
Abstract
Autologous adipose transplantation is rapidly gaining popularity for the restoration of soft tissue defects and lipoatrophy as well as for aesthetic improvements (e.g., facial reconstruction and rejuvenation). However, the current technique is crude that suffers from serious demerits, particularly the long-term unpredictability of volume maintenance due to resorption of the grafted adipose tissue and limited adipogenesis. We hypothesized that the adjuvant use of patient-derived adipose stromal vascular fraction (SVF) and platelet-rich fibrin (PRF) may enhance the overall outcome of autologous fat grafting in plastic and reconstructive surgery. Autologous SVF, with a mean cell number of (4.8±3.79)×107 cells/mL and a mean cell viability of 71.8%, and autologous PRF, with sustained release of multiple angiogenic growth factors, were created before surgical use. The following adipose tissue implants were injected subcutaneously into a rabbit ear's auricula according to the following study design: 2 mL adipose granules and 0.2 mL normal saline solution (AG+NS group), 2 mL adipose granules and 0.2 mL SVF (AG+SVF group), 2 mL adipose granules and 0.2 mL PRF (AG+PRF group), or 2 mL adipose granules combined with 0.1 mL SVF and 0.1 mL PRF (AG+SVF+PRF group). Histological examinations showed that the implanted adipose granules were well engrafted in the AG+SVF+PRF group, with a higher microvessel density 4 weeks postimplantation compared with the other three groups (p<0.01). Twenty-four weeks postimplantation, the resorption rates of implanted tissue in each group were 49.39%±9.47%, 27.25%±4.37%, 36.41%±8.47%, and 17.37%±6.22%, respectively, and were significantly different (p<0.01). The results demonstrated that the efficacy of adipose tissue implantation can be enhanced by using autologous PRF and SVF as therapeutic adjuvants, offering a clinically translatable strategy for soft tissue augmentation and reconstruction.
Introduction
Autologous adipose tissue transplantation is being established as a potential technique to correct soft tissue defects due to its minimal surgical invasion, easy harvest, and large yield of donor tissue for use. 4 However, the overall outcome of this method is often unpredictable. Indeed, free adipose tissue transfer rarely achieves long-term volume maintenance or sufficient tissue augmentation due to low tolerance of adipocytes to ischemia and slow revascularization rate of the fat transplants, leading to cell necrosis, apoptosis of the transplanted mature adipocytes, and graft volume shrinkage over time. 5 Of note, the transplanted fat can lose its volume to a rate as high as 70%, or even shrink to an incomputable extent, leading to the final failure of most, if not all, soft tissue reconstructive procedures.6,7
Recently, tissue engineering has emerged as a novel concept to address these limitations and to provide new therapeutic paradigms in which engineered adipose tissue can be custom-tailored for specific types of tissue repair.8–10 Typically, these strategies incorporate ex vivo cultured cells, manufactured scaffolds, and an artificial extracellular microenvironment that provides cues to induce new adipose tissue regeneration. However, caution must be exercised against the design of medical devices that lack translational potential or rely on the dogmatic combination of cells, scaffolds, and growth factors; the clinical translation of new therapeutics, including outside cells, is very complicated, if it is not impossible 11,12 Although obtaining adipose tissue-derived stem cells (ASCs) is easy, production of an adequate number of cells to meet the clinical need is both time consuming and expensive, in addition to safety concerns and myriad regulatory restrictions. 13
Stromal vascular fraction (SVF) cells can be obtained by centrifugation of collagenase-digested adipose tissue, which reveals a heterogeneous cell population, including endothelial cells, pericytes, smooth muscle cells, mast cells, leukocytes, and indeed, multipotent ASCs.14,15 Therefore, uncultured SVF offers an alternative to cell sources for adipose tissue regeneration that may tactfully circumvent many of the translational barriers in relation to ex vivo cell culture and delivery. Based on this concept, uncultured SVF cells (freshly isolated) were seeded on a porous collagen/gelatin sponge to regenerate new adipose tissue in vitro. 16 The use of angiogenic growth factors (e.g., fibroblast growth factor-2 [FGF-2]; vascular endothelial growth factor [VEGF]; and/or platelet-derived growth factor [PDGF-BB]) was found to increase cell infiltration and early angiogenesis.17,18 Therefore, it is logical to believe that the combined use of SVF and multiple angiogenic growth factors may synergistically increase overall adipose tissue growth.
Recent findings suggest that in either fat tissue engineering 19 or autologous fat transfer, 20 an appropriate controlled release of essential growth factors with the aids of scaffolding materials, is essential to achieve an optimized formation of adipose tissue. Although the use of manufactured biomaterials and exogenous growth factors is a common concept, it will be more advantageous if the development of scaffolding biomaterials and the delivery of recombinant human growth factors are also avoided. In this regard, growth factors and fibrin scaffolds obtained from patients' own blood are explored for therapeutic purposes, leading to a new research arena generally termed endogenous regenerative medicine. This new research direction may have the potential to accelerate the clinical translation of regenerative medicine.21–25
Clinical interest in exploitation of platelet-rich plasma (PRP), a platelet concentrate, for a wide variety of biomedical and engineering applications is based on its possibility as an easily attainable and safe source of multiple endogenous biologically active proteins that required in physiological wound healing and tissue regeneration. 25 Recently, autologous PRP has also been described as an adjuvant to fat grafting that may enhance the clinical outcome of plastic surgery. 26 Platelet-rich fibrin (PRF) belongs to a new generation of platelet concentrates that has been shown to have several additional advantages over traditional PRP, such as its lack of biochemical handling of blood and ease of production. 27 PRF contains high levels of growth factors, including PDGF-BB, VEGF, FGF-2, EGF, insulin-like growth factor-I, and transforming growth factor-β. 28 Although biological evidence points to the adjuvant use of platelet-rich preparations in adipose tissue engineering and transplantation,29–31 limited data are current available.
In the present study, we employed PRF and SVF as alternative therapeutic adjuvants for autologous adipose tissue transplantation. The use of adipose SVF as an alternative source of stromal/stem cells offers a new paradigm for cell transplantation. PRF that enriches with multiple growth factors is easy to apply in clinical practice and offers potential benefits, including angiogenesis and adipogenesis after autologous fat transplantation. The efficacy of adjuvant use of PRF and SVF in maintaining graft volume and enhancing graft survival was measured for up to 24 weeks in a rabbit ear model. Our data provide direct scientific evidence for developing a clinically translatable strategy for soft tissue reconstruction.
Materials and Methods
Animals
Thirty New Zealand rabbits aged 10 months, which were obtained from an USDA-licensed vendor (Experimental Animal Center, Fourth Military Medical University School of Stomatology), were used in the present study. All of the rabbits used were male, with an average weight 3.4–3.7 kg. The use of animals in this study and our experimental protocols were approved by the Institutional Animal Care and Use Committee at the Fourth Military Medical University, Xi'an, China.
Adipose granules
Under general anesthesia, a sterile field was created around the scapular region of each rabbit. Subcutaneous fat (adipose tissue) was excised in a standard surgical procedure. In total, 8–10 g of clean adipose tissue was harvested from each animal. This adipose tissue was then cut into small pieces (∼1 mm3) to make adipose granules for both transplantation and SVF isolation use.
SVF isolation
For SVF preparation, the obtained adipose granules were digested with 0.02% type I collagenase (Sigma) in phosphate-buffered saline (PBS) containing 1% penicillin. The obtained SVF was finally centrifuged and washed twice with PBS, as reported in the literature. 32 The cell number of SVF cells/mL was determined by a microscope, and the Trypan Blue exclusion technique was used to assess their viability. The mean cell number (cell number/mL SVF), percentage viability, total cell yield (total cell number/mL adipose granules), and percentage live cell yield (live cell number/mL adipose granules) of each sample were analyzed independently in triplicate. For transplant preparation, the mean live cell number in all SVF samples derived from adipose granules of different animals was standardized.
PRF preparation
PRF was prepared according to the reported method, with minor modifications. 33 Briefly, blood samples were drawn from the animals, and five milliliters of blood was (in 10 mL of dried monovettes without anticoagulant) centrifuged immediately by a laboratory centrifuge (TDZ5-WS; Xiangyi) for 10 min at 3000 rpm. PRF clot was in the middle layer of the resulting product that consisted of three layers. To obtain resistant fibrin membranes, the PRF clots were packed tightly into a sterile compress. Finally, the obtained PRF membranes were cut into few-millimeter fragments in sterile dishes for further use. Both PRF clots and membranes were prepared for a scanning electron microscope (SEM) observation (S-4800; Hitachi). The kinetics of PDGF-BB, VEGF, and FGF-2 release from prepared PRF was determined by an enzyme-linked immunosorbent assay (ELISA) method. Briefly, 500-μL PRF membrane fragments from each samples were immersed in 2-mL microcentrifuge tubes (n=6) containing 1 mL PBS. Then, all tubes were placed on a shaking table with continuous agitation at 37°C. After 4, 8, 12, 16, 20, and 24 days of incubation, the supernatant was collected for analysis, and the same amounts of fresh PBS were replenished into the tubes. The amount of the aforementioned three growth factors in the supernatants was determined by ELISA kits from R&D Systems (DB100). The bioactivity and stability of these factors in PRF were studied in terms of their capability to stimulate cell proliferation in cultured human dermal fibroblasts.
Design and injection of adipose tissue implants
Thirty rabbits were randomly divided into 15 pairs. Four ears of each pair were further randomly assigned into four groups that received differently designed biomaterial (adipose granules mixed with different adjuvants) implants. The following groups of designed adipose tissue implants were injected subcutaneously into a rabbit ear's auricula: 2 mL adipose granules mixed with 0.2 mL normal saline solution (AG+NS group), 2 mL adipose granules mixed with 0.2 mL SVF (AG+SVF group), 2 mL adipose granules mixed with 0.2 mL PRF (AG+PRF group), or 2 mL adipose granules mixed with 0.1 mL SVF and 0.1 mL PRF (AG+SVF+PRF group). The mixtures constituted an injectable homogeneous graft material and were observed with an SEM (Hitachi). After implantation, the animals had ad libitum access to water and a standard laboratory diet through the entire examination period.
Survival and absorption rates
The volume of the tissue implants was measured weekly during the 24-week period after implantation using the Peterson and Espersen equation: V=a×b×c×0.5, 34 where a, b, and c represented for the longitudinal diameter, the transverse diameter, and the thickness, respectively. The data of a, b, and c were determined by an animal B-type ultrasonic diagnostic apparatus (WED-9618V; Shenzhen Well.D Medical Electronics Co., Ltd.). The survival and absorption rates were then calculated via the following formulas: survival rate (%)=adipose tissue volume at each time point post-transplantation/implanted adipose tissue volume measured 1 day postimplantation; absorption rate (determined at weeks 4, 12, and 24) (%)=1−(adipose tissue volume at each time point post-transplantation/implanted adipose tissue volume measured 1 day postimplantation).
Histology
The maintenance of adipose tissue transplant at the implantation site was assessed by a histological examination 35 at weeks 1, 2, 3, and 4. At each time point, three pairs (six rabbits) were sacrificed, and the skin flap, including the implantation site, was fixed with 10% neutralized formalin solution and embedded in paraffin. Paraffin-embedded sections (4 μm in thickness) containing the implantation site as centrally as possible were deparaffinized and rehydrated for hematoxylin and eosin (HE) staining. To evaluate the survival of transplant, microphotographs were taken at a similar magnification, and six cross sections from three different ears were included. The same areas of interest were randomly selected (0.5×0.8 mm2, three portions per cross section) for the determination of the area of adipose tissue, where the area occupied by matured adipocytes at the implantation site for every portion was calculated.35,36
CD31 staining for microvessel density analysis
Microvessel density analysis was performed using the Weidner's method, 37 with minor modifications. The paraffin sections of the fatty tissue were stained for CD31 immunohistochemistry 4 weeks postimplantation. 38 Briefly, paraffin-embedded sections were dewaxed and rehydrated, and then incubated in 1% (v/v) hydrogen peroxide in methanol solution for 30 min to block endogenous peroxidase activity in the tissue. Nonspecific binding of immunoglobulins was blocked by incubation with 3% v/v normal goat serum. Then, the primary antibody of mouse anti-rabbit for CD31 (Abcam, Inc.) was added at a concentration of 10 μg/mL. After incubation overnight (4°C), the slides were rinsed with PBS for three times and then incubated with the biotinylated goat anti-mouse antibody (secondary antibody), according to the manufacturer's instructions, without dilution at 37°C for 50 min, followed by 50 min with a diluted avidin/biotin complex reagent from an avidin–biotin–peroxidase complex kit (Vector Laboratories). Finally, the sections were reacted with diaminobenzidine tetrahydrochloride (Sigma) at a concentration of 0.02% (w/v) in a Tris–HCl buffer (0.1 M, pH=7.2), containing 0.005% (v/v) hydrogen peroxidase. The slides were then weakly counterstained with hematoxylin, dehydrated through graded alcohols, and mounted with Permount (Fluka). The method for the microvessel density analysis from the CD31 staining was as follows: first, a region was selected where new regenerated blood vessels were dense, which was referred to as a hot spot, at 100× magnification. Then, brown cells were identified in the hot spot at 200× magnification. Each brown cell cluster or cell was calculated as a newly formed blood vessel, whereas the red blood cells (also brown) in the vessel cava were excluded. If a vessel cavum was more than the size of 8 blood cells, it did not look like a newly formed blood vessel and was excluded. Using 5 hot spots for examination at 200× magnification, the obtained data were statistically analyzed.
Statistical analysis
The survival and absorption rates of the four groups' transplanted fat tissue were analyzed by SPSS16.0 software (SAS Institute) using the analysis of variance method and the Fischer's protected least significant difference (PLSD) test. Differences in the microvessel density analysis between any two groups were compared and were statistically analyzed using the Fischer's PLSD method. Values with p≤0.05 in this study were considered statistically significant. All data were expressed as the mean±standard deviation, except for a partial decline in the percentage of in vivo vascularization data, which were expressed as the median and interquartile range (IQR) values.
Results
Adipose tissue implants
All of the designed adipose tissue implants used for each animal were autologous for each animal. The mean cell number of freshly isolated SVF from 30 New Zealand rabbits was (4.8±3.79)×107 cells/mL (range 2.2×107–6.1×107), and the mean cell viability was 71.8% (range 58%–80%). At the same time, by squeezing out the fluids in the fibrin clot, PRF was obtained in the form of a membrane before use (Fig. 1). 27 The PRF mean platelet count was 1,284,000/μL, with a range of 1,149,000/μL–1,386,000/μL. As determined by ELISA, 500 μL PRF contained 2396.9±421.2 pg/mL of PDGF-BB, 112.5±22.6 pg/mL of VEGF, and 65.2±13.7 pg/mL of FGF-2 (Fig. 2A). More than 80% of PDGF-BB, VEGF, and FGF-2 contained in PRF were gradually released within 12 days, and their sustained release kept more than 20 days (Fig. 2B–D). The released growth factors showed significant and durable biological effects on normal human dermal fibroblasts in terms of cell proliferation (data not shown).
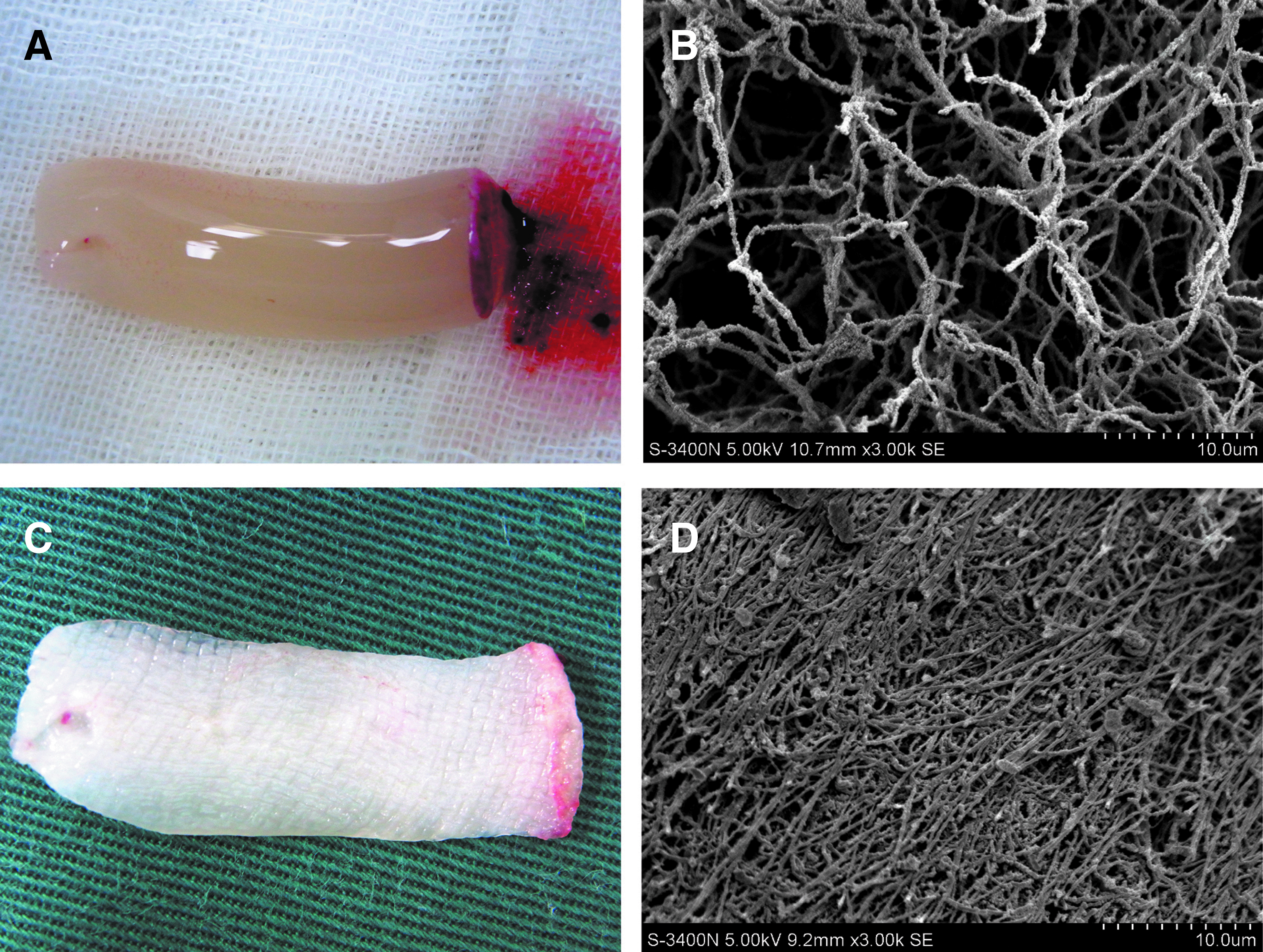
The preparation of platelet-rich fibrin (PRF).

The concentrations of angiogenic growth factors in PRF
According to the designed procedure, 2 mL adipose granules and 0.2 mL normal saline solution (AG+NS group) (Fig. 3A), 2 mL adipose granules and 0.2 mL SVF (AG+SVF group) (Fig. 3B), 2 mL adipose granules and 0.2 mL PRF (AG+PRF group) (Fig. 3C), and 2 mL adipose granules, 0.1 mL SVF and 0.1 mL PRF (AG+SVF+PRF group) (Fig. 3D) were individually used as the adipose tissue implants. Finally, all implants were injected with a 10-mL injection syringe pump and sterile injector. SEM observations showed that both adipose stromal cells and SVF can adhere to the fibrous structures of PRF in the implants (Fig. 4).
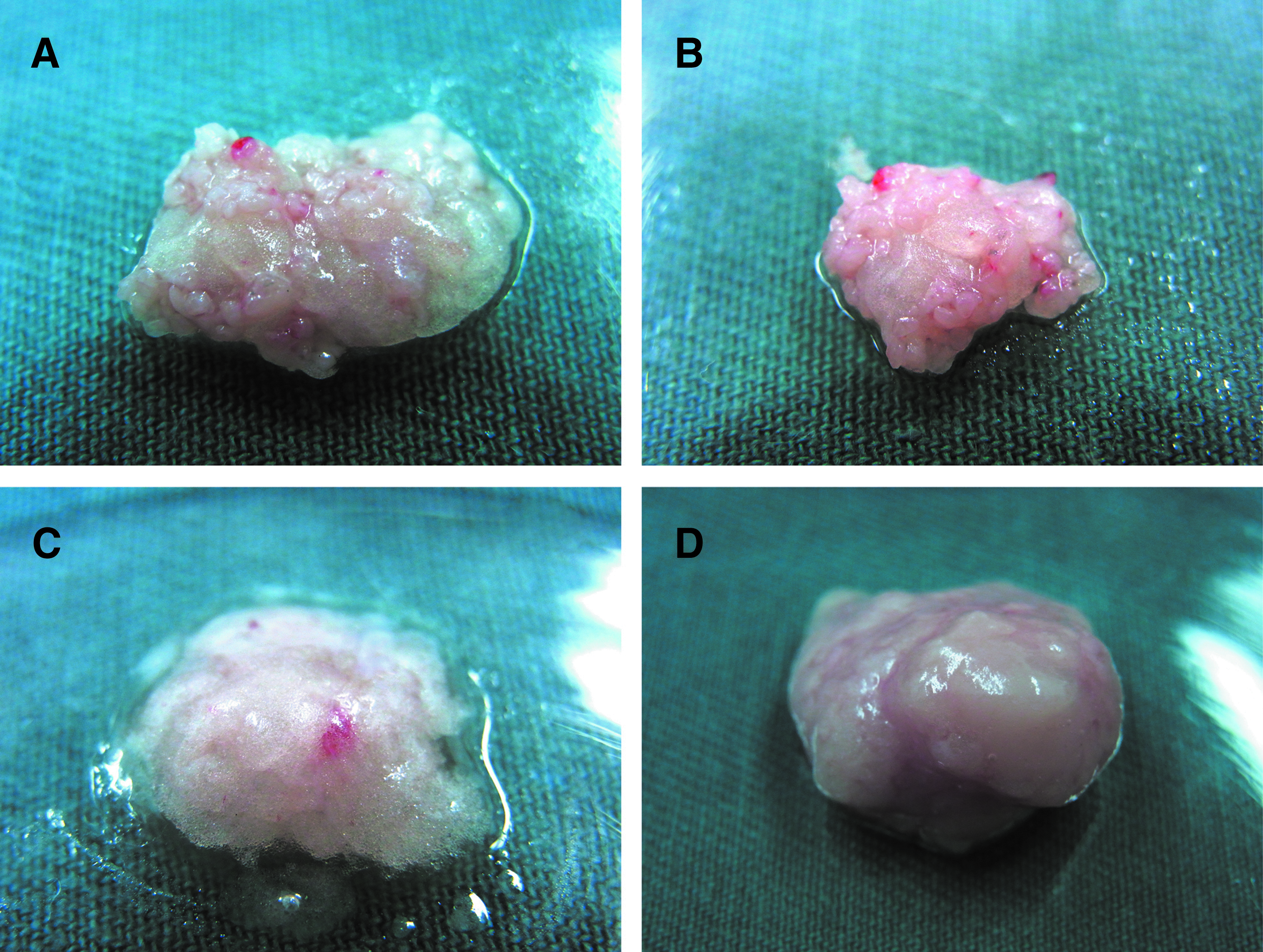
Designed adipose tissue implants for each group.
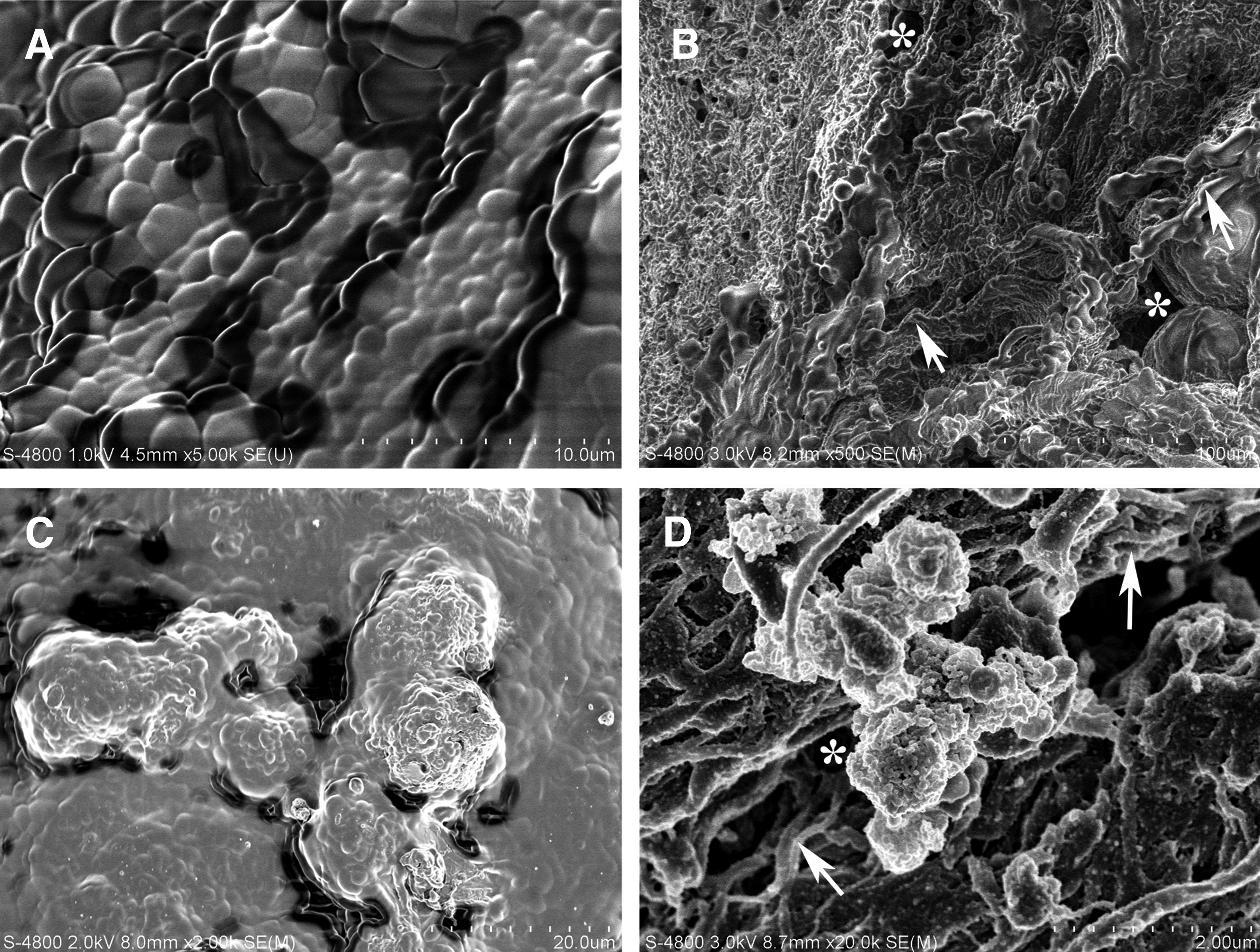
SEM photomicrographs of the designed implants.
Biomaterials implantation
The regions for adipose tissue implants were determined according to the procedure illustrated in Figure 5. The volume of each implant in the different groups was measured by a B ultrasound measurement 1 day postimplantation, and there were no statistical differences between the testing groups. During the overall investigating period, no adverse effects from the implants were found in any of the 30 animals.
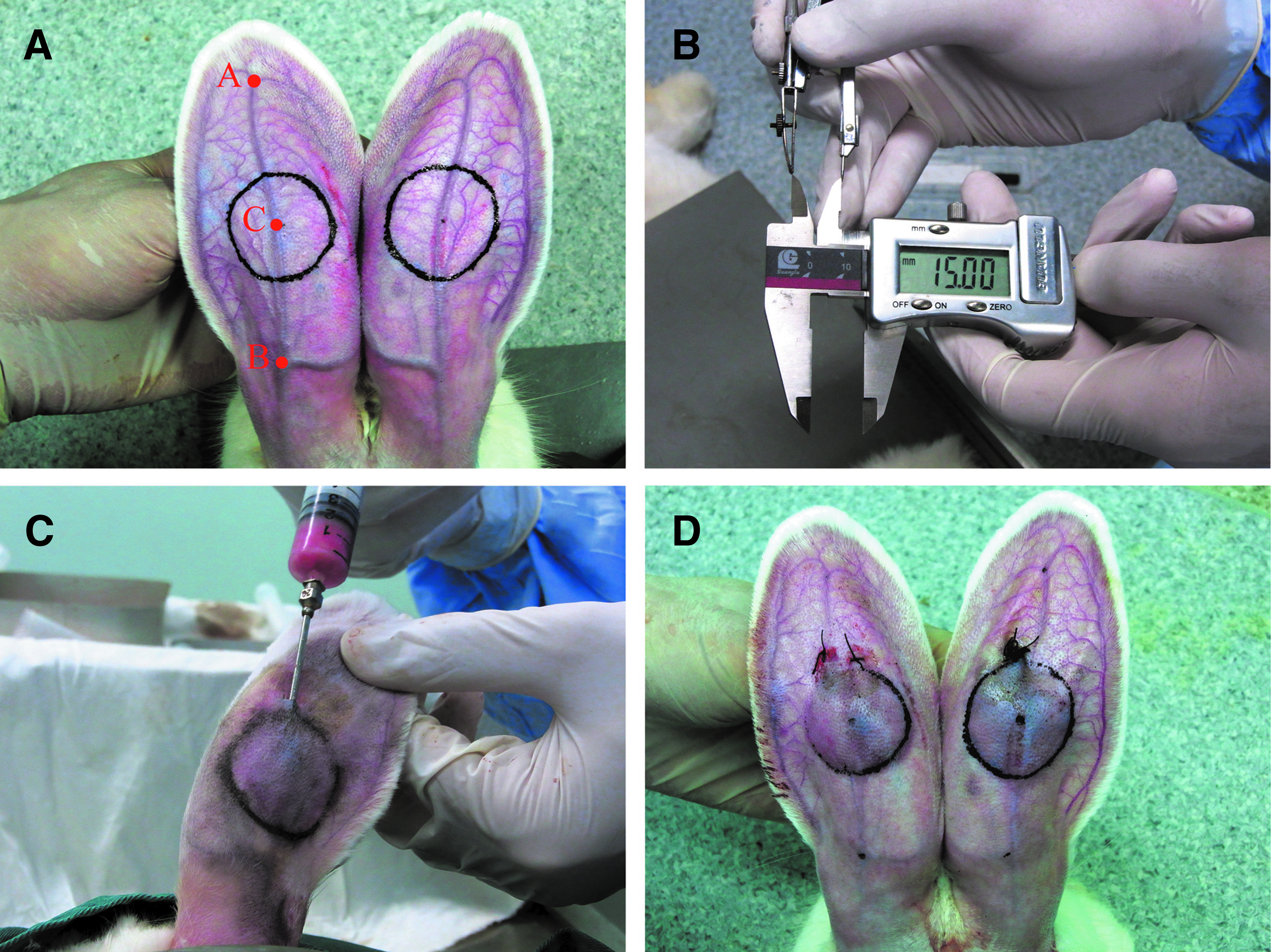
Determination of the region for adipose tissue implants
Histological analysis (1 week–4 weeks)
In the early stage (1 week–4 weeks), the AG+NS group showed the fastest tissue resorption with significant adipose tissue fibrosis. The fat cells were surrounded by inflammatory cell infiltration when observed on the HE-stained slides. Figure 6 shows the histological sections through the transplants at different time points postimplantation. In the tissue mass of the AG+PRF+SVF group at 3 or 4 weeks after transplantation, mature adipocytes accumulating lipids were observed that were histologically similar to normal adipose tissue, whereas those in other groups were less effective as measured by random counting of lipid from selected areas in different samples (data not shown). After 4 weeks, the implants obtained from the AG+PRF+SVF group exhibited good adipose structures with newly formed blood vessels. When quantifiably assessed from the histological examination, the volume maintenance (area of adipose tissue remaining) of implants in the AG+PRF+SVF group was higher than all of the control groups (p<0.05) 3 weeks postimplantation. There were also minimum fibrosis and inflammatory reactions in this group. There was no statistical difference between the AG+SVF group and the AG+PRF group (p>0.05) (Fig. 7). Interestingly, the AG+PRF+SVF group had a significant increase in the area of adipose tissue from weeks 1 to 2 and 3 to 4 after implantation; this increase did not appear in any other group. All three control groups showed a decreased area of remaining adipose tissue (Fig. 7).
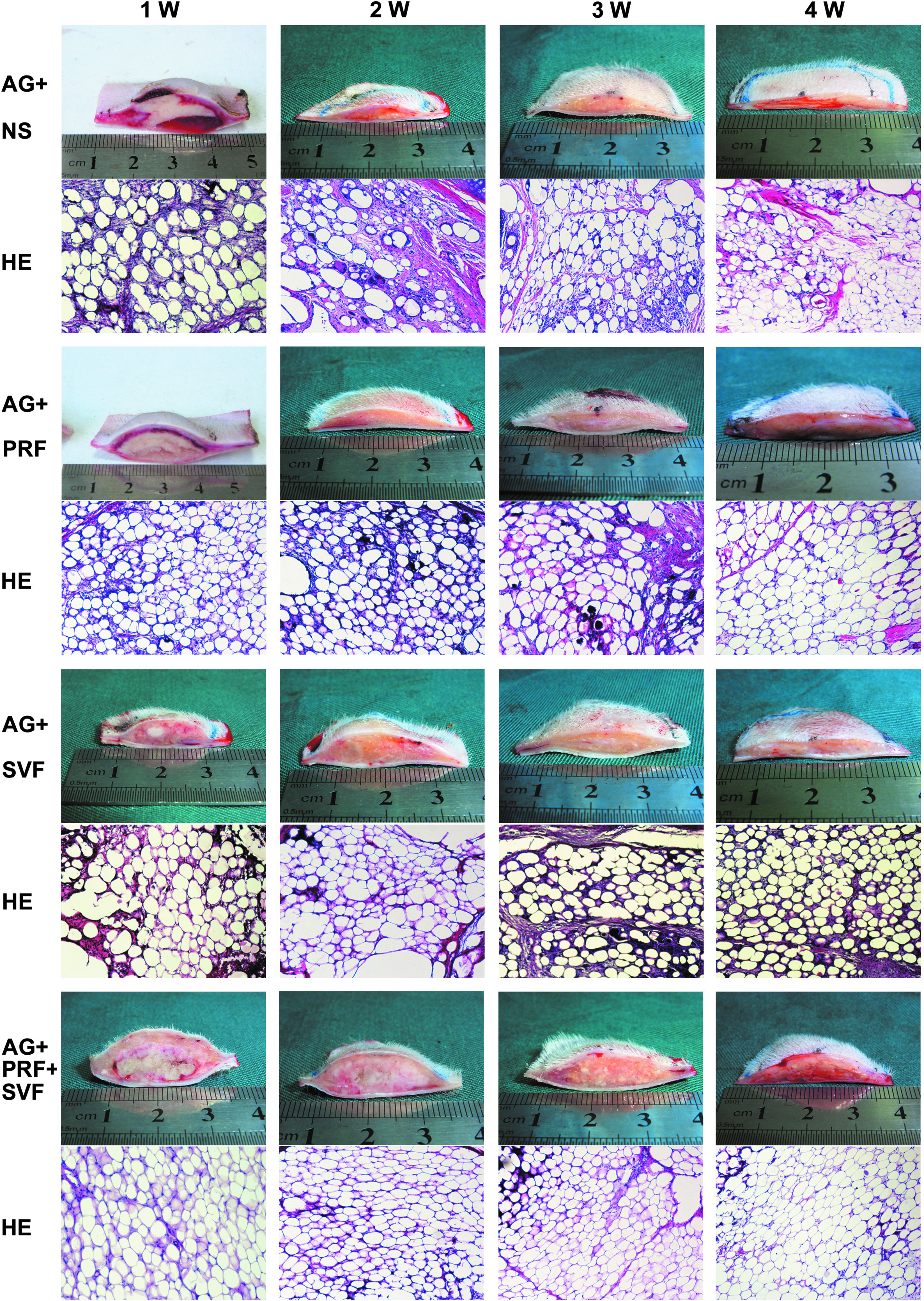
General samples (cross section from the “C” point as shown in Figure 5A while vertical with the central ear artery) and hematoxylin and eosin (HE) staining (×100) at weeks 1, 2, 3, and 4 postimplantation. In the adipose granules+normal saline solution (AG+NS) group, the adipose granules were enwrapped in fibrous tissue with many inflammatory cells 1 week postimplantation. The newly formed vessels began to appear at 3 weeks postimplantation with significant adipose tissue fibrosis. Then, inflammatory cells and tissue fibrosis began to decrease, but were still found 4 weeks postimplantation. In the AG+SVF+PRF group, fewer inflammatory cells and reduced adipose tissue fibrosis were found compared to the three controls 1 week postimplantation. The newly formed blood vessel began to emerge 1–2 weeks postimplantation. After 4 weeks, the implants obtained from the AG+PRF+SVF group showed good adipose structures with newly formed blood vessel networks. The adipose tissue reconstruction and blood vessel formation showed no obvious differences between the AG+PRF group and the AG+SVF group. They began to appear 2 weeks postimplantation, which was later than that of the AG+PRF+SVF group and earlier than that of the AG+NS group. Less adipose tissue fibrosis was observed in the AG+PRF and AG+SVF groups compared to the AG+NS group, in which it remained 4 weeks postimplantation. Color images available online at
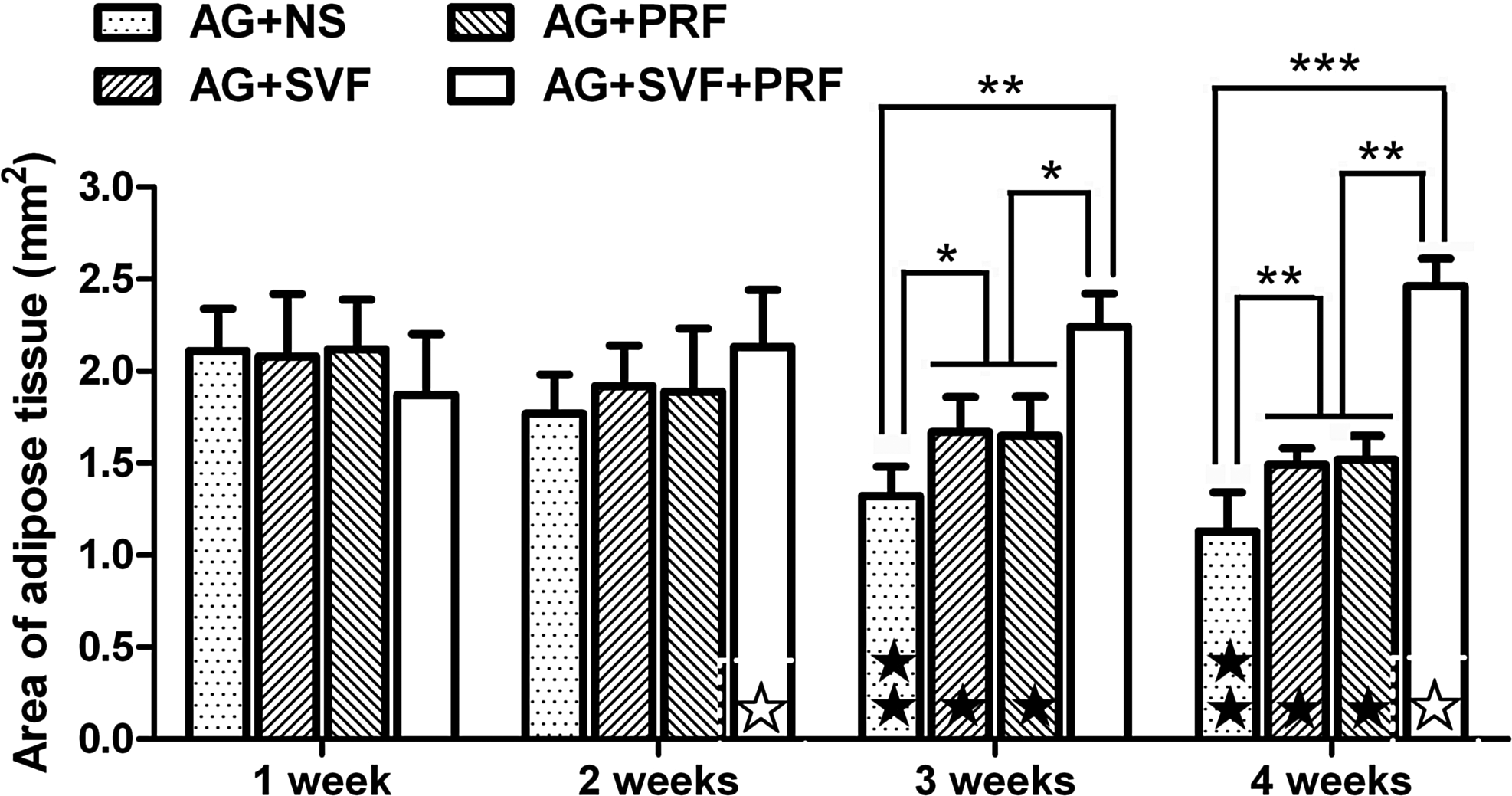
The area of adipose tissue remaining (determined by histological examination) within the implanted site at different time points. The implantation of a mixture of 0.2 mL adipose granules, 0.1 mL SVF, and 0.1 mL PRF (the AG+SVF+PRF group) represented the largest area of adipose tissue remaining when compared to the other three groups 3 or 4 weeks postimplantation. *p<0.05; **p<0.01; ***p<0.001; significant differences by Fischer's protected least significant difference (PLSD) test compared to the matched groups at the same time point. ★p<0.05; ★★p<0.01; significant value decreases along with the observation time (time-dependent effects) in the same group. ☆p<0.05, significant value increases in addition to the observation time (time-dependent effects) in the same group. The values are expressed as the mean±standard deviation for n=6.
24-week follow-up
Twenty-four weeks post-transplantation, a very obvious size difference between the groups appeared using macrography (Fig. 8) and B ultrasound measurements (Fig. 9). The survival rates of each group over the 24 weeks are shown in Figure 10; there were significant differences among the testing groups beginning 3 weeks postimplantation (p<0.05). At 24 weeks postimplantation, the implant absorption rate of the autologous fat granule transplantation combined with the PRF and SVF group (AG+PRF+SVF group) was 17.37%±6.22%, whereas the AG+NS group was 49.39%±9.47%; these results were significantly different (p<0.01). The absorption rates of adipose tissue implants in the AG+SVF group and the AG+PRF group were 27.25%±4.37% and 34.61%±8.47%, respectively. These values were much lower than those of the AG+NS group (p<0.05), whereas higher than those of the AG+PRF+SVF group (p<0.05). As for plastic surgery reconstruction, the absorption rate is a popular index for outcome evaluation. The data showing the absorption rates determined at 4, 12, and 24 weeks, according to B ultrasound measurements and their analysis, are shown in Figure 11.
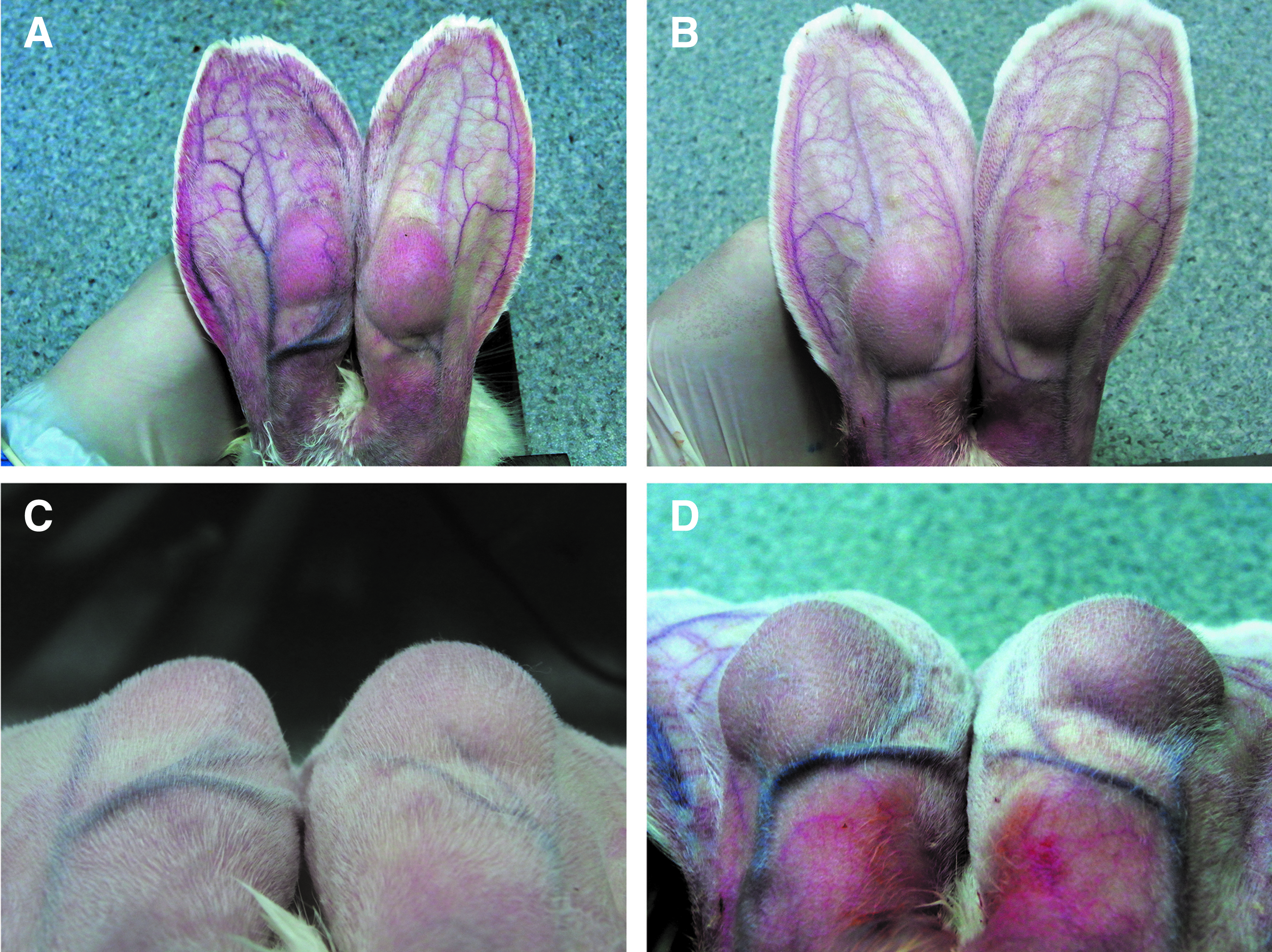
Twenty-four weeks postimplantation, the implantation size differences between the groups were very obvious by general observation (gross view). The AG+SVF+PRF group maintained a larger apophysis space compared to the three controls (from left to right: AG+NS group, AG+SVF group, AG+SVF+PRF group, and AG+PRF group, respectively).
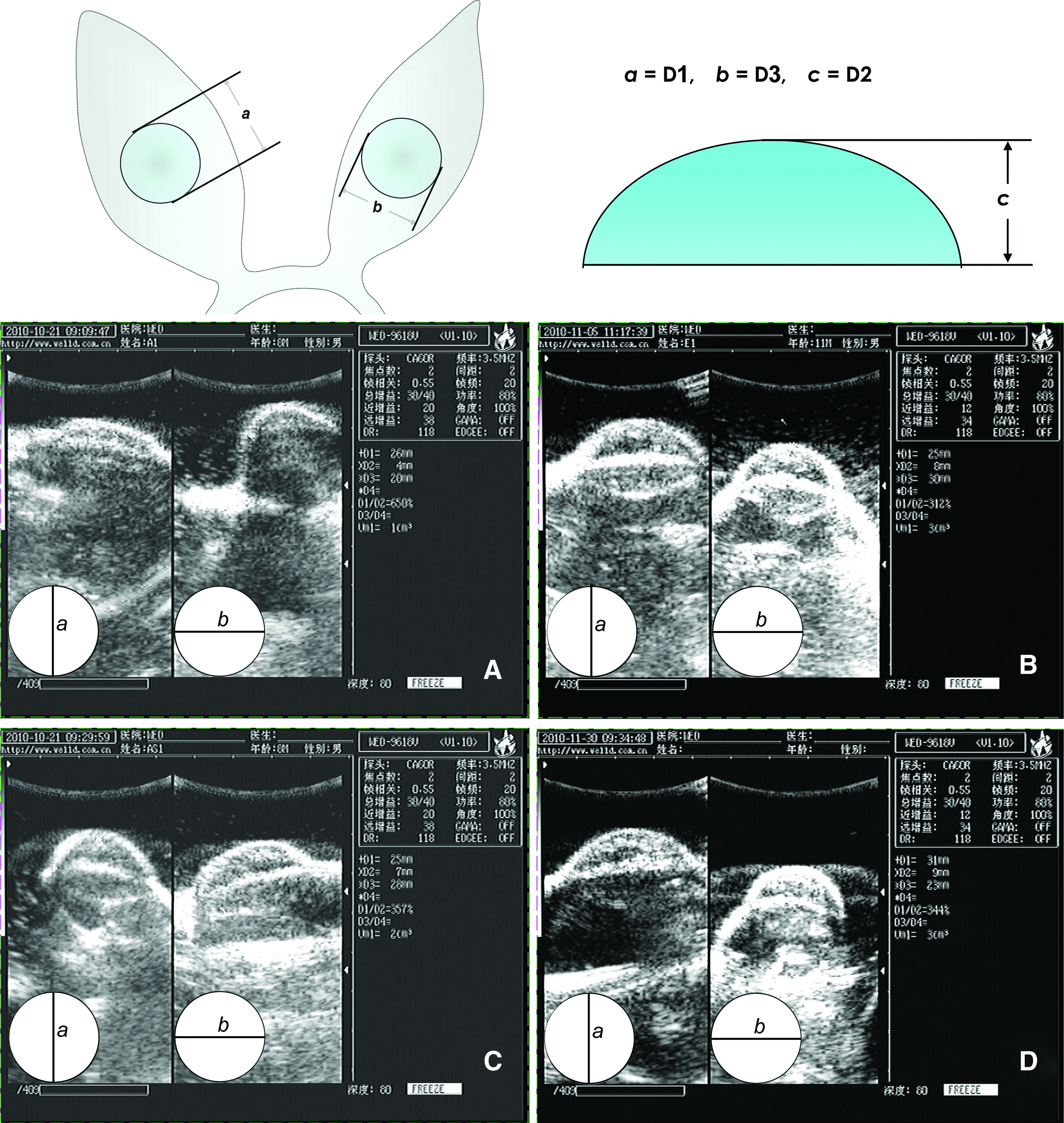
Schematic illustration of the B ultrasound measurement for the remaining implant size determination (V=a×b×c×0.5). The sonograms show the data (D1=a; D2=c; D3=b) obtained from the representative implants in different groups 24 weeks postimplantation (the direction of the probe showing in the lower left corner of each sonogram).
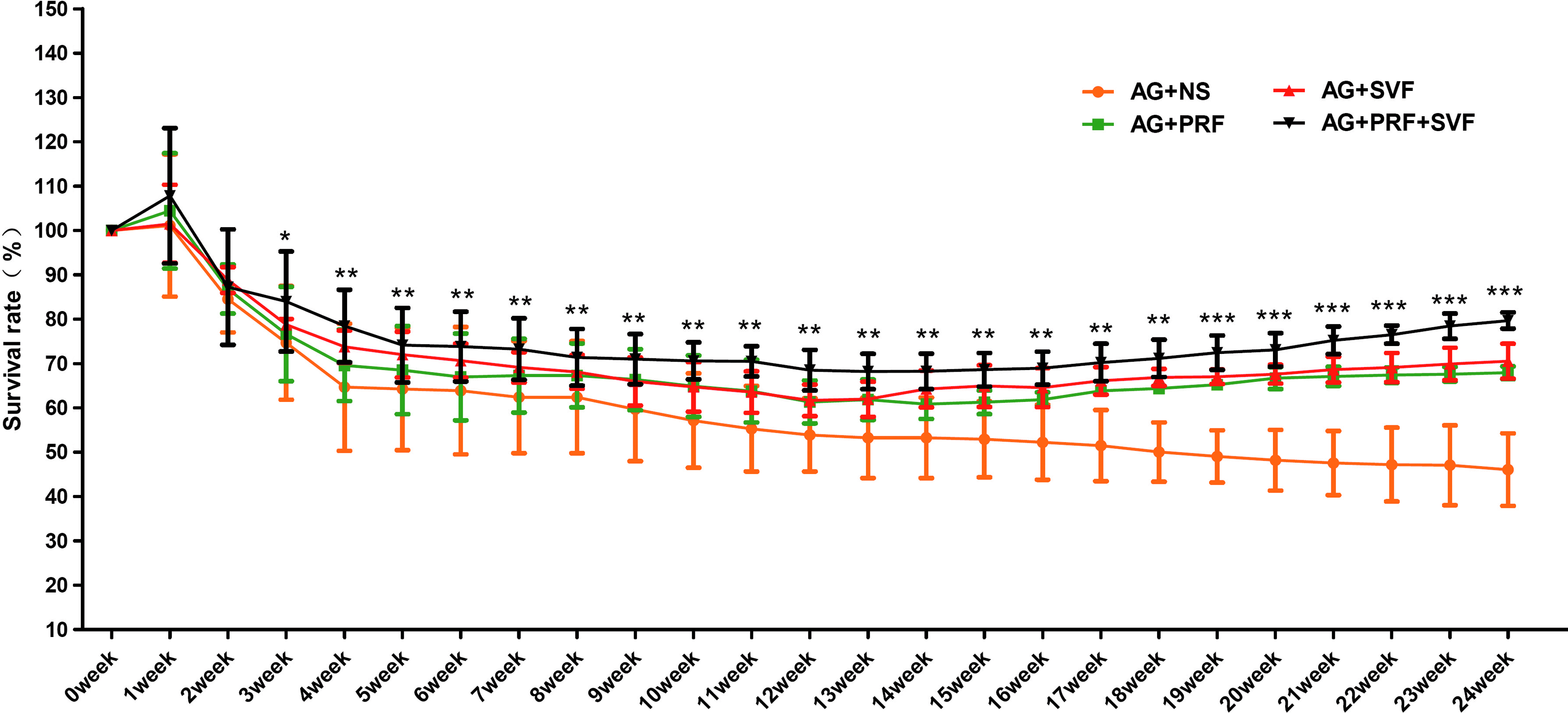
The survival rate analysis during a 24-week period using B ultrasound measurements (*p<0.05; **p<0.01; ***p<0.001). Color images available online at

The absorption rates determined at weeks 4, 12, and 24 postimplantation and their analysis. *p<0.05; **p<0.01; ***p<0.001; significant differences were measured by the Fischer's PLSD test and compared to the matched groups at the same time point. p<0.05; significant value increases along with the observation time (time-dependent effects on absorption rates) in the same group. The values are expressed as the mean±standard deviation for n=6.
Microvessel density analysis
Microvessel density analysis was performed with CD31 staining 4 weeks postimplantation (Fig. 12). The autologous fat granules combined with the PRF and SVF group (AG+PRF+SVF group) had the highest microvessel density of 83.80%±11.69% 4 weeks postimplantation relative to the other three groups (n=6, p<0.01). The AG+NS group had the lowest microvessel density rate of 50.60%±6.69%. The AG+SVF group and AG+PRF group (n=6, p<0.01) rates were 64.20%±7.50% and 64.40%±9.61%, respectively.
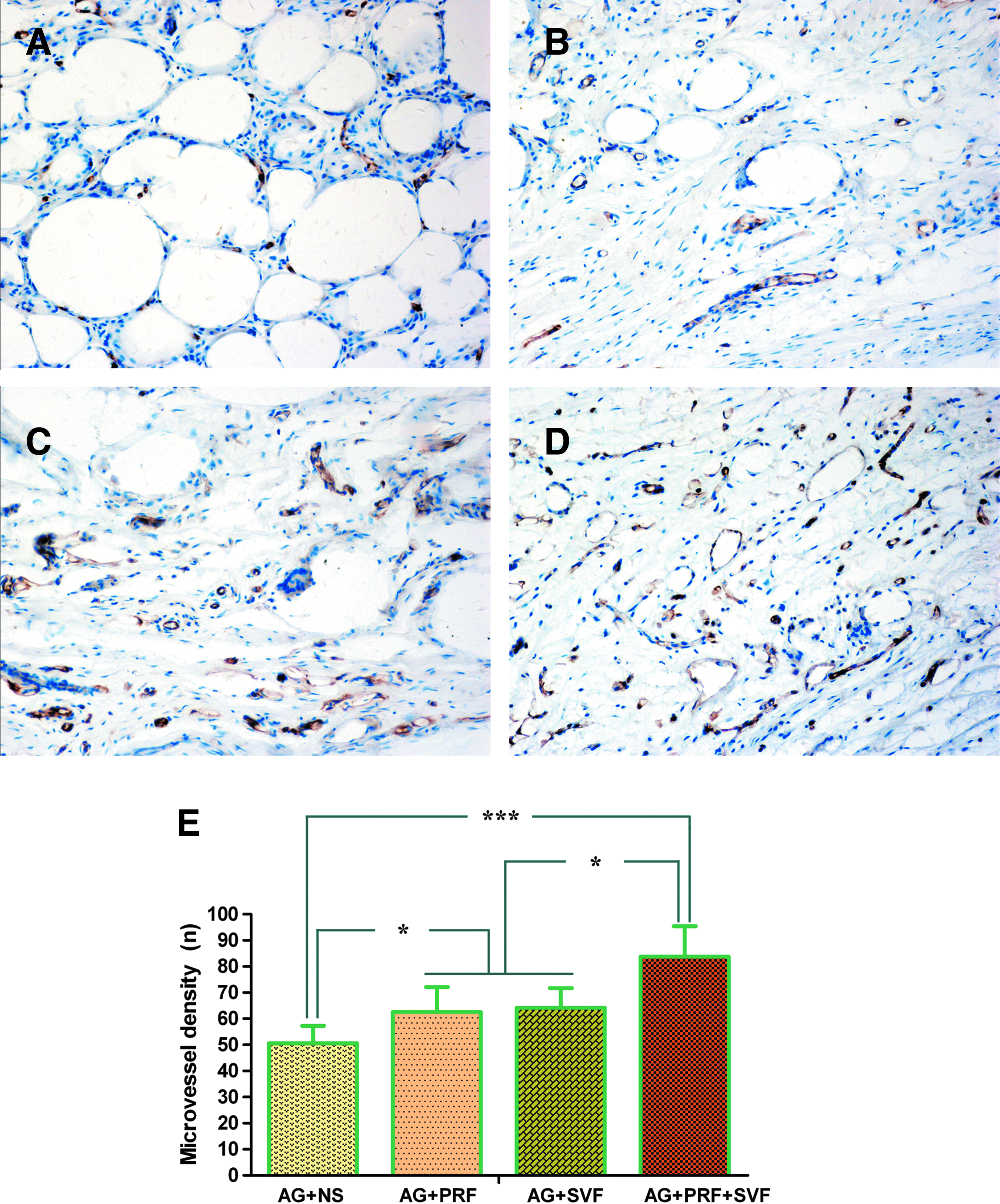
Immunohistochemical staining for CD31, a sensitive marker for endothelial cells, showing an extensive prevascular (brown area) network formed in the adipose tissue of the AG+PRF+SVF group 4 weeks postimplantation. Overview of a cross section in each group, showing frequent CD31+vascular structures (spheroid located in white oval) that appeared more frequently in the AG+PRF+SVF group, which was further confirmed by the microvessel density analysis.
Discussion
Due to the large numbers of patients involved, the use of adipose tissue grafts/substitutes is a rapidly growing field that may address current clinical needs relating to various soft tissue pathologies and defects. Of note, various levels of clinical success in terms of using autologous adipose tissue grafts have been reported.4–7 However, the transferred adipose grafts will not be useful unless they may maintain their shape and dimensions over time, and finally they are vascularized and integrated with the host tissue.29,38–40 In the present study, we hypothesized that the adjuvant use of a combination of PRF and SVF may augment/enhance autologous adipose tissue implantation. Our data showed that when mixed with PRF and SVF, the autologous adipose tissue transplants formed new adipose tissue in vivo within 4 weeks, as demonstrated by the enlargement of mature adipocytes within the transplants. Most importantly, the volume of the adipose tissue transplants was maintained after 24 weeks with good adipose structures and newly formed blood vessels (data not shown).
It is well recognized that poor vascularization and volume loss are two long-standing obstacles for fat tissue grafting.29,38–40 In the present study, we aimed to address these challenges in a rabbit ear model. Although adipose tissue engineering offers significant potential for soft tissue restoration, the bioengineered fat grafts are not clinically meaningful in plastic and reconstructive surgeries until their safety and efficacy are demonstrated in preclinical and clinical trials.3,8,38–41 We must be aware that new technologies (e.g., tissue engineering) not only must be scientifically sound but must also be practical and economical to be well suited for clinical applications.22–25,42 Clearly, the production and use of cell/tissue constructs are expensive and time consuming, rendering cell-based therapy a widespread clinical application impossible.43–47 In this study, uncultured SVF was used as an alternative to manipulated cells that composed the PRF, an autologous plasma product enriched in platelets that was used to augment autologous adipose tissue transplantation.29,30 The overall outcome of soft tissue augmentation relies on the enlargement of mature adipocytes after fat transplantation. The formation of new adipocytes through the differentiation of locally resident progenitor cell populations or exogenously transplanted preadipocytes included in a well-prepared SVF is proposed to be induced by PRF rich in growth factors. If this concept can address the volume reduction and poor vascularization of transplanted adipose tissues currently faced by plastic surgical operations, a simple, practical, and economical patient-derived product could enter a widespread clinical use shortly.
There is evidence that PRF may provide a sustained release of multiple growth factors important for wound healing while protecting them against proteolytic degradation48,49 According to the limited data obtained from our current study, PRF released multiple autologous growth factors gradually for more than 20 days, suggesting a potentially durable effect on tissue regeneration. Among the growth factors contained in PRF, the sustained release of PDGF-BB, VEGF, and FGF-2 was quantified in the present study, since these angiogenic growth factors are known to be potent therapeutic agents to stimulate angiogenesis.17–20 Our data obtained here suggest that the use of PRF is one of the most promising methods to enhance adipose tissue formation. The selection of appropriate biomaterials for cell and growth factor delivery is a key to adipose regeneration; unfortunately, the optimized scaffolds remain to be identified thus far.40,49–51 In this regard, autogenetic PRF scaffolds, in addition to their ability to release a pool of endogenous growth factors, served as a space-filling matrix for adipose implantation and localization, because they have the best characteristics to meet the clinical need of cell vehicles/scaffolds, such as good manageability, low cost, autologous nature, the absence of allergic reactions or other side effects of the patient.12,13,22,23
Delivering outside growth factors must also be considered in scaffold development in regenerative medicine.52,53 Ideally, multiple therapeutic agents need to be delivered in a specific spatiotemporal pattern and at an optimized ratio. 22 Based on this concept, the use of patient-derived products enriched with a pool of endogenous growth factors for repair and regenerative purposes has rendered an alternative to the need for delivery of recombinant growth factors. 54 Specifically, the synergistic effect of VEGF, PDGF, and FGF-2 is required for new blood vessel formation, 17 where VEGF is the initiating factor for early angiogenesis, while PDGF-BB can recruit smooth muscle cells to promote vascular maturity and stability. 53 This may explain why the autologous fat granules combined with PRF has increased the microvessel density in the AG+NS group from the rate of 50.60%±6.69% to that of 64.40%±9.61% in the AG+PRF group. The combination of autologous fat granules and SVF (AG+SVF group) also obtained a significant rate increase of the microvessel density when compared with the AG+NS group; the adipose stem cells involved in SVF may facilitate the formation of new blood vessels. Clearly, the AG+PRF+SVF group had the highest microvessel density of 83.80%±11.69% 4 weeks postimplantation relative to the other three groups, suggesting PRF and SVF may have a synergistic effect on angiogenesis in transplanted adipose tissues.
It is well recognized that the clinical use of cell-delivery therapeutics for tissue regeneration faces with numerous translational hurdles.55,56 In light of this, SVF contains an heterogeneous pool of cells that may avoid the need for cell isolation and expansion. 57 Of note, recent data have yielded positive outcomes using freshly isolated SVF as an uncultured/expanded stem cell source in advanced cartilage therapy 58 and adipose formation. 16 Furthermore, cryopreservation of SVF in a serum-free freezing medium has been tested, and the results suggest that cell viability and adipogenic differentiability of SVF can be maintained. This finding increases the usefulness of SVF cells in regenerative medicine. 59 It seems that the use of autologous SVF for cell therapy not only is safe and easy but may also facilitate its translation into the patient's healthcare. However, more studies are needed to clarify whether the technique described in the present study still works in a larger scale of tissue-defect models and if the autologous transplants can maintain their dimensions and shape over time at defect sites in humans.
The present study addresses a crucial issue in transplantation of autologous adipose tissue, namely its limited engraftment and subsequent loss of volume, although methods in relation to PRF and SVF preparation need to be further improved and investigated before their entering into clinic. We are aware that the additional use of PRF to adipose granules mixed with SVF results in a reduction rate in the implant absorption is only about 10% (from 27.25% to 17.37%). In perspective, a more effective release kinetics of growth factors from PRF may further enhance the final clinical outcomes, which may be potentially reached by using other adjuvants, such as heparin-conjugated biomaterials, into PRF. These biomaterials may bind to various growth factors such as VEGF, PDGF, and FGF-2, and hence sustainedly release their cargos for a durable effect on tissue regeneration. Future challenges in translational research on this technique include the elucidation of the molecular complexity of these implants, the identification of essential molecules/factors in PRF that determine the overall fate of the implanted tissue, the criteria to establish the dosing of the PRF/SVF combination, and the development of tailored products for each pathological situation. 23 This will improve the overall outcome in individuals suffering from severe soft tissue deficits.
Conclusion
The results obtained from the present study demonstrated that the adjuvant use of uncultured freshly isolated SVF cells and autologous PRF prepared at the bedside can augment adipose tissue transplantation in a rabbit ear model. Although the efficacy needs to be further demonstrated by preclinical and clinical trials, this concept offers an endogenous regenerative approach for soft tissue reconstruction. In prospect, in future reconstructive surgery requiring engineering of three-dimensional adipose tissue, the application of SVF and PRF may be also a potential alternative to the use of stem cells and growth factors. However, the elucidation of the molecular complexity of these implants and the events following their transplantation are in need of further investigation.
Footnotes
Acknowledgments
Funding from the National Natural Science Foundation of China (Nos. 31170942, 81070820, and 81071253) was gratefully appreciated.
Disclosure Statement
No competing financial interests exist.