
Abstract
Current biomedical imaging tools have limitations in accurate assessment of the severity of open and deep burn wounds involving excess bleeding and severe tissue damage. Furthermore, sophisticated imaging techniques are needed for advanced therapeutic approaches such as noninvasive monitoring of stem cells seeded and applied in a biomedical 3D scaffold to enhance wound repair. This work introduces a novel application of combined ultrasound (US) and photoacoustic (PA) imaging to assess both burn injury and skin tissue regeneration. Tissue structural damage and bleeding throughout the epidermis and dermis till the subcutaneous skin layer were imaged noninvasively by US/PA imaging. Gold nanoparticle-labeled adipose-derived stem cells (ASCs) within a PEGylated fibrin 3D gel were implanted in a rat model of cutaneous burn injury. ASCs were successfully tracked till 2 weeks and were distinguished from host tissue components (e.g., epidermis, fat, and blood vessels) through spectroscopic PA imaging. The structure and function of blood vessels (vessel density and perfusion) in the wound bed undergoing skin tissue regeneration were monitored both qualitatively and semi-quantitatively by the developed imaging approach. Imaging-based analysis demonstrated ASC localization in the top layer of skin and a higher density of regenerating blood vessels in the treated groups. This was corroborated with histological analysis showing localization of fluorescently labeled ASCs and smooth muscle alpha actin-positive blood vessels. Overall, the US/PA imaging-based strategy coupled with gold nanoparticles has a great potential for stem cell therapies and tissue engineering due to its noninvasiveness, safety, selectivity, and ability to provide long-term monitoring.
Introduction
S
Dramatic expansion of the tissue-engineering field during the past two decades has demonstrated the clinical feasibility of regenerative approaches for burn treatment. Among numerous promising materials and strategies in tissue engineering, stem cell-based therapies, in combination with 3D hydrogel systems, may serve to improve skin tissue regeneration. In particular, the therapeutic potential of adipose-derived stem cells (ACSs) has been proved both preclinically and clinically for regenerative medicine and dermatological plastic surgery.1,2 ASCs in culture exhibit multipotency showing differentiation into various cells such as adipocytes, chondrocytes, myocytes, and osteoblasts.3,4 ASCs express a variety of mesenchymal surface markers, including CD29, CD90, and CD105, similar to bone marrow-derived mesenchymal stem cells. The mechanism of ASCs contribution toward neovascularization during wound healing may include direct stem cell differentiation, but the role of paracrine secretion promotes angiogenesis and limits inflammation. ASCs have been shown to exhibit a vascular progenitor-like phenotype and to promote angiogenesis1,5,6 and can be induced, in vitro, to express an endothelial cell-like phenotype and function under the influence of physical and chemical cues.4,7
A key question for both stem cell biologists and clinicians is how implanted stem cells behave with regard to host cells and the microenvironment within injured tissue. A challenge to answer this question is that stem cells delivered to an injured site are difficult to accurately track without terminal histological analysis. In addition, clinically applicable imaging modalities for stem cell-based tissue engineering are still limited, and, thus, there is no effective clinical methodology to noninvasively and selectively demonstrate both stem cell localization and regeneration in the injured site over time. Hence, various advanced imaging modalities to track stem cells use exogenous contrast agents such as dyes, metallic nanoparticles, and genes.8,9 However, there is no single imaging system that is capable of simultaneous stem cell tracking and examination of burn injury depth and blood perfusion.
In this article, we introduce such an imaging system and approach—ultrasound (US)-guided photoacoustic (PA) imaging system augmented with gold nanoparticles. US imaging is based on the detection of US waves reflected from tissues and, as such, US imaging can provide anatomical images at reasonable depth with high spatiotemporal resolution. PA imaging is based on the irradiation of tissue with an electromagnetic pulsed wave followed by the detection of acoustic waves generated through conversion of absorbed energy into pressure transients on thermoelastic expansion. PA imaging, combined with US, allows for stem cell tracking with a relatively large penetration depth and high sensitivity using efficient contrast agents.10–14 In addition, various endogenous tissue components such as hemoglobin, melanin, and fat can be selectively visualized using spectral analysis of PA signals. Therefore, both blood vessel visualization and tracking of cells labeled with exogenous contrast agents are possible within the context of healing skin.14–16
Among numerous exogenous contrast agents for PA imaging, gold nanoparticles are a superior candidate to assist regenerative medicine due to their high optical absorption cross-section, excellent biocompatibility, and photostability.17,18 In addition, the optical properties of gold nanoparticles can be tuned by changing the size and the shape of the particles or by controlling particle aggregation. 19 Our group has demonstrated that gold nanoparticles can be loaded into stem cells without functional and biological side effects.17,18
The ultimate goal of this work is to develop an effective and simple imaging strategy for clinical applications in burn injury diagnosis and stem cell therapy. This work is focused on a combinatorial cell tracking/tissue mapping protocol to monitor ASC-mediated tissue regeneration. Our technique (Fig. 1) is designed to assist clinicians by providing an easy-to-use imaging tool during multiple clinical phases, including (i) diagnosis of burn severity, (ii) tracking of implanted stem cells, and (iii) monitoring of skin tissue regeneration. We developed an effective and safe stem cell tracking technique based on gold nanorods (AuNRs) as imaging contrast agents, and created a US/PA imaging protocol to quantify vascularization and blood perfusion in a burn wound bed. As a result, ASCs, encapsulated in a hydrogel dressing after AuNR labeling, could be selectively traced in the burn wound till 2 weeks. We also demonstrated that gold nanoparticle-coupled US/PA imaging did not negatively affect the biological behaviors of ASCs, and our imaging modalities could quantitatively and noninvasively assess skin tissue regeneration.
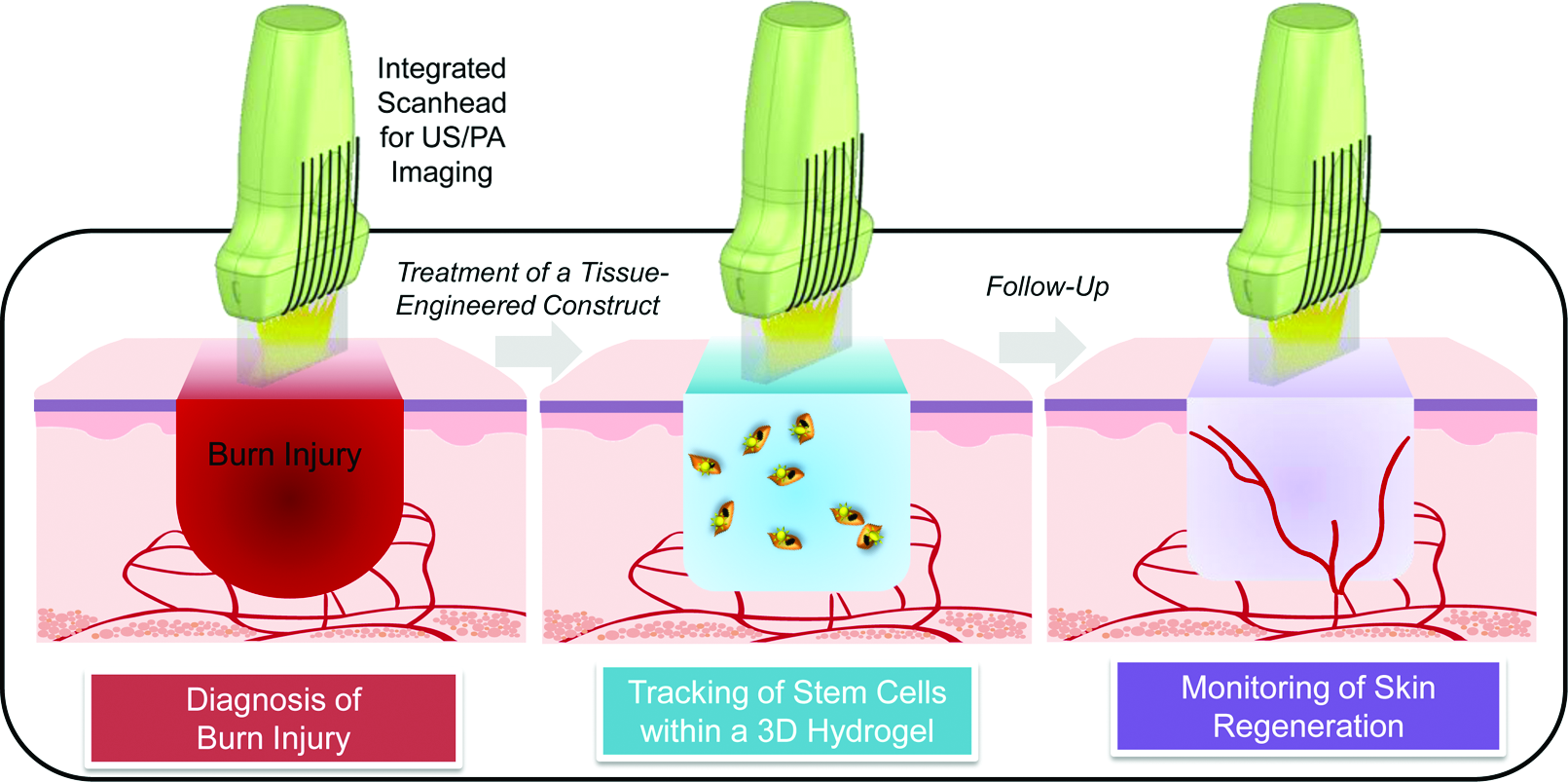
Illustration for the overall goal of the study. The developed technique is designed to assist clinicians by providing an easy-to-use imaging tool during multiple clinical phases, including (i) diagnosis of burn severity, (ii) tracking of implanted stem cells, and (iii) monitoring of skin tissue regeneration. PA, photoacoustic; US, ultrasound. Color images available online at
Materials and Methods
Preparation and analysis of silica-coated AuNRs
AuNRs were synthesized using a seed-mediated growth method as described elsewhere.
20
Briefly, gold acid (HAuCl4) was combined with cetyl trimethylammonium bromide (CTAB) and silver nitrate (AgNO3) and heated to 30°C. Ascorbic acid (C6H8O6) was slowly added to the solution to prepare the growth solution. The gold seed solution was made by adding CTAB, gold acid, and NaBH4 with 1100 rpm stirring. The seed and growth solutions were combined with 500 rpm stirring. AuNRs were PEGylated using mPEG-SH (MW=5 kDa; Laysan Bio) by overnight incubation. After PEGylation, AuNRs were coated with a layer of silica (SiO2) by adding tetraethyl orthosilicate in the isopropyl alcohol solution, resulting in nanoparticles (SiO2AuNR) having a net negative surface charge. To improve cellular uptake and SiO2AuNR stability, poly
Cell culture and SiO2AuNR labeling
For the rat ASC isolation, adipose tissues from the fat pads of Lewis rats (male, 8–12 weeks; Harlan) were digested using 0.05% collagenase type I (Sigma and Invitrogen), and cell pellets were collected from the stromal vascular fraction. For human ASCs, cells were commercially acquired from Lonza, Inc. For expansion, adherent cells were cultured in cell growth media: Dulbecco's modified Eagle's medium-low glucose with Glutamax I (Invitrogen) supplemented with 10% fetal bovine serum (Invitrogen) and 1% penicillin-streptomycin (Invitrogen). ASCs were passaged at a seeding density of 5000 cells per cm2 till passage 7. For cell labeling, silica and PLL-coated SiO2AuNRs were resuspended in the growth media and used to treat a confluent cell monolayer. After a 24-h incubation, the SiO2AuNR-containing culture media was replaced with growth media for subsequent incubation. Optical characteristics of the labeled cells were then measured after washing of the excess of nanoparticles. Specifically, 4 μM calcein acetoxymethyl (AM; Life Tech) in Dulbecco's phosphate-buffered saline (DPBS) was added to ASCs. After incubation for 45 min at 37°C in a humidified CO2 incubator, green fluorescent calcein AM-positive ASCs were regarded as viable. SiO2AuNRs were loaded to the cultured cells at a concentration of 4×107 NRs per cell.
ASC encapsulation into PEGylated fibrin hydrogels
As illustrated in Figure 2, to produce a 2 mL PEGylated fibrin gel (PFG), 250 μL fibrinogen (Sigma) (80 mg/mL) solution in DPBS (pH 7.8) was combined with 250 μL succinimidyl glutarate polyethylene glycol (SG-PEG-SG) solution (8 mg/mL; NOF America) and 500 μL cell suspension followed by addition of 1 mL thrombin (Sigma) solution (25 U, diluted with CaCl2 at 1:3 by volume) and 10 min incubation at 37°C. For the burn injury study, the tissue-engineered constructs were made as disk-shaped gels containing ASCs to cover the excised burn area. The gel (diameter=2.6 cm, surface area=5.3 cm2) was fabricated using a CellCrown™6 (Scaffdex) as described in Figure 2B. The bottom of CellCrown6 is sealed with sterile Parafilm M film, which was peeled off after gelation. For wound dressing after ASC-gel implantation, we used a double-dressing method. We at first applied Tegaderm™ (3M) on the top of the gel to prevent drying and Duoderm® (ConvaTec, Inc.) on the top of Tegaderm. Cell seeding density was either 0.2 or 1 million ASCs per mL, for ex vivo imaging studies using gold nanospheres and in vivo imaging studies, respectively. To fluorescently label ASCs for histological analysis, CellTracker™ CM-DiI dye (C68H105Cl2N3O; Life Tech), which is incorporated into the cell membrane, was used.
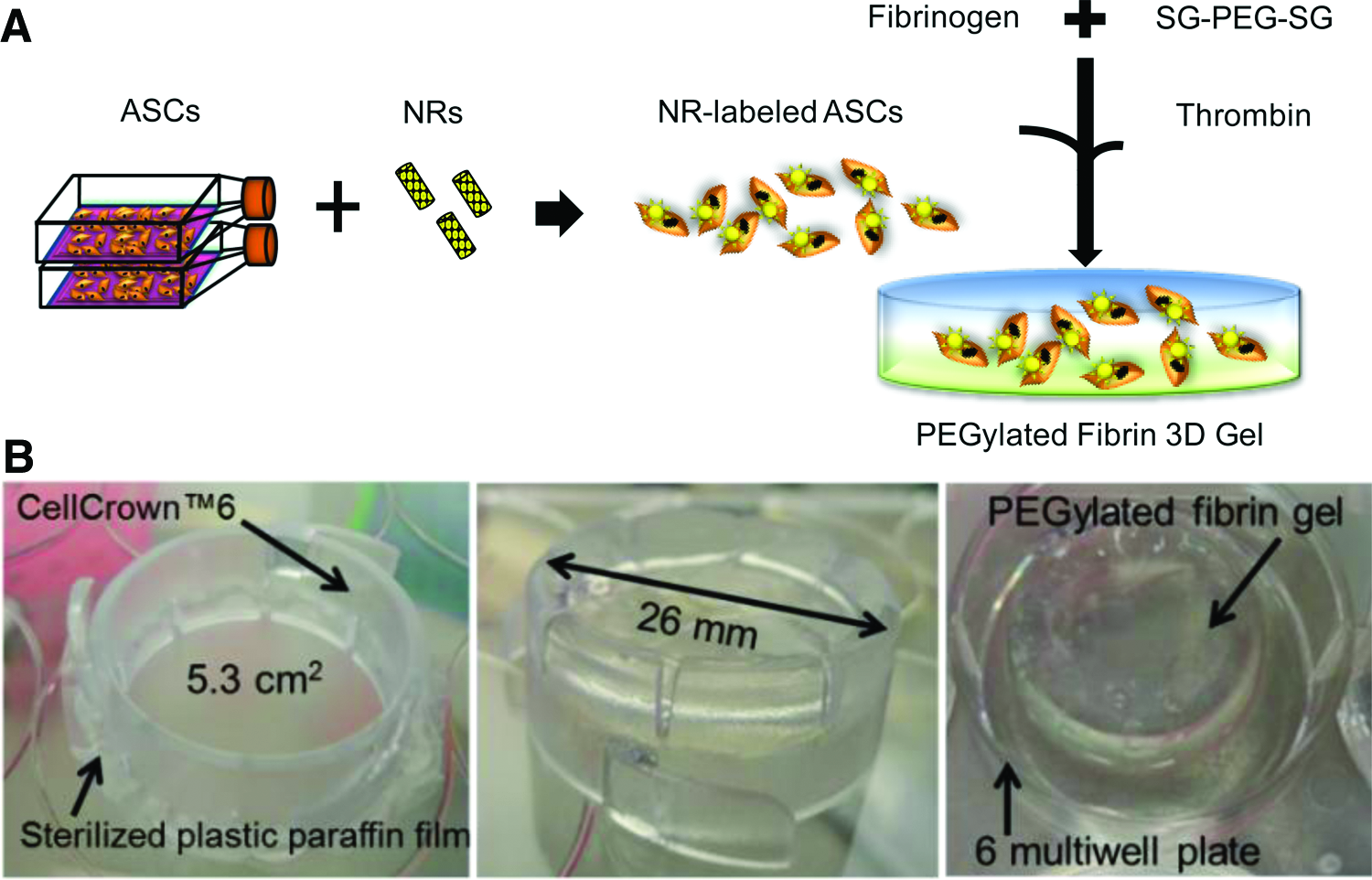
A 3D PEGylated fibrin gel including nanorod (NR)-labeled adipose-derived stem cells (ASCs) for burn injury treatment.
Rat burn injury model
The animal model for burn injury was a contact skin burn wound on the anterior dorsum of rats. Lewis rats (male, 8- to 15-week-old) were anesthetized using inhalation of 2% isoflurane. Under anesthesia, the respiratory motion of rats was monitored by the animal monitoring system (VisualSonics, Inc.). A heated brass plate was placed onto the depilated dorsal surface for different durations to produce various burn severities. Buprenorphine (0.05 g/kg) was administrated as an analgesic drug every 12 h till 48 h after burn injury. Animal surgery and care were performed following the Institutional Animal Care and Use Committee (IACUC) protocol (AUP-2010-00111). Rat housing and care were performed following the regulation and guidance of the Animal Resource Center in The University of Texas at Austin. The burn wound was created in the dorsal area of each rat. The diameter of the circular metal soldering device was ∼1.8 cm. The actual size of the wound was ∼2.3 cm. To study burn levels, we made injuries by varying the heating temperatures and durations: low (87°C for 30 s and 113°C for 10 s), middle (100°C, 30 s), and severe (113°C, 30 s). In addition, to study the postburn healing, we created a burn injury by heating at 87°C for 10 s. After burn injury, the behaviors and response of rats were monitored every day and weights were measured every 3 days. Each rat was housed individually. Combined US/PA imaging was used for in vivo evaluation of capillary fluid leakage as a measurement of severity of burn injury. Imaging was performed at 30 min after the contact burn to minimize any transient effects that can possibly influence PA signal intensity. In a preliminary study using gold nanospherical tracers (Supplementary Fig. S1; Supplementary Data are available online at
Combined US/PA imaging
US and PA signals were collected using an ultrasound imaging system (Vevo 2100; VisualSonics, Inc.) with a 20 or 40 MHz ultrasound array transducer (MS-250 or MS-550S; VisualSonics, Inc.). Tunable pulsed laser systems (Premiscan; GWU, Inc. and Vevo LAZR; Visual Sonics, Inc.) were used to deliver photons through an optical fiber bundle. The US transducer was integrated with the fiber bundle through which light irradiated the tissue below the scanhead similar to that shown in Figure 1. The US and PA signals were captured from the same 2D cross-section, and the scanhead was then mechanically scanned in the elevational direction by a motion axis to acquire 3D images. During mechanical scanning of the scanhead, signal capture was synced with physiological data of the rats using an animal monitoring system and the imaging data were acquired only when respiratory motion was minimized to avoid motion artifacts. To differentiate PA signals generated by the labeled stem cells from background tissue, multi-wavelength (680–960 nm) PA imaging was performed with fluences of 5–15 mJ/cm2.
Postprocessing of data
PA signal amplitudes are linearly proportional to the concentrations and absorption coefficients of the target.10,22 Therefore, by comparing acquired PA signals with reference absorption spectra, spectral unmixing of the different absorbers is possible. For this study, oxygenated and deoxygenated hemoglobin in blood vessels, and SiO2AuNR-loaded ASCs were assumed to be the main chromophores involved in PA signal generation. Hence, to distinguish these chromphores from each other, the offline data processing was performed following the real-time in vivo data acquisition. In the offline processing, the acquired raw US/PA signals were beamformed and interpolated to reconstruct 2D US and PA images. Laser energy at each wavelength and each cross-section was then compensated for PA images. At each spatial location, the compensated PA signals from multiple wavelengths were compared with optical absorption spectra of oxygenated and deoxygenated hemoglobin, 23 and the SiO2AuNR-labeled ASCs. If needed, the PA and spectroscopic PA (sPA) images were combined with US images by overlaying PA/sPA intensities higher than a user-defined threshold on the grayscale US images.
Blood vessel density change before and after burn injury was quantified using 3D PA signals after spectral analysis. First, PA signals classified as blood (oxygenated and deoxygenated hemoglobin) were subjected to a user-defined threshold to reduce background noise. Then, the continuity of the PA signals was analyzed and the small isolated segments were abandoned to obtain the blood vasculature. To extract the central path of the blood vasculature and analyze vessel morphology, the acquired blood vasculature was skeletonized using thinning algorithms.24,25 Then, blood vessel density was estimated by counting the number of voxels in the skeletonized vasculature compared with the total number of voxels in a given region of interest. Blood perfusion was quantified similarly, but vessel connectivity and morphology were not considered for quantitative analysis of blood perfusion and thus the total amount of PA signals, which is linearly proportional to hemoglobin concentration, was used in calculations. To quantify the networks and localization of new and preexisting blood vessels as well as perfusion, the imaging data were collected from animals (n=3) at day 14 after implantation of PFGs containing ASCs either with or without nanoparticle labeling. Data were represented as mean±standard deviation. A commercially available statistical software (JMP Pro 10; SAS Institute, Inc.) was used to analyze the significance in the results both before and 14 days after the treatment by a Student's t-test. Data with p-values lower than 0.05 were regarded as significant.
Blood vessel analysis using immunofluorescence staining of smooth muscle alpha-actin
To compare US/PA imaging results of blood vessels with histological analysis, we visualized smooth muscle alpha-actin (SMA), a pericyte marker, by immunofluorescence staining. Sample fixation was performed by incubating samples with 10% neutral buffered formalin overnight. The fixed samples were transferred/incubated in a series from 5% to 20% sucrose buffered solutions before cryomolding. The tissue blocks were frozen in the solution containing Tissue-Tek® O.C.T. compound and 20% sucrose (volume ration=1:2) by incubation in the 2-methylbutane, which was cooled in the nitrogen liquid. The frozen tissue blocks were stored at −80°C until analysis. The tissue sections (20 μm) were permeabilized with 0.5% Triton X-100 for 20 min. The washing buffer was TRIS-based buffer saline with Tween 20 (0.05%) (TBS-T). After TBS-T washing, 10% normal goat serum was treated to the sections for 1 h. Then, the samples were incubated in the primary antibody solution overnight at 4°C. The primary antibody solution was composed of anti-SMA antibody (ab7817; Abcam) diluted (1:100 dilution) in the 2.5% normal goat serum/TBS-T. To confirm the signal, normal mouse IgG (sc-2025; Santa Cruz) and primary antibody-omitted samples was used as a control. After removing the primary antibody solution next day and washing with TBS-T, the samples were incubated with secondary antibody solution containing Alexa 488-conjugated goat anti-mouse IgG (H+L) (Life Tech) with 2.5% normal goat serum/TBS-T for 1 h at room temperature. Cell nuclei were visualized by incubating the samples in 5 μg/mL DAPI (Life Tech) for 15 min. After mounting in fluorescence-antifading media (Life Tech), green fluorescence signals from SMA were detected and imaged using a Leica microscope (DMI 3000).
Results
In vivo US/PA imaging to assess burn severity
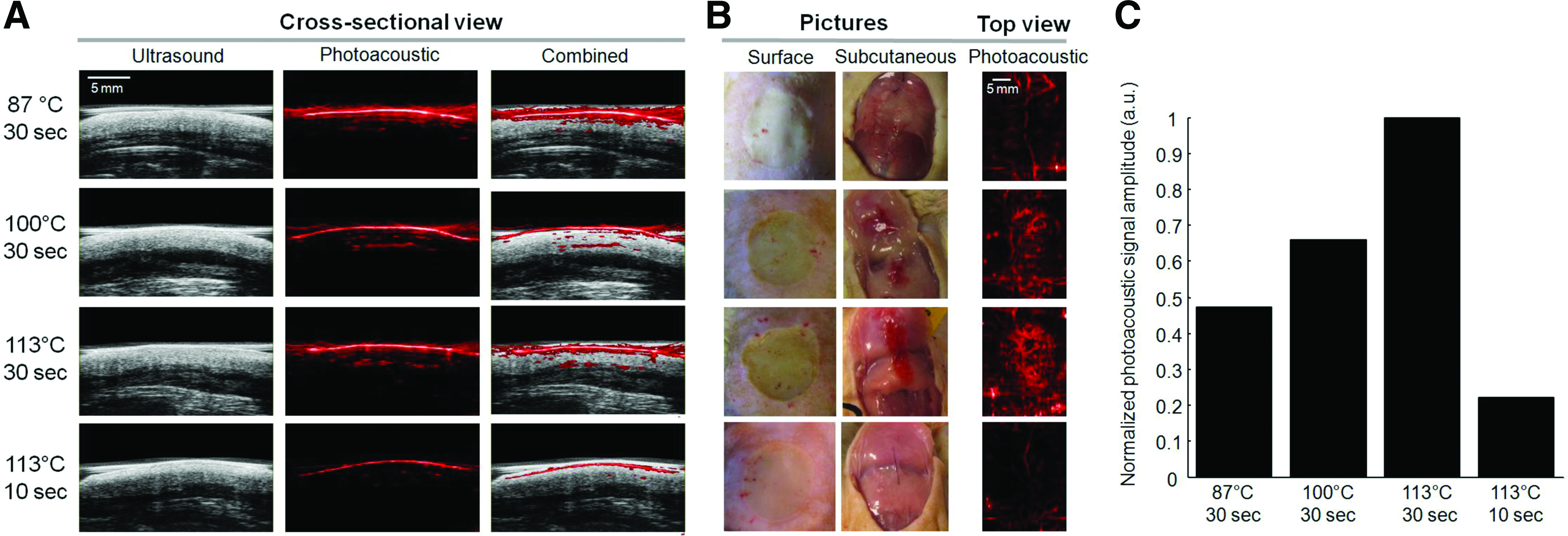
Visual inspection did not reveal significant differences in the superficial morphology of burn-injured skin depending on the severity of burn injury. However, in the low-level burn injury that resulted from heating at either 87°C for 30 s or 113°C for 10 s, there was no bleeding in the subcutaneous tissue, which mimicked first- and second-degree burns as shown in Figure 3. In contrast, we could observe significant bleeding throughout the fat tissue with concurrent tissue damage similar to third-degree burns where heating was performed at either 100°C or 113°C for 30 s. Cross-sectional US/PA images at a wavelength of 800 nm provided depth-resolved information regarding bleeding throughout the dermal tissue with associated tissue morphology. Moreover, top-view PA images clearly showed the strongest PA signal generation in the case of the highest temperature and the longest heating duration. Quantitative analysis of PA signal amplitude agreed well with subcutaneous bleeding levels confirmed after skin incision.
In vitro analysis of NRs as cell nanotracers for ASCs
Our previous experiments, described elsewhere, 18 have demonstrated significant cellular uptake of gold nanospheres into ASCs with no measureable loss in cell viability. This study investigated SiO2AuNR uptake by ASCs in vitro and selective visualization of the NR-labeled ASCs in the skin tissue. As shown in the UV-Vis spectra in Figure 4A, SiO2AuNRs have a longitudinal absorption peak at around 826 nm wavelength. After NR uptake by ASCs, the peak broadening was seen in the range of ∼700–900 nm. To demonstrate the feasibility of NRs as an ASC tracer, we measured the cellular uptake and toxicity in vitro. Figure 4B showed that ASCs could take up surface-modified NRs coated with PLL and silica (SiO2). There were no observable morphological differences between sham control and NR-treated ASCs. In addition, calcein AM staining demonstrated no significant cytotoxicity as a result of NR treatment. NRs that aggregated in the cytoplasm of ASCs could be visualized as dark brown and yellow-orange colored cells in bright and dark field images, respectively. Furthermore, Figure 4C indicated that PA imaging can detect and resolve various optical absorbers at different wavelengths (750 and 1205 nm) according to their absorption spectra. Specifically, the NR-labeled ASCs (green colored) could be detected through spectral analysis using multiwavelength PA imaging after cell injection into ex vivo porcine skin tissue. ASC localization was distinguished from epidermis (blue), blood (red), and fat (yellow).
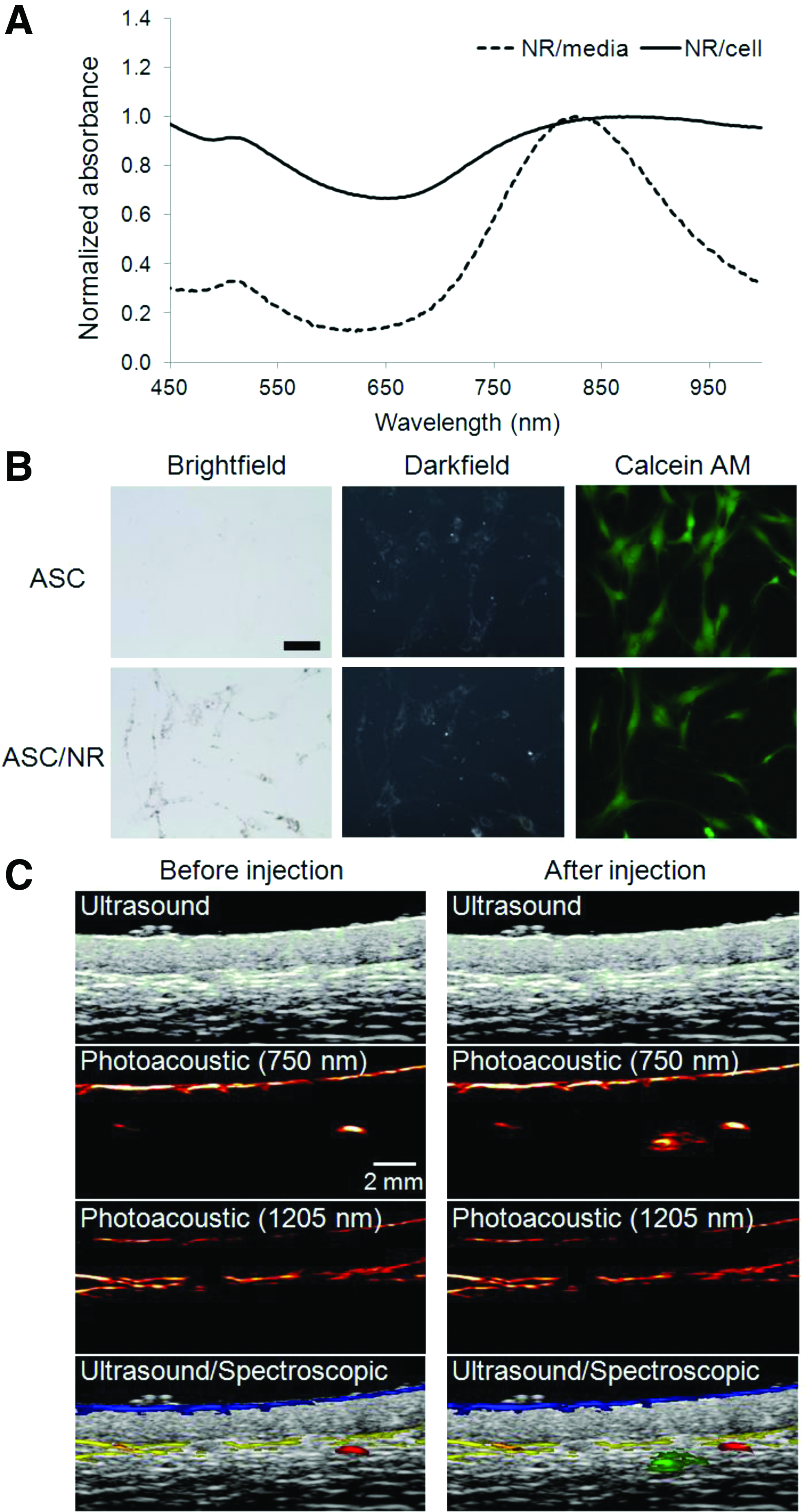
NR labeling of ASCs.
In vivo longitudinal sPA tracking of ASC treatment of burn injury
Results shown in Figure 5 demonstrate that combined US/PA imaging is capable of noninvasive and selective tracking of NR-labeled ASCs as well as blood vessels over the course of 2 weeks. Figure 5A–E show the “top view” PA images of burn tissue treated with labeled ASCs at five different time points (2 days before the treatment and 4, 7, 10, and 14 days after the treatment). These images clearly show overall changes in vascularization and gel degradation over time. However, since PA signals can be generated from various optical absorption sources, it was difficult to distinguish the distribution of the NR-labeled ASCs in the PA images at a single wavelength especially at day 14 after the treatment when the gels were almost fully degraded. In contrast, the NR-labeled ASCs as well as blood vessels were clearly distinguished in sPA images (Fig. 5F–J). Figure 5K–O represent the cross-sectional US and sPA images during the treatment using labeled ASCs. The combined cross-sectional US and sPA images provide depth-resolved morphological, functional, and cellular information—a distinct advantage of the developed imaging method. Specifically, morphological changes both before and after the ASC treatment along with wound closure are well portrayed in the US images. Cross-sectional sPA images selectively visualized the NR-labeled cells from background tissue over the time course of the study as well as provided physiological insights by tracking blood vessel location and oxygen saturation.

In vivo monitoring of microvasculature in the regenerated skin
The PA-derived maps of microvasculature were obtained from three different data sets to estimate tissue regeneration and re-establishment of blood perfusion. Figure 6A demonstrates changes in the vasculature both before burn injury and 14 days after burn injury and treatment with ASCs (nonlabeled). By comparing the photograph and the “top view” PA images in Figure 6A, the identifiable burn boundary in the photograph was outlined in the PA images using dotted lines. The PA images indicate significant blood vessel changes between the two time points. Quantitative analysis of the microvasculature was performed using the 3D PA imaging data. There was a statistically significant increase in blood vessel density during burn skin regeneration at 2 weeks after the burn and ASC treatment (Fig. 6B). In addition, relative to the change of blood vessel density in the normal tissue, the change in burned tissue was prominent, which implies participation of neovascularization in the burn tissue regeneration process. Similarly, blood perfusion in the injured region was also significantly increased over time as shown in Figure 6C. Histological verification is based on detection of positive SMA and CM-DiI signals in the fluorescence images of skin tissues (native and injured tissues), as shown in Figure 7. SMA-positive neo-vasculature was significantly higher in wound skin tissues compared with native and uninjured surrounding tissues. The majority of ASCs, which were visualized in red by CM-DiI, were detected on the surface of wound areas.


Smooth muscle alpha-actin (SMA) immunofluorescence of a regenerating skin and ASC localization. Tissue samples were harvested at day 14. DAPI (blue), CM-DiI (red), and SMA (green) fluorescent signals demonstrate nuclei, implanted ASCs, and SMA, respectively. Scale bar=100 μm. Color images available online at
Discussion
In burn injury assessment, the severity of tissue damage can be determined by evaluating the following key parameters: (i) surface morphology, (ii) sensation for pain and pressure, (iii) blood perfusion, and (iv) injured skin depth. 26 However, current clinical burn diagnostic methodologies for determining these parameters such as biopsy for histology and the pinprick test are generally not precise, not real time, and invasive. Severity assessment is a critical step in medical planning and will dictate interventions such as the extent of eschar removal and subsequent treatments, including dressings and skin grafts. 26 Laser Doppler imaging has been widely applied for burn severity assessment and can noninvasively assess microcirculation with high accuracy (>90%), but only a small part of the burn tissue can be examined without depth-resolved structural information and cellular data. 26 Therefore, a novel tool for burn injury monitoring needs to incorporate imaging that can noninvasively and rapidly give accurate information about burn depth and blood perfusion. Combined US/PA imaging was able to monitor blood leakage deep into the skin to the subcutaneous fat, caused by blood vessel damage, even though burn wounds had a similar appearance of surface morphologies. Different levels of burn injury were then quantified, the results of which may be clinically useful as the depth of skin burn injury is a primary determinant to diagnose burn degrees and to decide the correct treatment strategy. In contrast, combined optical coherence tomography and pulse speckle imaging gave a detailed view of the geographical wound environment. 27 However, these modalities could not collect specific signals from blood as well as epidermis and have relatively shallow imaging depth. In addition, our US imaging successfully visualized initial volumetric changes of wound tissue due to fluid exudation from damaged tissues and blood vessels (Supplementary Fig. S2).
In tissue-engineering field, stem cells tracking has been often performed using fluorescent dyes such as DiI. Even though these dyes are known to stably maintain the signal to trace stem cell localization in the long-term manner for several months, this strategy involves invasive tissue processing and histological analysis after treatment. To address this limitation, stem cell tracking has been explored using various imaging modalities, including magnetic resonance imaging (MRI), nuclear medicine, and optical imaging. Nuclear medicine imaging, such as positron emission tomography, can be an option to visualize stem cells with a nanomolar sensitivity, but stem cells cannot be monitored in the long term mainly due to the short half lives of radioisotopes till a few days.28–31 Bioluminescence and fluorescence imaging using genetic labeling of reporter genes such as luciferase and green fluorescent protein (GFP) via nonviral gene transfer (liposomes and electroporation) has advantages of real-time noninvasive tracking with long-term stability. 32 Even though localization and expansion of embryonic stem cells in the burn tissue by the GFP-based bioluminescence imaging technique for approximately 3 weeks has been demonstrated, this approach is not available for 3D multi-tissue visualization around implanted stem cells due to limited depth-resolved information. 33 In addition, this approach can be limited by the efficiency of genetic modification as well as safety issues, including risks from gene transfection and potential immunogenic responses.28–32 MRI using a metallic tracer such as superparamagnetic iron oxide nanoparticles can be used to label stem cells. However, it requires bulky and costly instrumentation and its application is still challenging due to low cell and nanoparticle detection sensitivity (1000 cells/mm3 at 3T and 500 cells/mm3 at 7T).28–31,34,35 US/PA imaging can also be effectively utilized in combination to track stem cells using endogenous and exogenous contrast agents, in addition to the aforementioned advantages of US/PA imaging in burned tissue diagnosis. The efficiency and mechanism of regeneration by stem cell-based therapies can potentially be understood by visualizing delivered cells with regard to blood vessels and tissue morphology. Compared with other clinical approaches, US/PA imaging can track stem cell behaviors with high sensitivity (<10 cells/mm3), excellent safety, spatial resolution comparable with that of US imaging (axially 40 μm and laterally 90 μm using the VisualSonics' MS-550S 40 MHz US array transducer), and long-term tracking ability (>2 weeks) as demonstrated in both the in vitro and in vivo experimental results. 22 Furthermore, stem cell tracking may be performed with concurrent visualization of skin morphology and wound closure.
In our previous studies, spherical gold nanoparticles (20 nm) could successfully trace ASCs in vitro without any negative effects. 18 In this study, we initially tested the tracking ability of spherical gold nanotracers for ASCs ex vivo (Supplementary Fig. S1). To detect labeled ASCs after burn injury treatment, ex vivo rat skin tissues were explanted at three different time points (1, 4, and 7 days after the treatment). Cross-sectional PA images overlaid on US images are shown for both labeled and unlabeled ASCs in gels. While the implanted gels with ASCs could not be detected without gold nanoparticle labeling and most PA signals were originated from background tissue such as hemoglobin and epidermis, strong PA signals were generated from the gold nanoparticle-labeled ASCs till 7 days after the burn treatment. In addition, using spectral analysis, the gold nanoparticle-labeled ASCs were distinguished from other optical absorbing components. Therefore, the results demonstrate the feasibility of PA imaging for the burn injury by demonstrating long-term, selective visualization of nanoparticle-labeled ASCs.
Although sPA imaging can selectively detect gold nanoparticle-labeled stem cells as shown in Figure 5, the quality of spectral analysis depends on the shape of the gold nanoparticles and resulting optical properties. For example, the absorbance of gold nanosphere-labeled ASCs and deoxygenated hemoglobin are somewhat similar within the wavelength range of 680–960 nm. The absorption of AuNRs with a sharp absorption peak, on the other hand, is significantly distinct from both oxygenated and deoxygenated hemoglobin. NRs can, therefore, be easily distinguished from background tissue. 36 Moreover, with a silica coating of gold nanoparticles, the thermal stability of the NRs in response to pulsed laser irradiation can be significantly enhanced with minimal changes in optical properties.21,37
PA imaging has emerged as a tool for blood vessel assessment, because hemoglobin can be directly visualized in PA imaging and, therefore, no endogenous contrast agents are required. In addition, quantitative analysis of blood vessels is possible due to the relatively high resolution and a linear relationship between hemoglobin concentration and PA signal intensity. There have been numerous studies to visualize and quantify blood vessels using PA imaging for various applications.10,11,38–40 For example, noninvasive assessment of tumor vascular development using PA imaging was demonstrated. 38 This study evaluated the increase of the total hemoglobin concentration as well as the vessel diameter in the tumor region in vivo. However, most of the vessel assessment studies using PA imaging were performed at a relatively shallow depth because the PA signal intensity and spatial resolution can be affected by increasing optical attenuation with depth. Neovascularization in the wound bed is one of the most critical steps for tissue regeneration. In the histological analysis of tissue samples harvested at day 14 after gel implantation, angiogenesis in the wound bed was demonstrated by staining SMA-positive blood vessels. We observed a significantly higher number of blood vessels in the wound tissue compared with normal surrounding skin tissue. Moreover, the regenerating skin tissue treated with ASC-PFGs also showed directional vascular growth toward the burned region. This may be caused by tissue contraction during wound closure and chemokine-induced angiogenesis toward the injured area.
In conclusion, our imaging-based monitoring process does not negatively affect the regenerative potential of delivered cells and is able to visualize the location of cells in a dynamic tissue microenvironment undergoing wound healing. This study aimed at introducing a methodology to apply combined US/PA imaging to burn injury assessment and ASC therapies. Our results indicate that the presented method is promising to noninvasively assess burn skin regeneration as well as burn injury levels while acquiring morphological, functional, and cellular information.
Footnotes
Acknowledgments
The authors thank Dr. Laura M. Ricles and Shannah L. Leal for synthesis of gold nanoparticles and silica coating. This work was supported in part by National Institutes of Health under grant EB015007.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.