
Abstract
Due to the poor regenerative capacity of adult mammalian skin, there is a need to develop effective skin substitutes for promoting skin regeneration after a severe wound. However, the complexity of skin biology has made it difficult to enable perfect regeneration of skin. Thus, animal models are being used to test potential skin substitutes. Murine models are valuable but their healing process involves dermal contraction. We have developed a device called a dome that is able to eliminate the contraction effect of rodent skin while simultaneously housing a bioengineered skin graft. The dome comes in two models, which enables researchers to evaluate the cells that contribute in wound healing from neighboring intact tissue during skin healing/regeneration. This protocol simplifies grafting of skin substitutes, eliminates the contraction effect of surrounding skin, and summarizes a simple method for animal surgery for wound healing and skin regeneration studies.
Introduction
S
Animal models that replicate the healing process of humans are of great importance to study skin regeneration and test the efficacy of skin substitutes. Several studies showed the direct contribution of cells from surrounding intact skin during skin healing.3,8–11 Porcine is an accepted model that closely mimics wound healing observed in humans and is used to study potential mechanisms and therapeutics. The thickness of the epidermal and dermal layer of porcine skin closely matches that of humans. 12 In addition, the composition of the lipid film of the skin surface, resemblance in hair coat, and attachment to underlying structures is very similar. Examining underneath the skin, there are additional similarities between pigs and humans, such as the vasculature, epidermal enzyme patterns, epidermal tissue turnover, and keratinous proteins.12,13 However, pigs are prone to a higher risk of infection and the housing and maintenance of these animals are laborious and costly. It is essential to screen in larger number of skin substitutes in smaller animals before examining their efficiency in bigger animals such as porcine. An inexpensive and easily accessible alternative animal model is the mouse. Murine models heal substantially faster and have a competent immune system making the morbidity of mice in wound research quite low.14,15 A paramount advantage of mice is the ability to develop transgenic and knockout models that enable researchers to investigate the molecular pathways controlling wound healing and skin regeneration. As a result, excisional wound healing models have been developed but not without their own limitations, especially in rodents.14,16
Structural and immunological comparisons of human and mouse skin
Human and murine skin have numerous similarities and differences.17,18 Human and mouse skin both are divided into layers. These layers include the epidermis, dermis, and subcutis.
The epidermis is mainly consisting of keratinocytes. The dermis is made up of extracellular matrix components, small blood vessels, and various immune cells. Whereas, the subcutaneous layer is composed of adipocytes, hair follicles, sebaceous glands, and sweat glands that are spread throughout the three layers. 19
However, mouse skin is relatively thinner, at only one-quarter the thickness of human skin. 20 Human epidermis has 5 to 10 layers of keratinocytes, compared with the two to three layers in mice. Thus, the turnover of the epidermis is much faster in the skin of mice. Furthermore, there is a high density of hair follicles distributed throughout, whereas human skin contains less hair follicles and is mainly interfollicular. 21 Furthermore, mouse skin is more regenerative as they do not develop keloids or significant scarring.20,22
Although there is a large overlap in the type of immune cells found in the skin of both mice and humans, such as macrophages, mast cells, αβ T cells, and additional innate lymphoid cells, 26 differences exist as well. For example, there are subtypes of dendritic cells in mice, such as CD8+ dendritic cells and dendritic epidermal T cells, and other inflammatory cells such as NK1.1+ T cells that are nonexistent in humans.23–25 These structural and immunological differences have an impact on wound healing. However, it is the observed wound contraction in mice that makes it particularly difficult to translate findings in mice to humans, as is discussed below.
Limitations of current rodent excisional wound healing models
The wound healing process in rodent models is different than that of humans, predominantly due to the process of contraction that is observed in rodents. This contractile activity is due to the ancillary muscle layer called the panniculus carnosus.12,14,16 This additional muscle layer permits rapid contraction of the skin in response to a wound, independent of deeper muscle layers, resulting in swift closure of any deformities. In contrast, the major mechanism of healing in humans involves reepithelialization and granulation tissue formation. As a result, studying skin regeneration in animal models such as rodents has been troublesome. During skin regeneration studies, it is essential to minimize any confounding factors, which might hide the regenerative capacity of the grafted skin substitute. As such, a method that can minimize this effect would be an important asset for investigating skin regeneration and the efficacies of skin substitutes. Therefore, it is essential to develop a better method that can first prevent dermal contraction and second encase a skin substitute.
Applications of the dome
Current methods for eliminating contraction in rodent wound healing involves suturing a silicone ring around the wounded area, which may induce inflammation in the local area and still allow for some contraction to occur.14,27 In addition, the use of adhesive dressings has also been attempted but its effect in restricting skin contraction is brief. Current methods and protocols make it difficult to apply a skin substitute, which can be very delicate, on animal models, resulting in a more vexatious surgery.14,27–29 The advantage of our dome is that the shoulder is placed directly underneath the skin; thus, the elastic skin itself fixes the dome to the mouse, eliminating any need for suturing. Afterward, the application of an adhesive, such as tissue glue, secures the dome to the dorsum and seals any openings outside of the dome itself. Our group has already used domes as a method of adhering a skin substitute to mice with high efficacy. 30 We used a skin substitute, which was composed of fibroblasts and keratinocytes in a scaffold. These cells can potentially reconstitute the dermal component of skin.3,31
Through the use of the dome, bioengineered skin grafts are safely housed and can be easily inserted into the wound area while effectively reducing dermal contraction in rodents.
Materials and Methods
Characteristics of the dome
To address wound contraction in rodents and concurrently encapsulate a skin substitute, we have developed two types of dome apparatuses made of Accura® ClearVue™ material, which is clear plastic that meets USP class VI standards, a perforated and nonperforated prototype (Fig. 1A, B). Both models have an 8 mm diameter, shoulder of 1.5 mm (shoulder to shoulder diameter of 11 mm), wall thickness of 0.25 mm, except for the top surface, which is 0.5 mm thick. The perforated model has 24 evenly spaced holes along the edge and 6 on the top, all with a diameter of 0.5 mm (Fig. 1B). This dome acts as a secure home for grafting of skin substitutes onto mice (Fig. 1C–E). The dome ensures that skin healing and regeneration is the result of the skin substitute and not contraction of surrounding intact skin.
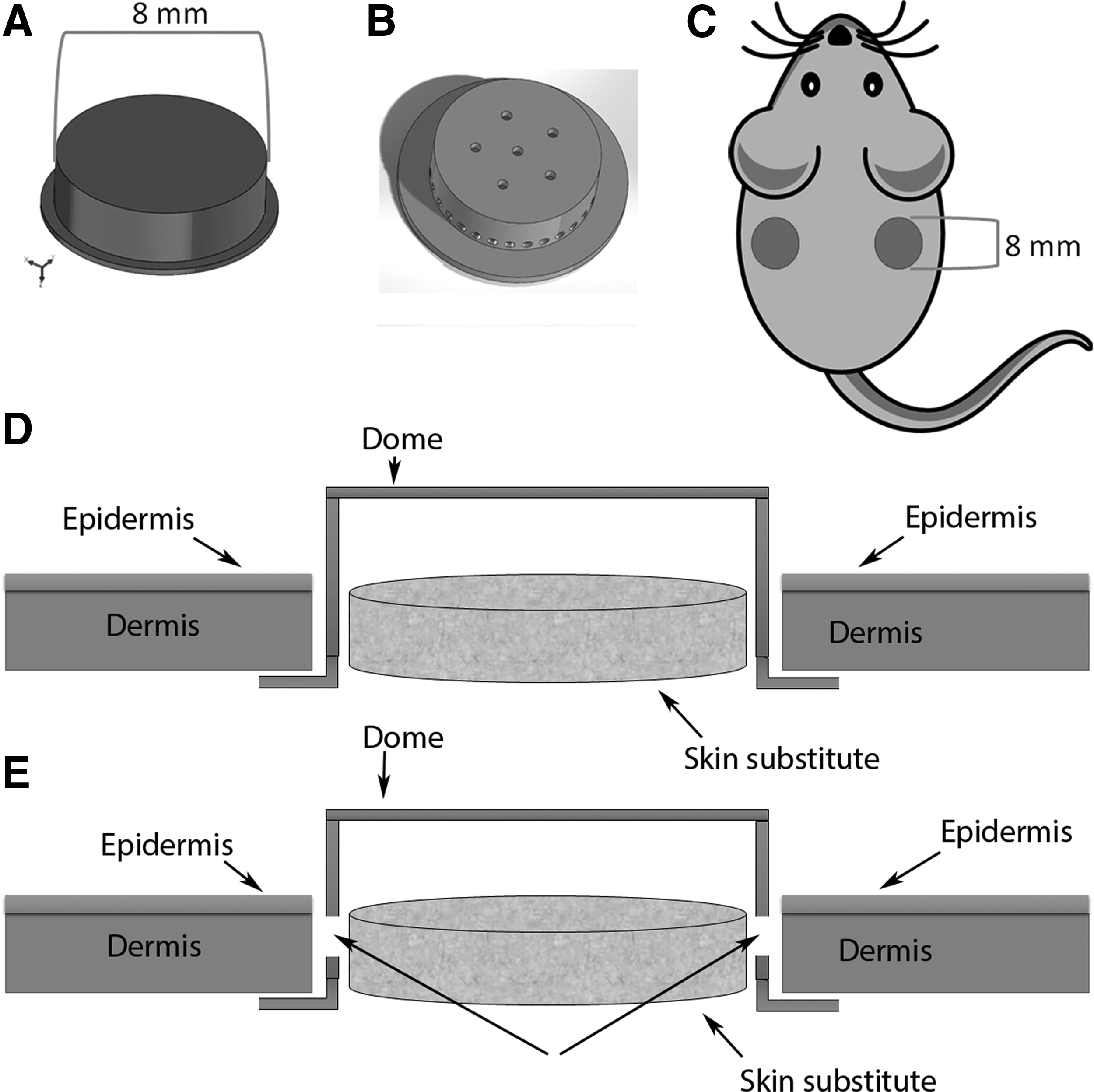
Representation of the dome to be used in skin healing/regeneration studies.
Experimental design
Researchers should note that the dome was developed specifically to house bioengineered skin substitutes and study its impact on skin regeneration. However, in wound healing or pharmacological studies, the dome can be used to evaluate the extent of cell contributions from surrounding intact tissue if that is part of the objectives.
Assuming the dome is suitable for your study, the twin wounds created on the dorsum allow for a treatment and control group both on the same mouse. Thus, one side of the dorsum will contain a dome without the skin substitute and the other side has a dome containing the skin substitute. The researchers will also have to consider if they want the dome to be perforated or not. In our experience, using a nonperforated dome gives us greater insight into if the skin substitute alone is effective in promoting skin regeneration, without the added mobilization of surrounding cells. Depending on the objective of examining the skin substitute, mice can be kept for a period of 2–3 weeks allowing the skin substitute enough time to regenerate the newly formed skin.
Mice
We used wild-type male C57BL/6 mice (10–11 weeks old). Animal experiments conducted in this study conform to the Animal Care and Use Committee of Sunnybrook Research Institute in Toronto, Ontario, Canada. Requirements for The National Institutes of Health Guidelines for the Care and Use of Experimental Animals were fulfilled. The entire protocol must be done under sterile conditions.
Preparation of the dome
The dome was developed at the Sunnybrook Research Institute department of Design and Machining Services. It can be stored at room temperature (24°C) for years. Domes are sterilized by incubating them in 70% ethanol for at least 5 min and air drying in a tissue culture hood followed by UV radiation for 30 min. The domes need to be contained in a sterile container. Due to the composition of the dome, there should not be any heating.
Anesthesia and creation of excisional wound
Before application of the dome, we put the mice under anesthesia (1–2% isofluorane with oxygen) until asleep and put eye gel on the eyes for protection (Fig. 2A). We gave an intraperitoneal injection of the analgesic buprenorphine (0.05–0.1 mg/kg body weight) and proceeded to shave the dorsal surface of the mouse. While the mouse is on its stomach, the skin in the middle of the back was pinched to raise it from the underlying structures, it should move freely (Fig. 2B). While holding the pinched skin, put the mouse on its side then used the biopsy punch to punch through both layers of the skin, including the panniculus carnosus (Fig. 2C). This will result in two equally sized holes on the dorsum. We punched just below the neck of the mouse to try to limit the chewing of the material and dome (Fig. 2D). Size of the wounds should be based on strain of mice, type of skin substitute, and size of the domes to be used.
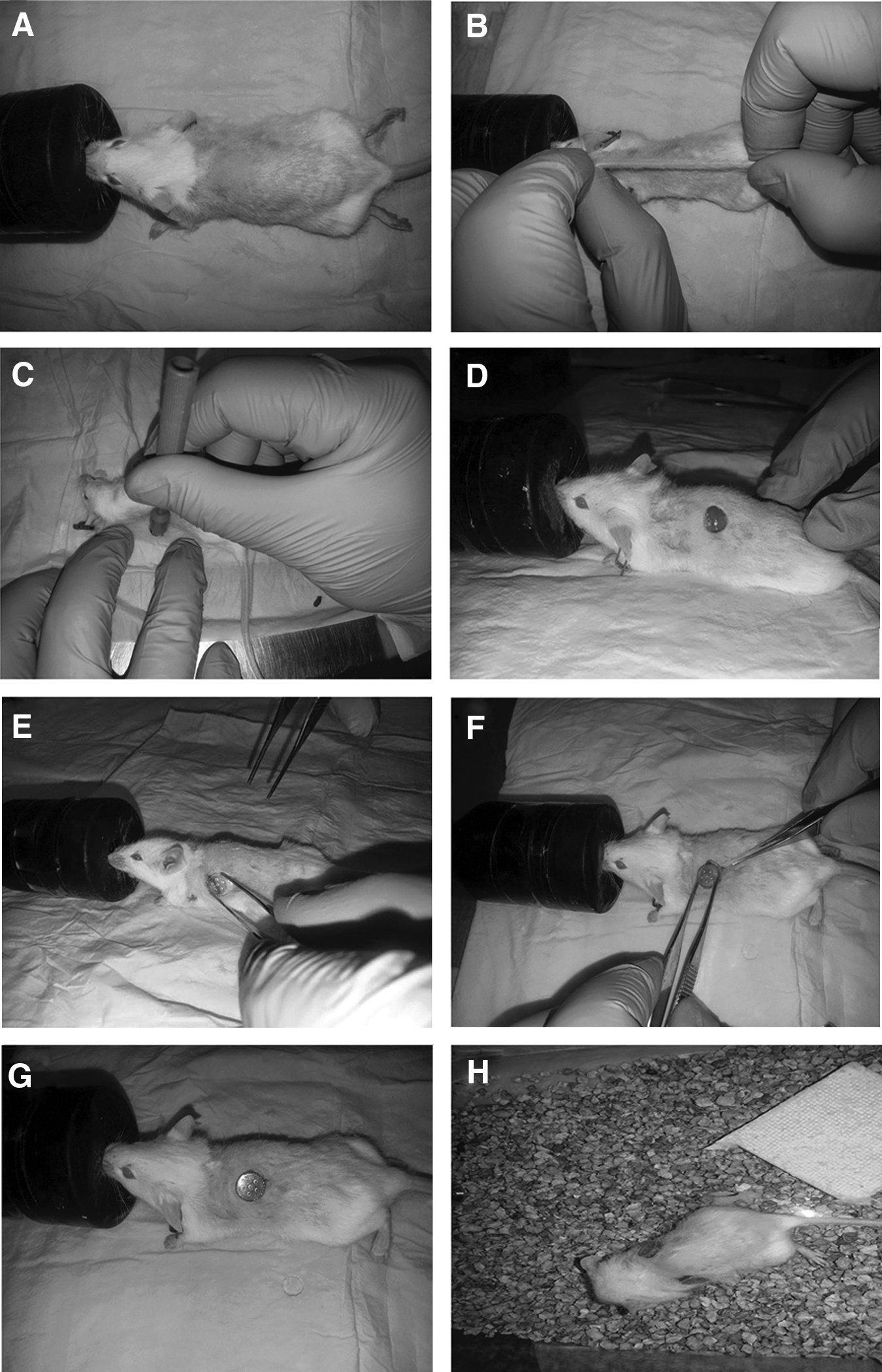
Preparation of the mouse for insertion of the dome.
Grafting of bioengineered skin substitute
If authors are to apply their test material, place it inside the dome before its application on the dorsum of their mice. We used two pairs of forceps, one to lift the skin at the edge of the wound and another to insert the shoulder of the dome underneath (Fig. 2E–H). The shoulder of the dome should be completely covered by surrounding skin. Tissue glue was used to seal the dome to the edges of the skin. Mice were placed under a warming lamp in individual recovery cages to avoid chewing of the dome. Following recovery from anesthesia, the mice were able to return to normal activity with the pair of domes embedded into their dorsum (see Supplementary Video S1; Supplementary Data are available online at
Image acquisition and image analysis
Image capture of skin sections stained via trichrome was done using the Zeiss Axiovert 200 light microscope at 20× and 40× magnification for quantification.
Harvesting of skin and histological analysis of wounds
Harvest the full wound from the dorsum of the back and fix in 10% formalin. The samples are then paraffin-embedded and placed on slides. Masson's trichrome staining was used for histological analysis. Paraffin-embedded slides were heated at 60°C then deparaffinized through citrosol and rehydrated through decreasing grades of ethanol. Slides were kept for 1 h in Bouin's solution at 56°C. Stain slides were consecutively in Weigert's iron hematoxylin solution, Biebrich scarlet-acid fuchsin solution, phosphomolybdic–phosphotungstic acid solution, and aniline blue solution.
Imaging and measurement of wound size
Sections stained via Masson's Trichrome were imaged using Axiovert 200 light microscope at 20× and 40× magnification for quantification. ImageJ was used to measure the length of the wound bed, which is evident by a lack of dark blue collagen staining.
Results
The reduction in healing through contraction enables an alternative method of recovery, which involves epithelialization and granulation tissue formation. 14 When we used the perforated dome for surgery, we observe that the newly formed skin is composed of almost a complete keratinization and constitution of granulation tissue (Fig. 3A). Considering that we did not have any epidermal component in our skin substitute, this suggests that neighboring cells made a large contribution to the wound healing process. Indeed, our perforated dome highlights the necessity of developing a device to limit contraction as well as contribution of surrounding tissue in a tissue regeneration context. The purpose of the nonperforated dome is to diminish the contribution of surrounding cells to the wound healing process to test the efficacy of the encapsulated skin substitute that researchers would want to investigate. When the wounded area is 100% barricaded with the nonperforated dome, we observed no keratinization with some extent of granulation tissue formation (Fig. 3B).
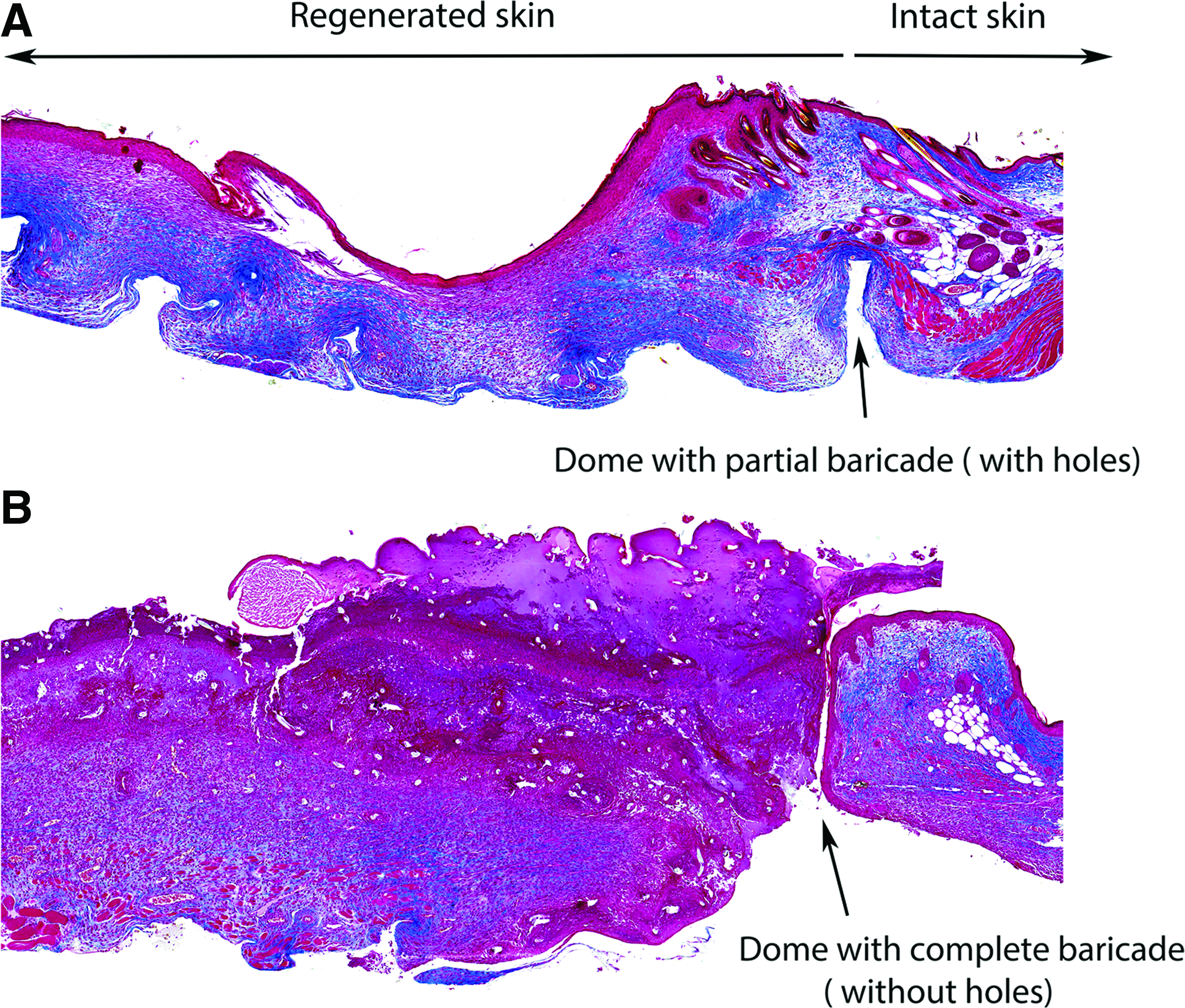
Masson's trichrome staining of regenerated skin using a skin substitute housed in a perforated and nonperforated dome.
To evaluate the advantages of our designed dome in preventing skin contraction, we performed excisional wound biopsy and applied the dome solely for preventing dermal contraction. We removed the dome at different time points postsurgery. Our results demonstrate that the wound size is four times larger when the mice have the dome on for 13 days versus 10 days (Fig. 4), showing the importance of keeping the dome on to prevent contraction of the skin and highlighting the significant effect of skin contraction in rodents during skin healing. Our data show that there is a direct correlation between the number of the days that wounds have dome and the final wound size at day 14 postsurgery (Fig. 4).

Number of days mice had the dome on correlate with the wound size (n = 3, correlation coefficient: 0.888, p < 0.0197).
Conclusion
The development of biological and synthetically derived skin substitutes has grown at a rapid rate. The use of mice for skin regeneration studies requires imitating the wound healing process as closely to humans as possible. However, this presents with numerous challenges due to numerous immunological and anatomical differences. One of the ongoing limiting features of mice in recapitulating human dermal wound healing is their capacity for wound contraction. In this study, we were able to show that we can effectively minimize dermal contraction in mice during wound healing without the added inflammation that comes with suturing, which is observed in other models. Furthermore, we developed two prototypes of our dome, which allow us to study the effect of skin substitutes with or without contribution of surrounding cells. We have already shown that this is an advantageous method for wound healing and skin regeneration studies. Further skin substitute studies need to be done with the dome to be validated as a reliable model.
Footnotes
Acknowledgments
We thank Michael Pozzobon and his team at the Sunnybrook Research Institute department of Design and Machining Services for manufacturing the domes.
Author Contributions
M.G.J and S.A.N designed the study. S.A.N, M.G.J, A.R.S and C.B performed the experiment, C.B analyzed the data and A.R.S, M.G.J and S.A.N wrote the manuscript.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.