
Abstract
Primary human hepatocytes are widely used for basic research, pharmaceutical testing, and therapeutic concepts in regenerative medicine. Human hepatocytes can be isolated from resected liver tissue. Preoperative portal vein embolization (PVE) is increasingly used to decrease the risk of delayed postoperative liver regeneration by induction of selective hypertrophy of the future remnant liver tissue. The aim of this study was to investigate the effect of PVE on the outcome of hepatocyte isolation. Primary human hepatocytes were isolated from liver tissue obtained from partial hepatectomies (n = 190) using the two-step collagenase perfusion technique followed by Percoll purification. Of these hepatectomies, 27 isolations (14.2%) were performed using liver tissue obtained from patients undergoing PVE before surgery. All isolations were characterized using parameters that had been described in the literature as relevant for the outcome of hepatocyte isolation. The isolation outcomes of the PVE and the non-PVE groups were then compared before and after Percoll purification. Metabolic parameters (transaminases, urea, albumin, and vascular endothelial growth factor secretion) were measured in the supernatant of cultured hepatocytes for more than 6 days (PVE: n = 4 and non-PVE: n = 3). The PVE and non-PVE groups were similar in regard to donor parameters (sex, age, and indication for surgery), isolation parameters (liver weight and cold ischemia time), and the quality of the liver tissue. The mean initial viable cell yield did not differ between the PVE and non-PVE groups (10.16 ± 2.03 × 106 cells/g vs. 9.70 ± 0.73 × 106 cells/g, p = 0.499). The initial viability was slightly better in the PVE group (77.8% ± 2.03% vs. 74.4% ± 1.06%). The mean viable cell yield (p = 0.819) and the mean viability (p = 0.141) after Percoll purification did not differ between the groups. PVE had no effect on enzyme leakage and metabolic activity of cultured hepatocytes. Although PVE leads to drastic metabolic alterations and changes in hepatic blood flow, embolized liver tissue is a suitable source for the isolation of primary human hepatocytes and is equivalent to untreated liver tissue in regard to cell yield and viability.
Introduction
T
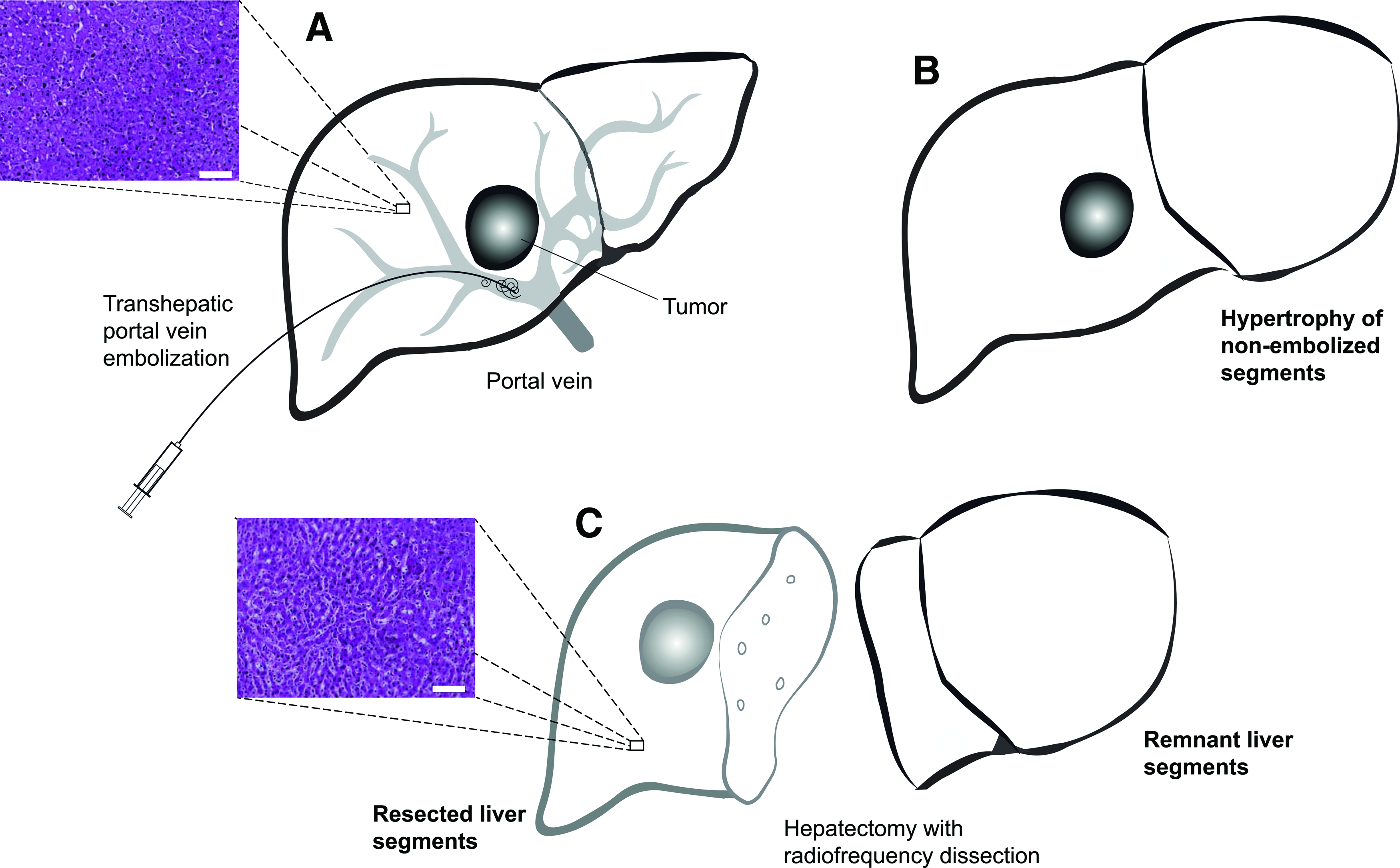
Liver surgery, ranging from small atypical resections to trisectorectomies with only one or two liver segments remaining, is possible because of the unique regenerative capacity of the liver. 11 The lost liver mass is replaced by compensatory growth of the remaining tissue. Extended liver resections harbor the risk of resulting in a too-small postoperative liver volume, which can cause delayed liver regeneration and can lead to postoperative liver insufficiency and liver failure.12–14 Portal vein embolization (PVE) is a common approach to decrease the risk of insufficient postoperative liver regeneration by inducing growth of the future remnant liver tissue before surgery.14,15 During PVE, the portal branch supplying the part of the liver that will be resected is embolized, which leads to a redirection of the portal blood flow to the portal branches of the nonembolized liver tissue 16 (Fig. 1). Because the arterial perfusion remains intact, the embolized areas of the liver do not become necrotic. The redistribution of the portal flow to the future remnant liver leads to hypertrophy of these segments, whereas the occlusion of the vessels in the embolized areas leads to shrinkage of those lobes.14,16
PVE.
PVE enables extended liver resections in patients with advanced tumors or tumors with an unfavorable anatomic location.17,18 Given that the liver tissue from partial hepatectomy is the most frequently used material for human hepatocyte isolation and PVE is increasingly performed to enable extended resections, an increasing percentage of donors for hepatocyte isolation have undergone PVE before surgery.17,18 Various parameters affecting the outcome of hepatocyte isolation have already been evaluated, but the impact of PVE on cell yield and cell viability after hepatocyte isolation has not been analyzed. Because the isolation procedure is rather expensive and time consuming, all parameters affecting hepatocyte isolation should be understood to increase the efficiency of isolation protocols and decide if it is worthwhile to isolate cells from a particular liver sample.
The aim of our study was to investigate the effect of PVE on the isolation of primary human hepatocytes. Therefore, we first performed a literature search to identify the parameters predictive of the outcome of hepatocyte isolation (Table 1). Next, we investigated the effects of sex, age, gamma-glutamyl transferase (GGT), indication for surgery, liver weight, cold ischemic time (CIT), digestion time, and the quality of the liver tissue. These factors have been shown to influence the outcome of hepatocyte isolation by multiple researchers.8,10,19,20,22,24–26,28 Furthermore, aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (AP), bilirubin, activated partial prothrombin time (aPTT), and Quick values were determined since these parameters are routinely taken before surgery and accessible before the isolation is performed. Then, we analyzed whether donors with or without PVE differed according to these parameters and described the outcome of hepatocyte isolation in both groups. Finally, in cultured hepatocytes, transaminase leakage and functional metabolic parameters were assessed.
The number of total references in literature and the number of publications with significant findings regarding the parameters in literature (performed on March 15, 2015).
ALT, alanine aminotransferase; AP, alkaline phosphatase; AST, aspartate aminotransferase; BMI, body mass index; CIT, cold ischemic time; GGT, gamma-glutamyl transferase; INR, International Normalized Ratio; PTT, partial prothrombin time.
Materials and Methods
Study design
A total of 262 liver specimens were collected for hepatocyte isolation from patients undergoing partial hepatectomy or liver transplantation in the Department of General, Visceral, and Transplantation Surgery at the Charité–Universitätsmedizin Berlin between September 2005 and October 2014. All experiments were performed with the informed consent of the patients and following the institutional and ethical guidelines. Reasons for not including hepatocyte isolations in the subsequent analysis were deviations from the standard operating procedure (n = 54), nonexistent information regarding the liver weight (n = 2), inconclusive data (n = 2), and liver explantation before transplantation (n = 14). A total of 190 hepatocyte isolation procedures were suitable for further analysis. These isolations were grouped as PVE and non-PVE in regard to the pretreatment of the patients.
Indication for surgery
For statistical analysis, all cases were classified into five diagnostic categories: hepatocellular carcinoma (HCC; category 1), carcinoma of intra- and extrahepatic biliary tract (category 2), colorectal metastasis (category 3), metastasis from other carcinomas (category 4), and benign diseases (category 5). A total of four patients could not be classified in any of these categories (Table 2).
Data are presented as number of cases (percentage of total number of cases).
Portal vein embolization
The portal vein was accessed through ultrasound- or computed tomography-guided transcutaneous puncture. A portography was performed, and a central portal branch was closed with coils or plugs. All patients of the PVE group underwent embolization of the right portal vein. The mean time interval between embolization and partial hepatectomy was 31 ± 2 days.
Clinical and isolation-related parameters
Age, sex, and the diagnosis of the donors were recorded routinely in every isolation protocol, in addition to the weight of the perfused liver tissues, collagenase digestion times, and CIT. CIT refers to the time of cold storage from the time the sample is taken in the operation room until the beginning of the first perfusion step. Preoperative GGT, AST, ALT, AP, bilirubin, aPTT, and Quick values were retrieved from the patient records, and the most recent value before surgery was used for our analysis (not earlier than 5 days before surgery).
Hepatocyte isolation
Liver specimens were obtained from the margin of the macroscopically tumor-free liver tissue immediately after resection. Samples were taken under sterile conditions, transferred into ice-cold (4°C) William's E medium, and immediately transported to the hepatocyte isolation laboratory to keep the CIT as short as possible. Hepatocyte isolation was performed under sterile conditions using our standard isolation protocol. The two-step collagenase perfusion is already reported elsewhere.19,29,30
Briefly, the liver specimen was first cannulated and then flushed with a 500 mL prewarmed (37°C) washing buffer (1.42 M NaCl, 67 mM KCl, and 100 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid [all chemicals from Carl Roth GmbH, Karlsruhe, Germany]) containing ethylene glycol tetraacetic acid (Serva, Heidelberg, Germany). The first perfusion step usually lasted 10–20 min. In the second step, the liver was perfused with a 100 mL prewarmed (37°C) digestion buffer (67 mM NaCl, 6.7 mM KCl, 100 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid, and 4.8 mM CaCl2H2O [all chemicals from Carl Roth GmbH]) supplemented with 100 mg collagenase P (Roche Diagnostics GmbH, Mannheim, Germany).
Collagenase digestion was performed until the liver tissue was visually and tactilely deemed sufficiently digested. The cannulas were removed, and the tissue was mechanically disrupted in a Petri dish while washing with an ice-cold (4°C) washing buffer [1.42 M NaCl, 67 mM KCl, and 100 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid] containing 5% human albumin to stop collagenase reaction. The resulting cell suspension was filtered through a gaze filter and centrifuged (50 g for 5 min at 4°C). Immediately after the first centrifugation, the cell suspension was purified using a density-gradient centrifugation (1474 g for 20 min at 4°C) with 25% Percoll solution (1.124 g/mL). Afterward, the cell pellets were washed with phosphate-buffered saline (PBS) followed by another centrifugation (50 g for 5 min at 4°C). The trypan blue exclusion tests were performed before and after purification for cell counting and viability determination.
Hepatocyte culture
Hepatocytes from PVE livers (n = 4) and non-PVE livers (n = 3) were cultured on collagen-precoated six-well plates immediately after isolation. The cells were seeded at a density of 1 × 106 viable cells per well. Cells were cultured up to 6 days in the William's E medium (Biochrom GmbH, Berlin, Germany) supplemented with 1 μM insulin (Lilly, Indianapolis, IN), 1 μM Fortecortin (Merck Serono GmbH, Darmstadt, Germany), 1 mM sodium pyruvate, 10 mM HEPES, 100 U/mL/100 μg penicillin/streptomycin, and 10% fetal calf serum (all from Biochrom GmbH). The cells were washed with PBS 4 h after plating, and the culture medium was changed again after 12 h. Afterward, the medium was changed every 24 h, and the supernatant was collected. For measurement of AST and ALT concentrations, the supernatant was stored at 4°C and analyzed within 12 h. Supernatant samples for measurements of albumin, urea, and vascular endothelial growth factor (VEGF) secretion were immediately stored at −80°C.
Measurement of biochemical parameters in the supernatant
Biochemical parameters were measured in supernatant samples after 2, 4, and 6 days of culture. AST/ALT enzyme activities were detected using the Fluitest® GOT AST and the Fluitest® GPT ALT detection kit (both Analyticon Biotechnologies AG, Lichtenfels, Germany). Measurements were performed in triplicate and according to the manufacturer's instructions. Urea was measured using the QuantiChrom™ Urea Assay Kit (BioAssay Systems, Hayward, CA). Albumin synthesis was measured using the Human Albumin ELISA Quantitation Set (Bethyl Laboratories, Montgomery, TX). VEGF secretion was measured using the Human VEGF Quantikine® ELISA (R&D Systems, Minneapolis, MN). Enzyme-linked immunosorbent assay measurements were performed in doublet and according to the manufacturer's instructions, with the exception of urea measurements that were performed at 450 nm instead of 430 nm, as recommended in the manufacturer's manual.
Histopathology
The results of the histopathological analysis of the resected liver tissue were taken as the basis for grading liver fibrosis or steatosis of the liver specimens that were used for hepatocyte isolation. Fibrosis and cirrhosis were assessed using a modified classification of Desmet and Scheuer. 31 A liver specimen was categorized as “no fibrosis” if no histological signs of fibrosis were found, as “fibrosis” if signs of mild, moderate, and severe fibrosis were observed, and as “cirrhosis” if definite cirrhotic changes were found. In regard to steatosis, the liver specimens were classified as “mild steatosis” (≤30% of hepatocytes contain fat) or “severe steatosis” (>30% of hepatocytes contain fat). The liver tissue was graded as “nonsteatotic” if no fatty hepatocytes appeared in histology.32,33
Statistical analysis
Data are expressed as the mean ± standard error of the mean. Statistical analysis was performed using GraphPad Prism 6.0 (GraphPad Software, Inc., La Jolla, CA). The nonparametric Mann–Whitney or Kruskal–Wallis test was used to analyze categorical parameters with two or more groups. The parametric unpaired t-test or the one-way ANOVA was applied for the Gaussian distribution. For correlation analysis, the Pearson correlation test or the Spearman correlation test was used (normal or nonparametric distribution). A p-value ≤0.05 was considered significant.
Results
Mean hepatocyte isolation outcome
The outcome of a total of 190 hepatocyte isolations was analyzed. The mean donor age was 60 ± 1 years. Hepatocyte isolation using the two-step collagenase technique resulted in a mean viable yield of 5.65 ± 0.46 × 106 cells/g and a mean viability of 77.82% ± 0.7%. The initial viable yield before Percoll purification was 9.50 ± 0.61 × 106 cells/g, and the initial viability was 73.92% ± 0.88%. The mean Percoll survival, describing the quotient of viable yield before and after Percoll, was 53.25% ± 1.49%.
Analysis of donor characteristics and clinical parameters in the entire cohort
All donor characteristics and clinical parameters known in the literature to affect the outcome of hepatocyte isolation were analyzed (Table 1). The correlation analysis showed that the sex of the donors, AST, bilirubin, Quick, and the quality of the liver tissue significantly affected the outcome of the hepatocyte isolation (Tables 3 and 4). Female sex proved to have a significant positive effect on viable yield before and after Percoll purification, whereas the viability and Percoll survival remained unaffected (Table 4).
Data are shown as p-values and Spearman correlation coefficient (r).
aPTT, activated partial prothrombin time.
Significant p-values and their corresponding correlation coefficients are shown in bold.
A p-value <0.05 was considered statistically significant.
Data are shown as mean ± SEM. To facilitate orientation, significant values are in bold.
p = 0.0175.
p = 0.0178.
p = 0.0362.
p = 0.0133.
p = 0.031.
p = 0.0181.
SEM, standard error of the mean.
High GGT values tended to result in lower hepatocyte yield, but there was no significant correlation between GGT values and hepatocyte yield, viability, or Percoll survival. The donor age had no effect on either the isolation outcome or the Percoll survival (Table 3). AST significantly influenced the Percoll survival (Table 3). High bilirubin values were negatively correlated with the viable cell yield both before and after Percoll purification, whereas Quick affected the viable cell yield before Percoll purification (Table 3).
The indication for surgery had no significant effect on the outcome of the isolation, although carcinoma originating from the intra- and extrahepatic biliary tract (diagnostic category 2) tended to result in a lower viable yield (Table 4). Although there was no difference between the isolation outcomes of liver specimens from nonfibrotic and fibrotic tissues, the liver specimens from cirrhotic livers had a significantly lower viable yield and viability before Percoll, as well as a significantly lower yield after Percoll (Table 4). Significant differences with respect to the viable yield and viability among nonsteatotic, ≤30% steatotic, and >30% steatotic liver specimens were not found. However, the cell yield after Percoll purification was significantly lower for hepatocytes isolated from livers with >30% steatosis compared with ≤30% steatotic or nonsteatotic livers (Table 4).
Analysis of hepatocyte isolation-related parameters in the entire cohort
CIT (mean: 23 ± 1.2 min) and the weight of the perfused liver specimen (mean: 32.2 ± 1.3 g) were significantly negatively correlated with viable yield and viability before Percoll, as well as viable yield after Percoll (Table 3). The liver weight was also significantly negatively correlated with viability after Percoll purification. The digestion time (mean: 11.6 ± 0.4 min) did not influence hepatocyte yield, but there was a significant negative correlation with viability before and after Percoll purification.
Comparison of the general characteristics of the PVE and the non-PVE groups
Of the 190 hepatocyte isolation procedures analyzed, a total of 27 isolations (14.2%) were performed with specimens from patients undergoing PVE before surgery. Three patients were diagnosed with HCC (category 1), 13 patients suffered from a carcinoma originating from the biliary tract (category 2), 9 patients were diagnosed with colorectal metastases (category 3), and 2 patients were diagnosed with metastases from another origin (ovarian carcinoma and gastrointestinal stromal tumor). None of the patients who received a PVE before surgery were diagnosed with benign disease.
A comparison of the above-analyzed hepatocyte isolation parameters of the PVE and the non-PVE groups showed that both groups were well matched according to age, sex, CIT, indication for surgery, liver weight, steatosis, and fibrosis. Differences between the groups were only found in the mean collagenase digestion time and GGT values. The digestion time was significantly longer in the non-PVE group (p = 0.0162), whereas the GGT serum levels in the patients were significantly higher in the PVE group (p = 0.0043).
Because the analysis of the entire study group had indicated that collagenase digestion time significantly influenced the viability before and after purification, all data from isolations with a digestion time ≥20 min or those without a documented digestion time were excluded from further analysis. A total of 27 isolation procedures of specimens with PVE and 122 isolation procedures of specimens without PVE were analyzed. No significant differences between the PVE and the non-PVE groups were found in regard to age, sex, CIT, AST, bilirubin, Quick, indication for surgery, liver weight, degree of steatosis or fibrosis, and collagenase digestion time (Fig. 2). However, there were still significantly higher levels of GGT in the PVE group (p = 0.0055).

Comparison of hepatocyte isolation outcomes in the PVE group versus the non-PVE group
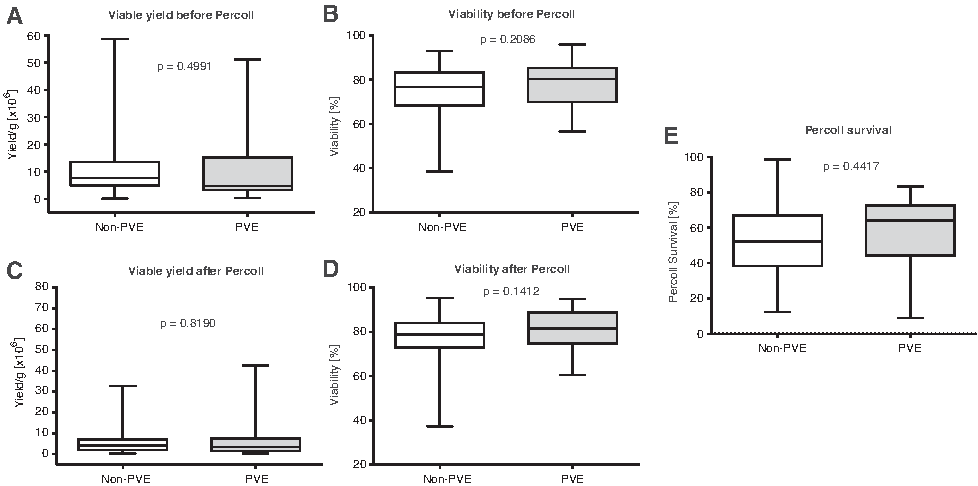
In the subgroup analysis, the mean initial viable cell yield for isolation procedures from PVE livers was 10.16 ± 2.03 × 106 cells/g compared with that of 9.70 ± 0.73 × 106 cells/g in non-PVE livers before surgery (p = 0.499) (Fig. 3). Similarly, there was no significant difference in the viable yield after Percoll purification (p = 0.819). The viability of human hepatocytes isolated from PVE livers was slightly higher but was not statistically significant—either before (p = 0.209) or after (p = 0.141) Percoll purification. Furthermore, the outcomes after Percoll purification were not different between the groups (p = 0.442).
Analysis of the hepatocyte isolation yield in surgical indication subcategories
Because the indication for surgery has been described in the literature to affect the outcomes of hepatocyte isolation procedures, we analyzed the outcomes of the PVE group versus the non-PVE group in indication categories 2 and 3 (the categories 1, 4, and 5 were not further analyzed because of the low number of patients in these groups). The results in both subcategories were similar to the overall result of PVE versus non-PVE. Significant differences could not be found in regard to the number of viable cells or the viability—when analyzed before and after Percoll purification. Although not significant, the viability was slightly better in the PVE group in both categories.
Enzyme leakage and metabolic function of cultured hepatocytes from PVE versus non-PVE livers
Hepatocytes from PVE livers showed a trend to lower AST and ALT leakage compared to those from non-PVE livers without reaching statistical significance (Table 5). Urea and albumin concentrations did not differ significantly between cultures of hepatocytes from PVE and non-PVE livers at any day of the culture period. VEGF secretion was slightly higher in hepatocytes from PVE livers at culture day 2 and slightly lower at culture day 4.
Data are shown as mean ± SEM and p-values.
PVE, portal vein embolization; VEGF, vascular endothelial growth factor.
A p-value <0.05 was considered statistically significant.
Discussion
In recent years, the use of PVE has steadily increased. This approach increased the number of patients who benefited from extended liver resection.15,17,34,35 PVE has become a common procedure for patients undergoing extended hepatectomy. 36 Consequently, an increasing number of hepatocyte isolation procedures are performed using the liver tissue from patients pretreated with PVE. The central question of this study was to determine whether those livers represent a suitable source for human hepatocytes or whether architectural and metabolic alterations because of PVE make hepatocyte isolation from those livers unfavorable because of this time- and resource-consuming procedure.
Several parameters predicting the outcome of hepatocyte isolation have already been described. To characterize our hepatocyte isolation cohort, we first used all relevant parameters for the characterization of our cohort, with the exception of the warm ischemia time and the time of Pringle maneuver, which were not available for all isolations (Table 1).
Interestingly, all parameters that can be influenced by the isolation procedure, namely CIT, digestion time, and weight of perfused liver tissue, had remarkable effects on the isolation outcome. A digestion time <20 min has already been reported to be favorable for good cell viability after isolation.10,24 The results of our analysis support this finding; by considering collagenase activity, an even shorter digestion time might be favorable.
Statements in the literature with respect to the impact of histopathological parameters on the isolation outcome are rather diverse: two studies found a significant impact of fibrosis and cirrhosis on both cell viability and cell yield.20,26 Lee et al. noted that fibrosis is closely associated with hepatic inflammation20,37 and assumed this factor to be the reason for lowered viability in fibrotic and cirrhotic organs.
Septal fibrosis is known to lead to collagenization between sinusoids and hepatocytes, which might create a new barrier for macromolecules.20,37,38 They, therefore, hypothesized that collagenase has only limited access to the extracellular matrix in the liver parenchyma. 20 Furthermore, the increased amount of collagen surrounding the vessels in fibrotic and cirrhotic organs is supposed to result in impaired digestion and, therefore, a lower cell yield. 20 Although we did not observe this negative effect of fibrosis on the hepatocyte isolation outcome, we found a negative effect of cirrhosis. Therefore, the mechanism mentioned above could apply to our findings as well because cirrhosis is the final path of inflammation and fibrosis. Whereas other authors reported either a significantly negative effect on cell viability 20 or a significantly increased viability because of steatosis 22 and a decreased yield, 26 our results do not show any influence of steatosis on either cell yield or cell viability before and after Percoll purification. However, hepatocytes isolated from organs with more than 30% steatosis had a significantly lower cell yield after Percoll purification. Fat accumulation in hepatocytes might lead to altered density of the isolated cells and impair density centrifugation, which then results in a higher loss of viable cells during the purification process. Because we could confirm that most of the previously described parameters are predictive of the outcome of hepatocyte isolation in our cohort, our results seem to be representative of the hepatocyte isolations from partial hepatectomies.
Our study shows that PVE does not negatively affect the outcome of hepatocyte isolation. We did not detect a lower yield or viability for the liver parenchyma after PVE compared with the nonembolized control group before or after Percoll purification. In fact, hepatocytes in the PVE group had a slightly better cell viability after the isolation.
Harada et al. had shown that hepatocytes in the PVE-treated liver lobes are smaller and atrophic compared with those in the nonembolized lobes, whereas the sinusoids were enlarged. 39 Exemplary H&E staining of a liver tissue obtained for isolation from a PVE liver showed the same characteristics (Fig. 1). Cell kinetic analysis performed in the same study revealed a high mitotic index in the nonembolized lobe, whereas the number of apoptotic cells was higher in the embolized lobe, especially in the periportal areas. However, no necrotic changes or inflammatory reactions were found in the embolized lobe. 39 Based on their finding of mild apoptosis in the periportal areas, the authors concluded that those cells must be sensitive to changes, such as a relative hypoxia, induced by PVE.39,40 Conversely, a relative hypoxia evoked by portal embolization could enhance the protection of hepatocytes against hypoxic stress during the isolation procedure, such as in ischemic preconditioning. 41
We hypothesize that this effect could at least explain a slightly better viability of cells isolated from PVE-treated livers. However, VEGF, which is known to be induced by hypoxic conditions, was not significantly elevated in cultured hepatocytes from PVE livers compared to the non-PVE controls.42,44
Interestingly, we found higher GGT values in the PVE group compared with those in the non-PVE group. Because GGT values had no significant influence in the analysis of the entire study group, a bias on the basis of this imbalance can be excluded. In fact, higher GGT values in the PVE group may be a characteristic feature of this group because patients receiving PVE usually have a high tumor burden in addition to biliary obstructions that may result in higher GGT values. Because higher GGT values have been associated with a worse outcome of hepatocyte isolation in the literature,19,20 one could assume that the PVE-treated liver parenchyma might be even better suited for hepatocyte isolation than anticipated.
Our preliminary analysis of the transaminase leakage and metabolic activity of cultured hepatocytes supports this hypothesis and suggests that hepatocytes from PVE livers might perform similarly compared to cells from non-PVE livers. Further studies with larger sample sizes need to be performed to strengthen this preliminary observation.
In conclusion, we demonstrated that, compared to nonembolized liver tissue, the liver specimens obtained from the portal venous embolized liver parenchyma do not have an impaired outcome with respect to cell yield and viability. Considering that a sufficient number of hepatocytes were isolated from diseased livers explanted during liver transplantation and livers rejected from transplantation because of severe steatosis or cirrhosis,26–28,44,45 the liver parenchyma treated with PVE is a suitable cell source that assures good cell yield with excellent viability.
Footnotes
Acknowledgments
The authors thank all members of the group for their excellent assistance. This study was funded by the German Research Foundation (DFG SA 2Nd151/1-1). The authors confirm that there were no conflicts of interest associated with this publication.
Disclosure Statement
No competing financial interests exist.