
Abstract
Changes in the biological apatite (BAp) c-axis orientation were investigated as a bone quality parameter in bone regeneration using hydroxyapatite/poly ɛ-caprolactone (HA/PCL) composite scaffolds. Three-dimensional (3D) HA/PCL composite scaffolds were fabricated using a layer manufacturing process in three grid sizes (200-, 600-, and 1000 μm) and grafted into the forearm ulna of New Zealand white rabbits. The cross-sectional areas of the bones regenerated from the scaffolds with 600- and 1000-μm grid sizes were significantly larger than those from the scaffold with 200-μm grid sizes, whereas bone mineral density in the regenerated regions did not differ between the three grid sizes. Moreover, the BAp c-axis orientation in the bones regenerated from the scaffolds with grid sizes of 600- and 1000 μm was not significantly different; however, both scaffolds showed enhanced BAp orientation, although the degree of BAp orientation was lower than that in intact bones. In conclusion, HA/PCL composite 3D scaffolds with 600- and 1000-μm grid sizes induced BAp c-axis orientation and showed good bone regeneration behavior in vivo.
Introduction
T
In contrast, recent studies have demonstrated the benefits of bioactive composite scaffolds using poly(
Although bone mineral density (BMD) is an essential index for assessing bone strength and fracture risk, the mechanical properties of bone are in fact determined not only by BMD but also by the other parameters of the bone tissue. 14 NIH consensus had reported that BMD is frequently used as a proxy measure and accounts for ∼70% of bone strength. 15 In particular, the change of BMD in the regenerating bone does not correspond with the recovery of its mechanical property. For example, Ishimoto et al. have reported that the recovery of mechanical property of regenerating bone was delayed when compared with the recovery of BMD of regenerating bone. 16 This report indicates the importance of considering bone quality as an essential factor that affects the bone's mechanical strength in the regenerated bone.
Thus, it is interesting to determine the set of bone quality-related parameters that control the mechanical properties of bone. Among the bone quality-related parameters, we previously reported that the c-axis orientation of biological apatite (BAp) is strongly correlated with bone mechanical functions because BAp shows a hexagonal crystal structure (space group of P63/m) and marked mechanical anisotropy along the a- and c-axis.17,18 The orientation of the BAp c-axis in the bone is nearly parallel to the direction of collagen (Col) fibril extension, 19 and the mechanical function of the bone as a Col/BAp composite can explain the anisotropy depending on the degree of preferential orientation. These observations of bone microstructure strongly indicate that BAp orientation can be used to evaluate intrinsic bone quality.20,21
In this study, we investigated BAp orientation as a bone quality parameter using bone regenerated using 3D HA/PCL composite scaffolds fabricated by LMP. The preferential orientation of BAp crystallites in the regenerated and intact rabbit ulnas was analyzed using a microbeam X-ray diffractometer (μXRD) system. To the best of our knowledge, this is the first study to assess the quality of bones regenerated using a 3D bioactive composite scaffold by studying bone microstructure.
Materials and Methods
Fabrication of HA/PCL scaffolds
PCL (MW = 65,000; Sigma-Aldrich) was dissolved in chloroform (20% wt/vol) at 40°C to prepare a PCL solution. HA (Sigma-Aldrich) was mixed with the PCL solution to prepare HA/PCL composites containing 50 wt% HA using a solvent casting method. The composite paste was extruded from a syringe and stacked layer by layer to fabricate 3D scaffolds with a rectangular grid shape using a robotic layer-manufacturing machine. 3D composite scaffolds were fabricated to have grid sizes of 200-, 600-, and 1000-μm (hereafter referred to as 200-, 600-, and 1000-μm scaffolds, respectively) (Fig. 1). The layer-manufactured scaffolds were rinsed in distilled water for at least 48 h and freeze dried for 72 h to completely remove residual solvent, such as chloroform. The experimental processes have been described previously and these scaffolds fabricated by this processes also show biocompatibility.12,13

HA/PCL composite scaffolds with various grid sizes produced by layer manufacturing process. Scaffolds with
Specimen preparation
All animal studies were approved by the Animal Core Committee at the Laboratory Animal Center of Osaka University Graduate School of Engineering. Twelve New Zealand white rabbits (male, ∼3 kg; CLEA Japan, Inc.) were used in this study. A 3-mm defect was introduced at the center of the ulna so that three different scaffolds could be grafted. After 24 weeks of regeneration after grafting, the forearm radius and ulna were simultaneously extracted and the tissues were fixed in 10% neutral-buffered formalin solution. The bone samples were then cut from the proximal region (Prox., elbow side) to the distal region (Dist., wrist side) with a 200-μm band saw (EXAKT Diamond Precision Cutting Systems, BS-300CP; Meiwa Fosis), and the samples were mechanically wet polished with a 2000-grit emery paper embedded with SiC particles.
Analysis of bone regeneration by bone mass evaluation
Bone mass was evaluated using an X-ray radiograph (XIE series; Chubu Medical Co.) and microcomputed tomography (μCT, SMX-100CT, voxel size set to 40 μm per side; Shimadzu). BMD was assessed by peripheral quantitative computed tomography (pQCT, Research SA+, voxel size set to 80 μm; Norland Stratec Medizintechnik GmbH). pQCT instrument was calibrated with a HA phantom of known density. The cortical bone region was defined by setting the threshold to 690 mg/cm3. 22 A 3D bone morphology model was reconstructed using 3D visualization software (VGStudio; Volume Graphics GmbH) based on μCT imaging.
Analysis of preferential orientation of the BAp c-axis
BAp orientation in bone samples was analyzed using a μXRD (D8 DISCOVER with GADDS; Bruker AXS). Cu-Kα (λ = 0.1542 nm) radiation at a tube voltage of 40 kV and tube current of 40 mA was used. The bone surface in the region of 500 μm was analyzed using parallel incident X-ray beams focused down to 100 μm by a monocapillary collimator. The specimen was swung and rotated at an appropriate angle range to obtain sufficient diffraction intensity along the bone's longitudinal axis: 13–20° for the ω axis and 0–360° for the Φ axis. The ω axis changes the incident angle and the Φ axis indicates the rotation of the specimen. Reflections were detected in the region where the normal vector to the (002) and (310) diffraction surfaces in the BAp crystals was tilted from that to the specimen surface by 7° or less. All diffracted X-rays were detected at various scattering Bragg angles of 2θ using a two-dimensional detector (HI-STAR; Bruker AXS). The detected radiation was counted for 1.2 Ks to obtain an appropriate XRD profile. Preferential orientation of the BAp c-axis was defined as a relative integrated intensity ratio of the (002) peak to the (310) peak obtained from the XRD profile. The experimental conditions have been described previously. 21 Measurements were performed on the cortical bone of the ulnar cross-section and the results were averaged. BAp orientation in each sample was measured five times. Moreover, the BAp orientation in the regenerated bone in each sample was compared with the degree of orientation of randomly oriented HA (NIST #2910) powder.
Statistical analysis
All data are presented as the mean ± standard deviations (SDs). Two-tailed unpaired Student's t test was performed, and p < 0.05 was considered statistically significant. SPSS version 14.0J software (SPSS, Inc.) was used for statistical analysis.
Results
Bone regeneration by 3D HA/PCL scaffolds
Bone regeneration by each of the three composite scaffolds after 24 weeks from introduction of the bone defect is shown in Figure 2. Although 24 weeks is a sufficient regeneration period after surgery, radiographic (Fig. 2a–c) and μCT (Fig. 2d–f) analyses indicated that the 200-μm scaffold had lower regenerative capacity than the 600- and 1000-μm scaffolds. pQCT was used to determine bone quantity to evaluate the degree of bone regeneration. The BMD of the cortical bone observed showed a threshold >690 mg/cm3, indicating that the degree of bone regeneration was much higher for the 600- and 1000-μm scaffolds than for the 200-μm scaffold (Fig. 2g–i). Only HA component of the HA/PCL scaffold was filmed on μCT images because PCL is a polymer material. Thus, residual HA of the scaffold was confirmed around the regenerated regions as shown by yellow arrows in Figure 2d–f. Moreover, pQCT images of the same regions from μCT images show low density area as shown by black arrows in Figure 2g–i. Therefore, for BMD analysis of regenerated bone, the influence of the residual HA in the scaffold could be removed when the cortical bone was analyzed because the BMD of residual HA was <690 mg/cm3, which is the threshold.
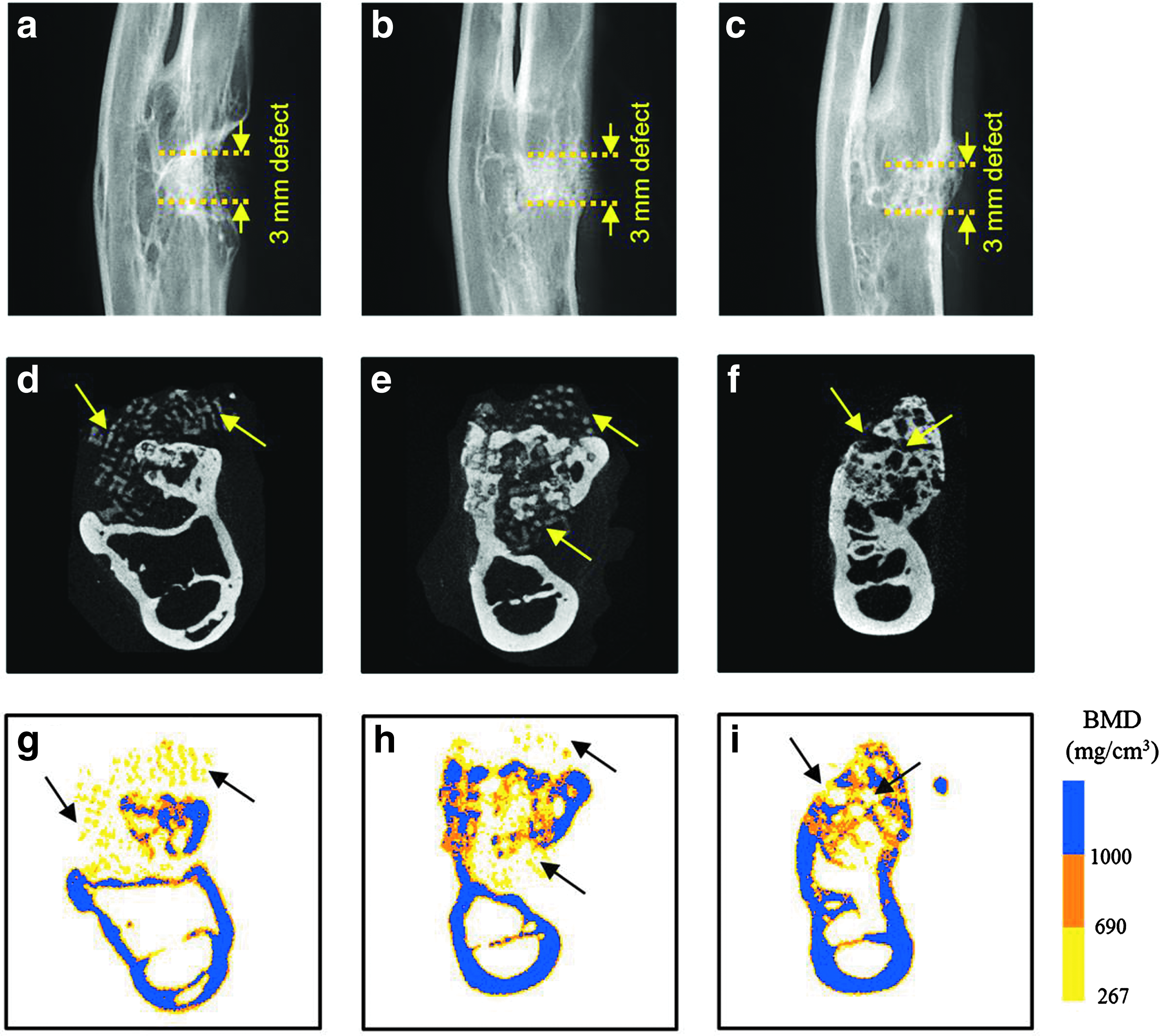
Radiographic, μCT, and pQCT images of rabbit ulna middiaphysis with 3D HA/PCL composite scaffolds at 24 weeks after operation.
Quantitative analysis of bone regeneration
Figure 3 shows the cross-sectional areas (CSAs) and BMD of the regenerated regions determined by pQCT. CSAs of the regenerated regions of the 200-μm scaffold were significantly lower than those of the 600- and 1000-μm scaffolds, whereas BMD of the regenerated regions showed no difference between the three scaffolds.
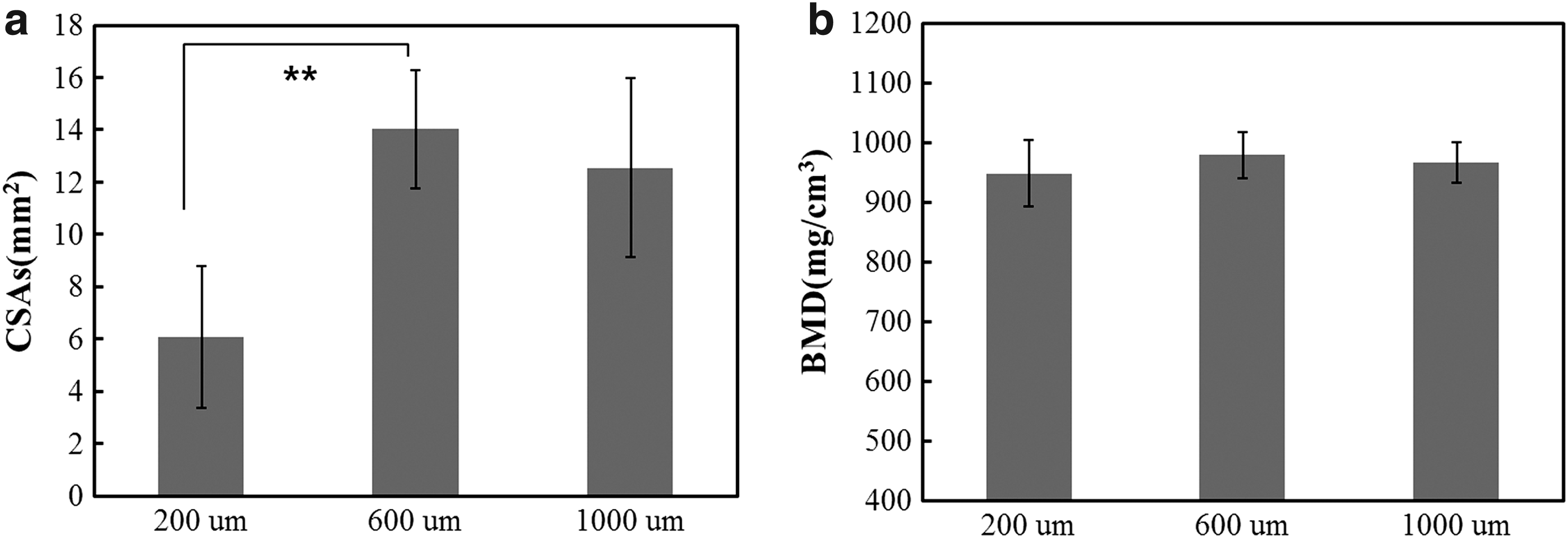
Quantitative analysis of bones regenerated from scaffolds with 200-, 600-, and 1000-μm grid sizes.
μCT images of regenerated regions
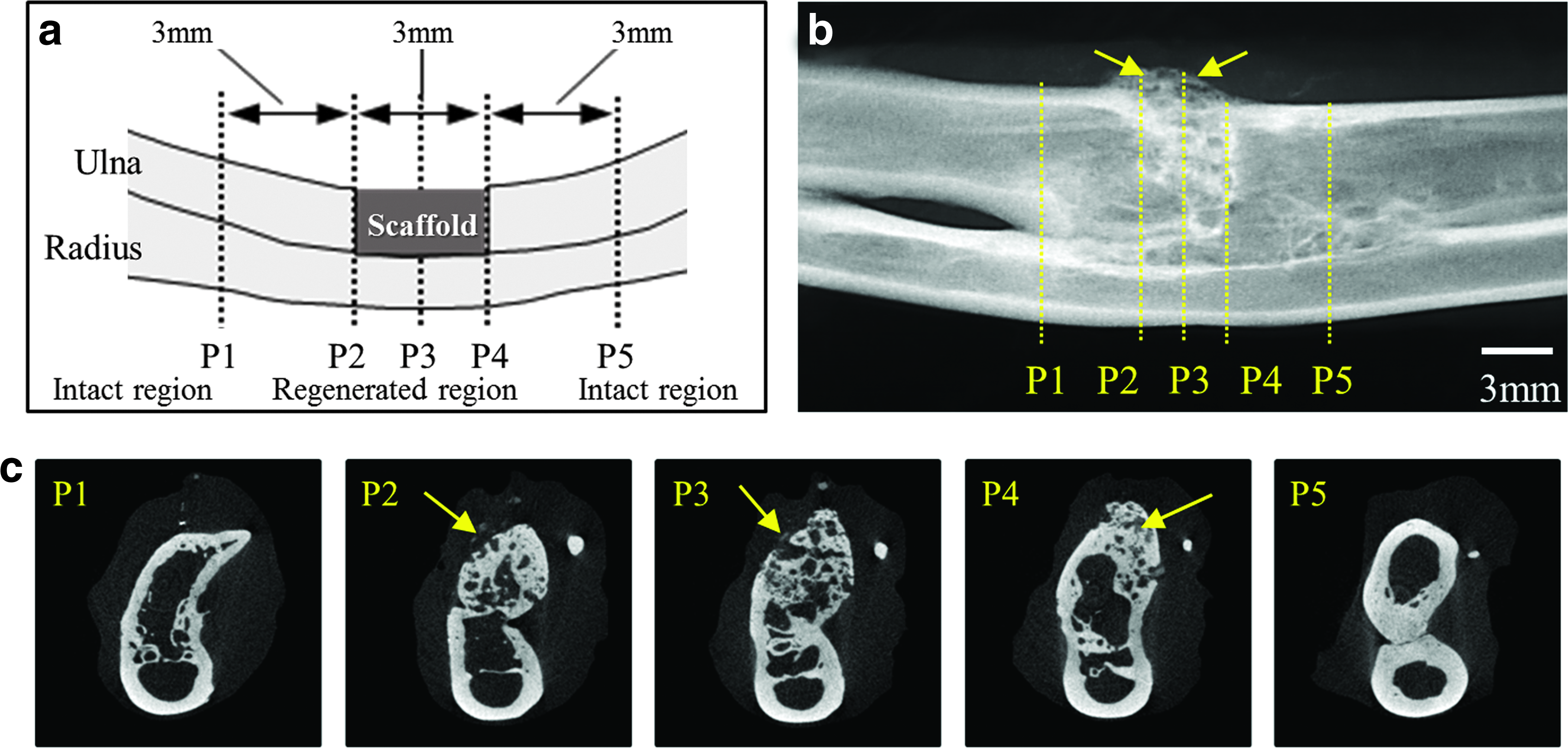
X-ray and μCT images of the regenerated regions from the 200-μm scaffold and areas away from the regenerated regions are shown in Figure 4. Figure 4b shows the radiographic image and Figure 4c shows the μCT image of the sliced plane direction for cross-sectional image analysis. The locations of sliced regions are marked P1–5 from the proximal regions of the ulna to the distal regions to expose the cross-sections (Fig. 4c). The areas proximal to the edges of the scaffold are P2 and P4. P1 and P5 indicate the intact regions away from the implanted scaffolds, and P3 is the part near the center of the scaffold (Fig. 4a). Figure 5 shows the soft X-ray and μCT images of the regenerated regions from the 600-μm scaffold. The location of the sliced regions is the same as shown in Figure 4. In the CT images (Fig. 5c), the contrast of regenerated regions in the ulna (P2, P3, and P4) was similar to the contrast of intact bone in the ulna (P1 and P5). And the regenerated regions showed a form of cortical bone and marrow cavity compared with the regenerated regions on the 200-μm scaffold (Fig. 4c). Thus, these indicate that new bones were well formed in the regenerated region. And residual HA component was observed in the regenerated region (arrows in Fig. 5c). These results indicate that the 600-μm scaffolds, with their well-interconnected pores, had a positive effect on new bone formation. 23 Figure 6 shows the soft X-ray and μCT images of the regenerated regions from the 1000-μm scaffold. The location of the sliced regions is the same as shown in Figure 4. New bones in the regenerated regions on the 1000-μm scaffold were well formed (P2, P3, and P4) and residual HA/PCL composites were observed in the regenerated region (arrows in Fig. 6c). These results indicate that the 200-μm scaffold had lower regenerative capacity than the 600- and 1000-μm scaffold. As a result, the 600- and 1000-μm scaffold with the well-interconnected pores had a positive effect on new bone formation.
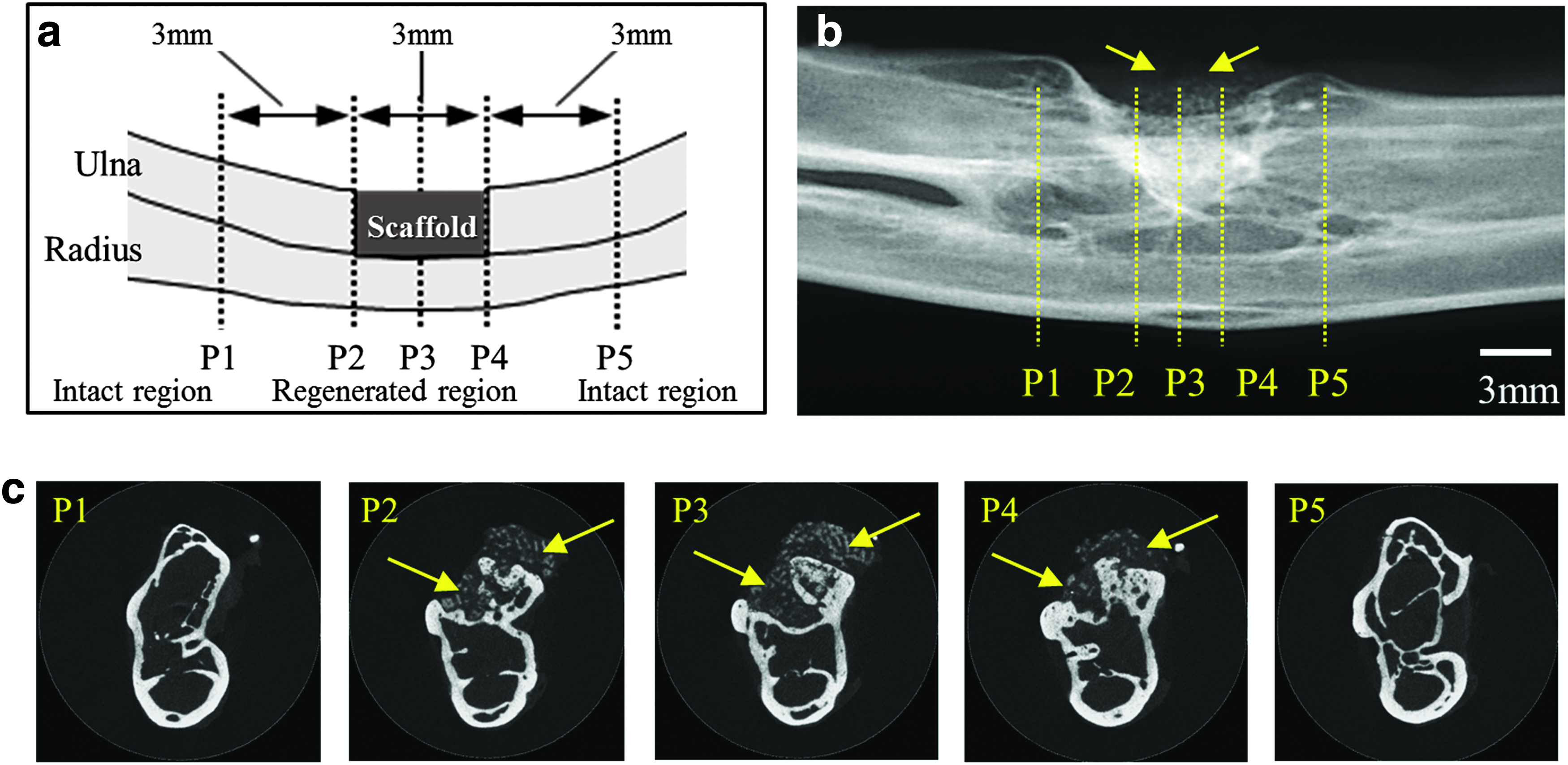
Radiographic and μCT images of bones regenerated using 3D HA/PCL composite scaffolds with 200-μm grid sizes.
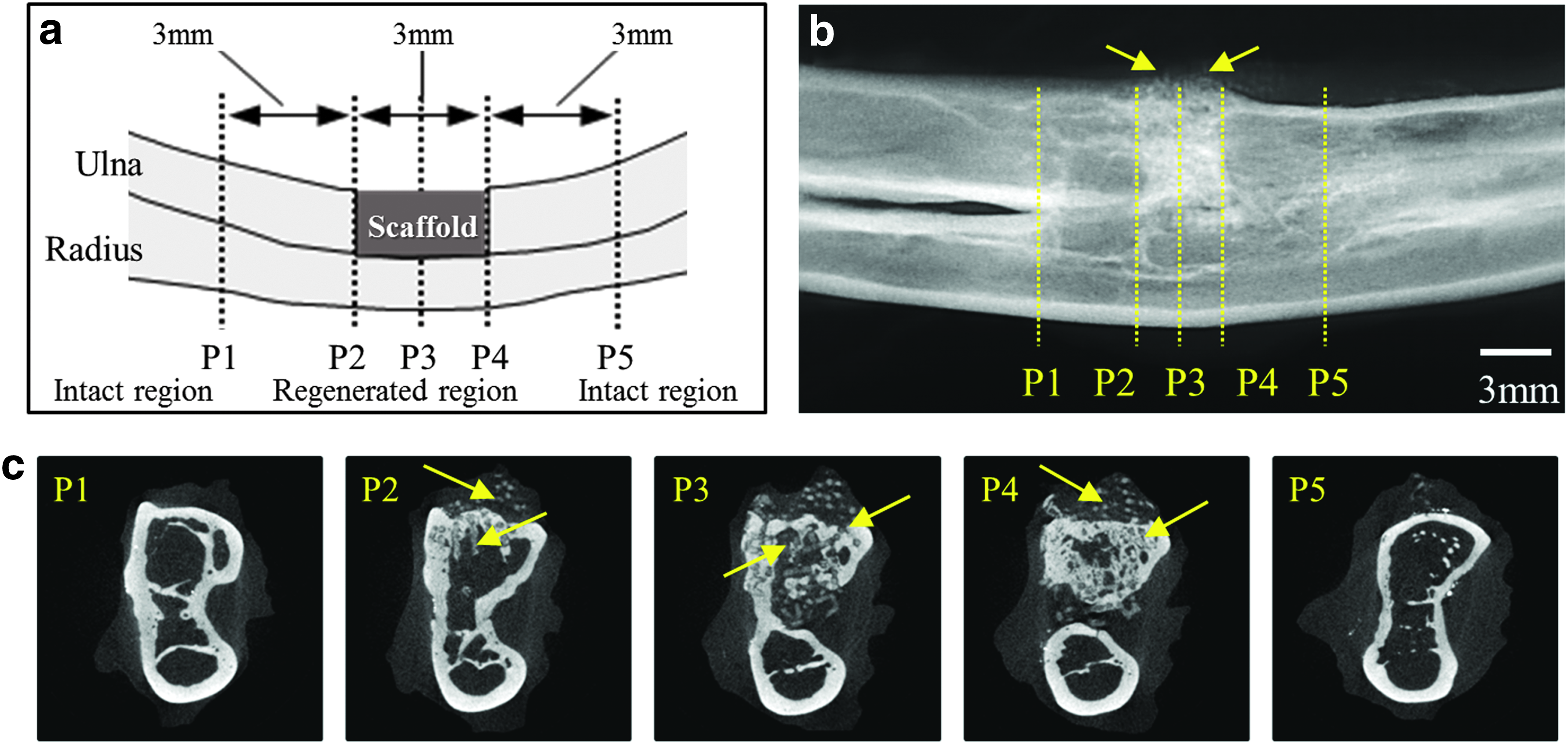
Radiographic and μCT images of bones regenerated using 3D HA/PCL composite scaffolds with 600-μm grid sizes.
Radiographic and μCT images of bones regenerated using 3D HA/PCL composite scaffolds with 1000-μm grid sizes.
Analysis of preferential BAp c-axis orientation
The five red points shown in Figure 7a indicate the measurement points of the BAp c-axis orientation along the longitudinal axis in the regenerated area (P2, P3, and P4) and intact cortical bone (P1 and P5). Figure 7b–d shows the BAp orientation at the regenerated regions and intact regions of the 200-, 600-, and 1000-μm scaffolds, respectively. In the previous study, during the early phase of regeneration of rabbit ulna (from 2 to 4 weeks), BAp orientation in the regenerated bone was lower than that of the intact bone, and continuous increase was observed until 24 weeks in the BAp orientation. 16 Therefore, we focused on the one point of 24 weeks postimplantation and analyzed and compared three different pore sizes of 3D scaffold. The degree of orientation of randomly oriented HA powder was 0.49 ± 0.03; thus, the degree for BAp orientation in the regenerated regions was >0.5, indicating c-axis orientation along the bone longitudinal direction. The regenerated regions, including the area proximal to the edge of the scaffold and the area near the center of the scaffold (P2, P3, and P4), showed lower degrees of BAp orientation than intact regions (P1 and P5) in the 200- (Fig. 7b), 600- (Fig. 7c), and 1000-μm (Fig. 7d) scaffolds. The degree of BAp orientation in the regenerated regions of 200-μm scaffold, including the area proximal to the edge of the scaffold and the area near the center of the scaffold (P2, P3, and P4), showed no significant difference compared with random orientation (HA powder) (Fig. 7b). However, the degree of BAp orientation in the regenerated regions of 600- and 1000-μm scaffolds showed significantly higher BAp orientation than the random orientation (Fig. 7c, d). Although the degree of BAp orientation was not so high, the degree was statistically higher than that for HA powder (p < 0.05).
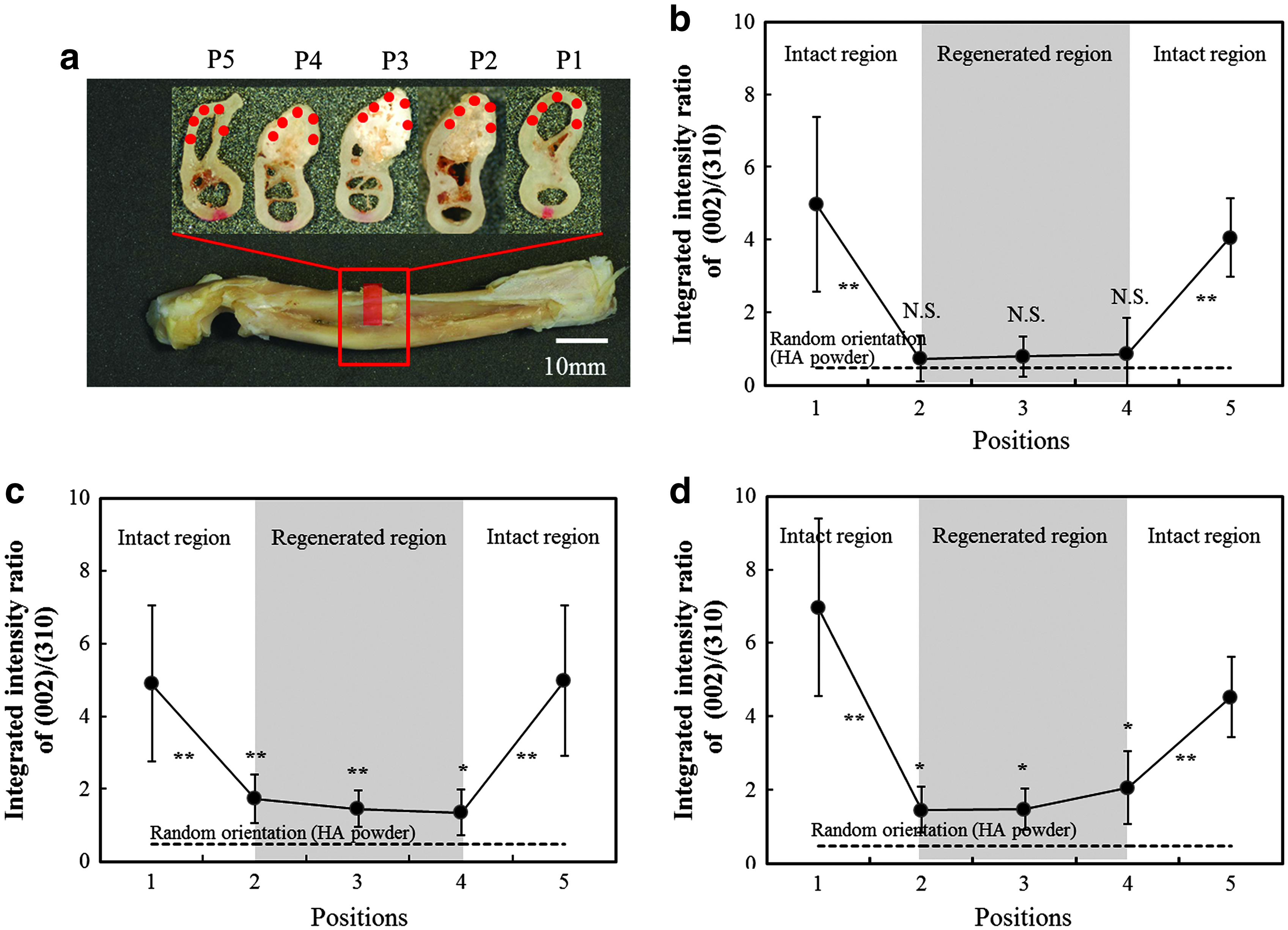
Orientation of BAp c-axis in the intact and regenerated areas.
Discussion
HA/PCL composite is a biocompatible, biodegradable, biologically active, and osteoconductive material,24,25 and HA is the major component of the mineral phase in bony tissue. Moreover, the results of in vivo test confirmed that there was no severe inflammation or adverse tissue reaction associated with the material implantation as shown in the previous report. 13 Therefore, HA/PCL composite can be used as an effective scaffold for bone regeneration.26,27 Using this composite, we designed a 3D scaffold with interconnected and uniaxially elongated pores for optimal bone regeneration.
In this study, we first investigated bone quality by determining the crystallographic orientation of nanoscale BAp crystals in bone regenerated from the 3D scaffolds. We previously fabricated HA/PCL composite 3D scaffolds with well-interconnected pores using LMP, which promoted stress shielding reduction owing to its low compressive modulus.12,13 The 200-μm scaffold showed lower regenerative capacity than 600- and 1000-μm scaffolds (Fig. 2). Moreover, quantitative analysis of CSAs of the 200-, 600-, and 1000-μm scaffolds showed that the 200-μm scaffold had smaller regenerated regions than the 600- and 1000-μm scaffolds did. The CSAs of the regenerated bone were not significantly different between the 600- and 1000-μm scaffolds (Fig. 3). Thus, the 600- and 1000-μm scaffolds showed similar bone regenerative capacity.
BAp orientation in the bone regenerated from the 600- and 1000-μm scaffolds was confirmed by the μXRD method (Fig. 7). This method is especially powerful for analyzing pathological bone tissue, such as in osteoporosis, 28 osteopetrosis, 21 and osteoarthritis. 29 We have previously reported that BAp in rabbit ulna (long bone) was oriented along the longitudinal axis, whereas HA powder showed the random orientation. 17 In this study, regenerated bone in the 200-μm scaffold exhibited the lowest degree of BAp orientation, which was significantly lower than that of the 600- and 1000-μm scaffolds. Moreover, degree of BAp orientation in the bone regenerated from the 600- and 1000-μm scaffolds was significantly higher than that for the HA powder, although it was slightly lower than that for intact bone. Total BAp orientation in the regenerated bone was determined by BAp orientation of new bone and the residual HA in the scaffolds, which has lowest degree of BAp orientation (0.39 ± 1.66), similar to HA powder. As a result, BAp orientation in the regenerated bone may be reflected by the influence of the residual HA in the scaffold. Thus, although the average BAp orientation in the regenerated bone decreased, the degree of BAp orientation was significantly higher than that of HA powder (p < 0.05). Therefore, the 600- and 1000-μm scaffolds induced preferential BAp c-axis orientation in the regenerated bone. The optimal pore size of 3D scaffold for bone regeneration is still controversial as there have been conflicting reports.30,31 In several reports, the pore size of ceramic scaffold for bone regeneration has varied from 20- to 1000-μm.32–34 The scaffold had pore size larger than 300-μm, which has been previously reported as the threshold pore size required for Haversian ingrowth. 35 Moreover, pore size larger than 300 μm is recommended for promoting vascularization and new bone formation.36–38 Furthermore, the height and diameter of column of scaffolds are also important factors for bone regeneration. We reported that BAp orientation of regenerated bone was dependent on the height of column of scaffolds. 39 In this study, the 200-μm scaffolds revealed low CSAs and the lowest degree of BAp orientation in the regenerated regions as shown in Figure 7b. In contrast, BAp orientation was induced in regenerated bone by the 600- and 1000-μm scaffold. These results indicated that the geometry of scaffold with suitable grid size is important for inducing new bone formation. In general, new bone growth into porous scaffolds depends on several factors, such as pore (grid) size, scaffold porosity, and interconnecting pores.40–44 Introducing well-controlled, highly interconnected porosity into scaffold materials can confer permeability, facilitate the diffusion of oxygen and nutrients, and create a 3D vascular network.41,45 Moreover, interconnected pore networks contribute to osteoblast proliferation, bone ingrowth, and angiogenesis into the scaffold. 45 Recently, Matsugaki et al. reported that the migration of osteoblasts could facilitate anisotropic morphogenesis in bone tissue, which is the formation of a highly anisotropic microstructure comprising BAp and Col fibrils. 46 Therefore, the induction of BAp orientation by 600- and 1000-μm scaffolds used in this study might be associated with the microenvironment in the HA/PCL 3D scaffold as already mentioned. Thus, findings from this study provide new understanding of induction of BAp orientation in the biodegradable HA/PCL 3D scaffolds. Importantly, analysis of BAp c-axis orientation is one of the most remarkable methods for bone tissue engineering.
Conclusions
We analyzed the bones regenerated using HA/PCL composite 3D scaffolds in the rabbit ulna. HA/PCL 3D scaffolds with unidirectional pores connected the defective regions with new bone, and the 200-μm scaffold showed lower regenerative capacity than the 600- and 1000-μm scaffolds did. The crystallographic orientation of the BAp c-axis was used as a quality parameter for the regenerated bone. Regenerated bone in the 200-μm scaffold exhibited the lowest degree of BAp orientation, which was significantly lower than that of the 600- and 1000-μm scaffolds. The 600- and 1000-μm scaffolds with unidirectional pores showed low degrees of BAp orientation, but the orientation was higher than that for HA powder. These findings strongly suggest that HA/PCL 3D scaffolds with grid size >600 μm can induce BAp c-axis orientation similar to the bone microstructure in intact long bones and may be suitable as bone substitutes.
Footnotes
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research (S) from the Japan Society for Promotion of Science (Grant No. 25220912) and basic science research program through the National Research Foundation of Korea (NRF) (2009-0093814).
Disclosure Statement
No competing financial interests exist.