
Abstract
A large animal model is required for the assessment of minimally invasive, tissue-engineering-based approaches to thoracic spine fusion, with relevance to deformity correction surgery for human adolescent idiopathic scoliosis. Here, we develop a novel open mini-thoracotomy approach in an ovine model of thoracic interbody fusion that allows the assessment of various fusion constructs, with a focus on novel, tissue-engineering-based interventions. The open mini-thoracotomy surgical approach was developed through a series of mock surgeries, and then applied in a live sheep study. Customized scaffolds were manufactured to conform with intervertebral disc space clearances that were required of the study. Six male Merino sheep aged 4–6 years and weighing 35–45 kg underwent the procedure mentioned earlier and were alloted a survival timeline of 6 months. Each sheep underwent a three-level discectomy (T6/7, T8/9, and T10/11) with a randomly allocated implantation of a different graft substitute at each of the following three levels: (1) polycaprolactone (PCL)-based scaffold plus 0.54 μg recombinant human bone morphogenetic protein-2 (rhBMP-2); (2) PCL-based scaffold alone; or (3) autograft. The sheep were closely monitored postoperatively for signs of pain (i.e., gait abnormalities/teeth gnawing/social isolation). Fusion assessments were conducted postsacrifice using computed tomography and hard-tissue histology. All scientific work was undertaken in accordance with the study protocol that was approved by the Institute's committee on animal research. All six sheep were successfully operated on and reached the allotted survival timeline, thereby demonstrating the feasibility of the surgical procedure and postoperative care. There were no significant complications and during the postoperative period, the animals did not exhibit marked signs of distress according to the previously described assessment criteria. Computed tomographic scanning demonstrated higher fusion grades in the rhBMP-2 plus PCL-based scaffold group in comparison to either PCL-based scaffold alone or autograft. These results were supported by a histological evaluation of the respective groups. This novel open mini-thoracotomy surgical approach to the ovine thoracic spine represents a safe surgical method that can reproducibly form the platform for research into various spine-tissue-engineered constructs and their fusion-promoting properties.
Introduction
I

Animal models in the study of spinal fusion have been used since the early 20th century (1913) and have been essential in the understanding of the factors pertinent to the process of spinal fusion. 6 Animal models have employed a suitable experimental environment to observe a statistically viable number of subjects within a defined time frame and to allow valid extrapolation of reproducible data and results to the clinical situation. 6 The physical size of the sheep spine is appropriate to allow spinal surgery to be carried out and to allow for an evaluation of the success of the study using fusion assessments. In this study, the thoracic spine is of specific interest, and the thoracic cavity of the sheep enables the simulation of an environment that is representative of an adolescent child, while allowing implant fixation techniques closely corresponding to those in the human patient.6–8
Given the historical and increasing use of sheep as a model for spine fusion studies, the sheep spine is chosen as a suitable fusion model in the current study.8–10 To date, sheep have been used in a large number of anterior interbody spinal fusion models and have been used to compare open thoracotomy and video-assisted thoracoscopic fusion models.11,12 Increasingly, bioactive growth factors in combination with biodegradable scaffolds resulting in biologically active substances are being studied with the intention of extending, enhancing or even replacing autologous bone graft.13–15
To the best of our knowledge, there is no existing preclinical large animal thoracic interbody fusion model allowing the assessment of tissue-engineering constructs such as biodegradable scaffolds (polycaprolactone [PCL]) and recombinant human bone morphogenetic protein-2 (rhBMP2) as a graft substitute to promote bony fusion.
This methods paper demonstrates a novel open mini-thoracotomy surgical approach to the ovine thoracic spine and represents a safe surgical method that can reproducibly form the platform for research into various spine bone tissue-engineering constructs and their fusion-promoting properties.
Materials and Methods
Animal model
All scientific work was undertaken in accordance with the study protocol that was approved by the Institute's committee on animal research. Six male Merino sheep aged 4–6 years and weighing 35–45 kg were operated on and survived to 6 months. The sheep underwent preliminary checks (visual exam, weighing) on arrival to the animal research facility before the intended date of surgery. Daily monitoring of the animals' general condition, eating, drinking, defecation, urinating, and gait was performed to ensure optimum health preoperatively. Any sheep exhibiting signs of malaise, difficulty in feeding, impaired bladder or bowel functions, or problems in mobilizing were excluded from the study. Titanium vertebral body screw and rod fixation implants were obtained from Medtronic (CD Horizon®M8 Titanium Multiaxial Screws, 5.5 mm rod.)
Surgical model
Surgeries were performed under strict aseptic conditions. The sheep were anesthetized with an intravenous induction of propofol (1%), (4 mg/kg, IV) and maintained with 50% oxygen in air, and isoflurane using a mechanical ventilator. The sheep were given buprenorphine (Temgesic®, 0.3 mg/mL) (0.005 mg/kg, IV) and ketorolac (Toradol®, 30 mg/mL) (0.5 mg/kg, subcutaneous) for pre-emptive and postoperative bi-modal pain management. All the sheep received prophylactic (ciprofloxacin [200 mg/100 mL] [5 mg/kg, IV]; cefazolin [Kefzol® 1 g] [20 mg/kg, IV]; gentamicin [80 mg/2 mL] [5 mg/kg, IV]) and postoperative parenteral antibiotic regimen. The animal's heart rate, oxygen saturation, and end-tidal carbon dioxide levels were monitored throughout the procedure. After the identification of disc levels of interest, the intervertebral discs were removed with ronguers, and bone graft substitutes were inserted after disc space distraction. Intra-operatively, a temporary indwelling chest drain catheter was inserted to generate a negative pressure within the right thoracic cavity to ensure adequate lung re-expansion in the event of iatrogenic damage to the lung pleura, and it was removed day-1 postoperatively. The sheep were transferred onto a custom-built hanging sling to support the animal in the immediate 24-h recovery period. Postoperatively, gait was visually assessed by experienced animal handlers on a daily basis. Any limp, signs of malaise or social exclusion were flagged as signs of mobility problems. Anecdotally, the sheep were seen to return to normal gait patterns 48 h postoperatively, hence exhibiting equal weight-bearing capacity in all four limbs, equal stride lengths, and speed. Stock diet and tap water was made available to the animal ad libitum. The animal's daily activity and wound condition was monitored on a regular basis. After 2 weeks of close monitoring at the research facility, the sheep were then transported to a recovery facility.
At designated timelines outlined earlier, the sheep were euthanized with sodium pentobarbitone (325 mg/mL). Spinal columns from T3 to L2 were dissected with retention of intersegmental ligamentous tissues, and specimens were stored at −20°C until further evaluation.
Scaffold
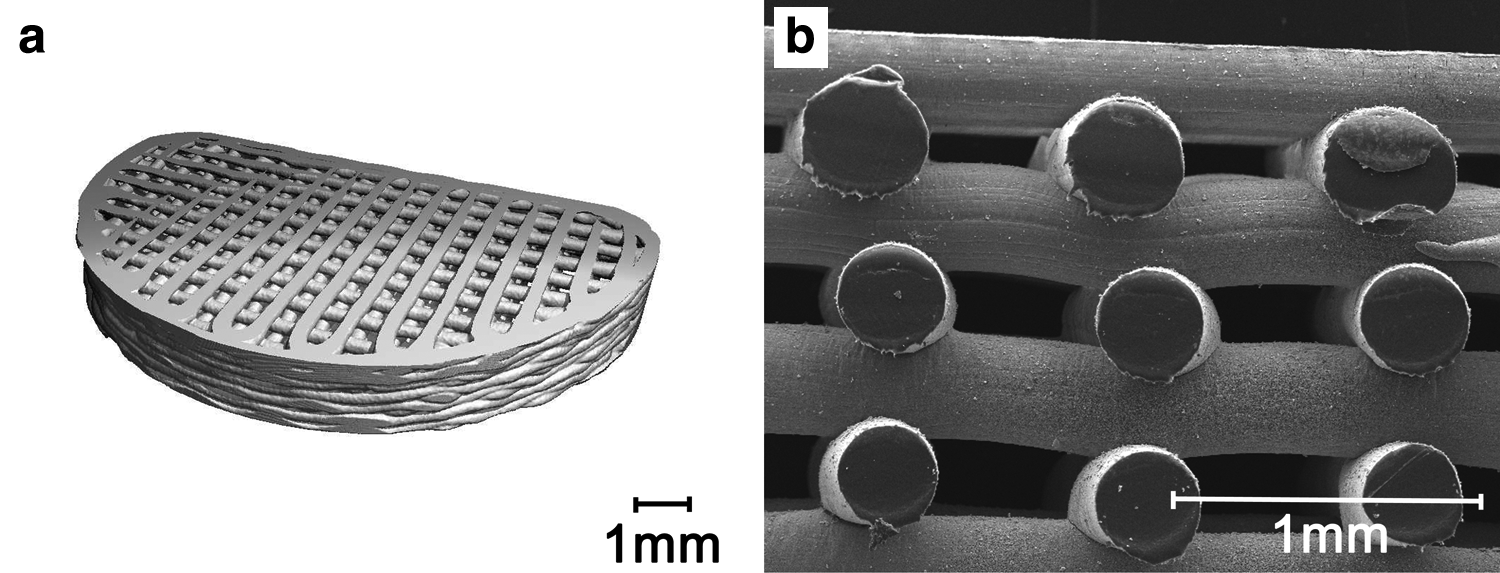
Scaffolds (2.5×9×15 mm3) were manufactured in house using biodegradable PCL and a computer-controlled extrusion-based additive manufacturing device (Dual BioExtruder) as described by Melchels et al. 16 The custom-designed scaffold conformed to the prepared spinal anterior intervertebral disc column, ensuring a low-profiled construct. A porosity of 60% and a 0–90° lay down pattern conferred desirable physiological and mechanical properties. 17
The scaffolds were coated with a biomimetic calcium phosphate (CaP) layer by immersion in concentrated simulated body fluid (×10), which has been shown to promote bone ingrowth and regeneration. 18 The CaP coating was confirmed qualitatively by Alizarin red staining and scanning electron microscopy of samples taken from batch-coated scaffolds as demonstrated in Figure 2. The scaffolds functionalized with commercially available rhBMP-2 (Medtronic INFUSE® Sofamore Danek Memphis) were lyophilized with Baxter Tisseel® fibrin sealant (Baxter AG) to act as a delivery medium for the rhBMP-2 by creating a mesh-like structure within the scaffold pores to promote cellular activities. Fibrin sealant has the ability to temporarily contain osteoinductive material before implantation, yet it releases these materials in vivo over time while it is being completely absorbed. 19 A total of 180 μL was functionalized onto the sterile scaffold comprising 60 μg thrombin (in 60 μL sterile water) and 540 μg rhBMP-2 (in 60 μL sterile water). rhBMP-2 at a concentration of 9 μg/μL was used to functionalize the CaP-coated PCL-based scaffold for implantation at levels randomized to receive the CaP-coated PCL-based scaffold plus rhBMP-2 (see next).
Computed tomography
To date, fusion assessments have been conducted on the six sheep of the 6-month timeline using high-resolution clinical computed tomography (CT) and histology as described next. Harvested thoracic spinal segments (T3 to L2) of all the animals were radiologically assessed using axial and sagittal reconstructions of CT scans performed on a high-speed scanner (Phillips Brilliance 64) with the following parameters: X-ray source current and voltage of 200 mA and 120 kV, respectively, and a 14 cm field of view at 0.7 mm slice thickness. Reformatted sagittal images (left parasagittal, mid-sagittal, and right parasagittal) were generated by Image J software and graded using the modified Sucato scale. 20 The percentage of disc fusion was calculated by dividing the osseous fusion area by the total discectomy area (as defined by the proximal and distal end plates and the posterior and anterior vertebral body margins for the joint in question). Each disc level was evaluated for fusion with use of a four-point grading scale whereby 0 points represent no fusion; 1 point, <50% fusion of the area of the disc space; 2 points, fusion between 50% and 75% of the area of the disc space; 3 points, fusion of more than 75% of the area of the disc space; and 4 points, complete fusion across the disc space. A score of 3 or 4 points was considered as representing solid fusion. 20 Reconstructed images as demonstrated in Figure 3 were graded twice by two independent reviewers in a blinded fashion.
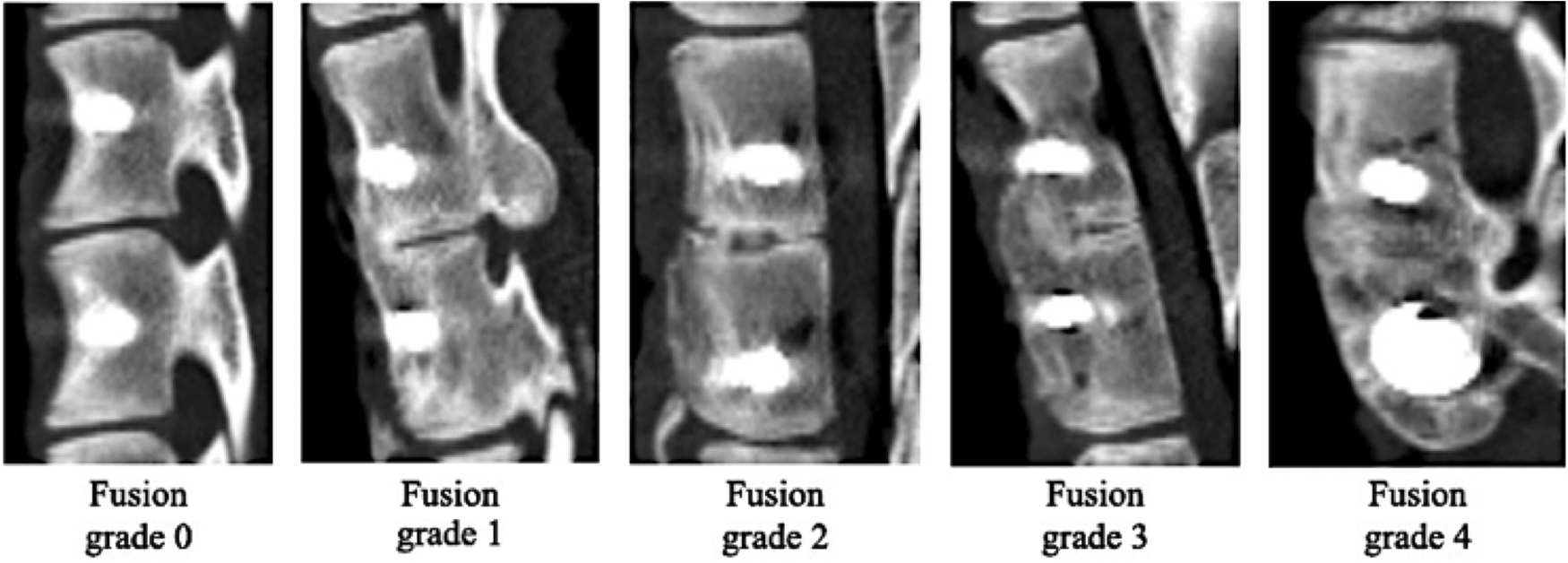
Representative sagittal CT images demonstrating the various fusion grades. Each disc level was evaluated for fusion with use of a four-point grading scale, where 0 points represent no fusion; 1 point, <50% fusion of the area of the disc space; 2 points, fusion between 50% and 75% of the area of the disc space; 3 points, fusion of more than 75% of the area of the disc space; and 4 points, complete fusion across the disc space. A score of 3 or 4 points was considered as representing solid fusion.
Histology
Spinal segments were fixed in 4% paraformaldehyde in an opaque container (the volume of which was∼10 times the specimen volume to achieve adequate fixation). Specimens were then dehydrated in a graded series of ethanols and embedded in acrylic resin (Technovit; Kulzer GmBH) followed by longitudinal sectioning with a high-speed, water-cooled, precision saw (EXACT 300 CP Band System) into parallel sections of 20 μm thickness. The sections were stained with Goldner's trichrome to provide differentiation of connective tissues (e.g., bone, bone marrow, cartilage, and fibrous tissue) as well as scaffold strut filaments. Histological evaluation was performed to compare the bone-bridging process that is associated with each of the tested implant materials. New bone formation and remodeling was observed using a light-inverted microscope (Olympus IX71).
Surgical Approach
An open mini-thoracotomy approach was chosen as the surgical method of choice in this ovine thoracic spine model. Partial lengths of three corresponding rib articulations were removed to create three individual windows at levels T6/7, T8/9, and T10/11. These thoracic windows allowed for direct exposure to the spinal levels mentioned earlier, which facilitated subsequent instrumentation. Instrumented levels were randomized to receive (1) CaP-coated PCL-based scaffold in combination with rhBMP-2, (2) CaP-coated PCL-based scaffold alone, or (3) control (autograft bone from mulched rib head). The following sections describe in a step-wise manner the open mini-thoracotomy surgical approach (i.e., positioning, landmark identification and incision, discectomy, screw placement, stablization of implant, closure of wound, and postoperative care).
Positioning
The sheep was positioned in the left lateral recumbent position in order to present the right hemithorax. The wool over the right hemithorax was carefully shorn to prepare a sterile surgical side according to the following landmarks: caudally from the level of the cranial edge of the pelvic brim to 10 cm above the scapula; and cranially and dorsally from the ridge of the spinous process to the ventrolateral border of the abdomen ventrally. The area mentioned earlier was sterilized with Betadine® solution to provide an aseptic surgical site.
Landmark identification
Landmark identification is crucial in allowing adequate surgical exposure of the ribs and thoracic spine levels of interest. Figure 4 demonstrates a pictorial series demonstrating the open-mini thoracotomy approach to the ovine thoracic spine model. An incision was made, extending caudally from the 13th rib to the 6th rib cranially above the plane of the palpable ventral ridge of the longissimus dorsi muscle as shown in Figure 4a. The surgical reflection of the longissiumus muscle reliably exposes the ribs of the right hemithorax. Following the identification of ribs 7, 9, and 11, careful dissection of the intercostal musculature and neurovascular bundle was undertaken to expose 5 cm lengths of each of the three ribs mentioned earlier (measured from the costovertebral joint) while remaining in the extra-pleural cavity as shown in Figure 4b. Care was taken to protect and preserve the lung parietal pleura at all times. A soft-tipped retractor was used to retract the lung safely from the surgical field. Once exposed, ribs 7, 9, and 11 were resected 3 cm from their corresponding costovertebral joints and removed by disarticulation of the rib heads, thus creating individual thoracic windows as represented in Figure 4c. Once adequate exposure is achieved, discectomy of the intervertebral disc spaces T6/7, T8/9, and T10/11 was undertaken (as described in the section “Discectomy”). Six consecutive vertebral screws were subsequently placed mid-body within the vertebral bodies of T6 to T11 inclusive represented in Figure 4d. The resected ribs were subsequently prepared later in the operation for the designated autograft treatment level by the mulching process as shown in Figure 5.
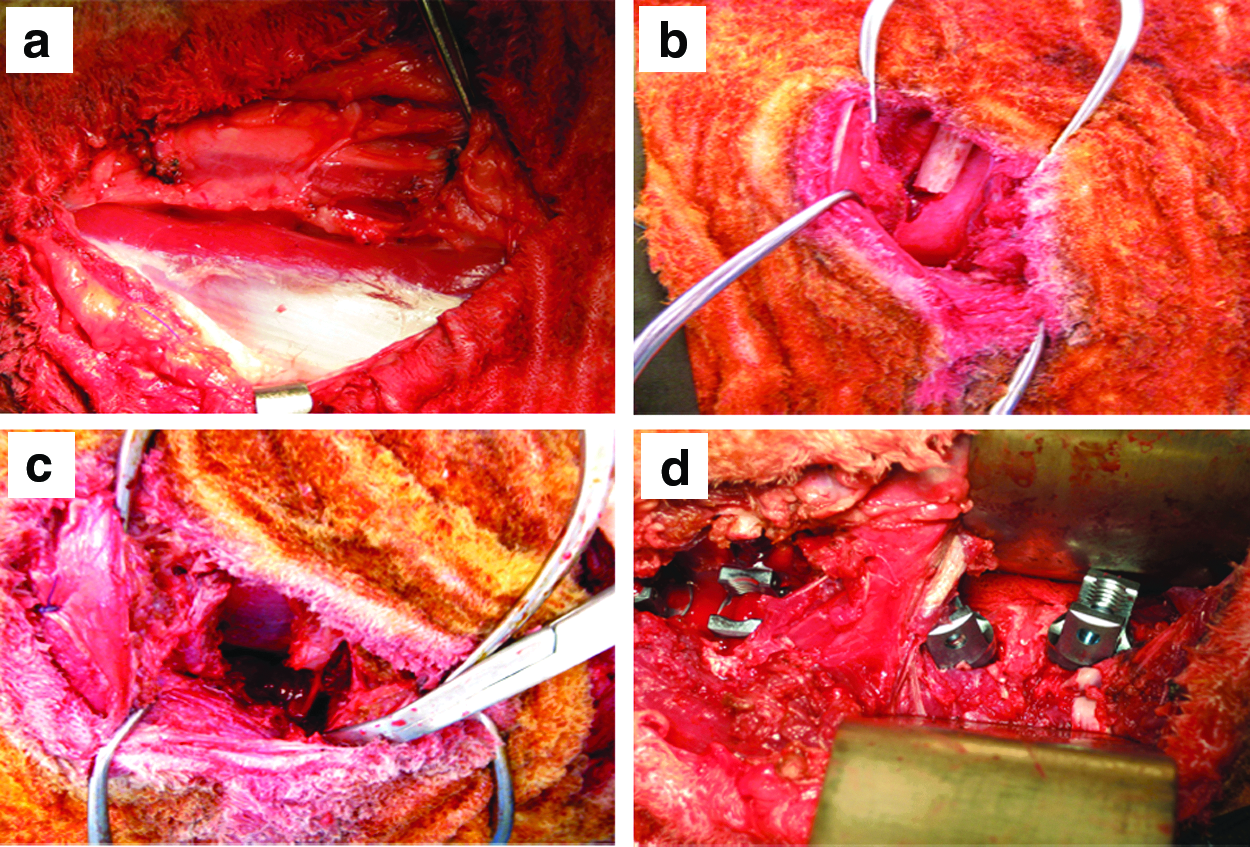
Pictorial series demonstrating the open mini-thoracotomy surgical approach to the ovine thoracic spine model.

The use of resected rib for autograft by a mulching process with orthopedic rongeurs.
Discectomy
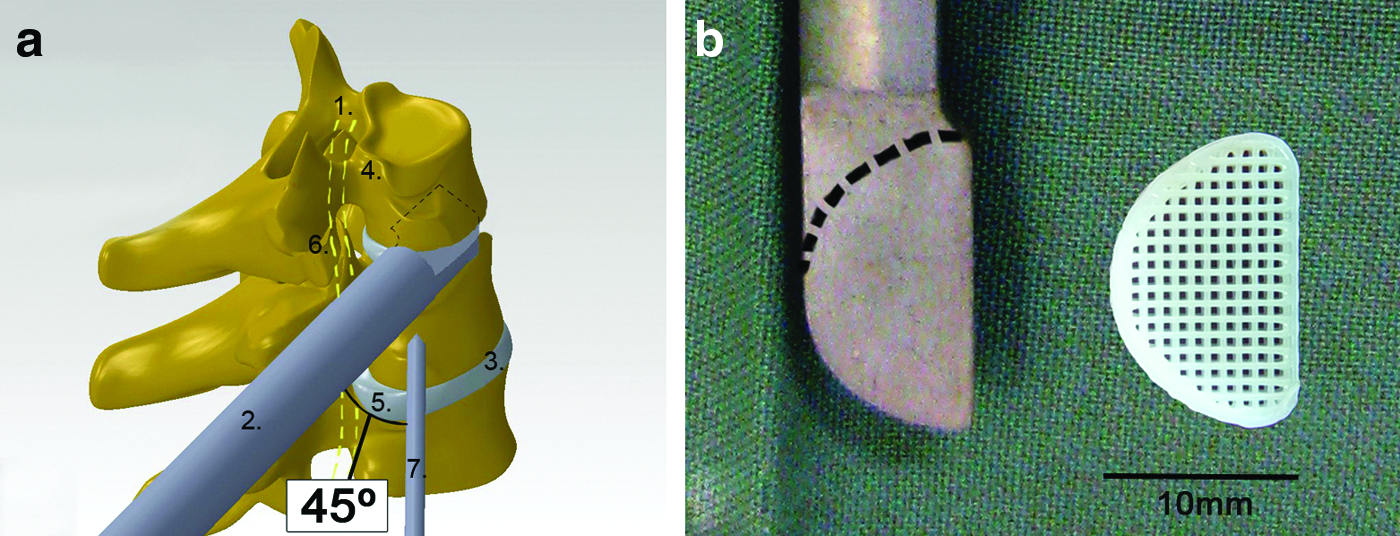
Once the rib heads of T7, T9, and T11 were removed, the corresponding intervertebral discs were exposed. Careful clearance of the intervertebral discs with ronguers was undertaken. A stainless-steel hand-held custom-made spacer device with a tip corresponding to the shape and dimensions of the scaffold was used to ensure adequate anterior disc space clearance in preparation for scaffold insertion as shown in Figure 6. After adequate intervertebral disc clearance, the implantation of either scaffold+rhBMP-2, scaffold alone, or autograft (mulched rib head) was undertaken.
Screw placement
In order to stabilize the implanted grafts within the intervertebral disc spaces, two titanium 25 mm multiaxial thoracic vertebral screws (CD Horizon® M8 multiaxial screws) were placed on the cranial and caudal thoracic vertebrae (on both sides of the vertebral bodies) of the instrumented disc space and secured with a 30 mm-length 5.5 mm-diameter titanium rod. Safe screw placement is crucial as the spinal cord is in close proximity, and great attention was taken to ensure the vertebral screws did not encroach or penetrate this vital structure. A secure construct was created with a mid-vertebral body placement of the vertebral screws, thus providing a stable environment to promote bony fusion. The final technique used for safe vertebral screw placements was developed as a result of numerous cadaveric dissections and mock surgeries.
After adequate intervertebral disc space clearance, the hand-held spacer device was snugly fitted into this space, effectively defining the plane of rotation of the thoracic spine as demonstrated in Figure 6. Segmental vessels in the thoracic spine were spared wherever possible. A defined point on the mid-body of the vertebral body and at the anterior border of the costovertebral joint was then identified. It was at this defined point that a 45° angle was generated ventrally between the fixed hand-piece spacer device and a single 1.6 mm Kirschner wire as shown in Figure 6. A 45° angled trajectory was found to reliably guide a safe mid-body thoracic vertebra screw placement. Once deemed to be satisfactory in both starting point and projected trajectory, a preliminary hole was drilled through the first (near) vertebral cortex and rechecked once more before countersinking with a 3.2 mm drill bit. Keeping to the 45° angle trajectory, a finder tool was used to penetrate through to the second (far) cortex and checked by manual palpation before definitive screw placement. The trajectory of the adjacent vertebral screw was referenced to the safely placed vertebral screw. Six consecutive vertebral screws were subsequently placed mid-body within the vertebral bodies of T6 to T11 inclusive.
Stabilization of implant
Once the vertebral body screws were secured on either side of the cleared disc space, the randomized grafts (CaP-coated PCL-based scaffold+rhBMP-2/CaP-coated PCL-based scaffold alone/autograft) were inserted after disc space distraction as shown in Figure 7. A single 30 mm titanium rod was locked across the two screw heads by tightening the screw caps. In order to provide a consistent torque for screw tightening, an extension of the screw caps detaches as soon as a torque limit is reached, serving as both a safety mechanism and ensuring secure screw cap placement. This process was repeated for all the treatment levels (T6/7, T8/9 and T10/11).
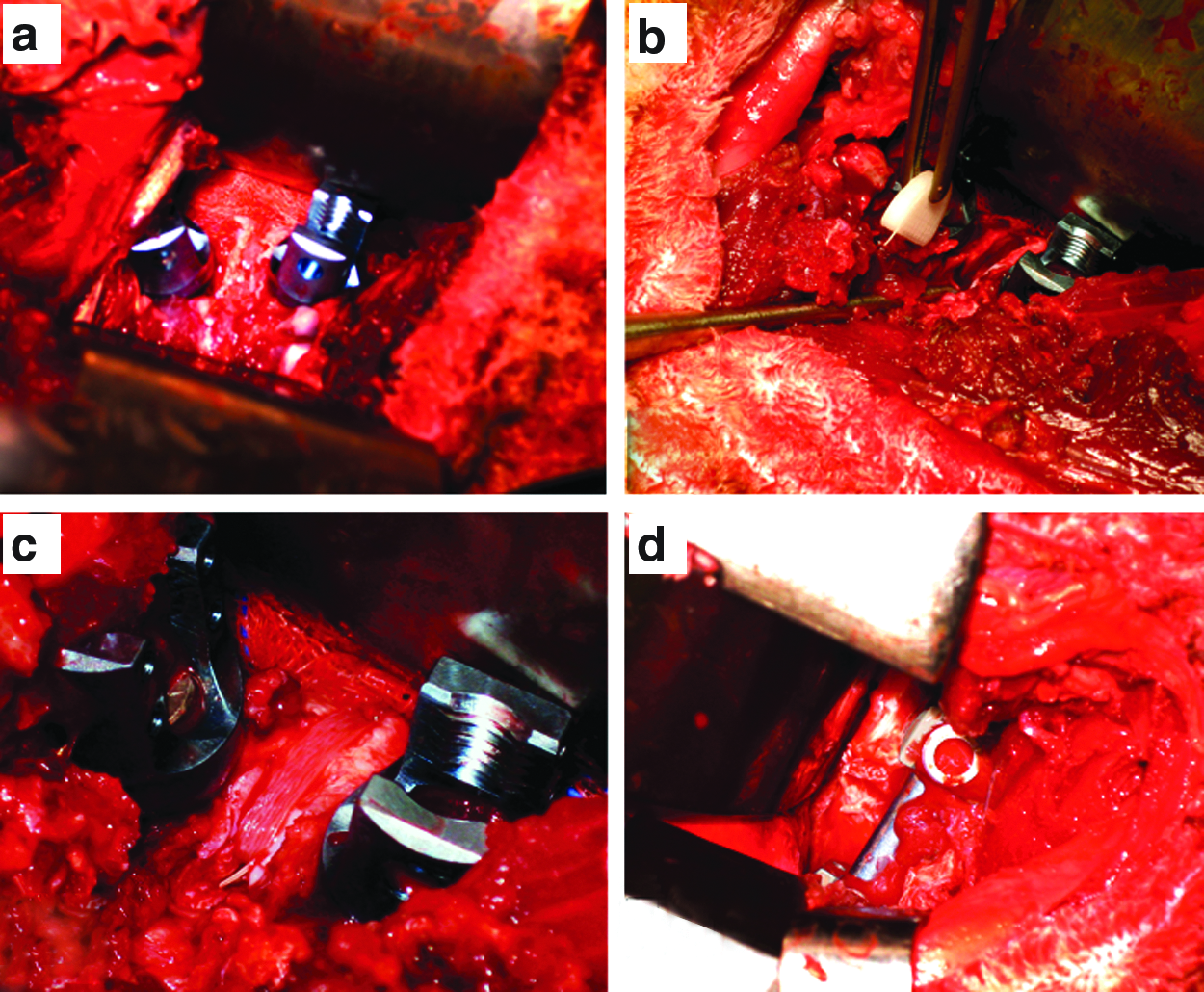
Pictorial series demonstrating the implantation process of a PCL-based scaffold.
Closure of the wound
The surgical wound was closed in layers with absorbable sutures having ensured hemostasis. A temporary indwelling chest drain catheter was inserted within the intrapleural space to generate a negative pressure within the right thoracic cavity to ensure adequate lung re-expansion in the event of iatrogenic damage to the lung pleura. The chest drain was connected to a filling chamber secured temporarily to the side of the animal.
Postoperative care
Each animal was cradled in a custom-built sling for 24-h postoperatively to provide mechanical support to the animal and to alleviate pain. A further two doses of prophylactic antibiotic and analgesia were given to the animal during this time. The temporary indwelling chest drain catheter was removed after 24 h had elapsed postoperatively. The animal was allowed to ambulate freely within the confines of a designated paddock for the next 2 days before release into the common sheep paddock. The sheep were closely monitored postoperatively for signs of pain (i.e., gait abnormalities/teeth gnawing/social isolation) by experienced animal handlers.
On attainment of the timelines mentioned earlier, the sheep were euthanized and subsequently underwent radiological and histological fusion analyses.
Results
All six animals have been successfully operated on, and all animals have gone on to the survival timeline of 6 months mentioned earlier, demonstrating the feasibility of the surgical procedure and postoperative care thereof. The open mini-thoracotomy approach allowed for visualization of the surgical field, and, therefore, facilitated the safe protection of the lung and major blood vessels such as the vena cava and aorta. There were no significant complications in any of the animals treated with this method, and postoperative pain and discomfort were minimal. The sheep were observed to return to near normal patterns of gait and social inclusion within the first 48 h.
The operative time takes on average 4 h with a further 1 h allotted for the save recovery of the animal. The recovery of the animal was facilitated by the use of a custom-built sling, which served to support the standing weight of the animal in the initial 24 h postoperative period. The supported standing weight served to alleviate any pain in this period. In addition, the sling effectively limited the amount of movement afforded by the sheep, therefore reducing the risk of prematurely dislodging the chest drain.
Computed tomography
Typical results seen within the 6-month group demonstrating overall higher levels of radiologically evident bony fusion in the rhBMP-2 plus PCL-based scaffold group in comparison to either the scaffold alone or the autograft groups are shown in Figure 8. Fusion levels for the scaffold plus rhBMP-2 group were comparable to, or slightly higher than, those of the autograft group. Fusion grades were much lower in the scaffold-only group in comparison to either the scaffold plus rhBMP-2 or autograft groups. Radiological assessment of the un-instrumented (nontreatment) levels showed no evidence of bone formation.

Representative reconstructed parasagittal CT images at 6 months demonstrating radiologically evident high fusion levels of
Histology
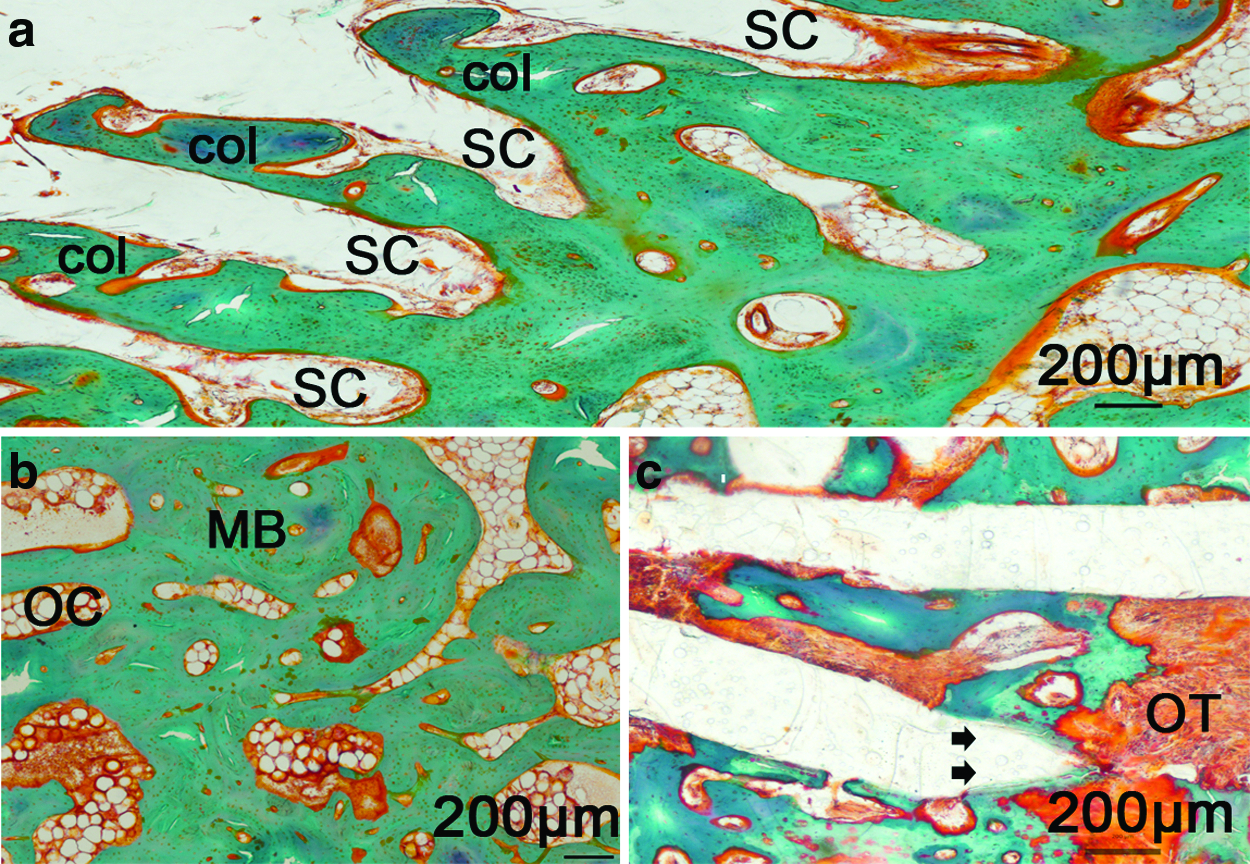
Representative histological evaluation of the 6-month group indicates that in the rhBMP-2 plus PCL-based scaffold group, well aligned columns of mineralized bone have formed in the struts of the scaffold filaments, indicating a high degree of osseointegration of the graft implant and therefore fusion (as demonstrated in Fig. 9a). In the autograft group (as demonstrated in Fig. 9b), there was histological evidence of mineralized bone and osteoclast formation, indicating integration of the autograft bone implant and fusion as with the rhBMP-2 plus PCL-scaffold group. There had been areas of extensive PCL-based scaffold strut graft resorption and evidence of osteoid formation in the PCL-based scaffold-alone group, suggesting a pseudoarthorotic process (as represented in Fig. 9a). This observation is in agreement with that seen radiologically, as there were comparable CT fusion grades between autograft and rhBMP-2 plus PCL scaffold.
Discussion
To the authors' knowledge, there has not been any published literature detailing the establishment of an experimental open mini-thoracotomy approach in a large animal thoracic spine model. This could be due to the fact that large animal spine surgery remains a technically demanding procedure with potentially serious consequences, including severe neurological damage, respiratory distress, and hemorrhage resulting in paralysis or even death if not meticulously carried out. Several animal models have been previously used to study spinal fusion, including anterior or posterior interbody, spinous process, laminar, facet, and posterolateral intertransverse process fusion methods as listed in Table 1.
The close proximity of the spinal cord particularly at the point of placement of the vertebral body screws is a particular concern, as incorrect screw placement with subsequent injury to the spinal cord will result in paralysis. The risk of incorrect screw placements are lessened by following the screw placement trajectory technique utilizing a 45° angle generated ventrally between the fixed hand-piece spacer device and a single 1.6 mm Kirschner wire described earlier. An angle trajectory is utilized to achieve a safe projection of screw placement within bone, as the spinal cord, being within the spinal column, is not directly visible intraoperatively.
The physical size of the thoracic cavity seen with healthy sheep aged 4–6 simulated an environment representative of an adolescent child. Techniques employed for implant fixation correspond to those used in the human patient.6,7
The open mini-thoracotomy approach developed here allows the surgeon to visualize an adequate surgical field, and it also facilitates protection of the lung parietal pleura. Perforation of this structure can result in lung collapse and subsequent fatal respiratory distress. A chest drain can be inserted within this cavity in the event of lung parietal pleura perforation to re-establish a negative pressure environment that is essential for lung expansion and adequate ventilation of the animal.
In addition to protecting the integrity of the lung parietal pleura with adequate surgical field exposure using a mini-open thoracotomy approach, further vital structures, namely the inferior vena cava and aorta, can be visualized and protected, thus preventing iatrogenic damage to these vessels, which could result in severe hemorrhage.
The authors propose that a mini-open surgical technique for the purposes of establishing a research model reduces the inherent morbidities seen in endoscopic techniques previously described. 8 Cunningham et al. 11 compared the interbody spinal fusions between open and endoscopic techniques in a sheep thoracic model and concluded that there were longer operative times, higher estimated blood loss, and increased animal morbidity in the endoscopy group. These complications were attributed to the learning curve associated with this technique as well as the more challenging instrumentation of the endoscopy procedures.
The open mini-thoracotomy approach to the sheep thoracic spine represents a novel technique through which the advantages of the conventional thoracotomy of direct visualization of the surgical site are coupled with the concept of a minimally invasive technique seen with endoscopic procedures. The open mini-thoracotomy developed here is intended to serve solely as a research model and was tailored specifically to the sheep anatomy. Partial rib resection with subsequent rib-spine joint disarticulation were necessary to allow sufficient access and adequate anterior column intervertebral disc clearance that are required to accept the custom-made PCL-based scaffold.
Radiological and histological results at 6-months post surgery indicated that the scaffold plus rhBMP-2 and autograft groups had comparable grades of fusion and evidenced new bone formation. The scaffold alone group, however, not only had lower grades of fusion in comparison to the other two groups but also exhibited osteoid formation, indicating pseudoarthrosis. These results demonstrate the ability of the surgical technique to allow a comparison between different types of interbody fusion constructs in the same animal.
The authors acknowledge that the results described represent a solitary time point (6 months), which, however within the scope of this technical paper, serves as a demonstration of the feasibility of the open mini-thoracotomy technique.
Conclusion
This method paper inaugurates in a step-wise manner a new surgical technique for interbody thoracic spine fusion in a sheep model, which when employed appropriately will serve to reduce the inherent risks of spine surgery in large animal models. The experimental large animal spine model established here will form the platform for further research into various bone tissue-engineering constructs and their fusion-promoting properties, in addition to the specific implant configurations mentioned in this article.
Footnotes
Acknowledgments
The authors would like to thank Maree Izatt, Nabeel Sunni, Cedryck Vaquette, Beau Brooker, Maria-Ann Woodruff, Edward Ren, Kristofor Bogoevski, Flavia Savi, Alan Carstens, and Eugene Verzin for their kind assistance and technical support with the study. In addition, the authors would like to acknowledge the Australian Research Council Future fellowship program of Prof. D.W. Hutmacher for funding a part of the study.
Disclosure Statement
No competing financial interests exist.