
Abstract
This study investigates the effects of seeding a chondrogenic and osteogenic scaffold with a bone marrow-derived cell concentrate (BMCC) and reports the histological and mechanical properties 3 months after implantation in the miniature pig. Twenty defects (7×10 mm) were created in the femoral condyles of 10 miniature pigs. The defects were left empty (E), filled with the grafted cylinder upside down (U) or with a combined scaffold (S) containing a spongious bone cylinder (Tutobone®) covered with a collagen membrane (Chondrogide®). In a fourth group, the same scaffolds were implanted but seeded with a stem cell concentrate (S+ BMCC). The animals were stained with calcein green after 2 weeks and xylenol orange after 4 weeks. After 3 months, the animals were sacrificed, and a mechanical analysis (Young's modulus), macroscopic, and histologic (ICRS Score) examination of the specimens was conducted. Young's modulus in the periphery was significantly lower for group E (67.5±15.3 kPa) compared with untreated controls (171.7±21.6 kPa, p<0.04). Bone defects were smaller in group S (10%±8%) compared with E (27%±7%; p<0.05). There was a trend toward smaller bony defects on comparing groups E and S+ BMCC (11%±8%; p=0.07). More red fluorescence was detected in group S+ BMCC (2.3%±1.1%) compared with groups E (0.4%±0.2%) and U (0.5%±0.2%, p<0.03). ICRS scores were higher for groups S (25.3±3.8) and S+ BMCC (26.2±5.2, p<0.01). In this animal model of osteochondral defects, stem cell concentrates enhance new bone apposition but fail to improve mechanical properties or histological appearance of cartilage regenerates in critical-sized defects.
Introduction
O
Most recent studies have demonstrated benefits of cell seeding on histological and mechanical properties of osteochondral reconstructions.8,9 Other groups could not detect the mechanical superiority of cell-seeded constructs compared with empty scaffolds. 10 Irrespective of whether cells are used or not, reconstruction of the subchondral bone remains the key element to osteochondral reconstruction. 11
In animal experiments, the mini pig has been frequently used to investigate osteochondral defects, as it is known that empty defects of 6×10 mm or beyond cause incomplete defect regeneration within 2 years.12,13 Different biomaterials have been implanted in these defects with or without cells.10,14 In contrast to isolated bone defects, autologous cell-seeded constructs do not improve the histological appearance of the regenerates. 10
For the evaluation of osteochondral reconstructions, histologic and mechanical examination protocols are suggested. 15 Mechanical properties of healthy cartilage and cartilage regenerates have been thoroughly investigated.16,17 The use of equilibrium modulus by creep indentation testing has been used in several animal models, including the mini pig. 10
Histological semi-quantitative scores of osteochondral regenerates have been used within several species to elucidate the effects of osteochondral reconstruction using various biomaterials.10,18
The purpose of this study is to investigate the advantage of seeding a composite osteochondral scaffold with an autologous stem cell concentrate by comparing the histologic and mechanic properties in the mini pig. The hypothesis is that cell-seeded constructs demonstrate equal mechanical and histologic properties as unseeded constructs or controls with empty defects or upside-down implanted bone cylinders.
Materials and Methods
Experimental design
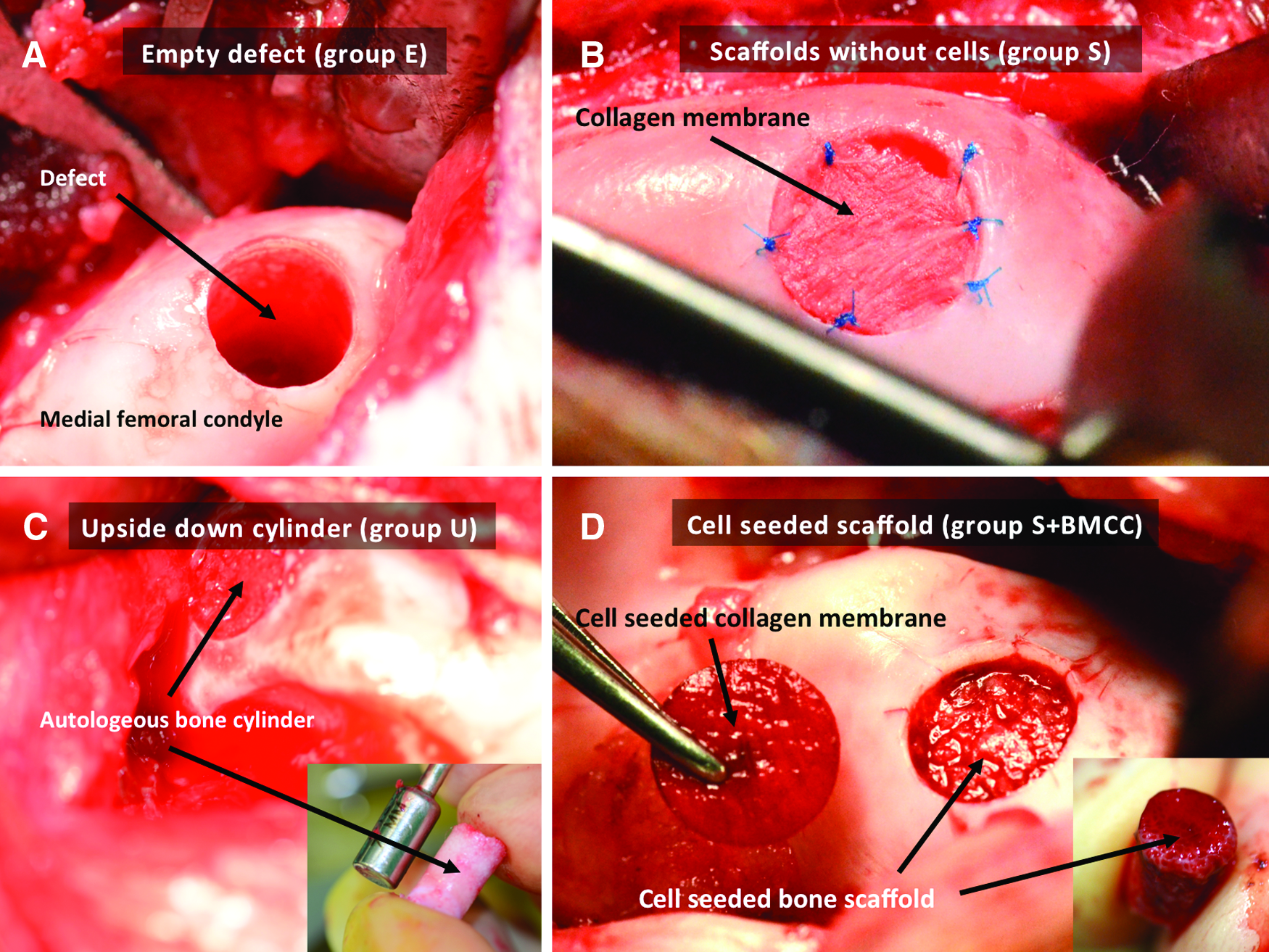
All operations and handling procedures were approved by the local district veterinary administration and complied with the animal protection act. A total of 11 skeletally mature Göttingen miniature pigs of female sex were used (manufacturer: Education and Research Institute Ruthe of the University of Veterinary Medicine Hannover, Foundation, Sarstedt, Germany). The mean age was 14 months, and the mean weight was 58.3±6.7 kg. All animals received a unilateral arthrotomy of the right knee joint. In each knee, two defects (width: 7 mm, depth: 10 mm) were created by an osteochondral articular transplant system (OATS™, Arthrex®, Naples, Florida) in the weight-bearing area of the medial or lateral femoral condyles. A total of 20 defects were analyzed. The defects were assigned to one of the following groups by a computer-generated random list: In group E, the defects were left empty. In group U, the cartilage of the osteochondral cylinders was removed, and the cylinder was reimplanted in the defect upside down. In group S, a xenogenic conical bone cylinder with a minimum diameter of 7 mm and a maximum diameter of 8 mm, a height of 9 mm (bovine origin, Tutobone®, Tutogen Medical, Neunkirchen a. Br., Germany) was impacted into the defect. When the surface of the cylinder was flush with the joint surface, a Luer instrument was used to adjust the surface to the articular concave shape. Then, a plunger was used to insert the cylinder further until it came to rest flush with the subchondral bone. An 8 mm-diameter osteoarticular transplant system (OATS. Arthrex) instrument was used to trim a collagen I/III scaffold (Chondrogide®, Geistlich Pharma, Wolhusen, Switzerland) to a round-shaped patch. The patch was put on the defect and secured by seven sutures using a non absorbable polypropylene (Prolene® 7-0, Ethicon, Johnson&Johnson, Norderstedt, Germany) suture. In group scaffold (S)+ bone marrow-derived cell concentrate (BMCC), the animals received a bone marrow aspiration on the left posterior iliac crest. A Jamshidi aspiration syringe was positioned on the dorsal aspect of the posterior iliac crest and advanced into the intramedullary cavity. After an injection of 2.000 IE heparine, an aspiration and concentration system (Marrowstim®, Biomed, Warsaw, IN) was used according to the guidelines of the manufacturer.19,20 Briefly, 20 mL of bone marrow aspirate were used to create 3 mL of concentrate. The concentrate was transferred in a custom-made cell-seeding device (manufactured by the Institutional Central Research Laboratories of Hannover Medical School (MHH); Fig. 1). The chamber underneath the scaffolds was filled with a dialysis and replacement solution (Gambro Dasco SpA, Medolla, Italy), 21 and it consisted of Na+ 117 mM, Mg++ 0.70 mM, and Cl-117 mM. After 20 min, the chamber was opened, and the scaffolds were transferred into the sterile field. The bone scaffold was advanced into the defect with a pusher. After contouring the surface 2 mm before the final position with a Luer instrument, the cylinders were advanced until the surface of the implants was in line with the subchondral bone. At this point, the cell-seeded membrane was attached with the cell-loaded side facing the implant and attached by 6–7 prolene sutures (size: 7-0 USP; Johnson and Johnson Medical, Brunswick, NJ; Fig. 2). After irrigation, the patella was reattached to the retinaculum with a Mersilene size 0 suture and the joints were closed with a PDS size 2-0 suture. Skin closure was achieved with staples.

The animals were allowed to move freely and were weight bearing as tolerated under analgesia with Ibuprofene (10 mg/kg of body weight/day) for 7–10 days. They were daily monitored for pain, distress, and discomfort and the lameness was scored weekly according to Winkler and Willen. 22 The weight and temperature were protocolled twice per week. After 2 weeks, a subcutaneous injection of Calcein green (Sigma Aldrich Chemical, Taufkirchen, Germany) with 10 mg/kg of body weight was administered, followed by another subcutaneous administration of Xylenol orange tetrasodium (Sigma Aldrich Chemical; 100 mg/kg of body weight) after 4 weeks.
Three months after the operation, the animals were sacrificed, and all soft tissue was removed from the knee joint.
Bone marrow analysis
In order to provide an idea of how many progenitor cells were transplanted, the number of fibroblast colony-forming units (CFU-F) were determined. Although the observed cell colonies were not identified by FACS analysis, the CFU-F has been used before to report the bone marrow characteristics. 6 The number of cells was counted within 1 mL of aspirate and concentrate using a hemocytometer (Sysmex SE-5000 Automated Hematology Analyzer, TOA Medical Electronics, Kobe, Japan). Cells were washed once and resuspended in culture media (DMEM/Ham's F-12 1:1; Biochrom, Berlin, Germany). Density centrifugation was used to obtain a cell pellet that was resuspended in the culture media mentioned earlier supplemented with 10% fetal calf serum, 200 U/mL Penicillin/Streptomycin (Gibco, Karlsruhe, Germany), 2.5 μg/mL Amphotericin B (Biochrom), supplemented with FGF-2 (3 ng/mL; Pepro Tech, Offenbach, Germany) buffered with HEPES buffer (Roth, Karlsruhe, Germany; pH 7.0), and, subsequently, plated in 75 cm2 culture flasks (Nunc, Berlin, Germany) and incubated at 37°C and 5% CO2 in a humidified atmosphere. The medium was changed every 3 days. In a previous study with the same culture media, 23 the fibroblast nature of these cells has been demonstrated using antibodies for collagen I and III and by the up-regulation of tenascin-C. Fibroblast colonies were Giemsa stained and counted using an inverted light microscope at 25×magnification. Any aggregate with at least 50 cells was scored as one colony. The results were expressed as CFU-F per 106 bone marrow cells.
Macroscopic analysis
The regenerated cartilage was examined using the International Cartilage Society (ICRS) Macroscopic Score, which determines the degree of defect repair, integration to the border zone, and the macroscopic appearance 24 (Appendix Table A1). The scoring was done by a blinded investigator from the own Institute (C. L.) and by a blinded, independent observer from a different Institution (A. B.) with assistance of an experienced pathologist (R. F.).
Mechanical characterization
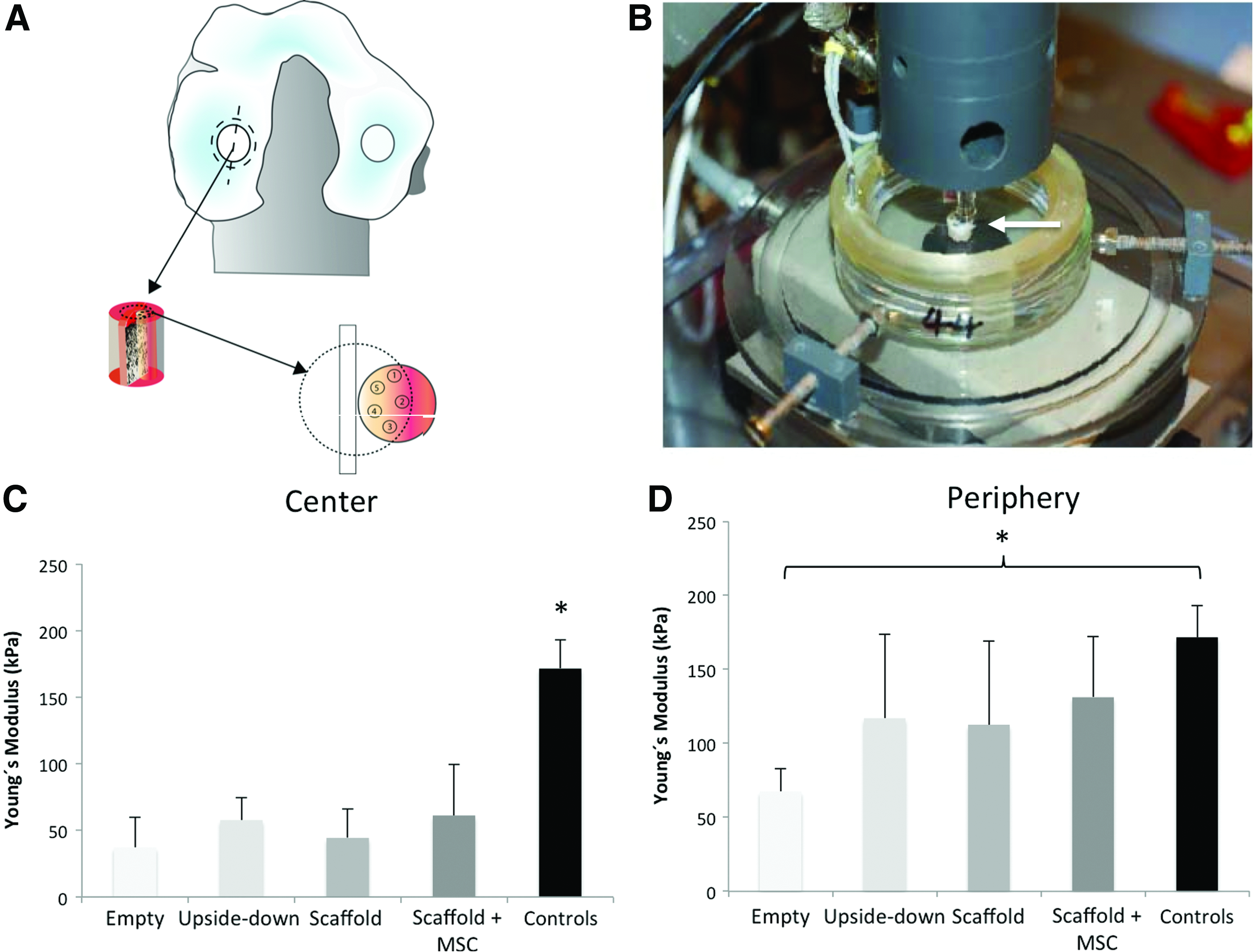
For mechanical characterization, the specimens were tested under creep indentation.17,25 A custom-built creep indentation machine [manufactured by the Institutional Central Research Laboratories of Hannover Medical School (MHH)] featuring a flat-end cylindrical indenter of 1.0 mm diameter was used to apply a force of 0.1 N until a steady-state maximum indentation depth was achieved (Fig. 3). The 10 mm-high cylindrical specimens containing the defect region and peripheral healthy articular cartilage with the underlying cortical and trabecular bone tissue were obtained using 6 mm-diameter tissue punches. The specimens were glued perpendicular to the dish floor. Then, the dish was filled with phosphate-bufferd saline (PBS) until it wet the specimen's upper surface. Three locations were measured in both the defect and healthy cartilage regions The graphical user interface to operate the test was programmed with LabVIEW™ 6.1 (National Instruments, Austin, TX). Creep indentation was first performed, followed by a needle-probe thickness measurement at the identical location; 26 all tests were performed at 37°C in 0.15 M PBS solution. An analytical solution was then applied to derive the Young's modulus assuming the Poisson's ratio of 0.42.
Histology and histomorphometry
The regenerates were split in the longitudinal plane using a micro saw (Martor, Solingen, Germany). Then, cylinders with 8 mm diameter and 10 mm depth were harvested using an osteoarticular transplantation system (OATS, Arthrex, Fig. 3A). Care was taken to ensure the integrity of the other half cylinder. With a 14 mm-diameter OATS instrument, a half cylinder was detached and stored in a 4% paraformaldehyde solution in PBS for 7 days. The samples were embedded in Technovit 9100 New1 (Heraeus-Kulzer, Hanau, Germany) according to the manufacturer's guidelines. 5 μm thin sections were cut using an RM2155 microtome (Leica, Bensheim, Germany) and adhered onto silane-coated slides. Photomicrographs were recorded with a Zeiss Axioskop 40 microscope equipped with a Zeiss AxioCam Mrc digital camera and Zeiss AxioVision software (Zeiss, Oberkochen, Germany).
Collagen II
For collagen II immunohistochemistry, sections were prepared with Xylol, monoethanolamine (MEA), and a series of diluted isopropanol/ethanol. Endogenous peroxidases were removed by treatment with 0.3% H2O2/PBS for 30 min. Sections were blocked for 30 min with phosphate-buffered saline−0.05% Tween20 (PBST) containing 10% goat serum (PBST-S). The sections were incubated with rabbit monoclonal collagen II antibody (Acris Antibodies, Herford, Germany) for 60 min at room temperature. The primary antibodies were diluted to 1:200 with PBS. Sections were washed twice with PBST and then incubated with the secondary antibody (Vectastain ABC Kit; Vector Laboratories, Burlingame, CA) for 30 min. Counterstaining was achieved using Harris hemalaun solution for 3 min. Sections were mounted with Aquatex® (Merck, Darmstadt, Germany). The negative control was prepared with PBST instead of the primary antibody. The ICRS Visual Histological Assessment Scale 24 was used for a semiquantitive analysis of the histological findings (Appendix Table A1).
Quantification of fluorochrome positive/defect areas
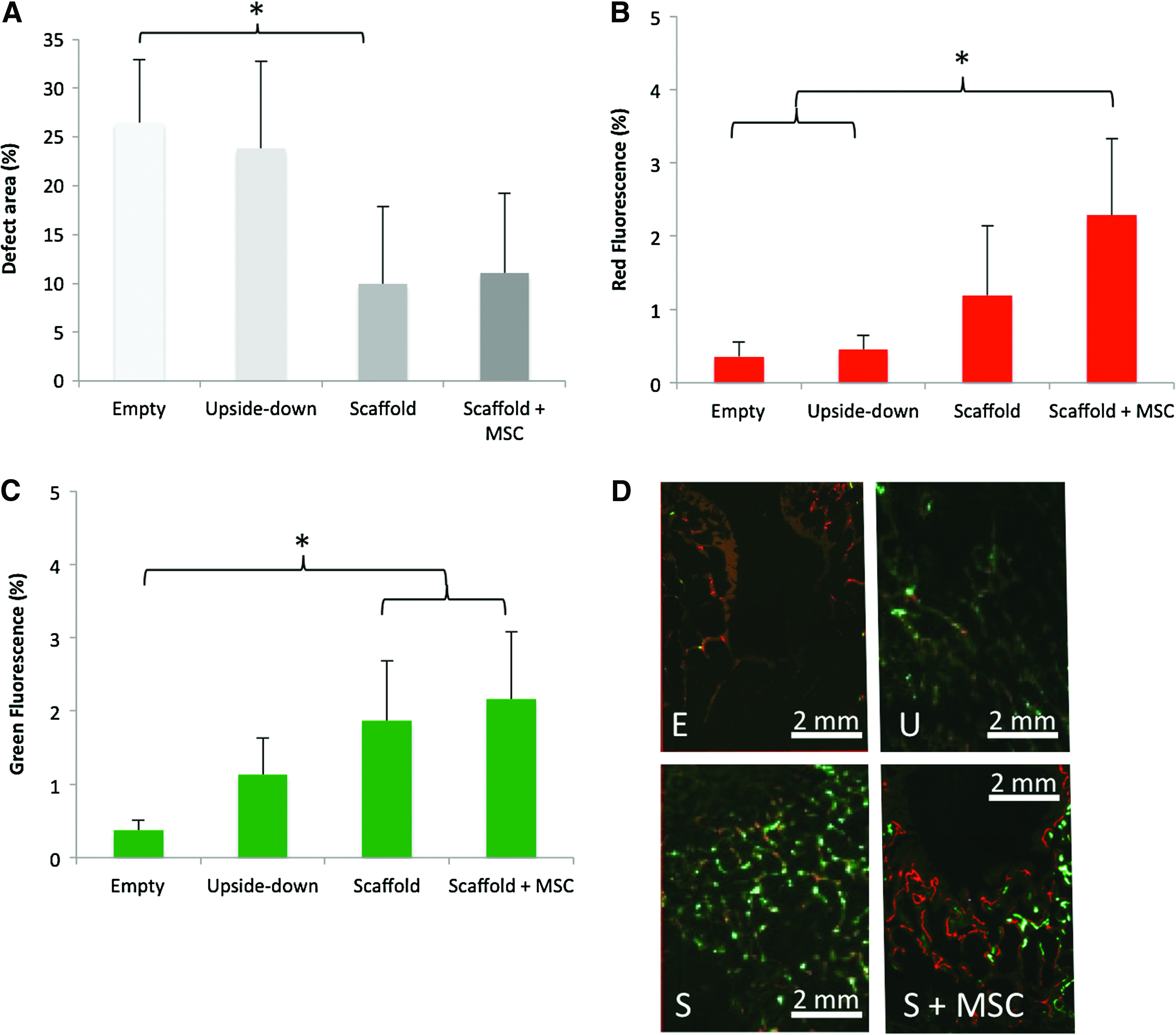
Quantification of fluorescence positive areas was performed using SigmaScan software. A region of interest was set to an area with a width of 6 mm and a height of 8 mm (Fig. 5D), and the fluorescence positive and defect areas are reported as a percentage of the entire area.
Tartrate-resistant acid phosphatase
Tartrate-resistant acid phosphatase (TRAP) is a glycosylated monomeric metalloenzyme that is highly expressed in osteoclasts, activated macrophages, and neurons. 27 TRAP staining was carried out using a manufacturer's protocol (387A-1KT; Sigma Aldrich, Inc., St. Louis, MO). The number of TRAP-positive cells was determined within an area of 8x6mm around the center of the defect (Figs. 6D and 7).


Higher magnification (40×) of the interface of the defect and the bordering bone showing the distribution of TRAP-positive cells. Color images available online at
Statistical analysis
Numerical data are reported using mean values and standard deviation (SD), such as range. Variables were analyzed using analysis of variance followed by Bonferroni's correction for multiple comparisons. Statistical significance was predetermined using a p-value of <0.05. The interobserver reliability was investigated and is reported as κ with a corresponding confidence interval. All statistical tests were computed using SPSS for Macintosh (version 20.0; IBM SPSS Statistics Corp., New York, NY).
Results
There were no wound complications, but two patella dislocations had occurred at final follow up. One animal was unable to walk after 5 days and was euthanized before finishing the study period. It was replaced by another animal receiving the same treatment after receiving consent from the local district veterinary administration. Lameness of the animals gradually improved, and the gait score according to Winckler and Willen 22 at final follow up was 3.8±1.4 (1–5) with no significant differences between the groups (p=0.95).
Bone marrow characteristics
In order to assess the number of cells that were transplanted, bone marrow characteristics were analyzed: An average of 3.1±0.1 mL (2.9–3.3 mL) of bone marrow aspirate was concentrated using the Marrowstim system. The number of nucleated cells counted within the aspirates ranged from 6.5 to 13.4 million/mL, with a mean of 10.7±2.6 million/mL. The mean number of CFU-F per one million nucleated cells obtained from the samples ranged from 30 to 60, with a mean of 46.0±11.0. The characteristics of the concentrates are reported in Table 1. Directly after seeding, the efficacy of the transfer of cells was visualized by Laser microscopy (Fig. 1F, G).
Mechanical properties
As a measure of the stiffness of the osteochondral reconstructions, Young's modulus was investigated. Young's modulus in the center of the defects was determined with 37.3±22.6 kPa (20–69 kPa) for group E, 57.8±16.9 kPa (44–82 kPa) for group U, 44.4±21.9 kPa (27–79 kPa) for group S, and 61.2±38.3 kPa (11–114 kPa) for group S+ BMCC. There was a significant difference in Young's modulus between all experimental groups and the controls (p<0.01; Fig. 3C).
Young's modulus in the periphery of the defects was determined with 67.5±15.3 kPa (range: 50–87 kPa) for group E, 117.0±56.8 kPa (64–194 kPa) for group U, 112.6±56.8 kPa (44–197 kPa) for group S, 131.2±41.2 kPa (94–194 kPa) for group S+BMCC, and 171.7±21.6 kPa (144–190 kPa) for the surrounding untreated cartilage. There was a significant difference in Young's modulus between group E and the controls (p<0.04; Fig. 3D).
Defect healing and evaluation
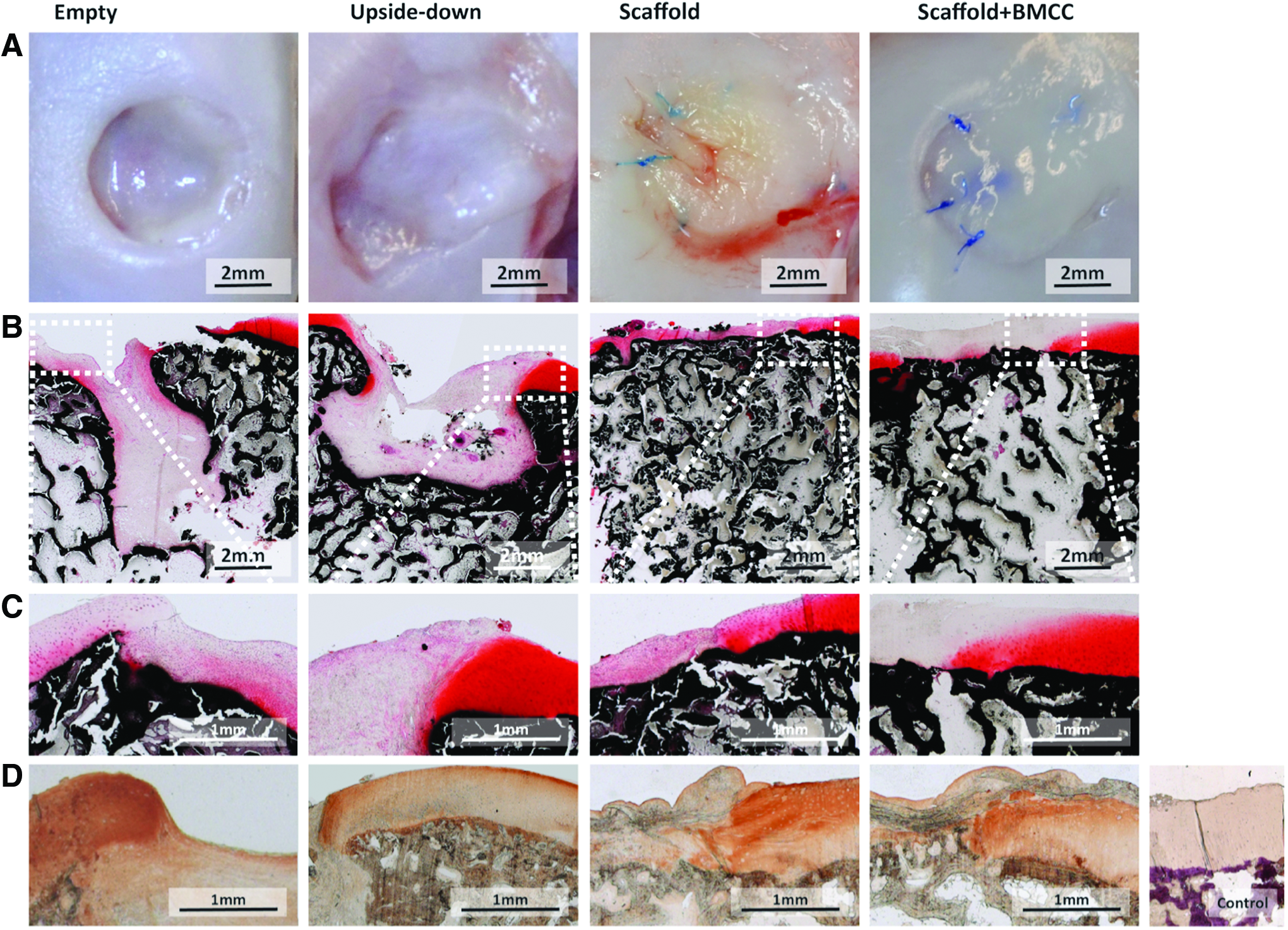
The regenerates were evaluated and scored by two independent observers macroscopically and histologically: Most of the empty defects (4/5) healed with a remaining fibrous cyst without trabecular bone (Fig. 4A, B). There was a gradual change from central fibrous tissue to fibrocartilage in 3 out of 5 specimens and no transition zone into the surrounding healthy hyaline cartilage (Fig. 4C). Macroscopic morphology of the regenerates was more diverse in the group with the upside-down cylinders. A remaining bone defect was found in 3 out of 5 animals. Hyaline cartilage formation was found on the overgrowing edges of the defect (Fig. 4D). In both groups S and S+BMCC, 4 out of 5 defects healed with reconstruction of the underlying subchondral bone plate. There was a transition zone from the regenerate with varying amounts of fibrocartilage into the surrounding hyaline cartilage (Fig. 4D).
The intraclass correlation coefficient was 0.81 (0.56 to 0.92) for the detection of the total defect area, 0.89 (0.84 to 0.98) for the measurements of red fluorescence, and 0.84 (0.63 to 0.94) for green fluorescence between both observers. Due to the high level of agreement, mean values of both observers were used for further analysis.
The area of defect was calculated with 27%±7% (21–34%) for group E, 24%±9% (16–35%) for group U, 10%±8% (0–19%) for group S, and 11%±8% for group S+BMCC. There was a significant difference between the groups (p<0.02). Subgroup analysis showed that there were less bone defects on comparing group E with S (p<0.05) and a trend toward less defect area on comparing groups E and S+BMCC (p=0.07, Fig. 5A).
The amount of red fluorescence staining was 0.4%±0.2% (0.08–0.57%) in group E, 0.5%±0.2% (0.3–0.7%) for group U, 1.2%±1.0% (0.3–2.4%) for group S, and 2.3%±1.1% (1.2–3.3%) for group S+BMCC (significantly higher than in groups E, U, p<0.03, Fig. 5B, D).
The amount of green fluorescence staining was 0.4%±0.1% (0.25–0.55%) in group E, 1.2±0.5 (0.8–1.9%) for group U, 1.9%±0.8% (0.7–2.6%) for group S, and 2.2%±0.9% (1.2–3.3%) for group S+BMCC. There was a significant difference between the groups (p=0.01). Subgroup analysis demonstrated a lower amount of green fluorescence in group E compared with both S (p<0.05) and S+BMCC (p<0.02; Fig. 5C, D).
ICRS and TRAP evaluation
The inter-reader κ for both macroscopic and microscopic ICRS scores was 0.68, which is interpreted as “substantial agreement” according to Landis and Koch Appendix Table A2, Spearman correlation: 0.91 for microscopic and 0.93 for macroscopic analysis, p<0.01). Therefore, the mean values of both observers were used for the exploration of the data. Microscopic ICRS scores were 4.1±1.2 (2.5–5.0) for group E, 6.8±1.2(6.0–8.5) for group U, 8.6±0.9 (6.5–10.0) for group S, and 8.5±2.2(6–11) for group S+BMCC (p<0.01). Macroscopic ICRS scores were 3.4±0.9 (2.5–4.5) for group E, 6.4±2.1 (4.5–9.0) for group U, 8.3±1.4(6.5–10.0) for group S, and 8.7±1.3(8–10.5) for group S+BMCC (p<0.01). There was no significant difference in the overall assessment. However, the ICRS total scores were 13.0±3.2 (10.0–16.0) for group E, 19.4±4.0 (15.5–25.0) for group U, 25.3±3.8 (19.0–28.5) for group S, and 26.2±5.2(18.0–31.0) for group S+BMCC (p<0.01). The scores of group E were significantly lower than those of groups S, S+BMCC (p<0.01; Fig. 6A–C).
The number of osteoclasts was found to be 87.8±63.0 in group E, 69.3±29.1 in group U, 60.0±36.8 in group S, and 47.6±31.9 in group S+BMCC. There was no significant difference between the groups (p=0.53). Representative sections of the defects are displayed in Figure 6D.
Discussion
This study showed that in miniature pigs the healing of osteochondral defects was enhanced in the presence of porous bone scaffolds covered with a collagen membrane. The addition of a bone marrow aspirate concentrate had only a limited benefit on bone synthesis within the scaffold. This is remarkable, as other studies using different cell types such as chondrocytes, osteocytes, adipose-derived stem cells, mesenchymal stem cells (MSCs), transgenic cells, or platelet-rich plasma28–30,33 showed significant benefits for the regeneration of meniscus, 4 cartilage, 31 or bone.32,33 Although it seems that the efficacy of regeneration supporting cells or bioactive molecules is not present in all cases, the benefits of porous scaffolds for stabilizing the defects and for providing a simple matrix for ingrowing cells are repeatedly reported.33–35 Obviously, the material the scaffolds are made of plays only a minor role, as different materials such as beta-tricalciumphosphate, 14 hyaluronic acid, and atelocollagen 10 or a combination of hydroxyapatite and beta-tricalcium phosphate showed comparable effects. Again, there were no general beneficial effects, when these different scaffolds were used along with different cell types. Therefore, our study underscores the limited value of adding cells to the construct when treating a critical-sized osteochondral defect in the weight-bearing area of the knee joint. The reasons for the often limited benefits of co-transplanted cells or of added bioactive molecules such as core binding factor beta (CBFβ), transforming growth factor beta (TGFβ), insulin-like growth factor one (IGF1), or keratogenin (KGN) are not really known, as the fate and the role of MSCs in the host organism is not fully understood. 42 It could be demonstrated that allogenic green fluorescence-labeled BMCC survive for approximately 11 weeks in mice, but the amount of new bone formation synthesized by these cells was very limited.36,37 Transplanted cells usually face a hostile immune system, they lack grown physiological connections with the host tissues, and the supply with nutrition and other factors is problematic. Moreover, the transplanted cells compete directly with mumerous host cell types that are recruited from the organism for the healing process. From this point of view, the benefit of transplanted cells mainly depends on the regeneration capacity of the host organism, which itself is dependent on parameters such as age or tissue-specific properties. Therefore and with regard to osteochondral defects, the most crucial point seems to be a sufficient porosity with a pore size of more than 300 μm and a high interconnectivity that is beneficial for rapid cellular ingrowth.38,39
In a recent study by Boos et al., 35 BMCC were compared with MSC cultured in-vitro and then transplanted in-vivo on a porous tricalcium phosphate ceramic scaffold. The results show that even though there is a clear deficit of MSC in a bone marrow aspirate concentrate, there is no increasing effect of isolating and proliferating MSC on the bone formation and vascularization of the constructs.
The role of MSCs for the regeneration of cartilage is a matter of debate: MSC play a key role during fracture healing, 40 and a transition of MSC into chondrocytes can be achieved both in-vitro 41 and in-vivo. 42 Small molecules such as CBFβ, TGFβ, IGF1, KGN, and more have been identified to trigger chondrocyte-specific gene expression in MSC and to protect chondrocytes in-vitro. 42
In-vitro, mechanical stimulation of MSC has improved proteoglycan and collagen contents of engineered chondrospheres. 43 In-vivo, Jiang et al. reported superior tensile properties of tricalcium phosphate scaffolds seeded with mature chondrocytes compared with empty scaffolds in a similar animal model, 9 but Im et al. found inferior mechanical behavior of osteochondral reconstructions using autologous chondrocytes compared with empty defects and with a biphasic scaffold. 10 Li et al. 44 have compared 8×105 seeded chondrocytes or MSCs and empty defects 6 months after implantation in a swine model and found the highest equilibrium compressive stress of 1.5 MPa in the regenerated cartilage produced by the MSC-seeded constructs. One can hypothesize that we would have found better mechanical properties with MSCs after proliferation, at least at a longer time interval.
The miniature pig was chosen for this study, because there is ample evidence in the literature that 10 mm deep defects exceeding 5.4 mm do not heal spontaneously in this model for approximately 2 years. 13 Even though in this study the diameter of the defects was maximized to 7 mm, there was a large variation in the endogenous healing response. Even in the empty or upside-down cylinder group, some defects healed nearly completely after only 3 months. More complete filling of the defects with less significant differences could be expected for longer observation periods. 14
This study has several limitations: A longer follow up of 1 year would have been desirable. 13 Differences between the groups were small and are likely to have become smaller during further follow up. 14 The group size of 5 is also small but was estimated according to sampling size evaluation before the investigation (Appendix Table A2). Further characterization of the heterogenic constructs at the molecular level creates difficulties due to the wide range of regenerate quality within the defects. The value for the clinical transfer of the data is limited due to the model limitations and the fact that surrounding tissue is mostly less favorable in a pathologic osteochondral defect. 45 For future studies, defined cell numbers with different cell phenotypes are of high interest.
Conclusions
This study shows that filling of osteochondral defects with a porous scaffold decreases the defect size compared with an autologous spongious bone cylinder or if defects are left empty. Additional transplantation of a stem cell concentrate increases local bone synthesis without affecting the mechanical performance or the histologic appearance of the implant. Reconstruction of the subchondral bone remains the key for successful reconstruction of osteochondral defects.
Footnotes
Acknowledgments
The authors wish to thank Ramses Forsyth from the Pathology Department of Ghent, Belgium (
Disclosure Statement
No competing financial interests exist.
Appendix
| <0 | Poor agreement |
| 0.0–0.20 | Slight agreement |
| 0.21–0.40 | Fair agreement |
| 0.41–0.60 | Moderate agreement |
| 0.61–0.80 | Substantial agreement |
| 0.81–1.00 | Almost perfect agreement |