
Abstract
Engineered cell sheets that are fabricated by using temperature-responsive culture dishes are now available in the clinical setting. Engineered chondrocyte cell sheets are used in clinical trials for treating focal articular cartilage defects. However, the efficacy of engineered chondrocyte cell sheets for treating diffusely degenerated articular cartilage remains unknown. In the present study, we assessed the utility of engineered chondrocyte cell sheets for treating diffusely degenerated articular cartilage in a monoiodoacetate (MIA)-induced arthritis animal model. At 1 and 3 weeks after intra-articular MIA injection into rat knees (1 w-MIA/3 w-MIA model), the degenerated cartilage at load-bearing area sized 1 × 3 mm was removed. Rats in each group were divided into three subgroups: Removal (R) group as control, Removal + Drilling (RD) group in which cartilage was removed followed by subchondral drilling, and Removal + Drilling + Sheet transplantation (RDS) group in which the removed cartilage area was covered with a 2 × 4 mm size of triple-layered chondrocyte cell sheet. In the histological assessment, the score of the RDS group in each model was significantly better than that of R and RD groups at 4 and 12 weeks, respectively, after the surgery. Our results demonstrated that the transplanted chondrocyte cell sheets improved cartilage repair even under such severe conditions as diffusely degenerated articular cartilage. Chondrocyte cell sheets appear to be useful as a treatment option for MIA-induced arthritis models.
Introduction
A
Cell-based regenerative and tissue-engineered therapies have been widely developed.1,2 One autologous tissue-engineered cartilage transplantation technique using atelocollagen gel developed in our group 3 received marketing approval and is covered by the national health insurance in Japan (JACC; Japan Tissue Engineering Co., Ltd., Gamagori, Japan). Although we reported good clinical outcomes using that technique in the patients with focal articular cartilage defect, it has some limitations, such as the use of scaffolds, and the need for an open surgery to cover the transplanted tissue with an autologous periosteum.4,5
Engineered cell sheets fabricated by using temperature-responsive culture dishes were established by Okano et al. 6 and are now used in regenerative therapies for several tissues in clinical research.7–10 We can create scaffold-free cartilage cell sheets by lowering the temperature to pile them up to the desired thickness because of their excellent adhesion.11–14 In addition, this approach does not require any enzymatic digestion, retaining the extracellular matrix. 14 Using this method, previous reports have shown successful articular cartilage regeneration of partial- and total-thickness cartilage defects in animal models.11,13 These layered cell sheets suppress degeneration of the articular cartilage by adhering to the injured cartilage, preventing the loss of proteoglycans and protecting the tissue from catabolic factors.12,15–18 Based on these results, a clinical study using these engineered cell sheets to treat focal osteochondral defects is underway. 16 However, there are also many patients with diffuse degenerative articular cartilage lesions due to osteoarthritis (OA) or rheumatoid arthritis. To our knowledge, there are no previous reports that elucidate the utility of engineered cell sheets for treating diffusely degenerated articular cartilage in an animal model. Therefore, in this study, we evaluated the efficacy of transplantation of a chondrocyte cell sheet for cartilage repair in a drug-induced arthritis animal model with diffusely degenerated articular cartilage.
Materials and Methods
This study was performed in accordance with the Guide for Animal Experimentation and was approved by the Committee of Research Facilities for Laboratory Animal Science (Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan).
Harvest and culture of chondrocytes
Chondrocytes were harvested from the articular cartilage of the femoral condyles of 4-week-old green fluorescent protein (GFP) transgenic rats (Japan SLC, Inc., Hamamatsu, Japan). The cells from the GFP transgenic rats were characterized for the expression of GFP fluorescence in their cytoplasm and nucleus. The harvested cartilage was minced and digested with trypsin (TrypLE Express; Life Technologies, Carlsbad, CA) for 30 min followed by digestion with 0.25% collagenase (Sigma-Aldrich, St. Louis, MO) for 4 h at 37°C. The isolated chondrocytes were filtered through a cell strainer (70 μm; BD Biosciences, San Jose, CA) and cultured in 35 mm temperature-responsive culture dishes (UpCell; CellSeed, Inc., Tokyo, Japan) at a density of 1 × 105 cells/dish in Dulbecco's modified Eagle's medium that was supplemented with 20% fetal bovine serum (Sigma-Aldrich) and 1% antibiotics (penicillin, streptomycin, and amphotericin B; BioWhittaker, Walkersville, MD) at 37°C in a humidified atmosphere containing 5% CO2. The medium was first aspirated 3 days after seeding to remove non-adherent cells and was replaced with fresh medium, which was further supplemented with 50 μL/mL of
Fabrication of layered chondrocyte cell sheets
After culturing the chondrocytes for 2 weeks on the temperature-responsive culture dishes, the cells were confluent and the dishes were brought to room temperature for ∼30 min. The chondrocytes were harvested as a triple-layered cell sheet by twice over-laying one layer on top of another cell sheet by using a pipetting method.19,20 The sheets were then cultured together for another week. 14 After fabrication of the chondrocyte cell sheet, these were fixed with 4% paraformaldehyde, mounted with O.C.T. compound (Sakura Finetek, Tokyo, Japan), and frozen at −20°C. Then, the blocks were cut into 5 μm sections. The properties of the chondrocyte cell sheets were assessed under fluorescence microscopy, and they were stained with Safranin-O fast-green.
Monoiodoacetate-induced arthritis model
A total of 12 Sprague–Dawley (SD) rats (24 knees) aged 8 weeks were used. In the arthritis group (12 knees), 1 mg of monoiodoacetate acid (MIA; Sigma-Aldrich) diluted in 50 μL of saline was injected into both knee joints percutaneously through the patellar tendon as previously reported. 21 In the control group (12 knees), 50 μL of saline was injected in the same manner. To identify the progression of MIA-induced arthritis, the animals were euthanized at 1 or 3 weeks post-injection. Tissue sections, including load-bearing area of medial femoral condyles, were harvested, cut, stained with Safranin-O fast-green, and histologically assessed by using the Mankin and Osteoarthritis Research Society International (OARSI) scores (Table 1).22,23
Implantation of the chondrocyte cell sheets
A total of 36 SD rats (72 knees) aged 8 weeks were used. The surgical intervention was performed 1 (1 w-MIA models) or 3 weeks (3 w-MIA models) after the MIA injection (Fig. 1). Intra-peritoneal injections of ketamine (1.4 mL/kg of body weight) and xylazine (0.4 mL/kg of body weight) were used for anesthesia. The medial parapatellar approach was used with the patella shifted laterally to expose the medial femoral condyle. To make the experiment as clinically relevant as possible, a 1 × 3 mm area of cartilage was removed by a curette from the load-bearing area of the medial femoral condyles. The cartilage was uniformly removed until the subchondral bone was exposed, but without damaging the bone. Next, the animals in the 1 w- and 3 w-MIA model were each randomly divided into three subgroups. In the removal (R) group, only cartilage removal was performed. In the removal + drilling (RD) group, the cartilage removal was followed by subchondral drilling (five holes) into the bed of the lesion by using a 25G needle until bleeding occurred. In the removal + drilling + sheet transplantation (RDS) group, the removed cartilage area was covered with a 2 × 4 mm size of triple-layered chondrocyte cell sheet without any suture (Fig. 2). After the surgical intervention, all of the rats were returned to their cages and allowed to move freely.
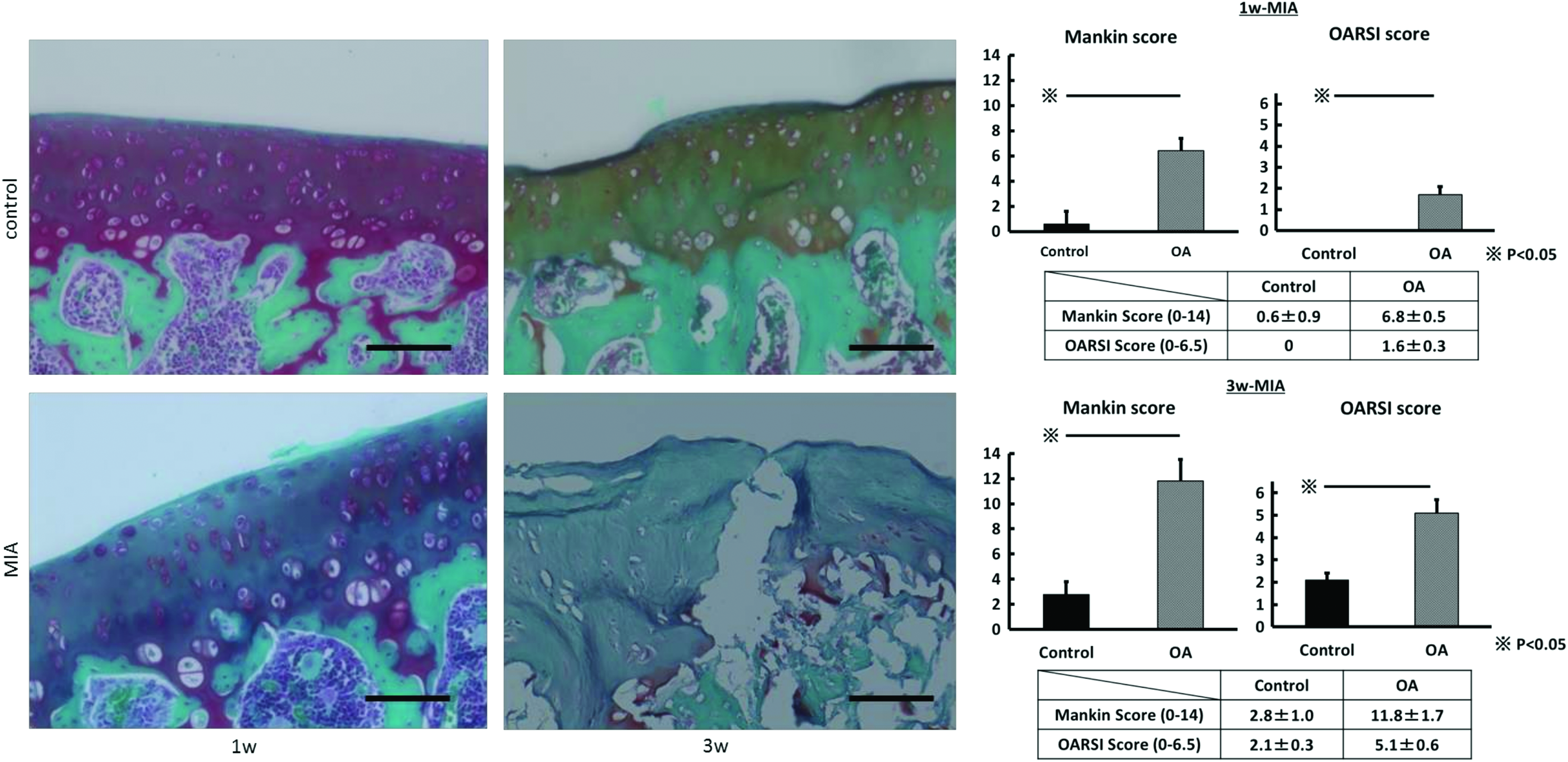
Histology images and Mankin/OARSI scores for the control versus osteoarthritis groups in the 1 w- and 3 w-MIA models; Scale bar = 100 μm. MIA, monoiodoacetate. 1 w, 1 week; 3 w, 3 week; OARSI, Osteoarthritis Research Society International. Color images available online at
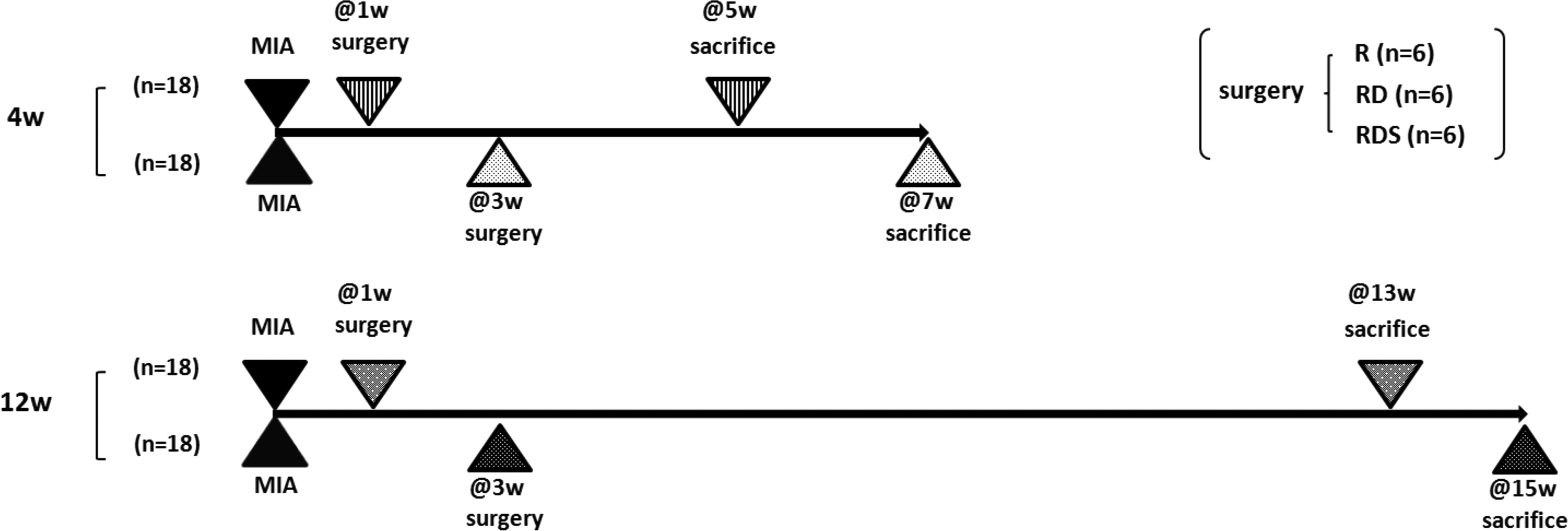
Protocol for each experimental group.
Macroscopic and histological assessment
Half of the rats from each group were sacrificed at 4 weeks after surgery (Fig. 2). The femoral condyles were dissected en bloc and evaluated by using a macroscopic scoring system established by Wayne et al. 24 ranging from 0 (worst) to 16 (best) points. Next, the medial femoral condyles were fixed in 4% paraformaldehyde phosphate-buffered saline (Wako Pure Chemical Industries Ltd., Osaka, Japan) for 24 h and then decalcified in distilled water containing 10% ethylenediaminetetraacetic acid for 3 weeks. The tissue was frozen and cryosectioned in a cryostat to 5 μm thickness along the sagittal plane, which included the mid-center of intervened medial femoral condyles. Each section was stained by Safranin-O fast-green for histological evaluation. Scoring was performed by using the modified International Cartilage Repair Society (ICRS) score, which ranges from 11 (worst) to 45 (best) points (Table 2).11,23,25,26
This system evaluates repair tissue based on the following 11 items. The total scores range from 11 to 45.
The sections were examined immunohistochemically by using monoclonal antibodies against GFP protein to determine the origin of the repair tissue. They were permeabilized with 0.2% Tween 20 at 4°C for 30 min, and Protein Block Serum-Free (Dako Japan, Inc., Tokyo, Japan) was used for 30 min to block nonspecific binding of immunoglobulins. The sections were incubated with an antibody against GFP (1:250; ab6662; Abcam, Cambridge, United Kingdom) overnight at 4°C. Finally, they were rinsed in phosphate-buffered saline, counterstained with 4′,6-diamidino-2-phenylindole, and analyzed under fluorescent microscopy.
To assess the long-term therapeutic effects, the second half of the rats from each group were sacrificed at 12 weeks after the surgical intervention and assessed both macroscopically and histologically (Fig. 2). The sections were scored separately by two examiners who were blinded to the group labels.
Cell-sheet localization using the in vivo imaging system
The layered chondrocyte cell sheets were fabricated by an aforementioned strategy by using chondrocytes harvested from 4 week-old SD rats. In addition, the cell sheets were labeled with XenoLight DiR (Perkin Elmer, Inc., Boston, MA) according to the manufacturer's instructions for in vivo imaging.
A total of six SD rats (12 knees) aged 8 weeks were used. They were divided into two RDS groups in the 1 w- and 3 w-MIA model. Then, transplanted chondrocyte cell sheets at the medial femoral condyle were visualized by in vivo imaging on an in vivo imaging system (IVIS) (Perkin Elmer, Waltham, MA). Living Image 4.3.1 software was used to analyze the images, and the filters were set to 710 nm for excitation and 760 nm for emission. The in vivo fluorescent images were acquired on postoperative days 0, 1, 3, 7, 14, and 28. The fluorescent signal intensity was measured in the knee by selecting a region of interest (ROI). The ROI was located on the cartilage removed area at the medial femoral condyle, and it was kept constant at the same scale for all samples.
Statistical analysis
The results are expressed as mean ± standard deviation for each parameter examined. Unpaired t-tests were used to analyze the histological comparisons between the MIA and control groups, as well as between 1 w-MIA and 3 w-MIA. One-way analysis of variance (ANOVA) tests followed by individual post hoc Fisher's protected least significant difference (PLSD) tests were used to analyze the macroscopic and histological assessments of each specimen in each experimental group. The fluorescent signal intensity in the in vivo imaging was statistically analyzed by using the repeated-measures ANOVA followed by individual post hoc Fisher's PLSD tests. p-Values <0.05 were considered statistically significant.
Results
Properties of the chondrocyte cell sheets
The triple-layered chondrocyte cell sheets formed three-dimensional structures with an abundant extracellular matrix that showed strong Safranin-O staining (Fig. 3a). The fluorescent signal from the GFP cell sheets was detected under fluorescent microscopy (Fig. 3b).

Histology images of a triple-layered chondrocyte cell sheet;
Histology of the MIA-induced arthritis model
In the 1 w-MIA group, the Safranin-O staining intensity was markedly reduced and the number of chondrocytes was decreased compared with those in the control group. In the 3 w-MIA group, the Safranin-O staining intensity was markedly reduced, the number of chondrocytes was decreased, and the surface of articular cartilage was damaged by deep fissures compared with those of the control group (Fig. 1). The histological assessment of the 1 w-MIA group using the Mankin and OARSI scores was significantly worse than that of the 1 w-Control group (p < 0.05). Similarly, the scores of the 3 w-MIA group were significantly worse than those of the 3 w-Control group (p < 0.05; Fig. 1). Further, the scores in the 3 w-MIA group were significantly worse than those in the 1 w-MIA group (p < 0.05). Thus, both OA groups showed significant degeneration of the articular cartilage, which progressed with time.
Macroscopic assessment
Four weeks after the surgical intervention, exposed subchondral bone and spur formation were observed in group R and little scar tissue had filled the defect in group RD, whereas some regenerated tissue resembling healthy cartilage was seen in groups RDS. On the gross appearance grading scale for the 1 w-MIA models, there was no significance among three groups. In the 3 w-MIA model, the RDS group showed significantly better scores than the other groups (p < 0.05) (Fig. 4A).
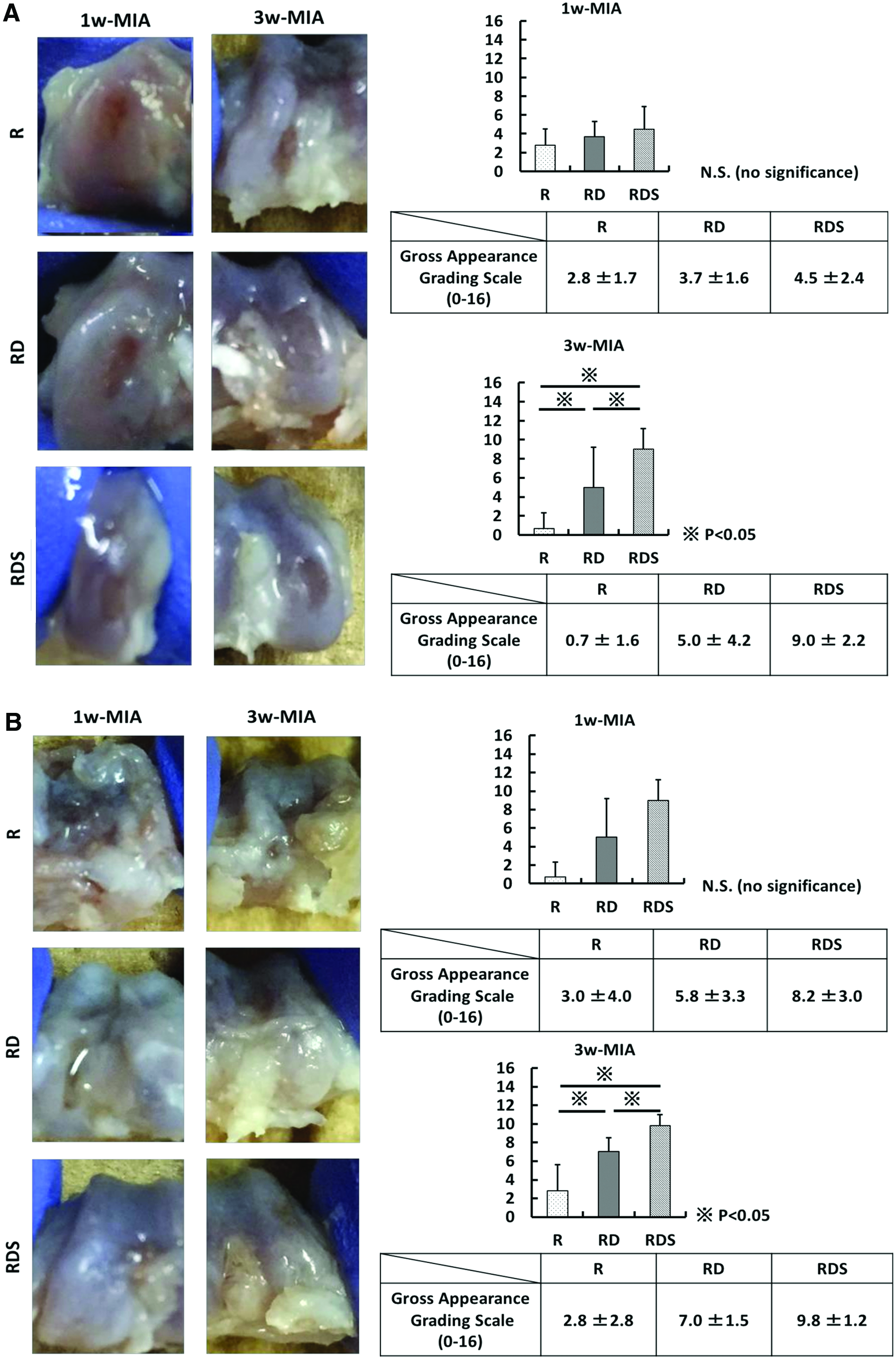
Macroscopic images (left) and gross appearance grading scale scores (right) for each group in the 1 w- and 3 w-MIA models at
Twelve weeks after the surgical intervention, severe deformity and spur formation were observed in group R and small amounts of scar tissue had filled the defect in the RD group, whereas some regenerated tissue was seen in the RDS group. On the gross appearance grading scale for the 1 w-MIA models, there was no significance among three groups. In the 3 w-MIA model, the RDS group had significantly better scores than the other groups (p < 0.05) (Fig. 4B).
Histological assessment
The histological findings were evaluated at 4 and 12 weeks after surgery (Fig. 2). At 4 weeks after surgery in the 1 w-MIA models, in the RDS group, the lesion was partially filled with hyaline-like cartilage that contained abundant glycosaminoglycans indicated by Safranin-O, but it was mostly covered by fibrous cartilage showing an absence of Safranin-O staining. In the R and RD groups, the lesions contained only fibrous tissue. At 4 weeks after surgery in the 3 w-MIA models, the lesion was largely covered by fibrous cartilage in the RDS group. In the R and RD groups, severe deformities and surface irregularities were observed (Fig. 5A). The modified ICRS scores for the 1 w-MIA models showed that the RDS groups had significantly better scores than the R and RD groups (p < 0.05). The scores for the 3 w-MIA models showed that the RDS groups had significantly better scores than the R and RD groups (p < 0.05) (Fig. 5A). There was no significance between the scores of the RDS groups in 1 w-MIA models and 3 w-MIA models.
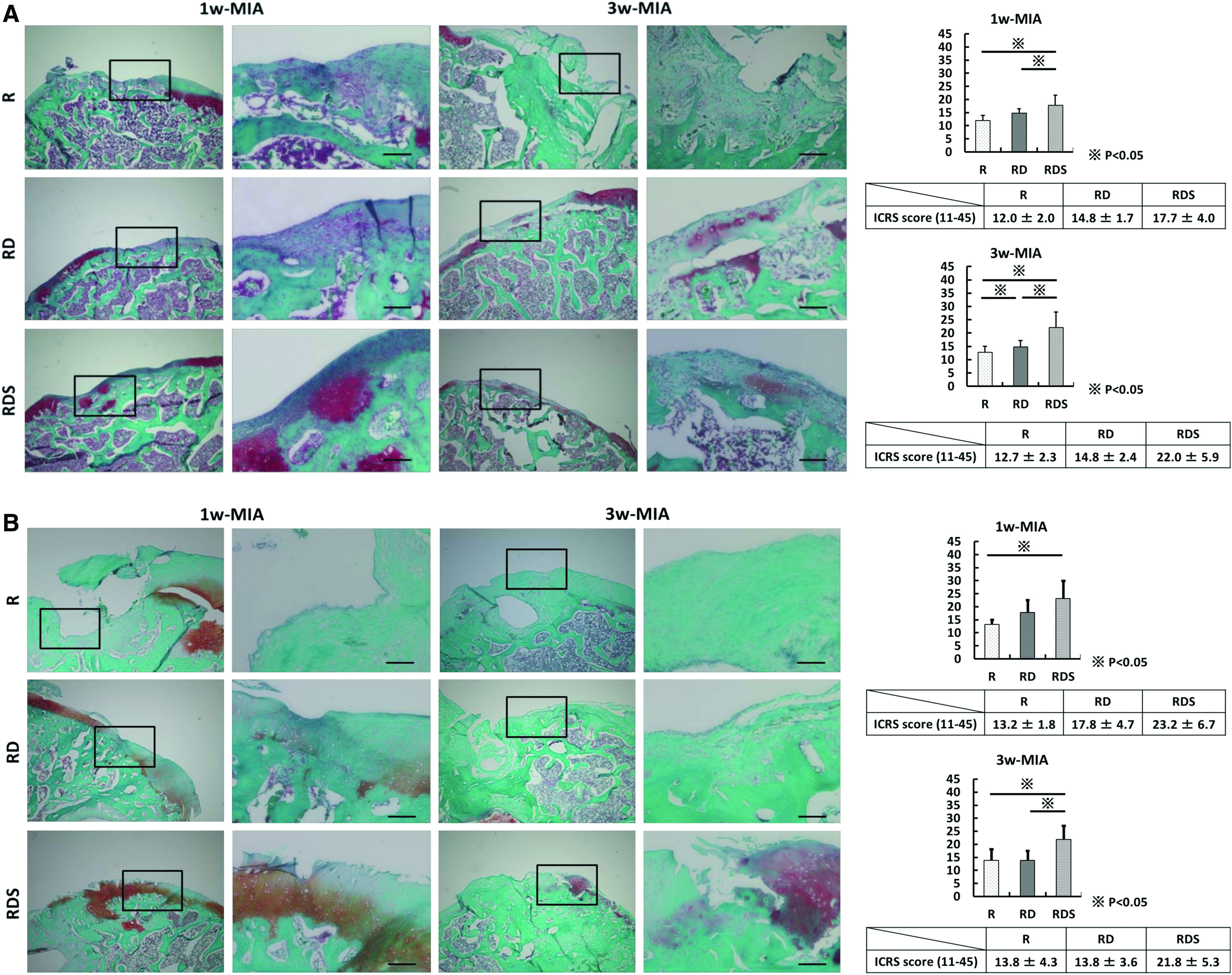
Histological images (left) and modified International Cartilage Repair Society scores (right) for each group in the 1 w- and 3 w-MIA models at
At 12 weeks after surgery in the 1 w-MIA models, the lesion was partially filled with hyaline-like cartilage, but it mostly contained fibrous cartilage in the RDS group. In the R and RD groups, severe deformities and surface irregularities were observed. At 12 weeks after surgery in the 3 w-MIA models, the lesion was partially filled with hyaline-like cartilage, but it was mostly covered by fibrous cartilage in the RDS group. In the R and RD groups, severe deformities and surface irregularities were observed (Fig. 5B). The modified ICRS scores for the 1 w-MIA models showed that the RDS groups had significantly better scores than the R groups. The scores for the 3 w-MIA models showed that the RDS groups had significantly better scores than the RD and R groups (p < 0.05) (Fig. 5B; Table 3). There was no significance between the scores of the RDS groups in 1 w-MIA models and 3 w-MIA models.
MIA, monoiodoacetate; R, removal; RD, removal + drilling; RDS, removal + drilling + sheet transplantation.
Localization of the transplanted cell sheets
The in vivo fluorescence imaging detected the fluorescent signal from the transplanted cell sheets in the knee joints until day 28 in the RDS group of 1 w- and 3 w-MIA models. Although the fluorescent signal intensities were not significantly different between them, the intensity in the 3 w-MIA model tended to be higher than that in the 1 w-MIA model over time (Fig. 6). On the one hand, no GFP signal was detected in the repaired cartilage under fluorescent microscopy in all specimens.
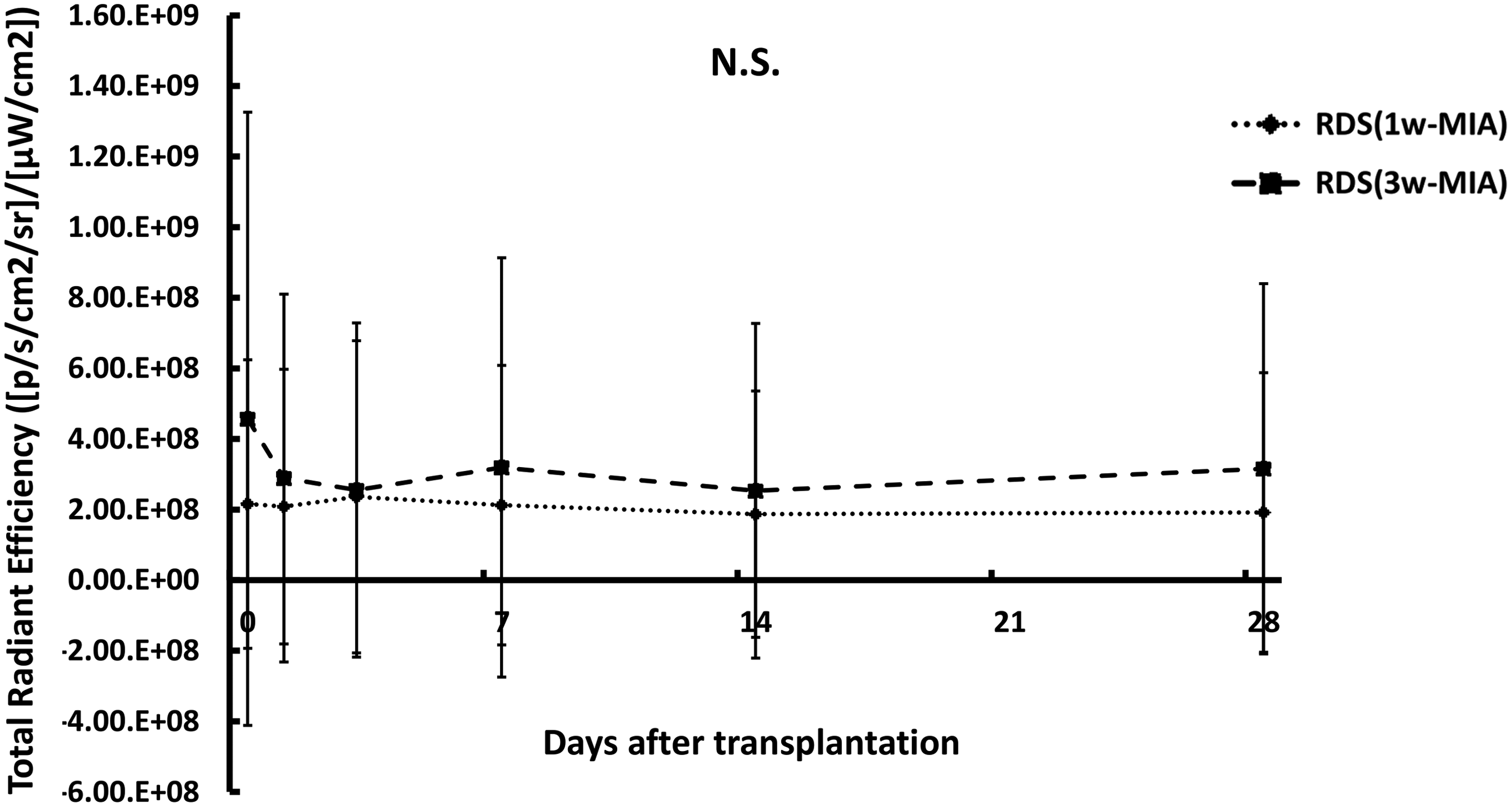
Fluorescent signal intensities from the transplanted cell sheets were detected in the knee joints until day 28 in each group in the 1 w- and 3 w-MIA models. However, there was no significant difference between 1 w-MIA and 3 w-MIA models.
Discussion
In the present study, we assessed the utility of engineered chondrocyte cell sheets for treating diffusely degenerated articular cartilage in an MIA-induced arthritis animal model. The chondrocyte cell-sheet transplantation led to significant repair of diffusely degenerated articular cartilage. This is the first article showing the therapeutic potential of chondrocyte cell sheets for MIA-induced arthritis models.
At 4 and 12 weeks after the surgery, gross appearance of the RDS group in the 3 w-MIA model was significantly better than the other groups. A relatively smooth articular surface and some regenerated tissue were detected in the RDS groups. In contrast, bony spur formation, partial subchondral bone exposure, and articular surface irregularities were seen in the R and RD groups. Although there was no significance, the gross appearance of the RDS group in the 1 w-MIA model showed better scores than the other groups at 4 and 12 weeks after the surgery (Fig. 4). The histological assessments of the RDS group in 1 w- and 3 w-MIA models at 4 and 12 weeks after surgery were significantly better than those of the R and RD groups (Fig. 5). These results suggest that the cell-sheet transplantation induces repair of the articular cartilage at the cartilage removed area. Several previous studies have reported successful articular cartilage regeneration by using cell sheets in partial- and full-thickness cartilage defect models.11,13 In such defect models, the articular cartilage surrounding the cartilage defect is essentially histologically normal. In the present study, we also created a cartilage defect by partially removing the degenerated cartilage in an MIA-induced arthritis model. Even though the articular cartilage surrounding the cartilage in our model was histologically and diffusely degenerated, transplantation of the chondrocyte cell sheets induced repair in the cartilage defect area. These results indicate the therapeutic potential of chondrocyte cell sheets not only for focal cartilage defects but also for diffusely degenerated articular cartilage. The advantages of cell-sheet technology include that they are easy to culture and expand and they can adhere well to the surface of cartilage. Because of their adhesiveness, they were previously assumed to work as a barrier that protects the defect site from the catabolic factors present in the joint fluid and that sequesters the progenitor cells from the bone marrow and adjacent cartilage, leading to good cartilage repair.11–13,19
To understand how chondrocyte cell sheets improve cartilage repair, it is necessary to assess the survivability and role of the transplanted cells and to determine the origin of repair tissue. However, the origin of the regenerated cartilage remains controversial. In a previous study by our group, 27 we determined the location of the transplanted cell sheets histologically by using GFP in a rat articular cartilage defect in a patellofemoral joint model and revealed that a large portion of the regenerated tissue was derived from the transplanted cell sheet itself. We also tried to determine the location of the transplanted cell sheets by using the IVIS imaging system and immunohistological assessments with an anti-GFP antibody. Because of the good adhesive ability of cell sheets, 17 they should adhere to the transplanted site and not be peeled off by repetitive load bearing and the mechanical forces that accompany knee joint motion, even when transplanted without any suture. Although the fluorescent signal was detected in the knee joints through day 28, no GFP-positive cells were found in the regenerated cartilage in both 1 w- and 3 w-MIA models under fluorescent microscopy. Therefore, the regenerated tissue was not derived from the transplanted cell sheet itself. It is possible that the difference of the transplanted site of load-bearing or non-load-bearing joint, or that integration between implanted tissue and the adjacent cartilage matrix was insufficient for adhesion because of the unique matrix organization of cartilage. 28 Several researchers have previously demonstrated the advantages of layered cell sheets. Takaku et al. 19 reported that only a small number of bioengineered chondrocytes at or near the surface of the cartilage layer induced the recipient cells to drive cartilage regeneration. Kaneshiro et al. 17 reported that layered cell sheets have a stronger chondroprotective effect than single-layer cell sheets. Layered chondrocyte cell sheets showed higher expression levels of Sox 9, integrin α10, Col 2 and 27, TGF-β, and PGE2 than single-layered chondrocyte cell sheets. In addition, the expression of catabolic factors such as MMP3, MMP13, and ADAMTS5 was decreased at the time of layering, whereas the expression of TIMP1, an inhibitor of MMP3, was increased.6,12 Therefore, we suspect that the cell sheet secreted humoral factors that prevented the further degeneration of the articular cartilage or accelerated biological cartilage regeneration.
We used an MIA-induced arthritis model for treating diffusely degenerated articular cartilage in this study. Surgically induced articular cartilage degeneration models, including the anterior cruciate ligament transection (ACLT) or meniscal transection (MNX), have been commonly used.29,30 In these models, the results are highly reproducible and progress rapidly, so that these are useful for short-term studies.26,31,32 However, we preferred the MIA-model over the ACLT- or MNX-models since in the latter continuous severe mechanical instability further deteriorates articular cartilage and could prevent cartilage regeneration even when cell sheets are applied.
In this study, we selected the Mankin and OARSI scores for the histological assessment of articular cartilage degeneration induced by MIA, and the modified ICRS scores for the assessment of articular cartilage repair. The Mankin score is quantitative, but it is used to quantify the severity of the OA and does not evaluate the natural repair process. 22 The OARSI OA cartilage histopathology assessment system is based on the histologic features of OA progression. 23 However, these histological scoring systems are inadequate for assessing the efficacy of therapeutic intervention for MIA-induced arthritis models. On the contrary, the modified ICRS histological grading system was previously used to assess the regeneration of articular cartilage.11,23,25,33
Here, we demonstrated the effects of engineered cell sheets in an MIA-induced arthritis model. We expect that these treatment methods would be effective not only for early staged degeneration of articular cartilage but also for relatively progressed degeneration, which were represented by the 1 w-MIA and 3 w-MIA models. To our knowledge, until now, based on a literature search no reports have shown any effective treatment options for diffusely degenerated articular cartilage models. Although Zhou et al. 32 and Van Buul et al. 34 tried to treat MIA-induced degenerative articular cartilage by using bone marrow-derived MSCs, there were no apparent effects of the treatment on the structural damage and synovial inflammation except for a reduction in MIA-induced pain. Therefore, this study might be the first report showing a novel treatment option using cell transplantation for MIA-induced arthritis models with diffusely degenerated articular cartilage.
Scaffold-free tissue engineering without growth factors is a desirable option for regenerative medicine. Previously, Ohki et al. 8 showed successful endoscopic epithelial cell-sheet transplantation for preventing esophageal strictures after endoscopic submucosal dissection for esophageal neoplasm. Performing chondrocyte cell-sheet transplantation arthroscopically would make the method less invasive. A simple cell injection can be used for repair of focal osteochondral defects, whereas engineered cell sheets can be applied not only for focal lesions but also for large osteoarthritic lesions because the transplanted cell sheets maintain their form. However, several problems remain to be solved. Autologous chondrocyte transplantation requires two surgeries for the collection of chondrocytes before in vitro culture of the cells to fabricate a cell sheet and a subsequent surgery for cell-sheet transplantation. This procedure requires the sacrifice of relatively normal articular cartilage. In the present study, we show the therapeutic potential of an allograft chondrocyte cell sheet in SD rats. Although further experiments are needed to examine the immune reaction after transplantation of the allograft chondrocyte cell sheets, allografting could potentially solve the problem of donor site morbidity. Despite these limitations, we conclude that the transplantation of chondrocyte cell sheets represents a promising treatment option for diffusely degenerated articular cartilage.
Footnotes
Author's Contributions
S.H.: Collection and assembly of data, data analysis and interpretation, and article writing; N.K.: Conception and design, collection and assembly of data, data analysis and interpretation, and article writing; Y.I., R.S., and M.I.: Collection and assembly of data, data analysis and interpretation; N.A.: Collection and assembly of data, data analysis and interpretation, and final approval of the article; and M.O.: Conception and design, data analysis and interpretation, and final approval of the article. The corresponding author acknowledges that all authors have read and approved this article.
Acknowledgment
This work was supported in part by a grant-in-aid to M.O. for scientific research from the Ministry of Education, Culture, Sports, Science and Technology Japan (no. 25253089).
Disclosure Statement
No competing financial interests exist.