
Abstract
Osteochondral defects of the talus pose a difficult therapeutic challenge. An experimental animal model of the ankle joint is not available. The aim of this study was to test a newly developed animal model for osteochondral defects of the ankle in vivo. Osteochondral defects were created in the talus of goat hind legs using a posterolateral surgical approach. The defects were filled with either autologous cancellous bone or donor demineralized bone matrix or left empty as control. After 12 weeks of healing, the specimens were analyzed with radiography, macroscopy, microcomputed tomography, histology, histomorphometry, and fluorescence microscopy. It was possible to create a standardized defect in each talus. The implanted material remained in place. The analyses showed that most bony tissue was generated in the defects filled with autologous bone and least in the control defects. Our findings show that a standard osteochondral defect can be created in the talus by a relatively simple procedure in a large animal that allows qualitative and quantitative evaluation. The model can be used in future experiments to investigate alternative treatment methods before they are introduced into clinical practice.
Introduction
The use of animal models is often an essential step in the testing of orthopedic procedures before clinical use in humans. 20 To our knowledge, an animal model for ankle OCDs is not described in the literature. The aim of this study was to test a newly developed caprine model for OCDs of the talus, by evaluating an established treatment (autologous cancellous bone graft), an alternative treatment (demineralized bone matrix [DBM]), and no treatment (control). We defined the following criteria for a successful model: (1) the animal's joint anatomy and body weight are comparable to humans, (2) the surgical technique is reproducible (regarding the operative approach as well as size and location of the OCD), (3) the morbidity of the animals is acceptable (defined as full weight bearing and free of pain within 1 week), (4) the repair is best after applying an established treatment and minimal in control defects, and (5) the method must be accurate enough to detect small differences between groups.
Materials and Methods
Animals, experimental design, and operative technique
The study was approved by the Animal Care and Use Committee of the University of Amsterdam, the Netherlands. Three adult female Dutch milk goats (Capra Hircus Sana) were used with an approximate age of 4 years and a weight of 50, 80, and 89 kg, respectively. All goats were healthy, according to physical examination and blood tests by a veterinarian. They were kept in group housing starting 2 weeks before surgery.
Surgery was performed on both ankles in a sterile fashion with the goat in the lateral decubitus position under general anesthesia with endotracheal intubation. Before anesthesia, intramuscular injections with prophylactic antibiotic (Pen & Strep, Fendigo sa/nv, Brussels, Belgium), ketamine 10 mg/kg (Alfasan International BV, Woerden, the Netherlands), and atropine 1.5 mg (Centrafarm Services BV, Etten-Leur, the Netherlands) were administered. Intravenous etomidate (B.Braun Melsungen AG, Melsungen, Germany) was injected to induce general anesthesia. Fentanyl 250 μg (Hameln pharmaceuticals gmbh, Hameln, Germany) and midazolam 15–20 mg (Dormicum, Roche Nederland BV, Woerden, the Netherlands) were injected intravenously, and repeated, when necessary. Isoflurane 1.0%–2.5% (Nicholas Piramal Limited, London, United Kingdom) was administered by inhalation.
A curvilinear skin incision was made just posterior to the lateral malleolus, parallel to the Achilles tendon (proximal) and the calcaneus (distal). After mobilization of the lateral saphenous vein, an arthrotomy was performed in the plane between the peroneal tendon (anterior) and the lateral saphenous vein (posterior). A Hohmann retractor was placed behind the medial talus to optimize exposure of the talus and protect the tendons and neurovascular structures. Full dorsiflexion of the ankle allowed maximal exposure of the articular surface of the talus (Fig. 1A). In the center of the talar trochlea, a custom-made drill socket with a diameter of 6 mm was placed, which ensured drilling to a precise depth of 6 mm. Under continuous cooling with saline, the defect was drilled perpendicularly to the talar surface, starting with a sharp drill and finishing with a milling cutter to achieve a flat base of the defect (Fig. 1B). A goat study investigating the natural course of knee defects showed that 6-mm defects do not heal spontaneously within 1 year. 21
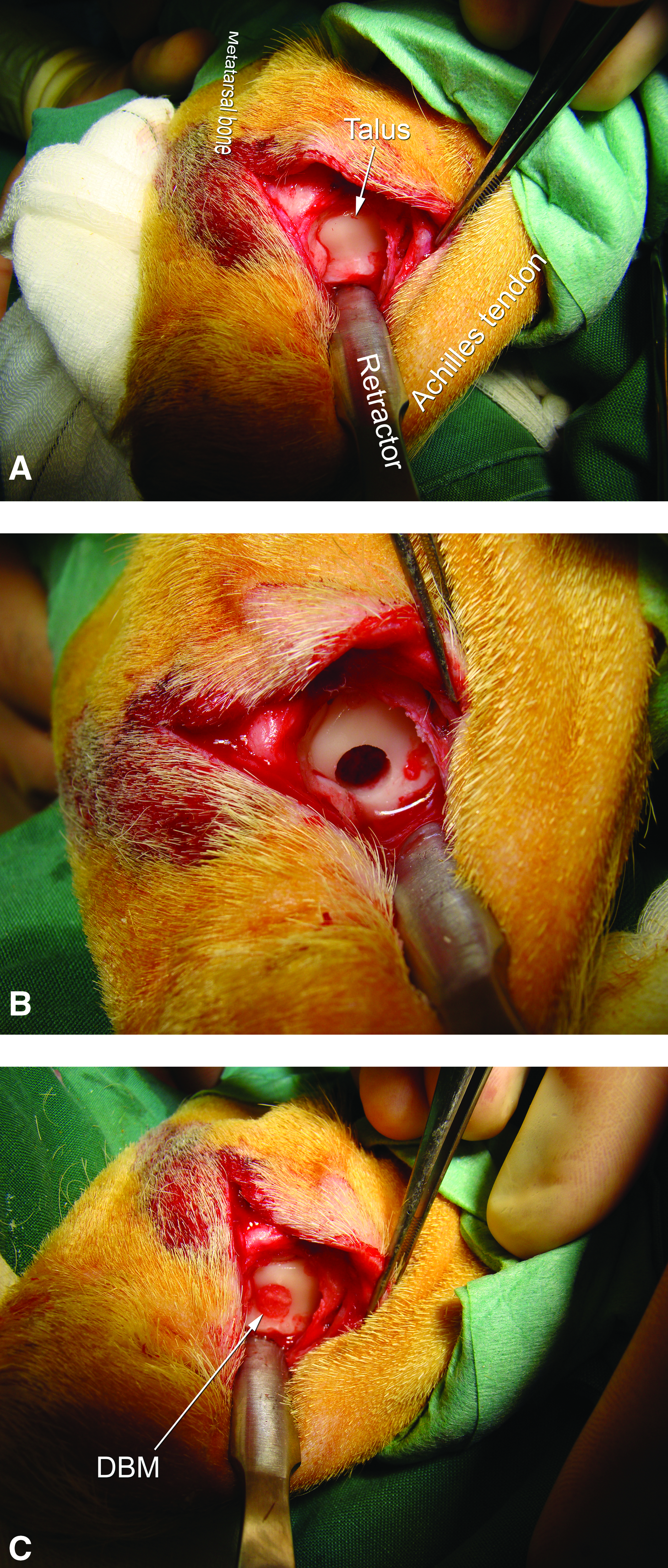
Digital pictures showing key aspects of the surgical technique. The talar dome was exposed through a posterolateral approach
Each defect was treated according to a predefined randomization scheme with autologous cancellous bone (harvested from the iliac crest) or a commercially available cortical demineralized bone matrix (Bonus™ DBM, Biomet BV, Dordrecht, the Netherlands) hydrated with normal saline, or left empty (untreated control). Filling up to the level of the articular cartilage surface (Fig. 1C) was ensured by inserting ample material press-fit and moving the ankle through a full range of motion (removing any abundant material above the surface of the defect due to the congruency of the ankle joint). The joint capsule and subcutaneous tissue were closed with interrupted 2–0 absorbable sutures, and the skin was closed with absorbable sutures placed in a continuous intracutaneous pattern.
Postoperatively, analgesic medication consisted of a single subcutaneous injection of 0.005 mg/kg buprenorfine (Temgesic®, Schering-Plough BV, Utrecht, the Netherlands), twice daily, as pain demanded (indicated by limping). After wound healing was completed, which took ∼1 week, the animals were kept outdoors in a large natural environment with food ad libitum and without activity restrictions. Eating habits, ambulatory activities, and health status were monitored daily.
After 12 weeks, the goats—back in the experimental animal center—were sacrificed by injecting a lethal dose of pentobarbital (Euthasol 20%, ASTfarma BV, Oudewater, the Netherlands) in the jugular vein, after they had been sedated with an intramuscular injection of ketamine 10 mg/kg (Alfasan International BV, Woerden, the Netherlands), xylazine 2 mL (Sedazine®, ASTfarma, Oudewater, the Netherlands), and atropine 1 mg (Centrafarm Services BV, Etten-Leur, the Netherlands).
Analyses
Radiography
Lateral radiographs of the ankles were taken before surgery and directly after surgery. Anteroposterior and lateral radiographs were taken after autopsy.
Macroscopy
The tali were excised directly after terminating the goats, and digital high-resolution photographs were taken of the talar and opposite articular surfaces. Macroscopic grading was performed by two observers. A general macroscopic articular evaluation system was used that awards zero to two points to each of five categories: range of motion, intra-articular fibrosis, restoration of contour, cartilage erosion, and appearance. 22 Ten points indicate a completely normal appearance, and zero points indicate a severely damaged joint surface. Furthermore, the talar articular surface was assessed according to the validated International Cartilage Repair Society (ICRS) cartilage repair assessment.23,24 This score consists of three items (i.e., degree of defect repair, integration to border zone, and macroscopic appearance) that are each assigned a maximum of 4 points, with a total of 12 indicating a normal appearance. The scores of the two observers were averaged and outliers with a difference of more than one point were scored again, until consensus was reached. 25
Microcomputed tomography
The talar heads were sawn off with a water-cooled band saw to optimize penetration of fixative for histological evaluation and allow placement of the tali in the microcomputed tomography (μCT) scanner. Specimens were fixed in 4% phosphate-buffered formaldehyde for 1 week. After they were submerged in 70% ethanol and subjected to a vacuum to remove all the air from the cancellous bone, they were scanned in a μCT scanner (μCT 40, Scanco Medical AG, Brütisellen, Switzerland). With the defects facing down, the specimens were mounted in cylindrical specimen holders and secured with synthetic foam. This setup ensured consistent scanning of the defects parallel to the axis of the scan tube. The resolution of the scans was 18 μm, the voltage 70 kV, the current 114 μA, and the integration time 1000 ms. To discriminate between bone and background, the reconstructions were segmented using an adaptive threshold procedure, which determines the minimum between the two peaks in the gray values histogram, representing bone and background, respectively. 26
For quantitative analysis, two cylindrical volumes of interest were defined: one representing the complete OCD, measuring 6 mm in diameter and 6 mm in depth, and one representing the central OCD, measuring 3 mm in diameter and 5 mm in depth. The latter volume of interest was defined at 5 mm in depth to avoid analyzing original bone at the base of the OCD. The ratio between bone volume and tissue volume (BV/TV) was determined for all volumes of interest using morphometric software (Scanco Medical AG, Brütisellen, Switzerland).
In addition to the six operated specimens, five unaffected goat tali from a spinal fusion study (unpublished data) were μCT scanned and analyzed in the same manner to obtain normative data.
Histology
After fixation, the specimens were dehydrated using ascending grades of ethanol (70% to 100%) in two steps a week, and embedded in methyl-methacrylate (BDH Laboratory Supplies, Poole, England). After cold polymerization, the undecalcified specimens were cut into coronal 5-μm sections with a Jung-K microtome (R. Jung, Heidelberg, Germany). Seventy-five central sections were obtained from each specimen. Every third section (n=25) was stained with the Goldner's trichrome method, giving the following staining pattern: green for mineralized tissue, red for osteoid, blue or black for cell nuclei, and light orange or red for cytoplasm. The Goldner stained sections were used for evaluation of mineralized bone tissue, osteoid, fat cells, osteocytes, osteoblasts, and osteoclasts. Every second out of three sections was stained with toluidine blue for examination of structural details and cell appearance of the articular surface of the defects. Every third out of three sections was left unstained for fluorescence microscopy. Two observers, blinded to the treatment modality, qualitatively assessed the stained sections using transmitted light microscopy.
Histomorphometry
One representative Goldner-stained mid-section of each talus was analyzed using a Leica DMRA microscope that was connected to Leica Qwin computer software (Leica Microsystems Imaging Solutions, Cambridge, United Kingdom). A special routine was written for quantitative measurements of bone parameters.
Three areas of interest were defined: (1) the center of the OCD, (2) close to the borders of the defect (lateral, medial, and bottom), and (3) close to the articular surface of the defect. Six representative measurement fields of 307,000 μm2 were selected and digitized at a magnification of ×200, resulting in one to three measurement fields for each area of interest (Fig. 2). The mineralized bone area (bone%) and osteoid area (osteoid%) were measured. The number of osteocytes, osteoblasts, and osteoclasts was counted at a magnification of ×400. All measurements were performed twice by one observer and once by a second observer, both blinded to treatment allocation. The mean of both observers is reported, and intraobserver and interobserver reliability were calculated.
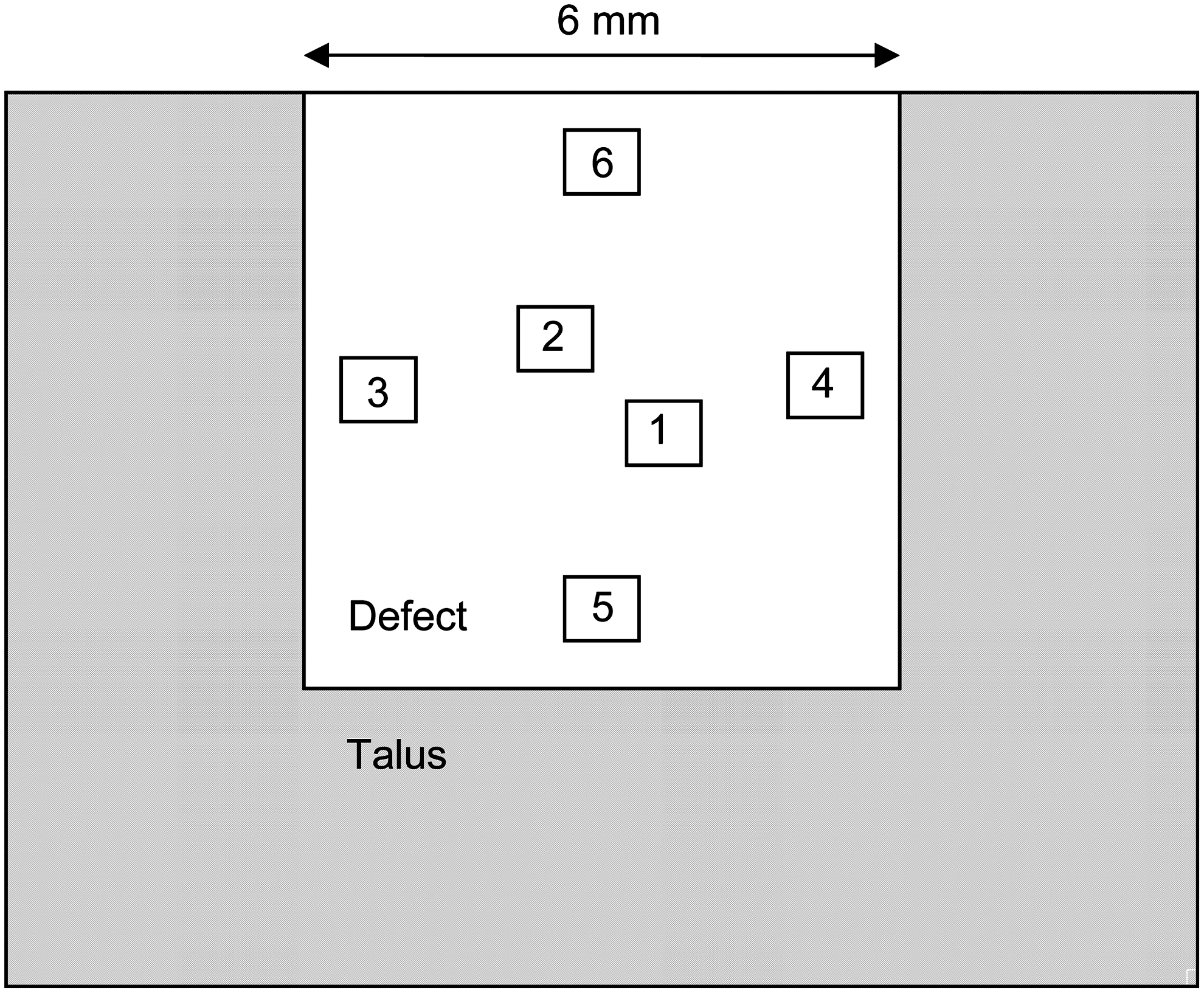
Schematic drawing showing the six measurement fields in which histomorphometry analysis was performed. The fields represent areas in the center (1–2), close to the borders (3–5), and close to the surface (6) of the defect.
Fluorescence microscopy
Fluorochrome labels were injected at three (oxytetracyclin 20 mg/kg), six (calcein green 10 mg/kg), and 9 weeks (alizarin red 25 mg/kg) after surgery. The dosages were based on the recommendations by van Gaalen et al. 27 One unstained section that was adjacent to the Goldner stained section was used for histomorphometry. Six measurement fields, (magnification, ×400), similar to the areas of interest of histomorphometry, were digitized using fluorescent filters. According to the manufacturer's guidelines, the D-filter (excitation 355–425 nm, emission 470 nm) was best used for oxytetracyclin and alizarin, and the I3-filter (excitation 450–490 nm, emission 515 nm) was best used for calcein, although each label was visible with both filters. One independent observer, blinded to treatment allocation, measured the distance between two consecutive lines at ∼10 locations within a measurement field. The mineral apposition rate (MAR, μm/day) of the bone was calculated as the average distance between the corresponding edges of two consecutive fluorescent bone labels, divided by the number of days between start and end of the administration period.
Statistical analysis
Individual quantitative results are presented. The treatment pairs were not statistically compared because of the small sample size. Mean and standard deviation (SD) were calculated of the μCT scans of five unaffected goat tali. To assess intra- and interobserver reliability of the histomorphometric measurements, intraclass correlation coefficients (ICCs) were calculated using SPSS version 18.0 (SPSS, Chicago, IL). ICCs of more than 0.75 are considered excellent. 28
Results
With the operative technique described, it was possible to create a standardized OCD in the talus. After surgery, the first two animals recovered well without complications. The goats were able to walk on their hind legs within 24 h. The third goat had persistent pain of the right ankle, despite treatment with subcutaneous analgesics for 2 weeks and intramuscular antibiotics (Pen & Strep, Fendigo sa/nv, Brussels, Belgium) for 1 week. There were no signs of infection. Surgical exploration of the painful ankle after 2 weeks revealed no pathology. Cultures showed no pathologic microorganisms. An exact cause could not be determined. The goat was terminated for ethical reasons 2 weeks following initial surgery. Obduction revealed no pathologic conditions. Histology of the right talus showed that the original DBM was still in situ (Fig. 3). In consultation with the Animal Care and Use Committee, the sacrificed animal was replaced by another goat, which recovered well from surgery and completed the follow-up period.
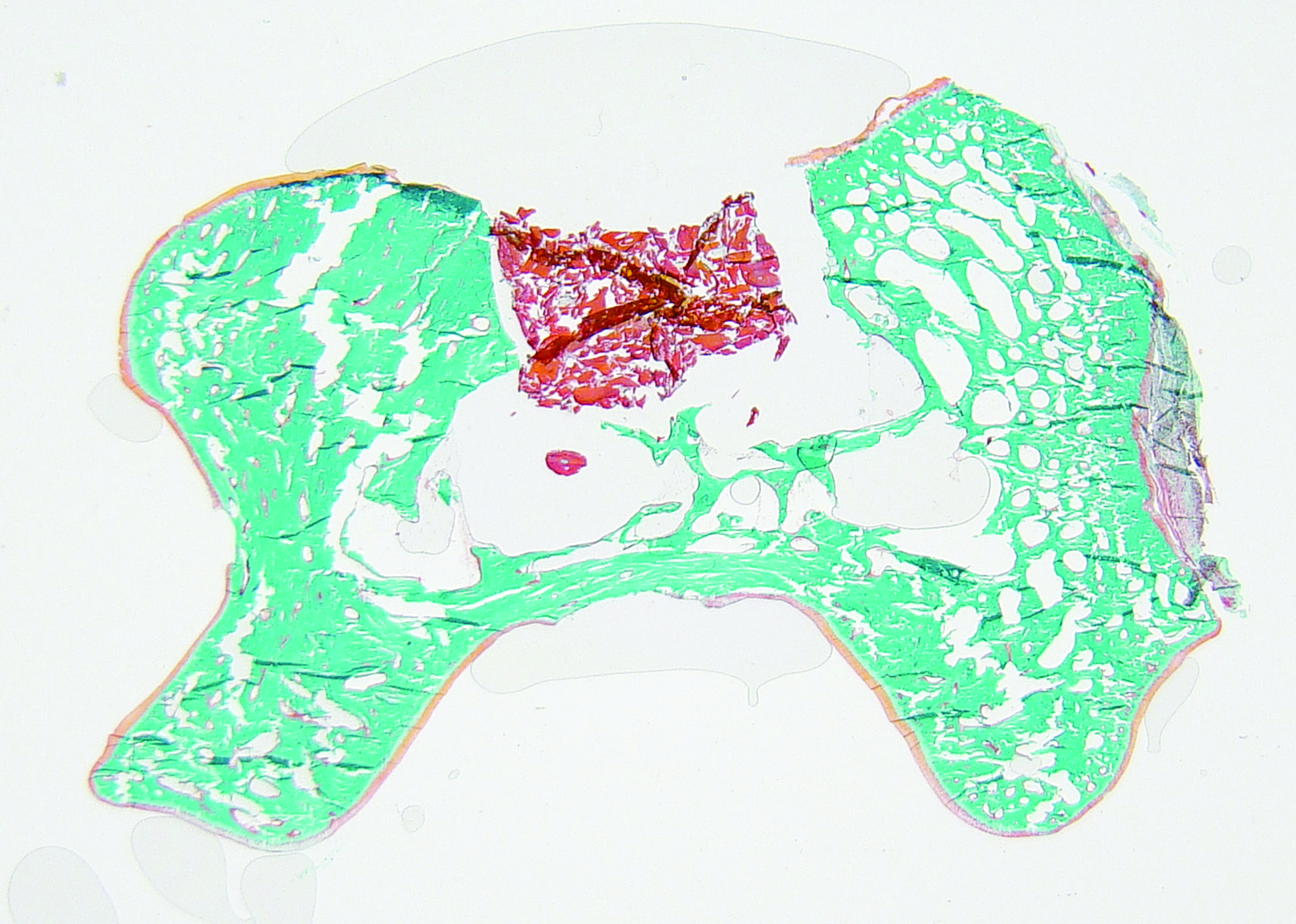
Histological section of a defect filled with DBM, 2 weeks after implantation, shows that the material remained in situ. Color images available online at
Radiography
Preoperative radiographs showed normal ankle joints without signs of osteoarthritis. Immediate postoperative radiographs showed the OCDs in three cases (one of each treatment); the defects were not visible in the other three. On the final radiographs after the 12-week period, none of the defects was visible.
Macroscopy
Macroscopic inspection of the ankle joints revealed no signs of inflammation. All defects were covered with tissue resembling fibrocartilage (Fig. 4). The surrounding talar cartilage and opposite joint surfaces appeared completely normal. The highest macroscopic assessment scores were achieved in an AB specimen and the lowest in a DBM specimen (Table 1).

Macroscopic view of three specimens.
AB, autologous bone; DBM, demineralized bone matrix; ICRS, International Cartilage Repair Society cartilage repair assessment23; L, left; R, right.
Micro-CT
In the complete 6-mm OCDs, BV/TV ranged from 0.10 to 0.45 (Table 2). In comparison, mean BV/TV of the five unaffected tali was 0.68 (SD, 0.06) in the complete cylinder and 0.70 (SD, 0.05) in the central 3-mm cylinder. The 3-mm central cylinders can be considered indicative for the regenerative capacity of the treatment applied because bone had regenerated from the borders and bottoms of the defects. In these 3-mm cylinders, the tali treated with autologous bone showed the most bone tissue, and the control group the least (Fig. 5).
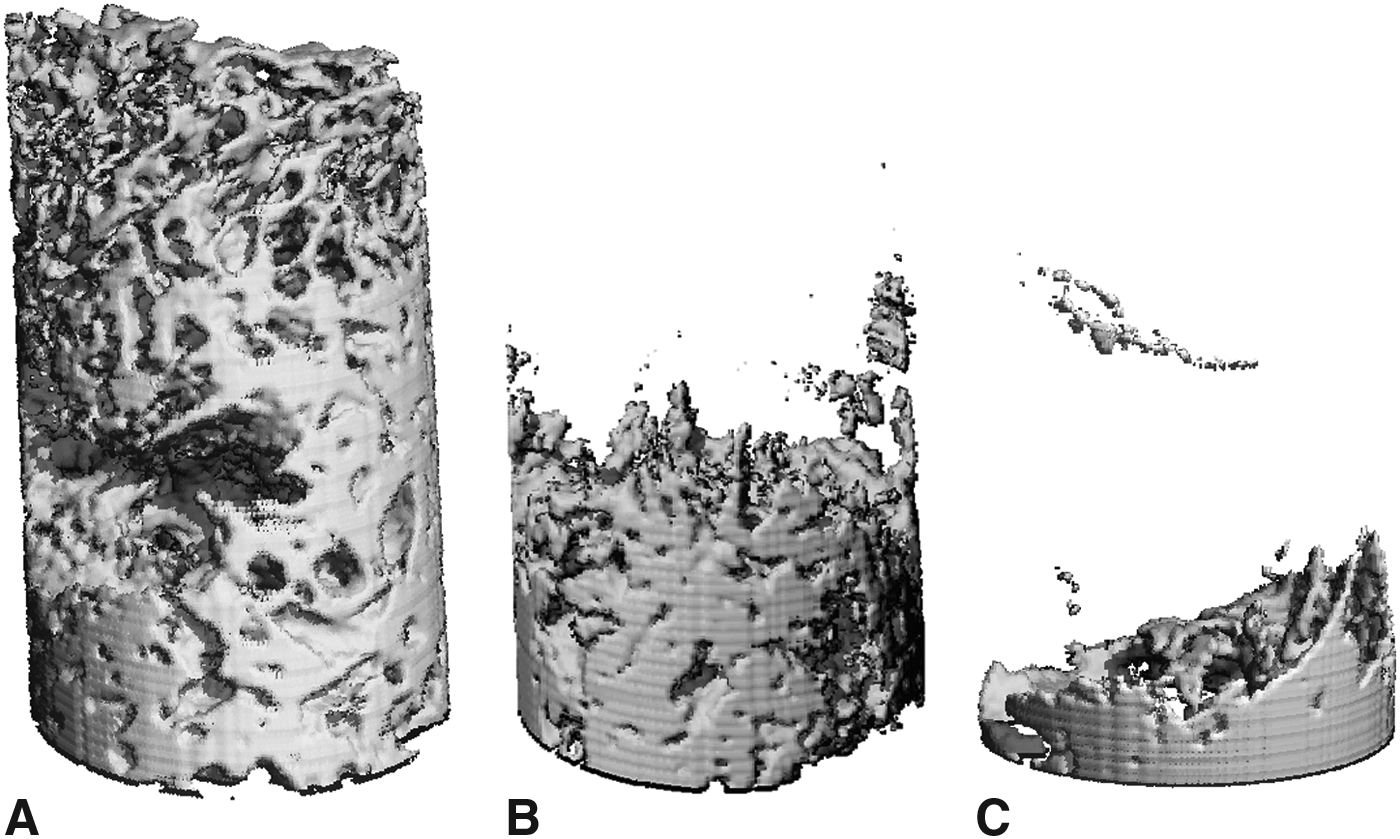
Three-dimensional reconstructions of microcomputed tomography scans. These volumes of interest represent central 3×5 mm cylinders.
Histology
In the OCDs treated with autologous bone, diffuse bone formation and near-complete filling was observed (Fig. 6A). There was continuing bone remodeling, as indicated by large areas of osteoid tissue and the presence of abundant osteoblasts and a rare osteoclast. At the articular surface, the defect was mainly composed of (mineralizing) fibrocartilage tissue with some chondrocytes embedded. Underneath the surface, there were areas of woven and lamellar bone.

Histologic sections with Goldner's trichome staining; magnification, ×25.
In the defects treated with DBM, some bone formation was observed—both lamellar and woven—with abundant osteoid in one specimen (Fig. 6B). Most bone was formed at the borders, but also some in the center of the defects. The original DBM was not visible. In one specimen, the surface of the defect was composed of a thick layer of fibrocartilage. In the other, the surface was mainly composed of connective tissue, fibroblasts, and leukocytes (lymphocytes and granulocytes).
The control defects did not heal (Fig. 6C). Some woven bone originated from the borders of the defects. Occasional mineralization of cartilaginous tissue at the surface suggested endochondral ossification. The greatest part of the defects was filled with fat cells and connective tissue.
Histomorphometry
Histomorphometry followed the same pattern as the μCT analysis (Table 3). Most bone formation was observed in the autologous bone pair; most osteoid formation was found in DBM. There was only one specimen (autologous bone) with bony and osteoid tissue in the measurement field of the surface. Osteoclasts were rarely found: only a single osteoclast was seen in one measurement field (center) in one specimen (autologous bone).
The intra- and interobserver reliability of the histomorphometric measurements were excellent; the lowest ICC was 0.80 (interobserver reliability of osteoblasts in the center; p=0.016), and the highest was 1.00 (intra- and interobserver reliability of bone% in all areas of interest; p<0.001).
Fluorescence microscopy
MAR varied from 0 μm/day in the areas where no bone growth was observed to 11 μm/day in the center of the defect in an autologous bone specimen (Table 4). The calcein green labels were best visible, followed by oxytetracyclin and alizarin, respectively (Fig. 7). The MAR could not be analyzed in two occasions because alizarin red labels could not be detected (see Table 4).

Fluorescence microscopy with I3 filter (excitation 450–490 nm, emission 515 nm), magnification ×400. Fluorochrome labels were injected at 3 (oxytetracyclin; yellow arrow), 6 (calcein; green arrow), and 9 weeks (alizarin; red arrow) to analyze the mineral apposition rate. Calcein was best visible, followed by oxytetracyclin and alizarin, respectively. Color images available online at
Discussion
A new caprine model was developed for the comparison of treatments for osteochondral ankle lesions. The model is presented in this study and seems feasible for the evaluation of new treatment options. Similar to the human ankle joint, the caprine ankle is congruent and able to bear high loads. The goat's body weight and metabolic and remodeling rates correspond to those of humans. 29 Furthermore, the proportion of cartilage to subchondral bone and the subchondral bone consistency is reportedly close to humans. 15 The operative technique described is reproducible, a standardized OCD can be created in each talus, and the implanted material remains in situ. Most importantly, there is a clear difference in outcome between defects treated with autologous cancellous bone and control defects. This was particularly shown by the quantitative analyses with μCT and histomorphometry. The mean BV/TV of the central OCDs was 0.25 in the autologous bone pair, 0.07 in the DBM pair, and 0.02 in the control pair (Table 2). Similarly, mean central bone% according to histomorphometry was 39.4 in the autologous bone pair, 15.5 in the DBM pair, and 0.2 in the control pair (Table 3). However, no definite conclusions can be drawn on the effectiveness of the treatment because of the low number of animals studied.
Previous animal studies have been performed predominantly on the stifle joint.15,30 These studies may be inadequate for assessing treatment modalities for ankle OCDs, as there are some specific differences between the knee and ankle. First, physiological cartilage properties differ. Congruent joints, such as the ankle, have a thin layer of cartilage to distribute the load and maintain an acceptable level of stress, whereas incongruent joints, such as the knee, have thicker areas of cartilage to increase the contact area between joint surfaces. 31 The cartilage of the ankle has a greater compressive modulus compared with the knee.16,31 Second, the knee and ankle joints seem to respond differently to cartilage injury. There appears to be a net anabolic response to injury in the ankle cartilage and a net catabolic response in the knee.19,32,33 Ankle cartilage may be more resistant to osteoarthritis development for a number of reasons, including higher equilibrium and compressive moduli, better intercellular communications, increased resistance to inflammatory molecules, increased metabolic activity, and higher congruency of the articular surfaces.19,34 Because of these differences, an animal model specifically developed for the ankle joint is required.
Although most animal models are designed for unilateral surgery, 30 a bilateral defect was created in the present model. This method reduces the number of animals needed and allows for a paired treatment comparison. A paired analysis may be a better strategy than unilateral evaluation or random assignment of treatment in bilateral models, since the regenerative capacities may differ from animal to animal (Tables 2 and 3).
Clinically, plain radiographs are obtained for the initial diagnosis of OCD and for follow-up. However, in the present animal model, radiographic evaluation as an outcome measure proved to be useless because the defects were not visible in most instances. In contrast, histomorphometry is traditionally used to measure bone formation and is considered the gold standard. 35 It is common practice to analyze representative areas of interest to approximate the total defect.29,36,37 Disadvantages of this method are a possible modification of the structure of the tissue by slice preparation and the long time required for all processing steps.35,38 MicroCT provides a fast and nondestructive technique to characterize and measure the three-dimensional geometric and density properties of a bone specimen. 39 Gielkens et al. 38 compared the intraobserver reliability of μCT and histomorphometry. They concluded that both analyses are reliable, but are used preferably in combination.
Fluorescence microscopy is a useful supplement to plain histology to detect the speed of regeneration during the follow-up period. 27 When using fluorescence microscopy, there is no need to sacrifice additional animals at a shorter follow-up period. The success of fluorochrome detection depends on various aspects, for example, the type, concentration, route of administration, and methods of visualization. 27 In the present study, the recommendations of van Gaalen et al. 27 were used. Unfortunately, the alizarin red labels were not always visible, without an obvious cause. In contrast, calcein green was clearly visible in all cases. No adverse events related to the injections of the fluorochrome labels were seen in this study.
The follow-up period was 12 weeks. Revascularization and conversion of a bone graft into a vital trabecular structure have been reported to occur at ∼3 months in the goat, which corresponds to 8 months in humans. 36 However, the regeneration process was ongoing, observed by large areas of osteoid tissue and the presence of abundant osteoblasts. The final situation may thus not be achieved after 12 weeks. In studies with multiple follow-up periods, no substantial regeneration of OCDs in the knee joint was observed after 24 weeks, suggesting that a follow-up period of 24 weeks may show the final outcome.9,14
The principal limitation of the present study is the limited number of animals used. In consultation with the Animal Care and Use Committee, only three animals were studied because the morbidity of the animals could not be anticipated, as this was the first time the ankle model was used. Out of the initial six ankles, one showed persistent pain. This goat was sacrificed, and the substitute goat recovered uneventfully. Thus, one out of eight ankles had inacceptable morbidity. This morbidity corresponds to that of other goat studies investigating cartilage repair.22,40,41 We therefore believe that following studies with the presented model are justified. Because of the small number of animals and the variability in reparative capacity of the goats, we cannot reliably draw conclusions on the investigated repair procedures. Larger studies with paired analyses are indicated.
Conclusions
The caprine model described in the current study seems suitable for the study of osteochondral ankle defect treatment in vivo. The operative technique is fairly simple and allows the creation of a standardized OCD for qualitative and quantitative evaluation. The goat model can be used in future experiments investigating alternative treatment methods for this challenging condition before introduction into clinical practice.
Footnotes
Acknowledgments
The authors would like to thank Mr. K.W. Meijer, Mr. G. Vink, and Mr. P. Sinnige for taking care of the animals. Mrs. J. Hogervorst is acknowledged for support with preparation of the histology sections. Biomet BV, Dordrecht, the Netherlands is gratefully acknowledged for financial support and supply of the DBM.
Disclosure Statement
Biomet BV, Dordrecht, the Netherlands, financially supported this study and provided the Bonus™ DBM. The company was not involved in the development of the study protocol, execution of the study, data analysis, or writing the article. No personal funding was received.