
Abstract
Introduction:
Therapeutic angiogenesis by autologous-peripheral blood mononuclear cells (A-PBMNC) implantation has been shown to be a safe and effective treatment for critical limb ischemia (CLI). We herein report our investigation of the long-term efficacy of implantation of A-PBMNC produced by selective filtration to treat patients with CLI, for which surgical bypass and/or percutaneous transluminal angioplasty are not possible.
Materials and Methods:
This is a prospective, and not a randomized, study based on a treated group who did not respond to conventional therapy (n=43) when implanted with A-PBMNC cells versus a historically matched control group. Patients of both groups were suffering from CLI Fontaine scale IV with chronic ulcers and various accompanying conditions (diabetes, heart disease, kidney failure, etc.). Treated patients were implanted with 12 mL of A-PBMNC, 0.2–0.3 mL for each bolus, collected by selective filtration from 120 mL of peripheral blood in the ischemic area of the limbs. Patients were not mobilized by granulocyte colony-stimulating factor, and the A-PBMNC treatment was repeated for a maximum of three times.
Results:
The A-PBMNC-treated group showed a statistically significant improvement of limb rescue of 95.3% versus 52.2% of the control group (p<0.001), and the result had been maintained for 2 years. The A-PBMNC group also showed reduction in pain at rest, increased maximum walking distance, and healing of the wound, which led to an overall improvement in the quality of life. Post-treatment radiological studies showed an improvement of vascularization with the formation of new collateral and by histological findings. Within 2 years of follow-up, none of the patients whom we treated showed any major or systemic adverse effects.
Conclusion:
The local injection of A-PBMNC showed striking early and long-term effects together with a favorable safety profile, significantly decreasing the risk of amputation. Our results are comparable with published data obtained by injection of bone marrow mononuclear cells, but with a lot less invasive approach. Moreover the intraoperative selective filtration system we used is fast, safe, not operator dependent, and easy to use in a sterile operating theatre. This system aims to produce fresh A-PBMNC as a valuable treatment option, particularly for those difficult patients who cannot undergo revascularization.
Introduction
T
Depending on the seriousness of the case, peripheral vascular pathologies do not respond frequently and sufficiently to conventional treatment such as drug therapy, percutaneous transluminal angioplasty, and vascular surgery. This means that 50% of cases are subject to therapeutic amputation, especially in situations of ischemia of the limb.2,3
Due to the difficulty in finding a solution, all specialized branches are focused on new care strategies to avoid solutions that are highly debilitating for the patient and to save the limb. 4 Over the last decade, research has focused its efforts on new care strategies and cellular therapy from different autologous sources (bone marrow, cord blood, peripheral blood, and adipose tissue) in peripheral vascular disease, obtaining positive clinical results.5–7 These can be included in the category of medicine and regenerative surgery, not only in the sense of repairs to damaged tissue but also in the broader sense with the true regeneration of that tissue. 8
The cell population in question is the autologous-peripheral blood mononuclear cells (A-PBMNC) isolated from peripheral blood. Recently, it has been demonstrated that these cells have the same differentiating and regenerating capacities as the bone marrow mononuclear cells (BMMNC).9,10 In addition, they are able to speed up tissue repair by means of neoangiogenesis, collagen deposit, and reepithelization.11–14
The A-PBMNC implant increases angiogenetic cytokine production in the muscle cells. An angiogenetic cytokine deficit in the muscle cells prevents the implanted cells from creating angiogenesis.9,15–18 This would suggest that the interactions between the cytokine and the messenger molecules released by the A-PBMNC activate the amplified release of angiogenetic cytokines by the muscle cells through a paracrine mechanism and activate the satellite stem cells in the muscle.9,10,15
Our study aims at demonstrating the therapeutic efficacy of A-PBMNC of patients with CLI and various accompanying conditions through a new selective filtration and cell concentration system, in which compliance is high for both the patient and the surgeon.
Materials and Methods
Patients and study design
We collected data based on a prospective, and not randomized, study based on a treated group implanted with PBMNC versus a historically control group.
Between 2011 and 2013, 43 patients aged 19–95 years, 25 male and 18 female, suffering from CLI (Fontaine scale IV) with chronic ulcers (Texas Wound Classification 1-C/3-D) shown in Table 1 and various accompanying conditions (diabetes, heart disease, kidney failure, etc.) shown in Table 2 who had not responded to conventional therapy, including nonsurgical and surgical revascularization (Table 3), were treated with the A-PBMNC implant (A-PBMNC group). For the historical control group we collected data from 43 patients, age-matched, with same comorbidities, treated with minor and major amputations, revascularization, saphenectomy, autologous-platelet-rich plasma (A-PRP), and dermal/epidermal graft as the treated group shown in Table 3.
Median (range).
Percentages are calculated on the overall number of previous treatments (n=97).
The treated patients signed informed consent documents, both to be included in the study and to undergo the procedure. All such studies should conform to the World Medical Association Declaration of Helsinki (1975). This study is part of a project approved by the University of Rome, Tor Vergata.
Inclusion criteria
Our trial included all the patients displaying signs and symptoms of CLI complicated by chronic ulcers. These patients may or may not have been subject to previous revascularization, major or minor amputation, or have suffered accompanying conditions in the past. Patients suffered CLI (level 4 La Fontaine scale) and chronic ulcers (Texas Wound Classification 1-C/3-D).
Exclusion criteria
Patients with malignancy within 10 years; patients with coagulation disorders; patients who are undergoing chemotherapy or immunosuppression, or have undergone such processes within the last 5 years; patients who have undergone radiotherapy in the zone subjected to surgery in the last 5 years; patients with ongoing systemic infection; patients with severe alteration of the liver and kidney function; HIV and hepatitis A, B, and C-positive patients.
Preoperative examinations
Both groups of patients were monitored in accordance with our protocol, which involves the general assessment of the patient through the following tests: blood chemistry (including preoperative complete blood count and procedures for the assessment of the cell concentration), arterial and venous Doppler tests, magnetic resonance angiography (MRA) or computed tomography angiography (CTA) with contrast agent (CA), swabbing the wound, biopsy of the lesion, and photographs of the various operating stages. All the patients undergo an advanced pre- and postoperative cycle of medication aimed at local cleansing and improvement of the lesion and surrounding area. Before proceeding with the treatment, an informed consent form is also completed in agreement with our transfusion center.
Clinical patients' evaluations
The initial assessment of the patients in both groups (T0) included:
• measurement of the dimensions of the ulcer (Ø of ulcer reepithelialization: percentage of reepithelialization [REEPIT]) • assessment of rest pain scale (RPS) on a subjective visual scale, in which 0 means no pain and 10 means irrepressible pain on the Visual Analogic Scale (VAS) • assessment of the maximal walking distance (WD) on a scale from 1 to 5, using the Skinner–Gardner protocol:
The scores are as follows:
1 for WD<200 m 2 for 200 m<WD<300 m 3 for 300 m<WD<400 m 4 for 400 m<WD<500 m 5 for WD>500 m
• assessment of limb rescue (LR). We also investigated the accompanying conditions, surgical operations undergone before our trial, and any major or minor amputations after the trial.
The procedure was repeated for at least three treatments, held at an interval of roughly 45 days from each other (T1, T2, and T3).
This enabled us to record the ulcer healing percentage (Ø of ulcer reepithelization: REEPIT), RPS, WD, and LR 45 days after each surgical session (T1, T2, T3, T4). We performed follow-up examinations 2 years after treatments and also monitored adverse effects.
A-PBMNC procedure and implants
A-PBMNC were collected by the WB Pall Celeris System (CE marked under the 93/42/EEC Medical Devices Directive). This is the only system in the market that enables us to work with selective filtration without the need for specific machinery. The system is aseptic and sterile and can be used to produce the A-PBMNC directly from 60 to 120 mL of peripheral blood taken in the operating theatre in less than 15 min.
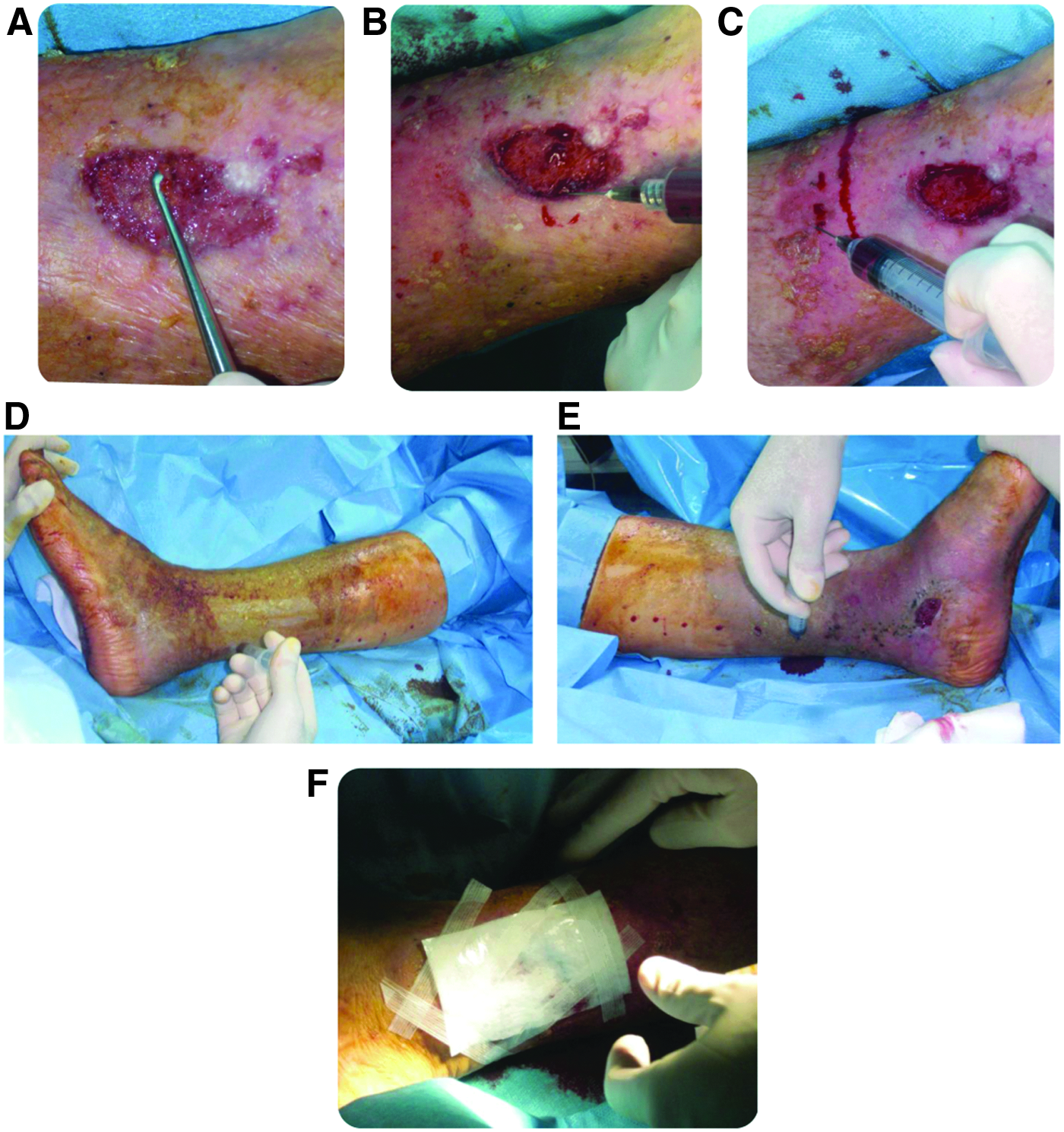
The filter can be used for the collection of peripheral venous blood and subsequent concentration of the autologous circulating mononuclear cells (A-PBMNC) by filtration. The system is fast (the process takes 15 min), safe, aseptic (disposable materials), and noninvasive (venous blood is taken), and easy to use in a sterile operating theatre (three phases). It consists of a blood collecting bag, a selective adsorption filter, a bag for the collection of the mononuclear cells, and a bag for the disposal of the separated blood. Around 60 to 120 mL of peripheral venous blood is taken with anticoagulant ACD-A, and the system is transferred to the upper bag (Fig. 1A). The system is suspended from a stand and the blood flows through the membrane of the selective filter, which retains the total nuclear and mononuclear cells through a process of adsorption (Fig. 1B). The residual blood is conveyed to the bag downstream of the filter and discarded. The filter is then back-flushed with 12 mL of saline solution (Fig. 1C), and the concentrated mononuclear cells retained by the filter are recovered to obtain a cellular A-PBMNC suspension of around 10 mL in the collecting bag (Fig. 1D). The cell concentrate is ready for infiltration in boluses of 0.2–0.3 mL each (Fig. 1E).

Procedure:
A cell yield of mononuclear cells (MNC) >85% is obtained from 100 mL of peripheral blood; 200 million MNC are concentrated from 120 mL of peripheral blood. The maximum enrichment of MNC and reduction of granulocyte contamination is obtained through recovery with 10–12 mL of saline solution.
A-PBMNC treatment protocol
The group of treated patients underwent the following protocol:
- Preoperatory: the wound bed is prepared through advanced medication using materials suitable for the removal of the necrotic tissue and cleansing, stimulation, and regeneration of the tissue, depending on the type and state of the wound. - Operatory A-PBMNC implant: patients were admitted in the hospital on a normal treatment basis (a two-night stay). In the operating theatre, we took 120 mL of peripheral venous blood from a dedicated access point and added 12 mL of ACD-A (anticoagulant by apheresis). This was then processed by the WB Pall Celeris system to obtain 12 mL of concentrated A-PBMNC. Sedation and/or local anesthesia then takes place to facilitate infiltration of the concentrate.
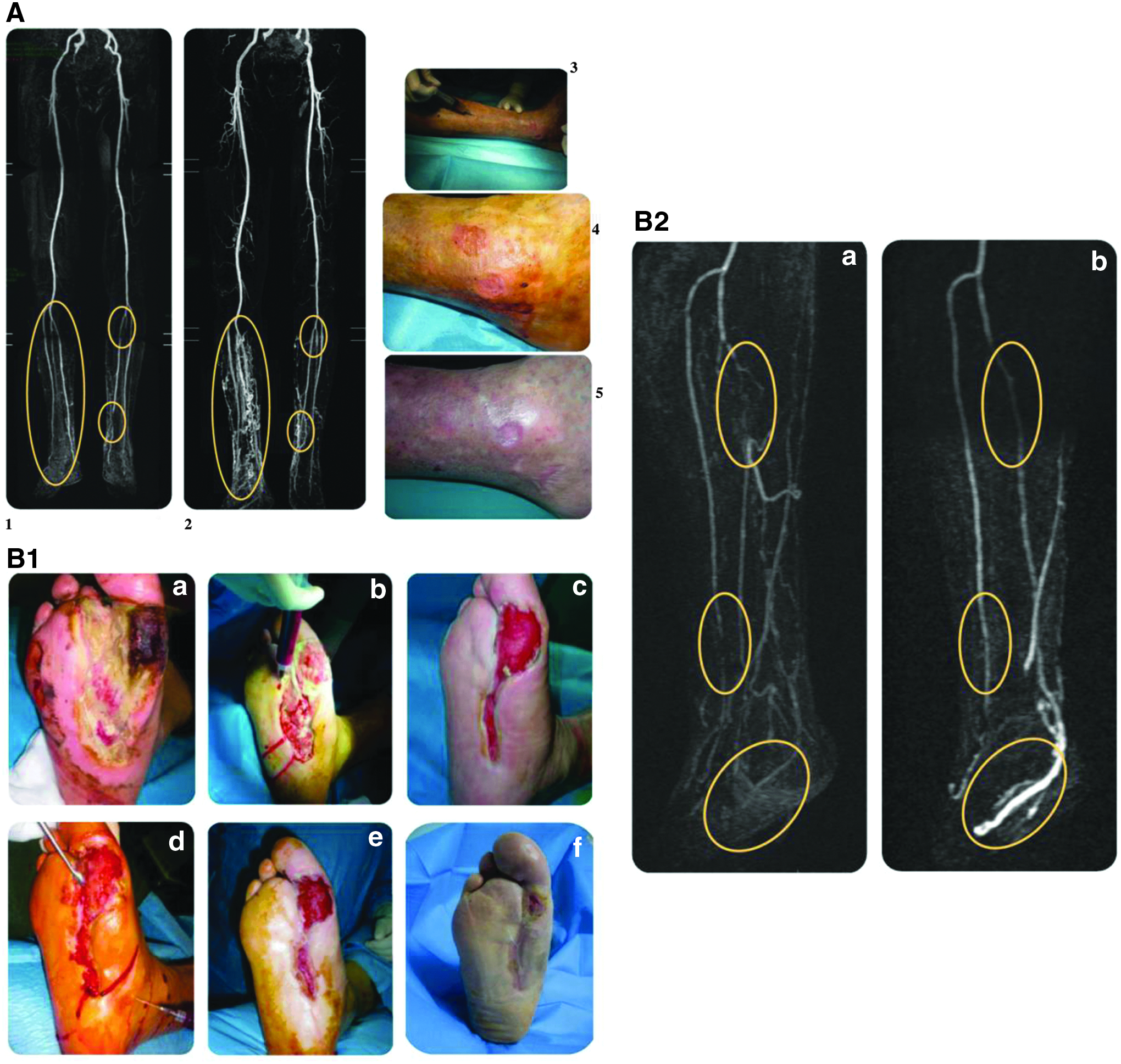
After appropriate surgical cleansing of the wound bed (Fig. 2A), we carried out multiple local, intralesional (Fig. 2B), and perilesional (Fig. 2C) intramuscular injections of our suspension (0.2–0.3 in boluses) along the relevant axis, at intervals of 1–2 cm and to a mean depth of 1.5–2 cm, using a 21G needle (Fig. 2D, E). After the A-PBMNC implant, the wound was always covered with hyaluronic acid medication (Hyalomatrix® PA; Fidia Farmaceutici) (Fig. 2F).
Operative time:
- Postoperatory: treatment with antibiotics and subcutaneous anticoagulants, and the patient is encouraged to return to daily functional mobility on the basis of his or her abilities.
- Postoperatory monitoring: advanced weekly medication in accordance with requirements.
MRA or CTA with CA at 6 months after the first A-PBMNC implant.
All our patients were subjected to standard medication with expanded polyurethane, to be replaced as required, during the intervals between the A-PBMNC treatments.
This procedure is repeated for three treatments at intervals of 45 days from each other.
Subjective and objective assessment tests.
Histological evaluation
Incisional punch biopsies (3 mm in diameter) of ulcers were obtained at baseline (T0), after two A-PBMNC treatments (T2) and at the end of treatments (T4). Microscopic evaluation of routinary hematoxylin–eosin-stained paraffin sections 19 was performed to verify the healing process.
Immunohistochemical study
For immunohistochemistry, 20 4-μm thick serial sections were deparaffinized, rehydrated, and after antigen retrieval and nonspecific peroxidase blocking, incubated with mouse monoclonal anti-human CD31 and CD68 (DakoCytomation), 21 and images were acquired by using a digital camera (E600 Eclipse; Nikon).
Statistical analysis
Mean and standard deviation and ranges were computed for summarizing the results. Subjects who were not tested because amputation occurred did not contribute to averaging data after their amputation. Despite the fact that this study was not a randomized controlled trial, we have also compared the data obtained in the group treated with A-PBMNC with data obtained in the control group (A-PBMNC: 64.61±16.96 years old, control group: 63.21±10.08 years old, p=0.666, t-test) previously treated in a conventional manner.
Mann–Whitney U-test has been used for comparing data between groups. Kaplan–Meier plot was done for reporting the percentage of salvaged limb in the group treated with A-PBMNC and the control group along time. Comparisons of peripheral blood data pre- and postfiltration were evaluated using the nonparametric Wilcoxon's signed-rank test.
Data were collected and reviewed in Microsoft Excel, and statistical analysis was performed using SPSS 16.0 (SPSS, Inc.). All two-tailed tests with a value of p<0.05 were considered statistically significant.
Results
The A-PBMNC-treated group showing a striking improvement of LR was 95.3% versus 52.2% of the control group, showing an increasing percentage of +43.1% (T4). The 95.3% of subjects with limb salvage remained unvaried also at T5, 2 years after the surgery. Conversely, in the control group, the percentage of subjects with salvaged limb was 52.2% at the end of the trial (T5). Figure 3 Kaplan–Meier graph shows the percentage of subjects with salvaged limb along the observation times (T4). The group treated with A-PBMNC showed 4.7% of subjects immediately amputated, but without other subjects being amputated along the period of observation. On the other hand, in the control group, the percentage of subjects needing amputation progressively increased up to 48.8% at the end of the trial. The seriousness of the initial conditions of all 43 patients, most of whom had accompanying conditions as shown in Tables 1 and 2, and the assessment scales that we used would inevitably have led to amputation of the limbs, affecting a good percentage of the patients if no revascularization operations using traditional surgical methods had been possible.
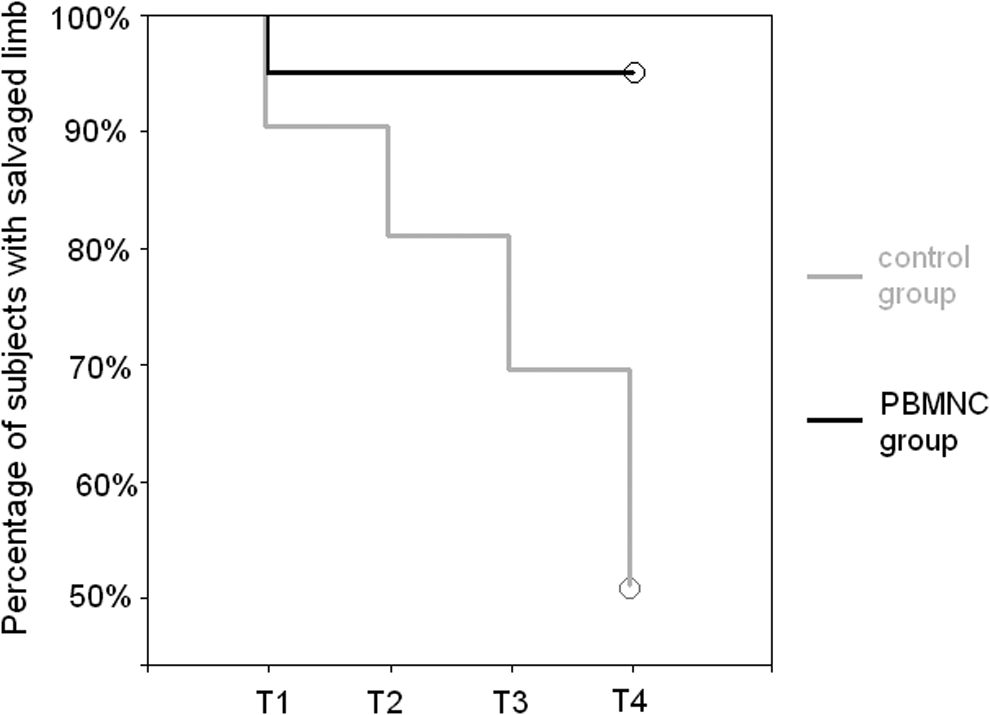
Kaplan–Meier plot of the percentage of cases with salvaged limb for the PBMNC group (black line) and the control group (gray line).
Only 2 of the 43 patients treated underwent amputation after A-PBMNC implants. However, one of these two sustained amputation following the interruption of the treatment, as he went to a center other than ours.
The other clinical parameters observed as shown in Table 4 and Figure 4 also showed a strong improvement in the A-PBMNC group after each treatment.
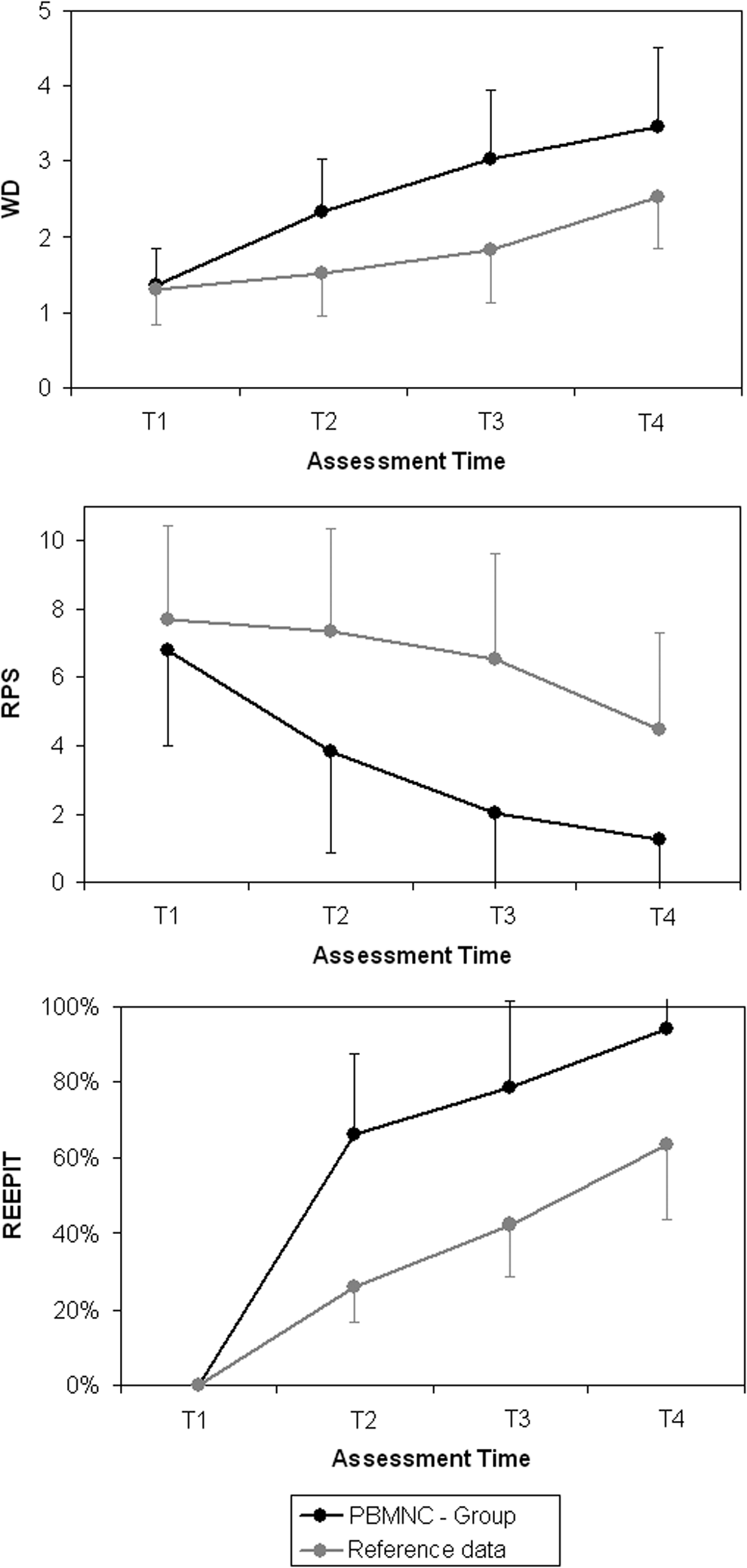
Mean and standard deviation of WD (above), RPS (in the middle), and REEPIT (below, in this graph we used T1 as baseline for all subjects) for the treated group data (black) in respect of reference data (gray) for the four assessment times. REEPIT, percentage of reepithelialization; RPS, rest pain scale; WD, walking distance.
Indicates a higher statistical significant difference.
Indicates a statistically significant difference.
PBMNC, peripheral blood mononuclear cell; REEPIT, percentage of reepithelialization; RPS, rest pain scale; SD, standard deviation; WD, walking distance.
Figure 4 shows an improved trend of the A-PBMNC group for WD, RPS, and REEPIT after each treatment with respect to the control group. WD and REEPIT were similar at T1 between the two groups, confirming the uniformity of the patients in both groups, and then improved significantly (p<0.001 T2–T3 and p<0.05 T4) in the A-PBMNC group (Table 4). The results obtained in terms of reduction of pain at rest, increased maximum WD, and healing of the wound led to an overall improvement in the quality of life for the patient after only the first operating session.
Despite the fact that our protocol consisted of three repeated cell implants, the number of sessions undergone depended on the improvement in the clinical condition of each patient; 8 patients underwent one A-PBMNC treatment only, 16 patients underwent two treatments in total due to the positive clinical outcome, and 19 patients only underwent three treatments in total.
Finally, in the A-PBMNC cellular concentrate, we observed a significant increase in lymphocytes, monocytes, and MNC postfiltration (p<0.001), but no change in platelet concentration (p=0.338) (Fig. 5).
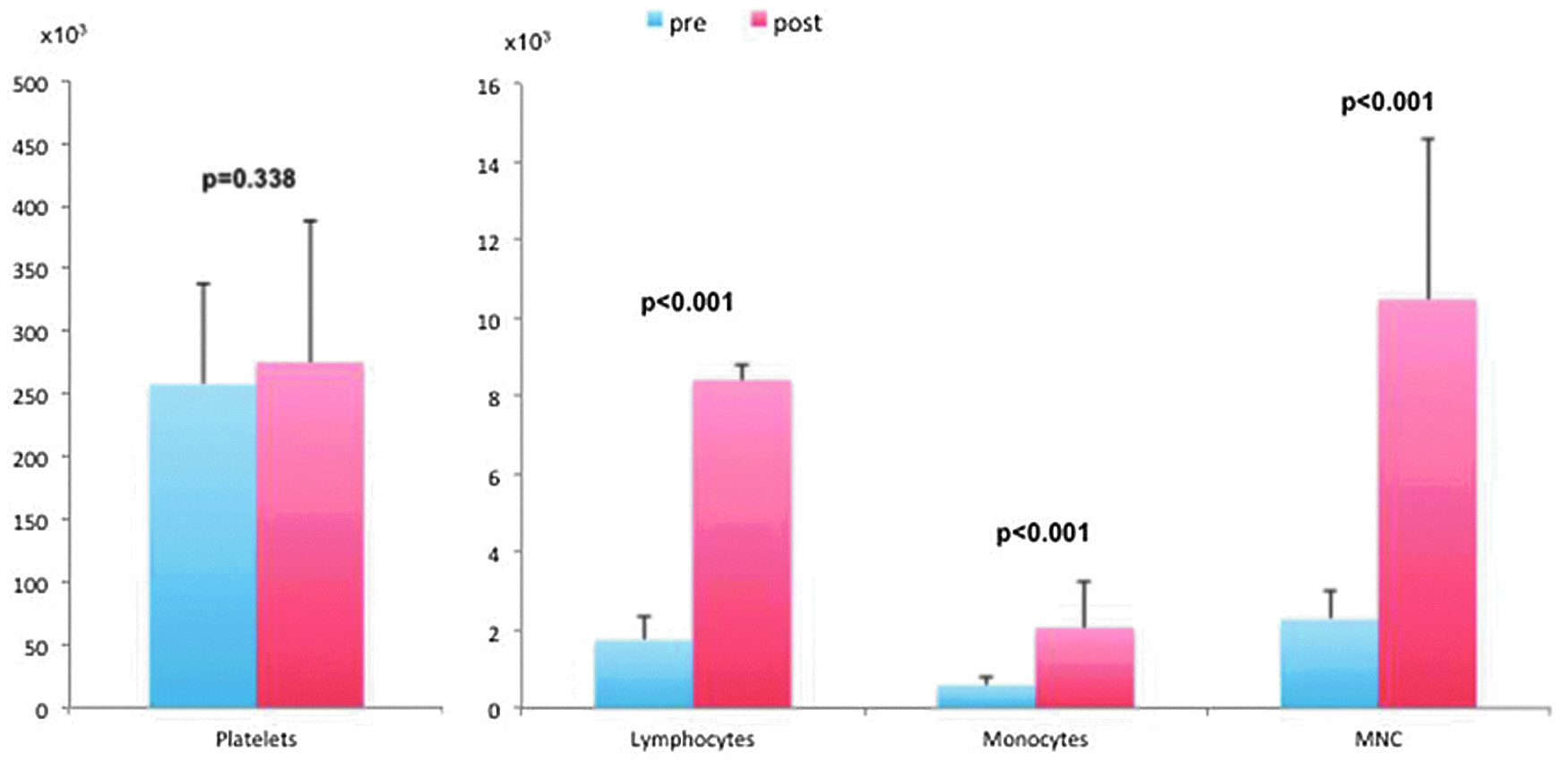
Peripheral blood analysis pre- and postfiltration. Cell count shown on Y-axis.
The total number of implanted cells for each patient (12 mL) was 125.65×106 and standard deviation was 49.63×106.
The main result is that the improvements obtained continued in the course of time.
In a follow-up of 2 years after the procedure, none of the patients whom we treated showed any major or systemic adverse effects. The only minor effect was pain in the period immediately following the operation (24–48 h), which was well tolerated by all the patients and could be controlled by minimum dosages of analgesic when required.
Microscopic evaluation
Representative microphotographs of hematoxylin–eosin staining are reported in Figure 6. A progressive healing of ulcers was documented in T2 compared with T0, and almost complete healing was observed in T4 biopsies. During T2 treatment, dermal granulation tissue displayed an increased number of monocytes (CD68+) and newly formed micro vessels (CD31+). After the A-PBMNC treatment in the underlying healed epidermis, the presence of the new vessels still persisted, whereas dermal inflammation and monocyte infiltration were highly reduced.

Microscopic aspects of chronic ulcer before, during, and after the treatments with A-PBMNC. Representative microscopic images of baseline (T0) skin punch biopsy showing the typical fibrin clot with cellular debris. During A-PBMNC treatment (T2, after two treatments), dermal inflammatory infiltrate rich in monocytes (CD68+ cells) and newly formed vessels (CD31+) are clearly evident. After A-PBMNC treatment (T4), skin punch biopsy shows complete healing with reepithelialization and the presence of residual dermal vessels, whereas dermal monocyte infiltrate is strongly reduced. Original magnification,×100. A-PBMNC, autologous-peripheral blood mononuclear cells; H-E, hematoxylin–eosin staining.
Imaging evaluation
The clinical results are supported by the postoperative examinations after 6 months from the first treatment, which were obtained using imaging methods (angio-CT or angio-MR with CA). Contrast densities were similarly obtained under identical imaging conditions. In Figure 7(A, B1, B2, C, D), the MRA/CTA showed a striking increase in the number of visible vessels and peripheral recanalization of double stenosis (Fig. 7A2, B2b). MRA of the treated group confirmed the formation of new collateral vessels due to the angiogenic capacity of A-PBMNC.
Clinical cases.
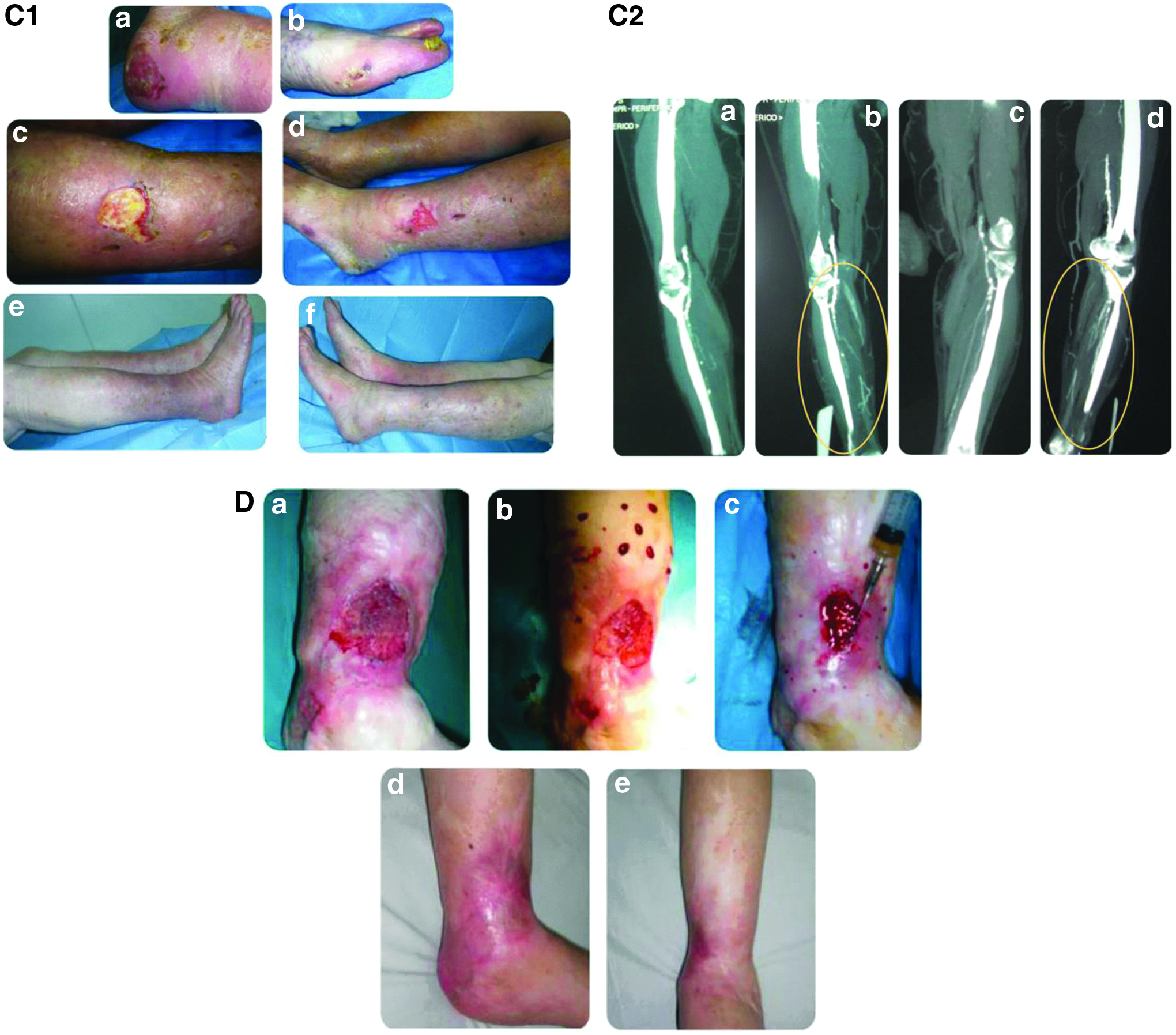
Figure 7 show the results after three treatments in four different patients with different comorbidities.
In these patients (Fig. 7A5, B1f, C1e, f, Dd, e), we obtained complete wound healing with excellent results in terms of skin quality, elasticity, and aesthetic satisfaction by patients.
Discussion
Cell therapy is an innovative and promising approach for the regeneration of damaged tissues. In particular, new scientific evidence shows the total mononuclears from peripheral blood as cells with high angiogenic and vasculogenic capacity and, in general, in tissue regeneration processes. Mononuclear cells, often indicated in scientific literature as peripheral blood mononuclear cells (A-PBMNC) are represented by the class of monocytes/macrophages and lymphocytes. Patients with CLI who suffer from rest pain, nonhealing ischemic ulcers, or necrosis (Fontaine III–IV) rarely respond to standard therapy as drug therapy (e.g., prostaglandine, anticoagulant etc.) and surgical revascularization (e.g., Stent implant, by-pass etc.) and are at high risk of limb loss and serious possible fatal vascular events. 22
The types of therapeutic cells used till date have been BMMNC,23,24 A-PBMNC,4,9,23 granulocyte colony-stimulating factor (G-CSF)-mobilized (M)-PBMNC,25–29 CD34-antigen-positive mononuclear cells,30,31 and CD133-antigen-positive cells. 32 Although BMMNC or M-PBMNC intramuscular implantation has been used most often, both therapies have some risks; to collect about 150–500 mL of BMMNC, general anesthesia of about 4 h duration is necessary, and to collect A-PBMNC, about 3 h of apheresis with G-CSF treatment is required.23–29
Various clinical trials have demonstrated that the transplant of A-PBMNC to induce angiogenesis and healing of injuries in ischemic tissues can be a successful new cell therapy for diabetic patients with critical ischemia of the limb.33–38 In addition, the literature also presents trials on critical patients, who could not be revascularized and were destined for amputation, treated with A-PBMNC obtained through apheresis, Ficoll, or mobilization with G-CSF, in whom the reduction of the percentage of amputations, reduction of the ulcer, pain at rest, an improvement in the WD, and also in the ankle–brachial index are shown.39–41
The effects of the A-PBMNC can be superimposed on those of the BM-MNC in tissue regeneration and neoangiogenesis. Retrieval of A-PBMNC is safer, less invasive, and less expensive.9,42,43 To date, A-PBMNC could only be concentrated with apheresis, with and without mobilization with G-CSF. The retrieval of A-PBMNC with apheresis requires specific costly equipment and is, however, longer and more invasive with respect to our method. In addition, this technique does not always allow the use of fresh cell concentrates because it processes 2–3 L of blood at a time, obtaining a consistent rate of cell concentrate that cannot be completely used in a single session. This is why the remaining part must be frozen for use in subsequent applications, worsening the properties and reducing the effectiveness in subsequent use. Furthermore, not all patients can be subjected to treatment with G-CSF because of the possible appearance of systemic problems such as toxicity and serious side effects, which do not justify the method because of the low risks/benefits ratio. In the final analysis, seeing that the correlation between the number of CD34+ and angiogenic effectiveness has not been demonstrated in vivo, mobilization is not necessary. 41
Another system that can be used to obtain A-PBMNC is Ficoll, which can only be used under a sterile hood and not directly in the operating theatre with the additional limitation of only being certificated for research and not for clinical use.
Autologous-peripheral blood mononuclear cells
It has recently been shown that A-PBMNC are able to create vasculogenesis through the local breakdown of the extracellular matrix and a chemotactic effect that facilitates the penetration of progenitor cells resident in the tissue. These new formations turn into perfectly operational complex vascular structures (vessels).44–46
It has also been shown that A-PBMNC and, in particular, circulating monocytes are powerful with high plasticity multiprogenitors able to differentiate into different types of tissues (endothelium, neurones, cardiomyocytes, osteoblasts, chondroblasts, adipocytes, and myoblasts) according to the tissue in which they are infiltrated, showing an ability that can be superimposed on mesenchymal bone marrow. Circulating monocytes CD14+ differentiate as a result of soluble factors released by the CD14− and through the connection with fibronectin or a substrate of collagen. 47 Kuwana et al. 48 had already identified a monocyte-derived cell population (monocyte-derived mesenchymal progenitors [MOMP]) in 2003, which expresses a strong mesenchymal differentiating ability. These cells infiltrate into the site of the lesion, adhere to the fibronectin, and are subjected to factors released by the surrounding cells and the lymphocytes differentiating into MOMP. Subsequently, the MOMP differentiate into tissue-specific cells in response to organ-specific stimuli given by the surrounding cells. In this process, the monocytes take part in the homeostasis of the damaged tissues regenerating them. In addition, it has been observed in vitro that both the CD34+ and CD34− cells, subpopulations of A-PBMNC, are necessary for the formation of new vessels. 49 By definition, CD34+ cells belong to the hematopoietic branch, but correlation between the regenerative and vasculogenic ability of the A-PBMNC and the number of CD34+ in this cell concentrate has not been demonstrated. 41
The great plasticity of the monocyte–macrophage cells can be inferred from their marked sensitivity to small changes in the tissue microenvironment. They can be activated through a process defined as polarization in accordance with two types of programs as follows:
• M1 (classic inflammatory activation), activated by bacterial molecules (e.g., LPS) and inflammatory cytokines (e.g., IFN-γ); • M2 (alternative activation), activated by anti-inflammatory cytokines (e.g., IL-4 and IL-10 and TGF-β), immune complexes, or glucocorticoids.
In the initial stages of the inflammatory process, the M1 polarization of the macrophages, which promote the inflammatory response eliminating the invader microorganisms, is activated. During the inflammatory stage of resolution, the macrophages are repolarized in the direction of M2, losing the reactivity to inflammatory stimuli and assuming the ability to eliminate damaged cells and tissues and, in particular, promote angiogenesis and tissue remodeling. 50 The local effect of the A-PBMNC injections may be amplified by using A-PRP at the local level, especially in the event of infections that are multiresistant to antibiotics, as we experience in chronic ulcers treatment.51–53
The angiogenic factors secreted by these cells are responsible for the effectiveness of this cell therapy.54,55 These cells can also be found in peripheral blood56,57 and contribute to physiological and pathological angiogenesis in the adult.58,59
Recently, Seta and Kuwana 47 have also shown that circulating monocytes are multipotent progenitor cells, which are able to behave like mesenchymal bone marrow. They are able to differentiate into other types of cells when implanted in the right environment and show great angiogenic ability. This fact also concurs with the angiogenic and vasculogenic ability and is demonstrated in vitro and on animal models. 44
Today, neoangiogenesis is described as angiogenesis, vasculogenesis, and arteriogenesis (formation of collateral circulation) when together, each being a different aspect of an integrated process. Angiogenesis consists of the formation of thin structures coated in endothelium with muscle walls made of smooth muscle and pericytes. These vessels have an important role in the repair mechanisms of damaged tissues. Vasculogenesis is regulated by growth factors such as VEGF or angiopoietin-1 and receptors, including VEGFR-1 (FLK-1), VEGFR-2 (KDR or FLK-2), or Tie-2 tyrosine kinase. 60 Hematopoietic stem cells are defined as CD34+ AC133+, CD34− AC133+, or CD34+ AC133−. CD34+ cells extracted from bone marrow or peripheral blood can be manipulated to form different cell lines. For example, when cultivated ex vivo with VEGF, the CD34+/AC133+ cells differentiate into endothelial cells, while nonfractionated hematopoietic mononuclear cells supply angiogenic cytokine and stem cells that are incorporated into collateral vessels by neoangiogenesis. 38
In diabetic and vasculopathic patients, neoangiogenesis is compromised by the difficulty of proliferation, adhesion, and incorporation of the peripheral circulation of endothelial progenitor cells, a subpopulation of A-PBMNC.33,61,62 Ischemia generally induces the formation of collateral vessels through the migration and proliferation of the endothelial cells from the pre-existing vessels.63–67
The results of our clinical study show the effectiveness and safety of the A-PBMNC obtained with the selective filtration system in patients with CLI and chronic ulcers. In particular, the new device permits the cellular retrieval of A-PBMNC in a simple, minimally invasive manner with extremely rapid enrichment times (<15′), obtaining highly vital and functional cells. The results obtained suggest that the A-PBMNC are a new cell therapy with high angiogenic ability in the treatment of patients with CLI and chronic ulcers.
These data were confirmed by histological evaluation of skin punch biopsy that clearly showed new formed vessels (CD31+) and complete healing and reepithelization of ulcers. Moreover, the improvement of neoangiogenesis is confirmed in postoperative imaging (CTA/MRA) after the A-PBMNC treatment.
For the first time, our trial made use of the WB Pall Celeris System in surgery for the development of clinical care protocols for pathologies of this kind, reducing healing and hospitalization times. In addition, the high level of satisfaction experienced by our patients is demonstrated by the reduced percentage of amputations with an LR of about 95% versus 50% of the control group according to data published. 39 The same satisfaction was also demonstrated by the reduction in RSP, increased WD, and the healing or high percentage of reepithelization of the chronic ulcer in our study according to previous literature.41,68,69
Conclusion
Our work demonstrates that the use of the filter is simple, fast, and enables a high yield of vital and functional cells (technical specifications of the WB Pall Celeris™ System). It is a disposable device, which requires no dedicated instruments or materials, and responds to the safety and sterile procedure requirements.
This method requires no centrifuging, maintenance of the equipment, or even specific personnel. The surgeon is able to carry out the procedure quickly and completely independently using a fast, effective, sterile, and disposable method to obtain the quantity of cell concentrate necessary for the procedure when this is needed.
The procedure is also less invasive and painful for the patient than the traditional methods, and the cell enrichment times are significantly reduced (15 min as against the current 3 h). Obviously, all of these also translate into considerable reduction in cost.
The A-PBMNC are a new cell therapy for the regeneration of high vasculogenic ability of tissue for the treatment of patients with chronic ulcers associated with autoimmune and other pathologies of an ischemic (also LR), vascular, diabetic, post-traumatic, or burn basis. The high level of compliance obtained with this new filter is indicated in all branches of regenerative surgery,47–70 including orthopedics, and also due to the fact that there is no need to suspend any ongoing personal drug treatment.
The continuation of our trials in the area of regenerative surgery with the assistance of cell therapy would suggest that these innovative techniques could be tried out in a variety of pathologies, which are difficult to treat at the present time as autoimmune diseases.
Our study showed a superior benefit of the A-PBMNC treatment of CLI also in diabetic patients with other comorbidities when compared with standard therapy.
Footnotes
Disclosure Statement
None of the authors has a financial interest in any products and in any other devices or drugs mentioned in this article. No funding was received for the research reported in the article.