
Abstract
Surgical site infection (SSI) is the most common cause of surgical failure, increasing the risks of postoperative mortality and morbidity. Recently, it has been reported that the use of antimicrobial dressings at the incision site help with prevention of SSI. Despite the increased body of research on the development of different types of antimicrobial dressings for this application, to our knowledge, nobody has reported a reliable large animal model to evaluate the efficacy of developed materials in a preclinical SSI model. In this study, we developed a porcine full-thickness incision model to investigate SSI caused by methicillin-resistant Staphylococcus aureus (MRSA), the leading cause of SSI in the United States. Using this model, we then evaluated the efficacy of our newly developed silver releasing nanofibrous dressings for preventing and inhibiting MRSA infection. Our results confirmed the ease and practicality of a new porcine model as an in vivo platform for evaluation of biomaterials for SSI. Using this model, we found that our silver releasing scaffolds significantly reduced bacterial growth in wounds inoculated with MRSA relative to nontreated controls and to wounds treated with the gold standard, silver sulfadiazine, without causing inflammation at the wound site. Findings from this study confirm the potential of our silver-releasing nanofibrous scaffolds for treatment/prevention of SSI, and introduce a new porcine model for in vivo evaluation of additional SSI treatment approaches.
Introduction
A
One possible treatment that was not considered in the SCIP guidelines is the use of postoperative dressings in addition to systemic antibiotics. 7 Recently, it has been shown that placement of antimicrobial dressings at the time of incision closure may represent the next step in prevention of SSI. 10 To this end, silver incorporated dressings have garnered increased interest.10,11 Unlike many antibiotics, bacterial resistance to silver is very rare.10,12,13
Different forms of silver are often used at incision sites. The most popular silver containing treatments include silver sulfadiazine (SSD), a cream containing silver salt; Acticoat® (Smith & Nephew, Inc.), a silver nanocrystalline containing dressing; and products with sustained release of silver such as Silverlon® (Argentum Medical LLC) or Aquacel® (ConvaTec, Inc.). In general, these topical silver treatments are applied on top of the wounds after the sites are surgically closed. Antimicrobial creams such as SSD (the gold standard) usually need to be reapplied multiple times postsurgery. Dressings containing silver are typically placed on top of the wound site and held in place with the aid of a secondary dressing or tape/bandage. Such treatments therefore create a barrier to the wound site by preventing bacterial entry into the wound site. Some silver may also leach into the wound through the incision site.
Although the use of silver dressings and topical creams in surgeries is becoming more prevalent, there are drawbacks associated with these approaches. One of the major concerns when using silver on the skin is argyria, a condition caused by inappropriate exposure to silver. 14 For instance, it has been shown that Acticoat is cytotoxic to keratinocytes 15 and causes argyria-like symptoms in burn patients. 16 Therefore, when designing silver dressings, it is essential to use the right form and concentration of silver.
We recently developed a novel antimicrobial dressing capable of releasing silver ions at a controlled rate. 17 The dressings comprised polylactic acid (PLA) nanofibers treated with a silver ion releasing coating. We previously showed the cytocompatibility of these dressings in vitro using human epidermal keratinocytes and human dermal fibroblasts. 17 These scaffolds are biocompatible and degradable and therefore can be implanted inside the body without need for a follow-up removal surgery. Thus, these dressings can be used not only as topical dressings but can also be inserted in the incision before closure of the wound site to prevent SSI. Insertion of scaffolds in the wound site negates the need for a secondary bandage and increases patient compliance. A goal of this study was to improve the antimicrobial properties of our scaffolds and evaluate their efficacy as implanted scaffolds in vivo with a physiologically relevant model of an infected incision. The primary goal of this study was to create and evaluate a physiologically relevant, large animal model for investigation of SSI treatment.
The most common and accepted animal model for evaluation of wound healing is the pig, given the well-documented similarities between porcine and human skin.18,19 In particular, the structure and thickness of the dermal and epidermal layers, time for epithelial regeneration, and the physiology of wound healing are very similar between pigs and humans.19–21 Therefore, porcine skin has been used as the gold standard preclinical model for study of human dermal repair. 21 However, the majority of previous wound healing studies use excisional wound models where dressings/scaffolds have been used as an external dressing for the excision site.22–24 Despite the widespread use of porcine skin for dermal repair, to our knowledge there is not a reliable pig model for studying wound infection. To address this need, we developed a new wound infection model in the pig.
Methicillin-resistant staphylococcus aureus (MRSA) was used to cause infection in our model. MRSA was chosen because it has become the leading cause of SSI in U.S. community hospitals. 25 A single case of SSI due to MRSA results in more than $60,000 of additional costs and increases risk of mortality up to sevenfold compared with uninfected controls. 26
The in vivo component of this study was designed in two phases. The first phase of the in vivo evaluations focused on selection of a MRSA concentration that caused infection in the animals, but not lethality of the animals. The second phase of the in vivo evaluations utilized the specific MRSA concentration determined in phase 1 to test antimicrobial efficacy of our nanofibrous silver releasing scaffolds in the SSI model in vivo.
Materials and Methods
Scaffold fabrication
Solid and porous fibers were electrospun as previously described.17,27,28 In brief, solid fibers were created by dissolving PLA (MW: 70,000 g mol−1; NatureWorks, Minnetonka, MN) in dichloromethane. Porous fibers were made with the use of chloroform and dimethyl formamide (all solvents obtained from Sigma, St Louis, MO). Mixtures were stirred at 80°C for 4 h to form an 11 wt% polymeric solution. The solutions were then used in a custom electrospinning system at an applied voltage of 15 kV, feed rate of 0.7 μL h−1, and spinning distance of 13–15 cm. Electrospinning was carried out at the environmental temperature of 30°C and relative humidity of 50% for solid nanofibers and 70% for porous nanofibers. Resultant nanofibers were coated with Silvadur ET (Dow Chemical Company, Midland, MI), at a silver concentration of 62.5 μg mL−1, for 1 h and then dried under a fume hood for 24 h to form a thin layer of antimicrobial coating 17 ; nanofibers were then cut and sterilized with ethylene oxide gas at room temperature for 24 h using the Anprolene AN74J Long Sterilizer System (Cole-Parmer Instrument Company, LCC, IL). After sterilization, the scaffolds were kept in a ventilated area for 2 days to ensure evaporation of any residual ethylene oxide.
Scaffold evaluation
Surface topography of the scaffolds was evaluated using scanning electron microscopy (SEM) (FESEM JEOL 6400 F) at 15 kV accelerating voltage. Scaffolds were sputter coated with gold using a Denton Vacuum Desk IV sputter coater to observe their surface morphology using SEM. Average fiber diameter was calculated using at least 30 measurements on different fibers of the web.
Percent moisture content analyses were performed by measuring the weight of scaffolds (n = 5) before and after submerging them in deionized water for 1 h. The following formula was used to calculate the percent moisture content:
In vitro analyses of antimicrobial efficacy of scaffolds
American Association of Textile Chemists and Colorists (AATCC) 147 protocol for disc diffusion test was utilized for in vitro antimicrobial analyses. Scaffolds (n = 3) were cut into circles (d = 1.6 cm), and directly placed onto a Mueller-Hinton (MH) agar (Difco Laboratories, Detroit, MI) plate inoculated with 0.5 McFarland suspension of MRSA bacteria (HPV107, ATCC® BAA-44™; Manassas, VA) in phosphate-buffered saline (PBS). Plates were then incubated overnight at 37°C with 5% CO2. Bacteriostatic activity was visually evaluated to determine the zone of inhibition around the scaffold.
Preparation of MRSA bacterial solutions for in vivo analyses
Commercially available MRSA strain (HPV107, ATCC BAA-44; Manassas, VA) was used for phase 1 of the in vivo evaluations. Bacteria were grown in cation-adjusted MH broth (Difco Laboratories) and plated on BBL™ Trypticase™ soy agar plates (Fisher Scientific). Inoculated agar plates were then incubated at 37°C and 5% CO2 overnight. After 24 h of incubation, five colonies were harvested from each plate and inoculated into 10 mL of MH broth. The broth was again incubated for 24 h at 37°C and 5% CO2. The bacterial concentration in each of the five samples was then estimated by determining the optical density of the bacterial suspension, using a UV–Vis spectrophotometer (Biomate3; ThermoElectron Corporation) at a wavelength of 600 nm. To confirm starting concentrations, an aliquot of the enrichment was serially diluted 10-fold into PBS and plated onto agar plates, in triplicate. Plates were incubated at 37°C and 5% CO2, and colonies were counted after 24 h. The enriched MRSA inoculum and dilutions were then transported to the surgical suite in cold storage (−4°C).
Surgical procedure
All animal procedures were approved by the Institutional Animal Care and Use Committee (IACUC) at North Carolina State University (IACUC No. 12-147-B). Six 45–50 kg female pigs (Yorkshire Crosses; Teaching Animal Unit, Raleigh, NC) were used in this study; two pigs in phase 1 and four in phase 2. In both phases, pigs were anesthetized using Isoflurane (Piramal Healthcare; Piramal Enterprises Ltd., Andhra Pradesh, India), intubated and maintained under Isoflurane during the surgery. The dorsum of each pig was clipped and aseptically prepped for surgery. The area was draped using a sterile field drape. Ten linear full-thickness skin incisions (length = 3 cm) were made on the back of each pig (Fig. 1) by first drawing the incision line with a sterile marker, spaced 5 cm apart in the craniocaudal direction and 2 cm from the midline (4 cm spacing in transverse direction). Incisions were created using a scalpel blade to the fascia of the lumbar muscles, making sure not to perforate or damage the fascia. This ensured that the wound depth was similar between all wounds on the same animal.
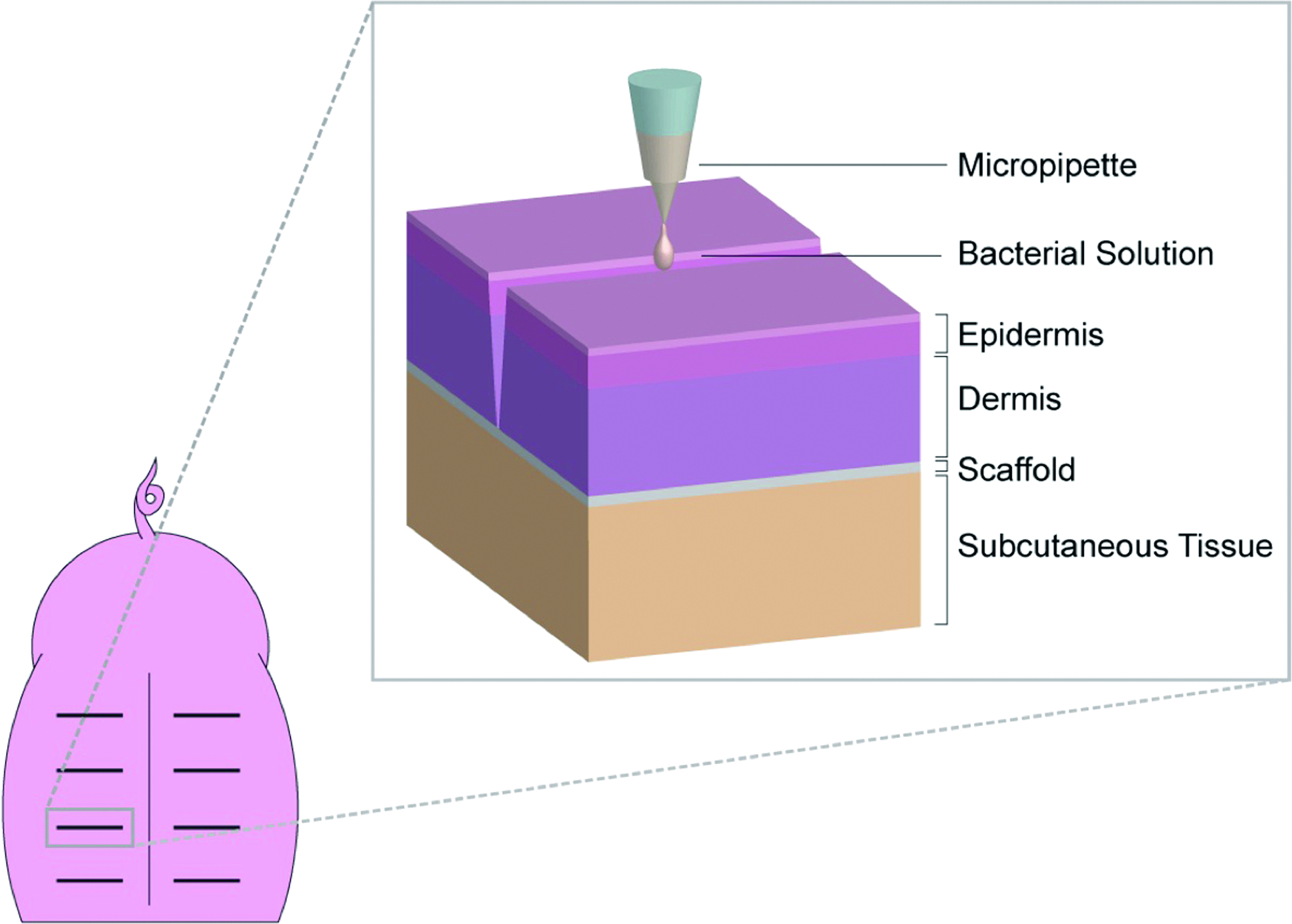
Inoculation of linear full-thickness skin incision on the back of a pig after placement of a scaffold under dermis layer superficial to the intact fascia. Color images available online at
For phase 1 of the study, which focused on the effect of bacterial concentration, 1 mL of each of the six bacterial concentrations was inoculated into the wound site under aseptic, surgical conditions, avoiding contact of the sample with the surrounding skin and changing instruments and gloves in between each site. Three technical replicates were considered for each bacterial concentration on a pig (n = 3/bacterial concentration). The wound was then closed by pulling up the ends of a preplaced subcutaneous suture that was then tied (Fig. 2). One additional cruciate suture was placed in the center of the incision to appose the skin edges (all in monocryl 3/0). One incision on each pig remained uncontaminated to serve as control. Gloves and sutures were changed between each bacterial inoculation. A dry porous nanofibrous bandage was placed postoperatively before recovery to protect the wounds in the immediate postoperative period. The bandages were kept in the wounds during the full experimental period. Postoperative analgesia was provided by buprenorphine (IV or IM) at the end of the surgery and repeated 8 h postoperatively. Prolonged analgesia delivery after postbuprenorphine delivery was maintained postoperatively by placing a 50 mcg fentanyl patch at induction. The two pigs were sacrificed 7 days after the surgery. In addition to wound scoring (explained in Wound assessment section), the pigs were monitored twice daily for systemic signs of infection. The bacterial concentration that caused the highest infection and inflammation at the wound site was selected to be used in the second phase of this study.

Experimental design for the two phases of the in vivo study: In phase 1, different concentrations of MRSA were used to inoculate wounds on two pigs. In phase 2, the effect of control PLA and antimicrobial PLA scaffolds on the uncontaminated wounds and wounds contaminated with 109 CFU/mL MRSA (selected base on the results of phase 1) were evaluated and compared to the wounds treated with gold standard (SSD) using four pigs. MRSA, methicillin-resistant Staphylococcus aureus; PLA, polylactic acid; SSD, silver sulfadiazine. Color images available online at
A similar surgical procedure was used in phase 2 of the study, which focused on evaluation of the antimicrobial efficacy of the silver ion releasing scaffolds. Control PLA and antimicrobial/silver-treated PLA scaffolds were cut into rectangles (3 × 4 cm2) and placed subdermally within the wounds immediately before injection of the inoculant into the wound site. This order was chosen as the wound was closed immediately following inoculation to avoid spillage of the inoculum. Bacterial strains were prepared as described above. Wounds were sutured and closed as described above. All treatments, including control PLA scaffolds, antimicrobial PLA scaffolds, and gold standard (SSD), were used in contaminated wounds on one pig (Fig. 2). On the same pig, control PLA and antimicrobial PLA scaffolds were used in uncontaminated wounds as controls. For each treatment group two technical replicates were included on each pig. These five groups were used on four pigs using a crossover design (Fig. 2). Two pigs were randomly selected and sacrificed at days 3 and 4. These two time points for sacrificing the animals were selected based on the results from phase 1 as described below. This experimental design allows for two technical replicates (for each treatment) in addition to two biological replicates (pigs), resulting in four data sets for each time point.
Wound assessment
The wounds were palpated and assessed daily for dehiscence (yes/no), discharge (on a scale of 0–3: 0 = no discharge, 1 = serous discharge, 2 = seropurulent discharge, and 3 = purulent discharge), and redness (scale of 0–3: 0 = no redness, 1 = redness at cruciate suture, 2 = redness around the entire incision, and 3 = redness beyond the borders of the incision) by three evaluators blinded to the treatment design. One of the evaluators was a board-certified veterinary surgeon (ACVS-SA and ECVS), with over 15 years of experience assessing wounds and incisions for inflammation and infection. The other two evaluators were trained by the veterinary surgeon.
Recovery of MRSA from harvested tissues
A 1 cm3 excisional biopsy punch was taken from the subcutaneous tissue of each wound site using sterile technique, and changing the blade and sterile gloves in between each sample. Harvested tissues were weighed and homogenized in 5 mL of PBS using a mortar and pestle. One milliliter of each homogenate was serially diluted 10-fold into PBS. All dilutions were plated in triplicate onto MRSA-specific agar plates (Hardy Diagnostics). Plates were incubated at 37°C overnight at 5% CO2. The next day, dilutions with between 30 and 300 colonies were visually counted and recorded to determine MRSA concentration.
Results
Scaffold evaluation
SEM analyses confirmed that the silver solution fully coated the solid PLA fibers (Fig. 3a). The uniformity of the coating on porous fibers was less than that on solid fibers (Fig. 3b). The coating did not block most pores on the surface of porous fibers (Fig. 3c). Fiber diameter measurements revealed that the average diameter of porous fibers was more than two times that of solid fibers (Table 1).
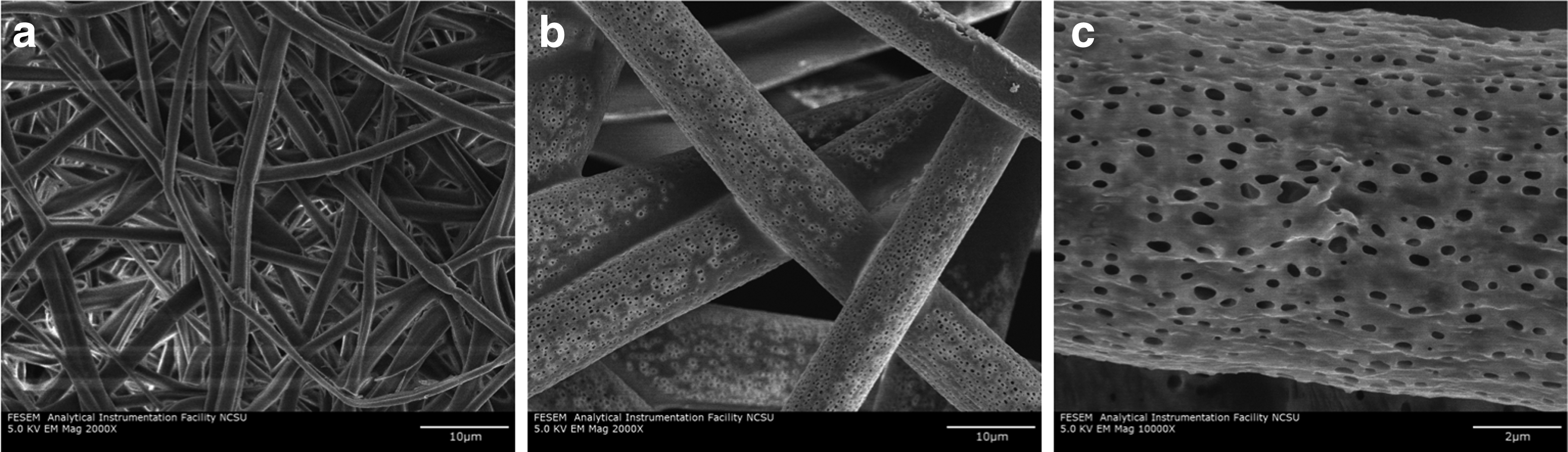
Scanning electron microscopy photographs of solid and porous PLA electrospun fibers coated with silver ion releasing coating at 2000 ×
In vitro antimicrobial evaluations of the solid and porous fibers treated with the silver ion releasing coating were conducted using the AATCC 147 protocol. 29 Both fiber morphologies exhibited strong antimicrobial properties against MRSA when treated with the silver ion releasing coating, as confirmed by large zones of inhibition (Fig. 4). Measurements of the zones of inhibition around the two scaffolds revealed a larger zone of inhibition for porous scaffolds compared with the scaffolds made of solid fibers, representing stronger antimicrobial properties for the porous scaffolds, as expected (Table 1).
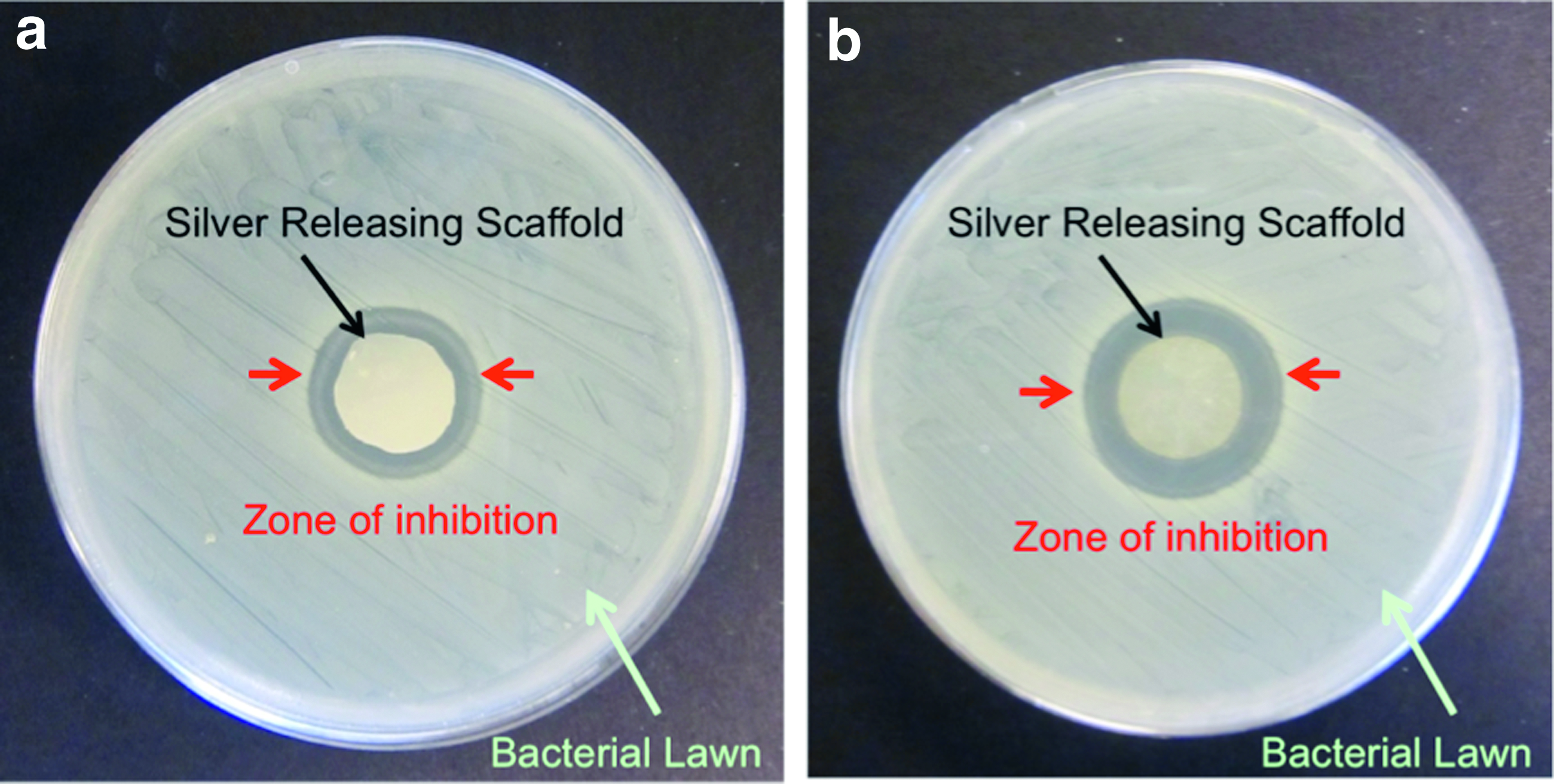
In vitro antimicrobial assessment (AATCC 147) of solid
Moisture pick-up analyses revealed higher absorption by porous fibers (372%) compared with solid fibers (172%) (Table 1).
In vivo evaluation, phase 1
No wound dehiscence and/or discharge were noted at any time point (days 1–7) during daily wound assessments. However, wounds infected with MRSA did exhibit inflammation as indicated by redness around the wounds. Inflammation of the wounds increased consistently with increasing bacterial concentration, as expected (Fig. 5). Twenty-four hours after surgery, all wounds exhibited redness at the cruciate suture (a common observation). Two days after surgery, the redness was no longer noticeable with control/noninoculated wounds and was decreased around wounds inoculated with 102 or 104 CFU mL−1 MRSA. Contrarily, red areas around wounds inoculated with higher concentrations of MRSA (106, 107, 108 and 109 CFU mL−1) were increased at this time point.
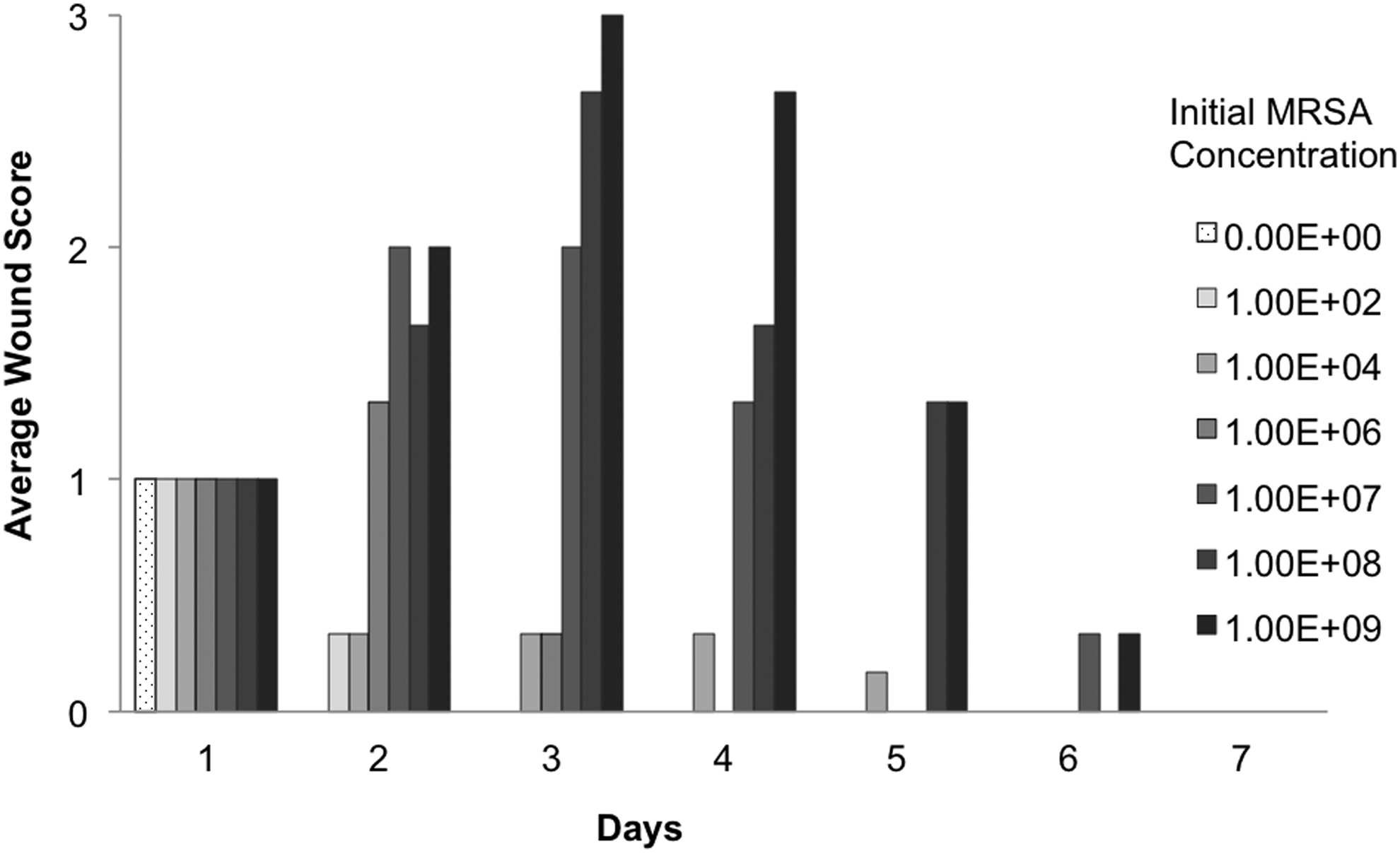
Wound scoring results for pigs inoculated with MRSA in phase 1. These results represent wound inflammation as monitored by redness around the wound using a scale system between 0 and 3 (0 = no redness, 1 = redness at cruciate suture, 2 = redness around the entire incision, 3 = redness beyond the borders of the incision).
While the redness associated with wounds inoculated with 102, 104, or 106 CFU mL−1 of MRSA continued to diminish on the following days, it significantly increased on day 3 for those wounds inoculated with higher bacterial concentrations (107, 108, and 109 CFU mL−1). At day 3 post surgery, when the largest red areas were reported, the redness started to fade for all wounds; by day 7, noticeable redness was not present on any wound (Fig. 5).
Quantification of MRSA from all wound sites showed that the concentrations were proportional to the initial bacterial concentrations used to inoculate the wounds (Fig. 6).
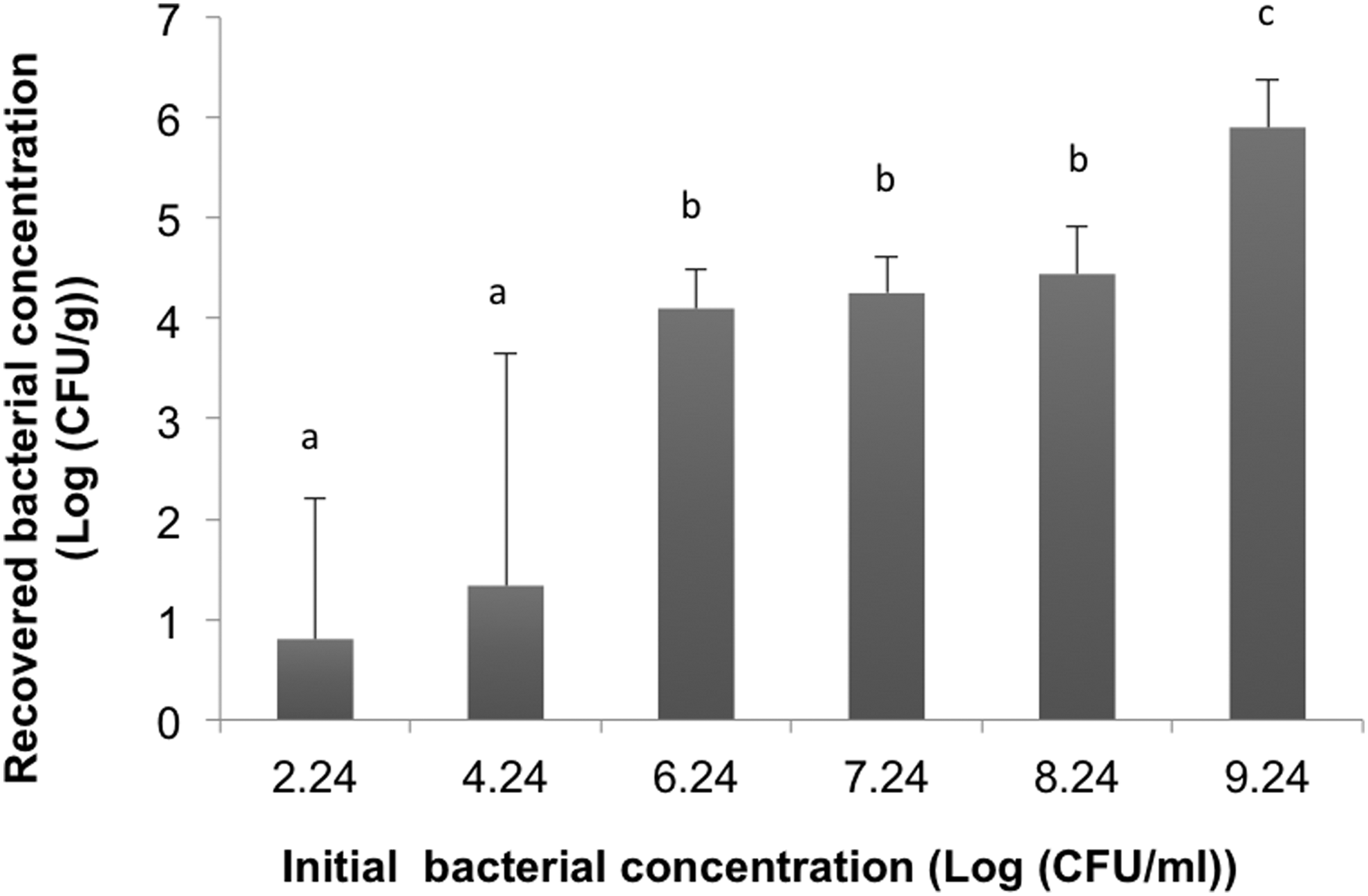
Concentration of recovered MRSA from wounds inoculated with different initial bacterial concentrations after 7 days in phase 1. Columns with different letters indicate significant difference (p < 0.05).
In vivo evaluation, phase 2
Visual assessment of wounds receiving different treatment protocols indicated that wounds treated with SSD (gold standard) exhibited greater redness and inflammation relative to all other wounds (Fig. 7). Some redness was observed around wounds treated with the silver releasing scaffolds as well as the untreated wounds. Control wounds (incisions performed but no bacterial inoculation) did not exhibit any sign of inflammation (Fig. 7).
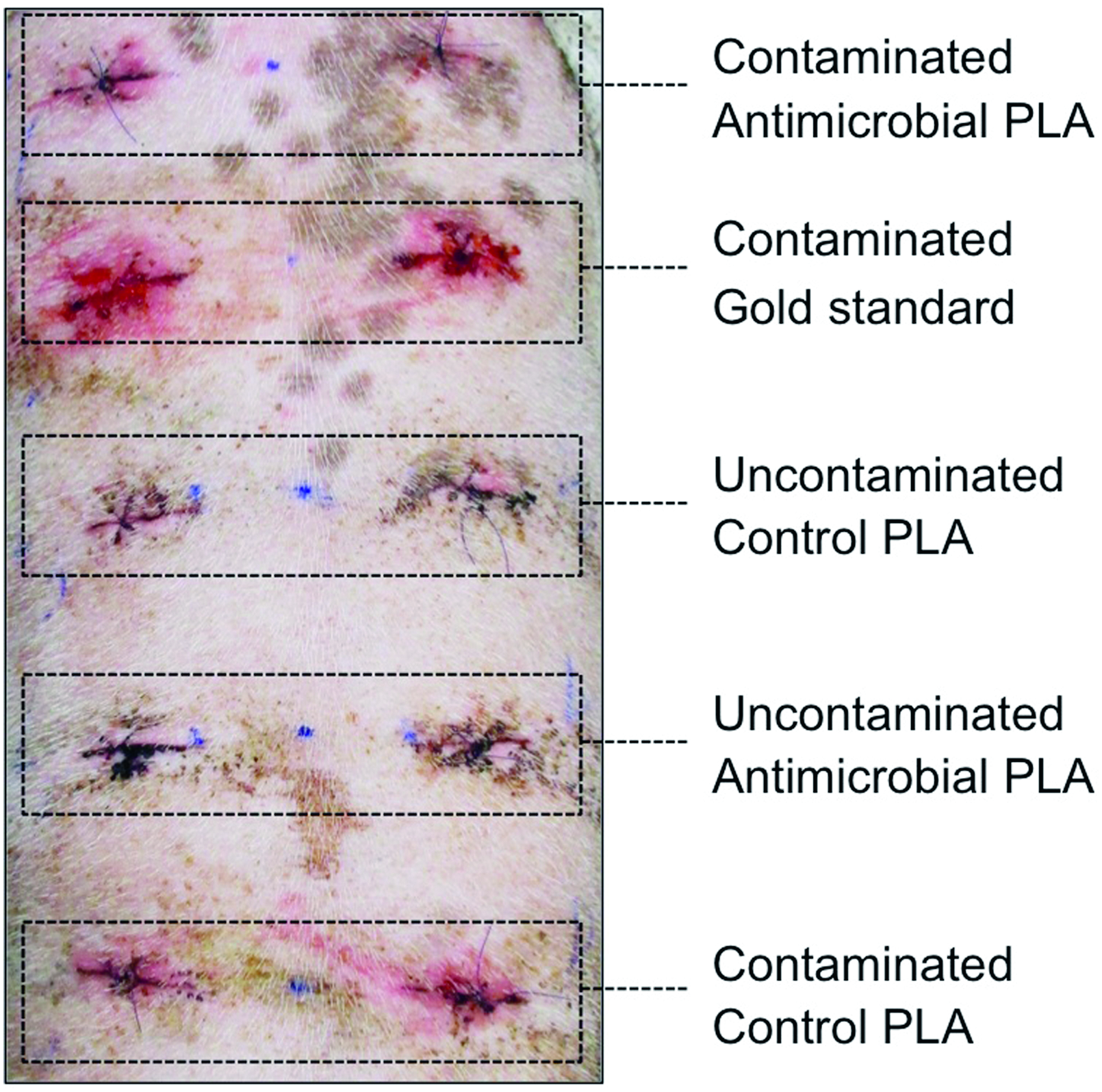
Representative photographs of wounds at day 4 of phase 2 inoculated with MRSA and treated as shown. Color images available online at
Average inflammation scores indicated that there was no significant difference between wounds receiving different treatments 1 or 4 days postsurgery (Fig. 8). However, on days 2 and 3 the average inflammation scores of wounds receiving different treatments differed significantly. Wounds treated with SSD exhibited the highest inflammation scores. There was no significant difference between wounds treated with antimicrobial scaffolds relative to untreated wounds on days 2 and 3 (Fig. 8).
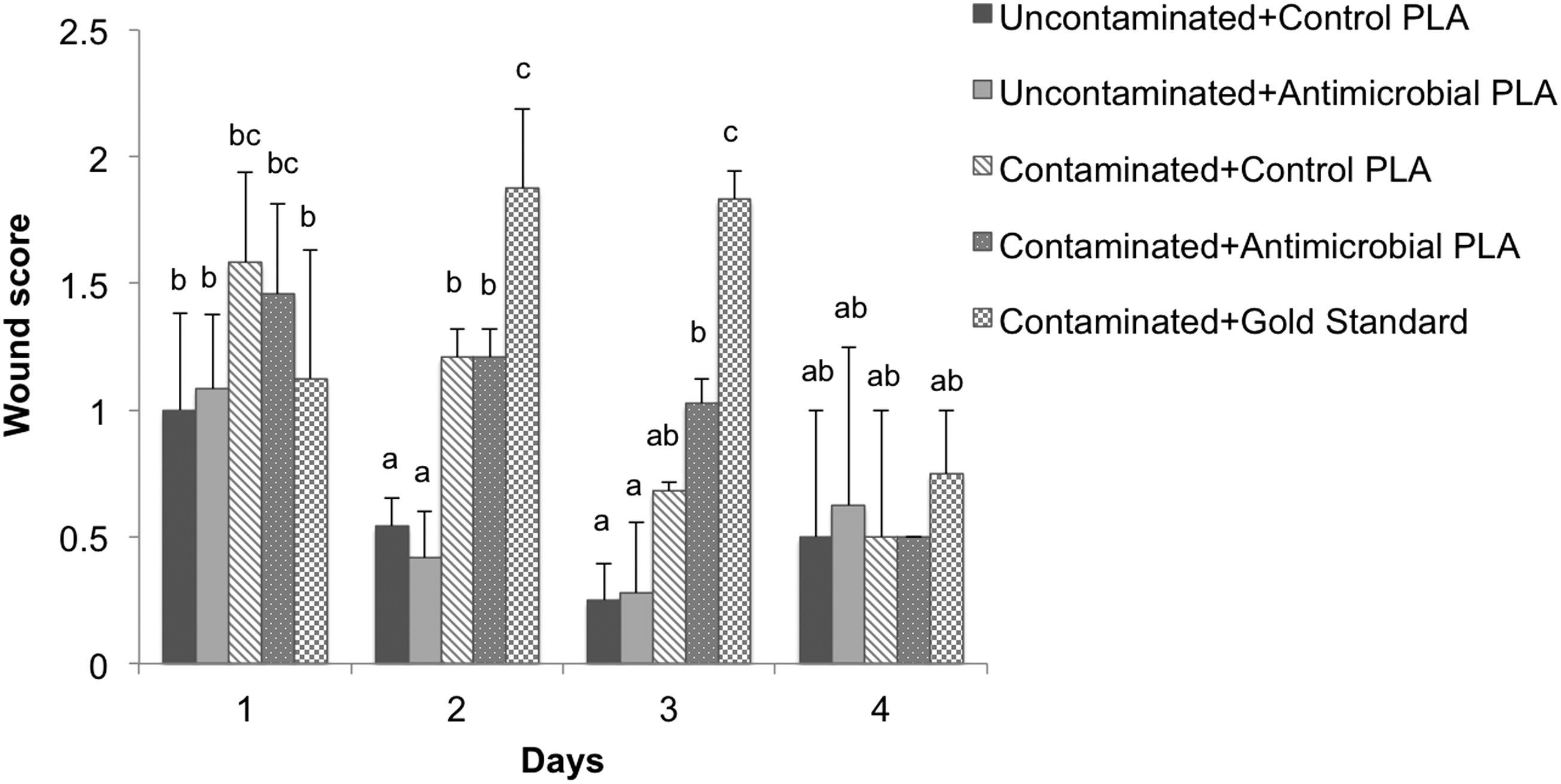
Phase 2 wound scoring results to monitor inflammation for pigs inoculated with MRSA receiving different treatments as shown. (0 = no redness, 1 = redness at cruciate suture, 2 = redness around the entire incision, 3 = redness beyond the borders of the incision; different letters indicate significant difference at p < 0.05. No significant difference was attained for different groups on days 1 and 4).
Bacterial quantification confirmed no bacterial growth in uncontaminated wounds. There was no significant difference in concentration of MRSA per gram tissue of contaminated wounds treated with antimicrobial PLA scaffolds relative to control PLA scaffolds and the gold standard at day 3 (Fig. 9). However, by day 4, wounds treated with antimicrobial scaffolds exhibited significantly lower bacterial concentration than wounds treated with control PLA scaffolds. Furthermore, while the difference was not statistically significant, the concentration of bacteria in the wounds treated with our antimicrobial scaffolds was also less than the concentration of MRSA in wounds treated with the gold standard, SSD (Fig. 9).

Recovered MRSA concentration at days 3 and 4 in phase 2 of the study. Columns with different letters indicate significant difference (p < 0.05).
Discussion
It is well known that infection impairs the repair of surgical wounds.30,31 In this study, we evaluate a new method to prevent SSIs via the use of a modified biodegradable antimicrobial scaffold. Previously, we developed and reported the utility of silver ion releasing biodegradable PLA electrospun nanofibers by loading PLA nanofibers that had a solid cylindrical morphology with a silver nitrate containing solution. 17 After the absorption of the solution to the scaffolds, they were dried to allow formation of a thin layer of antimicrobial coating on the fibers. 17
In this study, we hypothesized that the percent moisture content of the scaffolds would have a direct effect on absorption of the silver solution and, subsequently, the antimicrobial efficacy of the scaffolds. We therefore modified the morphology of the PLA fibers, introducing nanoscale pores to the fibers to increase the percent moisture content of the scaffolds and enhance their antimicrobial efficacy. We were able to successfully coat the porous PLA fibers with the silver ion releasing solution without blocking the pores on the surface of the fibers (Fig. 3). Absorption of the silver ion releasing solution was increased over two-fold (372% vs. 172%) with use of our porous fibers. Comparison of the in vitro antimicrobial properties of the silver releasing porous and solid fibers confirmed greater antimicrobial efficacy with use of the porous fibers. This can be explained by the higher rate of percent moisture content for porous fibers compared with solid fibers (Table 1).
To evaluate the antimicrobial efficacy of the silver releasing porous fibers in vivo, we developed a new SSI model using a porcine model. This model was created with the aim of causing infections, which are challenging to overcome by the immune system of healthy pigs, but do not cause lethality by infection of the animals. To accomplish this aim the appropriate type and concentration of bacteria needed to be tested and selected. In a pilot study, we induced infections with four different bacteria, including Pseudomonas aeruginosa, Acinetobacter baumannii, Staphylococcus pseudintermedius, as well as MRSA. The results of that pilot study indicated that infections caused by P. aeruginosa, A. baumannii, and S. pseudintermedius were quickly overcome by healthy pigs (data not shown). Of the four bacterial strains tested, MRSA was the only bacterial type that appeared to significantly challenge the immune system of pigs. Thus, MRSA was selected to induce infection. To determine the appropriate MRSA concentration to induce infection, the first phase of this in vivo study was designed and performed. The results from phase 1 confirmed that the higher the concentration of the inoculant, the higher the concentration of the recovered bacteria in the wounded tissue, as expected (Fig. 6). The recovered concentration of MRSA per gram tissue harvested from wounds inoculated with the highest bacterial concentration (1.75 × 109 CFU/mL) was 8 × 105 CFU/g.
Wound healing guidelines indicate that human wounds containing 106 CFU/g tissue will possibly experience impaired healing. 32 Therefore, 109 CFU/mL was selected for the second phase of the in vivo study focused on analyses of our antimicrobial scaffolds in infected wounds. Inflammation scoring of the wounds over the 7 day evaluation in phase 2 revealed that the infected wounds exhibited the greatest inflammation at days 3 and 4 postsurgery. Therefore, postop days 3 and 4 were selected as the time points for evaluation of results in the second phase of the in vivo study.
In the second phase of the in vivo evaluation, antimicrobial porous fiber scaffolds were subdermally placed in the wounds inoculated with 1.25 × 109 CFU/mL before suturing the wounds closed. Three control groups were also included in the experimental design: (1) antimicrobial scaffolds in uncontaminated wounds, (2) nontreated PLA scaffolds in contaminated wounds, and (3) nontreated PLA scaffolds in uncontaminated wounds. All groups were further compared to the gold standard of care, daily topical application of SSD cream to the wound site. SSD is a highly effective topical antimicrobial agent with slow release of silver ions that can inhibit the growth and proliferation of bacteria.33–35 SSD has been the standard treatment for burn wounds over the past two decades.36–38 It is still the most frequently used topical agent in the treatment of infections.36–38
Daily wound assessment postsurgery showed significantly higher inflammation scores for wounds treated with SSD compared with wounds treated with any of the three control treatments or our antimicrobial, degradable scaffolds (Fig. 8). Quantification of MRSA bacteria in the wound sites showed significantly fewer bacteria in wounds treated with our silver releasing antimicrobial scaffolds compared with control PLA scaffolds on day 4 postsurgery, confirming that efficacy of the antimicrobial scaffolds was a function of the silver ion releasing coating as opposed to any action of the PLA fibers alone. No significant difference was observed between the number of bacteria present in wounds treated with the gold standard SSD and the silver releasing scaffolds. Given the higher inflammation scores for SSD-treated wound sites relative to antimicrobial scaffold-treated wounds, and the need for daily reapplication of SSD, use of our degradable antimicrobial scaffolds is potentially a better choice for treatment of infected surgical wounds.
Conclusions
Although the efficacy of nanofibers in wound healing has been previously evaluated in excisional wounds, to our knowledge antimicrobial nanofibers have never been implanted in incisional wounds with the goal of SSI prevention. To evaluate the potential of our antimicrobial wound dressings to prevent SSI, we first needed to create an appropriate incisional model. We successfully created a model of SSI in vivo using a full-thickness infected wound in the pig.
This new incisional model can be used for evaluation of other antimicrobial treatments in preventing SSI. Such a model is critically needed at this time as SCIP has failed to decrease postoperative SSI complications. Using this new model, we were able to demonstrate the efficacy of our silver ion releasing, porous, and degradable dressings, which performed as well with respect to antimicrobial efficacy against MRSA as SSD, the current gold standard. Importantly, our dressings require no treatment postop (SSD requires daily reapplication) and caused less inflammation and redness at the wound site. This is the first study to use nanofibers for prevention of SSI. The results of this study cannot only be used by the CDC to determine new methods for reduction of SSI but can also be utilized by the nanofiber manufacturing industry to expand the applications of nanofibers to address critical applications in healthcare.
Footnotes
Acknowledgments
This research was supported by NIH/CTSA 550KR71418 (E.L.), NIH/CTSA 550KR61325 (E.L.), NSF/CBET 1133427 (E.L.), and a North Carolina Biotechnology Center Collaborative Funding Grant (E.L.). The authors acknowledge all the members of the Cell Mechanics Laboratory.
Disclosure Statement
No competing financial interests exist.