
Abstract
Adipose-derived stromal vascular fraction (SVF) cell populations are being evaluated for numerous clinical applications. The current study evaluated a point-of-care technology, the Tissue Genesis “TGI 1000” Cell Isolation System™, to perform an automated isolation of adipose-derived SVF cells to be used in the fabrication of a tissue-engineered vascular graft in the operating room. A total of seven patients were enrolled in this study and received femoral to tibial expanded polytetrafluoroethylene bypass grafts to treat peripheral arterial disease. Lipoaspiration of fat was performed on five patients, and the fat sample was processed immediately in the automated system in the operating room. The mean processing time, from the point of fat delivery into the instrument to removal of the SVF-containing syringe, was 70 min. The SVF cell population was evaluated for cell yield, cell viability, endotoxin levels, and microbial contamination. Samples of the SVF preparation were further subjected to microbiologic evaluation both microscopically before implantation of the graft and through a microbiologic screening using aerobic and anaerobic culture conditions. Mean cell yield was 1E5 cells per cc of fat, and endotoxin levels were below the FDA recognized standards. All SVF preparations were released for graft preparation, and the intimal surface of 90-cm-long grafts was pressure sodded with cells at a concentration of 2E5 cells/cm2. The sodded grafts (n = 5) and control grafts (n = 2) were immediately implanted and graft patency assessed for 1 year. One year patency was 60% for sodded grafts and 50% for control grafts. Automated preparation of autologous adipose-derived SVF cells for immediate use to create cellular linings on vascular grafts is feasible and safe.
Introduction
A
Automated systems for processing fat and deriving the SVF population have evolved with progressive improvements to achieve automation of processing, including software process control and integration of closed fluid paths.2–7 To achieve the goal of a hands-free, closed system for SVF isolation, an automated adipose processing and SVF isolation instrument was designed, constructed, and evaluated in a human clinical study. The instrument, commercially named the “TGI 1000” (Tissue Genesis, LLC), was evaluated for the ability to reproducibly isolate adipose SVF cells in the operating room and subsequently use the SVF cell population to sod expanded polytetrafluoroethylene (ePTFE) vascular grafts for use in patients suffering from peripheral arterial disease (PAD).
The Tissue Genesis TGI 1000 instrument is a completely closed, computer-controlled, and automated system. It is unique compared to other commercial systems in its relatively smaller size, and the use of computer-controlled valves to move solutions and products within the isolation system. This study is being conducted as an FDA-registered (
The patency of prosthetic (e.g., ePTFE, Dacron) femoral–tibial bypass grafts is inferior to vein bypasses in PAD patients.8–12 The decreased tolerance for smaller diameter outflow vessels, inherent thrombogenicity, susceptibility to infection, and lack of a viable luminal lining of cells are all contributing factors toward inferior results with synthetic grafts.13–15 Prosthetic graft failure is also attributed to progression of atherosclerosis, and a reduced flow state when grafts are anastomosed to small-diameter vessel (<6 mm). To circumvent these challenges, creation of a tissue-engineered vascular graft (TEVG) has been proposed as an approach to improve graft patency.6,16,17
Our hypothesis is that the process requires a readily available cell source with sufficient numbers and function to create a neovascular cell lining. Our current approach utilizes SVF cells isolated from lipoaspirated adipose tissue. The SVF cell population is heterogeneous and contains a significant population of endothelial cells as well as other cells (e.g., smooth muscle, endothelial progenitor cells) that represent the cellular components of blood vessels.18–25 Animal studies of adipose SVF-sodded grafts indicate the feasibility of creating TEVGs, point-of-care (POC), with evidence of reduced progression of neointimal thickening, and evidence of improved patency.3,6,7,26 SVF is therefore uniquely suited for TEVG creation. Herein we describe IDE feasibility clinical trial utilizing a POC technology, the Tissue Genesis “TGI 1000” Cell Isolation System™, to create a TEVG for femoral to tibial bypass grafting in PAD patients without available autogenous conduit.
Objectives
To determine the feasibility of using automated instrumentation, the Tissue Genesis “TGI 1000”™, to isolate SVF cells from adipose tissue in an operating room, and to obtain evidence of safety and preliminary information on the effectiveness of using the isolated SVF to sod synthetic ePTFE vascular conduits for femoral–tibial bypass grafting.
Primary endpoints of the study include (1) graft patency as assessed at 1, 3, 6, 9, and 12 months by duplex ultrasound and (2) safety of the procedure and implant. Secondary endpoints include (1) assisted primary patency, (2) secondary patency, (3) limb salvage, (4) wound healing, and (5) improvement in rest pain.
Study design
This was an initial cohort of a prospective, randomized, controlled, parallel group, phase
Inclusion criteria
To be eligible to participate in this trial, subjects had to meet all of the following criteria: (1) male or female ≥18 years old; (2) patients require a synthetic vascular graft, with the distal anastomosis to a tibial artery peroneal, anterior tibial, or posterior tibial artery, with continuous blood flow to the foot; (3) the distal anastomosis was to be no more distal than approximately the mid-calf; (4) Rutherford–Baker (RB) classification for PAD of five or less; (5) the proximal anastomosis had to be in the common femoral artery (CFA) or the superficial femoral artery; and (6) an arteriovenous fistula could not be created at the distal anastomosis.
Exclusion criteria
Included but not limited to the following: (1) lack of adequate subcutaneous fat stores to allow liposuction of 120 mL of adipose tissue; (2) limb-threatening acute ischemia in the affected leg; (3) active infection or malignancy at the time of implantation; (4) acute renal failure; (5) hepatic insufficiency; and (6) NYHA class
Materials and Methods
To date, seven patients with ischemic rest pain or life-limiting claudication have been enrolled in this study to receive either a cell-sodded or control ePTFE conduit. A continuous general anesthetic was used for lipoaspiration, automated cell isolation, operative exposure, and sodded-conduit implantation.
Lipoaspiration technique
A final tumescent fluid concentration of ∼0.1% lidocaine HCl and 1:1,000,000 epinephrine was created. Each patient's abdomen and bypass surgery site were widely prepped with 2% chlorhexidine gluconate. An iodine-impregnated drape was placed at the site of liposuction as well as the bypass site. The operative bypass field was exclusive of the lipoaspiration site. The abdominal subcutaneous fat was infused with the tumescent fluid and allowed to blanch before a 2 mm linear skin incision over or near the region targeted for lipoaspiration. A specimen of 60–120 mL of lipoaspirate was obtained using negative pressure of 18" Hg. Sixty milliliters of lipoaspirate was sent to the TGI “TGI 1000” for processing.
Briefly, the “TGI 1000” (Fig. 1) is an automated, point-of-care cell isolation instrument. It has a graphical user interface that requires minimal operator training and has a small footprint designed for the operating room. It comprises an instrument and one-time-use disposable that is functionally closed, which interfaces with the stand-alone desktop instrument to extract SVF from adipose tissue in about an hour. During this process, the tissue is washed and mixed with a proprietary digestive enzyme. The resultant SVF cell population is further washed and separated by centrifugation from the adipose cells and tissue matrix. The cells are suspended in a user-provided medium and provided in a syringe for immediate economical use. A typical yield is about 50 million viable SVF cells suspended in ∼30 mL of medium. Samples of this cell suspensate are taken for analysis.

The automated adipose tissue processing system. The instrument and associated kit, including the digestion chamber, tubing, and enzyme, provide a closed system for the preparation of the SVF. SVF, stromal vascular fraction.
Cell suspensate assays
Cell count was determined using a NucleoCounter instrument (ChemoMetec, San Francisco, CA). This analysis was performed in the operating room using instrumentation that was placed next to the “TGI 1000” (Fig. 2). A stat Gram stain of the cell suspension was obtained to assay for bacterial contamination of the SVF. Endotoxin level of the cell suspensate was assayed using the Charles River Endosafe-®-PTS™.

The automated adipose SVF isolation system being used in the operating room.
Graft wetting and sodding
The PTFE conduit was placed in a previously autoclaved stainless steel conduit tray on the sterile field. An 80 cm length of ePTFE was prewet with medium at a pressure of between 5 and 10 psi, as measured by pressure meter display (as previously described by Williams et al.3,7). Once the cell isolate was ready, the cell isolate was introduced into the prepared graft at 5–10 psi. Briefly, the cells are introduced into the lumen of the permeable graft after the distal end has been sealed. As medium passes through the graft material, a “weeping” of medium was observed on the outer surface of the graft (Fig. 3). The transluminal pressure and the medium flow deposit the SVF cells into the interstices of the conduit. The cell density used for sodding was controlled to ∼2 × the confluent endothelial cell covering on the luminal surface of a native human blood vessel.

During the process of adipose SVF cell sodding, the cell product is placed within the lumen of the graft and pressure applied to force the cells onto the luminal surface. This figure illustrates the beading of fluid that homogeneously appears on the abluminal surface of the graft during pressure sodding.
Sodded-conduit termini analysis
The terminus from each end of the sodded graft was excised before conduit implantation. Sodded-conduit termini were placed into labeled vials of fixative. Each sodded-conduit terminus was tangentially transected into four sections; one of which from each end was randomly selected, removed from the fixative, and stained with bisbenzimide (BBI) for cell counts. Cell nuclei were labeled with BBI by standard procedures and evaluated with a fluorescence microscope. Images of five random, representative endoluminal areas along the selected sample were obtained. The surface area represented by each interrogated image was documented. The number of positively labeled cell nuclei observed within each image was counted and recorded. These data allow calculation of an estimated mean nucleated cell density per unit area of sodded-conduit terminus (cells/cm2).
The remaining three samples from each sodded-conduit terminus were prepared for immunohistochemical analyses. Each sample was first stained with BBI to label cell nuclei and then reacted with one of three antibodies: von Willebrand factor (vWF), α-smooth muscle actin (α-SMA), or vimentin. Each sample was placed under a fluorescence microscope and images of random, representative endoluminal regions were obtained. Two exposures of each examined area were captured: one demonstrating BBI alone, and one demonstrating the antibody stain. These two isometric images were superimposed to allow determination of the number of positively labeled cells for each antibody stain.
Femoral to tibial bypass grafting
Femoral to tibial bypass grafting was performed after confirmation of a negative Gram stain and an endotoxin level ≤0.47 EU/mL for the cell suspensate. A vertical groin incision was utilized in all cases to expose the CFA, the vessel of origin for each bypass conduit. Distal target vessels for the cell-sodded conduits were anterior tibial (3), posterior tibial (1), and peroneal (1) arteries, respectively. Of the two control grafts, one had a posterior tibial and one a peroneal artery distal target. A medial approach was used to access the posterior tibial and peroneal arteries with a standard lateral approach to the anterior tibial artery. The distal anastomosis was created in an end-to-side manner in all patients without technical adjuncts.
Explant histology
Explant samples, when available due to surgical revision, were fixed in formalin and processed for paraffin sectioning. Sections were stained with hematoxylin and eosin and antibodies against vWF, alpha smooth muscle cell actin, and vimentin.
Results
Automated SVF isolation instrument
Lipoaspiration of fat was performed in five patients who received cell-treated grafts. Table 1 describes the patient demographics, the volume of fat obtained, and subsequent cell yield using the “TGI 1000” instrument. The “TGI 1000” automated SVF isolation system is illustrated in Figure 1 and its use in the operating room is shown in Figure 2. The mean yield of SVF cells was 159,244 cells/cc of fat processed. Each SVF isolate was evaluated for the presence of bacteria by Gram staining and all SVF samples were judged negative. Subsequent aerobic and anaerobic microbiologic evaluation of the SVF isolate also resulted in no evidence of bacterial contamination. The SVF cell populations were used to sod ePTFE vascular grafts with a mean cell density on the luminal surface of grafts determined to be 0.5 × 105 cell/cm2 of the graft luminal surface area. The total time from the beginning of lipoaspiration to the time of graft sodding completion and ready for implantation was 137 min, range of 120 to 140 min.
BMI, body mass index; N/A, not applicable; SVF, stromal vascular fraction.
Graft patency and clinical outcome
There were no adverse reactions observed associated with the isolation of a patient's own fat using lipoaspiration, the use of the “TGI 1000” system, the implantation of the sodded graft, and the subsequent implant phase of patient recovery. One-year follow-up was completed for seven patients. Sixty percent (total n = 5; three patent and two clotted) of the sodded grafts and 50% (total n = 2; one patent and one clotted) of the control GORE PROPATEN® grafts remain patent. RB scores improved in all patients and remained stable in the postoperative period for patent grafts and these data are summarized in Table 2. One sodded graft patient had thrombosis of the graft during the ninth month of enrollment and the graft was replaced with a nonsodded conduit. At 2 months, one patient had evidence of early thrombosis at the toe of the sodded graft and into the anterior tibial artery by duplex imaging. This was revised with a vein patch angioplasty and the graft was patent at discharge. The region of the excised graft that was patent at the time of explant was subjected to histologic evaluation and results are shown in Figure 5. At the 6-month follow-up visit, the graft was clotted as determined by duplex imaging, but the patient remained asymptomatic. He continues to do well clinically. One PROPATEN control graft thrombosed during month 7 and subsequently was replaced by another PROPATEN conduit. Patient demographics, graft patency, and clinical outcomes are outlined in Table 2. Histologic evaluation of explanted graft segments indicated a lack of cellular neointima formation.
Sodded-conduit termini analysis
BBI-positive cells were identified from randomly chosen, representative areas of the sodded-conduit termini across multiple images of each stained sample (Fig. 4). Each graft end was examined and the mean number of cells present on the grafts before implantation was calculated. For the five sodded grafts, cells were present on all graft ends on the lumen of the grafts as well as in the interstices. The mean cell density was 38,200 nuclei/cm2.
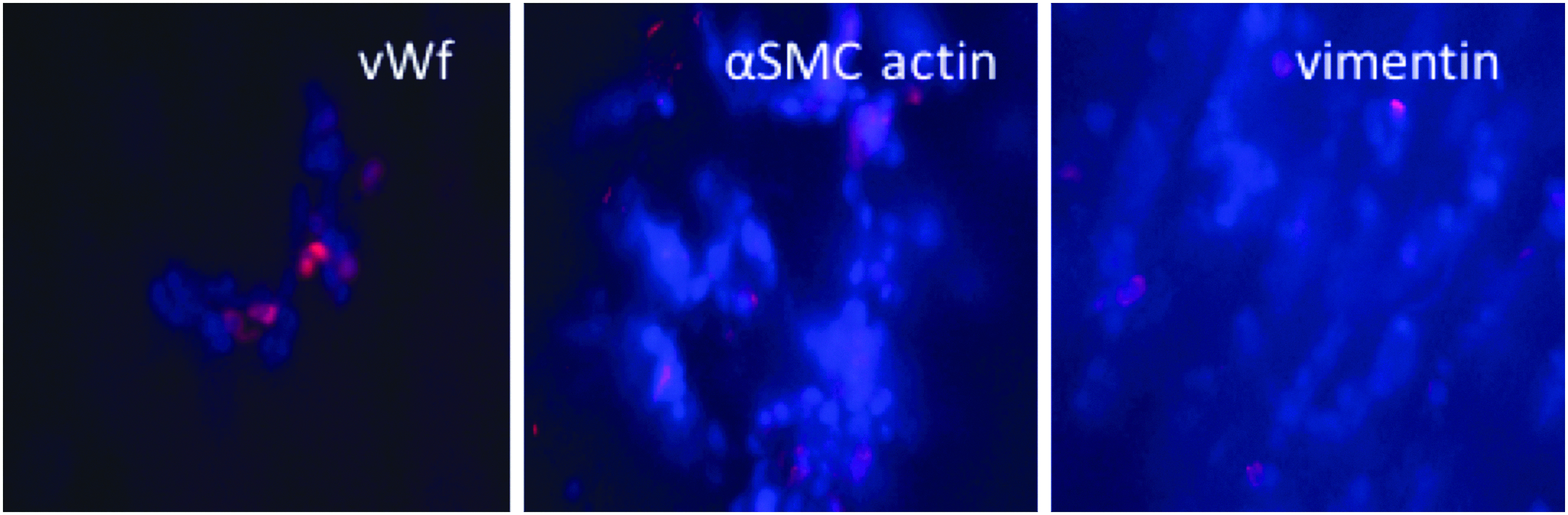
Characterization of the cells deposited on the luminal surface of grafts was performed using immunocytochemical assessment. The cells that are sodded onto the graft surface express antigens indicating their endothelial (vWF), smooth muscle (α-SMA), and mesenchymal (vimentin) characteristics. α-SMA, α-smooth muscle actin; vWF, von Willebrand factor.
In addition, samples from each graft termini were immunostained to evaluate the cell population adhered to the grafts before implant (Fig. 4). For each graft terminus evaluated, 100 BBI-positive cells were counted, and then the image was overlaid with the images from the immunohistochemical staining on the same sample of graft end. Cells that were stained positive for vWF, smooth muscle cells (SMC), or vimentin were counted, which allowed an estimated calculation of the percent of positively reacted cells.
Histology
Histological evaluation of the tissue response of two implanted grafts that were replaced or revised postimplant is illustrated in Figure 5. Both these vascular grafts were previously sodded with cells following their isolation using the Tissue Genesis (TG) instrumentation. The samples were prepared for evaluation using histology stains that determine whether cells normally present on a human blood vessel were present on these explanted grafts. In both cases, a lining of mature endothelial cells was observed on the inner surface of the grafts. This inner surface is in contact with the patients' blood while the graft is implanted. In both cases the histological examination determined that no blood clots were present on the inner lining. These findings support the conclusion that the treatment of these grafts with adipose-derived regenerative cells results in the formation of a nonthrombogenic cellular lining. The cells present were identified as endothelium based on immunocytochemical staining, the cells that line all native blood vessels in the body.
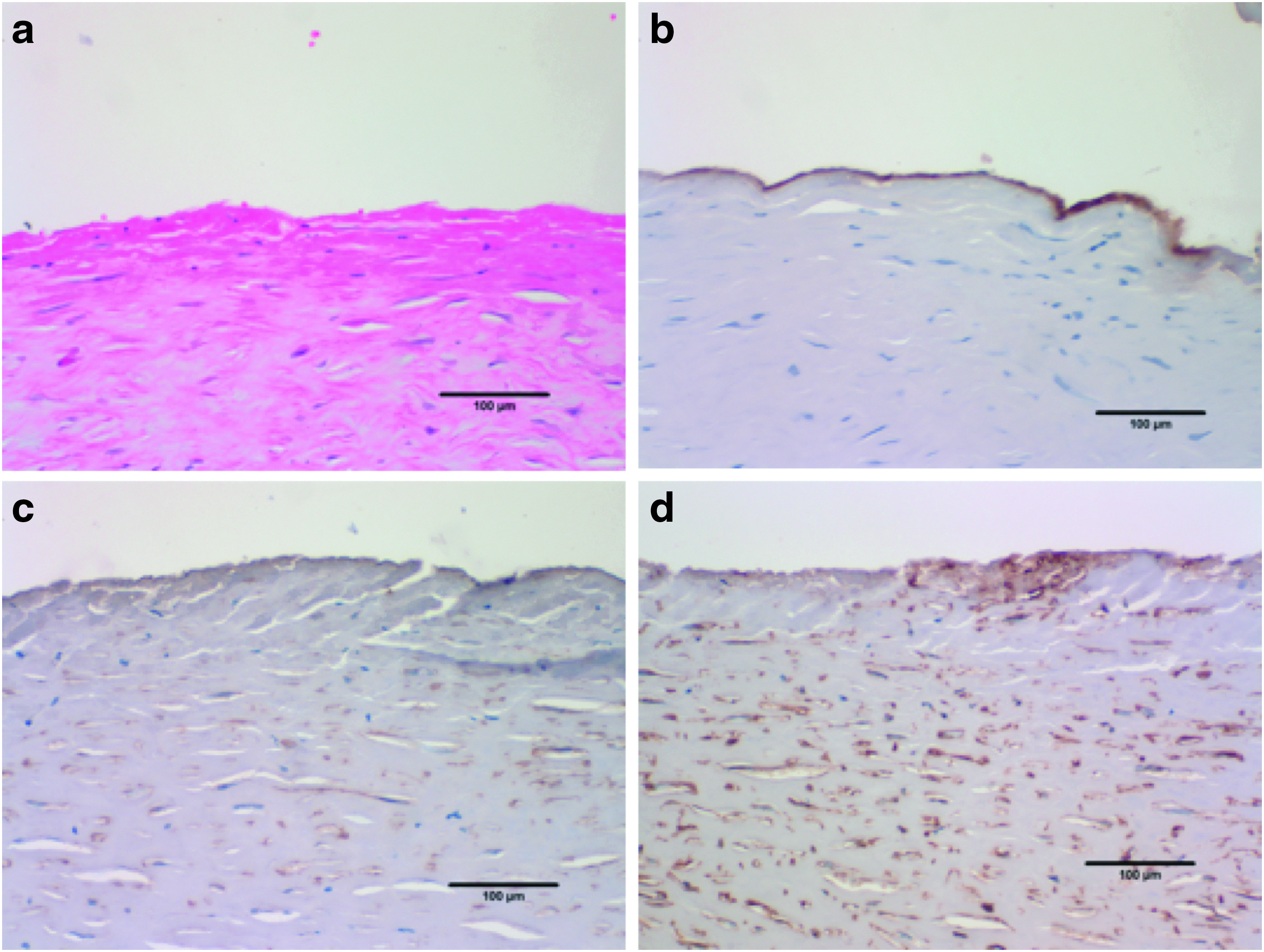
Photomicrographs of a sodded graft explant illustrating the cellular neointima formed on the ePTFE vascular graft.
Duplex ultrasound
Duplex ultrasound was utilized to assess graft patency at patient follow-up visits. Figure 6 illustrates the patency of a sodded graft and proximal and distal native vessel segments. The graft patency is provided in Table 2.

Duplex ultrasound images of
Discussion
Dr. Malcolm Herring heralded the creation of a TEVG in 1978 by transplanting endothelium from the intimal lining of a saphenous vein onto a synthetic Gortex® graft 27 in a canine model. The endothelial cells were harvested from the luminal surface of saphenous vein, mixed with autologous blood, and then “seeded” onto the porous graft.27,28 In vivo remodeling, with endothelial cell migration and subsequent proliferation, leads to the formation of a continuous endothelial cell monolayer on the luminal surface of the grafts. The TEVG was dynamic, with extracellular matrix produced by the various cellular components of the bioengineered construct.28–31 Although technically feasible, there are limitations of endothelial cell seeding of vascular grafts. A major challenge is the variable cell yield with ∼1 × 104 endothelial cells (EC) harvested per vein segment under ideal conditions. Ex vivo culturing is required to get the requisite cell number (typically >1 × 106) for graft seeding onto a synthetic polymer scaffold. The process of culture and graft seeding is labor-intensive, carries a risk of infection and is costly, and introduces several growth factors with untested effects when implanted clinically. These challenges of EC harvest and cell yield have therefore limited its widespread clinical application.32,33
In 1986, Jarrell and Williams identified adipose tissue as a source of cells that might be used for transplantation.34,35 Adipose tissue is a highly metabolic organ with important endocrine and paracrine functions. Initially, omental-associated fat was used, which is well vascularized and could give a yield of >1 × 106 endothelial cells per gram fat. 35 Cells were isolated using a modification of Wagner's original enzymatic methods using clostridial collagenase with subsequent centrifugation at a relative low speed of (400 g force). 25 At this speed, adipocytes rise to the top of the aqueous buffer and the SVF is pelleted. This heterogeneous cell population includes endothelial cells, endothelial cell progenitor cells, SMCs, pericytes, mesenchymal cells, and prohealing factors, uniquely suited for creation of a TEVG. The use of liposuction-derived subcutaneous fat in humans, thus avoiding a laparotomy, was a major advance in the creation of a TEVG. Liposuction-derived fat has the optimal cellular characteristics for cell sodding, with reproducible yields. Roughly 50 cc of fat can be obtained in ∼10 min. 36 In a pilot clinical study of 11 patients by Williams et al. in 1989, liposuction-derived SVFs (2 × 105 cells per cm2 of graft surface) were sodded onto ePTFE and implanted into 11 patients requiring an ilio-tibial bypass. At the 4-year follow-up of seven patients, graft patency was 60% without added morbidity for implantation of the sodded conduit. 7 In a preclinical study, a 4 mm SVF-sodded ePTFE graft was interposed in a canine carotid artery model. 37 In this canine trial, 100% of the SVF-sodded grafts remained patent at 20 weeks, whereas 50% of the control ePTFE grafts were occluded. The sodded grafts demonstrated a cellular lining similar to a native artery. 38 These preclinical and clinical data are promising and the results of these studies and many other preclinical studies led to the present phase I clinical trial using POC technology.
The “TGI 1000” is an adipose tissue processing system that provides an automated, computer-controlled, fully closed system for processing liposuction-derived adipose tissue and isolating the SVF cells for use. We believe the processing of adipose tissue using tissue dissociation enzymes, the isolation of the SVF cell population using centrifugation, and the subsequent use of this cell population to sod the internal surface of synthetic grafts represent a process that involves more than minimal manipulation. For this reason, an Investigational Device Exemption application was prepared and submitted to the FDA to support the proposed clinical studies. The TGI 1000 is unique from other commercial systems due to the shorter processing time and the hands-free operation requiring no user intervention during the processing period. After ∼1 h of fat processing, the isolated SVF cell population was used to pressure sod the prosthetic conduit, and the graft immediately implanted into the patients without any further manipulation. The present study demonstrates that the “TGI 1000” fat processing system can be integrated into vascular bypass graft surgery procedures within the operating room environment. The abdominal liposuction portion of each procedure did not result in any adverse events and the “TGI 1000” system functioned correctly to separate the cells from the adipose tissue. The cell preparation and sodding of the graft, including the microbiology and endotoxin evaluations, were completed without interrupting the ongoing vascular surgery procedure, so that the graft could be implanted in a timely manner.
Although a small sample size to date, this phase I clinical trial suggests that implantation of an SVF-sodded prosthetic graft is clinically feasible. The procedure was safe as there was no significant morbidity added to the liposuction procedure and graft preparation. Liposuction was technically easy without a significant learning curve. No bacterial contamination or oncological issues were identified in the year of follow-up.
Conclusion
Infrageniculate arterial vascular reconstruction utilizing nonautogenous conduit is hampered by a dismal 5-year patency rate. The automated SVF isolation system, the “TGI 1000,” provided sufficient cell numbers to perform intraoperating sodding of grafts in the operating room. Although a small cohort, this study suggests that the utilization of POC technology, with autologous, adipose-derived SVF to create a TEVG, is feasible and safe. SVF is a unique regenerative cell source with an ease of extraction, and a highly reproducible cell yield therefore relegating the need for culturing before clinical use. The challenging PAD patient cohort will add many rigors to the ultimate widespread application of this technology, but we are encouraged by our initial results.
Footnotes
Disclosure Statement
S.W., PhD, is a consultant to Tissue Genesis, LLC. P.K., PhD, is an employee of Tissue Genesis, LLC. K.L., MD, was previously an employee of Tissue Genesis, LLC. G.G., MD, was previously an employee of Tissue Genesis, LLC.