
Abstract
Most of the clinically available decellularized tissues are preserved in a freeze-dried state. Freeze-dried (FD) tissues can be preserved for long term, although a rehydration process is necessary before use. Currently, an immersion method is most commonly used in clinical procedures, but it is difficult for complicated and thick structure tissue rehydration. In this study, we tried to apply a vacuum pressure impregnation (VPI) technique for FD tissue rehydration. The water content of decellularized tissues can reach the water content of native tissues within 30 min using VPI, whereas it took 6 h to reach the same water content using the immersion method. Furthermore, heparin rehydrated aortas by VPI had more heparin release at each time point and therefore appeared more anticoagulant activity. We found that the VPI treatment promotes solution infiltration into materials, achieves complete rehydration of the decellularized tissues, and deep infiltration of heparin into the decellularized tissues, suggesting that VPI treatment could be applied as a rehydration method for biological materials.
Introduction
D
In this study, we propose a vacuum pressure impregnation (VPI) technique to rehydrate FD tissues. VPI has already been used in food and metalic material fields.12,13 In food field application, enzymes and seasoning are added into fruits and vegetables by VPI. 14 VPI treatment is mainly used for filling surface cracks in metal materials such as motors and coils by oils or epoxy resins. 15
There are two processes in VPI treatment, vacuum and pressurization processes. The vacuum process gives effective solution infiltrating into the materials by evacuating air from the materials. After the vacuum process, the materials are pressurized to deeply impregnate the solution into the material.
In this study, we set the first objective as the usage of a VPI method to quickly and precisely rehydrate FD tissues. As the second objective, we attempted to incorporate the functional molecules into FD tissues during rehydration by using the VPI method. The cornea, dermis, and aorta were used as model tissues for the rehydration experiment. The decellularized tissues were FD and used for VPI rehydration. Determining the appropriate conditions for quickly rehydrating decellularized tissues, while maintaining the mechanical property of the decellularized tissues was one of the goals in this study. In addition, a heparin incorporation test into the decellularized aorta was performed for evaluating the VPI.
Materials and Methods
Decellularized tissue preparation
In this study, decellularized tissues were used as model materials. The decellularized tissues were prepared by using a high hydrostatic pressure method (HHP). The porcine eye, aorta, and dermis were purchased from a local slaughterhouse (Tokyo Shibaura Organ Co. Ltd.). The conditions of the HHP decellularization were similar to previous reports.16,17 Briefly, corneas were harvested from eyes and immersed in phosphate-buffered saline (PBS) containing 3.5% (w/v) dextran (molecular weight: 70,000; Tokyo Kasei). After washing, the corneas were packed in a plastic bag with PBS containing dextran. The corneas were pressurized at 980 MPa at 10°C for 10 min using a cold isostatic pressurization machine (Dr. Chef. Kobelco). Then, the pressurized corneas were washed in the EGM-2 medium (TakaraBio, Inc.) containing DNase I (0.2 mg/mL) (Roche Diagnostics) at 37°C for 72 h. The decellularized corneas were preserved in PBS containing 3.5% dextran at 4°C until use. The aorta was trimmed of surrounding tissues and washed in saline. The epidermis and hairs of the dermis were removed using a scalpel and washed in saline. The aorta and dermis were packed in saline, and then pressurized at 980 MPa at 30°C for 10 min. After pressurization, the tissues were washed in DNase I concluding saline (400 U/mL) for 7 days and then 80% ethanol in saline for 3 days. The decellularized tissues were preserved in saline at 4°C.
An FD procedure was performed according to Polak and Pitombo 18 The preserved tissues were immersed in saline for 2 h. The tissues were frozen to −80°C at a rate of 1°C /min and stored over 48 h. The vacuum applied drying was performed at 100 mTorr for over 24 h.
VPI method
The vacuum process was performed by using a stainless steel evaporator (Asone). The evaporator had two cocks, one cock connected to a vacuum pump and another cock connected to a silicone tube to inject solutions. FD tissues were placed in the evaporator, the lid and the cocks were closed. The pressure in the evaporator was controlled by a pressure gauge, and solutions were aspirated to the evaporator through the silicone tube. The vacuum procedure was maintained for 5 min. Next to the vacuum procedure, the pressurization process was performed. The vacuumed tissues were packed in saline in a plastic bag. Hydrostatic pressure was applied using the isostatic pressurization machine. The tissues were pressurized at 10 Pa at 25°C for 5 min.
Evaluation of the saline rehydration of the tissues
Vacuum and pressure investigation
To investigate the effective vacuuming condition, the FD dermis (30×20 mm) was rehydrated by the VPI treatment at each vacuum pressure (−0.01, −0.05, and −0.09 MPa). Saline immersion rehydration was used as a control. The rate of rehydration was evaluated by measuring the uptaken water content of the dermises.
Pigment solution rehydration test
To visualize the water infiltration in the tissues, a pigment solution test was performed. The Toluidine Blue O solution (1%; Wako Pure Chemicals) in saline was used in the test instead of saline. The FD aorta (length: 20 mm) was rehydrated by using the VPI treatment and saline immersion for 30 min, respectively. After each treatment, the aortas were cut at the center (10 mm) and observed as cross sections.
Cornea rehydration and histological staining
FD corneas were rehydrated by VPI treatment and saline immersion for 30 min. The rehydrated corneas were evaluated by a hematoxylin–eosin stain.
Mechanical test of the rehydrated aortas
FD aortas (length: 20 mm) were rehydrated by VPI treatment and saline immersion for (30 and 360 min). Mechanical properties of the treated aortas and original porcine aortas were evaluated as follows: The samples were cut into dumbbell-shaped pieces (15–20 mm long and 2 mm wide). Stress–strain curves were measured with a creep meter RE2-33005 B (Yamaden Co., Ltd.). The stress–strain curve for each individual specimen was analyzed with regard to four parameters; the elasticity of the initial and second regions was analyzed from the stress–strain curve. 19
Heparin solution rehydration of the FD aortas and clotting assay
The FD aorta (length: 20 mm) was functionalized by a heparin solution. The sodium heparin solution (1000 U/mL) was added to the FD aortas by immersion and VPI treatment. The heparin solution-treated aortas were evaluated by Toluidine Blue O staining and clot assay. Clot assay was performed using porcine blood and the Lee-White test. 20 Briefly, the heparin-treated aortas were immersed in saline at 37°C. After given incubation times (1, 3, 6, 9, 12, 24 h), the saline was sampled (100 μL), and then the aortas were immersed in other fresh saline. The sampled saline was added to porcine whole blood (1 mL) at 37°C, at a shaking condition in centrifuge tubes. The clot formation time of the sampled solutions was evaluated every 3 min for 60 min. The clot formation time was defined as the point that the blood surface was not declined with inclining the tube.
Statistical analysis
All data are expressed as mean±standard deviation. Significant differences were determined by analysis of variance followed by Student's t-test and p-values less than 0.05 were considered significant.
Results and Discussion
Rehydration tests of decellularized tissues
Figure 1 shows the water content of the dermis after immersion or VPI treatments in saline. It was clear that with simple immersion, more than 6 h was needed to reach 50% water content; however, with VPI treatment at high vacuum (−0.09 MPa), the dermis was quickly rehydrated to more than 50% in just 30 min. To visualize the solution infiltration into the tissues, Toluidine Blue O solution rehydration was performed. The VPI-treated aorta was sunk in toluidine blue O solution, although the immersion treated (for 30 min) aorta was floated in the solution (Fig. 2A). This figure shows the air remnant in the immersion treated aorta. Cross sections of the middle part of the aortas are shown in Figure 2 B and C. The toluidine blue O solution completely infiltrated the aorta that was treated by VPI. However, the aorta that was treated by immersion was stained at only the outermost edge and innermost edge of the tissue. The central area of the aorta was not wet after immersion for 30 min.


It was found to be important that rehydration of the dried cornea without residual air in the tissue was more difficult than other dried tissue rehydration processes. 21 Decellularized cornea rehydration was compared by using immersion and VPI treatment in saline (Fig. 3). The residual air was observed in the immersion treated cornea, and saline infiltrated about a quarter of the area from the epithelial and endothelial sides. On the other hand, no residual air was observed in the VPI-treated cornea, and the structure of collagen matrices was maintained after rehydration.

Photographs and hematoxylin–eosin-stained sections of the decellularized cornea
Native tissues and tissue-engineered material preservation methodologies have been investigated for many years.22,23 The biomaterials made from native tissues such as decellularized tissues have complicated and dense 3D structures. 24 These structures make difficult the water infiltration into the dried tissues. From the results of this study, it is suggested that the VPI treatment is one of the most effective methods for dried tissue rehydration.
Mechanical test of the rehydrated aortas
Figure 4 shows stress–strain curves of the original aorta and saline rehydrated aortas. Table 1 represents the elasticity of the aortas. The saline immersed aorta (30 min) did not fully rehydrate, so the stress–strain curve was not smooth and elasticity could not be calculated. The VPI-treated aorta and saline immersed aorta (360 min) showed smooth stress–strain curves. The initial region elasticity (up to 0.15% strain) of the aorta was higher compared with the original aorta, and the second region elasticity (from 0.15% to 0.3% strain) was almost the same as that of the original aorta. The second region elasticity of the dried tissues showed the same value after saline rehydration; the value change was considered an effect of the FD procedure. 6

The stress–strain curve of the decellularized aorta, immersion treated aortas, and VPI-treated aorta. ⃞ Original aorta, immersion for 30 min,  immersion for 6 h, and ● VPI aorta.
immersion for 6 h, and ● VPI aorta.
n=3, ap<0.05.
VPI, vacuum pressure impregnation.
Heparin incorporation in the FD aortas by VPI method
To functionalize the FD aorta, heparin incorporation was performed by immersion and VPI treatment. After each treatment, the aortas were evaluated by a toluidine blue O stain. The VPI-treated aorta was clearly stained in all areas of the tissue, while the immersed aortas were slightly stained only in the outermost surfaces of the tissues (Fig. 5). To evaluate heparin release from the aortas, a clot assay was performed. Figure 6 shows the result of the clot assay. Negative control (saline) showed clot formation after 9 min. The heparin solution immersed aortas (30 min, 6 h) showed an anticlot formation elongation after 3 and 6 h from the release test. The VPI-treated aorta prevented clot formation after a 24-h release test. From these results, the VPI treatment is found to be an effective method for drug solution incorporation to the dried tissues and not negatively affected by the heparin anticoagulation property.

Toluidine blue O-stained sections of the immersion treated aorta

Clotting assay of the heparin incorporation aortas.
In conclusion, the VPI method showed advantages for FD tissues rehydration and heparin addition. Using the immersion method for rehydrating the FD tissues, the air in the tissues tended to remain at the center of the tissues because the solution infiltrated around the tissue, which could obstruct the escape of air to the outside (Fig. 7A). This problem was found to be solved by the VPI method. Under a low-pressure environment, there was little air in the FD tissue and the solution easily infiltrated into the tissue without air remaining. 13 As a result, the VPI treatment could quickly rehydrate FD tissues within 30 min (Fig. 7B). In addition, the VPI treatment was found to be effective to append drug into the FD tissues. In the previous work, drug solution infiltration into FD tissue is known/has proven to be difficult. In this study, we found that, because of the differences between the molecular weight and affinity for the tissues, FD tissues simply immersed into the drug solution, the solvents infiltrate into the center of the tissues more quickly than the solutes do. The difference is caused by molecular weight and affinity for the tissues. As the VPI treatment promotes the infiltration of a solution, the difference of the infiltration speed between the solvents and solutes is suppressed. As a result, the homogeneous infiltration of drugs and solute was accomplished by VPI treatment.
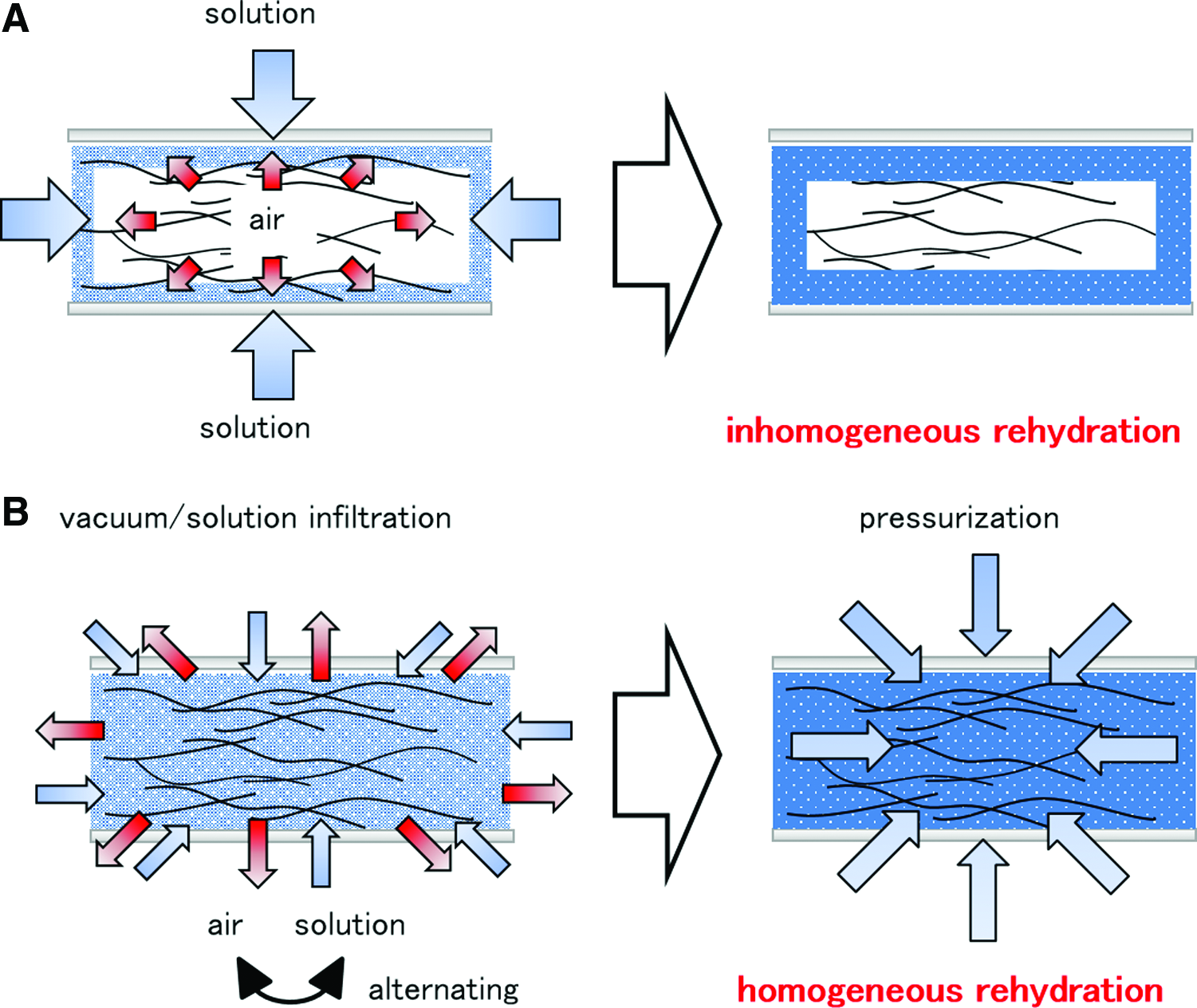
Schematic presentation of the immersion rehydration
In summary, VPI can be an effective method for the rehydration and drug incorporation of FD decellularized tissues, and can be accomplished quickly and easily. The drug solution is quickly infiltrated without air remnants in the tissues, suppressing the separation between the solvents and solutes. In this study, we can propose the feasibility of the VPI as a hopeful methodology for use in medical fields for rehydrating and functioning dried materials.
Conclusion
In this study, we found that the VPI treatment promotes solution infiltration into materials, achieves complete rehydration of the decellularized tissues, and deep infiltration of heparin into the decellularized tissues, suggesting that VPI treatment could be applied as a rehydration method for biological materials.
Footnotes
Acknowledgments
We thank Dr. Toshiya Fujisato for his assistance with HHP machine techniques. This work was supported, in part, by Grant-in-Aid for Young Scientists (B) and the Grant-in Aid from the Japan Society for the Promotion of Science (JSPS).
Disclosure Statement
No competing financial interests exist.