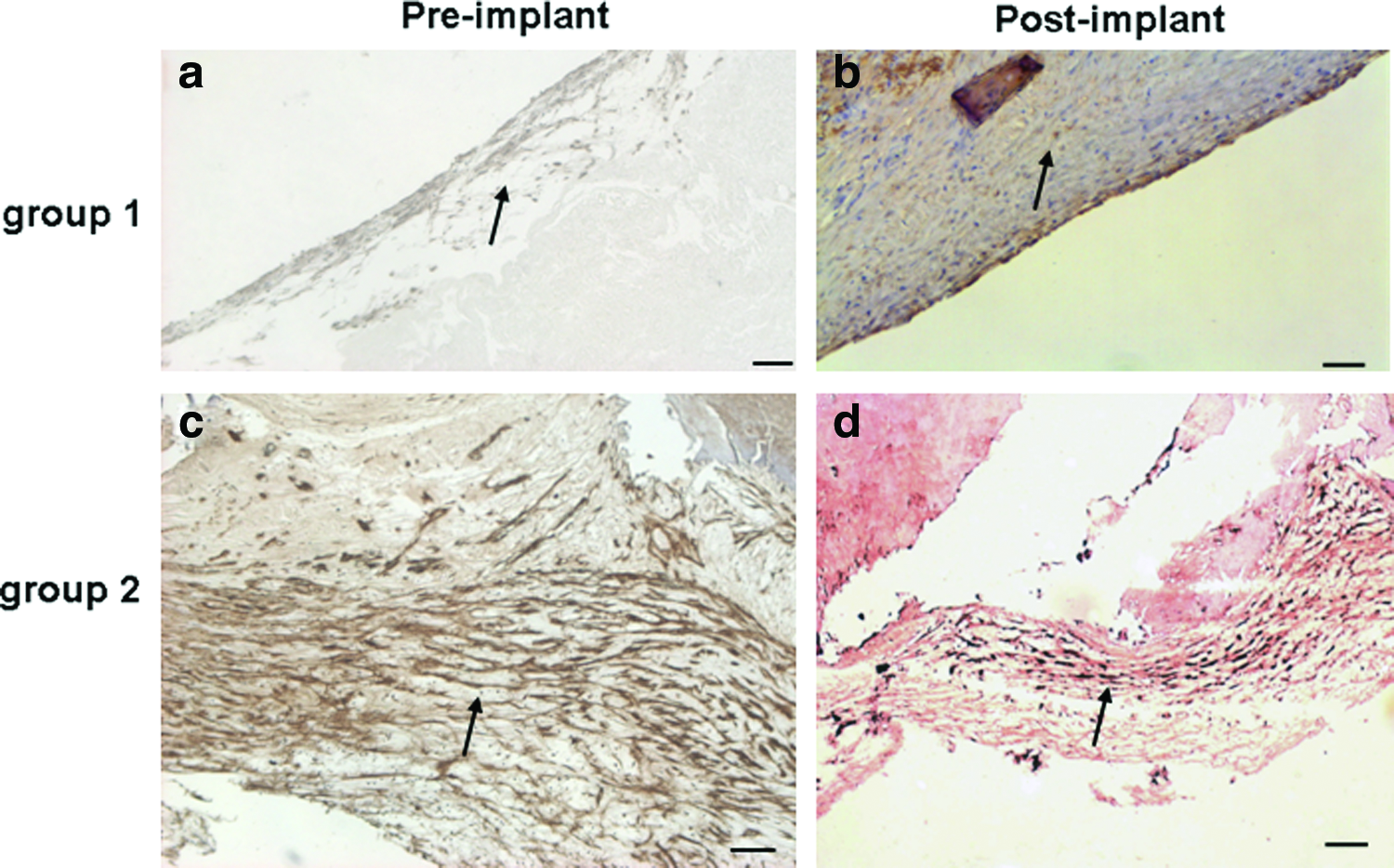
Smooth muscle actin-staining.
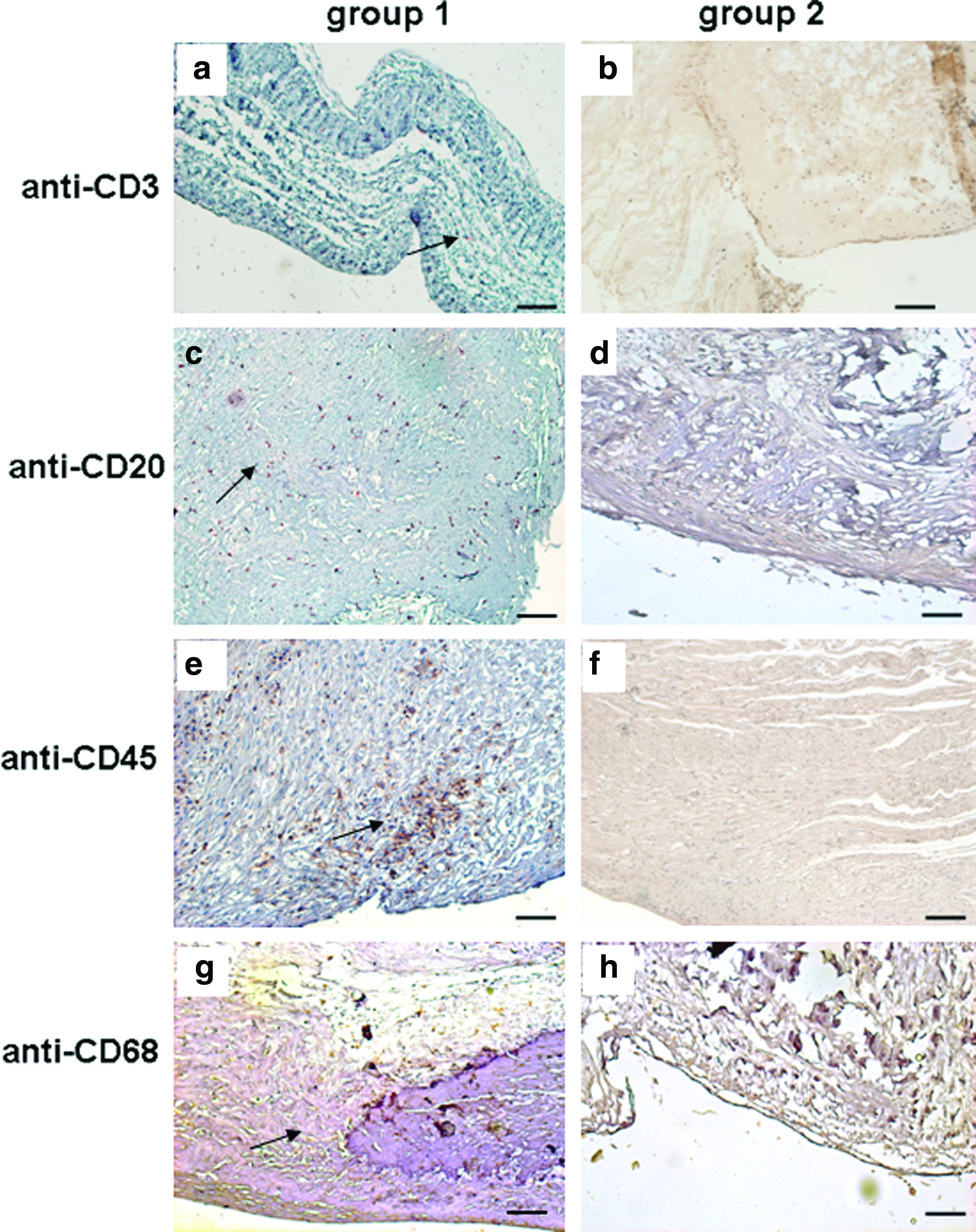
Immunohistochemical staining of inflammation.
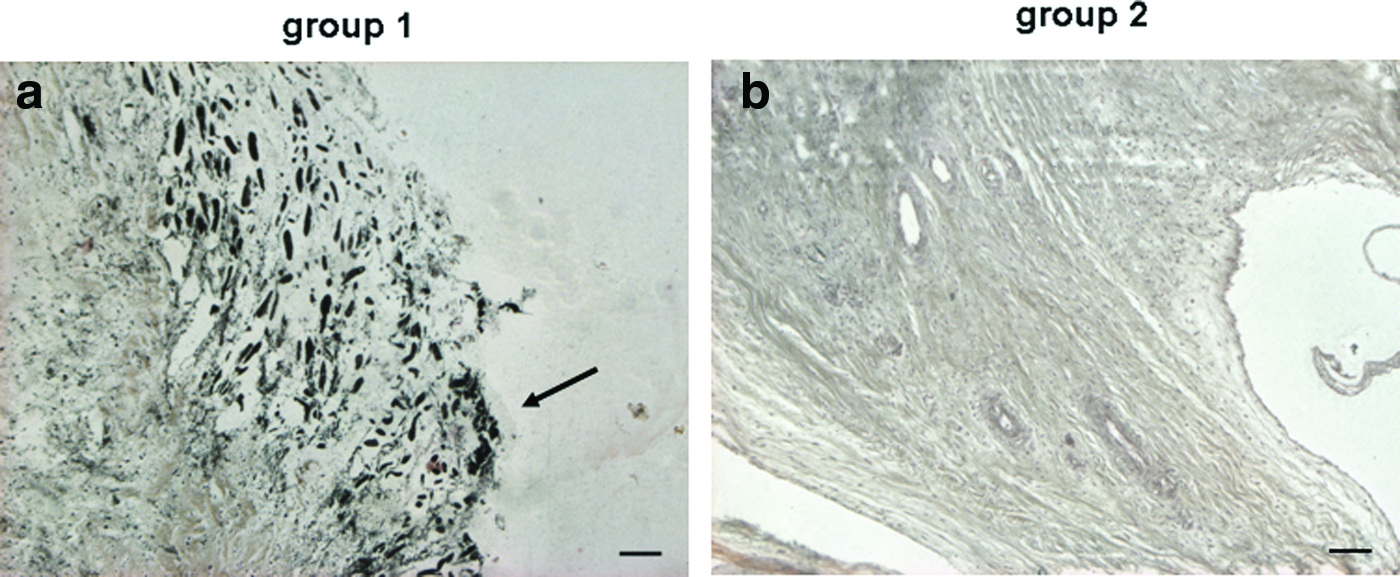
Histological staining of calcification. Von Kossa staining to identify calcification
Differences between baseline, 5-min postimplantation and 3-month follow-up were not seen, except in MAP mean between baseline and 3-month follow up.
paired t-test before and 3-month follow-up (significant p<0.05); ns=no significance.
RA, right atrium; RVP, right ventricle pressure; PAP, pulmonary artery pressure; MAP, mean arterial pressure; values are given in mmHg.
No differences between baseline, 5-min postimplantation and 3-month follow-up were analyzed.
paired t-test before and three months after implantation (significant p<0.05); ns=no significance.
Values are given in mmHg.
Values are given in mmHg; apaired t-test before and three-month follow-up (significant p<0.05).
Presence of smooth muscle cells (α-actin): absent 0, focal 1, complete 2.
Presence of endothelial cells (CD31): absent 0, focal 1, complete 2.
Paired t-test significance: p<0.05.
Inflammation was graded as follows: 0 absent, 1 micro >10 positive cells, 2 mild >20 positive cells, 3 moderate >40 positive cells, 4 strong >60 positive cells.
Von Kossa staining (calcification) was graded as follows: 0 absent, 1 micro small spots, 2 mild big spots, 3 moderate small and big spots, 4 strong big black areas.
Western blot analysis
In group 1, alpha-actin and calponin was found in the EC population as well as in the SMC fraction. This means that SMCs were found in the EC and SMC population. CD31 was detected in the EC fraction and not in the SMC population (Fig. 2a–c). These findings demonstrated a pure SMC population and contamination of ECs with SMCs. In addition, in the EC and SMC populations, no CD133+-cells were found. Whereas, in group 2, CD133+-cells demonstrated only CD133+-cells in this cell population, and in CD133 negative cell populations no CD133+-cells were found (Fig. 2d). Therefore, a pure CD133+ cell population was isolated from the bone marrow.
Echocardiography
Echocardiography performed shortly afterward, 6 weeks and 3 months after implantation demonstrated good opening and closing characteristics of the entire group of the implanted valves. Valve competence was maintained during follow-up, with 100% having no or minimal pulmonary regurgitation under echocardiography control (grade 0–1). No differences between the two study groups were detected.
Angiography
Shortly after implantation and at the time of explantation (3 months), angiography demonstrated good opening and closing characteristics of the implanted valves and trace regurgitation induced by the angiography catheter (grade 0–1). No differences were seen in both analyzed groups.
Hemodynamic measurements
During the deployment procedure, rhythm disturbances occurred in all animals. In addition, one sheep developed atrial fibrillation, which was pharmacologically improved to a sinus rhythm. The maximum of the first derivation and its minimum of both ventricles were unchanged compared to baseline at different time points (p=1.8 for group 1 and p=2.0 for group 2). Additionally, hemodynamic data are given in Table 1a and b, which shows no differences between baseline and 3-month follow-up. The mean arterial pressure in group 1 indicated a significant difference between baseline and 3 months (p<0.02). The peak-to-peak gradient across the valved stents was 2.6±0.9 and 2.0±0.5 mmHg (p=0.17) initially, and 5.0±2.0 and 3.5±0.4 mmHg (p=0.03) at follow-up in group 1 and 2, respectively (Tab. 2).
Postmortem investigation
Macroscopic analysis of the pulmonary heart valved stent demonstrated an orthotopic position in all analyzed sheep of both groups (n=10). Postmortem investigation of the leaflets revealed smooth surfaces without any thrombus formation of the two experimental groups. No paravalvular defects and no stent fractures of the implanted valved stents were observed. The valved stents were flexible and the leaflets were thin without any thickening. Cardiac structures were intact and no lesions were noticed. Figure 3a demonstrates an example of the native valve that was completely pushed aside (see black arrow). This was observed in all animals from both study groups. The analyzed valves in group 1 demonstrated a point-shaped covering of calcification in four of five (see black arrow in Fig. 3b), whereas in group 2, only one of five animals showed those signs of calcification (Fig. 3c). In Fig 3b and c, small amounts of blood are still visible after explantation.
The observed grade of calcification was 2.3±0.9 in group 1 and in group 2 0.5±0.6 (p=0.01).
Histology and immunohistochemistry
Hematoxylin–eosin staining showed general morphology of the leaflets in all analyzed leaflets before implantation and 3 months afterwards. The leaflets seeded with cells of group 2 demonstrated better cell-adhesion before and also after implantation in contrast to group 1 (Fig. 4a–d). The use of Movat pentachrome staining enabled visualization of the main classes of extracellular matrix components in ovine tissues of pulmonary leaflets. These include the major proteins, collagen (yellow) and elastin (red), as well as soluble molecules, such as proteoglycans and glycoproteins (blue). The black spots depict the nuclei of these cells. A classic formation of the matrix proteins in the four major tissue layers (arterialis, fibrosa, spongiosa, and ventricularis) was visible (Fig. 5a–d).
ECs demonstrated the typical morphology covering the SMCs: Anti-CD31 is an indicator for endothelial character before and after implantation in both analyzed groups (Fig. 6a–d). Anti-smooth muscle actin demonstrated existence of α-smooth muscle actin and an in-growth into the leaflets (Fig. 7a–d). In-growth into the leaflet was stronger with the cells derived from the bone marrow (see Fig. 8c, d, Table 3). No significant differences between the two groups regarding thickness, layer formation, general cellularity, and various cell types were revealed.
Anti-CD3, anti-CD20, anti-CD45, and anti-CD68 (Fig. 8a–h) staining revealed a small amount of inflammation in group 1 (grade 1–2). In contrast, in the valved stents of group 2, no signs of inflammation with anti-CD3, anti-CD20, anti-CD45, and anti-CD68 (grade 0) were observed (Table 3).
Von Kossa staining demonstrated mild to moderate calcification (grade 2–3) in the annular region of group 1, whereas the other areas did not reveal any calcification in four of five sheep. In contrast, in group 2, only microcalcifications (grade 1) were detected only in one of five sheep (Fig. 9a and b, Table 3). The vessel-like structures were found at the base of the leaflets in both groups.
Discussion
Percutaneous pulmonary valved stent implantation is an upcoming technique for younger patients, but also in older patients with congenital heart failure, developed to avoid on-pump operations. Its combination with tissue-engineered valves offers another advantage due to expected long durability. Unfortunately, there are still various problems.
Limitations and problems
The first is RVOT abnormalities in congenital heart diseases which are reconstructed by surgeons using allograft valves. These valves show some immunological response, which can lead to potential graft failure. 24 However, in one study dealing with RVOT reconstruction, much fewer immunological reactions were detected using decellularized human allograft valves in a long-term study compared to cryopreserved human allograft valves. 25 In contrast, two other groups demonstrated that decellularized xenografts cause some severe problems: inducing stenosis and inflammatory infiltration, for example, Matrix P Plus®- and Synergraft®-conduits.14,16,26 Matrix P Plus® was not associated with any calcifications, but the signs of inflammation and stenotic formation were very severe. 16 At the same time, Synergraft® conduits showed calcific deposits and foreign body-type reactions, which also resulted in a stenosis. 14 Therefore, these valve conduits are suitable for use in humans, but with a dramatic outcome. The histological staining and intensive analysis of some nonimplanted conduits indicated that they were not completely decellularized. These interesting results were found by Simon et al. and the Rüffer's research group.14,16
To avoid incomplete decellularization, our valved stents were completely decellularized as described elsewhere.19,21
In this study, we found good valve function and structural outcome after three months using echocardiographic, angiographic, histologic analysis, and postmortem investigation. In the echo- and angiocardiographic control, after 3 months, good opening and closing characteristics of the tissue-engineered valves were found. All of them demonstrated no or minimal regurgitation and a low transvalvular gradient. However, the transvalvular gradient was higher (p=0.03) in group 1 (ECs and SMCs derived from carotid artery; 5.0±2.0 mmHg) compared to group 2 (CD133+-cells derived from bone marrow; 3.5±0.4 mmHg) (Table 2). The higher transvavular gradient of group 1 could have been induced by the observed leaflet calcification.
Hemodynamic differences between the two study groups were not detected. However, the mean arterial pressure changed slightly in group 1.
EC function
Endothelial dysfunction has also been shown to be predictive of future adverse cardiovascular events, and is also present in inflammatory disease, such as rheumatoid arthritis and systemic lupus erythematosus. 8 In one publication, 8 the authors demonstrated that if endothelial dysfunction was present, the inflammation rate was higher than in healthy patients. So, in our mixed population, we suggest that the endothelial function is compromised because the Western blot analysis on the protein level demonstrated the same amount of ECs and SMCs in the EC fraction before seeding. Therefore, the ECs which are seeded onto the leaflets 3 days before implantation are not a pure fraction of ECs. This might be a disadvantage for group 1 because the mixture of cell populations might not provide good protection against inflammation and calcification.
Gehling et al. could demonstrate that CD133-cells can be induced to differentiate into ECs in vitro using the cytokines vascular endothelial growth factor and stem cell growth factor. 7 In our experiments, we only use the cytokine FGF.
It seems that the CD133+-cells in group 2 are more capable of protecting the leaflet from inflammation and calcification than the mixed cells of group 1.
Therefore, the ECs of the carotid arteries are not proved to work as valvular ECs. Here, CD133+-cells still have stem cell potential and, perhaps, that could be one reason why the valve is better protected against inflammation in case of different responses to the flow.
The poor outcome of group 1 is because of the use of mixed population of arterial EC and MF for seeding the surface of the valves. In vivo activation of the MF could lead to intimal proliferation and subsequent calcification of the implanted tissue.
Furthermore, Sodian et al. 3 demonstrated a generation of viable heart valves with good results. These findings could be a significant step in the development of new clinical strategies for the treatment of congenital heart defects by using CD133+ cells.
The reason we did not find any calcification in group 2 is not yet determined. However, the cause might be a better dispersion of these progenitor cells on the surface of the leaflets than in group 1. Nevertheless, the calcification process of the bioprosthetic valve is very complex as has been described elsewhere. 27
Cell isolation resources and seeding
Shinoka and his colleagues used bone marrow-derived MNCs for TEHV, but they curiously implanted them as vena cava inferior interposition grafts in juvenile lambs. 28 After isolation of bone marrow-derived MNCs, the viability of these cells was analyzed, and then directly used for cell seeding. Two hours after the seeding procedure, the valves were implanted. The results were promising because they have found ECs and smooth muscle, but they did not know if these MNCs came from the in vitro cultivation or from sheep's blood. In our studies, we used bone marrow-derived CD133+-cells, and these cells were cultivated for 30 days. Our results were also promising, but we needed more time for cell cultivation. This could be a disadvantage, but we wanted to know in which cell line these bone marrow-derived CD133+-cells will develop. Therefore, experiments with regard to this are planned, that is, via marking cells from in vitro cultivation.
Schmidt et al. used MF from ovine jugular veins and ECs from ovine carotid arteries. 29 These cells were cultivated and MF were seeded onto heart valved stents with fibrin as a cell carrier. These constructs were placed in a dynamic bioreactor and later seeded with ECs. Then, the valved stent was implanted transventricularly and explanted after 4 or 8 weeks. The valves were thickened, but the mechanical profiles demonstrated sufficient tissue strength. In contrast, our heart valved stents were thin and pliable in both groups, but better in group 2.
In contrast to our group, other groups isolated CD133+-cells from different cell sources: Sodian et al., 3 for instance, isolated them from cord blood and Schmidt et al. 4 from amniotic fluid. These human umbilical cord blood-derived cells were isolated and cultivated for 4–6 weeks. 3 However, Schmidt et al. isolated human amniotic fluid cells using the same isolation kit. 4 Both groups performed in vitro studies and showed good results. Additional in vivo experiments have not yet been performed. Therefore long-term studies are required. Another aspect is that these CD133+-cells derived from human umbilical cord blood were cryopreserved for 12 weeks. When a patient needs his own cord blood cells, one does not know whether his umbilical cord blood cells will work after 40 years. This question has not been answered yet.
Another research group isolated CD133+-cells from human bone marrow by a similar technique to ours. They sprayed these cells with fibrin onto their decellularized cryopreserved pulmonary valve, which was sutured into a metal bracket. After 7 days of cultivation in a bioreactor, a histological analysis followed. 5 Further in vivo studies are also required. All of these techniques, including ours should require one cell harvesting and one operation.
In contrast, Jordan et al. 6 isolated CD133+-cells from peripheral blood by using a sterile stem cell purification cartridge, which was placed in a femoral vessel by a more complicated technique: cells were cultured and later seeded onto the decellularized porcine pulmonary heart valve. The valves were unseeded, cell seeded, or conjugated with a CD133-antibody and implanted on-pump in sheep for 1 and 3 months. Interstitial cells and structure proteins of the conjugated valves increased from 1 to 3 months. No calcification was detected and the mechanical properties were greater in the conjugated group in contrast to the unseeded and cell-seeded group. These good in vivo results are a first step to construct a TEHV very quickly. However, the arteriovenous shunt by using this sterile cartridge easily cause complications in the patient that is, thrombosis in the groin.
Another research group isolated CD133+-cells from bone marrow, which were used to deliver a collagen patch on cryoinjured rat heart angiogenesis and arteriogenesis. 30 This working group demonstrated that the use of CD133+ cells produced no better results than the use of ECs and SMCs.
In our study, we used CD133+-cells from bone marrow since there will be patients who need a TEHV, but there are no CD133+-cells or other stem cells from amniotic fluid or cord blood, the bone marrow cell source will be of most interest.
Even growing of these progenitor cells is a time intensive method. Two groups found a way to use the cells directly after isolation that is more time saving.5,31 Kaminski et al. isolated CD133+-cells from the bone marrow using CliniMacs®. These cells and autologous fibrin were sprayed onto the valved stent and afterward the prepared construct was incubated in a dynamic bioreactor for 7 days. 5 This first experiment was done in vitro and might be a good alternative method to reduce longer waiting time for patients.
Hoerstrup and his group demonstrated a hybrid operation in nonhuman primates. 31 During one procedural step, they prepared the heart valved stent and obtained autologous bone marrow-derived MNCs and seeded them together with fibrin onto the valve. After mini-sternotomy, the construct was implanted transventricularly directly into the pulmonary position by a catheter. After 1 month, they showed the feasibility of this method and an adequate functionality of the implanted TEHV. They mentioned that use of this hybrid technique could reduce the number of conventional operations. 31
In contrast, in our study, we combined the percutaneous implantation technique with the tissue engineering of heart valves and we can demonstrate good results by using a mixed population of ECs and SMCs, but an even better result using CD133+-cells. Up to now, it is only possible to isolate the CD133+-cells from the bone marrow. Knowing that it is very difficult to separate CD133+-cells from the blood, nevertheless, it is easier and less invasive for the patient. This is still planned to be done in further studies.
Histology
Histologically, a confluent monolayer was demonstrated by CD31-staining in both groups. Immunohistochemistry revealed strong expression of α-smooth muscle actin and an in-growth into the leaflets in the two groups. However, it is still unknown if these α-smooth muscle actin or CD31-positive cells developed from the seeded CD133+-cells or were derived from cells of the ovine blood. In our further studies, we plan to characterize these cells.
This study describes our first results using CD133+-cells. These autologous cells show great potential for use in autologous tissue-engineered valved stent implantation. Analysis after CD3-, CD20-, CD45-, and CD68-staining confirmed no signs of inflammation in all animals in group 2, whereas in group 1, small amounts of inflammation were detected in all animals. So, small amounts of infiltration of B- and T-cells and macrophages were revealed in this group. In contrast, the valved stents seeded with CD133+-cells demonstrated no signs of inflammation. In addition, von Kossa staining revealed mild to moderate calcifications in the annular region of the valved stents as seen in group 1. In contrast, only microcalcifications were detected in one of five animals in group 2.
Conclusion
Autologous CD133+-cells derived from bone marrow had a better outcome with regard to calcification, inflammation, and transvalvular gradient compared to autologous cells derived from the carotid artery. Therefore, CD133+-cells are more advantageous for tissue engineering of heart valves.
Footnotes
Acknowledgments
This project is supported by the German Research Foundation, Bonn, Germany (LU663/7-2).
We gratefully thank Traudl Hansen, Signe Valentin, and Beke Sarrahs for their excellent technical assistance and Klaus Mück for preparing the application device.
Disclosure Statement
No competing financial interests exist.