
Abstract
Mouse models are invaluable tools for mechanistic and efficacy studies of the healing process of large bone defects resulting in atrophic nonunions, a severe medical problem and a financial health-care-related burden. Models of atrophic nonunions are usually achieved by providing a highly stable biomechanical environment. For this purpose, external fixators have been investigated, but plate osteosynthesis, despite its high clinical relevance, has not yet been considered in mice. We hereby proposed and investigated the use of an internal osteosynthesis for stabilizing large bone defects. To this aim, a 3.5-mm-long segmental bone defect was induced in the mid-shaft of the femur using a Gigli saw and a jig. Bone fixation was performed using a titanium microlocking plate with four locking screws. The bone defect was either left empty or filled with a syngenic bone graft or filled with a coralline scaffold. Healing was monitored using radiographs. The healing process was further assessed using microcomputed tomography and histology 10 weeks after surgery. With the exception of one mouse that died during the surgical procedure, no complications were observed. A stable and reproducible bone fixation as well as a reproducible fixation of the implanted materials with full weight bearing was obtained in all animals tested. Nonunion was consistently observed in the group in which the defects were left empty. Bone union was obtained with the syngenic bone grafts, providing evidence that, although such defects were of critical size, bone healing was possible when the gold-standard material was used to fill the defect. Although new bone formation was greater in the coralline scaffold group than in the left-empty animal group, it remained limited and localized close to the bony edges, a consequence of the critical size of such bone defect. Our study established a reproducible, clinically relevant, femoral, atrophic nonunion, critical-sized defect, low morbidity mouse model. The present study was successful in designing and testing in a small animal model, a novel surgical method for the assessment of bone repair; this model has the potential to facilitate investigations of the molecular and cellular events involved in bone regeneration in load-bearing, segmental-bone defects.
Introduction
In compliance with the reduction, replacement, refinement principles of laboratory animal use, in vitro testing of treatment modalities is advocated for the assessment of cytocompatibility and genotoxicity. The use of such in vitro approaches can also elucidate some mechanistic aspects. Recreating the spatial and temporal complexity of the microenvironment of the bone healing process (including physiological loading, vascular network, and immune response), however, can only be achieved with appropriately chosen and established animal models.6–8
While no species has been proven the ideal animal model for simulating the clinical milieu of human bone defects, large animal (such as dogs, pigs, and sheep) models have been used for preclinical studies.9–14 These models allow bone defects of clinically relevant volume and load-bearing conditions that simulate the clinical situation in humans. In contrast, small animal models, more specifically mice, are preferred for optimizing treatment modalities (such as drug dose–effect relationships), because variations in experimental parameters such as genotype (breed or strain), gender, age, weight, and husbandry conditions can be minimized. Limited inter-individual variability allows assessment of a large number of treatment modalities using a small number of animals in a cost-effective manner. Last but not least, mice are the gold standard for investigations aiming at understanding mechanistic aspects because of availability of (1) a comprehensive portfolio of molecular probes, (2) genetic knock-out/knock-in models, and (3) advanced, functional, imaging techniques that are either not available or are cumbersome in the case of large animals.7,15–19
Nonunions are not only a severe medical problem, but also a major financial health-care-related burden; hence, murine models mimicking this clinical condition are critically needed6,8 and have been developed using various osteosynthesis materials for bone defect stabilization.6–8,17,18,20–25 Models involving a nonlocked intramedullary pin and those that did not utilize osteosynthesis materials provide interfragmentary motion and have been used in studies of fracture healing, endochondral ossification, and hypertrophic pseudarthrosis.16,20,23,24,26–30 In contrast, models mimicking the atrophic nonunion clinical condition in a large diaphyseal bone defect require creation of bone defects in a highly stable biomechanical environment.25,31,32 Ex vivo analysis established that stabilization of mouse femurs using either a locking plate or an external fixator resulted in a rotational stiffness almost similar to the intact femur 21 and prompted their use for stable fixation in mice in vivo. Models based on external fixators were developed for stabilizing atrophic nonunion in mice and have provided tremendously useful data.17,33–36 In contrast, models based on plate osteosynthesis (which are routinely used in humans and large animals10,14,37–39) are poorly investigated despite their high clinical relevance.
We hereby established a load-bearing, critical-sized, segmental defect model that results in atrophic nonunion in mouse femurs and ensures: (1) appropriate and reproducible stabilization of the critical-sized, segmental, bone defect using locking plate osteosynthesis, as well as (2) accurate positioning of bone defects and reproducibility of the defect volumes.
Materials and Methods
Animals
Eighteen 10-week-old male athymic mice (NUDE NMRI-nu [nu/nu]; Janvier, St. Berthevin, France) were used in the present study. These mice were cared for in accordance with guidelines published by the European Committee for Care and Use of Laboratory Animals (Directive 2010/63/EU and the European Convention ETS 123). The Ethics Committee of the Faculty of Medicine Lariboisière Saint-Louis approved the experimental protocol (CEEA LV/2010-01-04).
Scaffolds
Scaffolds consisted of 3×3×3 mm Acropora sp. coral exoskeleton cubes (Biocoral®, Inoteb, France). This material consists of 99% calcium carbonate in the form of aragonite and 1% organic material (amino acids) and has communicating pores (mean pore diameter of 500 μm [range 200 to 800 μm] and porosity of 12%±4%).40,41 Each coral cube was carved by hand to the shape of cylinder (3.5 mm height; 2 mm diameter). The scaffolds were sterilized by autoclaving (a process that did not affect the Acropora coral composition 42 ), washed with phosphate buffered saline, and immersed in a complete culture medium for 24 h before implantation.
Surgical procedure and in vivo analysis
Experimental design
Mice were randomly assigned to three groups: (1) the defects were left empty (n=6 mice); (2) the defects were filled with syngenic bone graft (i.e., the defects were filled with massive bone grafts using the bone harvested from the ostectomy in mice of the defect-left-empty group; n=6 mice); (3) and the defects were filled with one Acropora cylinder per site (n=6 mice).
Anesthesia
Before initiation of each anesthesia procedure, buprenorphine (0.1 mg/kg animal weight; Buprecare® 0.3 mg/mL; Axience, Pantin, France) was administered subcutaneously as sedative and preventive analgesia. Before the surgical procedure, a single dose of enrofloxacine (0.05 mg/kg animal weight; Baytril® 5%; Bayer HealthCare, Puteaux, France) was also administered subcutaneously as microbial prophylaxis. Anesthesia was induced by intraperitoneal administration of xylazine (8 mg/kg animal weight; Rompun® 2%; Bayer HealthCare, Puteaux, France) and ketamine (100 mg/kg animal weight; Ketamine 500®; Virbac, Carros, France). Oxygen was delivered via flow-by throughout the surgical procedure. For postsurgery radiographic imaging procedures, anesthesia was induced, and maintained using ∼4% and 2% isoflurane (Forène®; Abbott, Arcueil, France) in oxygen, respectively.
Surgery
Animals were placed in ventral recumbency with the left hind limb in extension. The limb was clipped and prepared in the standard manner for aseptic surgery using 10% povidone iodine. An anterolateral approach was used to expose the anterior surface of the femur. Briefly, after a lateral longitudinal cutaneous incision along the femur extending from the hip joint to the stifle joint, the fascia lata was incised; the vastus lateralis muscle and the biceps femoris muscle were split to expose the full length of the femur preserving the sciatic nerve caudally and the articular capsule distally. An anterior titanium microlocking plate (10 mm long and 1.5 mm wide; MouseFix Plate XL; RISystem AG, Davos, Switzerland) was applied on the anterior femoral side (Fig. 1). Next, two holes were drilled using a 0.3-mm drill bit (Drill Bit 0.30 mm; RISystem AG, Davos, Switzerland) through the most proximal and most distal holes of the plate and two self-tapping locking screws (2 mm long, 0.47 mm outer diameter and 0.34 mm core diameter; MouseFix Screw 2 mm; RISystem AG, Davos, Switzerland) were inserted and locked to secure the plate (Figs. 1 and 2). The screws are connected to a stem, allowing precise insertion without the use of a conventional screwdriver. The stem twists off at the end of the screw-tightening step when the screw is locked. After drilling, two other screws were inserted, one in the hole near the proximal screw and the other near the distal screw, but not locked. A jig, especially designed for this purpose (Drill and Saw Guide; RISystem AG, Davos, Switzerland), was inserted on the stem of the two last screws and applied above the plate (Figs. 1 and 2). Gigli saws (0.22 mm; RISystem AG, Davos, Switzerland) were then inserted, one each in the two slots of the jig, and a 3.5-mm long mid-diaphyseal femoral ostectomy was subsequently performed; the resected bone was withdrawn and kept sterile using moist gauze compress. The jig was then removed and the two last screws locked (Fig. 2). The surgical field was copiously lavaged with sterile isotonic saline. The defect was either left empty or filled with the filling materials tested. In all animals, the fascia and subcutaneous planes were closed with a simple continuous suture pattern using 5.0 glycomer 631; skin closure was accomplished with a simple interrupted suture pattern using 4.0 glycomer 631. Analgesia was provided to all mice through a subcutaneous injection of buprenorphine (0.1 mg/kg animal weight) every 12 h postsurgery for three consecutive days.
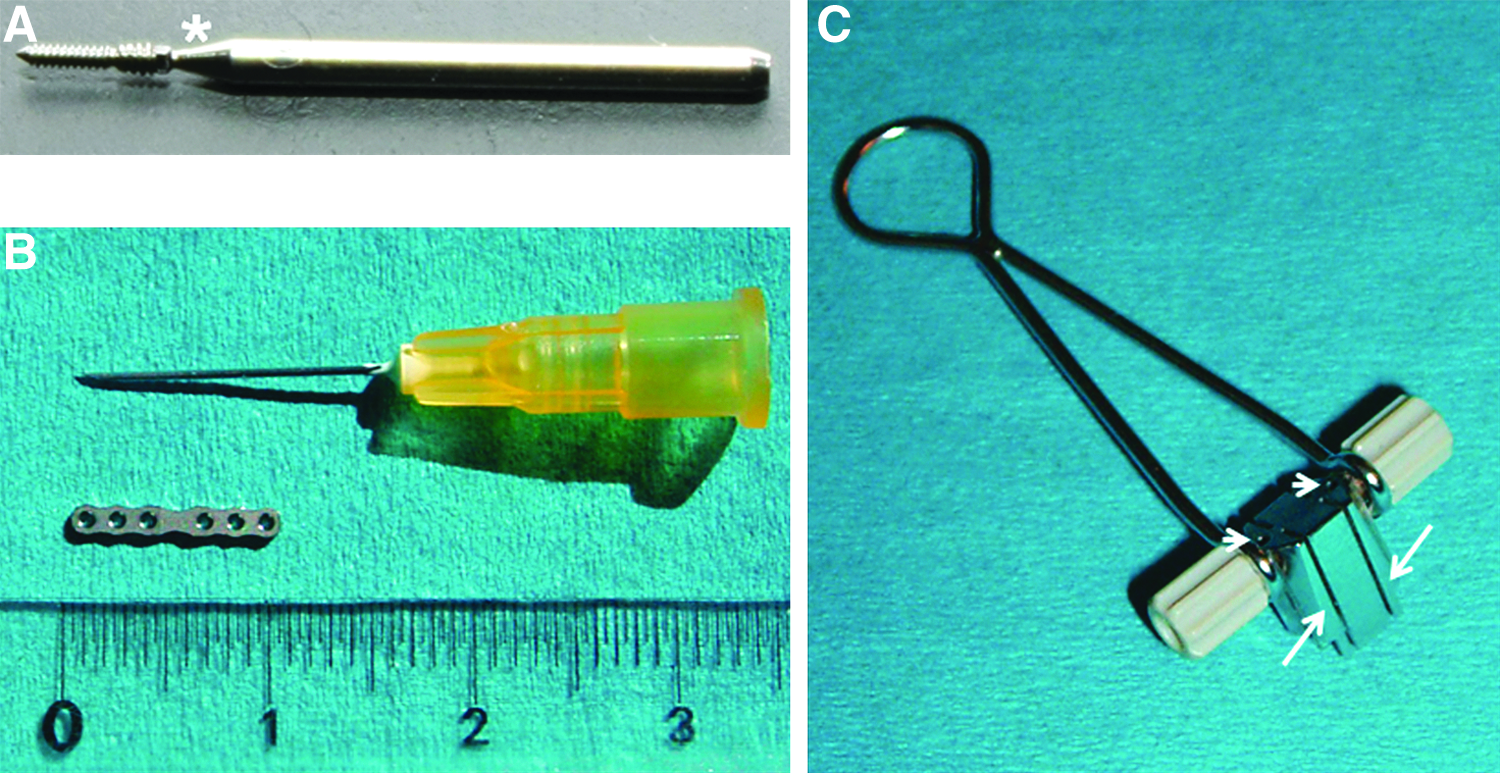
Instruments used for the plate osteosynthesis.
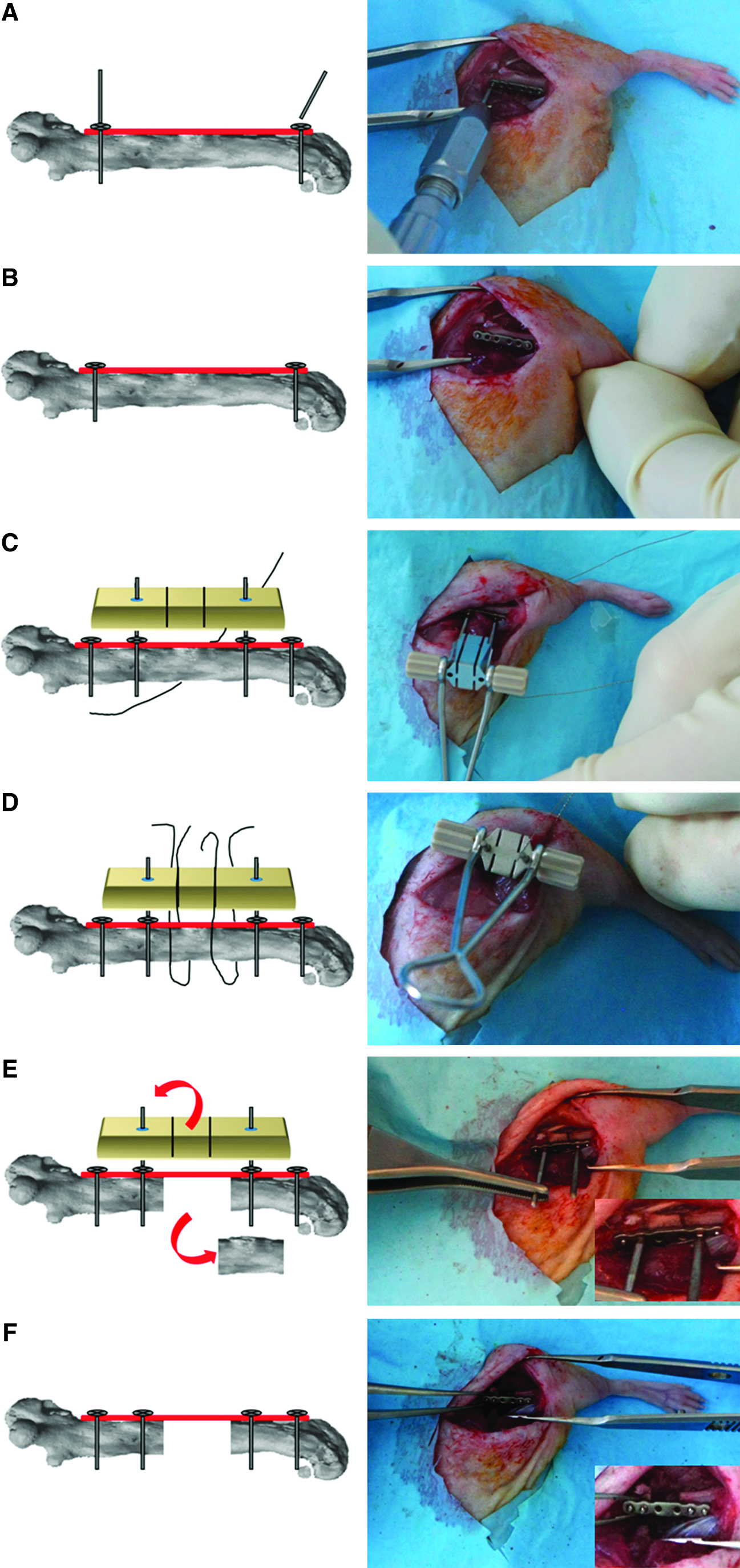
Key aspects in the surgical procedure.
Throughout the postoperative period, the mice were allowed to weight-bear. Food and water was available ad libitum. All mice were monitored every day, and any abnormal changes in their activity, appearance, temperament, vocalization, feeding behavior, and appearance of the surgical site were considered defined humane endpoints as previously described.43,44
Standard lateral digital radiographs (MX20; Faxitron X-ray Corp., Edimex, Le Plessis Grammorie, France; 26 kV, 10 s; 2×magnification; 20 lines/mm spatial resolution) were taken immediately after surgery and every 2 weeks for the next 10 weeks under volatile anesthesia. On the radiograph taken immediately after surgery, the length of the defect and the distance between the distal part of the plate and the most distal part of the knee were measured using an image-processing program (ImageJ software, Research Service Branch, National Institute of Mental Health).
Mice were sacrificed by overdose of barbiturate (Dolethal®, Vetoquinol, France) 10 weeks after surgery.
Collection and analysis of specimens
Immediately after euthanasia, all left femoral bones were excised. All overlaying muscle tissue was carefully removed. The femoral bones were fixed in 4% paraformaldehyde (pH 7.4) for 4 days. The plate and screws were removed after paraformaldehyde fixation of the respective tissue specimens.
Radiographic analysis
In the present study, bone union was defined as bone continuity observed on radiographs either throughout the defect or at the interface between the graft and the edges of the native bone. In contrast, nonunion was defined as lack of bone continuity in the defect-left-empty group and as the presence of a gap between the graft and the edges of the native bone in the two groups of animals whose defects had been filled with the materials tested in the present study.
Micro-CT scan analysis
All specimens were imaged and analyzed using high-resolution microcomputed tomography (micro-CT; Skyscan 1172; Skyscan, Aartselaar, Belgium). During scanning, the femoral bones were placed in polyethylene tubes filled with alcohol (75 volume percent). Radiographic projections were acquired at 80 kV and 100 μA with a fixed exposure time of 1000 ms, an aluminium 0.5 filter, and a 4-μm camera pixel size (2400×4000), with a voxel size of 7 μm. Four frames were averaged for each rotation increment of 0.9°. Three-dimensional images with a voxel average size of 13 μm were reconstructed using a Hamming-filtered back-projection, and the manufacturer's reconstruction software (NRecon; Skyscan, Aartselaar, Belgium). Analyses were performed in the same manner for each mouse with a volume of interest corresponding to the respective defect. For qualitative analysis, the number of united cortices in two orthogonal reconstructed views was recorded, and bone union was considered when four out of four cortices were united. For quantitative analysis of bone formation within the region of interest, resident software (CTAn, Skyscan, Aartselaar, Belgium) was used to obtain the volume of mineralized tissue. These volume values reflected (1) the newly formed bone in the defect left empty group, (2) the newly formed bone and the residual grafted bone in the syngenic graft group, and (3) the newly formed bone and the residual coral scaffold in Acropora coral scaffold group. A lower gray threshold of 45 grayscale indices (0.035 attenuation coefficient) and an upper gray threshold of 240 grayscale indices (0.186 attenuation coefficient) were applied for each mouse.
Histology
After micro-CT imaging, the excised and fixed femoral bones were embedded in methylmethacrylate resin and processed for undecalcified histology. All femoral bones were cut lengthwise using a circular water-cooled diamond saw (200 μm; Leitz 1600; Leica Inst., Nussloch, Germany). Two sections closest to the longitudinal mid-sagittal plane, and including the entire length of the implant, were selected. These sections were ground down to a thickness of 100 μm, polished, and surface-stained using Stevenel blue and van Gieson picrofuchsin stains.
Data analysis and statistical analysis
Values of the radiographic measurements and data of the mineralized tissues were expressed as mean±standard deviation (SD). Statistical analyses were performed using a commercially available software package (GraphPad Prism 5; GraphPad Software, Inc., La Jolla, CA).
Numerical data were analyzed statistically using the one-way analysis test. The confidence interval was set at 95% and the significant level at p<0.05.
Results
Surgical observations
The duration of the operative procedure, from the induction of anesthesia to skin closure, was 45 to 60 min. In all cases, osteosynthesis was easy to perform and did not require the use of either an operating microscope or a binocular loupe. No perioperative complications occurred, and correct positioning of the plate and screws was achieved in all cases. Based on radiographic measurements, the average length of the defect was 3.43±0.12 mm and the distance between the knee and the distal part of the plate was 2.65±0.56 mm. These values indicate a reproducible defect and plate positioning.
Clinical results
With the exception of one mouse (in the defect-left-empty group) that died during the surgical procedure, postoperative recovery was uneventful; the mortality rate was 5.5%. No specific postoperative animal care was required. All mice were allowed to move freely without any restrictions. Daily monitoring did not reveal any changes in activity, appearance, temperament, vocalization, and animal feeding behavior. Self-injuries or injuries induced by other mice (which were housed in the same cage) were never observed.
The animals returned to normal activity within 1 day following surgery. Although weight bearing on the operated limb was slightly reduced for the first five postoperative days, a normal gait pattern was observed in all animals after that time point and throughout the duration of the study. No wound complications or implant failures were observed. Stable bone fixation was obtained in all animals throughout the study.
Segmental bone repair assessment
Radiographic and micro-CT analysis
Radiographs provided evidence that bone healing did not occur in any animal of the defect-left-empty group at the 10 weeks postimplantation time point. Micro-CT examination confirmed the absence of union in the defect-left-empty group at this time point (Fig. 3; Supplementary Fig. S1; Supplementary Data are available online at
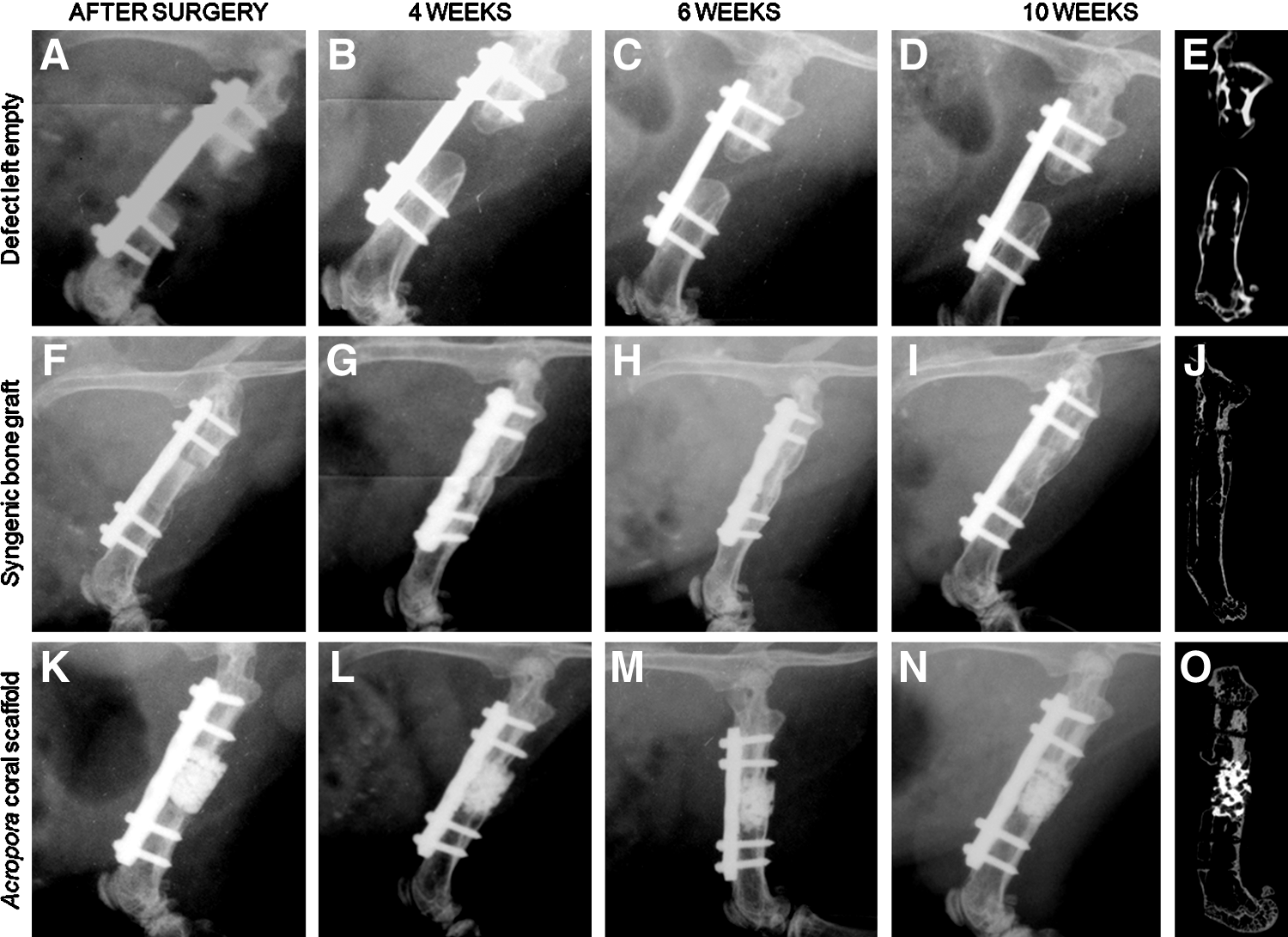
Representative radiograph and sagittal micro-CT reconstruction of the femoral bone of mice with a defect left empty
In the syngenic-bone-graft group, a gap between the graft and the edges of the native bone was observed on radiographs taken immediately postoperatively. In this animal group, the bone grafts remained stable throughout the study. By 10 weeks postimplantation, there were no more such gaps, and the radiographs revealed bone union in all animals. This result provided evidence of new bone formation between the graft and the surrounding native bone (Fig. 3; Supplementary Fig. S1). Examination of the micro-CT images revealed that four out of four cortices were united in four animals, whereas two out four cortices were united in the other two (out of six total) animals in this group.
In the animal group that had received Acropora coral scaffolds, the respective radiographs taken up to 10 weeks postoperatively revealed apposition of the scaffold to the bony edges in all animals tested. However, because the coral scaffold material contained minerals (specifically calcium carbonate), new bone formation could not be distinguished from the remaining scaffold material present in the defect on these radiographs (Fig. 3; Supplementary Fig. S1). No coral scaffold migration outside the defect was observed; instead, the coral scaffold remained in the defect in apposition to the bony edges for the duration of the study. Examination of the micro-CT images revealed that four out of four cortices were united in four (out of the six total) animals, whereas two out four cortices were united in the two other animals in this group (Fig. 3; Supplementary Fig. S1).
Histology
Histological analysis confirmed the absence of bone union in the defect-left-empty group (Fig. 4A). The medullary canals were obstructed by newly formed bone, with a rounded aspect, which emerged from the cortical edges of the osteotomy. These defects were mostly filled with fibrous tissue. No cartilage was identified.
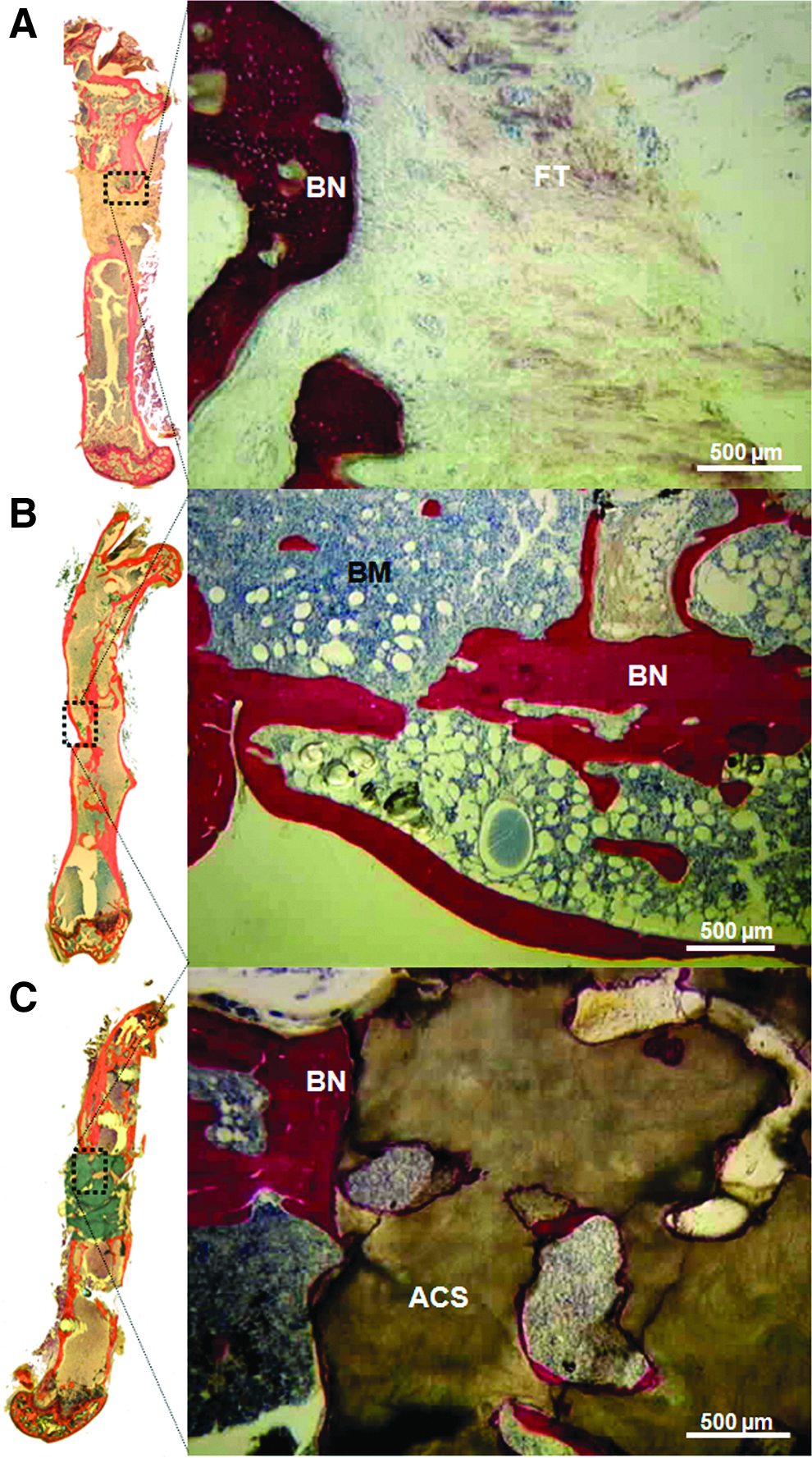
Representative histology of a defect left empty
In the syngenic-bone-graft group (Fig. 4B), the observed new bone formation integrated the graft into the native bone in all mice of this group. In four out of the six mice, complete bone continuity was observed between the graft and the surrounding bony edges; in these cases, bone marrow was also present. The other two mice, exhibited only partial re-establishment of bone continuity with either a proximal or distal union.
In the animal group that received the Acropora coral scaffolds (Fig. 4C), complete bone bridging of the segmental defect occurred in four out of the six animals tested. Similar to results observed in the syngenic-bone-graft group, only partial re-establishment of bone continuity was documented in the other two mice of this group (Supplementary Fig. S2). In addition, scant bone apposition was observed either around or inside the remaining coral scaffold close to the edges of the defects. Very little bone was observed inside the scaffold in all animals of this group; no bone was observed at a distance greater than 1 mm from the bony edges (Fig. 4C, Supplementary Fig. S2). Cartilage was never observed.
The volumes of mineralized tissue in the defect-left-empty group and in the syngenic-bone-graft group were 0.8±0.3 and 4.4±0.87 mm3, respectively. The volume of the mineralized tissue (i.e., newly formed bone and coral scaffold material) for the Acropora coral scaffold group was 8.9±0.7 mm3. The results obtained from the syngenic-bone-graft group and from the Acropora coral-scaffold group were significantly (p<0.001) higher than those obtained from the defect-left-empty group.
Discussion
A standardized, critical-sized, bone defect model at a weight bearing location in mice that is reproducible and effectively stable is an important contribution for the study of atrophic nonunion defects. To achieve effective stabilization, locking-plate osteosynthesis is routinely used in clinical situations and in large animal models. However, to the best of the authors' knowledge, use of locking-plate osteosynthesis in mice is highly challenging and has yet to be accomplished. 45
In the present study, we introduce for the first time the use of a titanium locking-plate for stabilizing a large segmental defect in a load-bearing location in small animals—specifically, mice. Among possible anatomical locations for such an application, the femur was chosen because of its geometry and dimensions: this is a tubular bone (∼12 mm long) with a relatively consistent inner and outer (∼1.5 mm) diameter that allows the creation of bone defects of consistent volume in a diaphyseal location. The straight and tubular anatomical features also compare favorably with (1) the triangular section of the tibial bone, (2) the small diameter of the radius,7,18 and (3) the curved shape of these bones.
From the surgeon's point of view, osteosynthesis with the plate was simplified by the use of the drill and saw guide and the design of the screws, which are self-tapping, have a drive shaft (that ensures precise guidance), and break once the screw is locked in the plate. 46 Ancillary tools enabled the surgeon to accurately position the plates and screws without either hip or knee-joint impediment. In fact, the distance between the distal part of the plate and the knee (an indicator of the positioning accuracy of the bone defect along the femoral shaft) was similar (2.65±0.56 mm) among all animals tested. In addition, the length of the osteotomy (i.e., 3.43±0.12 mm), whose dimensions were about twice the femur diameter, was similar to values (specifically, 1.8 to 3.0 mm) reported by other studies.18,27,31,33 Most importantly, the reproducibility of the surgical procedure was excellent, the length of the ostectomy was consistent across all animal as evidenced by the low SD (±0.12 mm). The osteosynthesis material used allowed accurate positioning of the plate before drilling; use of the drill and saw guide facilitated the creation of bone defects of reproducible size.
In the present model, only one mouse died during anesthesia, but no other complications were observed. Stable bone fixation was obtained in all animals tested and was substantiated by the absence of cartilage formation in the defects at the end of the study. These results are remarkable because the defect length represented about 25% of the femur length and twice the size of the femoral-shaft diameter. Moreover, the use of plate fixation prevented iatrogenic damage to the articular surface; this aspect contrasted strongly with the use of intramedullary nails, which may lead to lameness and impair in weight bearing.24,47 Another very important outcome of the present study was that morbidity–mortality was low (5.5%) and fully complied with the maximum rate of 5% to 10%, which is acceptable in animal research models of bone tissue engineering. 6
When the defects were on purpose left empty, lack of bone repair, characterized by the absence of callus formation and rounding of the bone ends, was observed for 10 weeks; these results provided evidence that these defects were of critical size. The fact that the remaining gap area consisted solely of fibrous tissue without cartilage and bone is an indication that this is a reliable model of atrophic pseudarthrosis. This model is thus appropriate for evaluating therapeutic modalities for treating segmental critical-sized bone defects that result in atrophic nonunion.16,23,48
Mechanical ex vivo studies have established that femur stabilization achieved either with a locking plate or with an external fixator produced rotational stiffness almost similar to that of the intact femur in mice. 21 Up to now, external fixators have been extensively used to stabilize bone defects in rodents.17,26,33,34,49 When considering the use of these modalities in experimental studies in which interindividual variability must be tightly controlled, their disadvantages may include (1) two- to three-fold variability in stiffness between individual fixators, 26 (2) potential loosening of the pins due to pins tracts infections,26,50–53 and (3) potential for self-injuries or injuries induced by other cage-mate animals.7,54 Because of these limitations, an internal fixation method was chosen in the present study. Our data provide evidence that the bone plate (1) allowed easy postoperative management of the animals with no loosening of the pins, and (2) prevented self-injuries or injuries induced by other mice housed in the same cage. In addition, and in contrast to the weight of an external fixator (which, since it is equivalent to 4% to 20% of the mouse body weight, may potentially alter the load bearing pattern and, for this reason and ultimately, thus affect the bone healing process),26,33,34 the weight of the locking plate used in the present study was low 17 (less than 0.1% of the mouse body weight; specifically, 0.05 g for the plate and screws compared to the characteristic body weight of 30 g for a 10-week-old athymic mouse). An important consideration in using an internal plate fixation is that an open surgical approach of the operated bone (which may potentially induce injury to surrounding soft tissues) is required. However, such surgical approach is both well described and easily standardized. In addition, open surgical procedures will be required for implanting noninjectable treatment modalities, regardless of the osteosynthesis device used. Last but not the least, while a limited and controlled interfragmentary motion is known to stimulate endochondral callus formation and bone healing, 55 segmental critical-sized bone defects and atrophic nonunions must remain in a stable biomechanical environment while bone healing occurs. 32
As part of the model development, we also sought to apply this new model in assessing massive bone graft substitutes, specifically syngenic bone grafts and Acropora coral scaffolds in mice. From a surgical point of view, it is worth mentioning that placement of massive syngenic bone grafts and coral scaffolds in the defect spaces was easily performed; moreover, no graft migration was observed during the study. In this respect, the present model has certain advantages over either intramedullary pins or nails that, when used, could damage articular surfaces and, above all, damage the intramedullary cavity, reduce the volume of the filler material tested,17,47 and prevent use of massive scaffolds.
From a biological point of view, among the mice whose cavities had been filled with syngenic bone grafts in the present study, four out of six animals exhibited new bone formation with bone bridging and re-establishment of a bone marrow cavity; taken together, this evidence underscores that bone healing is successful when the gold-standard material is used in filling the respective defects. A possible explanation for the absence of bone bridging in the two other animals from this group may be the known limited osteogenicity capacity of the cortical bone graft, which was used in the present study. Further investigations are required to either confirm or refute this explanation. Alternatively, the absence of consistent bone bridging could be explained by the stiffness of the osteosynthesis and the lack of interfragmentary movement in the present model. Moreover, in four out of the six animals that received massive Acropora coral scaffolds, a bony bridge was observed, but newly formed bone was limited to the vicinity of the bone resection edges. These data are in agreement with those of previous studies of large animals in which coral scaffolds did not induce healing of long, segmental, critical-sized bone defects.9,13,14 In other words, similarly to what was observed in the case of large animal models,9,13,14 osteoconduction alone was insufficient to produce consistent bone repair in this model. The present defect small animal model is, therefore, suitable for assessing treatment modalities that possess not only osteoconductive but also osteoinductive and/or osteogenic features.
The present model, however, has certain limitations. The volume of the bone defect and load-bearing conditions found in humans cannot be fully simulated in a small animal model. The surgical procedure is expensive 17 and technically more demanding than those involving insertion of an intramedullary pin. The plate used in the present study must be removed before micro-CT analysis, because it is less conductive to longitudinal radiographic investigations compared to either internal fixation plates that are polymeric56–59 (and thus do not interfere with X-ray visualization) or external fixators (which can be partially removed). Last but not least, in contrast to external fixators, 17 the stiffness of the osteosynthesis, a key regulator of the bone healing process, 55 is not amenable to modulation without additional surgery.
The present model could be used to evaluate cell-containing constructs because it provides a standardized, long bone defect with minimum variability (resulting from small variations in the mechanical milieu [experienced by tissue constructs] and in the tissue construct volume). In addition, the model described in the present study is compatible with the use of advanced in vivo imaging techniques such as bioluminescence, which does not require animal sacrifice in order to monitor the process of tissue healing at various time points during a study. Previous studies established that nude mice are suitable for assessing the osteogenic ability of human mesenchymal stem cells loaded on various material scaffolds in ectopic locations18,60–62; pertinent studies in orthotopic locations, however, are sparse. Such studies are currently under investigation by our research team and provide promising results using genetically modified human mesenchymal stem cells and bioluminescence imaging. 63 This approach could be a major contribution to the refinement and reduction principles of use of animals in orthopedics-related research in accordance with the three “R's” concept: reduction, refinement, and replacement.
To summarize, the present study establishes a novel, reproducible, murine, load-bearing, critical-sized femoral defect model, stabilized by plate osteosynthesis that involves about 25% of the femoral length and mimics clinically atrophic nonunion. Stable, reproducible fixation of the aforementioned defect and stability of the implanted biomaterials used as fillers of these defects were obtained with low morbidity–mortality. An addition to the armamentarium of bone tissue engineering, the present model is also suitable for assessing treatment modalities of atrophic nonunion that possess not only osteoconductive, but also osteoinductive and/or osteogenic capabilities. Furthermore, noninvasive monitoring of the molecular and cellular events involved in bone regeneration is possible in such a model, which complies with the refine/reduce/replacement principles of animal experimentation.
Footnotes
Disclosure Statement
Romano Matthys is the Chief Executive Officer of the RIS Company, which provided the osteosynthesis material used in the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.